33
A Day in the Life A Day in the Life of an MS3 of an MS3 Capstone I - May 27, 2008 Capstone I - May 27, 2008
| Date post: | 13-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | yashika54 |
| View: | 279 times |
| Download: | 1 times |

A Day in the Life A Day in the Life of an MS3of an MS3
Capstone I - May 27, 2008Capstone I - May 27, 2008

First, some basics…First, some basics…
The TeamThe Team The Call CycleThe Call Cycle The Key The Key
PlayersPlayers Round and Round and
Round we goRound we go Wards vs. Wards vs.
ClinicClinic

The first day . . .The first day . . . You are a superstar You are a superstar
MS3 on your first day MS3 on your first day of your Medicine of your Medicine rotationrotation
Your team is “on-call”Your team is “on-call” Your senior turns to Your senior turns to
you and your intern you and your intern and says…and says…
There’s a new admitThere’s a new admit You’re off to the ER!You’re off to the ER!

A Case-A Case-Your New Patient Your New Patient
5:52 pm5:52 pm
ID: 63 yo woman 2 wks s/p thoracic ID: 63 yo woman 2 wks s/p thoracic laminectomy, presenting with 1 hour of laminectomy, presenting with 1 hour of pleuritic chest pain.pleuritic chest pain.
Hot Tip # 1Hot Tip # 1 Be preparedBe prepared
ClothesClothes White CoatWhite Coat ToolsTools References-Maxwell’sReferences-Maxwell’s Clipboard like device-Clipboard like device-
H&P formH&P form Consider your Consider your
differential diagnosisdifferential diagnosis MI, PE, PNA, GERD, MI, PE, PNA, GERD,
Costochondritis, Costochondritis, Trauma, Esophageal Trauma, Esophageal Spasm . . . Spasm . . .

Taking a HistoryTaking a History
6:05 pm6:05 pm
HPI: Pt was in her USOH, complicated by mild COPD HPI: Pt was in her USOH, complicated by mild COPD until 1 hour prior to presentation when while watching until 1 hour prior to presentation when while watching tv she developed acute dyspnea and sharp L sided tv she developed acute dyspnea and sharp L sided chest pain radiating to her L arm and jaw, worse with chest pain radiating to her L arm and jaw, worse with inspiration and exertion. Pain is 8/10. Pt denies inspiration and exertion. Pain is 8/10. Pt denies nausea, diaphoresis, palpitations, leg pain or edema.nausea, diaphoresis, palpitations, leg pain or edema.

Still taking a historyStill taking a history ROSROS: Per HPI, pt : Per HPI, pt denies nausea, diaphoresis, palpitations, leg pain or denies nausea, diaphoresis, palpitations, leg pain or
edemaedema. Don’t forget all systems!. Don’t forget all systems!
PMH/PSHPMH/PSH: COPD, OA, Depression, Allergic rhinitis, GERD, : COPD, OA, Depression, Allergic rhinitis, GERD, Recent Recent laminectomylaminectomy
MedicationsMedications: Ipratropium, Citalopram, Lansoprazole, : Ipratropium, Citalopram, Lansoprazole, Salmeterol/Fluticasone Inhaled , Fluticasone nasal spraySalmeterol/Fluticasone Inhaled , Fluticasone nasal spray
AllergiesAllergies: NKDA: NKDA
FHFH: Father died from MI, age 72. Mother with CVA in her early 70’s. : Father died from MI, age 72. Mother with CVA in her early 70’s. Strong family history of hypertension.Strong family history of hypertension.
SocialSocial: Patient has been a : Patient has been a cigarette smokercigarette smoker since age 19. Reports that since age 19. Reports that she has quit, but also admits that she had a cigarette this morning. She she has quit, but also admits that she had a cigarette this morning. She denies any alcohol or other drug use. denies any alcohol or other drug use.

Quick QuizQuick Quiz O: O: P:P: Q: Q: R: R: S: S: T: T: A: A: A:A: A:A:
One hour PTAOne hour PTALeft-SidedLeft-SidedSharp painSharp painRadiates to left arm and jawRadiates to left arm and jaw8/108/10ConstantConstantAggravated by inspiration and exertionAggravated by inspiration and exertionNot alleviated by anythingNot alleviated by anythingPatient attributes the pain to “her Patient attributes the pain to “her heart”heart”

Physical Exam Physical Exam 6:20 pm6:20 pm VITALSVITALS: : P:110, R:20, BP:119/85, O2 sat 96% on 2L.P:110, R:20, BP:119/85, O2 sat 96% on 2L.
GENERALGENERAL: Patient is sitting up, appearing dyspneic and in pain.: Patient is sitting up, appearing dyspneic and in pain.
HEENTHEENT: The head is atraumatic. PERRLA. EOMI. There is no nasal discharge. Oropharynx is clear : The head is atraumatic. PERRLA. EOMI. There is no nasal discharge. Oropharynx is clear without visible lesions. Moist mucous membranes. without visible lesions. Moist mucous membranes.
NECKNECK: Supple. : Supple.
CHESTCHEST: : CTAB without any crackles, wheezes or rhonchi. Pain not reproducible withCTAB without any crackles, wheezes or rhonchi. Pain not reproducible with palpation.palpation.
CVCV: : Tachycardia, regular rhythm,Tachycardia, regular rhythm, Normal S1 and S2. No murmurs, rubs or gallopsNormal S1 and S2. No murmurs, rubs or gallops. .
ABDOMENABDOMEN: Soft, NT/ND without palpable HSM. : Soft, NT/ND without palpable HSM.
BACKBACK: : There is a healing midline scar in the mid to lower thoracic region without overlying erythema, There is a healing midline scar in the mid to lower thoracic region without overlying erythema, swelling or exudate. swelling or exudate.
EXTEXT: Warm and well perfused with brisk capillary refill. No clubbing, cyanosis or edema. : Warm and well perfused with brisk capillary refill. No clubbing, cyanosis or edema. There is no There is no tenderness to palpation of the calves bilaterally. tenderness to palpation of the calves bilaterally.
NEURONEURO: Patient is alert and oriented. Cranial nerves are intact and strength is symmetric upper and lower : Patient is alert and oriented. Cranial nerves are intact and strength is symmetric upper and lower extremities. extremities.
Differential DiagnosisDifferential Diagnosis
TraumaTrauma GERDGERD CostochondritisCostochondritis Esophageal SpasmEsophageal Spasm PneumoniaPneumonia MIMI PEPE

Hot Tip #2Hot Tip #2
Admitting the patientAdmitting the patient
Look up records, labs, studiesLook up records, labs, studies
References to help with diagnosis and References to help with diagnosis and treatmenttreatment
Admit ordersAdmit orders

Reviewing the medical Reviewing the medical record . . .record . . .
Look up your patient in the electronic medical record Orca-Harborview, UW, Children’s CIS-Children’s VA-CPRS
www.uwresidents.com If applicable, call primary care provider to notify
that patient is being admitted and to gather additional information


ReferencesReferences
Healthlinks Healthlinks http://http://healthlinks.washington.eduhealthlinks.washington.edu
UpToDate ?UpToDate ? MD ConsultMD Consult PubmedPubmed MicromedexMicromedex Patient HandoutsPatient Handouts
Pocket ReferencesPocket References



Studies/LabsStudies/Labs
Na | Cl | BUN Na | Cl | BUN / Glucose WBC\/ Glucose WBC\Hg Hg /PLT/PLTK | Bicarb | Cr \ /HCT\K | Bicarb | Cr \ /HCT\
141 | 102 | 13 141 | 102 | 13 / 90 5.4\/ 90 5.4\11.311.3/544/5444.1 | 25 | 0.6 \ /34\4.1 | 25 | 0.6 \ /34\
CaCa++ ++ 9.7, Mg 2.19.7, Mg 2.1 D-dimerD-dimer 1.071.07 Cardiac Enzymes Negative x1Cardiac Enzymes Negative x1INR 1.0 INR 1.0
ECG: Tachycardia, rate 110, ECG: Tachycardia, rate 110, no specific ST or T-wave no specific ST or T-wave changeschanges

Revisiting our Revisiting our DifferentialDifferential
MIMI
PEPE
Confirm suspicion of PE with CT-PA- Computed Confirm suspicion of PE with CT-PA- Computed Tomography with Pulmonary AngiogramTomography with Pulmonary Angiogram
But we can’t get the CT-PA right away so let’s But we can’t get the CT-PA right away so let’s admit her to the hospital in the meantime . . .admit her to the hospital in the meantime . . .

Admit OrdersAdmit Orders
6:45 pm6:45 pm Admit to Medicine Admit to Medicine Diagnosis: Pulmonary EmbolismDiagnosis: Pulmonary Embolism Condition: StableCondition: Stable Vitals: per routineVitals: per routine Allergies: NKDAAllergies: NKDA Activity: OOB TID with assistanceActivity: OOB TID with assistance Nursing: Call HO if HR>110, <50, T>38.5, BP>180/110, <100/40, RR>20, <6Nursing: Call HO if HR>110, <50, T>38.5, BP>180/110, <100/40, RR>20, <6 Diet: RegularDiet: Regular IV fluids: NoneIV fluids: None Medications:Medications:
Ipratropium MDI 2-3 puffs inhaled TIDIpratropium MDI 2-3 puffs inhaled TID Salmeterol/Fluticasone MDI 1 dose inhaled BIDSalmeterol/Fluticasone MDI 1 dose inhaled BID Citalopram 20mg PO q dayCitalopram 20mg PO q day Lansoprazole 20mg PO q dayLansoprazole 20mg PO q day
Labs: Troponin I, CK, CKMB x2 @ 2400 and 0600Labs: Troponin I, CK, CKMB x2 @ 2400 and 0600 Special: TEDs and SCDs, Consult PTSpecial: TEDs and SCDs, Consult PT Code Status: Full Code (be sure to discuss with patient)Code Status: Full Code (be sure to discuss with patient)
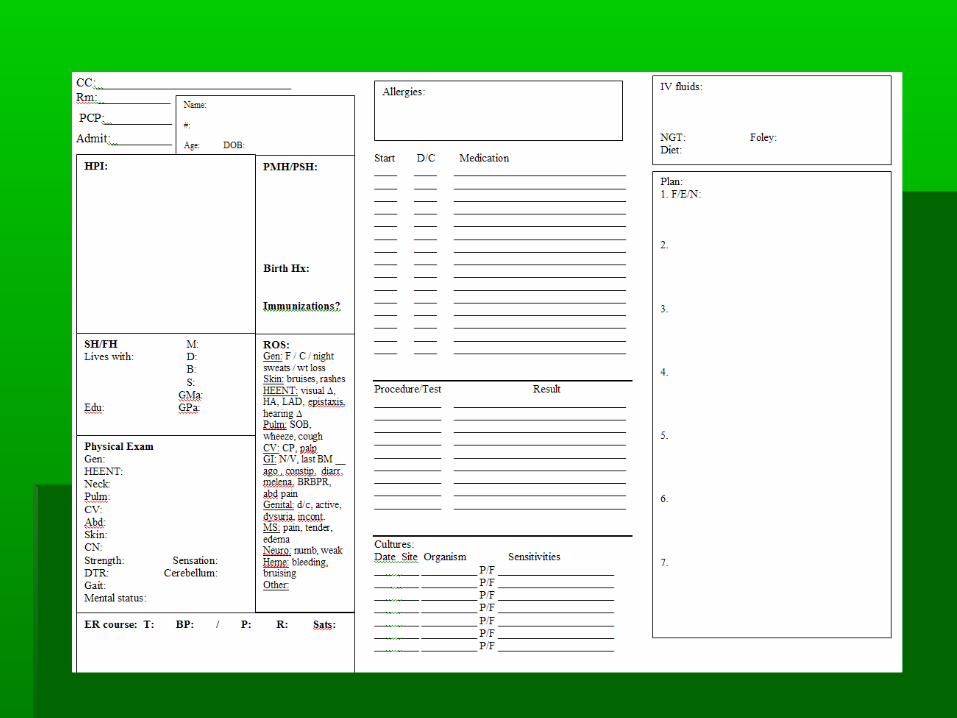
Hot tip #3Hot tip #3
Now that your patient is admitted, how do Now that your patient is admitted, how do you keep track of her information?you keep track of her information? Notecards, patient tracking templatesNotecards, patient tracking templates
Copies of H&P write-up and daily notesCopies of H&P write-up and daily notes
Make a “To-Do” list with boxes to be Make a “To-Do” list with boxes to be checked off, consult this list frequently! checked off, consult this list frequently!


““To-Do” ListTo-Do” List
□□ Check CT resultsCheck CT results
□□ Follow-up cardiac enzymesFollow-up cardiac enzymes
□□ Consult PTConsult PT
□□ Call SNF for discharge planningCall SNF for discharge planning
□□ Call PCPCall PCP

And 2 hours later . . .And 2 hours later . . .
9:45 pm9:45 pm CT Pulmonary CT Pulmonary
angiogram showed angiogram showed right segmental and right segmental and subsegmental subsegmental pulmonary embolus pulmonary embolus in RUL. in RUL.

Initiate TreatmentInitiate Treatment
Diagnosis of PE is confirmed by CT-PADiagnosis of PE is confirmed by CT-PA
Try suggesting a treatment plan to your Try suggesting a treatment plan to your resident, consult references for helpresident, consult references for help
Start patient on heparin drip per protocol, Start patient on heparin drip per protocol, transition to warfarin once therapeutictransition to warfarin once therapeutic

Heparin Heparin IV InfusionIV InfusionOrdersOrdersExampleExample

Hot tip #4Hot tip #4Be an active learner and Be an active learner and educatoreducator
Read as much as possible about your Read as much as possible about your patient’s diagnosis and treatment optionspatient’s diagnosis and treatment options
Come up with questions about your Come up with questions about your patient’s disease and bring in primary patient’s disease and bring in primary literature addressing those questions to literature addressing those questions to share with the teamshare with the team

Before going to sleepBefore going to sleep
Check in on patientCheck in on patient
Follow up additional labs/studiesFollow up additional labs/studies
Write up the H&PWrite up the H&P
Practice presentation! Don’t be afraid to Practice presentation! Don’t be afraid to practice with your residents . . .practice with your residents . . .

The Next MorningThe Next Morning Set your alarm so that Set your alarm so that
you wake up with time to:you wake up with time to: Freshen up (bring your Freshen up (bring your
toothbrush!)toothbrush!) Pre-roundPre-round Start progress notes for Start progress notes for
previously admitted previously admitted patients (if possible)patients (if possible)
Eat and hydrate (critical)Eat and hydrate (critical) Help your team with any Help your team with any
misc. choresmisc. chores

Hot tip # 5 - PreroundingHot tip # 5 - Prerounding Goal is to check in on patient and gather the Goal is to check in on patient and gather the
following informationfollowing information Overnight eventsOvernight events Current symptomsCurrent symptoms Recent vitals and trend for relevant vitalsRecent vitals and trend for relevant vitals Focused physical examFocused physical exam Current labs and study results from overnightCurrent labs and study results from overnight
Come up with a one line assessment and Come up with a one line assessment and preliminary planpreliminary plan
Leave plenty of time in your morning schedule Leave plenty of time in your morning schedule for these tasks!for these tasks!
RoundsRounds
VIDEOVIDEO

Tips to be a stellar Tips to be a stellar studentstudent
Attitude is everythingAttitude is everything Be on timeBe on time Embrace new experiencesEmbrace new experiences Be okay with not knowing and not being Be okay with not knowing and not being
perfectperfect Don’t make excuses; Don’t complainDon’t make excuses; Don’t complain Laugh at yourselfLaugh at yourself Take care of yourselfTake care of yourself

That’s all folks . . . That’s all folks . . .
Have fun!Have fun!
Enjoy patient care!Enjoy patient care!
Don’t be afraid to ask for help!Don’t be afraid to ask for help!
Questions?Questions?

















