Page 1
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Prescription benefit updates Individual/small group
Moda Health’s prescription program is a pharmacy benefit that offers members a choice of safe
and effective medication treatments. The program also helps you save money on prescription
drugs. Periodically, medication coverage changes will occur. These changes allow us to maintain
a comprehensive benefit and provide you with an open formulary and choice, and support the
program’s ongoing stability.
Our prescription program uses a tiered copay/coinsurance system. You and your doctor can
choose between the value, select, preferred or brand tier medications. What you pay for a drug
depends on your plan.
Please review the following expected pharmacy coverage updates. Please note, this information could change and does not represent every potential update to your benefits. Refer to your
member handbook for specific tier and coverage information.
Questions? Call our Pharmacy Customer Service team toll-free at 888-361-1610.
Value tier Select tier Preferred tier Non-Preferred tier Specialty tier
Value medications include
commonly prescribed
medications used to treat
chronic medical conditions
and preserve health.
Plans that do not include a
value tier benefit will have
medications categorized
under this tier paid at the
select or preferred tier
copay/coinsurance levels.
Generic medications are
considered by physicians
and pharmacists to be
therapeutically the same
as brand name
alternatives and at the
most favorable cost.
Generic medications
must contain the same
active ingredient as their
brand name counterparts
and be identical in
strength, dosage and
format.
This benefit level may
also include select brand
medications that have
been identified as
favorable from a clinical
and cost effective
perspective.
The preferred tier
includes brand and
specialty brand name
medications that have
been reviewed by Moda
Health and found to be
clinically effective at a
favorable cost when
compared with other
medications in the same
category.
This tier may also include
generic medications that
have been found to have
the same clinical
outcomes as their more
cost-effective generic
counterparts in the same
category.
This tier includes brand
name medications that
have been reviewed by
Moda Health and found
not to have a significant
therapeutic advantage
over their preferred tier
counterparts.
Certain prescription
medications are defined
as specialty products.
Specialty medications are
often used to treat
complex chronic health
conditions. Specialty
treatments often require
special handling
techniques, careful
administration and a
unique ordering process.
You must access
specialty medications
through the exclusive
specialty pharmacy.
Page 2
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Prescription coverage updates
These expected Moda Health prescription tier and coverage updates go into effect for 2018.
Product name Effective date Update
Bonjesta
(doxylamine/ pyridoxine)
New starts: 7/1/2018
Existing users: 10/1/2018
Change quantity limit on Bonjesta as follows: Limited to 60
tablets per 30 days.
Erleada
(apalutamide)
New starts: 7/1/2018
Existing users: 10/1/2018
Add quantity limit on Erleada as follows: Limited to 120 tablets
per 30 days.
Genvisc 850, Visco-3,
Supartz FX
(hyaluronate acid)
New starts: 7/1/2018
Existing users: 10/1/2018
Add prior authorization guideline on Genvisc 850, Visco-3, and
Supartz FX.
Lonhala Magnair
(glycopyrrolate nebulizer)
New starts: 7/1/2018
Existing users: 10/1/2018
Add quantity limit on Lonhala Magnair as follows: Limited to 1
unit per 30 days.
Marinol
(dronabinol)
New starts: 7/1/2018
Existing users: 10/1/2018
Change step therapy on Marinol as follows: Must try/fail at
least 1 of the following: Emend, Corticosteroid, 5HT3
antagonist OR megestrol regular strength suspension in the
previous 120 days.
Noctiva
(desmopressin)
New starts: 7/1/2018
Existing users: 10/1/2018
Add quantity limit on Noctiva as follows: Limited to up to 3.8g
(1 canister) per 30 days.
Syndros
(dronabinol solution)
New starts: 7/1/2018
Existing users: 10/1/2018
Change step therapy on Syndros as follows: Must try/fail at
least one of the following: generic dronabinol capsules OR
megestrol regular strength suspension in the previous 120
days.
Vancomycin capsules New starts: 7/1/2018
Existing users: 10/1/2018
Change quantity limit on vancomycin capsules as follows:
125mg: 56 caps per 30 days
250mg: 112 caps per 30 days
Zypitamag
(pitavastatin magnesium)
New starts: 7/1/2018
Existing users: 10/1/2018
Add step therapy on Zypitamag as follows: Must try/fail Livalo
(pitavastatin calcium) in the previous 120 days.
Zytiga 250mg tablets
(abiraterone)
New starts: 7/1/2018
Existing users: 10/1/2018
Changing quantity limit on Zytiga as follows: Limited to 90
tablets per 30 days.
Benlysta IV
(belimumab)
New starts: 4/1/2018
Existing users: 7/1/2018 Add prior authorization requirements on Benlysta IV.
Biktarvy
(bictegravir/ emtricitabine/
tenofovir alafenamide)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Biktarvy as follows: Limited to 30 tablets
per 30 days.
Bosulif
(bosutinib)
New starts: 4/1/2018
Existing users: 7/1/2018
Change quantity limit on Bosulif as follows:
100mg tablets: 90 tabs per 30 days
400mg tablets: 30 tabs per 30 days
500mg tablets: 30 tabs per 30 days
Carospir oral suspension
(spironolactone)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Carospir as follows: Limited to 600mL per
30 days.
Add step therapy on Carospir as follows: Must try/fail
spironolactone tablets in previous 120 days.
Page 3
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
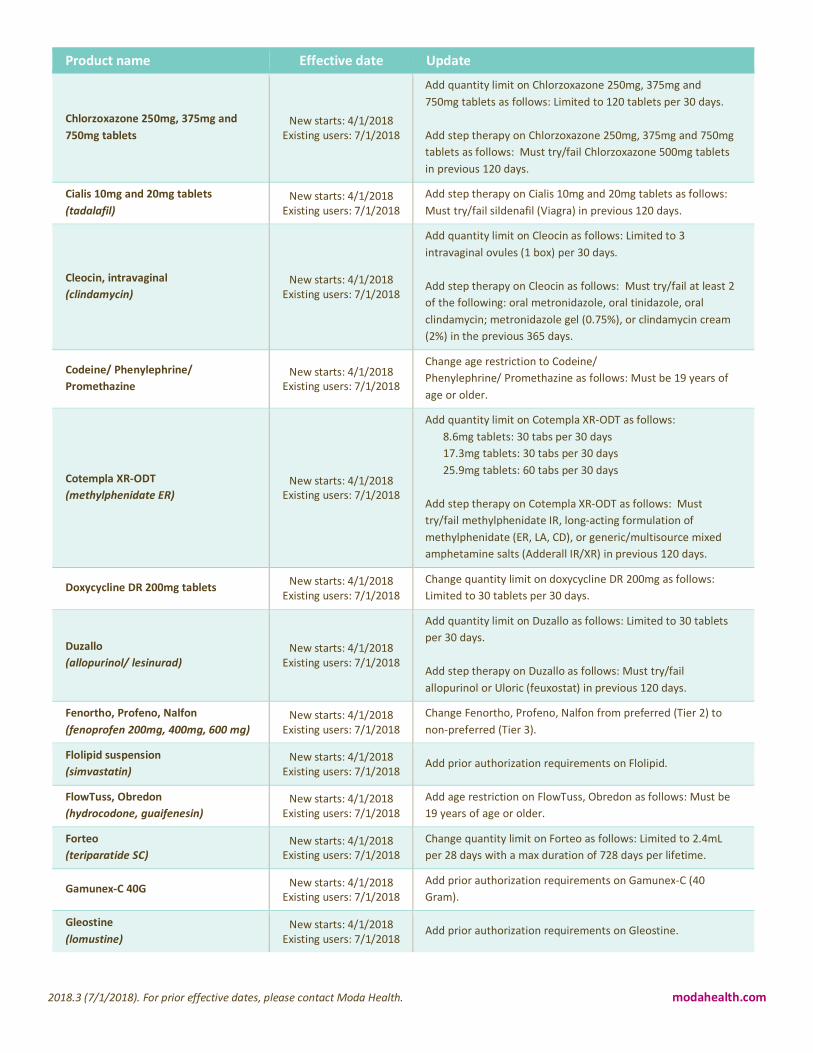
Product name Effective date Update
Chlorzoxazone 250mg, 375mg and
750mg tablets
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Chlorzoxazone 250mg, 375mg and
750mg tablets as follows: Limited to 120 tablets per 30 days.
Add step therapy on Chlorzoxazone 250mg, 375mg and 750mg
tablets as follows: Must try/fail Chlorzoxazone 500mg tablets
in previous 120 days.
Cialis 10mg and 20mg tablets
(tadalafil)
New starts: 4/1/2018
Existing users: 7/1/2018
Add step therapy on Cialis 10mg and 20mg tablets as follows:
Must try/fail sildenafil (Viagra) in previous 120 days.
Cleocin, intravaginal
(clindamycin)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Cleocin as follows: Limited to 3
intravaginal ovules (1 box) per 30 days.
Add step therapy on Cleocin as follows: Must try/fail at least 2
of the following: oral metronidazole, oral tinidazole, oral
clindamycin; metronidazole gel (0.75%), or clindamycin cream
(2%) in the previous 365 days.
Codeine/ Phenylephrine/
Promethazine
New starts: 4/1/2018
Existing users: 7/1/2018
Change age restriction to Codeine/
Phenylephrine/ Promethazine as follows: Must be 19 years of
age or older.
Cotempla XR-ODT
(methylphenidate ER)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Cotempla XR-ODT as follows:
8.6mg tablets: 30 tabs per 30 days
17.3mg tablets: 30 tabs per 30 days
25.9mg tablets: 60 tabs per 30 days
Add step therapy on Cotempla XR-ODT as follows: Must
try/fail methylphenidate IR, long-acting formulation of
methylphenidate (ER, LA, CD), or generic/multisource mixed
amphetamine salts (Adderall IR/XR) in previous 120 days.
Doxycycline DR 200mg tablets New starts: 4/1/2018
Existing users: 7/1/2018
Change quantity limit on doxycycline DR 200mg as follows:
Limited to 30 tablets per 30 days.
Duzallo
(allopurinol/ lesinurad)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Duzallo as follows: Limited to 30 tablets
per 30 days.
Add step therapy on Duzallo as follows: Must try/fail
allopurinol or Uloric (feuxostat) in previous 120 days.
Fenortho, Profeno, Nalfon
(fenoprofen 200mg, 400mg, 600 mg)
New starts: 4/1/2018
Existing users: 7/1/2018
Change Fenortho, Profeno, Nalfon from preferred (Tier 2) to
non-preferred (Tier 3).
Flolipid suspension
(simvastatin)
New starts: 4/1/2018
Existing users: 7/1/2018 Add prior authorization requirements on Flolipid.
FlowTuss, Obredon
(hydrocodone, guaifenesin)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on FlowTuss, Obredon as follows: Must be
19 years of age or older.
Forteo
(teriparatide SC)
New starts: 4/1/2018
Existing users: 7/1/2018
Change quantity limit on Forteo as follows: Limited to 2.4mL
per 28 days with a max duration of 728 days per lifetime.
Gamunex-C 40G New starts: 4/1/2018
Existing users: 7/1/2018
Add prior authorization requirements on Gamunex-C (40
Gram).
Gleostine
(lomustine)
New starts: 4/1/2018
Existing users: 7/1/2018 Add prior authorization requirements on Gleostine.
Page 4
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
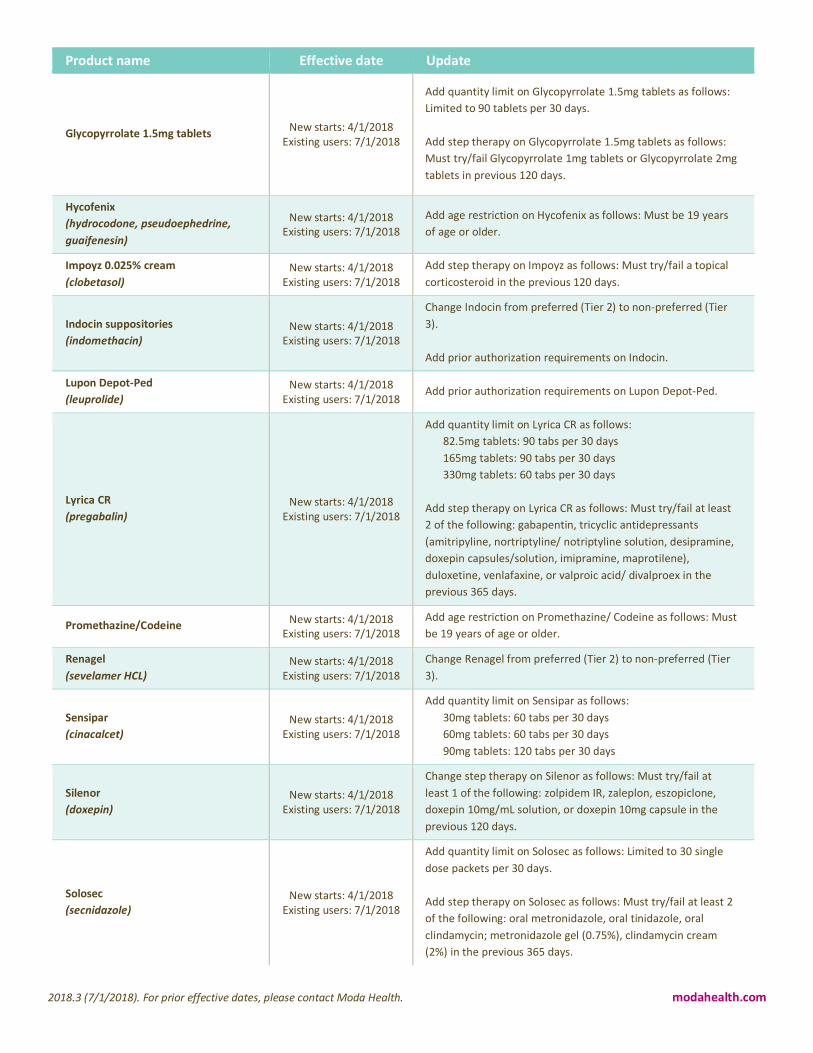
Product name Effective date Update
Glycopyrrolate 1.5mg tablets New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Glycopyrrolate 1.5mg tablets as follows:
Limited to 90 tablets per 30 days.
Add step therapy on Glycopyrrolate 1.5mg tablets as follows:
Must try/fail Glycopyrrolate 1mg tablets or Glycopyrrolate 2mg
tablets in previous 120 days.
Hycofenix
(hydrocodone, pseudoephedrine,
guaifenesin)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Hycofenix as follows: Must be 19 years
of age or older.
Impoyz 0.025% cream
(clobetasol)
New starts: 4/1/2018
Existing users: 7/1/2018
Add step therapy on Impoyz as follows: Must try/fail a topical
corticosteroid in the previous 120 days.
Indocin suppositories
(indomethacin)
New starts: 4/1/2018
Existing users: 7/1/2018
Change Indocin from preferred (Tier 2) to non-preferred (Tier
3).
Add prior authorization requirements on Indocin.
Lupon Depot-Ped
(leuprolide)
New starts: 4/1/2018
Existing users: 7/1/2018 Add prior authorization requirements on Lupon Depot-Ped.
Lyrica CR
(pregabalin)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Lyrica CR as follows:
82.5mg tablets: 90 tabs per 30 days
165mg tablets: 90 tabs per 30 days
330mg tablets: 60 tabs per 30 days
Add step therapy on Lyrica CR as follows: Must try/fail at least
2 of the following: gabapentin, tricyclic antidepressants
(amitripyline, nortriptyline/ notriptyline solution, desipramine,
doxepin capsules/solution, imipramine, maprotilene),
duloxetine, venlafaxine, or valproic acid/ divalproex in the
previous 365 days.
Promethazine/Codeine New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Promethazine/ Codeine as follows: Must
be 19 years of age or older.
Renagel
(sevelamer HCL)
New starts: 4/1/2018
Existing users: 7/1/2018
Change Renagel from preferred (Tier 2) to non-preferred (Tier
3).
Sensipar
(cinacalcet)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Sensipar as follows:
30mg tablets: 60 tabs per 30 days
60mg tablets: 60 tabs per 30 days
90mg tablets: 120 tabs per 30 days
Silenor
(doxepin)
New starts: 4/1/2018
Existing users: 7/1/2018
Change step therapy on Silenor as follows: Must try/fail at
least 1 of the following: zolpidem IR, zaleplon, eszopiclone,
doxepin 10mg/mL solution, or doxepin 10mg capsule in the
previous 120 days.
Solosec
(secnidazole)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Solosec as follows: Limited to 30 single
dose packets per 30 days.
Add step therapy on Solosec as follows: Must try/fail at least 2
of the following: oral metronidazole, oral tinidazole, oral
clindamycin; metronidazole gel (0.75%), clindamycin cream
(2%) in the previous 365 days.
Page 5
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Product name Effective date Update
Sprix
(ketorolac)
New starts: 4/1/2018
Existing users: 7/1/2018
Add step therapy on Sprix as follows: Must try/fail 1 generic
NSAID in previous 120 days.
Supprelin LA
(histrelin)
New starts: 4/1/2018
Existing users: 7/1/2018 Add prior authorization requirements on Supprelin LA.
Taytulla
(ethnityl estradiol/ noethindrone/Fe)
New starts: 4/1/2018
Existing users: 7/1/2018
Add step therapy on Taytulla as follows: Must try/fail at least 2
generic contraceptives in previous 365 days.
Tussicaps
(hydrocodone, chlorpheniramine ER)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Tussicaps as follows: Must be 19 years
of age or older.
Tussigon (tablet),
Hydromet (syrup)
(hydrocodone/homatropine)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Tussigon (tablet) and Hydromet (syrup)
as follows: Must be 19 years of age or older.
Tussionex
(hydrocodone, chlorpheniramine ER
12H suspension)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Tussionex as follows: Must be 19 years
of age or older.
Tuzistra XR
(codeine/chlorpheniramine)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Tuzistra XR as follows: Must be 19 years
of age or older.
Vemlidy
(tenofovir alafenamide)
New starts: 4/1/2018
Existing users: 7/1/2018
Add step therapy to Vemlidy as follows: Must try/fail tenofovir
300mg (Viread) in previous 120 days.
Vituz
(hydrocodone, chlorpheniramine)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Vituz as follows: Must be 19 years of
age or older.
Xhance
(fluticasone propionate)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Xhance as follows: Limited to 32mL (2
inhalation devices) per 30 days.
Add step therapy on Xhance as follows: Must try/fail at least 2
of the following inhaled nasal corticosteriods: mometasone,
fluticasone propionate/furoate, flunisolide, or beclomethasone
(Qnasl) in the previous 365 days.
Xigduo XR
(dapagliflozin/metformin)
New starts: 4/1/2018
Existing users: 7/1/2018
Change quantity limit on Xigduo XR as follows:
2.5/1000mg tablets: 60 tabs per 30 days
5/1000mg tablets: 60 tabs per 30 days
5/500mg tablets: 30 tabs per 30 days
10/500mg tablets: 30 tabs per 30 days
10/1000mg tablets: 30 tabs per 30 days
Ximino
(minocycline ER cap)
New starts: 4/1/2018
Existing users: 7/1/2018
Add quantity limit on Ximino as follows: Limited to 30 capsules
per 30 days.
Add step therapy on Ximino as follows: Must try/fail generic IR
Minocycline tablets or generic IR Minocycline capsules in the
previous 120 days.
Add age restriction on Ximino as follows: Must be 12 years of
age or older.
Zodex/Locort/
ZonaCort/Dexpack
(dexamethasone 1.5 mg blister pack)
New starts: 4/1/2018
Existing users: 7/1/2018
Change step therapy on Zodex/Locort/Zonacort/Dexpack
(dexamethasone 1.5 mg tablet taper packs) as follows: Must
try/fail dexamethasone 1.5 mg tablets.
Zurampic
(lesinurad)
New starts: 4/1/2018
Existing users: 7/1/2018
Change Zurampic from preferred (Tier 2) to non-preferred (Tier
3).
Page 6
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Product name Effective date Update
Zutripro
(hydrocodone, chlorpheniramine,
pseudophedrine)
New starts: 4/1/2018
Existing users: 7/1/2018
Add age restriction on Zutripro as follows: Must be 19 years of
age or older.
ArmonAir RespiClick
(fluticasone propionate)
New starts: 1/1/2018
Existing users: 4/1/2018
Add quantity limit on ArmonAir RespiClick as follows: Limited
to one inhaler per 30 days.
Add step therapy on ArmonAir RespiClick as follows: Must
try/fail Arnuity Ellipta, Flovent Diskus, Flovent HFA, or Qvar.
Asmanex, Asmanex HFA
(mometasone furoate)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Asmanex and Asmanex HFA from Value tier to non-
preferred (Tier 3).
Avonex, Avonex Pen
(interferon beta-1a)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Avonex and Avonex Pen from preferred (Tier 2) to
non-preferred (Tier 3).
Bethkis
(tobramycin)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Bethkis from preferred (Tier 2) to non-preferred (Tier
3).
Cayston
(aztreonam lysine)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Cayston from preferred (Tier 2) to non-preferred (Tier
3).
Copaxone
(glatiramer acetate)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Copaxone from preferred (Tier 2) to non-preferred
(Tier 3).
Fiasp
(insulin aspart (niacinamide))
New starts: 1/1/2018
Existing users: 4/1/2018
Add quantity limit on Fiasp as follows:
Vial: 40mL (4 vials) per 28 days
Pen: 30mL (10 vials) per 28 days
Add step therapy on Fiasp as follows: Must try/fail Humalog.
Gilenya
(fingolimod HCl)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Gilenya from preferred (Tier 2) to non-preferred (Tier
3).
Kitabis Pak
(tobramycin/nebulizer)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Kitabis Pak from preferred (Tier 2) to non-preferred
(Tier 3).
Lysodren
(mitotane)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Lysodren from preferred (Tier 2) to non-preferred (Tier
3).
Nexium 40mg capsule, packet
(esomeprazole trihydrate)
New starts: 1/1/2018
Existing users: 4/1/2018
Change quantity limit on Nexium 40mg capsule/packet as
follows: Limited to 60 capsules or packets per 30 days.
Plegridy, Plegridy Pen
(peginterferon beta-1a)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Plegridy and Plegridy Pen from preferred (Tier 2) to
non-preferred (Tier 3).
Pulmicort Flexhaler
(budesonide)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Pulmicort Flexhaler from Value tier to non-preferred
(Tier 3).
Rebif, Rebif Rebidose
(interferon beta-1a/albumin)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Rebif and Rebif Rebidose from preferred (Tier 2) to
non-preferred (Tier 3).
Shingrix
(Varicella-Zoster
GE/AS01/PF)
New starts: 1/1/2018
Existing users: 4/1/2018
Add quantity limit to Shingrix as follows: Limit to 2 doses per
365 days
Add age restriction to Shingrix as follows: Must be 50 years of
age or older
Page 7
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Product name Effective date Update
Sivextro
(tedizolid)
New starts: 1/1/2018
Existing users: 4/1/2018
Add quantity limit on Sivextro as follows: 1 tablet per day for a
duration of 6 days.
Add step therapy on Sivextro as follows: Must try/fail linezolid
600mg tablets.
Tecfidera
(dimethyl fumarate)
New starts: 1/1/2018
Existing users: 4/1/2018
Change Tecfidera from preferred (Tier 2) to non-preferred
(Tier 3).
Tobi
(tobramycin in 0.225% sod chlor)
New starts: 1/1/2018
Existing users: 4/1/2018 Change Tobi from preferred (Tier 2) to non-preferred (Tier 3).
Xyzbac, Mebolic
(multivit34/folic
ac/nadh/coq10)
New starts: 1/1/2018
Existing users: 4/1/2018 Add prior authorization requirements on Xyzbac and Mebolic.
Yescarta
(axicabtagene ciloleucel)
New starts: 1/1/2018
Existing users: 4/1/2018 Add prior authorization requirements on Yescarta.
This document is provided for informational purposes only, and is intended as a quick reference. For cost and further details of the coverage,
including exclusions, prior authorization requirements, any reduction or limitations and the terms under which the policy may be continued in
force, contact your producer or Moda Health.
Copyright © 2014 Moda, Inc. All Rights Reserved. Health plans in Oregon and Alaska provided by Moda Health Plan, Inc
Page 8
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com
Page 9
2018.3 (7/1/2018). For prior effective dates, please contact Moda Health. modahealth.com