Presented in collaboration with Nebraska ICAP, Nebraska DHHS HAI Team, Nebraska Medicine, and The University of Nebraska Medical Center Moderated by Mounica Soma Panelists: Dr. Trevor Van Schooneveld Angie Vasa, RN, BSN Kate Tyner, RN, BSN, CIC Margaret Drake, MT(ASCP),CIC Teri Fitzgerald RN, BSN, CIC Dr. Ishrat Kamal-Ahmed Guidance and responses were provided based on information known on 6/2/2020 and may become out of date. Guidance is being updated rapidly, so users should look to CDC and jurisdictional guidance for updates.
Transcript
Presented in collaboration with Nebraska ICAP, Nebraska DHHS HAI Team, Nebraska Medicine, and
peripheral or posterior distribution, mainly in the lower lobes
• Progression GGO into multifocal consolidative opacities, septal thickening, and development of a crazy paving pattern
Salehi S, et al. AJR. 2020;215:1-7Simpson S, et al. Radiology: CT Imaging, 2020;2 https://doi.org/10.1148/ryct.2020200152
Testing Primer
• The sensitivity of a test means how well it can correctly identify those who have COVID-19 infection
• The specificity of a test means how well it can correctly identify those who do not have COVID-19 infection
• The positive predictive value of a test is the likelihood that a positive test result indicates that a person is truly positive for COVID-19 infection.
• The negative predictive value of a test is the likelihood that a negative test result indicates that a person is truly negative for COVID-19 infection.
Tests Available
• Molecular Tests (PCR, NAAT)• Amplify RNA of the virus• Use Case = Diagnosis of acute infection
• Antigen Tests• Detect viral antigens• Don’t amplify• Use Case = Rapid diagnosis of acute infection
• Serology• Detect antibodies made by the immune system• Detected after acute infection develops• Use Case = defining previous infection, population prevalence
• Culture • Grow the virus• Slow and not widely available• Use Case = Defining infectivity period
Serology
• What we know• Robust and rapid serologic response of IgM,
IgA and IgG
• IgM rises within 5-7 days symptom onset
• Seropositivity at 14 days: IgM (88-94%), IgG (94-100%)
• Is a positive serology protective against subsequent infection and for how long?
Who to Test
• All persons with symptoms suspicious for COVID-19
• Previously testing was prioritized due to limited capacity• Patients being hospitalized• Healthcare workers and those who work in healthcare environments• Ambulatory patients at increased risk for poor outcomes or who work in high risk
environments• Older adults (age ≥ 65 years) • Those who are immunocompromised or have chronic medical conditions (e.g., diabetes,
chronic lung, heart, or kidney disease)• Long-term care facility residents or those who reside in other group settings (homeless
shelter, group home, etc.)• Public safety workers and first responders • Persons performing duties or administering care in settings where spread of COVID19 would
be particularly disadvantageous: group homes, prisons, assisted living facilities, long term care, etc.
TEST
Testing Asymptomatic Persons• Molecular tests
• Pre-organ transplant, bone marrow transplant• Not generally recommended outside of outbreak investigation
• LTCF, group settings, etc.• Being done widely…
• Admission screening• Likely low yield and potentially inaccurate in low prevalence settings
• Pre-procedural• Much debate, yield very low (false +?), potentially to preserve PPE
• Post-exposure testing not generally recommended• When and how often?• A negative doesn’t rule out subsequent development of disease
• Serology • May be a role• Define population prevalence, determine retrospectively if infected, monitor
healthcare workers, determine incidence of asymptomatic infection
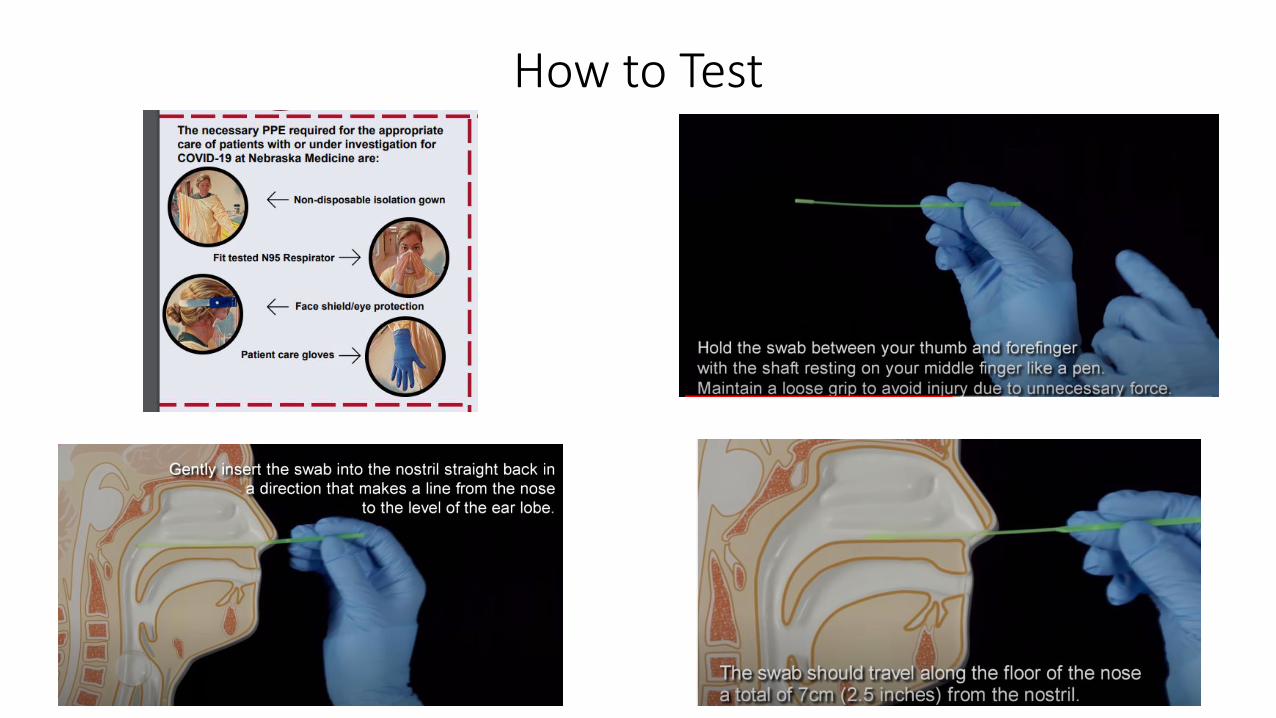
How to Test
Rapid Testing
• CLIA waived tests
• Results in 5-15 minutes
• Molecular
• Antigen and serologic coming
• Performance parameters undefined
• Reports of decreased sensitivity• Useful early in infection
• Good for ruling in, less so for ruling out
• Urgent care, ED, clinic??
Molecular Tests in Use at NM
• Numerous platforms available
• Nebraska Medicine currently using the following (TAT <18 hours)• Roche Cobas 6800 (COV19)• Laboratory developed test (NECoV19) • Regional Lab using a third platform
• NPHL using the CDC designed assay• Increasing capacity and batching
• Slight variations in how results are reported based on targets• Understand what is being reported at your facility
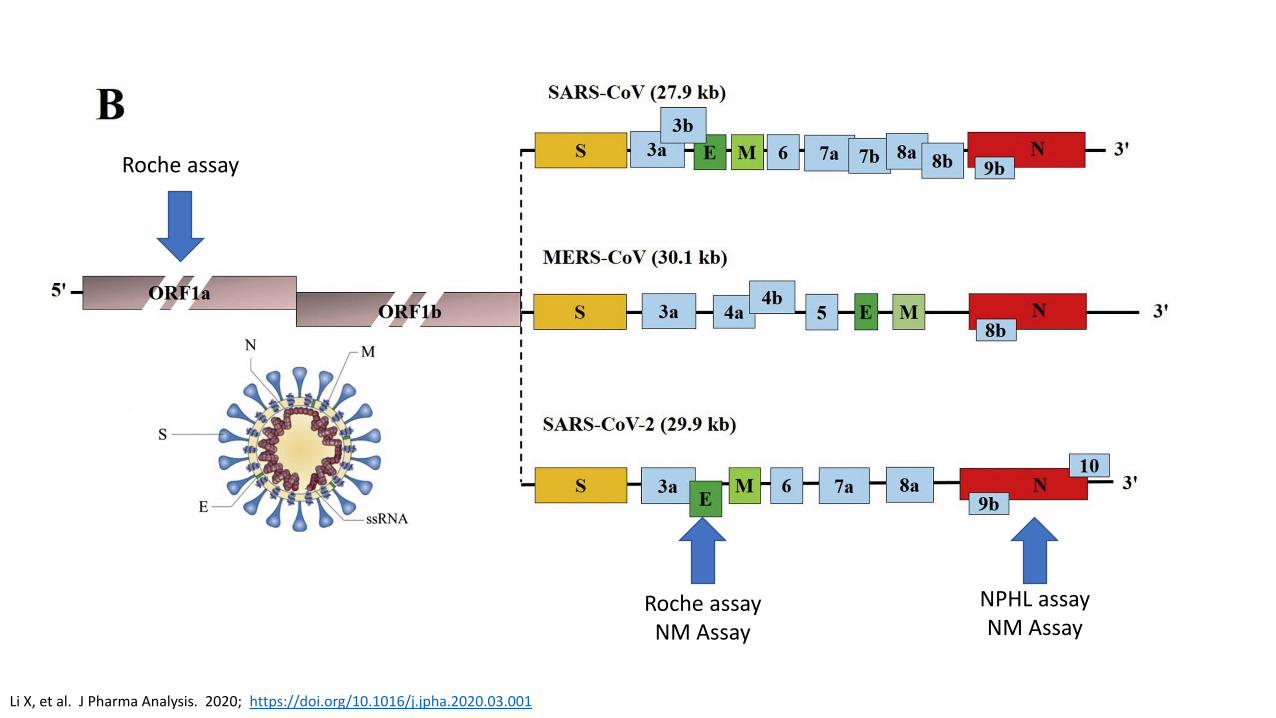
• Roche (E- and ORF1a-)• E- and ORF1a- not detected = COVID Not Detected• E- and ORF1a- detected = COVID Detected• Only E- detected = Presumptive positive
• E- is same in SARS-CoV-1 but this virus is not circulating• Invalid – test didn’t work Repeat swab
• NE COV Test (E- and N-)• E- not detected = Not Detected• E- detected Will be retested on next run for both E- and N-
• If either detected = COVID Detected• If neither detected = Inconclusive Repeat swab
Should I Get Two Tests in Symptomatic Person
• Depends on how well you did the swab
• Depends on the assay
• Depends on where you are in the illness course
• Early in the illness upper airway viral levels are very high but begin to decline after 7 days
• Numerous reports of patients presenting with typical symptoms and especially pneumonia and having a negative initial NP but then a second NP or lower respiratory tract specimen being positive
How good is the test?
Does our experience help us?
Inpatient Repeat Testing
• Reviewed all inpatient repeat testing 3/10/20-4/21/20 where initial result was negative or inconclusive• Utilized both Roche and NM assay
• Primarily NP• 99% first test, 94% second, 74% third
Characteristic Results (N=226)
Median Age (range) 60 (1-94)
Male 57%
Median Time Between 1st
and 2nd Test and 2nd and 3rd Test (days)
1.0, 2.9
Time from Symptom Onset to First Test
1-7 days 73%
8-14 days 12%
>14 days 2%
Asymptomatic Screening 13%
Negative Inconclusive Positive1st TestN=226
93% (209) 7% (17) 0% (0)
2nd TestN=226
98.5% (223) 1% (2) 0.5% (1)
3rd TestN=33
97% (32) 0% (0) 3% (1)
Our Recommendation on Second Test
• Outpatient repeat testing not usually indicated unless change in status (worsened, admitted, etc.)
• Inpatients are in a higher risk environment• Patients who have recently developed symptoms (7 days) usually can be ruled
out with one test• Implemented algorithm for determining who can be ruled out with one test
• Those who have a high-risk clinical presentation (typical symptoms, classic CT findings, known exposure, etc.), high risk exposure, or evidence of pneumonia should generally have a second test obtained• Preferably from lower respiratory tract if possible
Testing and Duration of Isolation
• Symptom-based vs. Test-based
• Symptom-based • Can exit isolation when symptoms resolve/improve• CDC = can exit isolation 10 days after symptom onset and 3 days after symptoms
subsidence (no fever, other symptoms improving)• Outpatient we are using 10 + 5 and immunocompromised 14 + 7
• Test-based• Require 2 tests done at least 24 hours apart to be negative• Inpatient we are using test-based strategy
• Evidence of prolonged viral RNA shedding (days to weeks)• Is this infectious virus???
Testing and Duration of Isolation• Emerging evidence that viral shedding ceases around day
10 after symptom onset• Detection of viral RNA vs. Detection of viable virus
• COVID19 patients who exited isolation based on symptoms and subsequently tested positive (N=285). • 108 underwent viral culture and no viable virus was detected• 790 contacts of were traced with zero confirmed transmissions.
• 73 COVID-19 positive patients, viable virus could not be isolated or cultured after day 11 of illness.
Viral Culture Detection After Symptom Onset
Wölfel, R. et al. Nature https://doi.org/10.1038/s41586-020-2196-x (2020).https://www.cdc.gov/coronavirus/2019-ncov/community/strategy-discontinue-isolation.htmlhttps://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030https://www.ams.edu.sg/view-pdf.aspx?file=media%5c5556_fi_331.pdf&ofile=Period+of+Infectivity+Position+Statement+(final)+23-5-20+(logos).pdf
UnknownsImmunocompromisedElderly
“Virus has not been successfully cultured more than 9 days after onset of illness. The statistically estimated likelihood of recovering
replication-competent virus approaches zero by 10 days”
Questions and Answer SessionUse the QA box in the webinar platform to type a question. Questions will be read aloud by the moderator, in the order they are received
A transcript of the discussion will be made available on the ICAP website
Dr. Trevor Van Schooneveld
Kate Tyner, RN, BSN, CIC
Margaret Drake, MT(ASCP),CIC
Teri Fitzgerald RN, BSN, CIC
Angie Vasa, RN, BSN
Dr. Ishrat Kamal-Ahmed
Moderated by Mounica Soma, MHA https://icap.nebraskamed.com/resources/