40
Preventing Injury from Falls and Immobility STARTER PACK WEBINAR #1
Preventing Injury from Falls and ImmobilitySTARTER PACK WEBINAR #1
Welcome to the Starter Pack• Webinar #1 –
– Why this is important – Establishing a Team– Best practices– Understanding the Measures– Completing a gap analysis– First Steps
• Gap Analysis Tool• Webinar #2
– How to prioritize the identified gaps – Using science of improvement concepts– How to create a good action plan
• Action Plan
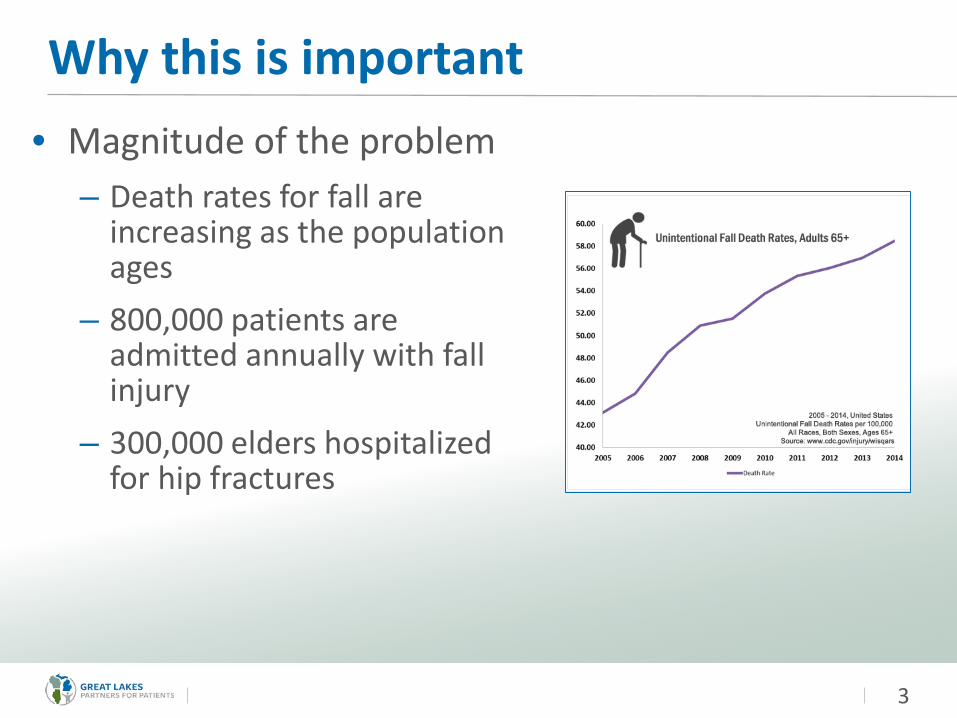
Why this is important• Magnitude of the problem
– Death rates for fall are increasing as the population ages
– 800,000 patients are admitted annually with fall injury
– 300,000 elders hospitalized for hip fractures
3
Why this is important• Inpatient Falls - US
– One of the most common incidents reported in hospitals– 3-20% of patients fall at least once– 700,000-1,000,000 patients fall in US hospitals a year– Agency for Healthcare Research and Quality. (January 2013). “Preventing Falls in
Hospitals: A Toolkit for Improving Quality of Care.” http://www.ahrq.gov/professionals/systems/hospital/fallpxtoolkit/fallpxtoolkit.pdf
• Costs - US– Avg cost of one fall without serious injury $3,500– Avg cost of two falls without serious injury $16,500– Avg cost of a fall with serious injury $27,000– $34 Billion US dollars spent annually– Wu S, , Keeler E, Rubenstein L, Maglione MS, Shekelle, PG 2010 A Cost
effectiveness analysis of a proposed national falls prevention program , Clinical Geriatric Medicine. 26, 751-766
4
Beyond monetary cost
5
• Even with out injury: fear of falling– Reduced mobility– Loss of functional independence
• Even without serious injury– Increased length of stay– Decreased ambulation, new walking
dependence• Consequences of Injury
– Loss of independence– Institutionalization– Death
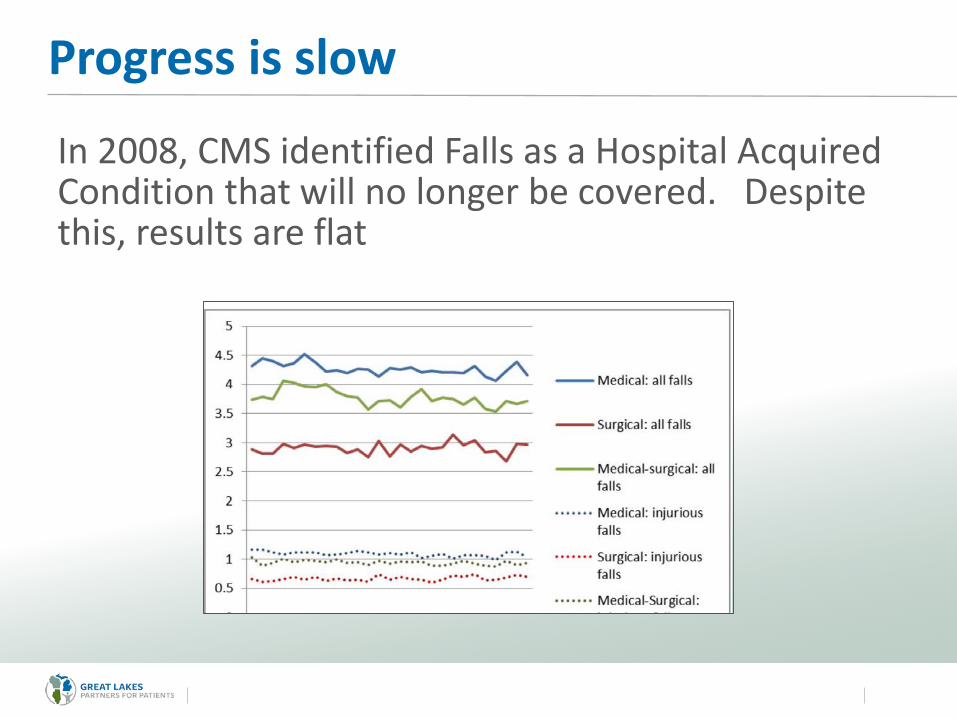
Progress is slow
In 2008, CMS identified Falls as a Hospital Acquired Condition that will no longer be covered. Despite this, results are flat
The HIIN Bold Aim
Reduction in Injuries from Falls
in 3 years
16 HIINs working towards this Aim!
7
What BOLD Action is Necessary?
8
Build structures to achieve the aim
GOAL FirstSTRUCTURE Second
First Things First
9
• Are we ready?• Is there urgency?• Is there leadership
support?• Who owns this effort?• What resources are
needed?• What if we are not
ready for full-scale change?
Assess the readiness before you proceed
Establishing the Team“Doing more with many”
Key Components Successful improvement relies on effective teams
Key Disciplines – Nurse– Physician– Rehab– Pharmacist – Quality– Case Management– Who else?
Key Roles
11
• Project Champion – a senior leader who will provide support, remove barriers
• Team Leader – a person with authority to make changes
• Team members – front line staff that do the work
Ready, Set Go
12
Best Practices
Survey YOUR Landscape• Review your BIG data
for trends– Time of day– Location– Activity– Assisted– Hospital units– Primary root cause
14
• Go to the GEMBA– Staff Interviews– Patient Interviews– Environmental Safety
Rounds
Learn from Falls
• Conduct a post fall huddle with the patient within one hour. – Quickly assess for slipping or tripping hazards
– Review circumstances while memories are fresh
– Use an interdisciplinary response team – leadership, pharmacy, rehab, physician
– Drill down on unassisted falls as a system failure
• Share fall event circumstances across units and in regular safety briefings.
15
Examine your “go to” practices Are you getting the results you want?
Evidence says…• Sitters• Signage• Alarms
Don’t Work
16
Quigley, P. (2015, Nov)Evidence levels: Applied to Select Fall and Fall Injury Prevention Practices. Rehabilitation Nursing. Retrieved at: http://onlinelibrary.wiley.com/doi/10.1002/rnj.253/full
What does work
• Interdisciplinary approach to assessment and care planning
• Managing and preventing delirium through medication management and progressive mobility
• Engaging patients and families through structured education
17
Screening or Assessing
Screening
• Check the box• Limits critical thinking• Score can change from
moment to moment
Assessing
• Review of circumstances of last fall• Review of medications• Physical examination• Mobility Assessment• Cognitive Assessment
18
Multidisciplinary Approach
Multifactorial Assessment
For High Risk / Older Patients • Gait, balance and mobility
assessment• Medication review• Cognitive assessment• Heart rate and rhythm• Postural hypotension• Feet and footwear• Home environmental hazards • American Geriatric Society Clinical
Practice Guideline: Prevention of Falls in Older Persons
Care Planning
Interventions to Address Risk• Minimize medications• Provide individually tailored exercise
program• Treat vision impairment (including
cataracts)• Mange postural hypotension• Manage heart rate and rhythm
abnormalities• Supplement vitamin D• Manage foot and footwear problems• Modify the home environment• Provide education and information
19
Assess for Injury Risk Certain patients are at a higher risk for injury if a fall occurs
ABCS of Injury Risk• A – Age > 85• B – Bones – Osteporosis, hx of fx, bone disease• C – Coagulation – On blood thinners• S – Surgery in current episode of care
Provide Optimal Post Fall Care• Protocols for assessment for injury post fall for
patients on blood thinners
20
Prevent and Manage Delirium in Older Adults
Medication Debridement• Use BEERs criteria to assess
medication regime for high / risk or vulnerable patients – Upon Admission
– Post Fall
• Remove sedatives / hypnotics from order sets
• Partner with caregivers in monitoring effects of medications
Mobility• Provide assistance for
regular ambulation• Provide adequate footwear• Gait belts in every room• Adaptive equipment
accessible to patients and staff
• Staff Mobility Training• Mobility Aid
21
Provide Structured Falls Education
• Educate about fall risks– Medications– Tripping hazards– Orthostatic hypotension, especially in morning– Footwear– Rolling equipment and furniture
• 45 Min Instruction + Designated Educator = Results
• Haines, T, Hill A, Hill K, McPhail S, Oliver D, BrauerS, Hoffman T Beer C. Mar 2011) Patient Education to Prevent Falls Among Older Hospitalized Inpatients: A Randomized Controlled Trial. Archives of Internal Medicine. 2011: 171(6) 516-524.
22
Maintain a Safe EnvironmentIt takes a village• No Pass Zone• Interdisciplinary Environmental
Safety Rounds• Clutter Rounds• Equipment Safety Checks• Bathroom Safety Inspection for
Hazards– Path from bed to toilet– Grab bars & toilet frame– Toilet height– Height of toilet– High threshold in shower– Objects projecting into
surrounding space
23
Leadership and ALL Frontline Staff Working Together
Intentional Rounding / ToiletingWHY?• 45% of Falls related to
toileting• Improves patient
satisfaction• Improves staff efficiency
HOW? • Staff must own the work
flow• Test toileting scripts to
promote cooperation
Determine who should be at arms length
“Safety trumps privacy”
Resources that will help
• Medication Review Guidelines: American Geriatrics Society. 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults.Journal of the American Geriatrics Society. Retrieved at: http://onlinelibrary.wiley.com/doi/10.1111/jgs.13702/full
• ABCS Injury Risk Assessment Department of Veteran Affairs Falls Prevention Toolkit. Retrieved at: http://www.patientsafety.va.gov/professionals/onthejob/falls.asp
• CAPTURE Falls Project Website: Interdisciplinary teamwork, mobility and medication assessment tools, training videos on Mobility, Post Fall Huddle at the Bedside, Sample Forms. Retrieved at:http://www.unmc.edu/patient-safety/capturefalls/index.html
• Post Fall Protocols for Patients on Blood Thinners. Safe From Falls 3.0 Roadmap(2015) Minnesota Hospital Association. Retrieved at: http://www.mnhospitals.org/Portals/0/Documents/ptsafety/falls/SAFE%20from%20FALLS%203.0%20Roadmap.pdf
25
More Resources
• Sample Mulitfactorial Assessment and Care Plan. From NICE Guidelines, UK (2013)http://www3.hants.gov.uk/multifactorial_falls_risk_assessment1_scottish_care_homes_report.pdf
• Environmental Safety Recommendations: Creating a Safe Environment to Prevent Toileting –Related Falls(December 2014)MN Hospital Association Research Report. Retrieved at: http://www.mnhospitals.org/Portals/0/Documents/ptsafety/falls/CreatingASafeEnvironmenttoPreventToiletingRelatedFallsReport.pdf
• Environmental and Equipment Safety Checklist. VA National Center for Patient Safety Falls Tool kit. Checklist is found in the Falls Policy Link. Retrieved at: http://www.patientsafety.va.gov/professionals/onthejob/falls.asp
26
27
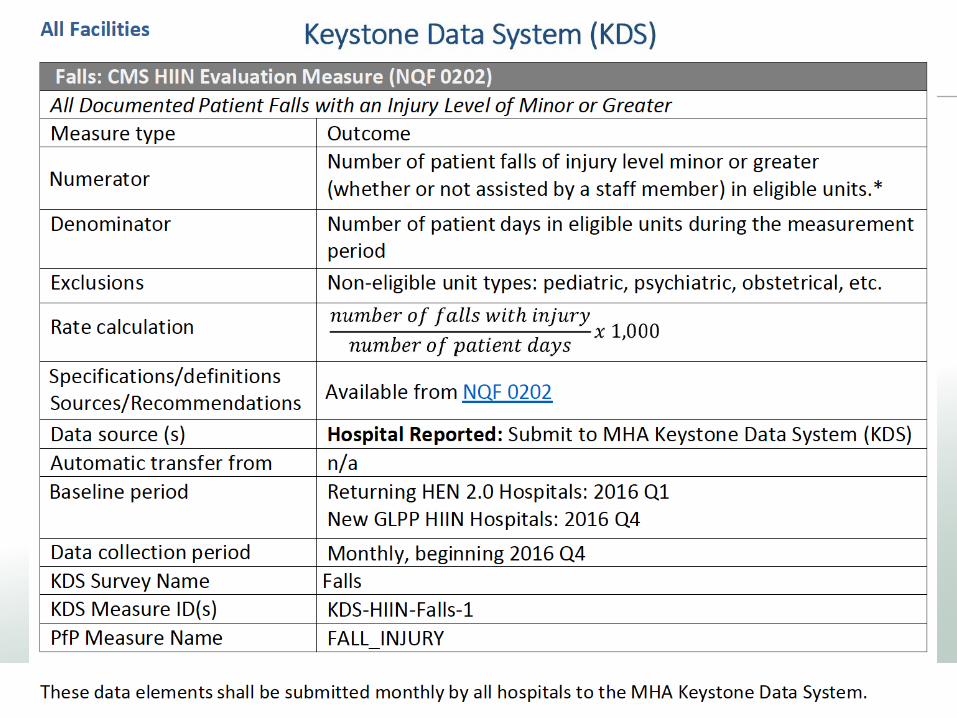
Understanding the Measure
Presentation Title Footer 29
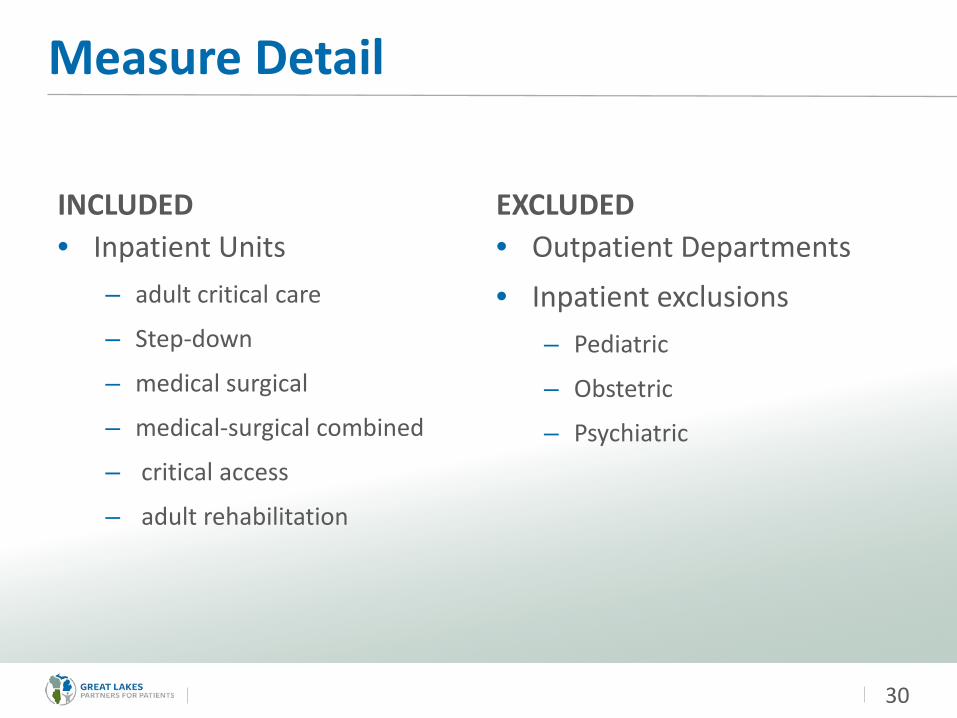
Measure Detail
INCLUDED• Inpatient Units
– adult critical care
– Step-down
– medical surgical
– medical-surgical combined
– critical access
– adult rehabilitation
EXCLUDED• Outpatient Departments• Inpatient exclusions
– Pediatric
– Obstetric
– Psychiatric
30
DATA CHALLENGES
• Catching up on lagging data• Comparisons
– HIIN Comparisons
• Benchmarks– Compare to self or compare to others?
31
Resources that can help
• NQF 0202 Measure Specifications. Includes NDNQI Benchmarks https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwiG0-T-iIbRAhUEQyYKHSqMCSkQFggaMAA&url=http%3A%2F%2Fwww.qualityforum.org%2FWorkArea%2Flinkit.aspx%3FLinkIdentifier%3Did%26ItemID%3D70964&usg=AFQjCNFdBcMh72uJ6RQ5GELbcxMsND68yg&bvm=bv.142059868,d.eWE
32
Next Steps:Complete a Gap AnalysisMake a Plan!
Where Are You Now?• Analyze your hospital’s current
state using the Gap Analysis Tool
Be honest – look at policy AND practiceReview 5 ChartsInterview 5 patientsInterview 5 staff
34
STARTHERE
Get Started
• Create a list of opportunities from Gap Analysis• Prioritize• Where do you want to go?• How do you decide?
35
Reflections
• How do you know where to start?– What do you already have?
– What can you build upon?
– Where is the energy?
• Start small, tapping into front line staff.
• Think BIG about structure and leadership.
36
Next Steps
• Perform your Gap Analysis• Access the resources provided - make notes and ask
questions• View Webinar #2
– How to engage and involve stakeholders– Learn about PDSA and Small Tests of Change
• Decide the next level of HIIN support– Onsite assistance– Improvement Action Network– Other
37
Tools that help build a foundation– AHRQ - An Evidence Based Handbook for Nurses. Retrieved at:
http://archive.ahrq.gov/professionals/clinicians-providers/resources/nursing/resources/nurseshdbk/
– Department of Veteran Affairs Falls Prevention Toolkit. Retrieved at: http://www.patientsafety.va.gov/professionals/onthejob/falls.asp
– Hospital Elder Life Program (HELP). Delirium assessment, prevention and management tools for clinicians and patients Retrieved at: http://www.hospitalelderlifeprogram.org/
– Transforming Care at the Bedside How-to Guide: Reducing Patient Injuries from Falls. Retrieved at: http://www.ihi.org/resources/Pages/Tools/TCABHowToGuideReducingPatientInjuriesfromFalls.aspx
– The American Geriatrics Society 2013 Clinical Practice Guidelines: Prevention of Falls in Older Adults Summary of Recommendation. Retrieved at: http://www.americangeriatrics.org/health_care_professionals/clinical_practice/clinical_guidelines_recommendations/prevention_of_falls_summary_of_recommendations
38
Tools that help build a foundation– Institute for Clinical Systems Improvement (ICSI) Prevention of Falls (Acute Care)
Protocol, April 2012. Retrieved at: https://www.icsi.org/_asset/dcn15z/Falls.pdf
– Falls in older people: assessing risk and prevention. National Institute for Health and Care Excellence (NICE) (2013) UK. Retrieved at: https://www.nice.org.uk/guidance/cg161
– CAPTURE Falls Toolkit. Interdisciplinary teamwork tools, post fall huddles, medication and mobility assessment tools. http://www.unmc.edu/patient-safety/capturefalls/index.html
– VA National Center for Patient Safety Falls Toolkit. Retrieved at: http://www.patientsafety.va.gov/professionals/onthejob/falls.asp
39

Thank you!

















