jo ur nal home p age: www. elsev ier .com/ locate / reprotox
regnancy outcome following gestational exposure toNF-alpha-inhibitors: A prospective, comparative,bservational study
rna Diav-Citrina,b,∗, Anna Otcheretianski-Volodarskyc,vetlana Shechtmana, Asher Ornoya,b
The Israeli Teratology Information Service, Israel Ministry of Health, Jerusalem, IsraelThe Hebrew University Hadassah Medical School, Jerusalem, IsraelThe Division of Clinical Pharmacy, the Hebrew University of Jerusalem, Israel
r t i c l e i n f o
rticle history:eceived 2 May 2013eceived in revised form 29 October 2013ccepted 14 November 2013vailable online 24 November 2013
eywords:nti-TNF-�
a b s t r a c t
Objective: To evaluate pregnancy safety of anti-TNF-� medications.Design: Prospective, comparative, observational study done at the Israeli Teratology Information Servicebetween 2002 and 2011.Results: 83 anti-TNF-�-exposed-pregnancies (97.6% in the first trimester, T1) were followed-up andcompared with 86 disease-matched (DM) and 341 non-teratogenic-exposed (NTE) pregnancies. Theanti-TNF-� group consisted of 35 infliximab-, 25 etanercept-, and 23 adalimumab-exposed pregnan-cies. The rate of major congenital anomalies did not significantly differ between the three groups [3/65
(4.6%) (anti-TNF-�, T1), 5/79 (6.3%) (DM), 8/336 (2.4%) (NTE)], even after excluding genetic or cytogeneticanomalies [3/65 (4.6%) (anti-TNF-�, T1), 4/79 (5.1%) (DM), 6/336 (1.8%) (NTE)]. There were no cases ofVATER/VACTERL association.Conclusion: The present study suggests that anti-TNF-� treatment does not pose a major teratogenic riskin humans. This conclusion is based on relatively small numbers of exposed pregnancies and should beinterpreted with caution. Larger studies are needed to establish anti-TNF-� pregnancy safety.
. Introduction
Infliximab, etanercept, and adalimumab are tumor necrosisactor-� inhibitors (anti-TNF-�) produced by genetic engineering.nfliximab is a mouse-human chimeric monoclonal IgG1 anti-ody, etanercept is a TNF receptor-IgG1 fusion human protein,nd adalimumab is a fully human monoclonal antibody. Anti-TNF-
medications have led to a vast improvement in the treatmentf inflammatory conditions. These new biopharmaceuticals targetnflammatory cytokines, and are used in the treatment of autoim-
une diseases including rheumatoid arthritis, psoriatic arthritis,uvenile idiopathic arthritis, ankylosing spondylitis, and inflamma-ory bowel diseases. Many of these illnesses are more common in
omen and occur during reproductive age. When anti mouse TNF-
monoclonal antibody was administered to pregnant mice, thereere no teratogenic effects [1]. The three anti-TNF-� antibodies,
∗ Corresponding author at: The Israeli Teratology Information Service Israel Min-stry of Health, P.O. Box 1176, Jerusalem 9446724, Israel. Tel.: +972 2 5080441;ax: +972 2 6474822.
infliximab, etanercept, and adalimumab, have a large molecularweight of approximately 149 kDa, and are, therefore, not expectedto cross the human placenta in significant concentration in thefirst trimester of pregnancy. It is hypothesized, however, that theFab’ fragment may passively cross the placenta in low levels inthe first trimester during the period of organogenesis. Placentaltransfer of infliximab, etanercept, and adalimumab close to termhas been documented [2–5]. The terminal elimination half-livesof these molecules are relatively long: 4 days for etanercept [6], 19days for infliximab [7], and 15–19 days for adalimumab [8]. Humanpregnancy experience with these medications is rather limited. It isbased mostly on case reports, small case series, regulatory agencyrecords, manufacturer’s registries, and preliminary data presentedat scientific meetings published as abstracts. Human pregnancydata on infliximab specifically [9] and on anti-TNF-� medicationsin general [10] has been summarized in two recent review articles.
Carter et al. [11] published a case report describing VATERassociation in a neonate born to a mother who was treated
with etanercept during pregnancy. They reviewed the TNF-�-antagonists use in pregnancy report to the US Food and DrugAdministration. They reported that 24 of the 41 children withcongenital anomalies born to mothers who took infliximab or
tanercept during pregnancy had one or more anomalies that areart of the VACTERL association [12]. They concluded that maternalreatment with TNF antagonists pose an increased risk for VATER orACTERL association. A critical editorial [13] and a letter to the edi-
or [14] published in the same journal raised questions and pointedut numerous methodological problems in this study. The analysisuffers from selection bias, is based on voluntary reports lacking aenominator of total number or pregnancies with maternal anti-NF-� treatment and, therefore, cannot be used for risk calculation.poradic reports of isolated anomalies that could be a part of theACTERL association do not establish this diagnosis. The diagnosisequires a constellation of anomalies in the same patient. Thetudy did not address potential confounders. In addition, placentalransmission of these molecules during the first trimester of preg-ancy, covering the period of organ formation, is not expected inignificant amounts, and makes the suggested causation betweenACTERL association and anti-TNF-� medications, unlikely.
Contrary to the reports by Carter et al. [11,12], human pregnancyxperience with TNF-� antagonists has been mostly reassuring5,15–28]. A summary of the reports of pregnancies with exposureo anti-TNF-� medications is presented in Table 1.
The primary objective of the present study was to prospectivelyvaluate the rate of major congenital anomalies after mater-al treatment with TNF-�-antagonists (infliximab, etanercept, ordalimumab) during pregnancy compared with two compari-on groups: (1) pregnant women with autoimmune diseases notreated with anti-TNF-� medications during pregnancy (disease
atched), (2) pregnant women counseled for non-teratogenicxposure. Secondary endpoints of interest were pregnancy out-ome, birth weight, and gestational age at delivery.
. Materials and methods
Pregnant women counseled by the Israeli Teratology Informa-ion Service (TIS), Jerusalem, in regard to the TNF-�-antagonists,nfliximab, etanercept, or adalimumab, between the years 2002 and011, were enrolled in the present prospective comparative obser-ational study. Exposure during the first trimester of pregnancyas defined when the pregnant woman received an anti-TNF-�
efore pregnancy, but conception occurred within 5 eliminationalf-lives from medication administration, or if the woman wasreated during pregnancy before 13 completed weeks from herast menstrual period. Outcome was compared with two compar-son groups in a similar time frame: (1) pregnant women withimilar autoimmune diseases not treated with anti-TNF-� medi-ations during pregnancy at a 1:1 ratio. This disease matched (DM)roup was selected according to their disease from the Israeli TISatabase and was either treated with medications other than anti-NF-� excluding methotrexate, or untreated during pregnancy; (2)regnant women counseled for non-teratogenic exposure (NTE)t a 1:4 ratio. This group was randomly selected from the IsraeliIS database according to their exposure and included womenounseled during pregnancy in regard to exposures known to beon-teratogenic or fetal toxic such as analgesics like paracetamol,
ow dose diagnostic radiation, topical preparations with negligibleystemic exposure, antibiotics (penicillins or cephalosporins), oralontraceptives taken no longer than the 5th week of pregnancy,air dye or house-cleaning agents. Pregnancies of women who havehronic diseases were not included in the NTE group. Details ofxposure were collected during pregnancy, at the initial contactith the TIS and before pregnancy outcome was known, using a
tructured questionnaire. Verbal consent to participate in the studyas given by the woman at initial contact. Since the study was
bservational no Institutional Review Board approval was required.n addition, the following information was recorded at the initial
Toxicology 43 (2014) 78– 84 79
contact: maternal demographics, medical and obstetrical histories,and exposure details (dose, duration, and timing in pregnancy,additional exposures). Retrospective cases were not included in thestudy. Pregnant women who contacted the TIS after an anomalyhad been identified on prenatal testing were also excluded. Preg-nancy outcome was actively sought after the expected date ofdelivery in the exposed and comparison groups. Follow-up wasconducted by a telephone interview with the woman to obtaindetails on the pregnancy outcome, gestational age at delivery,birth weight, congenital anomalies and neonatal complications.In cases of anomalies an attempt to obtain medical records wasmade. In addition, all exposures were ascertained. It was verifiedthat the exposure/s the woman was counseled for indeed occurredduring pregnancy. Details on any dose modifications during preg-nancy, exact timing and duration of treatment, and additionalexposures during pregnancy were also ascertained. The vast major-ity of infants in Israel are delivered in hospital. Each neonate inIsrael undergoes at least two physical examinations before beingdischarged from the hospital. All neonates in the present studywere delivered in hospital. The interview was conducted afterthese physical examinations. Data collection methods were sim-ilar in the exposed and comparison groups. Major anomalies weredefined as structural abnormalities in the offspring that have seri-ous medical, surgical or cosmetic consequences. The focus of thestudy was on anomalies that occur during the period of organo-genesis in the first trimester of pregnancy. Therefore, an inguinalhernia in a term infant, as well as cryptorchidism, that occur laterin pregnancy, were not considered major anomalies. Children withminor anomalies or functional problems without any morphologi-cal changes (e.g. ankyloglossia, umbilical hernia that spontaneouslyclosed, systolic heart murmur with normal echocardiography) orinfants with complications of preterm delivery were not consideredas having major anomalies. Cardiac septal defects are structuralanomalies of the heart, and are considered major anomalies inthe present study, even if spontaneously resolved, unless the clo-sure occurred during the neonatal period. Any ventricular septaldefect carries a risk of infectious endocarditis and may requireprophylactic antibiotics before invasive procedures. Horseshoe kid-ney is classified as a major anomaly because it carries a risk forrenal cancer especially Wilms’ tumor, renal calculi and obstruc-tive uropathy. Primary congenital hypothyroidism is considered amajor anomaly in the present study because it requires lifelongreplacement therapy. In addition, its etiology in the majority ofcases, is either thyroid ectopy or athyreosis, both resulting from firsttrimester events. Abnormalities detected by prenatal ultrasonogra-phy (if verified postnatally or by autopsy) were included in ourstudy, since antenatal screening for major anomalies is routinelyperformed in Israel. The classification of anomalies was done by acertified pediatrician blinded to the exposure group. An interna-tional expert was consulted in case of classification difficulty. Thus,the analysis of major congenital anomalies was performed amonglive-born infants, pregnancy losses with confirmed anomalies, andelective terminations of pregnancy due to prenatally diagnosedanomalies. In the case of multiple births, each live-born offspringwas included in the analysis. Gestational age was defined fromthe last menstrual period. Miscarriage was defined as spontaneouspregnancy loss before or at 20 completed weeks, whereas stillbirthwas defined as spontaneous pregnancy loss beyond 20 completedweeks. Preterm delivery was defined as birth before 37 completedweeks. All co-authors had access to the study data and had reviewedand approved the final manuscript.
2.1. Statistical analysis
Categorical data were compared using �2 or Fisher exact testsand are expressed as ratios or percentages. Continuous data are
80 O. Diav-Citrin et al. / Reproductive Toxicology 43 (2014) 78– 84
Table 1Summary of reports of pregnancies with exposure to anti-TNF-� medications.
Reference Medication n (n T1) Anomalies Design
Katz et al., [15] Infliximab 96 (58) - Tetralogy of Fallot- Intestinal malrotation
Manufacturer’s data retrospective voluntary reportscompared to National health statistics
Chambers et al. [16] EtanerceptInfliximab
294
- Trisomy 18 Prospective comparative OTIS study (abstract)
Mahadevan et al. [17] Infliximab 10 (9) None Retrospective international chart review
Lichtenstein et al. [18,19] Infliximab 117* - VSD*- Anencephaly*
Prospective observational multicenter registry in NorthAmerican patients with CD TREAT
Roux et al. [20] EtanerceptAdalimumab
2 (2)1 (1)
None Prospective small case series
Berthelot et al. [21] InfliximabAdalimumabEtanercept
3 (1)2 (1)10 (10)
None French rheumatologist website questionnaire
Carter et al. [12] EtanerceptInfliximab
2219
24/41 had one or moreanomalies that are partof the VACTERLassociation
Review of malformed and exposed in FDA Adverse EventReporting System
Rump and Schönborn [22] Etanercept 8 - Megacolon Case series
Zelinkova et al. [3] Infliximab 4 (4) - Polydactyly Lt hand Case series
Verstappen et al. [23] InfliximabEtanerceptAdalimumab
61 (61) [3 anti-TNF-] - CDH- Pyloric stenosis
British Society for Rheumatology Biologics Register(prospective)
Schnitzler et al. [24] InfliximabAdalimumab
35 (35)7 (7)
- Trisomy 18 Belgian comparative observational study
Weber-Schoendorfer et al. [25] InfliximabAdalimumab
25 (25)28 (28)
- Neurofibromatosis- VSD- Growinghemangiomas
Prospective uncontrolled cohort, Berlin TIS (abstract)
Hultzsch et al. [26] Etanercept 26 (26) - Renal agenesis- Hypoplastic Lt heart &hypospadias- Wolf Parkinson WhiteSyndrome
Prospective uncontrolled cohort, Berlin TIS (abstract)
Chambers et al. [27] Adalimumab 66 (66) Major anomalies in3.1%, no evidence ofpattern
Prospective comparative OTIS study (abstract)
Viktil et al. [28] EtanerceptAdalimumab
22 (20)3 (3)
None Norway Medical Birth Registry linked to prescriptiondatabase comparative study
Mahadevan et al. [5] InfliximabAdalimumabCertolizumab
11 (11)10 (10)10 (7)
None Prospective PIANO Registry
n availa– ists; CF – Preg
p(dfgbmVaU
3
naotielp
was 50 mg (IQR 50–50) for etanercept, and 20 mg (IQR 20–20) foradalimumab. Concurrent medications during pregnancy in addi-tion to the anti-TNF-� were taken by 43.4% of the women and arepresented in Table 2. Co-administration of methotrexate within 1
Table 2Distribution of medications in the anti-TNF-� (concurrent) and the DM groups.
Medications Anti-TNF-� (%) DM (%)
Steroids 10.8 3.5nb-DMARDs 20.5 64.0Blood thinners 3.6Steroids and nb-DMARDs 4.8 18.6nb-DMARDs and blood thinners 2.4 3.5Steroids, nb-DMARDs and blood thinners 1.2
– exposed pregnancies; (n T1) – pregnancies exposed in the first trimester; when
congenital dysplasia of hip; OTIS – Organization of Teratology Information SpecialDA – Food and Drug Administration; TIS – Teratology Information Service; PIANO
resented using mean ± SD or median with interquartile rangeIQR), and compared using the ANOVA or Kruskal–Wallis test,epending on whether they followed normal distribution, or not,or three groups, or using Student-t or Mann–Whitney tests, for tworoups. The p-values presented in the tables are for a comparisonetween the three groups. For pair-wise comparisons Bonferroniethod was applied. Statistical calculations were done using SPSSersion 19 or Epi InfoTM software (Center for Disease Controlnd Prevention, Atlanta Epidemiology Program Office, Atlanta, GA,SA).
. Results
A total of 83 TNF-�-antagonist-exposed pregnancies, 86 preg-ancies of women with autoimmune diseases not treated withnti-TNF-� medications during pregnancy, and 341 pregnanciesf women counseled for non-teratogenic exposure, were prospec-ively followed-up. The anti-TNF-� group consisted of 35 (42.2%)
nfliximab, 25 (31.1%) etanercept, and 23 (27.7%) adalimumabxposed pregnancies. Exposure to an anti-TNF-� medication ateast in the first trimester of pregnancy occurred in 81 of 83 (97.6%)regnancies. In the two remaining pregnancies the anti-TNF-� was
ble; * – cited by Chambers et al. [10]; VSD – ventricular septal defect; Lt – left; CDHD – Crohn’s Disease; TREAT – Therapy, Resource, Evaluation, and Assessment Tool;nancy IBD And Neonatal Outcomes.
administered only later in pregnancy, starting in the second or thirdtrimesters. The median gestational week of treatment discontinu-ation was 9 (IQR 4–28). The median infliximab dose per infusionwas 300 mg (IQR 255–300) with a median interval of 8 weeksbetween infusions (IQR 4–8), whereas the median weekly dose
nb-DMARDs – non-biologic disease modifying antirheumatic drugs; azathioprine,6-mercaptopurine, methotrexate (only in the anti-TNF-� group), mesalamine,sulfasalazine, or hydroxychloroquine; Blood thinners: low dose aspirin or lowmolecular weight heparin.
O. Diav-Citrin et al. / Reproductive
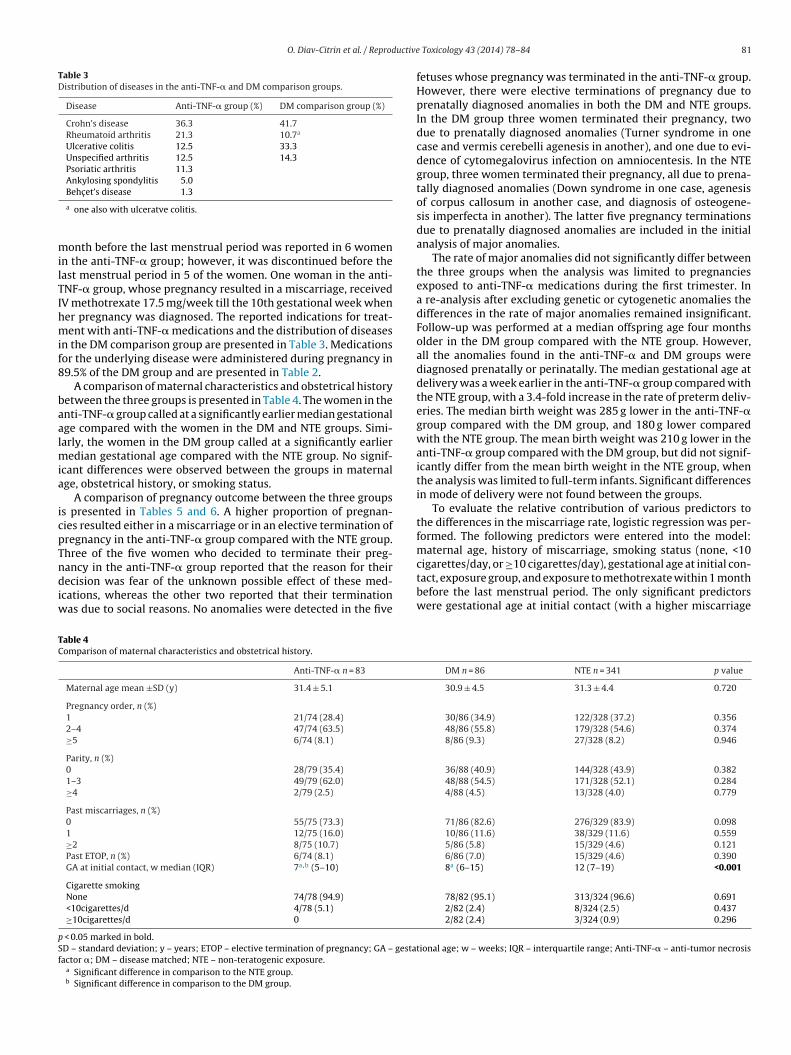
Table 3Distribution of diseases in the anti-TNF-� and DM comparison groups.
Disease Anti-TNF-� group (%) DM comparison group (%)
cigarettes/day, or ≥10 cigarettes/day), gestational age at initial con-
TC
pSf
Behc et’s disease 1.3
a one also with ulceratve colitis.
onth before the last menstrual period was reported in 6 womenn the anti-TNF-� group; however, it was discontinued before theast menstrual period in 5 of the women. One woman in the anti-NF-� group, whose pregnancy resulted in a miscarriage, receivedV methotrexate 17.5 mg/week till the 10th gestational week whener pregnancy was diagnosed. The reported indications for treat-ent with anti-TNF-� medications and the distribution of diseases
n the DM comparison group are presented in Table 3. Medicationsor the underlying disease were administered during pregnancy in9.5% of the DM group and are presented in Table 2.
A comparison of maternal characteristics and obstetrical historyetween the three groups is presented in Table 4. The women in thenti-TNF-� group called at a significantly earlier median gestationalge compared with the women in the DM and NTE groups. Simi-arly, the women in the DM group called at a significantly earlier
edian gestational age compared with the NTE group. No signif-cant differences were observed between the groups in maternalge, obstetrical history, or smoking status.
A comparison of pregnancy outcome between the three groupss presented in Tables 5 and 6. A higher proportion of pregnan-ies resulted either in a miscarriage or in an elective termination ofregnancy in the anti-TNF-� group compared with the NTE group.hree of the five women who decided to terminate their preg-ancy in the anti-TNF-� group reported that the reason for their
ecision was fear of the unknown possible effect of these med-
cations, whereas the other two reported that their terminationas due to social reasons. No anomalies were detected in the five
able 4omparison of maternal characteristics and obstetrical history.
Anti-TNF-� n = 83
Maternal age mean ±SD (y) 31.4 ± 5.1
Pregnancy order, n (%)1 21/74 (28.4)
2–4 47/74 (63.5)
≥5 6/74 (8.1)
Parity, n (%)0 28/79 (35.4)
1–3 49/79 (62.0)
≥4 2/79 (2.5)
Past miscarriages, n (%)0 55/75 (73.3)
1 12/75 (16.0)
≥2 8/75 (10.7)
Past ETOP, n (%) 6/74 (8.1)
GA at initial contact, w median (IQR) 7a,b (5–10)
Cigarette smokingNone 74/78 (94.9)
<10cigarettes/d 4/78 (5.1)
≥10cigarettes/d 0
< 0.05 marked in bold.D – standard deviation; y – years; ETOP – elective termination of pregnancy; GA – gestaactor �; DM – disease matched; NTE – non-teratogenic exposure.
a Significant difference in comparison to the NTE group.b Significant difference in comparison to the DM group.
Toxicology 43 (2014) 78– 84 81
fetuses whose pregnancy was terminated in the anti-TNF-� group.However, there were elective terminations of pregnancy due toprenatally diagnosed anomalies in both the DM and NTE groups.In the DM group three women terminated their pregnancy, twodue to prenatally diagnosed anomalies (Turner syndrome in onecase and vermis cerebelli agenesis in another), and one due to evi-dence of cytomegalovirus infection on amniocentesis. In the NTEgroup, three women terminated their pregnancy, all due to prena-tally diagnosed anomalies (Down syndrome in one case, agenesisof corpus callosum in another case, and diagnosis of osteogene-sis imperfecta in another). The latter five pregnancy terminationsdue to prenatally diagnosed anomalies are included in the initialanalysis of major anomalies.
The rate of major anomalies did not significantly differ betweenthe three groups when the analysis was limited to pregnanciesexposed to anti-TNF-� medications during the first trimester. Ina re-analysis after excluding genetic or cytogenetic anomalies thedifferences in the rate of major anomalies remained insignificant.Follow-up was performed at a median offspring age four monthsolder in the DM group compared with the NTE group. However,all the anomalies found in the anti-TNF-� and DM groups werediagnosed prenatally or perinatally. The median gestational age atdelivery was a week earlier in the anti-TNF-� group compared withthe NTE group, with a 3.4-fold increase in the rate of preterm deliv-eries. The median birth weight was 285 g lower in the anti-TNF-�group compared with the DM group, and 180 g lower comparedwith the NTE group. The mean birth weight was 210 g lower in theanti-TNF-� group compared with the DM group, but did not signif-icantly differ from the mean birth weight in the NTE group, whenthe analysis was limited to full-term infants. Significant differencesin mode of delivery were not found between the groups.
To evaluate the relative contribution of various predictors tothe differences in the miscarriage rate, logistic regression was per-formed. The following predictors were entered into the model:maternal age, history of miscarriage, smoking status (none, <10
tact, exposure group, and exposure to methotrexate within 1 monthbefore the last menstrual period. The only significant predictorswere gestational age at initial contact (with a higher miscarriage
82 O. Diav-Citrin et al. / Reproductive Toxicology 43 (2014) 78– 84
Table 5Comparison of pregnancy outcome.
Anti-TNF-� n = 83 DM n = 86 NTE n = 341
Multiple gestations 0 0 6 twin setsDelivery of live-born infant, n (%) 67/83 (80.7)a 77/86 (89.5) 328/341 (96.2)Miscarriage, n (%) 9/83 (10.8)a 5/86 (5.8) 10/341 (2.9)ETOP, n (%) 5/83 (6.0)a 3/86 (3.5) 3/341 (0.9)Stillbirth, n (%) 1/83 (1.2) 1/86 (1.2) 0Ectopic pregnancy, n (%) 1/83 (1.2) 0 0Major anomalies, n (%) 3/65* (4.6) 5/79 (6.3) 8/336 (2.4)Major anomalies, excluding genetic or cytogenetic anomalies, n (%) 3/65* (4.6) 4/79 (5.1) 6/336 (1.8)
ETOP – elective termination of pregnancy; Anti-TNF-� – anti-tumor necrosis factor �; DM – disease matched; NTE – non-teratogenic exposure;a Significant difference in comparison to the NTE group.* Among women treated with anti-TNF-� medications during the first trimester of pregnancy.
Table 6Comparison of age at follow-up, mode and time of delivery, and birth weight.
Anti-TNF-� n = 83 DM n = 86 NTE n = 341 p value
Age at F/U, m median (IQR) 14 (5–35) 16a (4–42) 12 (6–19) 0.031Mode of deliveryVaginal uncomplicated, n (%) 43/66 (65.2) 50/76 (65.8) 223/326 (68.4) 0.823Cesarean section, n (%) 22/66 (33.3) 19/76 (25.0) 84/326 (25.8) 0.419Vacuum delivery, n (%) 1/66 (1.5) 7/76 (9.2) 19/326 (5.8) 0.146GA at delivery, w median (IQR) 38a (37–40) 39 (37–40) 39 (38–40) <0.001Preterm delivery, <37 w, n (%) 15/66a (22.7) 11/77 (14.3) 22/327 (6.7) <0.001Birth weight, g median (IQR) 2975a,b (2528–3276) 3260 (2900–3475) 3155 (2853–3483) 0.002Birth weight of full-term infants, g mean (±SD) 3085b ± 520 3295 ± 394 3211 ± 456 0.049
p < 0.05 marked in bold.GA – gestational age; w – weeks; F/U – follow-up; m – months; IQR – interquartile range; g – grams; SD – standard deviation; Anti-TNF-� – anti-tumor necrosis factor �;D
rsf0
t
TM
DtFs
M – disease matched; NTE – non-teratogenic exposure.a Significant difference in comparison to the NTE group.b Significant difference in comparison to the DM group.
ate among women calling early during gestation) (p < 0.001) andmoking of less than 10 cigarettes/d (p = 0.010). The adjusted ORor miscarriages in the anti-TNF-� vs. NTE group was 1.96 (95%CI
.64–5.96).
The reported major anomalies and the details of exposures inhe anti-TNF-� and DM groups are listed in Table 7.
able 7ajor congenital anomalies in the anti-TNF-� and DM groups.
Group Type of anomaly Details of exposure, additional exposures,maternal illness
Anti-TNF-� VSD Adalimumab 40 mg/2 w TO pregnancy,azathioprine 50 mg/d till w 9, Crohn’sdisease
M – disease matched; * – not included in the re-analysis excluding genetic or cytogehroughout pregnancy; w – week; T1 – first trimester; HCQ – hydroxychloroquine; MTX –
The results of the present prospective comparative study sug-
gest that treatment with the anti-TNF-� medications, infliximab,etanercept, or adalimumab, is not associated with an increased riskof major anomalies. These results, however, are consistent with
Pregnancy outcome,GA (w), sex, BW (g)
F/U comments
Delivery, 40, F, 2075 Small VSD diagnosed on U/S at w 20, prenataland postnatal echocardiography,spontaneously closed at 6 m
Delivery, 36, M, 3190 Diagnosed on prenatal U/S
Delivery, 31, F, 2740 Fetal edema diagnosed on late U/S, DIC,thrombocytopenia, anemia, severe RDS,edema, ecchymosis, jaundice (phototherapy),PDA, renal failure, recurrent blood exchange,PLT/PC/FFP transfusions, ampicillin, gentamicinfor 3d, vancomycin for 6d, TPN from 2nd d,died on 10th d pathologic diagnosis on PM
ETOP, 22 Diagnosed on amniocentesis, maternal age 38
Delivery, 42, F, 3400 Diagnosed on prenatal U/S, normal kidneyfunction till age 2.5 y
Delivery, 36, F, 1888 Offspring treated with thyroxine, the motherwas euthyroid in pregnancy
ETOP, 20 Diagnosed on prenatal U/S at w 14 and 20
Delivery, 37, F, 2600 Surgical correction on 2nd d of life
netic anomalies; VSD – ventricular septal defect; TE – tracheoesophageal; TO – methotrexate; LMP – last menstrual period; SLE – systemic lupus erythematosus;trasound; DIC – disseminated intravascular coagulation; RDS – respiratory distressen plasma; TPN – total pareneteral nutrition; PM – post mortem.
uctive
m[
ngoe
op
ltsTi(ilaeNm1
ngptia
w(nwfgtfgasgmcislsmed
bulsupttttdI
[
[
O. Diav-Citrin et al. / Reprod
ost human pregnancy experience with anti-TNF-� medications5,15–28].
The rate of major anomalies in the present study did not sig-ificantly differ between the anti-TNF-�, the DM, and the NTEroups. There was no specific pattern of anomalies in the offspringf women in the anti-TNF-� group, supporting lack of teratogenicffect.
No case of VACTERL/VATER association was reported among theffspring of women treated with anti-TNF-� medications duringregnancy in the present study.
A non-significant trend toward a higher risk of major anoma-ies in both groups with autoimmune diseases was observed inhe present study. Inflammatory bowel disease has been incon-istently associated with increased risk of congenital anomalies.he risk of congenital anomalies among offspring of women withnflammatory bowel disease was found to be 2.37-fold increased95% CI 1.47–3.82, p < 0.001) in a meta-analysis [29]. However, noncreased risk of congenital anomalies was found in other relativelyarge studies [30,31]. The association between rheumatoid arthritisnd congenital abnormalities has been even less consistent. Reedt al. [32] did not observe an increased risk for birth defects, whileørgaard et al. [33] found an increased risk for congenital abnor-alities in 1994–1997 [OR 2.57, (95% CI 1.59–4.16)], but not in
998–2006.A sample size of 67 livebirths or elective terminations of preg-
ancy due to prenatally diagnosed anomalies in the anti-TNF-�roup with a ratio of 1:4.9 to the NTE comparison group with 80%ower, a baseline risk of 2.4% for major anomalies, enables detec-ion of a 4.95-fold increase in the rate of major anomalies. The studys not powered to find a smaller increase in the overall rate of majornomalies or in the rate of specific rare anomalies.
The higher rate of miscarriages found in the anti-TNF-� groupas associated with an earlier gestational age at initial contact
with a higher miscarriage rate in women calling earlier in preg-ancy), and to a lesser extent, with maternal smoking, but notith the exposure, as verified by the regression analysis. A 3.4-
old increase in the rate of preterm deliveries in the anti-TNF-�roup compared with the NTE group might be associated withhe underlying diseases [29,34]. A lower median birth weight wasound in the anti-TNF-� group compared with both the DM and NTEroups. The birth weight may be affected by the underlying diseasectivity [29,34,35], as well as by the use of concurrent immuno-uppressive medications known to be associated with intrauterinerowth restriction [36]. The median gestational week of anti-TNF-�edication discontinuation was 9 (4–28), before significant pla-
ental transfer of these molecules is expected. It should be keptn mind that women in the anti-TNF-� group probably had a moreevere disease to become eligible for this treatment, and were moreikely to be on concomitant immunosuppressive medications andteroids. Discontinuing their disease modifying anti-TNF-� treat-ent relatively early during pregnancy might have resulted in
xacerbation of the disease, and subsequent higher rate of pretermeliveries and lower birth weight.
The present study has certain limitations and advantages. It isased on TIS population, which may not represent the general pop-lation, but has two comparison groups from the same TIS. Other
imitations of the study are: reliance on maternal interview as aource for outcome data in most cases, a nonrandomized design,sing a group of three different anti-TNF-� medications, limitedower for specific rare defects, and lack of data on periconcep-ional disease activity. However, applying the same procedure tohe three arms of the study and the prospective nature minimize
he potential biases. Due to ethical considerations randomized con-rolled trials are often not feasible in pregnancy. The fact that allata are from a single center also minimizes some potential biases.
n addition, there were two comparison groups: a DM group with
[
[
Toxicology 43 (2014) 78– 84 83
similar diseases without anti-TNF-� treatment and a group coun-seled for NTE. Medical records were available for most cases withanomalies including discharge letters, echocardiography results, orinformation from the child’s pediatrician. Another advantage of thepresent study is that data were available on elective terminationsof pregnancies and were included in the analysis.
In conclusion, the present prospective observational compara-tive cohort study suggests that the use of anti-TNF-� medicationsduring pregnancy is not associated with an increased risk for majoranomalies. One should keep in mind that this conclusion is basedon relatively small numbers of exposed pregnancies, and should beinterpreted with caution. Larger studies are needed to establish thepregnancy safety of anti-TNF-� medications. Further studies withexposure late in pregnancy are needed to address their potentialeffect on the infant’s developing immune system.
Conflict of interest
The authors have no conflict of interest to disclose.
Acknowledgments
This work is part of the Pharm D thesis in Clinical Pharmacy ofthe Hebrew University of Mrs. Anna Otcheretianski-Volodarsky.
Appendix A. Supplementary data
Supplementary data associated with this article can be found,in the online version, at http://dx.doi.org/10.1016/j.reprotox.2013.11.004.
References
[1] Treacy G. Using an analogous monoclonal antibody to evaluate the reproductiveand chronic toxicity potential for the humanized anti-TNF alpha monoclonalantibody. Hum Exp Toxicol 2000;19:226–8.
[2] Vasiliauskas EA, Church JA, Silverman N, Barry M, Targan SR, DubinskyMC. Case report: evidence for transplacental trasfer of maternally admin-istered infliximab to the newborn. Clin Gastroenterol Hepatol 2006;4:1255–8.
[3] Zelinkova Z, de Haar C, de Ridder L, Pierik MJ, Kuipers EJ, Peppelenbosch MP,et al. High intra-uterine exposure to infliximab following maternal anti-TNFtreatment during pregnancy. Aliment Pharmacol Ther 2011;33:1053–8.
[4] Murashima A, Watanabe N, Ozawa N, Saito H, Yamaguchi K. Etanercept duringpregnancy and lactation in a patient with rheumatoid arthritis: drug levels inmaternal serum, cord blood, breastmilk and the infant’s serum [Letter]. AnnRheum Dis 2009;68:1793–4.
[5] Mahadevan U, Wolf DC, Dubinsky M, Cortot A, Lee SD, Siegel CA, et al.Placental transfer of anti-tumor necrosis factor agents in pregnant patientswith inflammatory bowel disease. Clin Gastroenterol Hepatol 2013;11:286–92.
[6] Lee H, Kimko HC, Rogge M, Wang D, Nestorov I, Peck CC. Population phar-macokinetic and pharmacodynamic modeling of etanercept using logisticregression analysis. Clin Pharmacol Ther 2003;73:348–65.
[8] Weisman MH, Moreland LW, Furst DE, Weinblatt ME, Keystone EC, Paulus HE,et al. Efficacy, pharmacokinetic, and safety assessment of adalimumab, a fullyhuman anti-tumor necrosis factor-alpha monoclonal antibody, in adults withrheumatoid arthritis receiving concomitant methotrexate: a pilot study. ClinTher 2003;25:1700–21.
[9] Djokanovic N, Klieger-Grossman C, Pupco A, Koren G. Safety of infliximab useduring pregnancy. Reprod Toxicol 2011;32:93–7.
10] Chambers CD, Johnson DL. Emerging data on the use of anti-tumor necrosisfactor-alpha medications in pregnancy. Birth Defects Res A Clin Mol Teratol2012;94:607–11.
11] Carter JD, Valeriano J, Vasey FB. Tumor necrosis factor-alpha inhibition andVATER association: a causal relationship. J Rheumatol 2006;33:1014–7.
12] Carter JD, Ladhani A, Ricca LR, Valeriano J, Vasey FB. A safety assessment oftumor necrosis factor antagonists during pregnancy: a review of the Food andDrug Administration database. J Rheumatol 2009;36:635–41.
13] Koren G, Inoue M. Do tumor necrosis factor inhibitors cause malformations inhumans? [editorial]. J Rhematol 2009;36:465–6.
14] Winger EE, Reed JL. Was risk properly assessed in Carter, et al’s safetyassessment of tumor necrosis factor antagonists during pregnancy? [Letter].J Rheumatol 2009;36:2122.
15] Katz JA, Antoni C, Keenan GF, Smith DE, Jacobs SJ, Lichtenstein GR. Outcome ofpregnancy in women receiving infliximab for the treatment of Crohn’s diseaseand rheumatoid arthritis. Am J Gastroenterol 2004;99:2385–92.
16] Chambers CD, Johnson DL, Jones KL. Pregnancy outcome in women exposed toanti-TNF-alpha medications: the OTIS rheumatoid arthritis in pregnancy study[abstract]. Arthritis Rheumat 2004;50:S479–80.
17] Mahadevan U, Kane S, Sandborn WJ, Cohen RD, Hanson K, Terdiman JP, et al.International infliximab use during pregnancy for the induction or main-tenance of remission in Crohn’s disease. Aliment Pharmacol Ther 2005;21:733–8.
18] Lichtenstein GR, Feagan BG, Cohen RD, Salzberg BA, Diamond RH, Chen DM,et al. Serious infections and mortality in association with therapies for Crohn’sdisease: TREAT registry. Clin Gastroenterol Hepatol 2006;4:621–30.
19] Lichtenstein GR, Feagan BG, Cohen RD, Salzberg BA, Diamond RH, Price S,et al. Serious infection and mortality in patients with Crohn’s disease: morethan 5 years of follow-up in the TREATTM registry. Am J Gastroeneterol2012;107:1409–22.
20] Roux CH, Brocq O, Breuil V, Albert C, Euller-Ziegler L. Pregnancy in rheuma-tology patients exposed to anti-tumour necrosis factor (TNF)-alpha therapy.Rheumatoloy (Oxford) 2007;46:695–8.
21] Berthelot JM, De Bandt M, Goupille P, Solau-Gervais E, Lioté F, Goeb V, et al.Exposition to anti-TNF drugs during pregnancy: outcome of 15 cases and reviewof the literature. Joint Bone Spine 2009;76:28–34.
22] Rump JA, Schönborn H. Conception and course of eight pregnancies infive women on TNF blocker etanercept treatment [German]. Z Rheumatol2010;69:903–9.
23] Verstappen SM, King Y, Watson JD, Symmons DP, Hyrich KL, BSRBR ControlCentre Consortium, BSR Biologics Register. Anti-TNF therapies and pregnancy:
outcome of 130 pregnancies in the British Society for Rheumatology BiologicsRegister. Ann Rheum Dis 2011;70:823–6.
24] Schnitzler F, Fidder H, Ferrante M, Ballet V, Noman M, Van Assche G, et al.Outcome of pregnancy in women with inflammatory bowel disease treatedwith antitumor necrosis factor therapy. Inflamm Bowel Dis 2011;17:1846–54.
[
[
Toxicology 43 (2014) 78– 84
25] Weber-Schoendorfer C, Fritzsche J, Schaefer C. Pregnancy outcome in womenexposed to adalimumab or infliximab: the experience of the Berlin Institutefor Clinical Teratology and Drug Risk Assessment [abstract]. Reprod Toxicol2011;31:267–8.
26] Hultzsch S, Weber-Scoendorfer C, Schaefer C. Pregnancy outcomes after expo-sure to etanercept [abstract]. Reprod Toxicol 2011;31:260.
27] Chambers CD, Johnson DL, Jones KL, Luo Y, Xu R, Jimenez JL, et al. Pregnancyoutcomes in women exposed to adalimumab for the treatment of rheumatoidarthritis: an update on the OTIS Autoimmune Diseases in Pregnancy Project[abstract]. Birth Defects Res A Clin Mol Teratol 2012;94:325.
28] Viktil KK, England A, Furi K. Outcomes after anti-rheumatic drug use beforeand during pregnancy: a cohort study among 150,000 pregnant women andexpectant fathers. Scand J Rheumatol 2012;41:196–201.
29] Cornish J, Tan E, Teare J, Teoh TG, Rai R, Clark SK, et al. A meta-analysis on theinfluence of inflammatory bowel disease on pregnancy. Gut 2007;56:830–7.
30] Mahadevan U, Dandborn WJ, Li DK, Hakimian S, Kane S, Corley DA. Pregnancyoutcomes in women with inflammatory bowel disease: a large community-based study from Northern California. Gastroenterology 2007;133:1106–12.
31] Bortoli A, Pedersen N, Duricova D, D’Inca R, Gionchetti P, Panelli MR,et al. Pregnancy outcome in inflammatory bowel disease: prospective Euro-pean case-control ECCO-EpiCom study, 2003–2006. Aliment Pharmacol Ther2011;34:724–34.
32] Reed SD, Vollan TA, Svec MA. Pregnancy outcomes in women with rheumatoidarthritis in Washington State. Matern Child Health J 2006;10:361–6.
33] Nørgaard M, Larsson H, Pedersen L, Granath F, Askling J, Kieler H, et al. Rheuma-toid arthritis and birth outcomes: a Danish and Swedish nationwide prevalencestudy. J Intern Med 2012;268:329–37.
34] de Man YA, Hazes JM, van der Heide H, Willemsen SP, de Groot CJ, Steegers EA,et al. Association of higher rheumatoid arthritis disease activity during preg-nancy with lower birth weight: results of a national prospective study. ArthritisRheum 2009;60:3196–206.
35] Bowden AP, Barrett JH, Fallow W, Silman AJ. Women with inflammatory pol-yarthritis have babies of lower birth weight. J Rheumatol 2001;28:355–9.
36] Pirson Y, Van Lierde M, Ghysen J, Squifflet JP, Alexandre GP, van Ypersele deStrihou C. Retardation of fetal growth in patients receiving immunosuppressivetherapy [Letter]. N Engl J Med 1985;313:328.