34
® ADLS is a registered trademark of the American Medical Association V 3.0 β 2007 ® 1 “Preparing Our Communities” Welcome!
® ADLS is a registered trademark of the American Medical AssociationV 3.0 β 2007
®
1
“Preparing Our Communities”
Welcome!

V 3.0 β 2007 2
Faculty Disclosure
• For Continuing Medical Education (CME) purposes as required by the American Medical Association (AMA) and other continuing education credit authorizing organizations:– In order to assure the highest quality of CME programming,
the AMA requires that faculty disclose any information relating to a conflict of interest or potential conflict of interest prior to the start of an educational activity.
– The teaching faculty for the BDLS course offered today have no relationships / affiliations relating to a possible conflict of interest to disclose. Nor will there be any discussion of off label usage during this course.

® ADLS is a registered trademark of the American Medical AssociationV 3.0 β 2007
®
3
Rapid Evaluation of a DISASTERThe R.E.D. Survey
A review of the NDLS principles
V 3.0 β 2007 4
Objectives• List the three steps of the R.E.D. Survey• Describe the Incident Survey• Discuss the DISASTER paradigm• List the action steps of MASS Triage• Describe the Casualty Survey

V 3.0 β 2007 5
R.E.D. Survey
The Rapid Evaluation of a DISASTERconsists of three steps: • Step 1: Incident Survey• Step 2: MASS Triage• Step 3: Casualty Survey
V 3.0 β 2007 6
Step1: Incident SurveyIncident “ABCDE exam”
A = AwareB = BarrierC = CommunicateD = D.I.S.A.S.T.E.R.E = Enter (Exit)
Before Patient Care Initiated!
V 3.0 β 2007 7
DISASTER ParadigmD DetectionI Incident ManagementS SecurityA Assess HazardsS SupportT Triage / TreatmentE EvacuationR Recovery Does your need exceed
your resources in any of these areas?

V 3.0 β 2007 8
D-I-S-A-S-T-E-R ParadigmDetection
• Awareness that resources are being overwhelmed – Is Need > Resources? Yes is a disaster!– Requires knowing your capabilities and
capacities, right here “local”, right now!• Detection of potential cause of the event
– Not all disasters are obvious– (e.g. biological vs. Chemical, etc)
V 3.0 β 2007 9
D-I-S-A-S-T-E-R Paradigm Incident Management
• National Incident Management System (NIMS)
• Provides orderly chain of command• Clearly defined roles, responsibilities
and lines of communication• Who is the incident commander?
V 3.0 β 2007 10
D-I-S-A-S-T-E-R Paradigm Safety & Security
• Identify and mitigate obvious threats to Safety and Security– Secondary devices? (e.g. second bomb)– Ongoing action by perpetrator?– Power lines, gas leaks, building collapse– Crowd surge from patients, families, media– Time of day– Weather forecast, etc.
V 3.0 β 2007 11
D-I-S-A-S-T-E-R ParadigmAssess Hazards
• Priority One– Protect yourself and your team first!– Don’t become part of the problem!– Utilize personal protective equipment– Medical decontamination methods
• Your next priorities– Protect the public– Protect the patients– Protect the environment
• Avoid tunnel vision on the ill and injured
V 3.0 β 2007 12
D-I-S-A-S-T-E-R ParadigmSupport
• What resources are needed?• Who has them?
– Local– Regional– State – Federal
• When will they arrive?– Minutes, Hours, or Days
V 3.0 β 2007 13
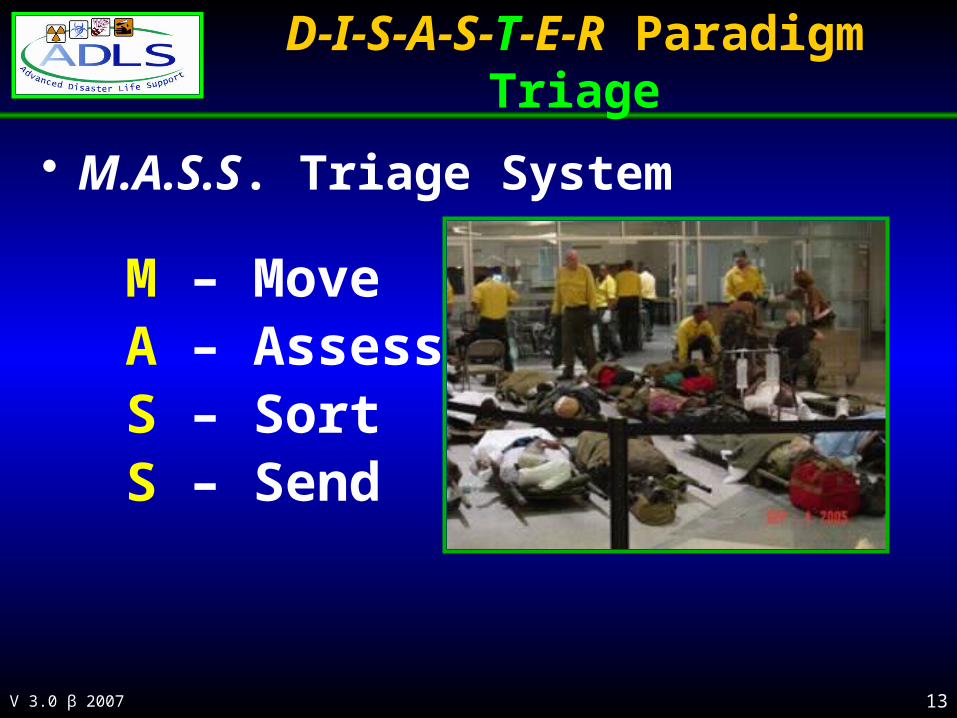
D-I-S-A-S-T-E-R ParadigmTriage
• M.A.S.S. Triage System
M – MoveA – AssessS – SortS – Send

V 3.0 β 2007 14
D-I-S-A-S-T-E-R ParadigmTreatment
• Treatment continues until:– All patients transported to healthcare areas– Resources unavailable to provide treatment– Comfort is Care!
• Treatment locations– Scene, hospitals, secondary treatment areas
• Documentation– Patient Identification / Triage Tag– Medical Record

V 3.0 β 2007 15
D-I-S-A-S-T-E-R ParadigmEvacuation
• What is your route?• Patient evacuation from scene
to hospital or treatment area– Consider routes, vehicles,
staging areas• Public evacuation of elderly,
poor, nursing homes, etc.– Special needs patients
• Hospital evacuation during a catastrophic event– Flooding, power outages– Facility contamination
• Essential part of your plan!

V 3.0 β 2007 16
D-I-S-A-S-T-E-R Paradigm Recovery
• Long-term goal of the event!• Minimize event’s impact
– Injured victims, families, rescue personnel– Community, state, and nation– Environment
• Preparedness Plan must include• Begins… when the incident occurred• Ends… often years later

V 3.0 β 2007 17
Step1: Incident Survey
Aware Barrier
Communicate
DISASTER
Enter Or Exit

V 3.0 β 2007 18
Step 2: MASS Triage• Grouping, then sorting patients• Determine the seriousness of their
injuries / illness and the likelihood of their survival
• To achieve the greatest good for the greatest number possible
• Dependent on resources available
V 3.0 β 2007 19
Triage Categories
• “ID-me”! “Identify Me”– A mnemonic for sorting patients during triage
I – ImmediateD – DelayedM – MinimalE – ExpectantD - DEAD

V 3.0 β 2007 20
Triage Categories• Triage category decision making is
dependant upon these three variables?• Injury / illness
– Is a life, limb, or vision threatening condition present?
• Intervention– Can I perform the needed medical
intervention on this patient? • Transportation
– When can I transport this patient?

V 3.0 β 2007 21
Step 2: M.A.S.S Triage• Move
• Anyone who can walk is told to MOVE to a collection area• Remaining victims are told to MOVE an arm or leg
• Assess • Remaining patients who didn’t move (help these first)
• Sort • Categorize patients by “ID-me”• Immediate, Delayed, Minimal, Expectant, Dead
• Send• Transport IMMEDIATE patients first• Send to Hospitals and Secondary Treatment Facilities
V 3.0 β 2007 22
Triage Documentation• Medical record
– It is often the only medical record available on the patient
• Communication– Vital, often only, link to information
• Identification• History & Physical• Treatment • Old medical records• Contact information• Personal message

V 3.0 β 2007 23
M.A.S.S Triage
Key Principle of MASS Triage:
• Group, …then Sort,
…then Transport!
V 3.0 β 2007 24
Step 3: Casualty Survey
Early patient assessment during a mass casualty incident includes:
A: AirwayB: BreathingC: CirculationD: ?E: ?

V 3.0 β 2007 25
Step 3: Casualty Survey
Early patient assessment during a mass casualty incident includes:
A: AirwayB: BreathingC: CirculationD: Differential Dx, Detection & DeliveryE: ?
V 3.0 β 2007 26
Step 3: Casualty Survey
D: Differential Dx, Detection & Delivery:• What could be causing this casualty?• What antidote or intervention needed? • Head & Neck:
• Pupils, Secretions, Neuro, Tenderness, Trauma• Chest:
• Breathing, Heart R&R, Tenderness, Trauma• Abdomen:
• Pain, N&V, Diarrhea, Tenderness, Trauma
V 3.0 β 2007 27
Step 3: Casualty SurveyIs a life-saving medical or surgical
intervention needed? • Airway:
• Manual, ET Intubation, Needle Cricothyroidotomy• Breathing:
• Needle Decompression• Circulation:
• Uncontrolled bleeding management,• Pericardiocentesis
• Detection of agents and antidote delivery
V 3.0 β 2007 28
Step 3: Casualty Survey
Early patient assessment during a mass casualty incident includes:
A: AirwayB: BreathingC: CirculationD: Differential Dx, Detection & DeliveryE: Evaluate or Evacuate (Exit)

V 3.0 β 2007 29
Step 3: Casualty Survey
AirwayBreathing
Circulation
DDxDetectionDelivery
Evaluate Or
Evacuate (Exit)

V 3.0 β 2007 30
R.E.D. Survey• Completed the Rapid Evaluation of a
DISASTER• Step 1: Incident Survey• Step 2: MASS Triage• Step 3: Casualty Survey
V 3.0 β 2007 31
SummaryNow you can:• List the three steps of the R.E.D. Survey• Describe the Incident Survey• Discuss the DISASTER paradigm• List the action steps of MASS Triage• Describe the Casualty Survey
V 3.0 β 2007 32
Thank You!
Questions?
V 3.0 β 2007 33
Contact information
Ray E. Swienton, MD, FACEP
Co-Director, EMS, Disaster Medicine & Homeland Security SectionDivision of Emergency Medicine, Department of SurgeryUniversity of Texas, Southwestern Medical Center at Dallas5323 Harry Hines Blvd.Dallas, Texas 75390-8579
Email: [email protected]
Voice: (817) 271-7801

V 3.0 β 2007 34
Last Slide• Intentionally blank

















