Behavior, Lifestyle, and Social Determinants of Heart Health: From Research to Policy, Planning, Programs & Services Lawrence W. Green Office of Extramural Prevention Research Public Health Practice Program Office Centers for Disease Control and Prevention U.S. Department of Health & Human Services York University Forum, Toronto, Feb. 20, 2003
Transcript
Behavior, Lifestyle, and Social Determinants of Heart Health: From Research to Policy, Planning, Programs &
Services
Lawrence W. Green
Office of Extramural Prevention ResearchPublic Health Practice Program Office
Centers for Disease Control and PreventionU.S. Department of Health & Human Services
York University Forum, Toronto, Feb. 20, 2003
Health Promotion, Health Protection, and Disease Prevention
Social structure,conditions
Culture, lifestyle, attitudes &
policies about risk
Risk behaviors &Environmental exposures
Adversehealth events
Health Promotion
Primary Prevention &Health Protection
Sequelae, Outcomes
Secondary Prevention Tertiary Prevention
Lesson 1. Social determinants operate as background & as distal determinants on most of the proximal determinants of health.
Self-care
Determinants of Health* More Distal More Proximal
Income & social status Gender Education Employment &
working conditions Physical environment Biology & genetic
endowment
Personal health practices & coping skills
Healthy child development
Health & social services Culture Social support networks Social environment
*Tonmyr et al., The population health perspective… Chronic Diseasesin Canada 23:123-129, Fall 2002.
Lesson 2: The Social Determinants Imperative and Opportunity
From tobacco control experience, we know that some work with other sectors and work within the health sector on more distal determinants is essential to long-term success
Many, if not most, social determinants are:– More proximal, and/or– Amenable to health sector intervention, and/or– Amenable to collaboration with other sectors
Achieving Health for All*
*Epp, Jake. Achieving health for all: a framework for health promotion. Ottawa: Minister of Supply and Services, 1986.
AIM
HEALTHCHALLENGES
HEALTHPROMOTIONMECHANISMS
IMPLEMENTATIONSTRATEGIES
REDUCINGINEQUITIES
INCREASINGPREVENTION
ENHANCINGCOPING
SELF-CARE MUTUAL AID HEALTHYENVIRONMENTS
FOSTERINGPUBLIC
PARTICIPATION
STRENGTHENINGCOMMUNITY
HEALTH SERVICES
COORDINATINGHEALTHY PUBLIC
POLICY
ACHIEVING HEALTHFOR ALL
0
1,000
2,000
3,000
4,000
5,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990
Num
ber o
f Cig
aret
tes
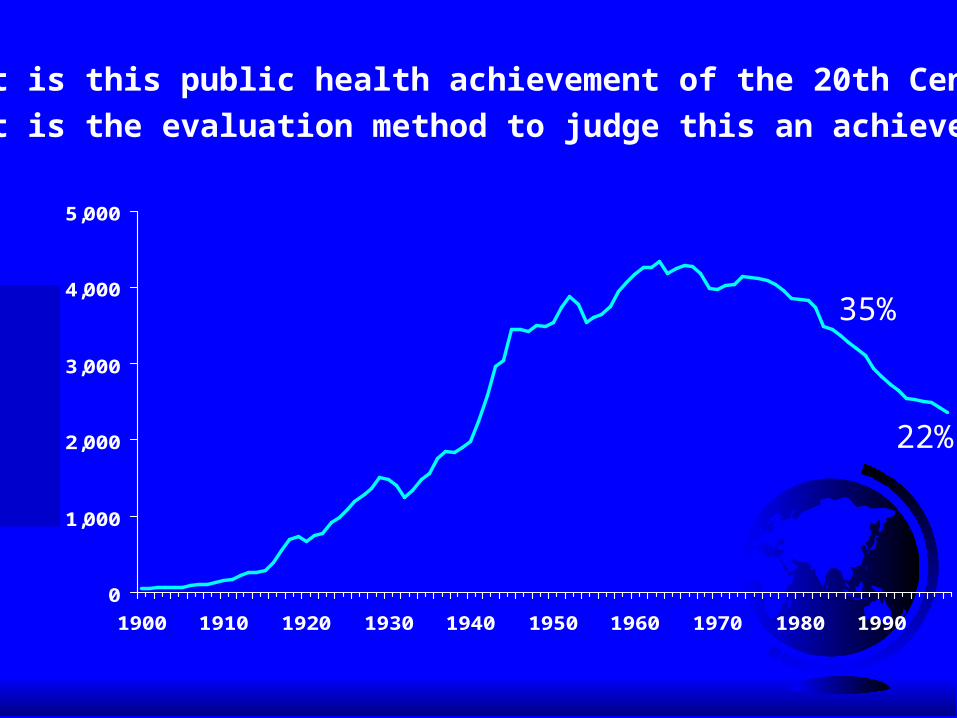
What is this public health achievement of the 20th Century?What is the evaluation method to judge this an achievement?
35%
22%
0
1,000
2,000
3,000
4,000
5,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990
Num
ber o
f Cig
aret
tes
Source: USDA; 1986 Surgeon General's Report
Great Depression
End of WW II
Nonsmokers’Rights
Movement Begins
1st SurgeonGeneral’s Report
Fairness DoctrineMessages on TVand Radio
Federal CigaretteTax Doubles
BroadcastAd Ban
Adult Per Capita Cigarette Consumption and Major Historical Events—United States, 1900-2000
MasterSettlementAgreement
NicotineMedications Available Over the Counter
1st Smoking-Cancer Concern
1st World Conferenceon Smoking and Health
Surgeon General’sReport on EnvironmentalTobacco Smoke
1st Great American Smokeout
Lesson 3: Surveillance--Making Lesson 3: Surveillance--Making Better Use of Natural ExperimentsBetter Use of Natural Experiments Key to establishing baselines & trend lines that can
be projected to warn against neglect Key to putting an issue on the public policy agenda Key to showing change in relation to other trends,
policy and program interventions Key to comparing progress in relation to objectives
and programs, over time and between jurisdictions.
Lesson 4: Evaluation of ecological approaches to prevention on community-wide or province-wide scale should not attempt to isolate the components.
Common disease prevention $1,500 - 15,000Secondary or tertiary care $20,000 - 100,000
Source: Warner KE. Smoking cessation: Alternative strategies: Financial implications. Tobacco Control , Autumn 1995.
Lesson 6: Effectiveness and benefit may increase with intensity, but cost-utility and cost-effectiveness often decline. Intensity limits reach. -->Issue of inequalities.
Estimated Efficacy (6-month quit rates),Reach (number using), and Impact of
Lesson 7: Cost-benefit and cost-effectiveness depend as much on the reach as on the efficacy of interventions.
Change in Per Capita Cigarette ConsumptionChange in Per Capita Cigarette ConsumptionCalifornia & Massachusetts versus Other 48 States, 1984-1996California & Massachusetts versus Other 48 States, 1984-1996
-25
-20
-15
-10
-5
0
5
Perc
ent R
educ
tion
Other 48 States California Massachusetts
1984-1988 1990-1992 1992-1996
What Worked? Making Better What Worked? Making Better Use of “Natural Experiments”Use of “Natural Experiments”
Comprehensive program Comprehensive program andand tax increases in CA tax increases in CA and MA resulted in: and MA resulted in: – 2 - 3 times faster decline in adult smoking prevalence2 - 3 times faster decline in adult smoking prevalence– Slowed rate of youth smoking prevalence compared Slowed rate of youth smoking prevalence compared
to the rest of the nationto the rest of the nation– Accelerated passage of local ordinancesAccelerated passage of local ordinances
Similar, though later, experience in OR & AZ, Similar, though later, experience in OR & AZ, and in population segments of FLand in population segments of FL
Components of Components of Comprehensive Comprehensive Tobacco Control ProgramsTobacco Control Programs
Community Programs Community Programs Statewide ProgramsStatewide Programs Chronic Disease Chronic Disease
ProgramsPrograms School ProgramsSchool Programs EnforcementEnforcement
Counter-MarketingCounter-Marketing Cessation ProgramsCessation Programs Surveillance and Surveillance and
EvaluationEvaluation Administration and Administration and
ManagementManagement
Lesson 8: The Ecological Lesson 8: The Ecological ImperativeImperative
Need to address the problem at all levelsNeed to address the problem at all levels– IndividualIndividual– Organizational, institutionalOrganizational, institutional– CommunityCommunity– State, regionalState, regional– National, internationalNational, international
Need to make these levels of intervention Need to make these levels of intervention mutually supportive and complementarymutually supportive and complementary
Percent Reductions in Per Capita Cigarette Percent Reductions in Per Capita Cigarette Consumption Attributable to Non-Price Public Consumption Attributable to Non-Price Public
A critical mass of personal exposure is A critical mass of personal exposure is needed for individuals to be influencedneeded for individuals to be influenced
A critical mass of population exposure is A critical mass of population exposure is necessary to effect detectable community necessary to effect detectable community responseresponse
A critical distribution of exposure is A critical distribution of exposure is necessary to reach segments of the necessary to reach segments of the population who are less motivatedpopulation who are less motivated
$0 $2 $4 $6 $8 $10 $12
Massachusetts
California
Arizona
Oregon
NCI/ RWJF
NCI
CDC/ RWJF
CDC
Per Capita Spending on TobaccoPrevention and Control--FY1997
Dollars Per Capita
Lesson 10: The Environmental Lesson 10: The Environmental ImperativeImperative
Environments provide opportunities Environments provide cues Environments enable choices Social environments reinforce positive
behavior and punish negative behavior Legal penalties and financial incentives can
be built into environments
100-Percent Smokefree Ordinances, by Year of Passage
1985 1986 1987 1988 1989 1990 1991 1992*0
24
6
810
12
14
16
18WorkplaceRestaurantRestaurant and Workplace
Number ofOrdinances
Year* Through September 1992.Source: National Institutes of Health, National Cancer Institute (1993). Smoking and Tobacco Control - Monograph 3. Major Local Tobacco Control Ordinates in the U.S. US Dept. of Health and Human Service. Public Health Service, National Institutes of Health. NIH Publ. No. 93-3532.
Tobacco Vending Machine Ordinances
1985 1986 1987 1988 1989 1990 1991 1992*
0
2040
60
80100
120
140
160
180Total BanPartial Ban
Number ofOrdinances(Cumulative)
Year* Through September 1992.Source: National Institutes of Health, National Cancer Institute (1993). Smoking and Tobacco Control - Monograph 3. Major Local Tobacco Control Ordinates in the U.S. US Dept. of Health and Human Service. Public Health Service, National Institutes of Health. NIH Publ. No. 93-3532.
Lesson 11: The Educational Lesson 11: The Educational ImperativeImperative
Public awareness of risks and benefitsPublic awareness of risks and benefits Public interest in lifestyle optionsPublic interest in lifestyle options Public understanding of behavioral stepsPublic understanding of behavioral steps Public attitudes toward the options & stepsPublic attitudes toward the options & steps Public outrage at the conditions that have Public outrage at the conditions that have
put them at risk or in dangerput them at risk or in danger Personal and political actionsPersonal and political actions
Lesson 12: The Evidence-Based Lesson 12: The Evidence-Based Imperative: The Need to Bridge...Imperative: The Need to Bridge...
““best practices” indicated by research to their application best practices” indicated by research to their application in practice in underserved areasin practice in underserved areas
““best practices” from research to the most appropriate best practices” from research to the most appropriate adaptations for special populationsadaptations for special populations
The success of individual behavior changes of the The success of individual behavior changes of the affluent to the system changes needed to reach the less affluent to the system changes needed to reach the less affluent, less educated…affluent, less educated…
University-based, investigator-driven research to University-based, investigator-driven research to practitioner- & community-centered researchpractitioner- & community-centered research
Breaking the Intervention-Based Research and Planning Habit
1. Select off-the-shelf 1. Select off-the-shelf Intervention or Intervention or Service to be StudiedService to be Studied
2. Assess Response2. Assess Responseto the Intervention orto the Intervention orServiceService
*Adapted from Australia Commonwealth Dept of Health, 2001
“Best Practices”Diffusion researchDissemination
The Lenses of Health The Lenses of Health Professionals and Lay People Professionals and Lay People
“ “Objective”Objective” Indicators Indicators of Healthof Health
SubjectiveSubjectiveIndicatorsIndicatorsof Healthof Health
ProfessionalProfessional LaypersonLayperson
LW Green, Inst of Health Promotion Research, Univ. British Columbia, Vancouver, BC V6T 1Z3Adapted from Yukon Bureau of Statistics, Whitehorse, 1995
Understanding Differences Among Understanding Differences Among Public’s Perception of Needs, the Public’s Perception of Needs, the Health Sector’s Assessments, and the Health Sector’s Assessments, and the Political AssessmentsPolitical Assessments
““ActualActualneeds”needs”
Public’sPublic’sperceived needs,perceived needs,
prioritiespriorities
Resources,Resources,feasibilities,feasibilities,
policypolicy
BB
CC
DDAAAA
EE
LW Green, Inst of Health Promotion Research, Univ. British Columbia, Vancouver, BC V6T 1Z3
Strategies to Reconcile Strategies to Reconcile Perceived & Actual Needs, & Perceived & Actual Needs, & ResourcesResources
Participatory Research Participatory Research
AAA
Community Community mobilizationmobilization& organizational& organizationaldevelopmentdevelopment
Health EducationHealth Education
(advocacy)(advocacy)
LW Green & MW Kreuter, Health Promotion Planning: An Educational and Ecological Approach, 1999.
Definition of Definition of Participatory Research Research (www.ihpr.ubc.ca/guidelines.html)
----Systematic investigation...Systematic investigation...--Actively involving people in a learning process...--Actively involving people in a learning process...--For the purpose of social action (new services, resource --For the purpose of social action (new services, resource
allocation, regulation or policy) conducive to [their/their allocation, regulation or policy) conducive to [their/their constituents’] health or quality of life.constituents’] health or quality of life.
--What Participatory Research is not...--What Participatory Research is not...--not just involving people more intensively as subjects of --not just involving people more intensively as subjects of researchresearch














































![Environmental Practices of Batanguenos as Input to Model ......2018/05/04 · This research is anchored on the theory of Lawrence W. Green, PRECEDE – PROCEED Model [5]. This model](https://static.documents.pub/doc/80x56/60988f550de4e447b0283290/environmental-practices-of-batanguenos-as-input-to-model-20180504-this.jpg)




