82
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | samuel-fox |
| View: | 219 times |
| Download: | 0 times |
Preconception Counseling and Preconception Counseling and Management of Diabetic Patients Management of Diabetic Patients During PregnancyDuring Pregnancy
Ghorbani H.MDGhorbani H.MD
Fellow of EndocrinologyResearch Institute for Endocrine Sciences
2007 Oct-18
Preconception CounselingPreconception Counseling
Prepregnancy evaluation and counseling of women DM Prepregnancy evaluation and counseling of women DM →→ minimize minimize the risk to the the risk to the F&MF&M
Poor glycemicPoor glycemic control during control during organogenesisorganogenesis→ → spontaneous spontaneous abortionabortion & congenital & congenital anomalies anomalies
Thus, the importance of evaluating glycemic control before Thus, the importance of evaluating glycemic control before
conception cannot be overstated.conception cannot be overstated.
Uptodate 2007

Preconception Care of Women With DiabetesCongenital malformations 6-9% vs. general population risk of 2- 3%.
Congenital defects account for 50% of perinatal mortality
Diabetes associated malformations are more often lethal or significantly disabling and generally involve 1 or more organ systems.
Spontaneous abortion in poorly controoled diabetes twice the rate in women without diabetes.
J Perinat Neonat Nurs Vol. 18, No. 1, pp. 14–25 c 2004
CONGENITAL MALFORMATIONS AND SPONTANEOUS ABORTIONS
The malformations most commonly associated with diabetes occur before the 7th week after conception
The finding of multiple associated anomalies suggests a"hit"during blastogenesis that occurs during the
first 4 weeks of fetal development
Anomalies during blastogenesis tend to be more severe than those that occur during organogenesis (weeks 4 to 5 after conception) And may increase the risk of spontaneous abortions
joslins textbook 2005
Thus, interventions to control glycemia and reduce the risk of malformations must begin before conception and continue through the first 7 weeks after conception.
joslins textbook 2005
The institution of strict glycemic control, as
soon as the woman with diabetes determines
that she is pregnant, very often is too late
to prevent structural damage to fetal organs
which have already formed.
Preconception Care of Women With Diabetes
J Perinat Neonat Nurs Vol. 18, No. 1, pp. 14–25 c 2004

Information and counselling should be provided to all women of reproductive age with diabetes
A meta-analysis has demonstrated a significantly lower prevalence of major congenital anomalies in offspring of women who attended for prepregnancy counselling (relative risk, 0.36; 95% CI, 0.22–0.59; absolute risk, 2.1% v 6.5%).
Management of women with diabetes before conception
MJA • Volume 183 Number 7 • 3 October 2005


PERICONCEPTIONAL CARE OF WOMEN WITH DIABETES
Because most pregnancies of diabetic women are either unplanned
or
without prenatal care until organogenesis has occurred, the efficacy of the intervention has been limited.
Education combined with accessibility to preconception care is the cornerstone of care
Obstet Gynecol Clin N Am 34 (2007) 225–239
A complete history and physical examination should be performed at the preconception visit.
This evaluation should include:
Information on the duration and type of diabetes
History of acute and chronic complications
Current and past glucose management
Physical activity, comorbid medical conditions
Gynecologic and obstetric history
Family issues .Uptodate 2007
Diabetes complications review
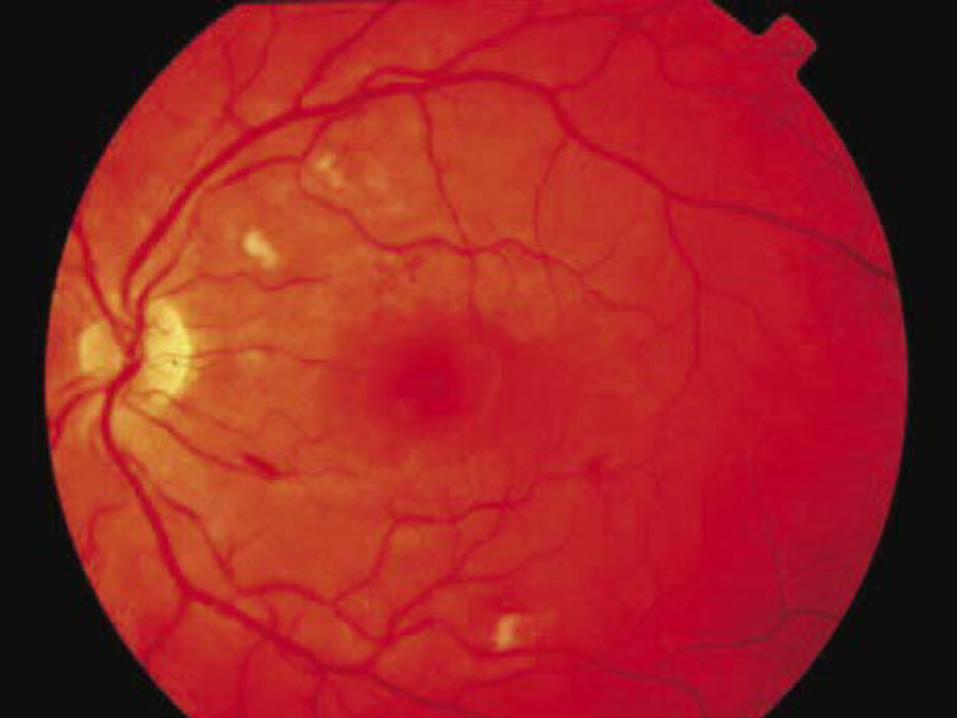
Retinopathy:
The eye examination should be conducted through dilated pupils by a person experienced in retinal examination .
Preexisting retinopathy may progress more rapidly in pregnancy .
Retinopathy that requires laser therapy should be treated before pregnancy.
MJA • Volume 183 Number 7 • 3 October 2005
Nephropathy:Overnight or 24 hour urine sample to quantify the albumin excretion rate.
Patients with pre-existing microalbuminuria are more likely to develop preeclampsia
If renal function is significantly impaired (cr> 0.2mmol/L), there is an increased risk of progression to dialysis during pregnancy
MJA • Volume 183 Number 7 • 3 October 2005

In patients with diabetic nephropathy and mild to moderate renal dysfunction ( cr 1.4 mg/dL and GFR over 90 mL/min), pregnancy per se does not worsen long-term outcom
Pregnancy seems to accelerate renal function
deterioration in women with moderate to severe renal dysfunction at the beginning of pregnancy.
Nephropathy:
Obstet Gynecol Clin N Am 34 (2007) 225–239

Macrovascular disease:
Pre-existing heart disease, requires cardiological review before conception
Significant CHD should be treated before pregnancy .
MJA • Volume 183 Number 7 • 3 October 2005

IdeallyIdeally, all antihypertensive , all antihypertensive drugsdrugs should be should be stopped stopped before conception if the BP remains before conception if the BP remains belowbelow 130/80 mmHg130/80 mmHg with dietary salt restrictionwith dietary salt restriction..
Methyl dopaMethyl dopa
HydralazineHydralazine
B-blockerB-blocker
Ca canal blockerCa canal blocker
ACEI and ARBs are contraindicatedACEI and ARBs are contraindicated
Thiazid is relatively contraindicatedThiazid is relatively contraindicated
BP should be managed aggressivelyBP should be managed aggressively
Management of hypertension
Uptodate 2007

Autonomic neuropathy:
The presence of autonomic neuropathy resulting in gastroparesis, orthostatic hypotension or hypoglycaemic
unawareness may severely complicate the management of
diabetes in pregnancy.
Other related issues:
Thyroid function should be measured for women with T1D
MJA • Volume 183 Number 7 • 3 October 2005
Management of hyperlipidemiaManagement of hyperlipidemia
StatinsStatins are are contraindicatedcontraindicated & should be & should be discontinued before conceptiondiscontinued before conception
HypertriglyceridemiaHypertriglyceridemia treat with treat with diet diet , , supplementation with supplementation with medium chain TGmedium chain TG and
use of intravenous heparin
Joslin text book 2005
BacteriuriaBacteriuria
Women should be Women should be screenedscreened for for asymptomatic asymptomatic bacteriuriabacteriuria and those with and those with positive testpositive test results should results should be be treatedtreated to prevent development of pyelonephritis to prevent development of pyelonephritis
Uptodate 2007
Clinically proven ischemic CAD →pregnancy is contraindicated.
women with diabetic Autonomic neuropathy involving the
CV system → fixed heart rate → pregnancy should be avoided.
Gastroenteropathy is a relative contraindication to pregnancy.
Women with active untreated PR should be counseled to delay pregnancy until after laser photocoagulation
Preconception CounselingPreconception Counseling
J Perinat Neonat Nurs Vol. 18, No. 1, pp. 14–25 c 2004
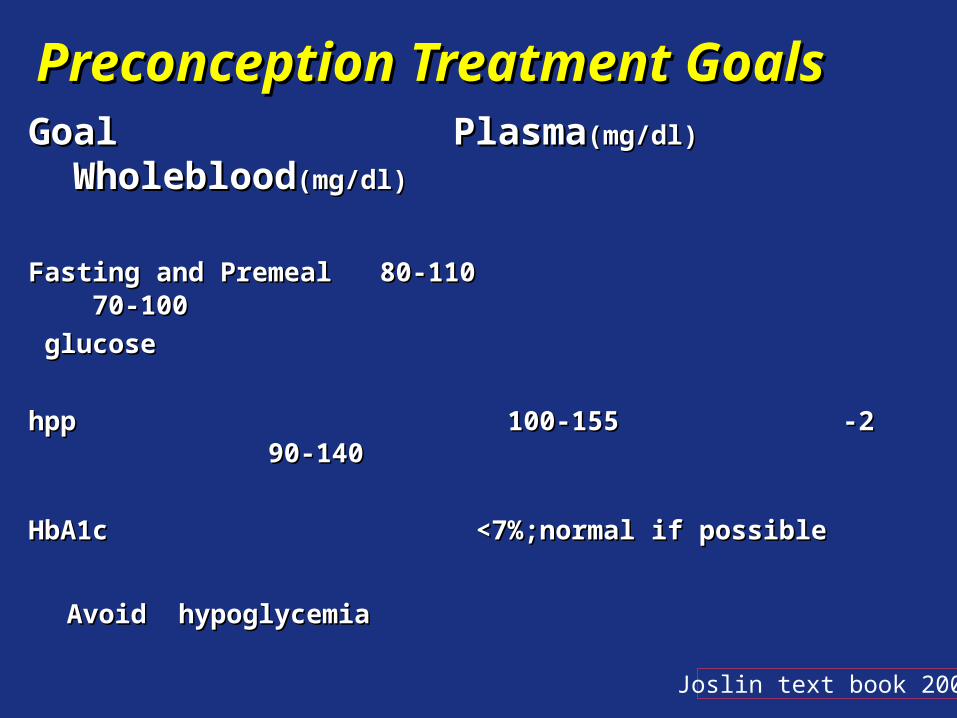
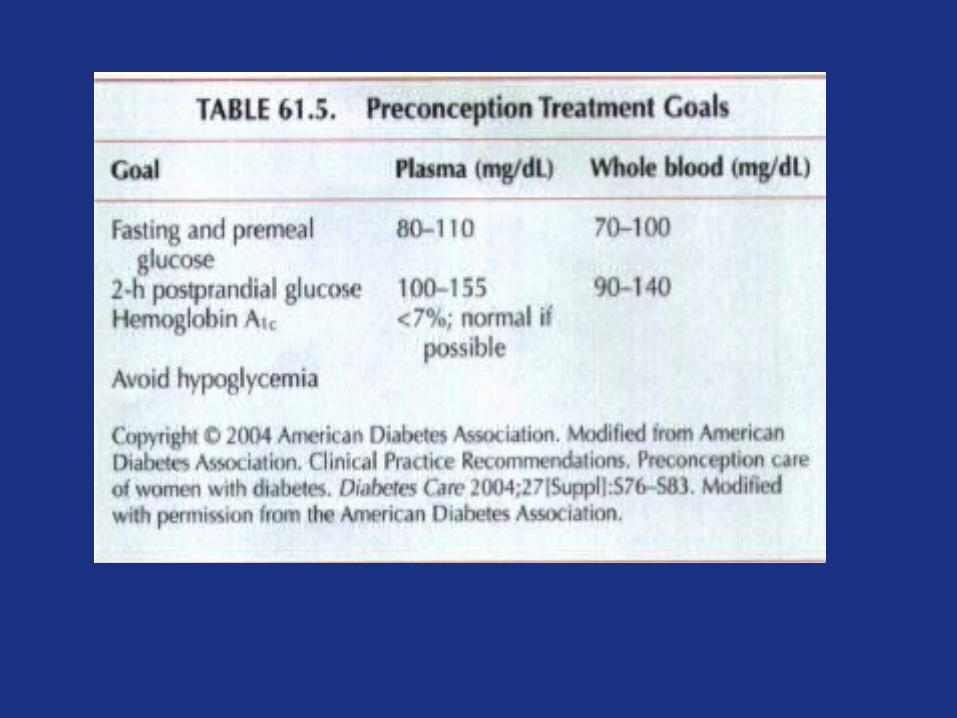
Preconception Treatment GoalsPreconception Treatment Goals Goal PlasmaGoal Plasma(mg/dl)(mg/dl) Wholeblood Wholeblood(mg/dl)(mg/dl)
Fasting and Premeal 80-110 70-100Fasting and Premeal 80-110 70-100
glucoseglucose
22--hpp 100-155 90-140hpp 100-155 90-140
HbA1c <7%;normal if possibleHbA1c <7%;normal if possible
Avoid hypoglycemiaAvoid hypoglycemia
Joslin text book 2005

WHITE CLASSIFICATION OF DMWHITE CLASSIFICATION OF DM DURING PREGNANCYDURING PREGNANCY
Gestational DMGestational DMClass A : diet alone ,any duration or ageClass A : diet alone ,any duration or ageClass B : age at onset > 20 y& duration < 10yClass B : age at onset > 20 y& duration < 10yClass C : age at onset 10- 19 or duration 10 Class C : age at onset 10- 19 or duration 10 –– 19 y 19 yClass D : age < 10 y or duration > 20 y or background Class D : age < 10 y or duration > 20 y or background retinopathy or HTN ( not preeclampsia)retinopathy or HTN ( not preeclampsia)Class R : proliferative retinopathy or vitreous HEClass R : proliferative retinopathy or vitreous HE
Class F : nephropathy with p. uria > 500 mgClass F : nephropathy with p. uria > 500 mgClass RF : R & FClass RF : R & FClass H : heart dxClass H : heart dxClass T : prior renal transplantationClass T : prior renal transplantation
Joslin textbook 2005
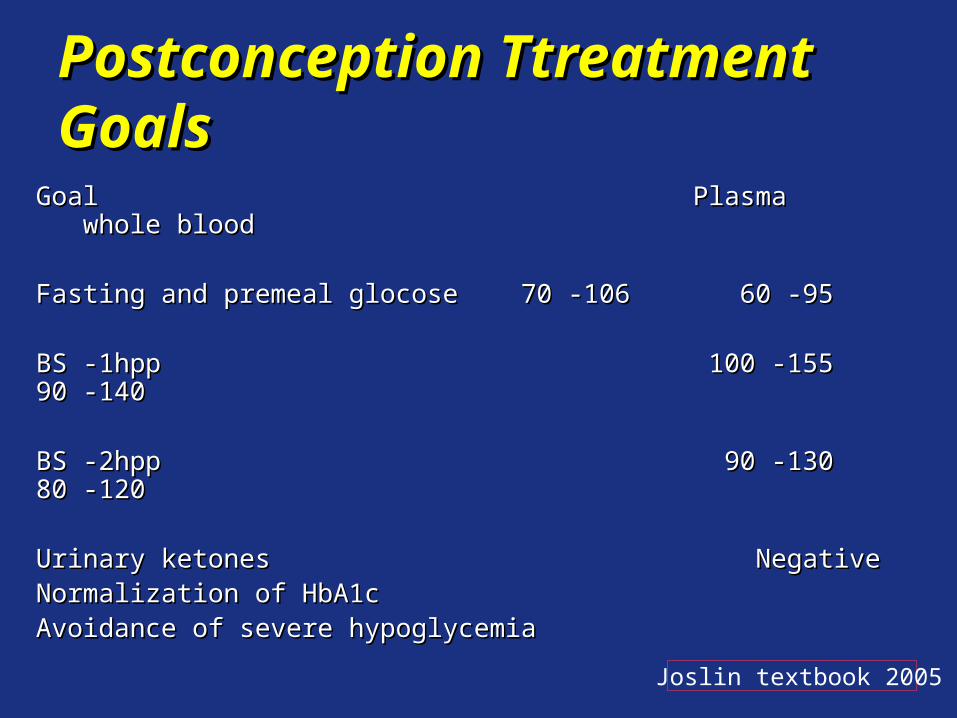
Postconception Ttreatment GoalsPostconception Ttreatment Goals
Goal Plasma whole bloodGoal Plasma whole blood
Fasting and premeal glocose 70 -106 60 -95Fasting and premeal glocose 70 -106 60 -95
BS -1hpp 100 -155 90 -140BS -1hpp 100 -155 90 -140
BS -2hpp 90 -130 80 -120BS -2hpp 90 -130 80 -120
Urinary ketones NegativeUrinary ketones Negative Normalization of HbA1cNormalization of HbA1c
Avoidance of severe hypoglycemiaAvoidance of severe hypoglycemia
Joslin textbook 2005
Management during pregnancy
Routinely review women every 1–4 weeks during the first 30 weeks and then every 1–2 weeks until delivery, depending on diabetes control and the presence of diabetic and obstetric complications.
It is recommended that tests be performed fasting and 1–2 hours after meals.
The HbAlc level should be monitored every 4–8
weeks and kept within the normal range.
MJA • Volume 183 Number 7 • 3 October 2005
Women should be monitored for signs or progression of diabetic complications, particularly:
Retinopathy
Proteinuria
Proteinuria should be assessed by dipstick at regular intervals, and quantitated where appropriate .
Management during pregnancy
MJA • Volume 183 Number 7 • 3 October 2005
Complications of Diabetes during Pregnancy

pregnancy per se does not appear to hasten the natural progression to ESRD for most women
This This dependsdepends upon the upon the initial degreeinitial degree of renal of renal impairmentimpairment..
The risk is substantially increased in women with a The risk is substantially increased in women with a crcr aboveabove 2.0 2.0 mg/dL , many of whom have more than mg/dL , many of whom have more than 2 g2 g of of proteinuria per dayproteinuria per day..
NEPHROPATHY
Uptodate 2007
NEPHROPATHY
These findings can be considered These findings can be considered relativerelative contraindicationscontraindications to pregnancy to pregnancy . .
A A GFR below 50GFR below 50 mL/min before pregnancy is mL/min before pregnancy is associatedassociated with a high prevalence of with a high prevalence of HTNHTN and and fetalfetal wastagewastage
Uptodate 2007
MicroalbuminuriaMicroalbuminuria
Degree of glycemic controlDegree of glycemic control
Blood pressureBlood pressure
PregnancyPregnancy
The four major factors that have been associated The four major factors that have been associated with the development and progression of DNwith the development and progression of DN::
Uptodate 2007

These agents are a reasonable option for the treatmentThese agents are a reasonable option for the treatment
of HTN in pregnant women with of HTN in pregnant women with DNDN,,microalbuminuriamicroalbuminuria , ,
or or microvascular microvascular diseasedisease . .
Lowering BPLowering BP, , reducing microalbuminuriareducing microalbuminuria, and, and improving improving glycemicglycemic control have a protective effect on the glomeruli control have a protective effect on the glomeruli and decrease the GFRand decrease the GFR
CCBs mayCCBs may have have similarsimilar renal protective effects as renal protective effects as ACEI ACEI
Uptodate 2007

EFFECT OF NEPHROPATHY ON EFFECT OF NEPHROPATHY ON PREGNANCYPREGNANCYOvert nephropathy is associated with a variety of pregnancyOvert nephropathy is associated with a variety of pregnancy
complicationscomplications::
Fetal growth restrictionFetal growth restriction
Nonreassuring fetal statusNonreassuring fetal status
PreeclampsiaPreeclampsia
As a consequence, As a consequence, preterm deliverypreterm delivery and and cesareancesarean birth birth are often required for maternal or fetal indications are often required for maternal or fetal indications . .
Uptodate 2007
Patients with preexisting diabetes are at increased risk of hypertensive complications during pregnancy:
Chronic HTN
Preeclampsia—eclampsia
Preeclampsia--eclampsia superimposed on chronic HTN
Gestational HTN
Hypertensive disorderHypertensive disorder
joslins textbook 2005
Hypertensive disorderHypertensive disorder
– Chronic HTN: before or up to 20Chronic HTN: before or up to 20thth weeks of weeks of gestation & if HTN continue after 12 week after gestation & if HTN continue after 12 week after pregnancypregnancy
– Preeclampsia-eclampsia : ≥ 140/90 mmhg ,usually Preeclampsia-eclampsia : ≥ 140/90 mmhg ,usually after 20after 20thth weeks of gestation with proteinuria more weeks of gestation with proteinuria more than 300mg/24 hrsthan 300mg/24 hrs
– Preeclampsia-eclampsia superimposed on chronic Preeclampsia-eclampsia superimposed on chronic HTNHTN
– Gestational HTNGestational HTNjoslins textbook 2005
Start treatment from Start treatment from BP ≥ 130/ 80BP ≥ 130/ 80 mmHg mmHg especially ifespecially if microalbuminuria microalbuminuria or or proteinuriaproteinuria is presentis present
Hypertensive disorderHypertensive disorder
joslins textbook 2005
Ophthalmic assessmenOphthalmic assessmen Comprehensive Comprehensive eye examinatineye examinatin in pt with in pt with planing for pregnancyplaning for pregnancy
who become pregnant should have a comprehensive eye who become pregnant should have a comprehensive eye examinationexamination in the in the first trimesterfirst trimester and and close f/uclose f/u throughout throughout pregnancy and for pregnancy and for one year postpartumone year postpartum..
Frequent Frequent monitoringmonitoring is helpful to look for early is helpful to look for early worsening ofworsening of retinopathy as glycemic control improvesretinopathy as glycemic control improves
Laser Laser photocoagulation should be considered for women with photocoagulation should be considered for women with severe preproliferativesevere preproliferative diabetic retinopathy diabetic retinopathy . .
Uptodate 2007
RetinopathyRetinopathy
Risk of progression of retinopathy increase in pregnancyRisk of progression of retinopathy increase in pregnancyRisk is influenced with :Risk is influenced with :
severity of baseline retinopathyseverity of baseline retinopathy
HbAlc more than 6 SD above normal
intensively treated pt has 1.6 fold increase risk of retinopathy intensively treated pt has 1.6 fold increase risk of retinopathy
Conventionally treated pt has 2.4 fold increase in retinopathyConventionally treated pt has 2.4 fold increase in retinopathyIn DCCT study ,no difference in level of retinopathy in pt who In DCCT study ,no difference in level of retinopathy in pt who
became pregnant as compared with pt who never p.became pregnant as compared with pt who never p.
joslins textbook 2005

Formal eye review should be at least 3-monthly if:
baseline retinopathy is present
If there is a rapid improvement in glycaemic control
There has been a long duration of pre-existing diabetes.
Management during pregnancy
MJA • Volume 183 Number 7 • 3 October 2005
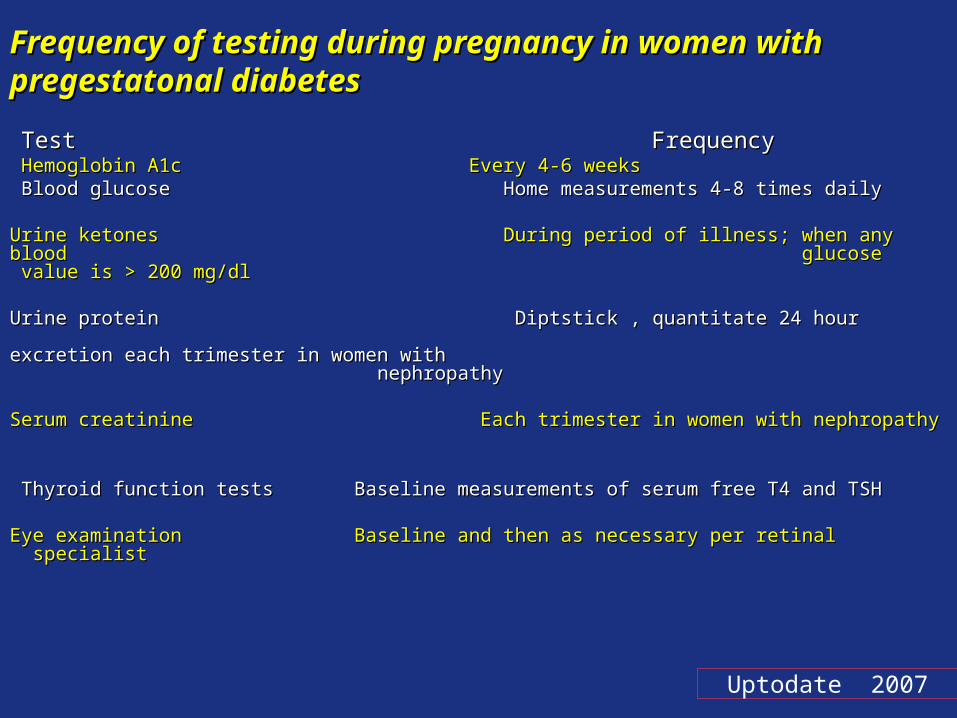
Frequency of testing during pregnancy in women with Frequency of testing during pregnancy in women with pregestatonal diabetespregestatonal diabetes
Test FrequencyTest Frequency Hemoglobin A1c Every 4-6 weeksHemoglobin A1c Every 4-6 weeks Blood glucose Home measurements 4-8 times dailyBlood glucose Home measurements 4-8 times daily
Urine ketones During period of illness; when any blood Urine ketones During period of illness; when any blood glucose value is > 200 mg/dl glucose value is > 200 mg/dl
Urine protein Diptstick , quantitate 24 hour Urine protein Diptstick , quantitate 24 hour excretion each trimester in women with excretion each trimester in women with
nephropathy nephropathy
Serum creatinine Each trimester in women with nephropathySerum creatinine Each trimester in women with nephropathy
Thyroid function tests Baseline measurements of serum free T4 and TSHThyroid function tests Baseline measurements of serum free T4 and TSH
Eye examination Baseline and then as necessary per retinal specialistEye examination Baseline and then as necessary per retinal specialist
Uptodate 2007
Fetal SurveillanceFetal SurveillanceThe priciple is to The priciple is to verify fetal viability in the firstverify fetal viability in the first trimester trimester
Validate Validate fetal structuralfetal structural integrity in the integrity in the secondsecond trimester trimester
Monitor Monitor fetal growthfetal growth during most of the during most of the thirdthird trimester trimester
And ensure And ensure fetal well-beingfetal well-being in in late thirdlate third trimester trimester
Maternal- Fetal Medicine Textbook 2004
Fetal surveillanceFetal surveillance
In the past, unexplained fetal death occurred in In the past, unexplained fetal death occurred in 10-30% 10-30% of of type 1 diabetic pregnancies associated with type 1 diabetic pregnancies associated with macrosomiamacrosomia, , hydramnioshydramnios, , preeclampsiapreeclampsia,and ,and vascular diseasevascular disease..
Fetal surveillance Fetal surveillance is of utmost importance in optimizing a is of utmost importance in optimizing a good outcome good outcome for both for both mothermother and and fetusfetus
Endocrinol Metab Clin N Am 35 (2006) 79–97

USUS is the most useful tool for the assessment of the fetus is the most useful tool for the assessment of the fetus..It can be used to:
Estimate gestational age
Screen for structural anomalies
Evaluate growth
Assess amniotic fluid volume
Determine fetal status dynamically through Doppler
and biophysical studies Endocrinol Metab Clin N Am 35 (2006) 79–97
Fetal surveillanceFetal surveillance
Macrosomia is usually defined as fetal weight greater than 4.0 kg to 4.5 kg or birth weight above the 90th percentile for gestational age
Macrosomia occurs in approximately 88% of fetuses in whom the abdominal circumference and estimated fetal weight both exceed the 90th percentile
Fetal surveillanceFetal surveillance
Endocrinol Metab Clin N Am 35 (2006) 79–97

US is essential for the evaluation of congenital anomalies .
A structural ultrasonogram can detect both neural tube defects and major cardiac defects
US is performed in the third trimester for the assessment ofgrowth and development and the presence of macrosomia.
Fetal surveillanceFetal surveillance
Endocrinol Metab Clin N Am 35 (2006) 79–97

In women who have diet-controlled gestational diabetes, fetal surveillance is not initiated usually until 40 weeks
Most centers defer testing until the 35th week if there is excellent glycemic control, but testing is started much earlier in women who have poor control, nephropathy,or hypertension
Antepartum surveillance surveillance
Endocrinol Metab Clin N Am 35 (2006) 79–97
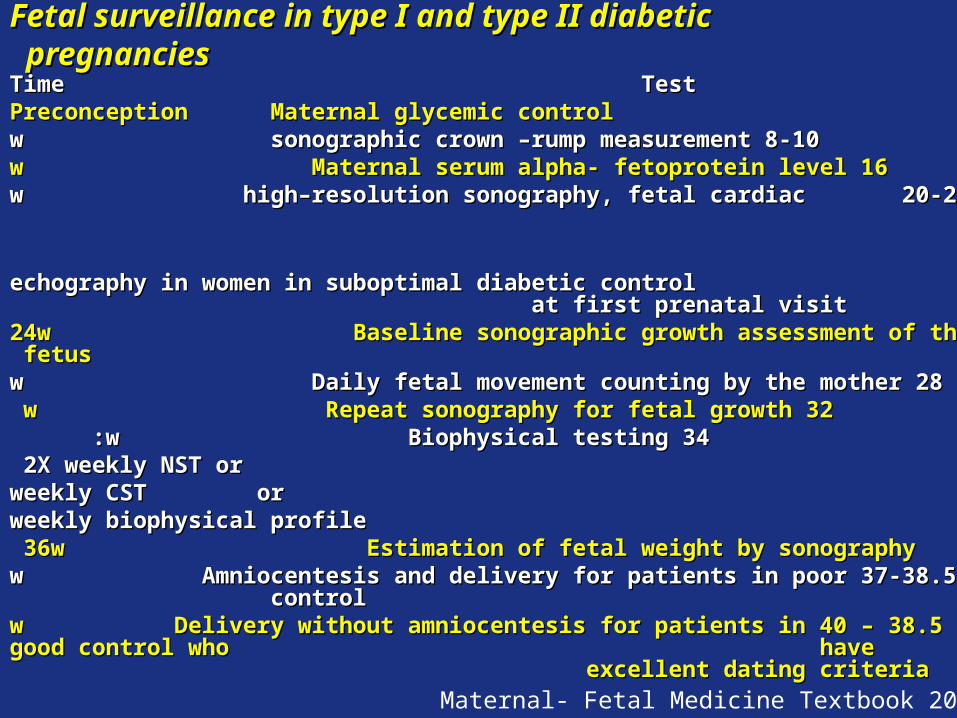
Fetal surveillance in type I and type II diabetic pregnanciesFetal surveillance in type I and type II diabetic pregnancies
Time TestTime TestPreconception Maternal glycemic controlPreconception Maternal glycemic control
8-108-10 w sonographic crown –rump measurementw sonographic crown –rump measurement1616 w Maternal serum alpha- fetoprotein levelw Maternal serum alpha- fetoprotein level
20-2220-22 w high–resolution sonography, fetal cardiac w high–resolution sonography, fetal cardiac echography in women in suboptimal diabetic control echography in women in suboptimal diabetic control
at first prenatal visit at first prenatal visit 24w Baseline sonographic growth assessment of the fetus24w Baseline sonographic growth assessment of the fetus
2828 w Daily fetal movement counting by the motherw Daily fetal movement counting by the mother3232 w Repeat sonography for fetal growthw Repeat sonography for fetal growth
3434 w Biophysical testingw Biophysical testing : : 2X weekly NST or2X weekly NST or weekly CST orweekly CST or
weekly biophysical profileweekly biophysical profile36w Estimation of fetal weight by sonography36w Estimation of fetal weight by sonography
37-38.537-38.5 w Amniocentesis and delivery for patients in poor controlw Amniocentesis and delivery for patients in poor control 38.538.5 – – 4040 ww Delivery without amniocentesisDelivery without amniocentesis for patients in good control who for patients in good control who
have excellent dating criteria have excellent dating criteria
Maternal- Fetal Medicine Textbook 2004

TESTS OF FETAL WELL - BEINGTESTS OF FETAL WELL - BEING testtestfrequencyfrequencyReassuring resultReassuring resultcommentcomment
Fetal movement Fetal movement countingcounting
Every night Every night from 28 wfrom 28 w
Ten movement in <60 minTen movement in <60 minPerformed in all patientsPerformed in all patients
Non- stress testNon- stress testTwice Twice weeklyweekly
Two heart – rate acceleration Two heart – rate acceleration in 20 minutesin 20 minutes
Being at 28-34 w with Being at 28-34 w with insulin dependent diabetesinsulin dependent diabetes
Contraction stress Contraction stress testtest
weeklyweeklyNo heart rate decelerations in No heart rate decelerations in response to ≥ 3 contrations in response to ≥ 3 contrations in
10 minutes10 minutes
Same as for non stress testSame as for non stress test
Ultrasound Ultrasound biophysical profilebiophysical profile
weeklyweeklyScore of 8 in 30 minutesScore of 8 in 30 minutes33 movement =2movement =2
11 flexion = 2flexion = 2
3030 sec breathing = 2sec breathing = 2
22 cm amniotic fluid = 2cm amniotic fluid = 2
Maternal- Fetal Medicine Textbook 2004
CONFIRMATION OF FETAL MATURITY BEFORE INDUCTION CONFIRMATION OF FETAL MATURITY BEFORE INDUCTION OR PLANNING CESAREANOR PLANNING CESAREAN
• Phosphatidyl glycerol > 3% in amniotic fluid collected from vaginal Phosphatidyl glycerol > 3% in amniotic fluid collected from vaginal pool or by amniocentesispool or by amniocentesis
• Completion of 38.5 weeks gestationCompletion of 38.5 weeks gestation
• Normal LMPNormal LMP
• First pelvic examination before 12 weeks confirm dates.First pelvic examination before 12 weeks confirm dates.
• Sonogram before 24 weeks confirm datesSonogram before 24 weeks confirm dates
• Documentation of more than 18 weeks by fetoscope of FHTDocumentation of more than 18 weeks by fetoscope of FHT
Maternal- Fetal Medicine Textbook 2004

Medications used in management of premature labour
β-sympathomimetic agents given to suppress uterine contractions and corticosteroids given to enhance fetal lung maturity .
Following administration of salbutamol, there may be a rapid rise in blood glucose level
Alternative tocolytic agents such as nifedipine are recommended. Following administration of corticosteroid, the rise in blood glucose level usually starts about 6–12 hours later, and may persist for up to 5 days
BS level monitored every 1–2 hours until glycaemic control has stabilised
MJA • Volume 183 Number 7 • 3 October 2005

DeliveryDelivery should be at term unless obstetric or medical factors dictate otherwise (eg, fetal macrosomia, polyhydramnios, poor metabolic control, preeclampsia,IUGR).
Vaginal delivery is preferable unless there is an obstetric or medical contraindication.
Birthweight exceeds 4250–4500g warrants consideration of elective caesarean section.
MJA • Volume 183 Number 7 • 3 October 2005

Indication for deliveryIndication for delivery diabetic pregnancydiabetic pregnancy
Fetal Fetal Non reactive, Positive CSTNon reactive, Positive CST
mature fetusmature fetus Sonographic evidence of fetal growth arrestSonographic evidence of fetal growth arrest
Decline in fetal growth rate with decreased amnionic Decline in fetal growth rate with decreased amnionic fluidfluid
4040 – – 4141 w gestationw gestation
Maternal Maternal Severe preeclampsiaSevere preeclampsia
Mild preeclampsia, mature fetusMild preeclampsia, mature fetus Markedly falling renal functionMarkedly falling renal function
Obstetric Obstetric ppreterm labor with failure of tocolysisreterm labor with failure of tocolysis
Mature fetus , inducible cervixMature fetus , inducible cervix
Maternal- Fetal Medicine Textbook 2004


Fetal Monitoring
Evaluations for neural tube defects and other congenital malformations begin with triple-screen testing at approximately 15 to 21 weeks of gestation.
A fetal anatomic survey is performed at 18 weeks of gestation .
Fetal echocardiography may be performed at 20 to 22 weeks of gestation

Indications for screening for CADIndications for screening for CAD::
Cardiac evaluationCardiac evaluation
women 35 years or older withe one or more:
Hypertension (blood pressure> 130/80mm Hg)
,Smoking
Positive family history
Hypercholesterolemia (LDL >100 mg/dL,HDL :<40 mg/dL)
Renal disease (microalbuminuria or nephropathy)

Fetal Monitoring
Ultrasound is used at 28 weeks of gestation to evaluatefetal growth and the quantity of amniotic fluid.
Fetal surveillance,including nonstress test and biophysical profile as well as maternal monitoring of fetal activity is
initiated in the third trimester to reduce the risk of stillbirth .
labor and Delivery
The method of delivery is based on the usual obstetric indications,as well as on fetal weight and the presence or absence of active retinal changes. Infants of diabetic mothers are more likely to be macrosomic.
Cesarean sections are recommended for fetuses of an estimated weight greater than 4,500 g.
It is important to maintain euglycemia during labor or prior
to a scheduled cesarean section .
Postpartum Management
Insulin dosing should be titrated daily toward the preconception dose as necessary.
Urine microalbumin, thyroid function, and HbAlcshould be reevaluated .
The American Academy of Pediatrics considers the ACEIs captopril and enalapril safe for use by the breastfeeding mother and are resumed in patients with nephropathy,
microalbuminuria and hypertension .
First trimesterFirst trimester
Same as preconception counseling careSame as preconception counseling care
Evaluate risk factorsEvaluate risk factors
Second trimesterSecond trimester
Visit the pt every 2 to 4 weeks or more if pt has complications or Visit the pt every 2 to 4 weeks or more if pt has complications or glycemic control is suboptimal .glycemic control is suboptimal .
Maternal analyte screening : screening for aneuploidy or neural Maternal analyte screening : screening for aneuploidy or neural tube defects ( tube defects ( αα fetoprotein ,unconjucated estriol ,HCG,inhibin fetoprotein ,unconjucated estriol ,HCG,inhibin A )A )
Diabetes does not increase the risk of fetal aneuploidy.Diabetes does not increase the risk of fetal aneuploidy.
Sonography : at 18 weeks of gestation Sonography : at 18 weeks of gestation
Third trimesterThird trimester
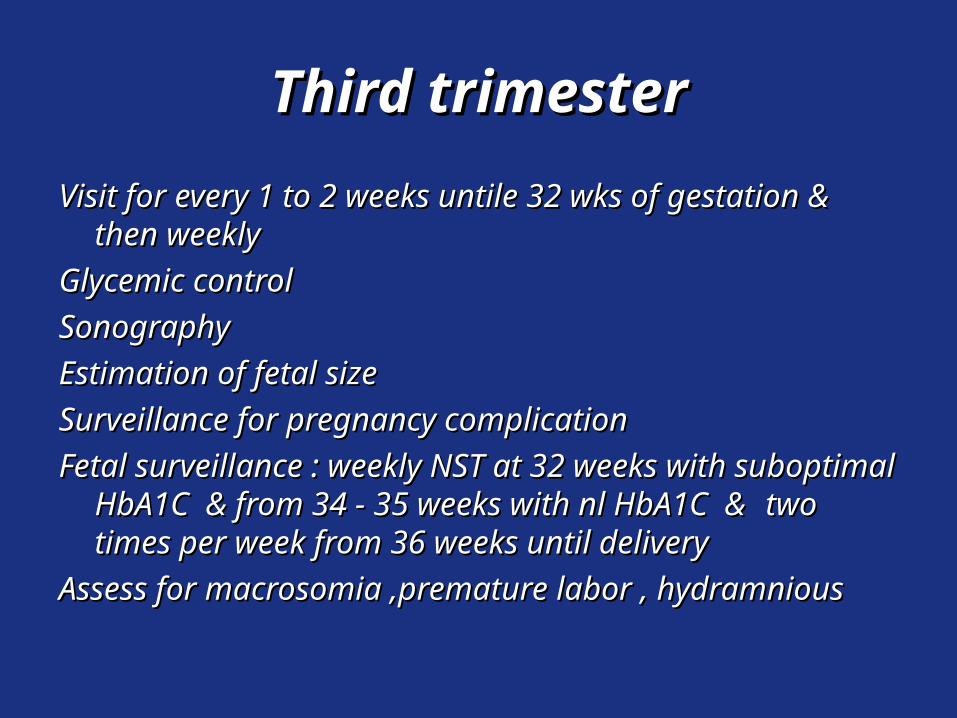
Visit for every 1 to 2 weeks untile 32 wks of gestation & then Visit for every 1 to 2 weeks untile 32 wks of gestation & then weekly weekly
Glycemic controlGlycemic control
Sonography Sonography
Estimation of fetal size Estimation of fetal size
Surveillance for pregnancy complicationSurveillance for pregnancy complication
Fetal surveillance : weekly NST at 32 weeks with suboptimal Fetal surveillance : weekly NST at 32 weeks with suboptimal HbA1C & from 34 - 35 weeks with nl HbA1C &HbA1C & from 34 - 35 weeks with nl HbA1C & two times two times per week from 36 weeks until deliveryper week from 36 weeks until delivery
Assess for macrosomia ,premature labor , hydramnious Assess for macrosomia ,premature labor , hydramnious
Fetal SurveillanceFetal Surveillance
The goals of management of diabetic pregnancy are to The goals of management of diabetic pregnancy are to prevent stillbirth and asphyxia while minimizing maternal prevent stillbirth and asphyxia while minimizing maternal morbidity associated with delivery. This involves morbidity associated with delivery. This involves monitoring fetal growth in order to select the proper monitoring fetal growth in order to select the proper timing and route of delivery. The first is testing fetal well- timing and route of delivery. The first is testing fetal well- being at frequent intervals and fetal sizebeing at frequent intervals and fetal size..
The priciple is to verify fetal viability in the first trimesterThe priciple is to verify fetal viability in the first trimester
Validate fetal structural integrity in the second trimesterValidate fetal structural integrity in the second trimester
Monitor fetal growth during most of the third timesterMonitor fetal growth during most of the third timester
Ensure fetal well-bing in the late third trimesterEnsure fetal well-bing in the late third trimester
Fetal SurveillanceFetal Surveillance

glycemic control plays an important role in reducing the frequency of fetal and neonatal complications.
) HbA1C values are useful in evaluating a woman's glycemic control early in pregnancy .
One goal of preconception care of women with diabetes is to evaluate glycemic control and recommend adjustments in diet, medications, and lifestyle, as needed, to achieve euglycemia.
Type 2 diabetics on oral anti-hyperglycemic agents should be switched to insulin therapy preconceptionally
Prepregnancy evaluation and counseling of women DM Prepregnancy evaluation and counseling of women DM
→→ minimize the risk to the minimize the risk to the F&MF&M
Women who are in poor glycemic control during the Women who are in poor glycemic control during the period of fetal organogenesis, which is nearly period of fetal organogenesis, which is nearly complete by seven weeks postconception, have a complete by seven weeks postconception, have a high incidence of spontaneous abortion and fetuses high incidence of spontaneous abortion and fetuses with congenital anomalies with congenital anomalies
Thus, the importance of evaluating glycemic control in Thus, the importance of evaluating glycemic control in
women with DM and achieving good glycemic women with DM and achieving good glycemic control before conception cannot be overstated.control before conception cannot be overstated.
Hyperglycemia is probably the most important determinant Hyperglycemia is probably the most important determinant of these risks.of these risks.
This conclusion is supported by repeated observations that This conclusion is supported by repeated observations that normalizing blood glucose concentrations before and normalizing blood glucose concentrations before and early in pregnancy can reduce the risk of spontaneous early in pregnancy can reduce the risk of spontaneous abortion and congenital malformations to nearly that of abortion and congenital malformations to nearly that of normal women normal women
The three major potential fetal/pregnancy complications The three major potential fetal/pregnancy complications among women with pregestational diabetes are: congenital among women with pregestational diabetes are: congenital malformations, spontaneous abortion, and macrosomia. malformations, spontaneous abortion, and macrosomia.
Information and counselling should be provided to all women of reproductive age with diabetes
A meta-analysis has demonstrated a significantly lower prevalence of major congenital anomalies in offspring of women who attended for prepregnancy counselling (relative risk, 0.36; 95% CI, 0.22–0.59; absolute risk, 2.1% v 6.5%).
Management of women with diabetes before conception
Assessment of renal functionAssessment of renal function
Spot urine for microalbumin /cr or time Spot urine for microalbumin /cr or time collection for 24 hrscollection for 24 hrs
Serum crSerum cr
Cr> 2mg/dl & GFR < 50 ml/min. & proteinuria Cr> 2mg/dl & GFR < 50 ml/min. & proteinuria more than 2 gr /day can be considered more than 2 gr /day can be considered relative contraindications to pregnancy relative contraindications to pregnancy

Initial prepregnancy assessment should document baseline Initial prepregnancy assessment should document baseline renal function, include protein excretion, serum creatinine, renal function, include protein excretion, serum creatinine, and creatinine clearanceand creatinine clearance
The risk of permanent decline in renal function is substantially The risk of permanent decline in renal function is substantially increased in women with a urine creatinine concentration increased in women with a urine creatinine concentration above 2.0 mg/dL many of whom have more than 2 g of above 2.0 mg/dL many of whom have more than 2 g of proteinuria per dayproteinuria per day..
These findings can be considered relative contraindications to These findings can be considered relative contraindications to pregnancypregnancy . .
A creatinine clearance below 50 mL/min before pregnancy is A creatinine clearance below 50 mL/min before pregnancy is associated with a high prevalence of hypertension and fetal associated with a high prevalence of hypertension and fetal wastagewastage
Preconception treatment goalPreconception treatment goal
PlasmaPlasma– FBS: 80-110FBS: 80-110
– 2hpp : 100-1552hpp : 100-155
– HbA1C : < 7% ; normal if possibleHbA1C : < 7% ; normal if possible
– Avoid hypoglycemiaAvoid hypoglycemia
Joslin text book 2005

Cardiac evaluationCardiac evaluation
Testing may include one or more of the following :
electrocardiogram, echocardiogram, and exercise
tolerance testing with the recognition that the resting
electrocardiogram is the least sensitive of these tests.
Thyroid disordersThyroid disorders
Prepregnancy evaluation should include measurement of Prepregnancy evaluation should include measurement of serum TSHserum TSH

Preconception counselingPreconception counselingEducation Education
Maternal risk assessmentMaternal risk assessment
Fetal risk assessment
Metabolic goals should be established prior to conception
Self-management skills should be reviewed.
Nutrition counseling to establish an individualized meal plan should be provided.

Daily folic acid : 1 mg prior conception & continue after Daily folic acid : 1 mg prior conception & continue after conceptionconception
Mental health professional should be availableMental health professional should be available
A formal dilated funduscopic examination and clearance for pregnancy by an ophthalmologist

Treatment of Diabetes during Pregnancy
Home blood glucose monitoring is performed a minimum of four times daily,including before breakfast, 2 hours after meals,
before driving,and with signs or symptoms of hypoglycemia .
Premeal and middle-of-the-night testing may be necessary in some patients.
First-void urine samples are tested for ketones.
Insulin requirements: what to expect
Hypoglycaemia, especially overnight, is more frequent from the 6th to 18th weeks of gestation
Insulin requirements can fall after 32 weeks
Any fall greater than 5%–10% should lead to an assessment of fetal wellbeing

First trimester ultrasound examinationFirst trimester ultrasound examination
First trimester USFirst trimester US examination is often obtained to examination is often obtained to document viabilitydocument viability
As the rate of spontaneous As the rate of spontaneous abortion is higherabortion is higher in diabetic in diabetic women women
andand
To assist in estimation of To assist in estimation of gestational agegestational age
Uptodate 2007
Fetal assessment
Screening for fetal anomalies should be done with first and second trimester
ultrasound and a fetal echocardiogram between 20 and 22 weeks’ gestation. As
Obstet Gynecol Clin N Am 31 (2004) 907– 933

Fetal Risk

Obstetric management
US examination for fetal morphology should be offered at 18–20 weeks .
Further examinations to assess fetal growth should be performed at 28–30 weeks and repeated at 34–36
weeks .
The latter will help to determine the timing and route of delivery .
MJA • Volume 183 Number 7 • 3 October 2005

















