Preventing Falls in Older Adults: State of the Science Preventing Falls in Older Adults: State of the Science Laurence Rubenstein, MD, MPH Greater Los Angeles VA GRECC Professor of Medicine, UCLA British Columbia Injury Prevention Conference November 19-20, 2008
Transcript
Preventing Falls in Older Adults: State of the Science
Preventing Falls in Older Adults: State of the Science
Laurence Rubenstein, MD, MPHGreater Los Angeles VA GRECC
Professor of Medicine, UCLA
British Columbia Injury Prevention ConferenceNovember 19-20, 2008
Studies & meta-analysesAGS/BGS practice guidelines--update
Famous Fallers
Case ReportCase Report
78 year old gentlemanGood general healthGave a 1-hour graduation speech on October 20, 2004…
AP/Wide World Photos
What happened?What happened?
Broke left knee & right armNever fully recoveredCould his fall have been prevented?
Fall Incidence in Older Adults[rate/person/yr] or [rate/bed/yr]
Fall Incidence in Older Adults[rate/person/yr] or [rate/bed/yr]
Home Hospital Nsg Home
Any fall .3 1.5 1.7
Severe fall .03(10%) .3 .35(20%)
Fracture .01 .05 .07
Hip fx .003 .02
Rubenstein LZ, Josephson KR. Clin Geriatr Med. 2002(May);18(2):141-158
Falls MortalityFalls Mortality
Accidents: the 5th leading cause of death in older adultsDeaths from falls: 2/3 of accidental deaths72% of U.S. fall-related deaths occur in the 13% of population age 65+
Rubenstein LZ, Josephson KR. Clin Geriatr Med. 2002(May);18(2):141-158
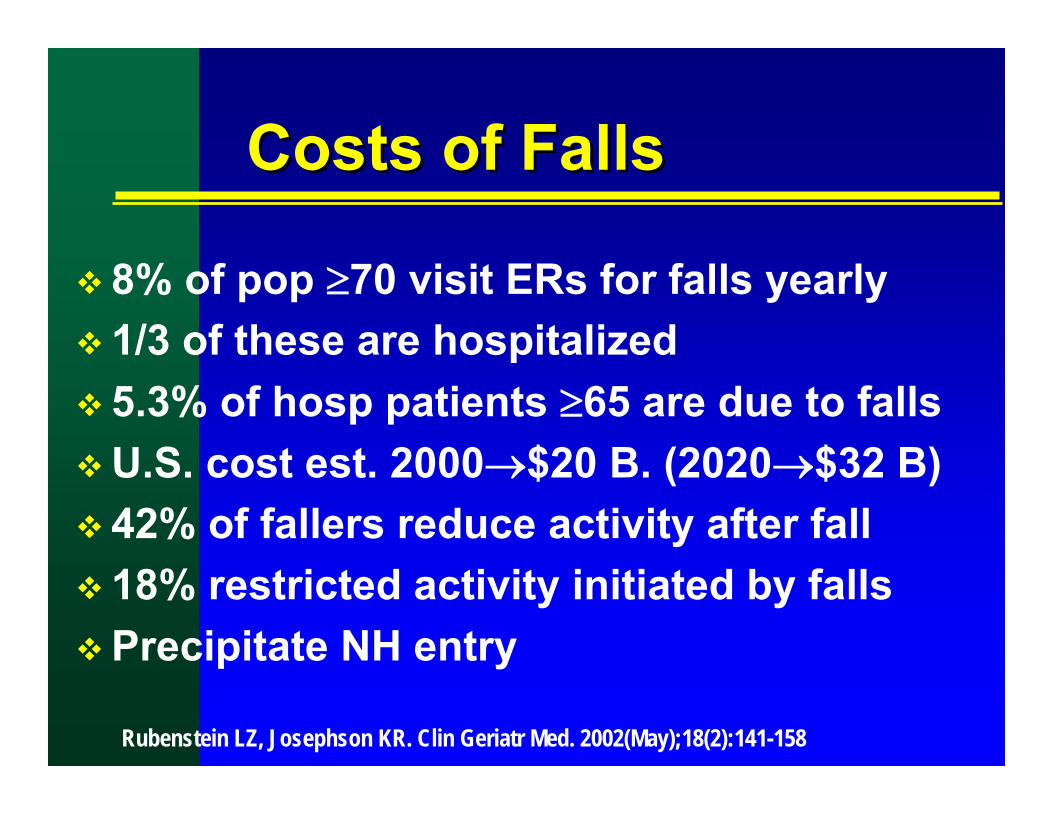
Costs of FallsCosts of Falls
8% of pop ≥70 visit ERs for falls yearly 1/3 of these are hospitalized5.3% of hosp patients ≥65 are due to fallsU.S. cost est. 2000→$20 B. (2020→$32 B)42% of fallers reduce activity after fall18% restricted activity initiated by fallsPrecipitate NH entry
Rubenstein LZ, Josephson KR. Clin Geriatr Med. 2002(May);18(2):141-158
Falls are #1 cause of NH litigation
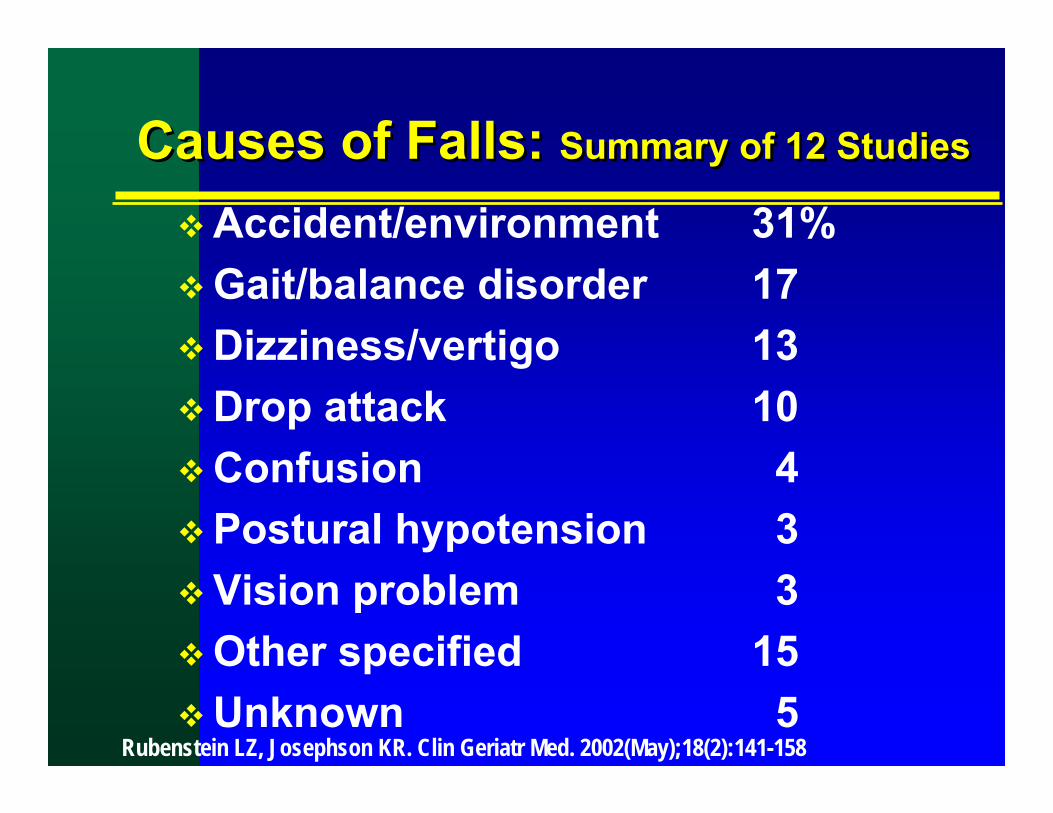
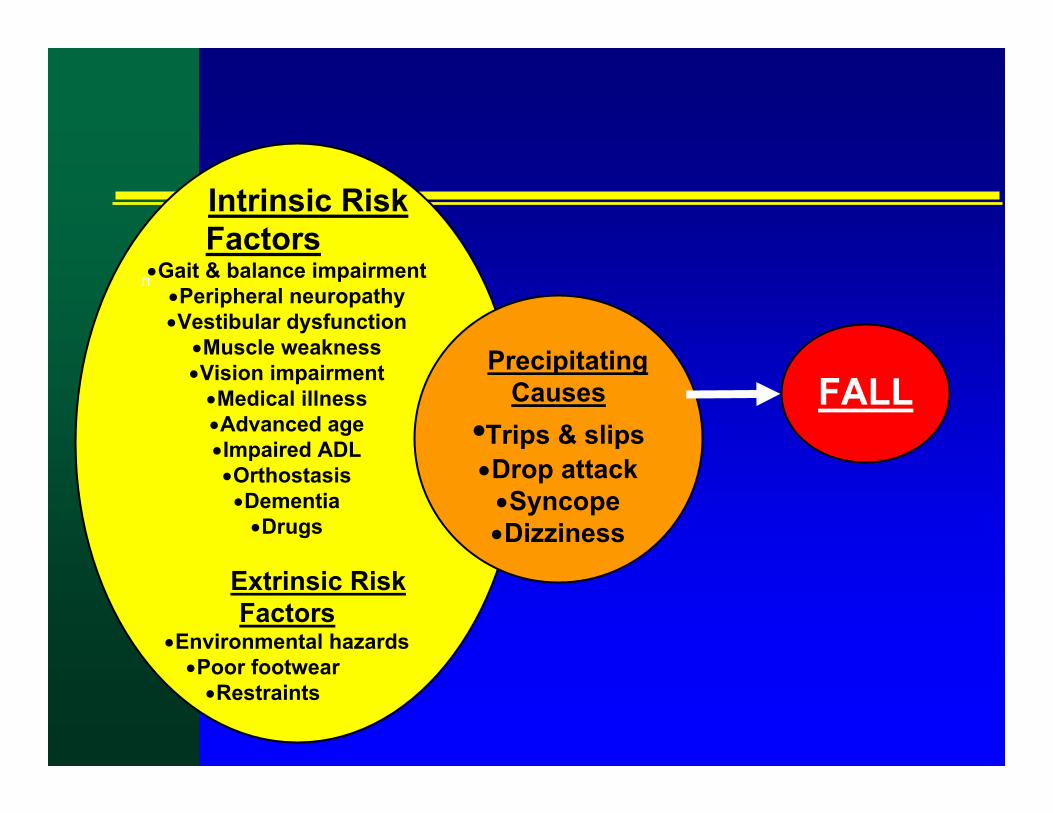
Causes of Falls: Summary of 12 StudiesCauses of Falls: Summary of 12 Studies
Most can accurately identify patients at higher risk of fallsProbably helpful to sensitize community living elders of their fall risk & what to doImportant for medico-legal purposes in hospitals & NHs: You need to show you’re doing something that is organized and current.
But …virtually all patients in hospital and NHs come out as “high risk.”
Fall Prevention: Growth of RCTsFall Prevention: Growth of RCTs
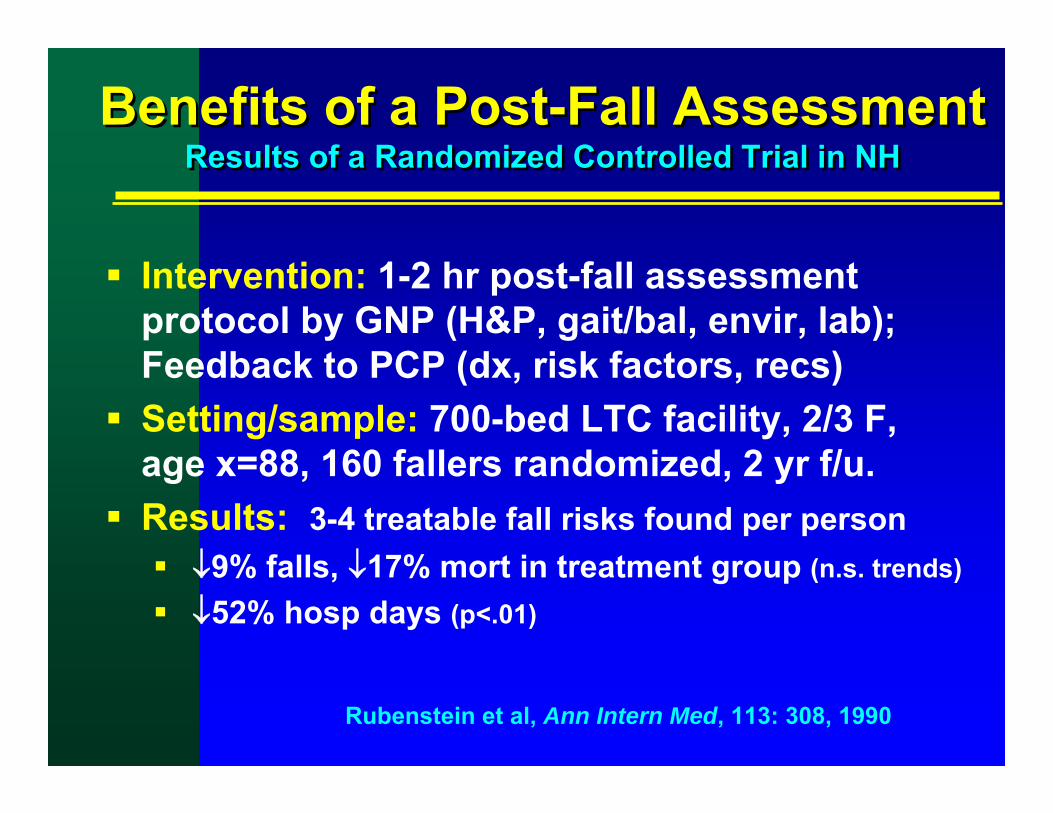
Benefits of a Post-Fall AssessmentResults of a Randomized Controlled Trial in NH
Benefits of a Post-Fall AssessmentResults of a Randomized Controlled Trial in NH
Intervention: 1-2 hr post-fall assessment protocol by GNP (H&P, gait/bal, envir, lab); Feedback to PCP (dx, risk factors, recs)Setting/sample: 700-bed LTC facility, 2/3 F,age x=88, 160 fallers randomized, 2 yr f/u.Results: 3-4 treatable fall risks found per person
↓9% falls, ↓17% mort in treatment group (n.s. trends)↓52% hosp days (p<.01)
Rubenstein et al, Ann Intern Med, 113: 308, 1990
Prevention of Falls in the Elderly Trial (PROFET)
Prevention of Falls in the Elderly Trial (PROFET)
Randomized trial of post-fall assessment of fallers seen in ED & assessed by 7 days.
N=397, ≥65 (mean age 78); LondonAssessment revealed many causes and risk factors and generated many referrals. 12-month follow-up: Intervention group had reduced risk of falls (OR=.39) & hospital admissions (OR=.61). Controls had greater decline in function.
Close J, Ellis M, Hooper R, et al. Lancet. 1999(Jan 9);353(9147):93-97
Clinical Approach to the Faller Clinical Approach to the Faller
Assess & treat any injuryDetermine likely precipitating cause(s)
“Falls History”“Falls History”Circumstances & prodrome of fall
sudden LOC, sudden leg weakness, tripped/slipped/hazard, position change, head back, tight collar, cough/urination, palpitations/angina, dizziness/giddiness
Major medical problemsesp. cardiovascular, neurologic
Impaired central processing (eg, dementia, delirium, stroke, drugs)
The “Aging Home ”Often An Obstacle CourseThe “Aging Home ”
Often An Obstacle Course
Old & rickety furniture & appliancesUnsafe stairs with poor handrailsThrow rugs, frayed carpetsElectrical cords, objects on floorPoor lightingSub-optimal height of bed, toilet, chairsAccumulated clutter of a lifetime
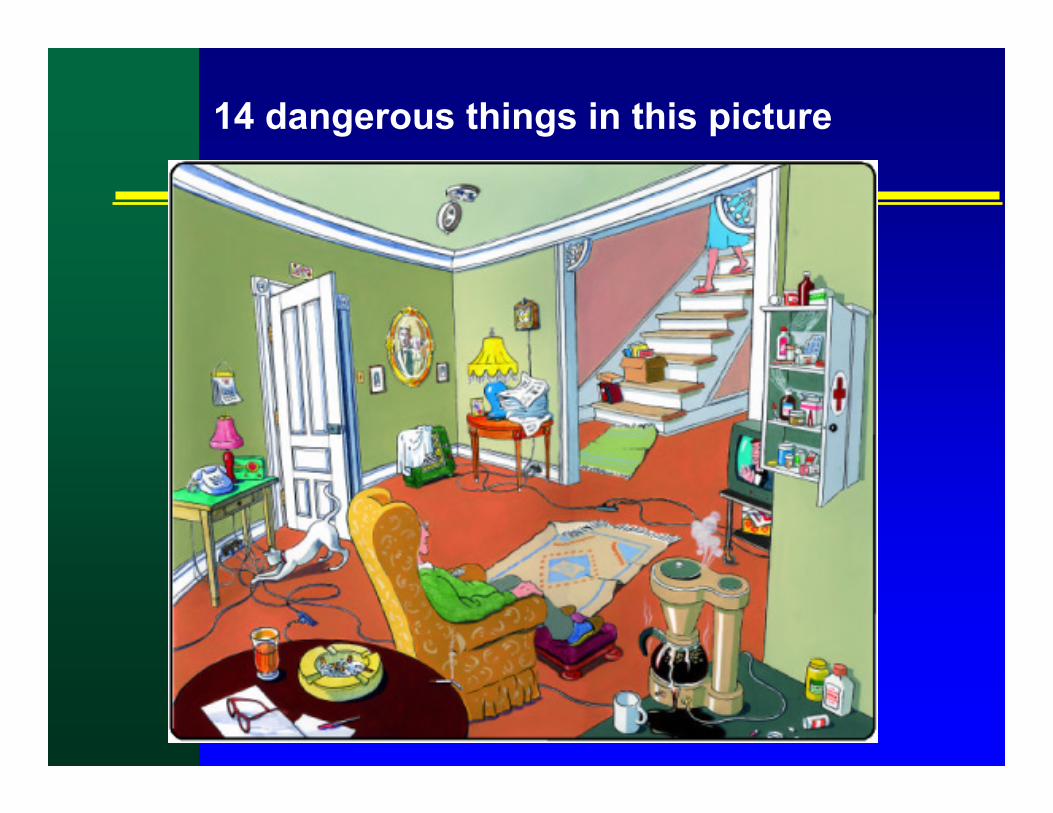
14 dangerous things in this picture
• Stairs without handrail• Deactivated fire alarm• Cloth on space heater• Overloaded outlets• Loose extension cords in pathways• Smoking. Cigarettes unattended• No automatic shut-off on coffee pot• Open bottles of medicine• Old medications in cabinet• Loose rugs• Flip-flop slippers• Clutter on staircase• Newspapers too close to lamp• No handle & no deadbolt on door
From Public Health Canada
The FICSIT Trials:Frailty & Injuries: Coop Studies of Intervention Techniques
The FICSIT Trials:Frailty & Injuries: Coop Studies of Intervention Techniques
7 independent randomized controlled trialsN: Total = 2328, Mean = 333, Range = 100-1323Sites: Atlanta, Boston, Farmington, New Haven, Portland, San Antonio, Seattle
Variety of interventions to reduce falls & frailty, all included exerciseExercise lasted 10-36 weeks, ≥2 year follow-upPooled effects on falls: .90 (95% CI, .81-.99) ▪ Effect for balance exercises: .83 (.70-.98)
Tai-chi group also signif better in: balance, physical performance & fear of falling
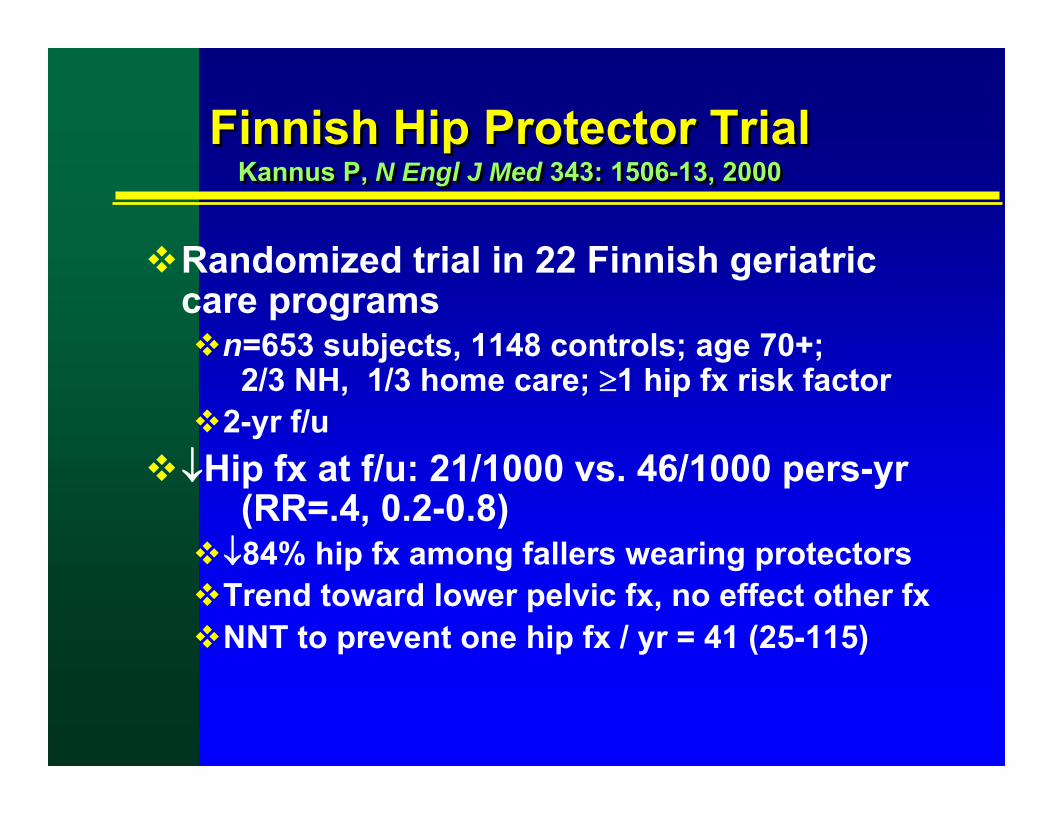
Finnish Hip Protector TrialKannus P, N Engl J Med 343: 1506-13, 2000
Finnish Hip Protector TrialKannus P, N Engl J Med 343: 1506-13, 2000
Randomized trial in 22 Finnish geriatric care programs
n=653 subjects, 1148 controls; age 70+; 2/3 NH, 1/3 home care; ≥1 hip fx risk factor
2-yr f/u↓Hip fx at f/u: 21/1000 vs. 46/1000 pers-yr
(RR=.4, 0.2-0.8)↓84% hip fx among fallers wearing protectors Trend toward lower pelvic fx, no effect other fxNNT to prevent one hip fx / yr = 41 (25-115)
Safehip
HipGuard
KPH
CuraMedica
Hip Protectors – Examples
HIPS
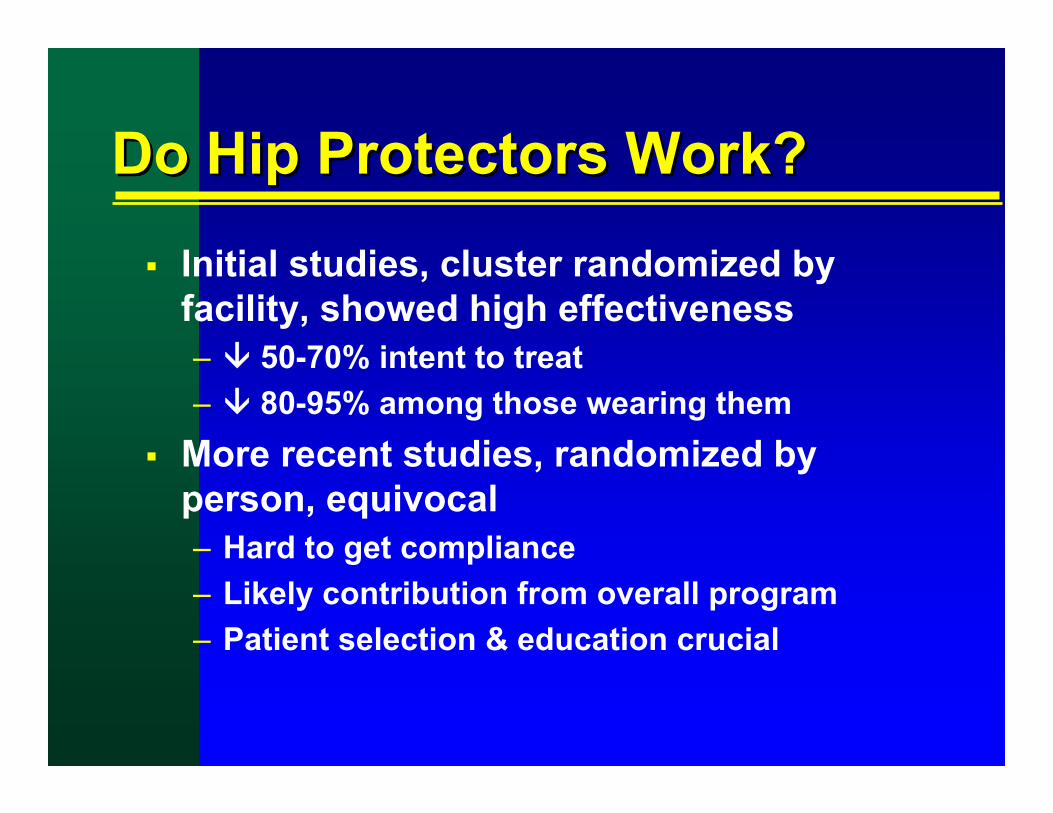
Do Hip Protectors Work?Do Hip Protectors Work?
Initial studies, cluster randomized by facility, showed high effectiveness– 50-70% intent to treat– 80-95% among those wearing them
More recent studies, randomized by person, equivocal– Hard to get compliance– Likely contribution from overall program– Patient selection & education crucial
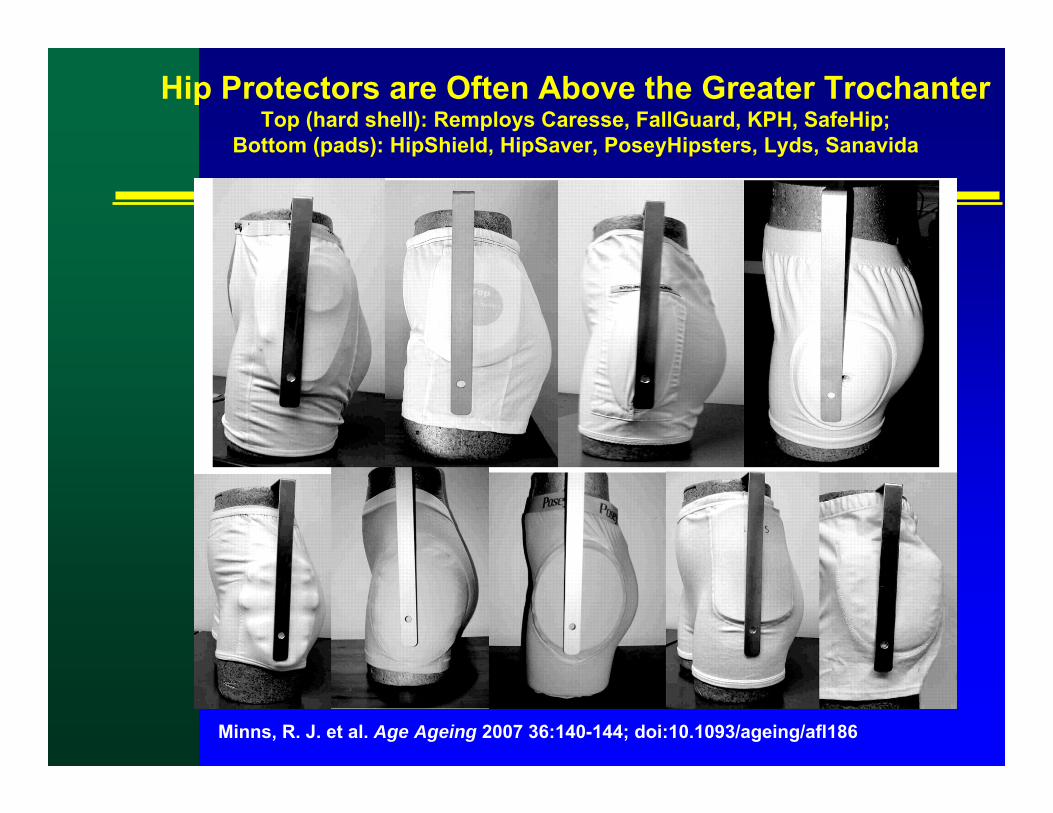
Minns, R. J. et al. Age Ageing 2007 36:140-144; doi:10.1093/ageing/afl186
Hip Protectors are Often Above the Greater TrochanterTop (hard shell): Remploys Caresse, FallGuard, KPH, SafeHip;
Vitamin D Effect on Falls: Meta-analysisBischoff-Ferrari JAMA 291:1999-06, 2004.
Vitamin D Effect on Falls: Meta-analysisBischoff-Ferrari JAMA 291:1999-06, 2004.
Pooled 5 RCTs, N=1237Vit D reduced OR for falls by 22% (Corrected OR 0.78; 95% CI 0.64-0.96)Effect independent of Ca+ supplement, duration of Rx, sexBaseline Vit D levels not measured
Can Cataract Surgery Reduce Falls? Harwood et al, Br J Ophthalmol 2005:89:53-9
Can Cataract Surgery Reduce Falls? Harwood et al, Br J Ophthalmol 2005:89:53-9
RCT of women age 70+ w/ cataracts randomized to surgery or 12-mo wait listFalls measured by diary + q3mo f/u12 mo results:
34% lower fall rate in surg group (p=.03)3% vs 8% had fractures (p=.03)Surg assoc w/ better activity, anxiety, depression, confidence & visual disability
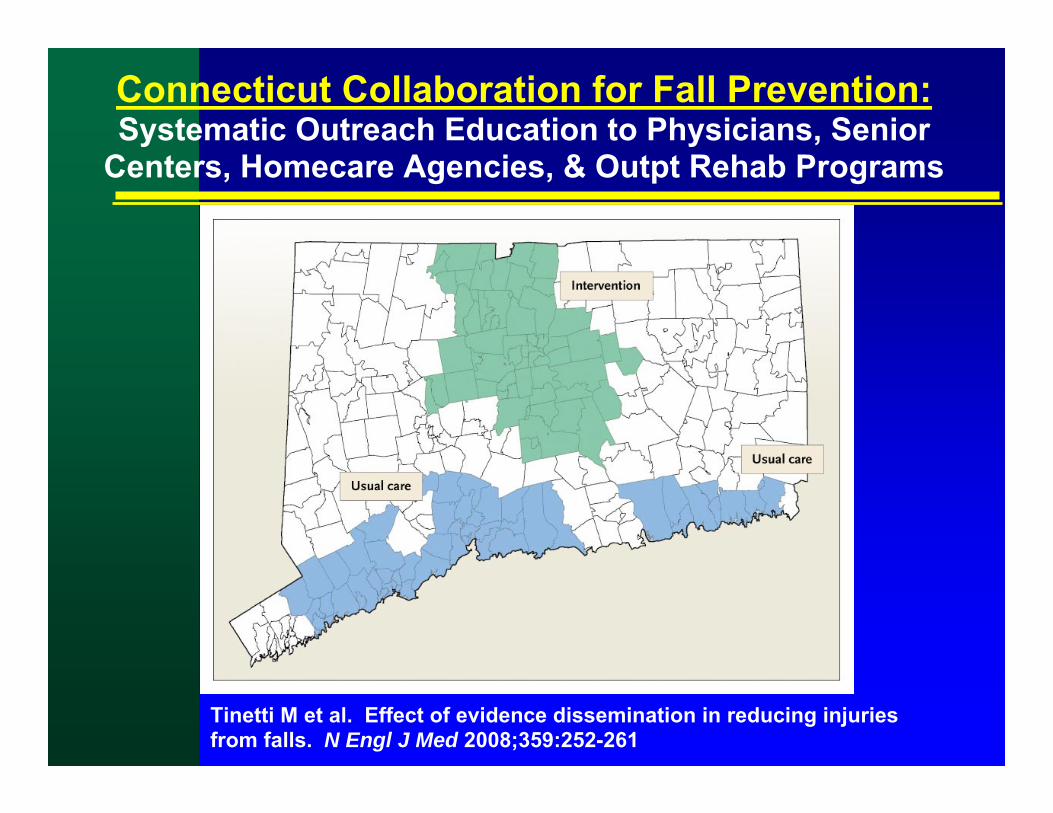
Tinetti M et al. Effect of evidence dissemination in reducing injuries from falls. N Engl J Med 2008;359:252-261
Connecticut Collaboration for Fall Prevention:Systematic Outreach Education to Physicians, Senior
Connecticut Collaboration: Adjusted Annual Rates of Serious Fall-Related Injuries and Use of Medical Services per 1000 Persons 70 Years of Age or
Older during the Preintervention, Intervention, and Evaluation Periods
The “Yaktrax” gait stabilizing device – RCT:• ↓58% RR outdoor falls on snow & ice (p<.03)• ↓87% RR injurious falls on snow & ice (p<.02)
• most intervention group falls occurred w/o device
McKiernan FE, JAGS 53:943, 2005
Vibrating Insoles may improve balancePriplata AA, et al. Vibrating insoles & balance in elderly people. Lancet 2003; 362:1123.
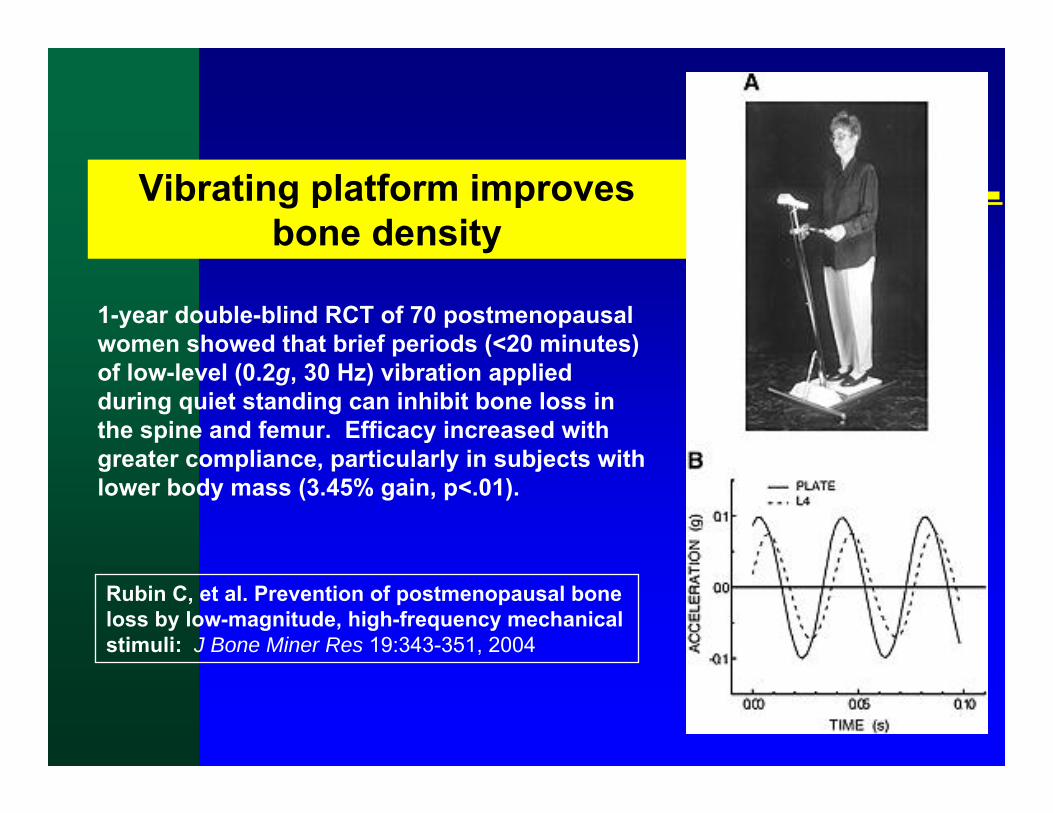
1-year double-blind RCT of 70 postmenopausal women showed that brief periods (<20 minutes) of low-level (0.2g, 30 Hz) vibration applied during quiet standing can inhibit bone loss in the spine and femur. Efficacy increased with greater compliance, particularly in subjects with lower body mass (3.45% gain, p<.01).
Rubin C, et al. Prevention of postmenopausal bone loss by low-magnitude, high-frequency mechanical stimuli: J Bone Miner Res 19:343-351, 2004
Vibrating platform improves bone density
Controlled whole body vibration to decrease fall risk in NH residents Bruyere, et al, Arch Phys Med Rehab 86:303,2005
Controlled whole body vibration to decrease fall risk in NH residents Bruyere, et al, Arch Phys Med Rehab 86:303,2005
Oliver, D. et al. BMJ 2007;334:82
Meta-analysis for multifaceted interventions in hospital--falls (random effects model)
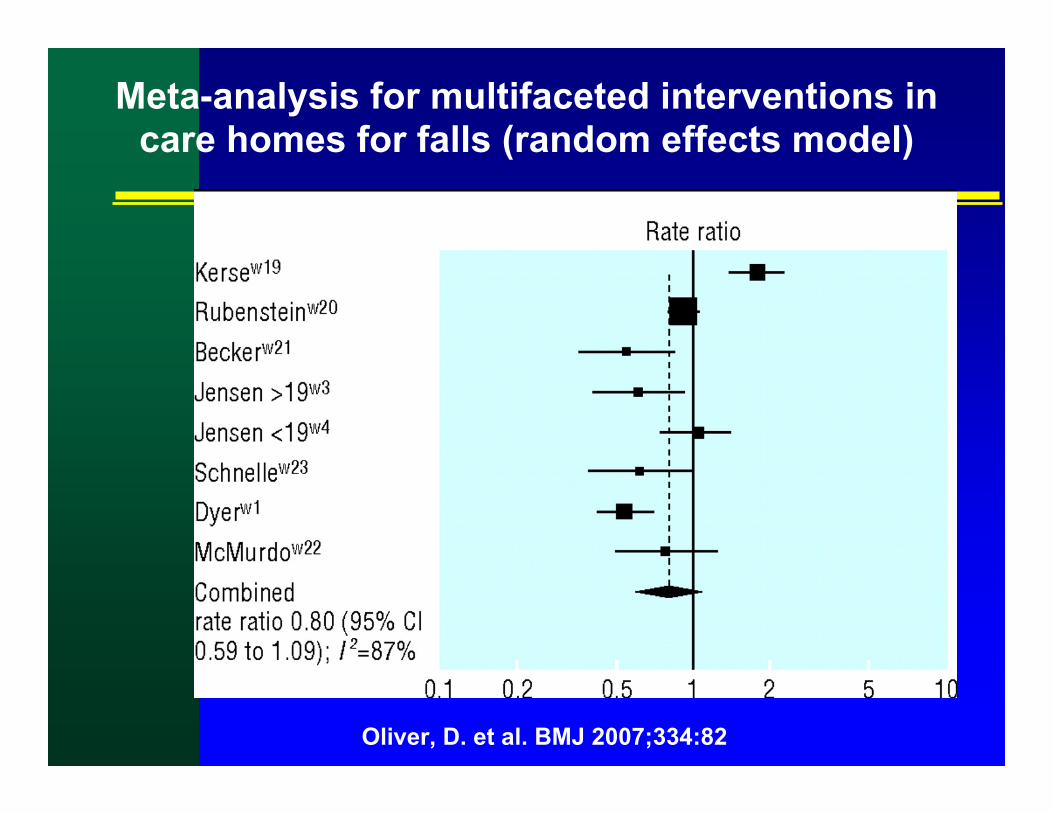
Oliver, D. et al. BMJ 2007;334:82
Meta-analysis for multifaceted interventions in care homes for falls (random effects model)
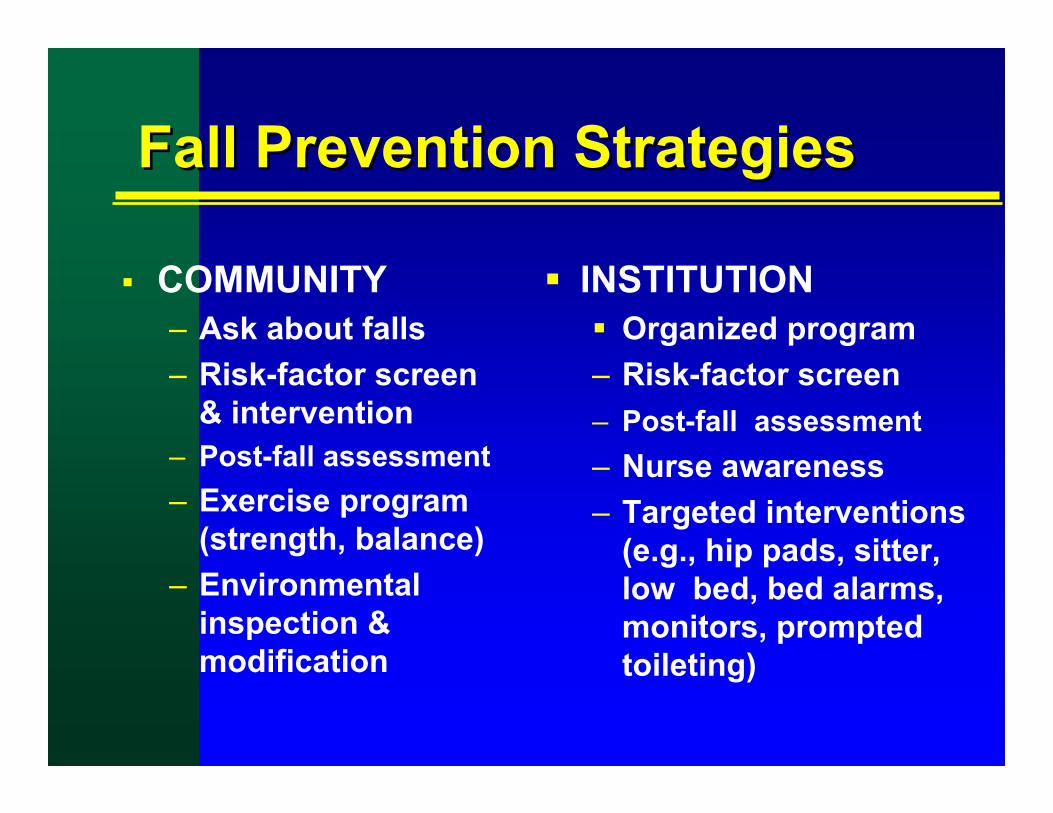
Fall Prevention StrategiesFall Prevention Strategies
COMMUNITY– Ask about falls– Risk-factor screen
& intervention– Post-fall assessment– Exercise program
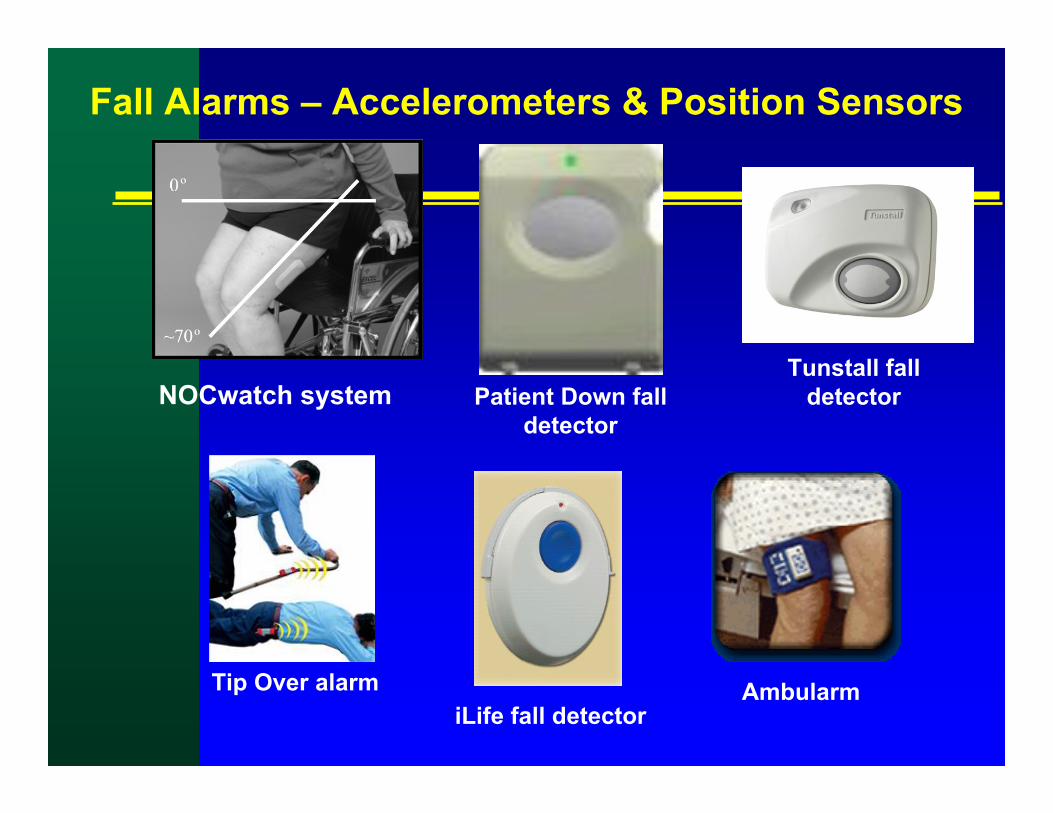
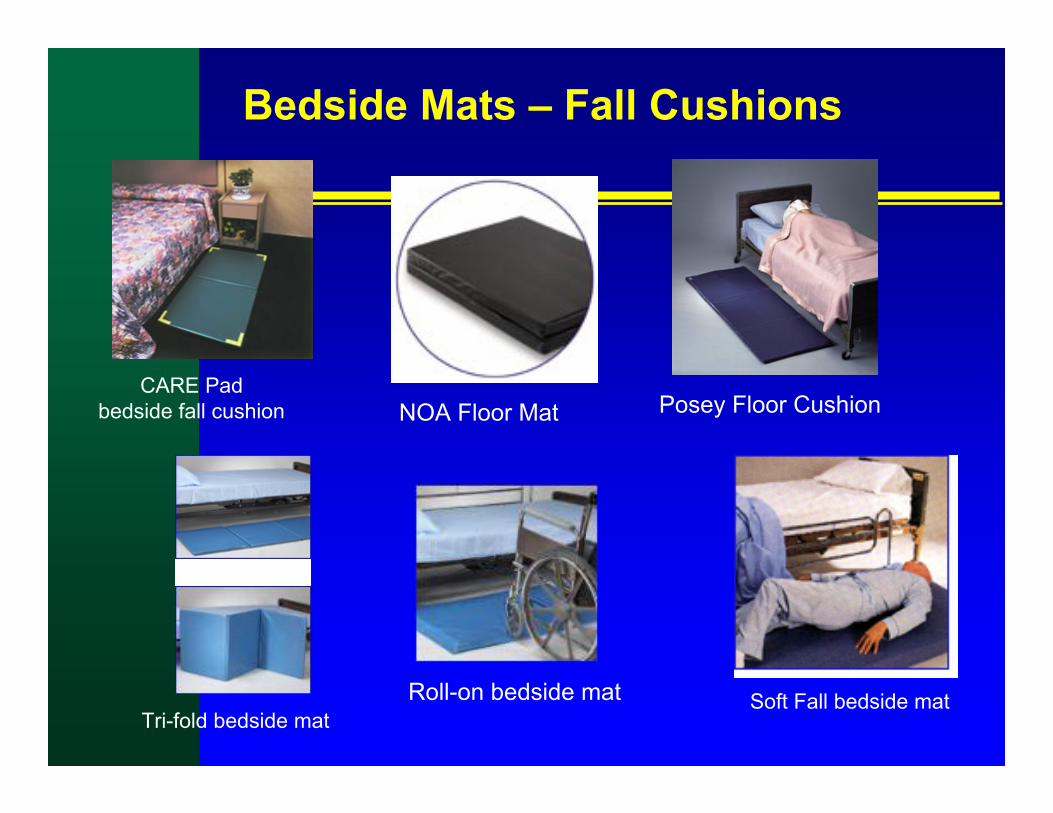
(e.g., hip pads, sitter, low bed, bed alarms, monitors, prompted toileting)
Evidence Based Guideline for Fall Prevention (AGS-BGS-AAOS Task Force, 2001) SUMMARY
Evidence Based Guideline for Fall Prevention (AGS-BGS-AAOS Task Force, 2001) SUMMARY
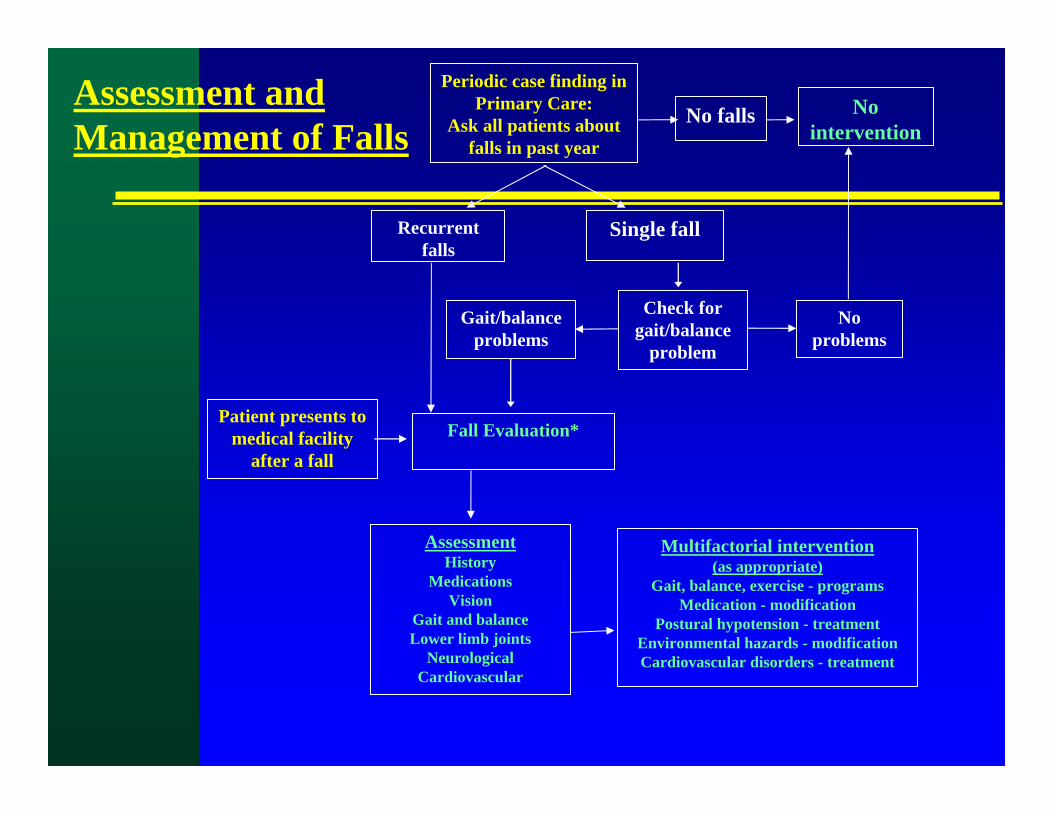
Assessment– Inquire about falls, gait, balance at routine visits (at least annually).– Screen persons reporting a problem (e.g., “get up & go” test).– Assess persons failing screen, or w/ >1 fall:
Hx of fall circumstances, meds, chronic illness, mobility levelExamine gait, balance, orthostasis, vision, neuro, cardiovascular
Management of Fallers– Multi-component interventions: assessment & f/u, exercise, gait