87
Precocious Puberty Precocious Puberty Insights in Management Insights in Management Katrina L. Parker, MD Pediatric Endocrinology Morehouse School of Medicine
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | ashlyn-lamb |
| View: | 224 times |
| Download: | 0 times |
Precocious Puberty Insights in Precocious Puberty Insights in ManagementManagement
Katrina L. Parker, MD
Pediatric Endocrinology
Morehouse School of Medicine
Precocious PubertyPrecocious Puberty
At the end of the presentation participants:Will be able to define pubertyWill be able to define precocious puberty
and its causesBe able to describe types of treatment for
precocious pubertyDescribe problems associated with
precocious puberty
Landmark Case of Precocious Landmark Case of Precocious PubertyPuberty
5 year old Lina Medina of Peru– Menses onset age 8 months– Breast development age 4– Advanced bone maturation age 5 – Was evaluated for abdominal tumor due to
increasing abdominal size at age 5– On 5/14/1939 gave birth to a 2.9 kg baby boy
PubertyPuberty
The process of physical maturation manifested by an increase in growth rate and the appearance of secondary sexual characteristics
Results in the individual having the capacity to reproduce
Changes are a result of ↑gonadotropin & sex steroid secretion
Mechanism of Puberty Mechanism of Puberty
GnRH stimulates pituitary gonadotropins (LH & FSH)
During childhood pubertal Gn secretion is initially low due to downregulation
Negative feedback of hypothalamic-pituitary-gonadal axis
As puberty progresses, episodic release of LH– Increased amplitude & frequency– Progressive secretion extends over the 24 hr period
Mechanism of why puberty occurs is unknown
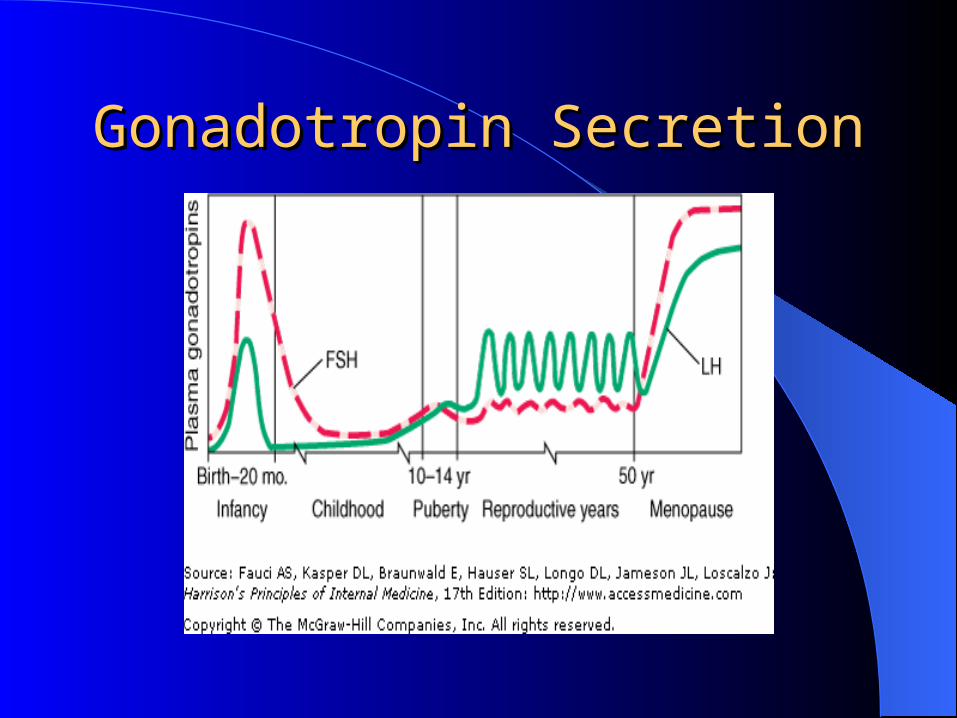
Gonadotropin SecretionGonadotropin Secretion
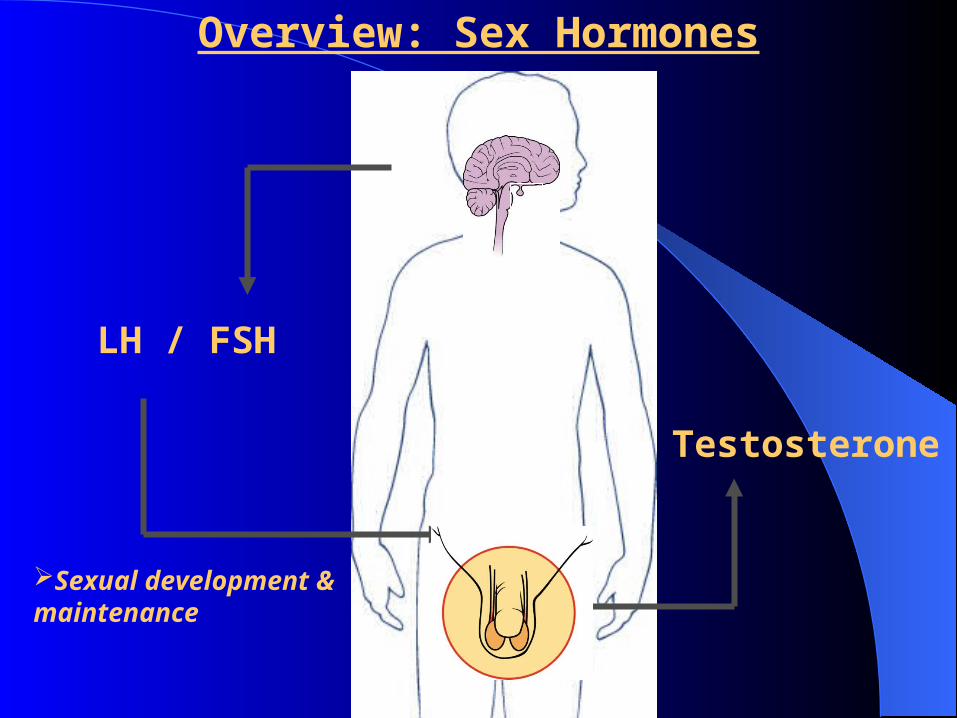
LH / FSH
Testosterone
Sexual development & maintenance
Overview: Sex Hormones
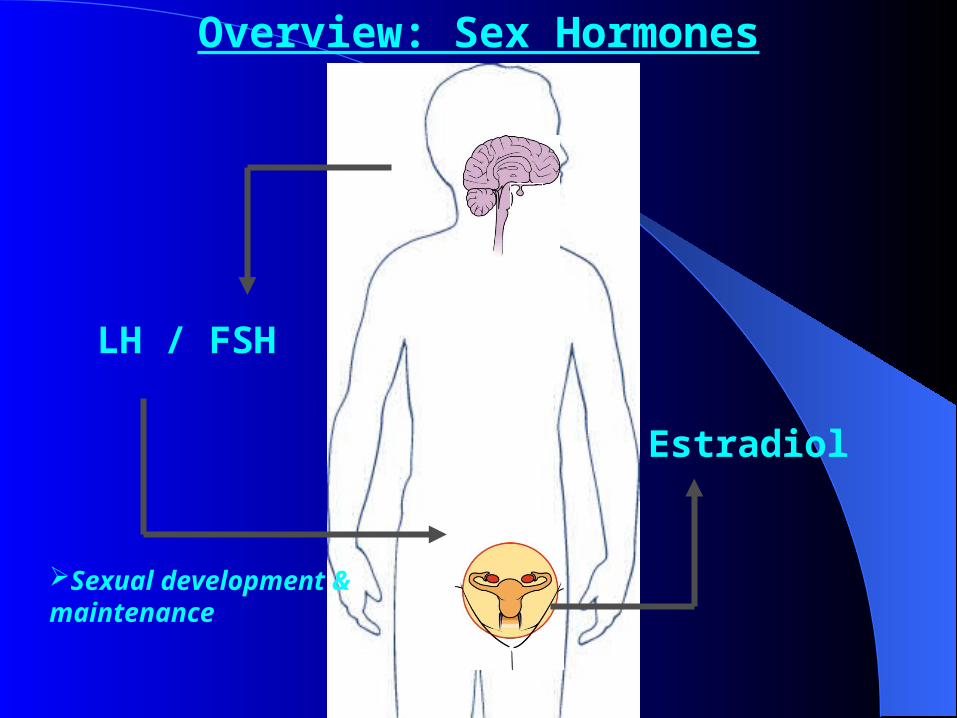
LH / FSH
Estradiol
Sexual development & maintenance
Overview: Sex Hormones
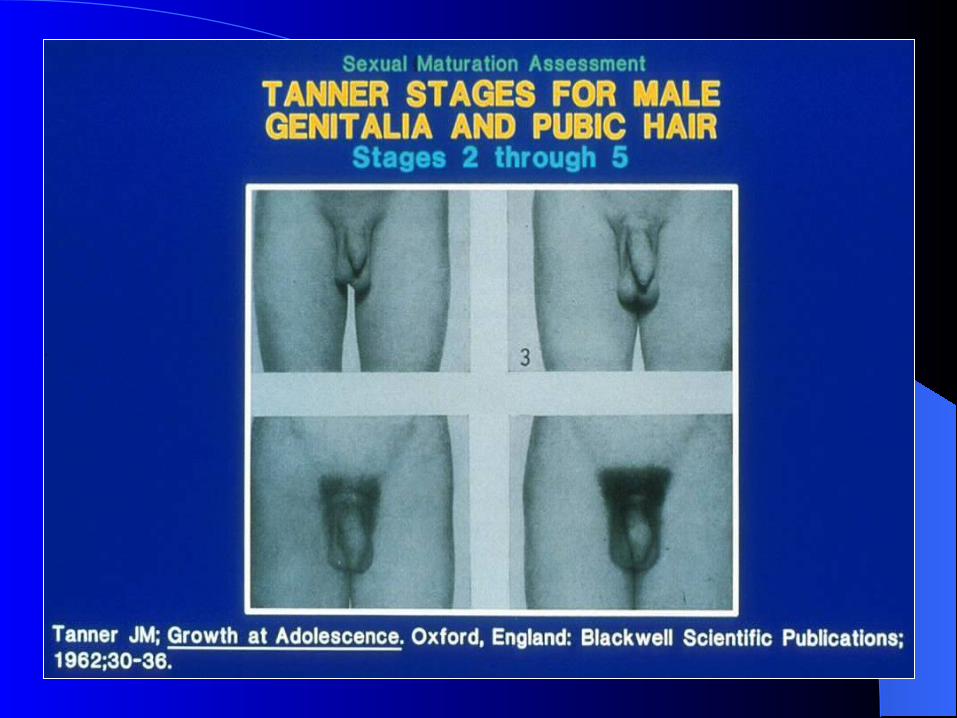
Pubertal DevelopmentPubertal Development
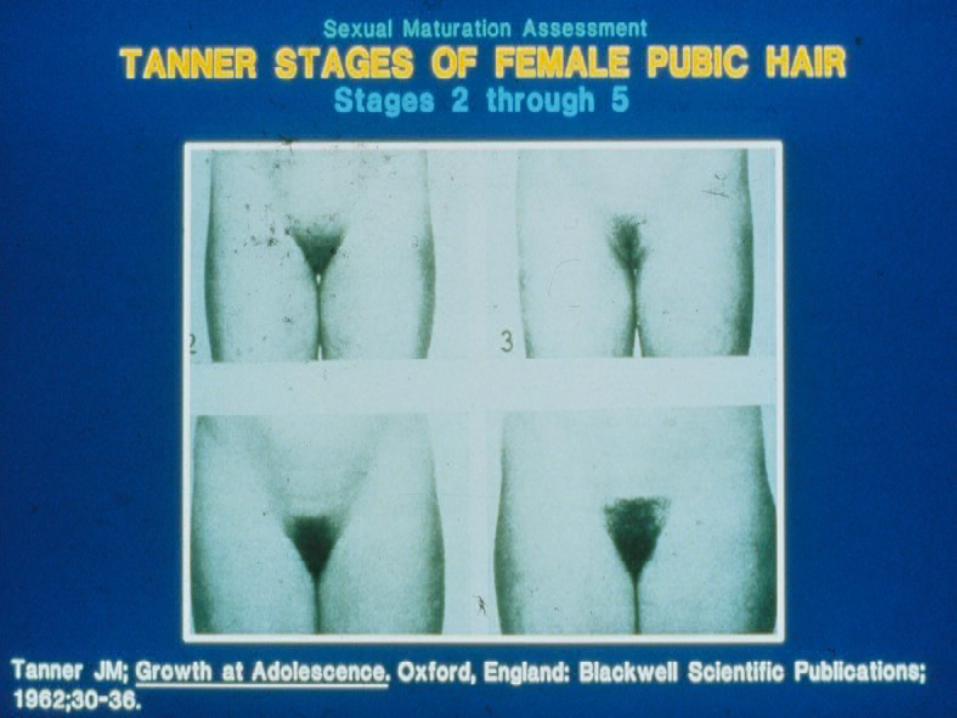
Puberty is divided into five Tanner Stages – Each stage represents
the extent of testicular enlargement and pubic hair growth in males
The appearance of thelarche and pubic hair growth in girls
Normal PubertyNormal Puberty
Traditionally had been defined as the appearance of any secondary sexual maturation after the age of 8 in girls and 9 years in boys
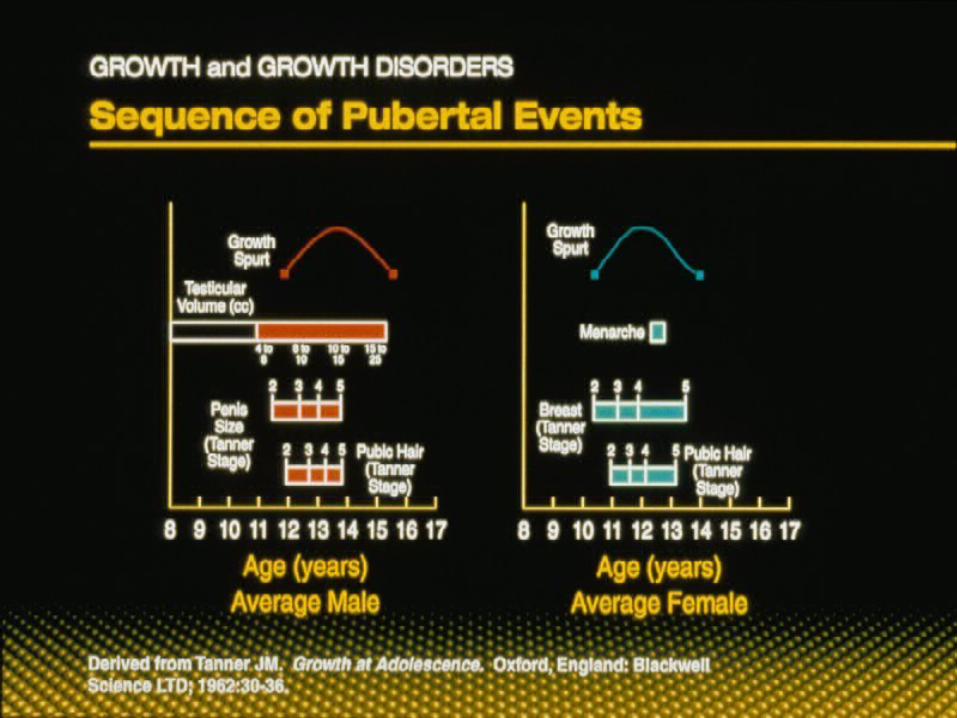
Progression of PubertyProgression of Puberty
May progress very slowly In short burst with no visible change in
overall The earlier the onset, the slower the tempo
Normal pubertyNormal puberty
In males – First sign of puberty is enlargement of testicular
volume– Followed by the appearance of pubic hair and
accumulation of lean body mass– Growth spurt is noted toward the end of their
sexual maturation (late TS III or early TS IV)
PUBERTY
AVERAGE AGE of ONSET:
1. GIRLS 10 to 11 years (range 8 to 13
years)
2. BOYS 11 to 12 years (range 9 to 14
years)
PUBERTYINITIAL SIGNS OF PUBERTY:
1. GIRLS – Breast Development
2. BOYS – Testicular Enlargement
Volume > 3.0 cm³ Length > 2.5 cm
Problems with The Definition of Problems with The Definition of PubertyPuberty
In girls– Breast development maybe difficult to assess
using visual inspection– Discerning breast from fat tissue is a key
concern in overweight girls– Key- palpate under the aerolar
Problems with The Definition of Problems with The Definition of Puberty (cont)Puberty (cont)
In boys– First sign of puberty is not noticed– Need to compare testicular volume with
orchidometer
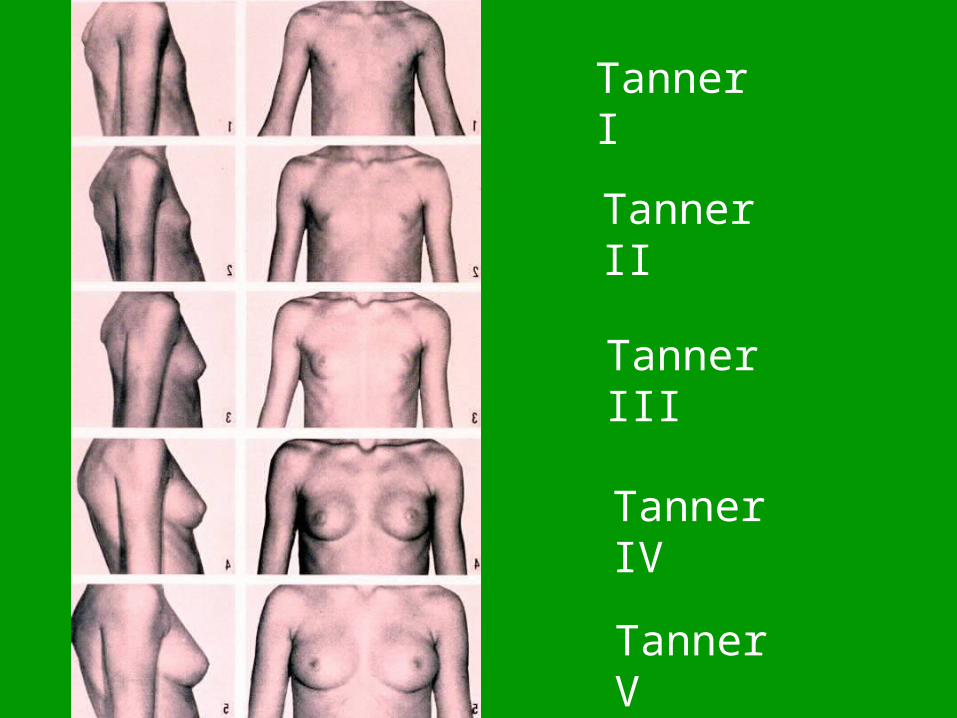
Tanner I
Tanner II
Tanner III
Tanner IV
Tanner V
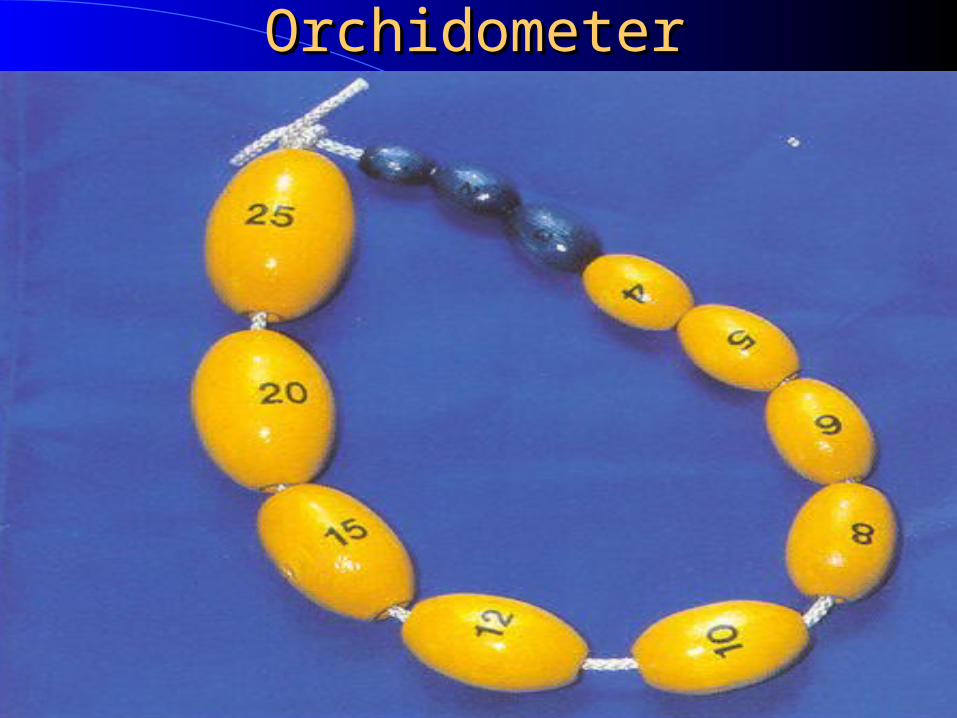
OrchidometerOrchidometer
Factor That Affect PubertyFactor That Affect Puberty
GeneticsRace/EthnicityPrevious nutritionSubcutaneous fatBirth weight
Factors That Affect PubertyFactors That Affect Puberty
Exposure– PCB in utero
Girls started puberty earlier
– Elevated levels of phthalates Puerto Rico outbreak in the 1980s & 1990s
Obesity– Increased leptin and estrogen production– Insulin stimulation of ovaries & uterus
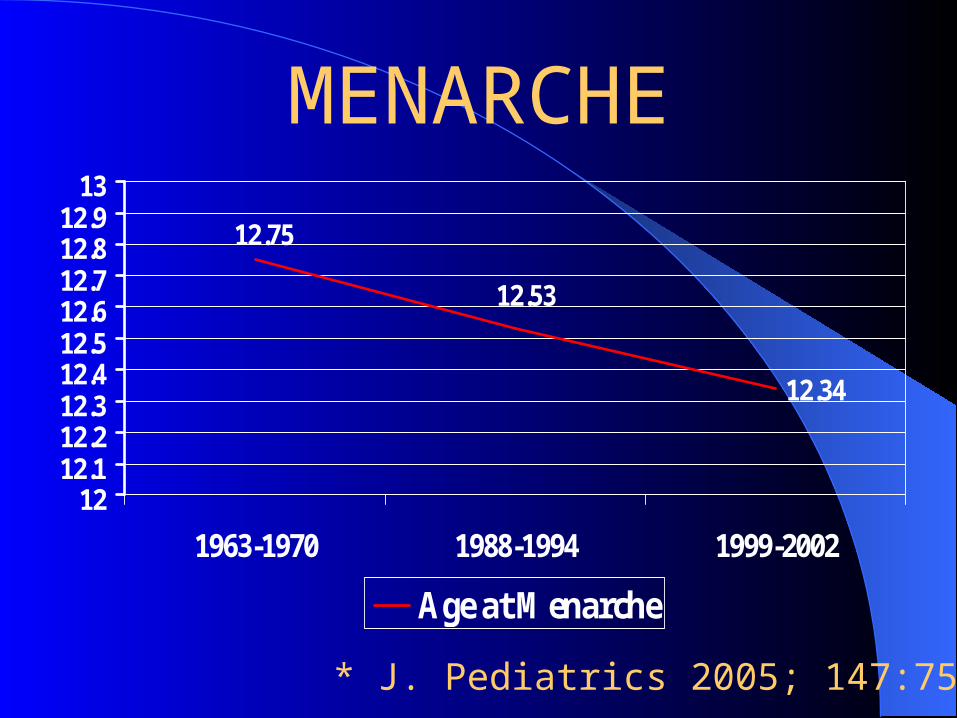
MENARCHE
12.34
12.53
12.75
1212.112.212.312.412.512.612.712.812.9
13
1963-1970 1988-1994 1999-2002
Age at Menarche
* J. Pediatrics 2005; 147:753-760
Are Children Entering Puberty Are Children Entering Puberty Earlier?Earlier?
Expert panel convened to settle a debate Are data sufficient to establish or suggest a
secular trend in the timing of puberty onset and/or progression?
Data from 1940-1994 was evaluated
Conclusions from data analysis have not been consistent– Limited data comparability among studies– Different populations – Different time periods – Studies used different methods
Pediatric Research In Office Pediatric Research In Office SettingSetting
In 1997, a survey was conducted in 225 clinicians in pediatric practices
Pediatricians rated the amount of sexual maturation on girls undergoing complete physical examinations
ResultsResults
Data was analyzed on 17,077 girls– 9.6% were AAF– 90.4% were CF
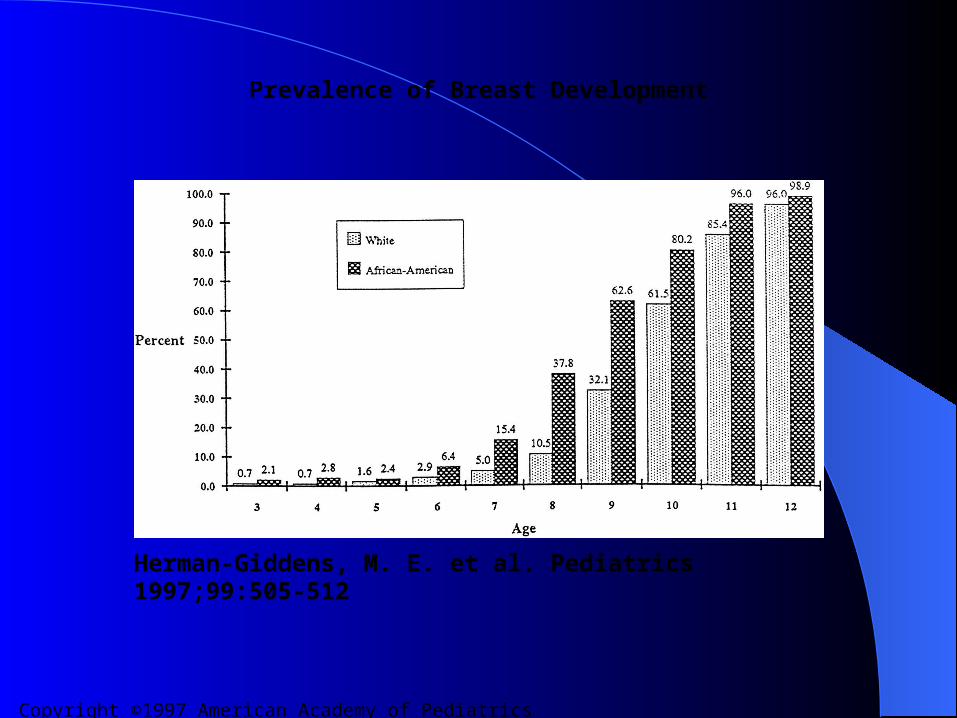
Results:– 1% of CF & 3% of AAF are TS II pubic hair by age 3– 6.7% of CF & 27.2% of AAF are TS II by age 7– 14.7% of CF & 48.3% of AAF are TS II by age 8
Results (cont.)Results (cont.)
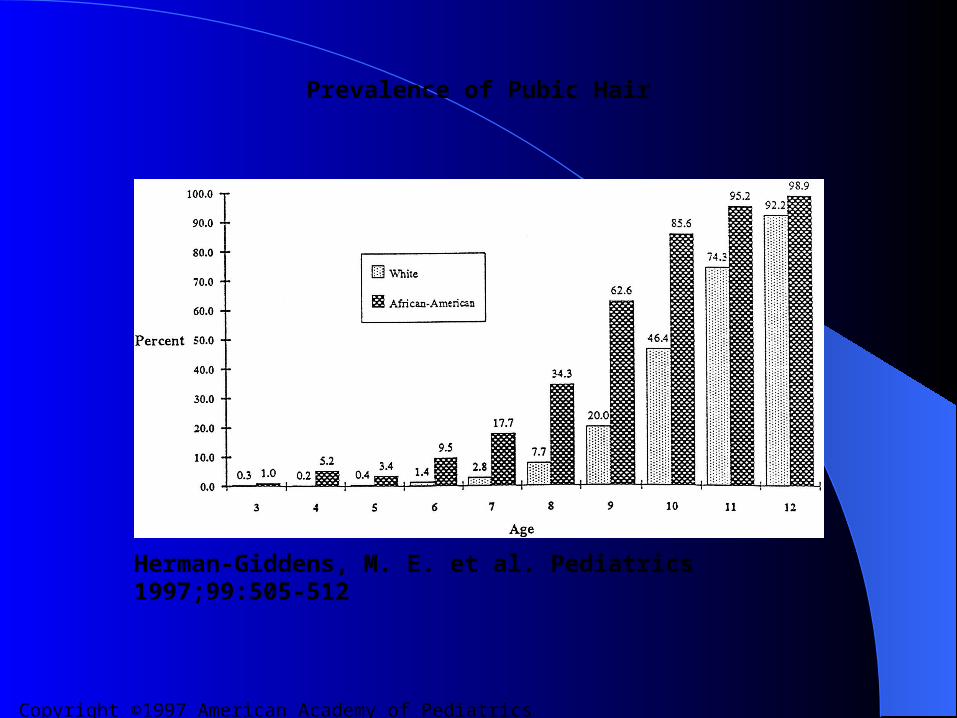
The mean age for onset of pubic hair development was – 8.78 years for AAF and 10.51 years for CF
The mean age for menses was– 12.16 years for AAF and 12.88 years for CF
The mean age of onset of breast development was age – 8.87 years for AAF and 9.96 years for CF
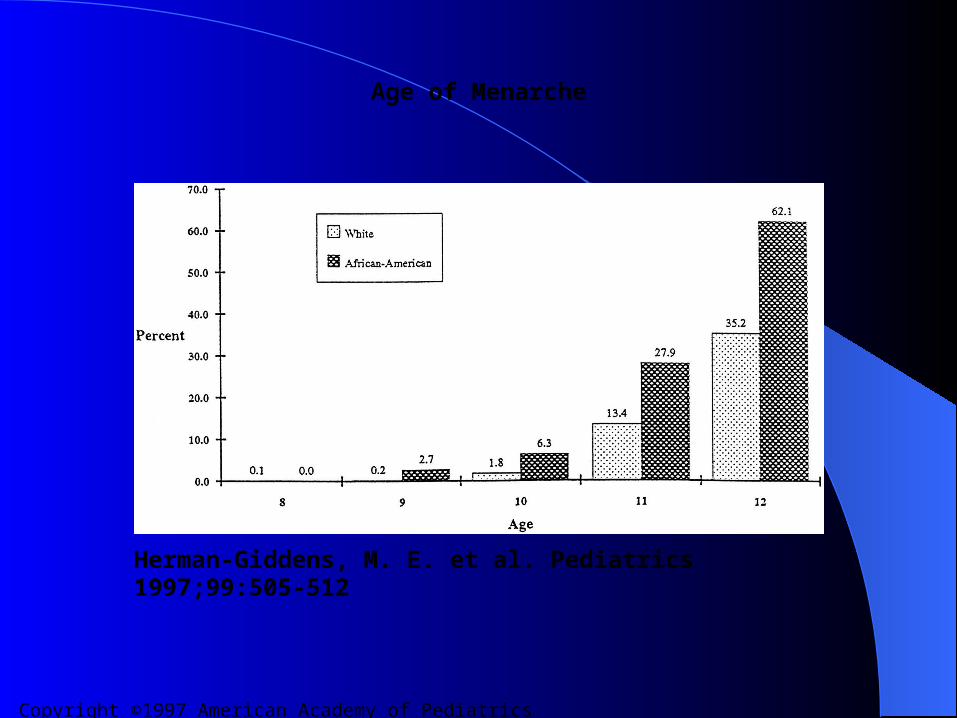
Copyright ©1997 American Academy of Pediatrics
Herman-Giddens, M. E. et al. Pediatrics 1997;99:505-512
Age of Menarche
Copyright ©1997 American Academy of Pediatrics
Herman-Giddens, M. E. et al. Pediatrics 1997;99:505-512
Prevalence of Breast Development
Copyright ©1997 American Academy of Pediatrics
Herman-Giddens, M. E. et al. Pediatrics 1997;99:505-512
Prevalence of Pubic Hair
ConclusionsConclusions
Lead to new guidelines that changed the definition of precocious puberty
Breast development and pubic hair are occurring significantly earlier than suggested
Lawson Wilkins Pediatric Lawson Wilkins Pediatric Endocrine SocietyEndocrine Society
Recommendations:– Breast development before 7 years in Caucasians and
age 6 in African-Americans is considered precocious– Warrants evaluation
There are no comparable data published in boys No change in the recommended age that boys be
evaluated
LWPES GuidelinesLWPES Guidelines
Use these guidelines ONLY in healthy girls with no signs of neurological or other disease that may pathologically advance puberty.
LWPES RecommendationsLWPES Recommendations
In boys– Fewer data are available on ages and patterns of
pubertal development– ? Lower interest in studying male puberty– ? May reflect less cultural awareness

Precocious PubertyPrecocious PubertyWhen puberty begins early & progresses
earlyOnset is occurring earlierTraditional definition
– Onset < age 8 in girls– Onset < age 9 in boys
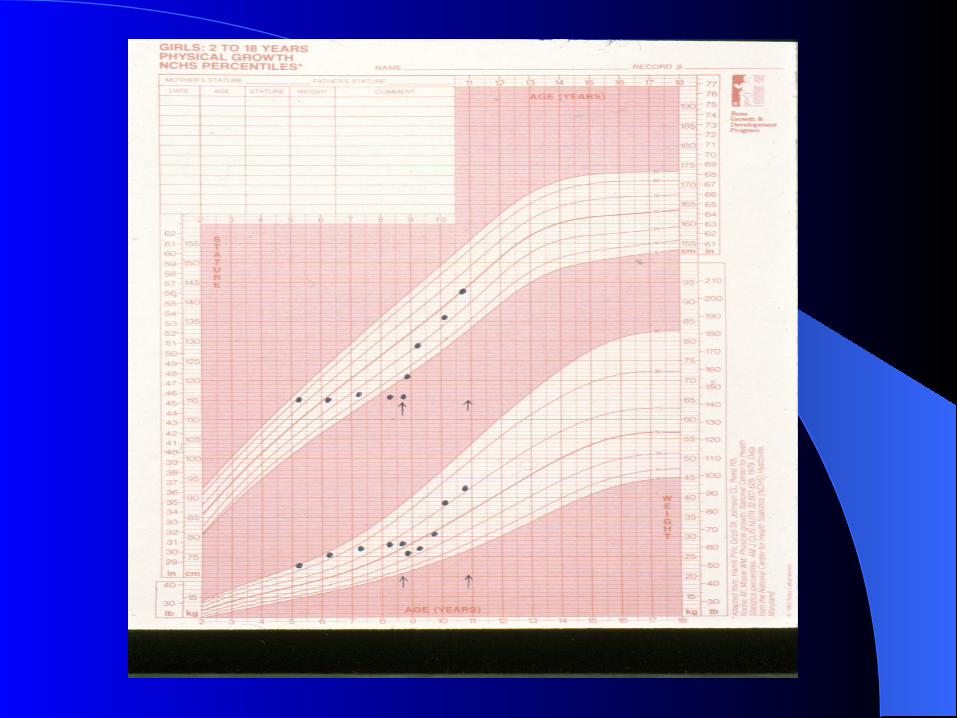
Idiopathic type is the most common Height age, weight age and bone age all advanced Early closure of epiphyseal growth plates results in
adult short stature below genetic potential
Precocious PubertyPrecocious Puberty
Gonadotropin-dependent– Involves the premature activation of the hypothalamic-
pituitary-gonadal axis Gonadotropin-independent
– Secretion of sex steroids is independent of pituitary gonadotropin release
The prevalence – is estimated to be between one in 5,000 to 10,000
children annually in the United States.
Precocious PubertyPrecocious Puberty
Isosexual– Appropriate for sex
Contrasexual or heterosexual– Appropriate sex for the opposite sex
This terminology is cumbersomeUse of feminization in males &
masculinization in females should adequately designate these conditions
Differential Diagnosis of GnRH-Differential Diagnosis of GnRH-dependent precocious pubertydependent precocious puberty
Idiopathic Constitutional CNS lesions
– Hypothalamic hamartoma– Malignancies
Astrocytoma Ependymoma Glioma (maybe assoc with NF Type 1) Pineal tumors
Differential Diagnosis (cont) Differential Diagnosis (cont)
Miscellaneous– Significant head trauma– CNS infections (meningitis, encephalitis, abscess)– Empty sella syndrome– Ventricular cysts– Granulomas– Prior CNS irradiation– Congenital hydrocephalus– De Morsier syndrome
Secondary to GnRH-independent precocious puberty
Incomplete GnRH independent Incomplete GnRH independent precocious pubertyprecocious puberty
Males– Gonadotropin secreting tumors– Excessive androgen production– Testicular tumors (choriocarcinoma)– Virilizing congenital adrenal hyperplasia– Premature Leydig and germinal cell maturation– Extragonadal (i.e hepatoblastoma, germ cell tumors)
Activating mutation of LH receptor
Incomplete GnRH independent Incomplete GnRH independent precocious puberty (cont) precocious puberty (cont)
Females– Severe hypothyroidism– Ovarian cysts– Estrogen secreting neoplasm– Exposure to exogenous estrogen
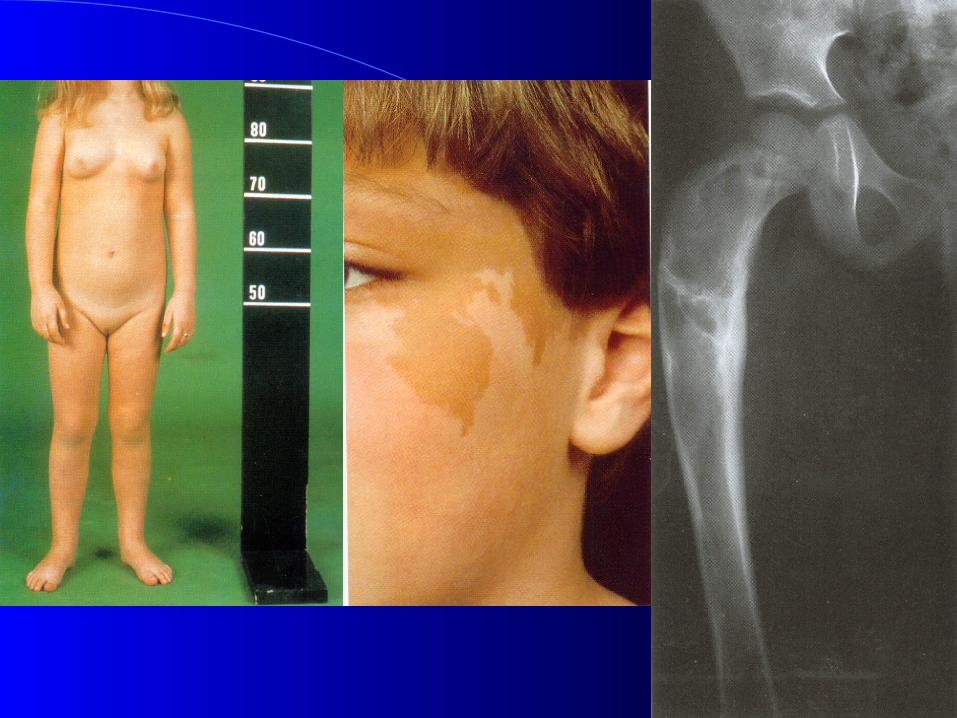
Males and females– McCune Albright Syndrome
Incomplete Sexual PrecocityIncomplete Sexual Precocity
Females– Androgen secreting tumors– Virilizing congenital adrenal hyperplasia
Males– Estrogen secreting tumor

HistoryHistory
Age at onset of signs and symptoms Rate of progression Growth velocity
Family historyHormone exposurePrevious or current CNS abnormalitiesGelastic seizures
Diagnostic EvaluationDiagnostic Evaluation
History & physical exam– Height, weight, arm span, U/L ratio– Skin, hair, thyroid and neurological findings– Breast/pubic hair staging– Inspection of vaginal mucosa– Testicular/phallus size
Hormonal TestingHormonal Testing
Baseline elevation of FSH and FSH response to GnRH provocative testing
LH levels are consistent with early puberty– LH/FSH ratio > 1.0
Estradiol/testosterone levels may rise to the early pubertal range
Testing (cont.)Testing (cont.)
TSH Plasma 17-OH Progesterone, DHEASOther testing:
– Bone age, skeletal survey– Pelvic ultrasound– MRI of the brain
In malesIn males
Same evaluation in females, except also obtain:– Testosterone– Beta hcg– Specialized testing for LH receptor mutation
TherapyTherapy
Treat the underlying causeGnRH analogue
– Lupron depot ped, leuprolide acetate – Histrelin acetete
Monitor therapy– Plasma estradiol/testosterone levels– Growth velocity– Breast/testicular size regression
Variations of Pubertal PubertyVariations of Pubertal Puberty
Premature AdrenarchePremature ThelarchePremature menarche
Premature AdrenarchePremature Adrenarche
Development of pubic hair before age of 7 years in Caucasian girls and age 6 in African American girls
? Early maturation of the adrenal zona reticularis
Higher levels of basal and stimulated DHEA levels when compared to prepubertal children
Premature AdrenarchePremature Adrenarche
Linear growth velocity and skeletal maturation is slightly advanced
Maybe associated acne and axillary odorNo evidence of systemic virilizationExclude adrenal neoplasm and enzymatic
defects
Premature adrenarchePremature adrenarcheHistory
– Racial and ethnic background– History of IUGR, FH of NIDDM, HTN, PCOS higher
risk group20% of patients with precocious puberty present
with premature adrenarcheObtain baseline bone age, androgens (DHEAS,
androstenedione, 17OH-P, free testosterone, fasting lipid panel, SHBG)
Radiographic imaging R/O CNS or adrenal pathology should be reserved in minority of cases
Premature adrenarchePremature adrenarche
Independent of the hypothalamic pituitary gonadal axis
Biochemical evidence is found as early as 6 years in normal children – Increased basal dehydroepiandrosterone sulfate
(DHEAS)– Relative increase in ACTH
Mechanism is not known
AdrenarcheAdrenarche
Adrenal androgens– Begin to rise at about 6-8 years of age– Occurs approximately 2 years prior to an
increase in pubertal gonadotropin pulses and increased pituitary GnRH sensitivity
– Increase in DHEA and DHEAS production continues until age 14-16
Premature ThelarchePremature Thelarche
Has been diagnosed during two age periods– During the first two years of life
caused by the persistent increased infant gonadotropin secretion
Development almost always regress before 24 months of age
Premature Thelarche (cont.)Premature Thelarche (cont.)
Second period– After 6 years of age– May be symmetric or asymmetric
Maybe a consequence of temporarily increased ovarian steroid secretion
Premature ThelarchePremature Thelarche
May be symmetrical or unilateralIs not accompanied by other signs of
pubertyNormal estrogen levels, and heightBone age is normal or slightly advancedRare ovarian cystMay be first sign of precocious puberty
EvaluationEvaluation
Correct diagnosis– Idiopathic or pathologic
History– Any neurological diseases?
Personality changes Headaches or visual symptoms
– Drug exposure
Problems in Girls With Problems in Girls With Precocious PubertyPrecocious Puberty
Are taller than peers initially Compared to their peers:
– Maybe more likely to have psychological problems– Unintended pregnancies– Higher rates of substance abuse
Increased incidence of PCOS ? Increased breast cancer risk Unsure of the long term effects on bone mineral
density

In GnRH dependent precocious puberty – Characterized by an acceleration of growth and
bone maturationEarly growth manifests as tall stature for
age As bones continue to be exposed to sex
steroids, growth plates mature and fuse – Result in overall decreased adult height
Physical examinationPhysical examination
Findings on exam can further direct your evaluation – effects of androgens (acne, hirsuitism,
increased muscle mass and clitromegaly)
Minimum bone age determination– If advanced, pursue further evaluation
GnRH stimulation test

Treatment Options Treatment Options
TreatmentTreatment
GnRH agonist– Desensitizes the pituitary– Blocks LH and FSH secretion– Prevents continued sexual development for the
duration of the treatmentGrowth may almost stop while on therapy± addition of growth hormone remains
controversy
GnRH AgonistGnRH Agonist
Nona- or deca peptides that are structurally similar to endogenous GnRH
Are available as subcutaneous and intranasal preparations– Are given as daily or monthly depot injections– Lupron depot Ped, leuprolide acetate, or
histrelin
Side effects of GnRH AgonistSide effects of GnRH Agonist
Usually mild Therapy has been available for greater than 20
years– Not possible to say there will be no long term
complications in some patients
During therapy– Hot flashes, skin rashes– Pain at the injection site– Sterile abscess at the injection site in 10% of patients

Histrelin Implant Therapy for Histrelin Implant Therapy for Precocious PubertyPrecocious Puberty
11 girls with CPPAge at diagnosis: 6.5 years (range 2-9
years)GnRH Stimulation Test
– Peak LH 23 ± 28 miu/ml– Peak FSH 20 ± 25 miu/ml
All girls underwent implant placement
Histrelin Implant StudyHistrelin Implant Study
Girls were divided into 2 Groups:– Group A: 6 girls were followed for 15 months
after implant insertion– Group B: 5 girls had their implant removed
after 9 months
GnRH Stimulation test were performed– Group A 6, 9, 12 & 15 months– Group B 6 & 9 months
ResultsResults
In all girls – Breast development regressed– Growth velocity decreased– Bone age advancement slowed – Basal Gn and stimulated response and estradiol
levels were suppressed
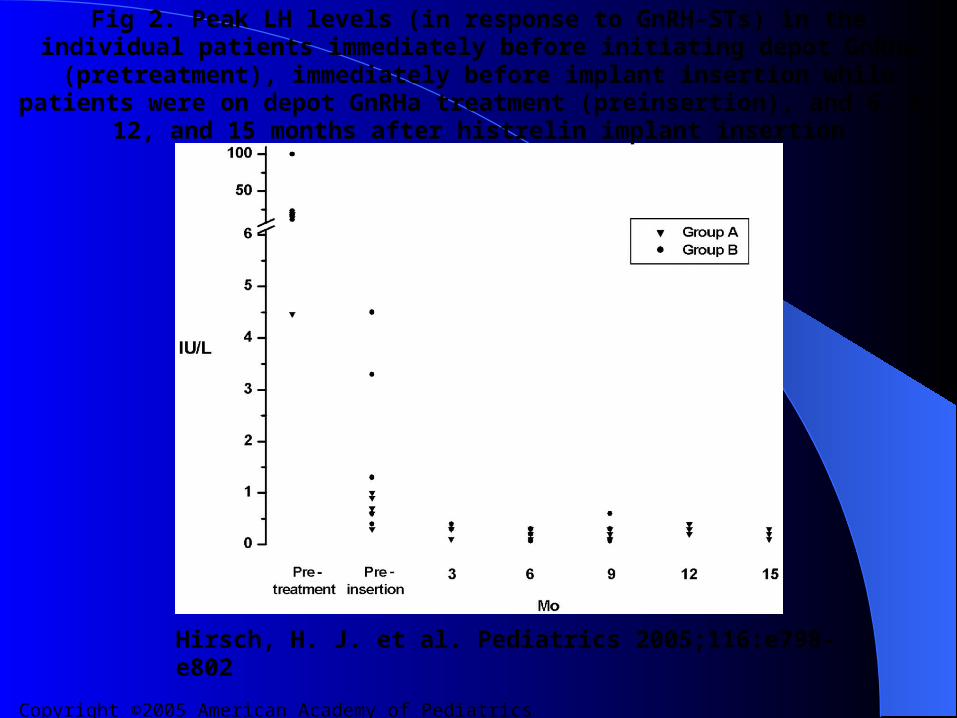
Copyright ©2005 American Academy of Pediatrics
Hirsch, H. J. et al. Pediatrics 2005;116:e798-e802
Fig 2. Peak LH levels (in response to GnRH-STs) in the individual patients immediately before initiating depot GnRHa (pretreatment), immediately before implant insertion while patients were on depot GnRHa treatment (preinsertion), and 6, 9, 12, and 15
months after histrelin implant insertion
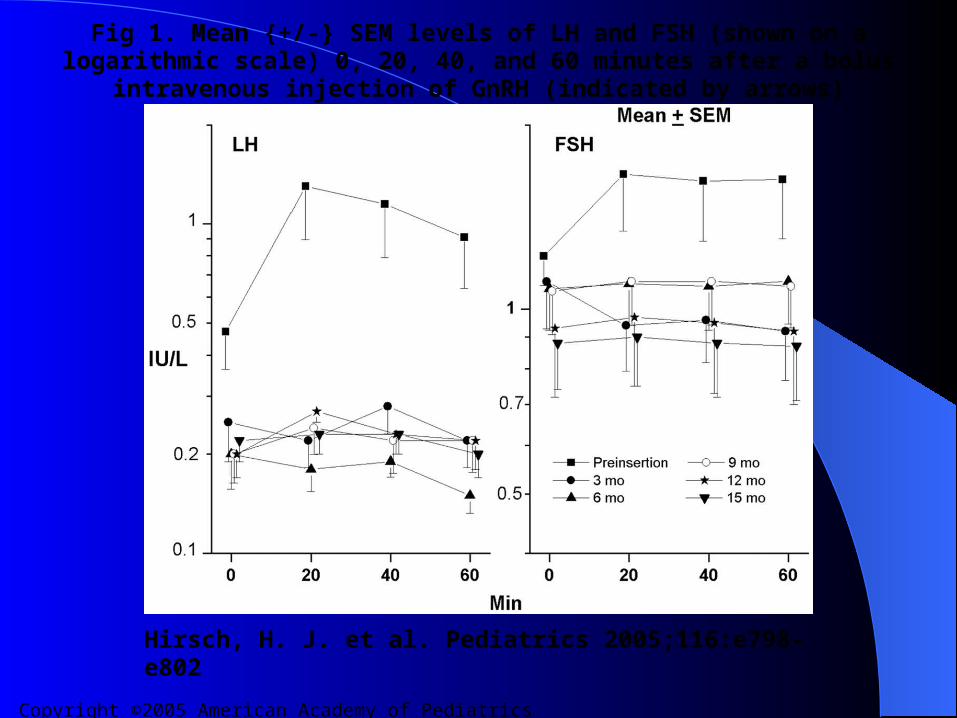
Copyright ©2005 American Academy of Pediatrics
Hirsch, H. J. et al. Pediatrics 2005;116:e798-e802
Fig 1. Mean {+/-} SEM levels of LH and FSH (shown on a logarithmic scale) 0, 20, 40, and 60 minutes after a bolus intravenous injection of GnRH (indicated by arrows)
SupprelinSupprelin®® LA LA
SUPPRELIN® LA – Is 12-month implant for treating central
precocious puberty (CPP) – Was approved by the FDA in May, 2007 – Is inserted on the inner aspect of the upper arm

Copyright ©2005 American Academy of Pediatrics
Hirsch, H. J. et al. Pediatrics 2005;116:e798-e802
Fig 3. Implant site in 1 patient 6 months after implant insertion
Side Effects of Histrelin Acetete Side Effects of Histrelin Acetete
At the insertion site– Bruising– Pain– Swelling– Erythema– Soreness– in clinical signs of puberty during the first
month
Contraindications of Histrelin Contraindications of Histrelin AcetateAcetate
Not recommended – for usage < age 2– Women who are pregnant or who become
pregnant
Discontinuation of TherapyDiscontinuation of Therapy
Age to discontinue therapy must be individualized Resumption of the hypothalamic-pituitary-gonadal
axis begins promptly Menses resumes within 12-18 months, up to 4.5 yr Spermatogenesis resumes Documented pregnancy Little or no growth spurt Hyperandrogenism
SummarySummary
Pubertal development is occurring earlier in children
Precocious puberty occurs more commonly in girls
The exact incidence of precocious puberty in males is unknown
Various treatment modalities are available to arrest pubertal development
QUESTIONSQUESTIONS

















