Safety of Peg Tube Insertion in Patients with ALS Using Propofol Sedation in an Outpatient Surgical Center Pamela Kittrell MSN RN CCRC Clinical Research Nurse Senior The University of Texas Health Science Center at San Antonio
Transcript
Safety of Peg Tube Insertion
in Patients with ALSUsing Propofol Sedation in an Outpatient Surgical Center
Pamela Kittrell MSN RN CCRC
Clinical Research Nurse Senior
The University of Texas Health Science Center at San Antonio
Objectives
• Review the nutritional needs of the ALS
patient
• Explain the different methods used in tube
placement
• Discuss the results of the PEG tube
outpatient placement study and apply
them in a clinical setting
Background Historically
50% dead within 3 years
20% live 5 years
10% live 10 years
Worse prognosis if: Bulbar onset (30% show symptoms at onset)
FALS
Simultaneous arm/leg onset
Older age at diagnosis
Onset <40: 8.2 yr; onset 61-70: 2.6 yr
AAN Guidelines
• In patients with ALS, impaired oral food intake, enteral
nutrition via PEG should be considered to stabilize body
weight
• Insufficient data to support or refute specific timing of
PEG insertion in ALS patients
• Peg should be considered for prolonging survival in
patients with ALS
Procedure Options
Percutaneous Endoscopic Gastrostomy (PEG)
Percutaneous Endoscopic Jejunostomy (PEJ)
Radiologically Inserted Gastrostomy (RIG)
Complications
• Aspiration
• Bleeding
• Bowel
perforation
• Peritonitis
• Death
• Local infection
• Buried bumper
• Tube
blockage/breakdown
• Stoma leakage
• Inadvertent peg tube
removal
Our Study
Primary
• To review the authors’ experience of PEG
tube placement in patients with
amyotrophic lateral sclerosis with different
degrees of impaired respiratory function
• Secondary• To demonstrate the safety profile, peri-procedural and
post-interventional complications of PEG tube insertion
performed in an outpatient surgical center.
What we did
Retrospective medical records review
of patients treated at the University of
Texas Health Science Center of San
Antonio ALS clinic who were referred
for PEG tube placement using propofol
sedation at an outpatient surgical
center between 2011-2014
Methodology
• Three year period:
– Total referrals to Gastroenterology 145
• Less those that did not meet criteria 27
• Total number of charts reviewed 118
• Less those who refused peg 28
76% of all referrals resulted in peg placement• 24% of all referrals were refused
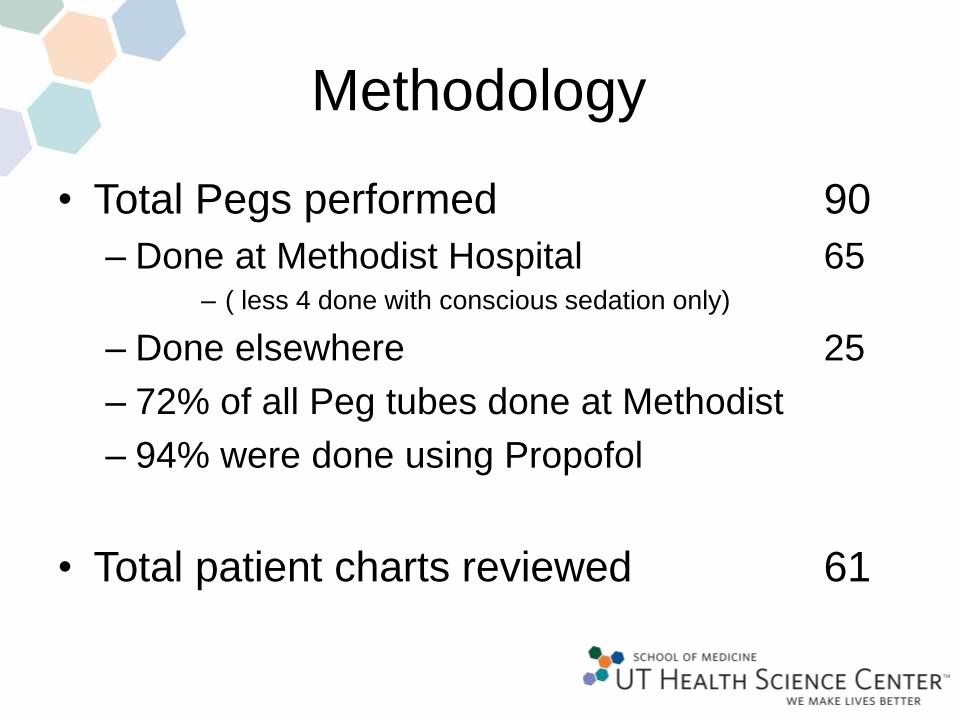
Methodology
• Total Pegs performed 90
– Done at Methodist Hospital 65– ( less 4 done with conscious sedation only)