Massimo Puoti Dept of Infectious Diseases ASST Grande Ospedale Metropolitano Niguarda Milano Pre-workshop Education Course Evaluation of End-stage Liver Disease 12th Co-infection Workshop 2016 2 Jun 2016 - 3 Jun 2016 Berlin, Germany
Transcript
Massimo Puoti
Dept of Infectious Diseases
ASST
Grande Ospedale Metropolitano Niguarda
Milano
Pre-workshop Education Course
Evaluation of End-stage Liver Disease
12th Co-infection Workshop 20162 Jun 2016 - 3 Jun 2016
Berlin, Germany
Disclosures
Massimo Puoti acted
• in a consultancy capacity for Abbvie, BMS, BoehringerIngelheim, Janssen, GSK, ViiV, Gilead Sciences, MSD
• as a speaker at company-sponsored events for Abbvie, BMS, Boehringer Ingelheim, Janssen, Gilead Sciences, GSK, ViiV, Roche, Roche Diagnostics, MSD, Beckman,
During this lecture data on not licensed products and on off labeluse of licensed products will be discussed
Causes of death in the Swiss HIV Cohort
study 2005-09
Ruppik M. et al. Changing patterns of causes of death in the SHCS 2005-2009. CROI 2011.
Poster # 789. Available at: http://www.retroconference.org/2011/PDFs/789.pdf.
ESLD: definition
• End-stage liver disease (ESLD) is the final decompensationphase in the liver trajectory.
• It is characterized by episodic, acute exacerbations, oftenrequiring hospitalization.
• Life-threatening complications, such as varicealhemorrhage or hepatoma, combine with multiple debilitating symptoms, including ascites, extreme fatigue, pruritus, and cachexia.
• Patients may also experience cognitive decline, rangingfrom mild chronic impairment to severe hepaticencephalopathy and coma.
• Many suffer from psychological distress and depression.
Boyd K et al Hepatology 2012
Diagnosis of Cirrhosis:
the pieces of the puzzle
Blood Tests & US
Fibroscan
Physical examBiopsy
Progression of Cirrhosis
Compensated Advanced ChronicLiver Disease
Liver Stiffness:< 10 not not probable
10-15 suggestive>15 highly suggestive
Metavir F4
Ishak S 5-6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4 Ishak S 6
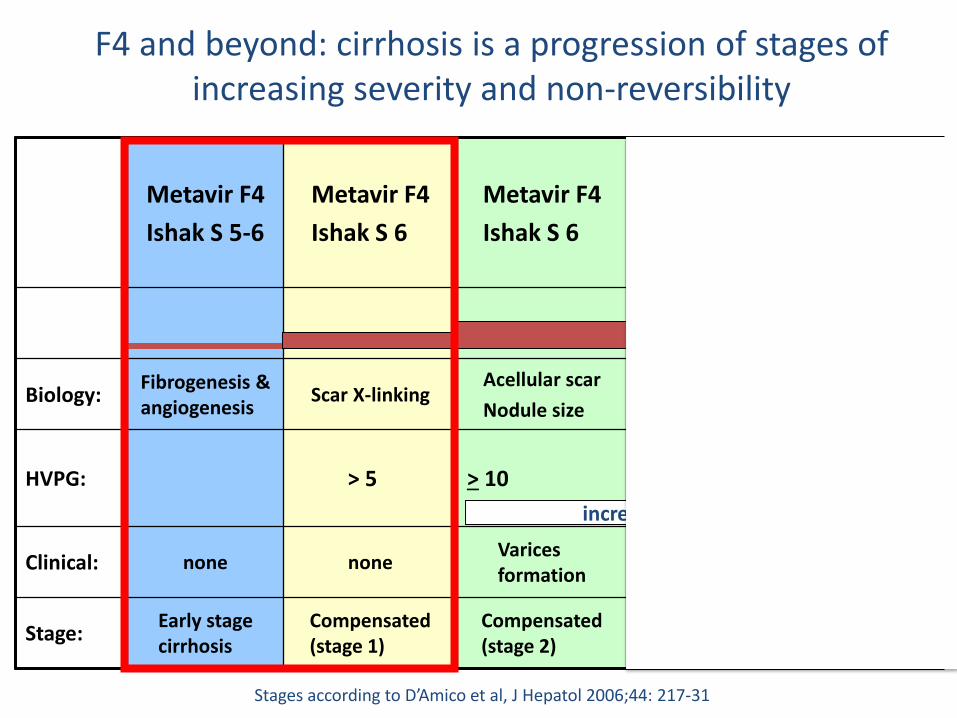
Biology:Fibrogenesis & angiogenesis
Scar X-linkingAcellular scar
Nodule size
Insoluble scar & small nodules
Scars & large nodules
HVPG: > 5 > 10 > 12 > 12
Clinical: none noneVarices formation
Ascites
(without VH)
VH
(+ ascites)
Stage:Early stage cirrhosis
Compensated (stage 1)
Compensated (stage 2)
Decompensated (stage 3)
Decomp(stage 4)
Stages according to D’Amico et al, J Hepatol 2006;44: 217-31
F4 and beyond: cirrhosis is a progression of stages of increasing severity and non-reversibility
increasing vasodilatation
Evaluation of End Stage Liver Disease
• Diagnosis of Cirrhosis
– HCVRNA + - TE + Blood Tests + US
Increased intrahepatic resitance is the initial mechanism leading toPortal hypertension in Cirrhosis
Fibrous tissue
Regenerative Nodules
Vasoconstriction
Microthrombi?
PORTAL HYPERTENSION
Increased Resistance
Varices
HVPG
HVPG (hepatic vein-portal pressuregradient), measuredby an interventionalradiologist = difference betweenthe free hepatic veinpressure and the wedged hepatic veinpressure
> 20 mmHg Treatment failure and mortality in acute variceal bleeding
Hepatic Venous Pressure Gradient as a predictor of decompensation in Cirrhosis
Ripoll et al Gastroenterology 2007
Liver Stiffness Measurement by
Transient Elastometry (FibroScan®)
• Stiffness in KPa median of 5-10 determination with IQR
• Measurement with IQR > 30% lower validity
• No reference “normal” range
• High intra and interobserver agreement (0.98) between trained physicians or nurses (training=100 tests) 1
• Pheasibility is influenced by BMI and steatosis 1
• Results could be biased by:– the extent of necroinflammatory activity 2,3
– Macronodular pattern of cirrhosis and perisinusoidal fibrosis4
• Reflects the elevation of portal pressure: correlation with LSM if HVPG < 10 mmHg4
1 Fraquelli M et al. Gut 2007; 2 Coco B et al J Viral Hepatitis 2007; 3 Arena U et al
Hepatology 2008;4 Ganne-Carriè N et al. Hepatology 2008; 4 Vizzuti Hepatology 2007
Liver stiffness as a predictorof HVPG levels and of CSPH
The Portal Hypertesive state is enhanced becausean increase in portal venous inflow
Fibrous tissue
Regenerative Nodules
Vasoconstriction
Microthrombi?
PORTAL HYPERTENSION
Increased Resistance
Varices
Splancnic vasodilation Increased blood flow
Effective Hypovolemia
Activation NeurohumoralSystem
Sodium & Water retentionHypervolemia
Increased Cardiac Output
Metavir F4
Ishak S 5-6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4 Ishak S 6
Biology:Fibrogenesis & angiogenesis
Scar X-linkingAcellular scar
Nodule size
Insoluble scar & small nodules
Scars & large nodules
HVPG: > 5 > 10 > 12 > 12
Clinical: none noneVarices formation
Ascites
(without VH)
VH
(+ ascites)
Stage:Early stage cirrhosis
Compensated (stage 1)
Compensated (stage 2)
Decompensated (stage 3)
Decomp(stage 4)
Stages according to D’Amico et al, J Hepatol 2006;44: 217-31
F4 and beyond: cirrhosis is a progression of stages of increasing severity and non-reversibility
increasing vasodilatation
Progression of Cirrhosis
Compensated Advanced ChronicLiver Disease
Not Clinically Significant Portal Hypertension (HVPG <10 mmHg) Liver Stiffness < 20KPa & PLT > 150.000No US signs of portal hypeertension No Need EGDS repeat Blood Tests & TE at laest yearly
Clinically Significant Portal Hypertension (CSPH) Liver Stiffness > 20 Kpa &/or PLT < 150000 need for EGDS
Without Varices surveillanceWith Varices
Small folllow upLarge treatment
Liver Stiffness:< 10 not not probable
10-15 suggestive>15 highly suggestive
Progression of Cirrhosis
Compensated Advanced ChronicLiver Disease
No CSPH
CSPH
Without Varices
With Varices
Liver Stiffness:< 10 not not probable
10-15 suggestive>15 highly suggestive
1%*
3%*
* 5 years mortality
Baveno VI conference on Portal Hypertension:Surveillance of Oesophageal Varices
ScreeningEndoscopy Results
Liver Disease Stage
Ongoing Liver damage
Follow up EGDS intervals
Treatment
Negative No CSPH/CSPH w/o Varices
Yes 2 years None
Negative No CSPH/ CSPH w/o Varices
No 3 years None
Small Varices CSPH with varices
Yes 1 year None
Small Varices CSPH with varices
No & no cofactors
2 years None
Medium or Large Varices
CSPH with Varices
Any 1 year NSBB or Carvediolol or
EBL
CSPH: Clinically Significant Portal Hypertension. NSBB: Non Specific Beta Blockers EBL Endoscopic Band Ligation
Reducing portal pressure by treating Eeiologyand reducing Increased Resistance and by reducing portal flow
Fibrous tissue
Regenerative Nodules
Vasoconstriction
Microthrombi?
PORTAL HYPERTENSION
Increased Resistance
Varices
Splancnic vasodilation Increased blood flow
Effective Hypovolemia
Activation NeurohumoralSystem
Sodium & Water retentionHypervolemia
Increased Cardiac Output
NSBB or Carvediole
Etiological Treatment
1 block
2 block
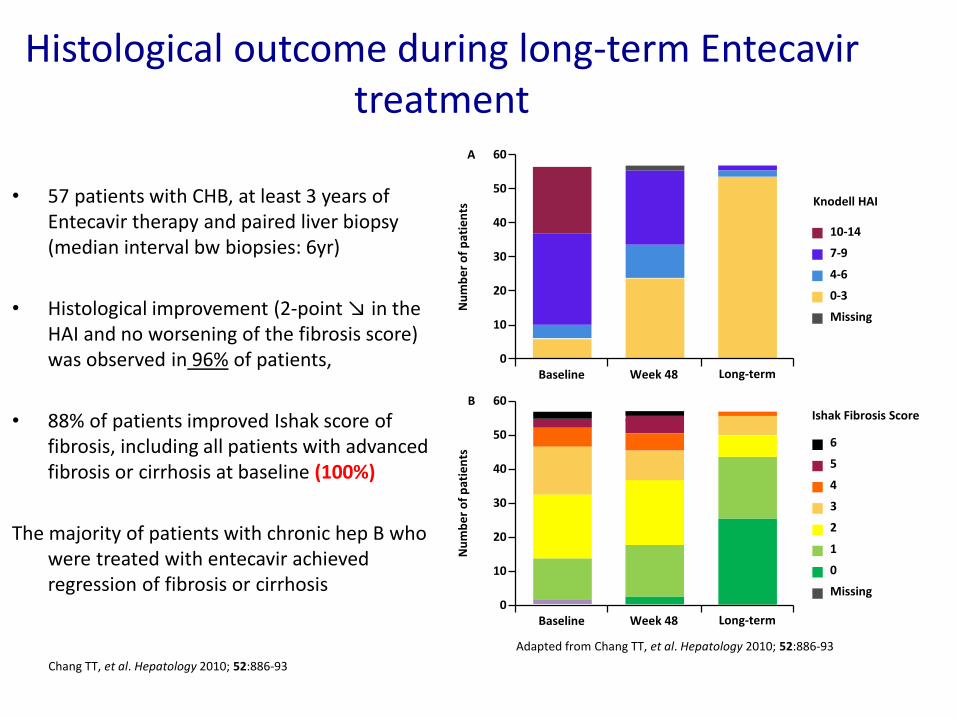
Histological outcome during long-term Entecavir treatment
• 57 patients with CHB, at least 3 years of Entecavir therapy and paired liver biopsy (median interval bw biopsies: 6yr)
• Histological improvement (2-point ↘ in the HAI and no worsening of the fibrosis score) was observed in 96% of patients,
• 88% of patients improved Ishak score of fibrosis, including all patients with advanced fibrosis or cirrhosis at baseline (100%)
The majority of patients with chronic hep B who were treated with entecavir achieved regression of fibrosis or cirrhosis
Chang TT, et al. Hepatology 2010; 52:886-93
Adapted from Chang TT, et al. Hepatology 2010; 52:886-93
0
10
20
30
40
50
60
Baseline Week 48 Long-term
Nu
mb
er
of
pat
ien
ts
B
0
10
20
30
40
50
60
Baseline Week 48 Long-term
Nu
mb
er
of
pat
ien
ts
A
Knodell HAI
10-14
7-9
4-6
0-3
Missing
Ishak Fibrosis Score
6
5
4
3
2
1
0
Missing
Distribution of Metavir fibrosis stages in pre-treatment and post-treatment liver biopsies
61% patients with F4 at baseline had cirrhosis regressionto lower METAVIR stages
F4
F3
F2
F1
Pre-treatment Post-treatment
38 2 (5%)
7 (18%)
14 (37%)
15 (39%)
Nu
mb
er
of
pati
en
ts
4
0
2
0
1
0
3
0
0
D’Ambrosio et al Hepatology. 2012
Area of fibrosis (%)
Baseline Bx After SVR
0
2.5
5
7.5
10
12.5
15
17.5
20
22.5
25
Morphometry 1 Morphometry 2
• 38 patients, Hepatitis C cirrhosis, Child-Pugh A
• 24/48 weeks standard bitherapy and SVR
• Paired biopsy, mean interval : 6 years
Effect of SOF+RBV on Hepatic Venous Pressure Gradient
SOF+RBV in Compensated and Decompensated Cirrhotics with Portal Hypertension
SOF + RBV
Observation
Week 0 24 48 9672
Arm 1
n=25
Arm 2
n=25
HVPG Assessment
RBV 1000–1200 mg
Arm 1n=25
Arm 2n=25
All With Paired HVPG n=37
Male, n (%) 18 (72) 20 (80) 28 (76)
Mean age, y (range) 55 (43–69) 56 (44–69) 55 (44–69)
There were clinically meaningful improvements in portal hypertension in addition to improvements in liver biochemistry, CTP and MELD scores
The effect of SVR12 and viral suppression on HVPG is being monitored at 1 year post-treatment
Observation Period in Patients with BL HVPG ≥12 mmHg* (24 weeks)
Changes After Treatment in Patients with BL HVPG ≥12 mmHg (n=33)
SOF+RBV in Compensated and Decompensated Cirrhotics with Portal Hypertension
-30
-20
-10
0
10
20
30
40
n=2
HV
PG
Ch
ange
(%
) n=2a
30
20
10
0
-10
-20
-30
-40
-50
-60
-70
-80H
VP
G C
han
ge (
%)
Patients with >20% decrease (8/33)
Baseline MELD Score <10 ≥10
aPatients with HVPG ≤12 mm Hg at end of treatment
*No patient had HVPG ≤12 mm Hg at end of observation period
HVPG = hepatic venous pressure gradient A reduction in HVPG ≥20% or below the 12-mm Hg threshold markedly reduces the risk of variceal bleeding, and varices may decrease in size
a a a
Evaluation of End Stage Liver Disease
• Diagnosis of Cirrhosis
• Diagnosis of Portal Hypertension and Esophageal Varices
– US
– HVPG ( restricted to small subgroups)
– EGDS
• F1 (small) +/-red signs
• F2 (medium) +/-Red Signs
• F3(large) +/-Red Signs
Metavir F4
Ishak S 5-6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4
Ishak S 6
Metavir F4 Ishak S 6
Biology:Fibrogenesis & angiogenesis
Scar X-linkingAcellular scar
Nodule size
Insoluble scar & small nodules
Scars & large nodules
HVPG: > 5 > 10 > 12 > 12
Clinical: none noneVarices formation
Ascites
(without VH)
VH
(+ ascites)
Stage:Early stage cirrhosis
Compensated (stage 1)
Compensated (stage 2)
Decompensated (stage 3)
Decomp(stage 4)
Stages according to D’Amico et al, J Hepatol 2006;44: 217-31
F4 and beyond: cirrhosis is a progression of stages of increasing severity and non-reversibility
increasing vasodilatation
Progression of Cirrhosis
Compensated Advanced ChronicLiver Disease
DecompensatedCirrhosis
Variceal Haemorrage
One Non Bleeding Complications AscitesHepatic Encephalpathy
Two Complications
20%*
30%*
88%*
* 5 years mortality
Cirrhosis: Diagnosis of complicationsAscites
• Identification: US and Physical exam
• Evaluation: Paracentesis ( First Episode or Suspect of Spontaneous Bacterial Peritonitis)
• Classification– Not Complicated
• Mild ( Volume & Diuretic Response)
• Moderate (Volume & Diuretic Response)
Cirrhosis: Diagnosis of complicationsHepatic Encephalopathy
• DEFINITION OF HE IN CIRRHOSIS Hepatic encephalopathy is a braindysfunction caused by liver insufficiency; it manifests as a wide spectrum of neurological or psychiatric abnormalities ranging fromsubclinical alterations to coma.
• According to its time course, HE is subdivided into– Episodic HE
– Recurrent HE denotes bouts of HE that occur with a time interval of 6 monthsor less.
– Persistent HE denotes a pattern of behavioral alterations that are alwayspresent and interspersed with relapses of overt HE.
• According to the existence of precipitating factors, HE is subdividedinto– Nonprecipitated or
– Precipitated, and the precipitating factors should be specified. Precipitatingfactors can be identified in nearly all bouts of episodic HE type C and should beactively sought and treated when found
Hepatic Encephalopathy: precipitating factors
Cirrhosis: Diagnosis of complicationsHepatic Encephalopathy: Grading
Evaluation of End Stage Liver Disease
• Diagnosis of Cirrhosis
• Diagnosis of Portal Hypertension and Esophageal Varices
• Diagnosis and Clasification of Complications– Non complicated Ascites:
• Identification: US, History & Physical examination
• Evaluation
– Paracentesis ( 1° Episode or Suspect of PBS)
• Grading ( volume + Diuretic response)
– Hepatic Encephalopathy
• Identification : Neuropsychological tests only in special circumstances toifdentify covert forms
• Grading: according to Physical examination and Histiry
• Classification: Time course & precipitating factors
Complications of AscitesRefractory Ascites and SBP
• REFRACTORY ASCITES is defined as fluid overload that– is unresponsive to sodium-restricted diet and highdose diuretic treatment
(400 mg per day of spironolactone and 160 mg per day furosemide), or– recurs rapidly after
• Failure of diuretic therapy may be manifested by– minimal to no weight loss together with inadequate (<78 mmol per day)
urinary sodium excretion despite diuretics, or – development of clinically significant complications of diuretics, e.g.,
encephalopathy, serum creatinine greater than 2.0 mg/dL, serum sodium lessthan 120 mmol/L, or serum potassium greater than 6.0 mmol/
• SPONTANEOUS BACTERIAL PERITONITIS dx made in the presence of an elevated ascitic fluid absolute polymorphonuclear leukocyte (PMN) count (i.e., ≥250 cells/mm3 [0.25 x 109/L]) without an evident intra-abdominal, surgically treatable source of infection
Complications of Ascites:Hepato Renal Syndrome
• Diagnostic Criteria– cirrhosis with ascites;
– serum creatinine greater than 1.5 mg/dL;
– no improvement of serum creatinine (decrease to a level of 1.5 mg/dL or less) after at least twodays with diuretic withdrawal and volume expansion with albumin (The recommended dose ofalbumin is 1 g/kg of body weight per day up to a maximum of 100 g/ d);
– absence of shock;
– no current or recent treatment with nephrotoxic drugs;
– absence of parenchymal kidney disease as indicated by proteinuria >500 mg/day, microhematuria(>50 red blood cells per high power field), and/or abnormal renal ultrasonography.
• Type I is characterized by rapidly progressive reduction in renal function as definedby a doubling of the initial serum creatinine to a level greater that 2.5 mg/dL or a 50% reduction of the initial 24-hour creatinine clearance to a level lower that 20 mL per minute in less than 2 weeks.
• Type II does not have a rapidly progressive course and is a commonly associatedwith death in patients who do not die of other complications of cirrhosis
Clinical/Biochemical Indicator
1 point 2 points 3 points
Serum bilirubin(mg/dL)
< 2 2 - 3 > 3
Serum albumin(g/dL)
> 3.5 2.8 – 3.5 < 2.8
Prothrombine time(s > control)
< 4 4 - 6 > 6
Encephalopathy(grade)
none 1 or 2 3 or 4
Ascites absent slight moderate
Points are summed, and the total score is classified according to severity as follows:
GROUP A (mild) = 5 – 6 points
GROUP B (moderate) = 7 – 9 points
GROUP C (severe) = 10 – 15 points
Child-Pugh classification and scoring of liver diseases