Introduction The ability to opacify the central circulation with ultra- sonic reflectors after the injection of a variety of fluids was described in 1968 [1]. Over the next few years sever- al solutions were proposed to extend the contrast en- hancement. However, the first generation of ultrasound contrast agents (USCA) used free bubbles too large and unstable to pass the pulmonary circulation after pe- ripheral intravenous injection, and their echo-enhanc- ing effect lasted too short for a useful ultrasound exami- nation [2, 3]. Nycomed Amersham has pioneered the development of USCA, contributing to the develop- ment of the first commercially available ultrasound con- trast agent that can pass the pulmonary circulation, Alb- unex. However, also this agent and other agents of the same generation have not been widely used in echocar- diography because the air filled microbubbles often do not persist in the circulation long enough for adequate imaging. In addition, although tissue enhancement in the myocardium after intravenous injection of Albunex has been reported [4], practical use of these agents may require central venous injections [5]. NC100100 is a new ultrasound contrast agent developed by Nycomed Amersham, able to provide tissue enhancement in the different organs of the body following a peripheral in- travenous injection. NC100100 consists of perfluorocar- bon microbubbles that are stabilised with a surfactant and are within a well-defined size range (median diame- ter of approximately 3 mm), well below the size of red blood cells. NC100100 is prepared as a easy-to-use, non-toxic formulation. Due to the low diffusibility and blood solubility of the gas, to the controlled size distri- bution of the microbubbles, and to the flexibility of the shell, NC100100 is a free-flowing tracer capable of crossing the pulmonary capillary bed following periph- eral intravenous injection, is stable enough for the dura- tion of the US examination, and provides echo enhance- ment useful for clinical requirements. Clinical applica- tions of NC100100 have been studied both in cardiology and in radiology. Left ventricular opacification One common clinical indication for echocardiography is to assess global and regional left ventricular (LV) func- tion, a task that depends on the ability to distinguish the endocardial border from the LV blood pool. Unfortu- nately, despite the best efforts of experienced echocardi- ographers and the availability of high-quality equipment, poor acoustic windows or endocardial dropout, particu- larly in the apical views [6, 7], often limits the endocardial border definition. Both at rest and during stress, poor im- age quality impairs the detection of wall motion abnor- malities as well as the possibility of obtaining accurate measurements of myocardial wall thickness. Several au- thors have documented the efficacy of USCA in reducing the frequency of inadequate echocardiographic studies in clinical trials [8, 9, 10]. NC100100 has shown its effica- cy in this indication, improving the endocardial border delineation and the confidence in the adequacy of the wall motion assessment from the post injection echocar- diography compared with the pre-injection (Fig. 1) [11]. Myocardial perfusion Historically, it has not been possible to directly assess myocardial perfusion with standard non-contrast echo- cardiography. Segmental left ventricular (LV) wall mo- tion abnormalities are characteristic of myocardial in- farction. However, regional wall motion abnormalities are seen in transient ischaemia and chronic ischaemia (“hibernating myocardium”) as well as when scar tissue is present. Acute ischaemia (“stunned myocardium”) cannot be distinguished from acute myocardial necrosis by wall motion assessment alone [12]. Therefore, perfu- sion information in addition to morphology and func- tion is required of an imaging method for the correct di- agnosis and workup of patients with known or suspected acute ischaemic syndrome, and myocardial contrast echocardiography (MCE) has the potential for provid- ing such information [13]. Eur. Radiol. 9 (Suppl. 3), S 343–S 346 (1999) Ó Springer-Verlag 1999 European Radiology Preliminary experience with NC100100, a new ultrasound contrast agent for intravenous injection C. Marelli Nycomed Amersham, Nycomed Imaging AS, Clinical R& D, P.O. Box 4220 Torshov, N-0401 Oslo, Norway
Transcript
Introduction
The ability to opacify the central circulation with ultra-sonic reflectors after the injection of a variety of fluidswas described in 1968 [1]. Over the next few years sever-al solutions were proposed to extend the contrast en-hancement. However, the first generation of ultrasoundcontrast agents (USCA) used free bubbles too largeand unstable to pass the pulmonary circulation after pe-ripheral intravenous injection, and their echo-enhanc-ing effect lasted too short for a useful ultrasound exami-nation [2, 3]. Nycomed Amersham has pioneered thedevelopment of USCA, contributing to the develop-ment of the first commercially available ultrasound con-trast agent that can pass the pulmonary circulation, Alb-unex. However, also this agent and other agents of thesame generation have not been widely used in echocar-diography because the air filled microbubbles often donot persist in the circulation long enough for adequateimaging. In addition, although tissue enhancement inthe myocardium after intravenous injection of Albunexhas been reported [4], practical use of these agents mayrequire central venous injections [5]. NC100100 is anew ultrasound contrast agent developed by NycomedAmersham, able to provide tissue enhancement in thedifferent organs of the body following a peripheral in-travenous injection. NC100100 consists of perfluorocar-bon microbubbles that are stabilised with a surfactantand are within a well-defined size range (median diame-ter of approximately 3 mm), well below the size of redblood cells. NC100100 is prepared as a easy-to-use,non-toxic formulation. Due to the low diffusibility andblood solubility of the gas, to the controlled size distri-bution of the microbubbles, and to the flexibility of theshell, NC100100 is a free-flowing tracer capable ofcrossing the pulmonary capillary bed following periph-eral intravenous injection, is stable enough for the dura-tion of the US examination, and provides echo enhance-ment useful for clinical requirements. Clinical applica-tions of NC100100 have been studied both in cardiologyand in radiology.
Left ventricular opacification
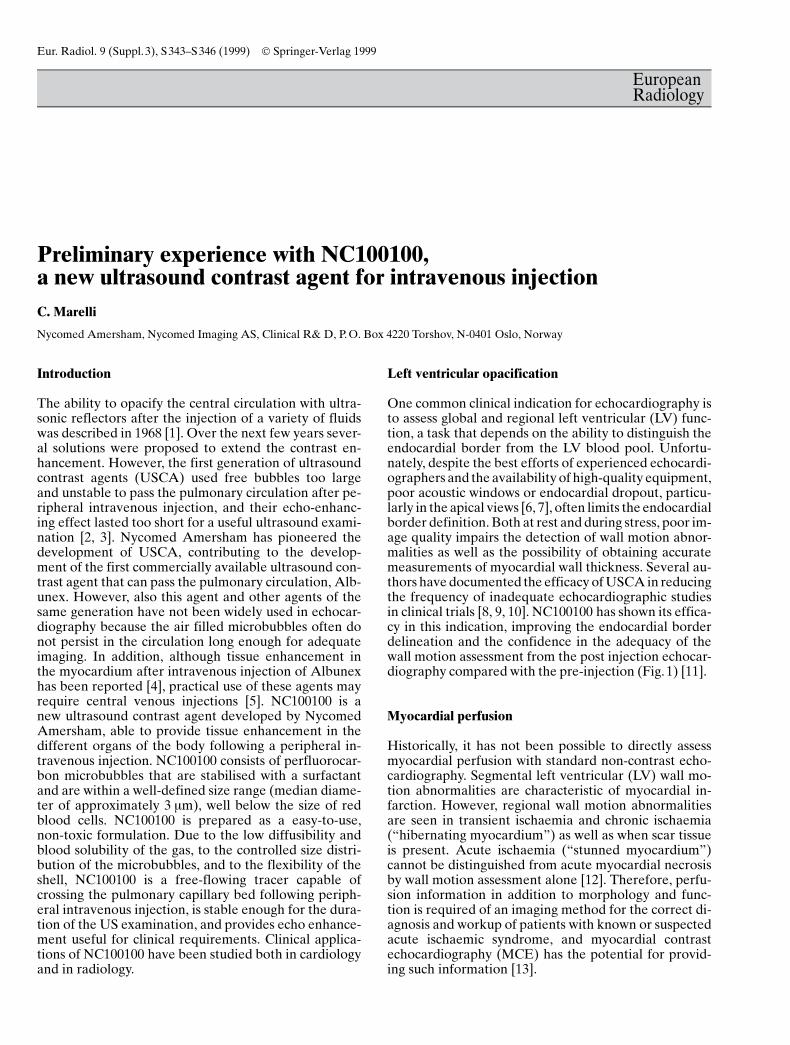
One common clinical indication for echocardiography isto assess global and regional left ventricular (LV) func-tion, a task that depends on the ability to distinguish theendocardial border from the LV blood pool. Unfortu-nately, despite the best efforts of experienced echocardi-ographers and the availability of high-quality equipment,poor acoustic windows or endocardial dropout, particu-larly in the apical views [6, 7], often limits the endocardialborder definition. Both at rest and during stress, poor im-age quality impairs the detection of wall motion abnor-malities as well as the possibility of obtaining accuratemeasurements of myocardial wall thickness. Several au-thors have documented the efficacy of USCA in reducingthe frequency of inadequate echocardiographic studiesin clinical trials [8, 9, 10]. NC100100 has shown its effica-cy in this indication, improving the endocardial borderdelineation and the confidence in the adequacy of thewall motion assessment from the post injection echocar-diography compared with the pre-injection (Fig.1) [11].
Myocardial perfusion
Historically, it has not been possible to directly assessmyocardial perfusion with standard non-contrast echo-cardiography. Segmental left ventricular (LV) wall mo-tion abnormalities are characteristic of myocardial in-farction. However, regional wall motion abnormalitiesare seen in transient ischaemia and chronic ischaemia(ªhibernating myocardiumº) as well as when scar tissueis present. Acute ischaemia (ªstunned myocardiumº)cannot be distinguished from acute myocardial necrosisby wall motion assessment alone [12]. Therefore, perfu-sion information in addition to morphology and func-tion is required of an imaging method for the correct di-agnosis and workup of patients with known or suspectedacute ischaemic syndrome, and myocardial contrastechocardiography (MCE) has the potential for provid-ing such information [13].
Eur. Radiol. 9 (Suppl.3), S343±S 346 (1999) Ó Springer-Verlag 1999
EuropeanRadiology
Preliminary experience with NC100100,a new ultrasound contrast agent for intravenous injectionC. Marelli
Nycomed Amersham, Nycomed Imaging AS, Clinical R& D, P. O. Box 4220 Torshov, N-0401 Oslo, Norway
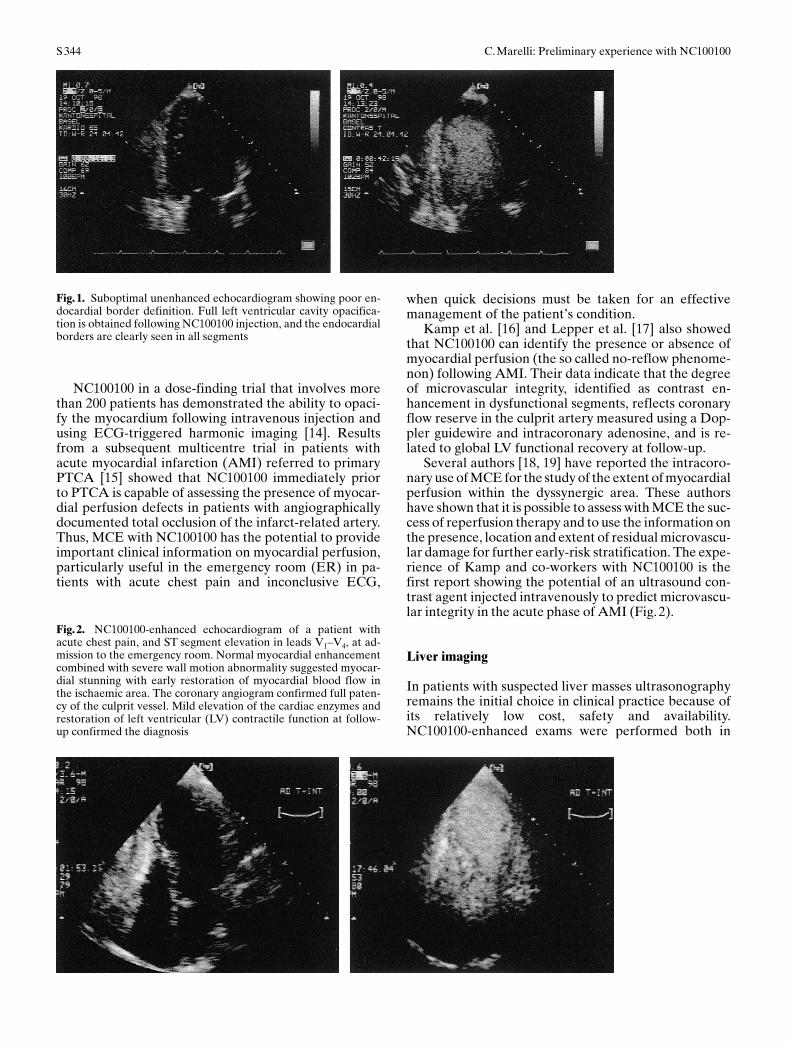
NC100100 in a dose-finding trial that involves morethan 200 patients has demonstrated the ability to opaci-fy the myocardium following intravenous injection andusing ECG-triggered harmonic imaging [14]. Resultsfrom a subsequent multicentre trial in patients withacute myocardial infarction (AMI) referred to primaryPTCA [15] showed that NC100100 immediately priorto PTCA is capable of assessing the presence of myocar-dial perfusion defects in patients with angiographicallydocumented total occlusion of the infarct-related artery.Thus, MCE with NC100100 has the potential to provideimportant clinical information on myocardial perfusion,particularly useful in the emergency room (ER) in pa-tients with acute chest pain and inconclusive ECG,
when quick decisions must be taken for an effectivemanagement of the patient's condition.
Kamp et al. [16] and Lepper et al. [17] also showedthat NC100100 can identify the presence or absence ofmyocardial perfusion (the so called no-reflow phenome-non) following AMI. Their data indicate that the degreeof microvascular integrity, identified as contrast en-hancement in dysfunctional segments, reflects coronaryflow reserve in the culprit artery measured using a Dop-pler guidewire and intracoronary adenosine, and is re-lated to global LV functional recovery at follow-up.
Several authors [18, 19] have reported the intracoro-nary use of MCE for the study of the extent of myocardialperfusion within the dyssynergic area. These authorshave shown that it is possible to assess with MCE the suc-cess of reperfusion therapy and to use the information onthe presence, location and extent of residual microvascu-lar damage for further early-risk stratification. The expe-rience of Kamp and co-workers with NC100100 is thefirst report showing the potential of an ultrasound con-trast agent injected intravenously to predict microvascu-lar integrity in the acute phase of AMI (Fig.2).
Liver imaging
In patients with suspected liver masses ultrasonographyremains the initial choice in clinical practice because ofits relatively low cost, safety and availability.NC100100-enhanced exams were performed both in
C.Marelli: Preliminary experience with NC100100S 344
Fig.1. Suboptimal unenhanced echocardiogram showing poor en-docardial border definition. Full left ventricular cavity opacifica-tion is obtained following NC100100 injection, and the endocardialborders are clearly seen in all segments
Fig.2. NC100100-enhanced echocardiogram of a patient withacute chest pain, and ST segment elevation in leads V1±V4, at ad-mission to the emergency room. Normal myocardial enhancementcombined with severe wall motion abnormality suggested myocar-dial stunning with early restoration of myocardial blood flow inthe ischaemic area. The coronary angiogram confirmed full paten-cy of the culprit vessel. Mild elevation of the cardiac enzymes andrestoration of left ventricular (LV) contractile function at follow-up confirmed the diagnosis
the vascular (blood pool) and delayed (reticuloendothe-lial) phase in a multicentre study involving more than130 patients with known or strongly suspected focal sol-id liver lesions using fundamental, harmonic and powerDoppler imaging. Blood-pool-phase scanning showedsignificant enhancement of normal hepatic vessels andtumour vascularity. Hepatic metastases typicallyshowed a very rapid enhancement of signal intensitywith power Doppler imaging. In the delayed phase he-patic enhancement, due to the uptake of the microbub-bles in the reticuloendothelial cells, was observed for aslong as 45 min. Malignant tumours did not take up con-trast on delayed scans. A characteristic echogenic rim
enhancement was observed around malignant tumours,and harmonic mode was superior to fundamental modein depicting this characteristic finding (Fig. 3). The con-spicuity of some tumours was improved on the delayedscans, and tumours as small as 3 mm in diameter wereseen on post- but not on pre-contrast scans [20, 29].
Other radiological indications
NC100100 offers the potential of investigating the pres-ence and extent of tumour masses and vascularity of avariety of parenchymal organs in the body. One of thelimitations of unenhanced Doppler, even with favour-able vessel angle, is the problem of depiction of smallvessels with slow or low flow [21]. Given the up to 25-dB enhancement of the Doppler signals produced byUSCA, the expectation is that such agents would pro-vide a better depiction of small vessels and thereby im-prove the ability to differentiate areas with normal andabnormal vascularity [22, 23]. For example, preliminaryexperience with power Doppler imaging of the dog pros-tate, before and after injection of NC100100, demon-strated a significant improvement in the visibility of theintraprostatic vascular pattern on post-contrast imagescompared with unenhanced scans, facilitating the detec-tion of tumour masses. Doppler enhancement within theprostate persisted for several minutes and the imageswere found to correspond well with pathology (Fig.4)[24]. The potential usefulness of NC100100 in patientswith suspected prostate tumours will be explored.
C.Marelli: Preliminary experience with NC100100 S345
Fig.3. Characteristic pattern of malignant tumours of the liver.Note the echogenic rim enhancement around the lesions, whichshow no uptake
Fig.4. Dog prostate tumour (T). A Baseline imagingof the prostate before injection of NC100100.B NC100100-enhanced image shows a tumour insidethe prostate. C The pathological specimen demon-strates the extent of the tumour within the prostateparenchyma
Safety of tissue perfusion agents
Regardless of their chemical composition, there is a pos-sibility that some microbubbles may become temporari-ly entrapped in the microcirculation, due to their size[25]. Microembolization should be suspected if tissueenhancement is static (as seen on B-mode imaging) andfollows tissue motion, or if tissue enhancement lastslonger than opacification of the blood pool [26]. The ad-vantage of the preformed, stable and flexible gas micro-spheres in NC100100 is the control of particle size in theinjected product, which reduces the likelihood of micro-embolization. NC100100 has been tested in clinical tri-als in more than 1000 patients in cardiological and ra-diological indications, showing an excellent safety pro-file [27, 28, 29].
Conclusion
Preliminary clinical experience with NC100100 hasshown promising results for both contrast-enhancedgrey-scale and Doppler imaging in cardiological and ra-diological indications. Thanks to its characteristicsNC100100 has the potential for future use in daily clini-cal practice.
Acknowledgements The images shown in this article were kindlyprovided by P. Hunziker Kantonspital Basel, Switzerland; A.Nagy and D. Rovai, CNR Institute of Clinical Physiology, Pisa, Ita-ly; E. Leen, Royal Infirmary, Glasgow; and F. Forsberg, ThomasJefferson University Hospital, Philadelphia, USA. The advice ofE.K. Hagen, Y. Kloster, P. B. Gordon and J. éstensen is acknowl-edged with thanks.
References
1. Gramiak R, Shah PM (1968) Echocardiography of the aorticroot. Invest Radiol 3: 356±366
2. Ophir J, Parker KJ (1989) Contrast agents in diagnostic ultra-sound. Ultrasound Med Biol 15: 319±333
3. Voci P, Morris H, Marelli C (1996) The history of contrast ultra-sonography and the development of echocontrast agents. In:Voci P, Caretta Q (eds) Myocardial contrast echocardiographyin cardiology and cardiac surgery. CEPI, Rome, pp 13±31
4. Silverman PE, TenCate FJ, DeJong N et al (1989) IntravenousAlbunex injections increase intramyocardial backscatter. Cir-culation 80 (Suppl. II): 369 (abstr.)
5. Villanueva FS, Glasheen WP, Sklenar J et al (1992) Successfuland reproducible myocardial opacification during two-dimen-sional echocardiography from right heart injection of contrast.Circulation 85: 1557±1564
6. Visser CA, Kan G, David GK et al (1982) Echocardiographic-cineangiographic correlation in detecting left ventricular aneu-rysm: a prospective study of 422 patients. Am J Cardiol 50:337±341
7. Freeman AP, Giles RW, Walsh WF et al. (1985) Regional leftventricular wall motion assessment: comparison of two-dimen-tional echocardiography and radionuclide angiography inhealed myocardial infarction. Am J Cardiol 56: 8±12
8. Grayburn PA, Weiss JL, Hack TC et al. (1998) Phase III multi-center trial comparing the efficacy of 2% dodecafluoropentaneemulsion (Echogen) and sonicated 5% human albumin (Alb-unex) as ultrasound contrast agents in patients with suboptimalechocardiograms. J Am Coll Cardiol 32: 230±236
9. Cohen JL, Cheirif J, Segar D et al. (1998) Improved left ven-tricular endocardial border delineation and opacification withOptison (FSO69), a new echocardiographic contrast agent. JAm Coll Cardiol 32: 746±752
10. Ikonomidis I, Holmes E, Narbuvold H et al. (1998) Assessmentof left ventricular wall motion and delineation of the endocar-dial border after intravenous injection of Infoson during do-butamine stress echocardiography. Coron Artery Dis 9: 567±576
11. Nycomed Amersham, data on file12. ACC/AHA (1997) Guidelines for the clinical application of
echocardiography: executive summary. J Am Coll Cardiol 29:862±879
13. Kaul S (1997) Myocardial contrast echocardiography: 15 yearsof research and development. Circulation 96: 3745±3760
14. Marwick TH, Brunken R, Meland N et al. (1998) Accuracy andfeasibility of contrast echocardiography for detection of perfu-sion defects in routine practice: comparison with wall motionand technetium-99 m sestamibi single-photon emission tomog-raphy. J Am Coll Cardiol 32: 1260±1269
15. Kamp O, Lepper W, Vanoverschelde JL et al. (1998) Efficacyof intravenous NC100100 in first acute myocardial infarctionfor detection of myocardial contrast defects (abstract). Eur JCardiol Abstr 780
16. Kamp O, Lepper W, Vanoverschelde JL et al. (in press) Intra-venous myocardial contrast echocardiography for serial assess-ment of perfusion defects in patients with first acute myocardialinfarction referred for primary PTCA
17. Lepper W, Franke A, Hoffmann R et al. (1998) Myocardialperfusion dynamics in patients with acute myocardial infarctionundergoing primary PTCA as assessed by myocardial contrastechocardiography and coronary flow reserve measurement(abstract). Circulation 98 (Suppl. I):I-502
18. Ito H, Tomooka T, Sakai N et al. (1992) Lack of myocardialperfusion immediately after successful thrombolysis: a predic-tor of poor recovery of left ventricular function in anterior my-ocardial infarction. Circulation 85: 1699±1705
19. Agati L, Voci P, Bilotta F et al. (1994) Influence of residual per-fusion within the infarct zone on the natural history of left ven-tricular dysfunction after acute myocardial infarction: a myo-cardial contrast echocardiographic study. J Am Coll Cardiol24: 336±342
20. Needleman L, Leen E, Kyriakkopoulou K et al. (1998)NC100100: a new US contrast agent for fundamental and har-monic imaging of hepatic lesions (abstract). Radiology 209: 189
21. Cosgrove D (1996) Ultrasound contrast enhancement of tu-mours Clin Radiol 51 (Suppl. 1):44±49
22. Goldberg BB, Liu JB, Forsberg F (1994) Ultrasound contrastagents: a review. Ultrasound Med Biol 20: 319±333
24. Forsberg F, Ismail MT, Merton DA et al. (1998) Ultrasoundcontrast imaging of normal and abnormal canine prostates. JUltrasound Med 16:S1±S148
25. Nanda NC (1992) Echocontrast enhancers: How safe are they?Adv Echo Contrast 2: 19±24
26. Beppu S, Matsuda H, Shishido T et al. (1997) Prolonged myo-cardial contrast echocardiography via peripheral venous ad-ministration of QW3600 injection (Echogen): its efficacy andside effects. J Am Soc Echocardiol 10: 11±24
27. Myreng Y, Mùlstad P, Ytre-Aas K et al. (in press) Safety of thetranspulmonary ultrasound contrast agent NC100100: a clinicaland haemodynamic evaluation in patients with suspected orproven coronary artery disease. Heart
28. Binder T, Assayag P, Baer F et al. (1999) NC100100, a newechocontrast agent for the assessment of myocardial perfusion.Safety and comparison with MIBI-SPECT in a randomizedmulticenter study. Clin Cardiol 22: 273±282
29. Goldberg BB, Leen E, Needleman L et al. (1998) NC100100enhanced US imaging of the liver: a phase II double-blind, pla-cebo-controlled, dose-finding trial in adults with focal liver dis-ease. Radiology 209: 23 (abstr.)
C.Marelli: Preliminary experience with NC100100S 346