20
PREOPERATIVE TRANSARTERIAL EMBOLISATION (TAE) OF SPINAL TUMOURS ID NO : IRIA -1204
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | claude-cole |
| View: | 217 times |
| Download: | 0 times |

PREOPERATIVE TRANSARTERIAL EMBOLISATION (TAE) OF SPINAL TUMOURS
ID NO : IRIA -1204

ABSTRACT
AIM: Preoperative embolisation of hypervascular spinal tumors which has been helpful for tumour resection , to minimise blood
loss during surgery and to control tumor growth.
MATERIALS : Using polyvinyl alcohol particles and gel foam
METHODS: During the period of 2013-2014 , four patients with spinal tumours underwent transarterial embolisation of spinal tumours of
which one was giant cell tumour of sacrum ,another two cases were vertebral haemangioma , another one was giant cell tumour of lumbar vertebra
Patients underwent transarterial embolisation followed by surgery except giant cell tumour of sacrum who was treated with transarterial embolisation to reduce the tumour size
RESULTS : There were no symptomatic complications associated with embolisation and average estimated surgical blood loss was less.
CONCLUSION: Preoperative embolisation of hypervascular spinal tumors is a safe and effective method to devascularise the spinal tumours
and can make complete resection possible and make unresectable tumour resectable. Superselection or flow control is necessary to achieve effective devascularisation and to avoid complications

SPINAL TUMOURS
• Bone tumors include a variety of lesions, both primary and metastatic.
• The treatment modalities for bone tumors vary, but in general surgical excision is the treatment of choice with other adjunctive therapies.
• Surgery for many bone tumors is complex due to several factors including tumor bulk, vascularity, vicinity to vital structures and potentially inaccessible location of the lesion.
• Transarterial Embolisation (TAE) is one of the important adjuvant treatment modalities and in some cases it may be the primary and curative treatment

TAE
• Preoperative TAE has proved to be effective in both primary and metastatic bone tumors.
• It reduces tumor vascularity and intraoperative blood loss, allows better definition of tissue planes at surgery affording more complete excision, and hence reduced recurrence.
• There are several techniques and embolic agents available, but the ultimate aim is to achieve tumor devascularization.
CATHETER ANGIOGRAPHY
• Catheter angiography is performed prior to Embolisation to identify the tumor feeding vessels and to determine the safety of Embolisation.
• Particular attention should be paid when performing Embolisation in the spine to avoid the spinal arteries.
• After identification of tumor feeding arteries and the vessels to be avoided, the artery is catheterized. The choice of catheter depends on the size of the feeding vessel.
• TAE is mostly performed using a coaxial catheter system

EMBOLISING AGENT
1) POLY VINYL ALCIHOL - sizes ranging from 50 to 1000 μm; the commonest size used is in the 300-500 μm range.
• PVA has several desirable characteristics which makes it a commonly used agent.
• It is capable of penetrating and occluding the tumor blood supply, and it is relatively inexpensive and easy to handle. However, PVA particles can aggregate and form clumps causing catheter occlusion and some unpredictability in the level of Embolisation.
2)GELFOAM OR GELATIN SPONGE is a dissolvable sponge-like material; is considered a temporary Embolisation agent; the occluded artery usually recanalizes within a month.
GEL FOAM
Polyvinyl alcohol

CASE 1
•Middle aged male with Severe low back pain •L4 vertebral body Haemangioma with collapsed vertebral body was diagnosed. •Pre operative stabilisation was done •Referred for trans arterial embolisation
Post stabilised vertebral body Embolisation using gel foam
Showing tumour blush

CASE 2
• Middle aged male with Severe back pain.
• On CT – polka dot appearance in L1 vertebra and striations in vertebral body with erosion of posterior vertebral body of L1.
• MRI - T2 slight hyperintense and T1 hyperintense lesion L1 vertebra with extradural component causing spinal cord compression at that level.

L 1 VERTEBRAL BODY HAEMANGIOMA
MRI CT
T2 SAGGITAL T1 SAGGITAL AXIAL

TAE
Right D12 & L1 was embolised using PVA
Left L1 was not embolised since artery of adamkiewicz arising from same feeder

Left L1 was not embolised since artery of adamkiewicz arising from same feeder
POST EMBOLISATINHAIRPIN BEND OF ADAM KIEWICZ ARTERY FROM LUMBAR ARTERY

HAEMANGIOMA OF LUMBAR SPINE
• Vertebroplasty for vertebral hemangiomas is generally indicated for lesions without neurological deficit.
• When patients present with spinal pain or cord compression with neurological deficit, radiation or decompression surgery is the treatment of choice but Massive hemorrhage is often encountered during surgery from these highly vascular lesions
• TAE is a useful adjunctive method to reduce perioperative blood loss
RADICULAR ARTERY ANATOMY

CASE - 3
• 30 years old antenatal mother presented with low back ache and referred as uterine fibroid for usg & MRI
• USG revealed a heteroechoic mass posterior to uterus in the pelvis
• Antenatal MRI & post natal CT showed eccentric expansile lytic lesion arising from the sacrum displacing gravid uterus and bladder anteriorly extending upto lateral pelvic wall on both sides & diagnosed as sacral giant cell tumour
• Post natal image guided biopsy proved as giant cell tumour
• Referred for feeding artery embolisation after delivery

ANTENATAL MRI
large hypointense expansile lesion arising from S3 , displacing pelvic organs anteriorly with no invasion of adjacent stuctures.
T2 AXIAL T2 SAGTTAL

POSTNATAL CONTRAST CT
Highly vascular expansile large mass with necrotic areas from sacrum
AXIAL CORONAL REFORMATTED 3D
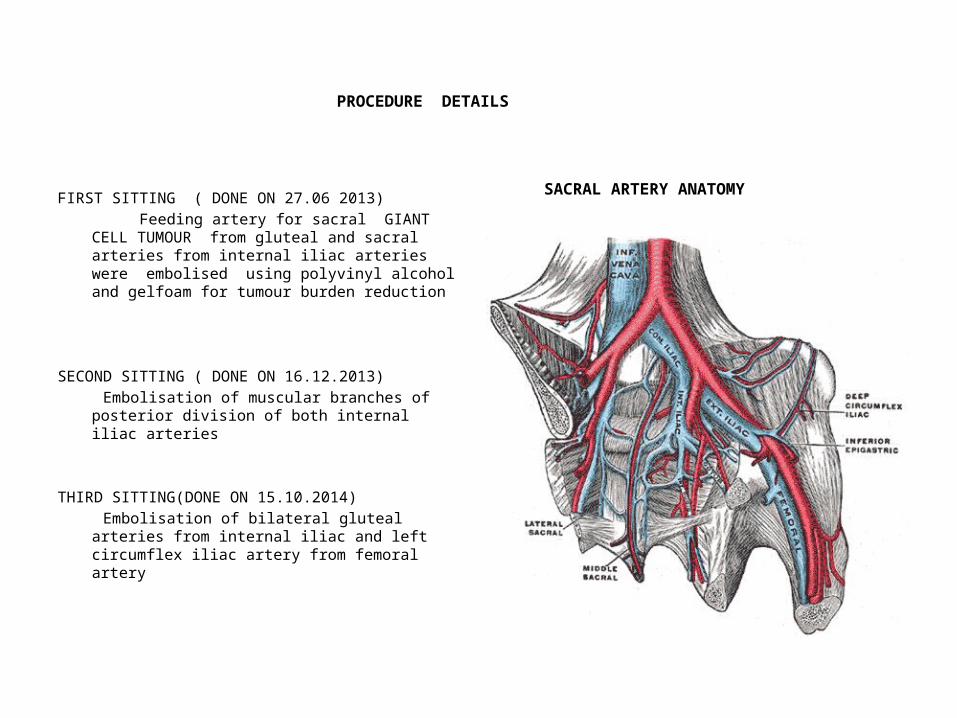
PROCEDURE DETAILS
SACRAL ARTERY ANATOMYFIRST SITTING ( DONE ON 27.06 2013)
Feeding artery for sacral GIANT CELL TUMOUR from gluteal and sacral arteries from internal iliac arteries were embolised using polyvinyl alcohol and gelfoam for tumour burden reduction
SECOND SITTING ( DONE ON 16.12.2013)
Embolisation of muscular branches of posterior division of both internal iliac arteries
THIRD SITTING(DONE ON 15.10.2014)
Embolisation of bilateral gluteal arteries from internal iliac and left circumflex iliac artery from femoral artery

FIRST SITTING
Left Superior gluteal artery showing tumour blush Embolisation done with alcohol and gelfoam

THIRD SITTING
CIRCUMFLEX ILIAC ARTERY EMBOLISATION
Injection from femoral artery showing
circumflex iliac artery Selective catheterisation of
circumflex iliac artery

THIRD SITTING
Post embolisation of cirmcumflex iliac artery Feeder from left internal iliac artery

GIANT CELL TUMOUR OF SACRUM
GIANT CELL TUMOUR OF SACRUM
• Giant cell tumors are benign locally aggressive and highly vascularized bone tumors.
• The most common sites of origin are distal femur, proximal tibia and distal radius.
• Surgery is the treatment modality of choice for these long bone GCT
• The spine is rarely involved and the most common location in the spine is the sacrum.
• Sacral GCTs are difficult lesions to treat surgically. Radiotherapy is contraindicated because of its potential to induce malignant transformation
GIANT CELL TUMOUR OF SACRUM EMBOLISATION
• Embolisation is an alternative treatment method for non-resectable tumor & devascularization
• Embolisations can be performed at 2 to 4 months intervals with the end point being the lack of a hypervascular mass
• GCTs may also occur in the areas of the spine other than the sacrum and studies have demonstrated the efficacy of TAE in these circumstances

CONCLUSION
Preoperative transarterial embolisation of hypervascular spinal tumours is safe
It appears to limit blood loss during surgery and to allow complete tumour resection including those tumours initially believed to be unresectable
Appropriate technique such as superselective catheterisation and blood flow control,including protection of the normal branches ,preferential flow and flow reversal are necessary to achieve efficient devascularisation and to avoid complications
THANK YOU

















