Occupational and Environmental Medicine 1997;54: 1-6 METHODOLOGY Series editors: T C Aw, A Cockcroft, R McNamee Preventive effectiveness of pre-employment medical assessments Wim de Kort, Frank van Dijk Abstract Objectives and methods-Health gain, prevention of health loss, and avoidance of financial risk all seem to be driving forces for the use of pre-employment medical assessment. An attempt is made to measure the effect of implementing the pre-employment medical assessment on these end points. The anticipated maxi- mum preventive effect (preventive effec- tiveness) of selection by means of pre-employment medical assessments for work related risks and the potential for disablement in individual workers can be calculated or estimated. Necessary para- meters include test validity characteris- tics and epidemiological data for both the adverse outcome to be prevented, and risk factors of concern. Results-The preventive effectiveness can be expressed as the effort (number of actions) needed to prevent one adverse event-for example, one case of occupa- tional disease or one case of long term disablement. Actions include: a pre- employment health assessment, rejection of the candidate, individual precautions, adjustments of the job, and adjustments of the job environment. It seems that the preventive effectiveness of many actions can be low, implying that large numbers of actions are needed to prevent one adverse outcome. Discussion-The medical assessment should consist of no more questions and tests than are required relevant to the stated aim. Particularly, when the pre- employment medical assessment is used to reject candidates at risk, the use of tests should be carefully weighted. If the pre- ventive effectiveness is considered to be too low, then the question or test should not be incorporated for selection pur- poses. The application of a so called "expert judgment" should be based on professional guidelines wherever possible and should be made clear. The benefit of reducing the incidence of a serious adverse event by one may outweigh the costs of rejecting many candidates. Conclusions-The concept of preventive effectiveness may help to reach evidence based occupational medicine, which starts at the pre-employment medical assessment. (Occup Environ Med 1997;54:1-6) Keywords: pre-employment health assessment; preven- tive effectiveness; risk avoidance To produce substantive policy in occupational medicine, it is necessary to gain insight into the quality aspects of the methods to be used.' An important one of these is the pre-employ- ment medical assessment. This assessment will, among other functions, be a means of personnel selection and as such it is essential that assessment is both sufficiently accurate and reliable. The contents of the pre-employ- ment medical assessment differ widely and may include a history (often taken by ques- tionnaire), a medical examination, and addi- tional (laboratory) tests. A pre-employment medical assessment may include all of these items extensively, or may merely consist of a simple self administered questionnaire. This article focuses on methodological aspects of such a screening process. More specifically, attention will be given to the anticipated maxi- mum preventive effect (preventive effective- ness) of selection by such medical assessments on work related health risks, risks to others, the potential for absenteeism, and disablement in individual workers. Pre-employment medical assessment The content and the relevance of pre-employ- ment medical assessment of fitness for work have held centre stage since the emphasis was placed on the possible contribution that such an assessment could make to the prevention of occupational disease, absence through sick- ness, and work disablement. The pre-employ- ment medical assessment is used to assess whether a candidate is sufficiently skilled to perform the job adequately from a medical point of view. Moreover, the pre-employment medical assessment presents an opportunity to ease the entrance to the work force for people with certain health risks, medical impairments, or handicaps. When the results of a pre- employment health examination show a lack of balance between job demands and antici- pated performance of the candidate, measures to lower risk can be taken. Such measures may be aimed at the candidate (rejection or not; individual precautionary adjustments), the job, or the job environment. However, health gain is not the only motivation for the use of pre-employment medical assessment. The involvement of the employer, the insurance companies, and pension funds with the grow- ing cost containment problems of sick leave Occupational Toxicology and Nutrition Division, TNO Nutrition and Food Research Institute, PO Box 360, NL-3700 AJ Zeist, The Netherlands W de Kort Coronel Institute, Academic Medical Centre, University of Amsterdam, The Netherlands F van Dijk Correspondence to: Professor F van Dijk, Coronel Institute, Academic Medical Centre, Meibergdreef 15, 1105 AZ Amsterdam, The Netherlands. Accepted 29 July 1996 I on February 20, 2022 by guest. Protected by copyright. http://oem.bmj.com/ Occup Environ Med: first published as 10.1136/oem.54.1.1 on 1 January 1997. Downloaded from
Transcript
Occupational and Environmental Medicine 1997;54: 1-6
METHODOLOGY Series editors: T C Aw, A Cockcroft, R McNamee
Preventive effectiveness of pre-employmentmedical assessments
Wim de Kort, Frank van Dijk
AbstractObjectives and methods-Health gain,prevention of health loss, and avoidanceof financial risk all seem to be drivingforces for the use of pre-employmentmedical assessment. An attempt is madeto measure the effect ofimplementing thepre-employment medical assessment onthese end points. The anticipated maxi-mum preventive effect (preventive effec-tiveness) of selection by means ofpre-employment medical assessments forwork related risks and the potential fordisablement in individual workers can becalculated or estimated. Necessary para-meters include test validity characteris-tics and epidemiological data for both theadverse outcome to be prevented, andrisk factors of concern.Results-The preventive effectiveness canbe expressed as the effort (number ofactions) needed to prevent one adverseevent-for example, one case of occupa-tional disease or one case of long termdisablement. Actions include: a pre-employment health assessment, rejectionof the candidate, individual precautions,adjustments of the job, and adjustmentsof the job environment. It seems that thepreventive effectiveness of many actionscan be low, implying that large numbersof actions are needed to prevent oneadverse outcome.Discussion-The medical assessmentshould consist of no more questions andtests than are required relevant to thestated aim. Particularly, when the pre-employment medical assessment is usedto reject candidates at risk, the use of testsshould be carefully weighted. If the pre-ventive effectiveness is considered to betoo low, then the question or test shouldnot be incorporated for selection pur-poses. The application of a so called"expert judgment" should be based onprofessional guidelines wherever possibleand should be made clear. The benefit ofreducing the incidence of a seriousadverse event by one may outweigh thecosts ofrejecting many candidates.Conclusions-The concept of preventiveeffectiveness may help to reach evidencebased occupational medicine, whichstarts at the pre-employment medicalassessment.
(Occup Environ Med 1997;54:1-6)
Keywords: pre-employment health assessment; preven-tive effectiveness; risk avoidance
To produce substantive policy in occupationalmedicine, it is necessary to gain insight intothe quality aspects of the methods to be used.'An important one of these is the pre-employ-ment medical assessment. This assessmentwill, among other functions, be a means ofpersonnel selection and as such it is essentialthat assessment is both sufficiently accurateand reliable. The contents of the pre-employ-ment medical assessment differ widely andmay include a history (often taken by ques-tionnaire), a medical examination, and addi-tional (laboratory) tests. A pre-employmentmedical assessment may include all of theseitems extensively, or may merely consist of asimple self administered questionnaire. Thisarticle focuses on methodological aspects ofsuch a screening process. More specifically,attention will be given to the anticipated maxi-mum preventive effect (preventive effective-ness) of selection by such medical assessmentson work related health risks, risks to others,the potential for absenteeism, and disablementin individual workers.
Pre-employment medical assessmentThe content and the relevance of pre-employ-ment medical assessment of fitness for workhave held centre stage since the emphasis wasplaced on the possible contribution that suchan assessment could make to the prevention ofoccupational disease, absence through sick-ness, and work disablement. The pre-employ-ment medical assessment is used to assesswhether a candidate is sufficiently skilled toperform the job adequately from a medicalpoint of view. Moreover, the pre-employmentmedical assessment presents an opportunity toease the entrance to the work force for peoplewith certain health risks, medical impairments,or handicaps. When the results of a pre-employment health examination show a lackof balance between job demands and antici-pated performance of the candidate, measuresto lower risk can be taken. Such measures maybe aimed at the candidate (rejection or not;individual precautionary adjustments), thejob, or the job environment. However, healthgain is not the only motivation for the use ofpre-employment medical assessment. Theinvolvement of the employer, the insurancecompanies, and pension funds with the grow-ing cost containment problems of sick leave
OccupationalToxicology andNutrition Division,TNO Nutrition andFood ResearchInstitute, PO Box 360,NL-3700 AJ Zeist, TheNetherlandsW de KortCoronel Institute,Academic MedicalCentre, University ofAmsterdam, TheNetherlandsF van DijkCorrespondence to:Professor F van Dijk,Coronel Institute, AcademicMedical Centre,Meibergdreef 15,1105 AZ Amsterdam,The Netherlands.Accepted 29 July 1996
I
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D
and work disablement has led to the notionthat pre-employment medical assessment canpresent a method of (financial) risk avoidance.A relevant factor in this setting is the exis-
tence in various countries of legislation-suchas, the Dutch "Arbeidsomstandighedenwet"(Working Environment Act)-which hasallowed pre-employment medical assessmentswhen certain work is to be performed. Despitethe general renunciation by numerous govern-mental and international bodies, includingprofessional associations, of a purely economi-cally based risk avoidance, the pre-employ-ment medical assessment is still commonlyused by many, including some of these inter-national bodies.3 The attention of the mediafocuses on disorders in which hereditary ten-dencies may play a part (with the help of socalled genetic screening) and checking aspir-ing employees for the use of alcohol or other(illicit) drugs and for possible infection byhuman immunodeficiency virus (HIV).
Codes ofpracticeWhen a person has a certain endogenous oracquired tendency, it may imply that in a par-ticular working environment he or she willperform less effectively than average, or willrun an above average risk of injury or detri-mental health effects-such as occupationaldisease, incapacity, or disablement. Such arisk can also denote risks for third parties. Inepidemiological terminology, such a person isspoken of as being susceptible, or having anindividual risk factor. The pre-employmentmedical assessment is a means of identificationand selection for a risk factor, but beforereaching a conclusion about this, severalaspects should be considered. In 1968, Wilsonand Jungner, in a World Health Organisationpublication, focused attention on the princi-ples on which the establishment of a screeningprogramme for the general population couldbe based.4 Employees of the National Institutefor Occupational Safety and Health have sug-gested ways of translating these into the fieldof occupational health care.5 This translationplaces a focus on specific characteristics of thepopulation of workers and on some less con-ventional possibilities for intervention. Inoccupational health, one does not alwaysimmediately speak of disease or disorder, butmuch more often of a risk factor in the form ofa tendency or of noticable non-pathologicalvariables. Also, the working environmentoffers conditions which are more readily andmore specifically open to intervention thanconditions in the general environment or athome.
Individual authors,68 textbooks,9-'l profes-sional organisations,"2 and governmental orinternational bodies,"-'7 do present well for-mulated advice or guidelines for medicalassessments, but only briefly refer to the gen-erally accepted principles already mentioned.They do not generally take into account, or doso only in passing, the limitations of the testsand the methods to be used. In particular, theactual or possible preventive effect of certain
pre-employment medical policies is not takeninto consideration. Yet, a discussion on limita-tions of medical testing is important, because alack of precision or absence of predictive valuemay leave too much room for personal inter-pretations, if not intentional or unintentional,discrimination.
Recently the Dutch "KoninklijkeNederlandse Maatschappij ter bevorderingvan de Geneeskunst" (Royal Dutch MedicalAssociation) has published a code of practicefor pre-employment medical assessment.'8The impetus for this protocol included aDutch Bill on pre-employment medical assess-ments, and research carried out in TheNetherlands. 19 20 This code of practice alsoonly contains generally formulated goals anddeals with procedural aspects. Briefly, it statesthat the pre-employment medical assessmentshould aim at judging the balance between theability of a certain candidate to sustain a workload and the presumed work load of the job inquestion. Conditionally, the pre-employmentmedical assessment must be performed: (a)before work is started; (b) on the one remainingcandidate; (c) by an independent sufficientlytrained physician; (d) if, and only if, there arejob demands which can be translated intomedical terms of reference; (e) if the contentsof the medical assessment (questions, physicalexamination, laboratory tests, etc) are relevantto the stated aim; and (f) while respectingphysical and psychological integrity of the can-didate's privacy. Also, the code of practicedeals with important other procedural aspects,such as those about exchange of information,the reporting of results, the access to docu-ments, the possibility of a re-examination,andthe procedure for dealing with complaints.
Preventive effectiveness ofapre-employment medical assessmentThe preventive effectiveness of a pre-employ-ment medical assessment can only be esti-mated with the validity characteristics of thetests to be used, and with the epidemiology ofthe risk factors of the effects of concern. Thus,the preventive effectiveness is expressed as theeffort-the number of actions-needed to pre-vent one adverse event-for example, one caseof occupational disease or one case of longterm disablement.
VALIDITY CHARACTERISTICS OF THE TESTSUSED; POSITIVE PREDICTIVE VALUEValidity and reliability (reproducibility) oftests vary enormously. Hardly any of the testsfor showing a particular risk factor are entirelyvalid. People are missed who do carry the riskfactor, whereas others are wrongly designatedas risk carriers. Mostly use is made of the testattributes sensitivity and specificity to ascer-tain the validity of a given test. In combinationwith the actual prevalence of a risk factor in agiven population the test standards give anindication of the certainty that the risk factoridentified is actually present in a given person;this is the prognostic or positive predictivevalue (PPV). The PPV is thus the proportion
2
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D
Preventive effectiveness ofpre-employment medical assessments
of those people with a positive test result whoactually carry the risk factor. It should benoted that the description of PPV used in thescientific literature is unfortunate as what ismeant here is not an attempted prognosis of apossible subsequent appearance of a workrelated ailment, but only the correct predictionof the presence of a risk factor.A general equation can be derived from
which the PPV can be calculated for a positivetest result-that is, a result which predicts thepresence of a risk factor (Kleinbaum et al,198221).
PPV= ap(1)asp + (1 - b)(l -p)
where: a= sensitivity of the test; b=specificity of the test; p = prevalence of therisk factor.
Example 1Imagine that the atopy of people applyingfor the job of technician responsible forlaboratory animals needs to be ascer-tained, as those with atopic reactions areespecially at risk of allergic reactions inthis work environment. The identificationof people as atopic or non-atopic maythus be used as a selection criterion. Bothsensitivity and specificity of the test usedto identify these people-namely, a ques-tionnaire in combination with an evalua-tion of the IgE concentration in blood, are90% under optimal conditions. Theprevalence of atopy in the general popula-tion of the Netherlands is about 5%. Apositive test result implies that somebodyis identified as being atopic. When thedetails of this example are filled in inequation 1, the outcome is that of thosewith a positive result, 32% are correctlyidentified with atopy and thus areexcluded from the selection process. Itfollows that 68% of the test positive can-didates will incorrectly be identified asatopic, but will nevertheless be excludedfrom the selection process.
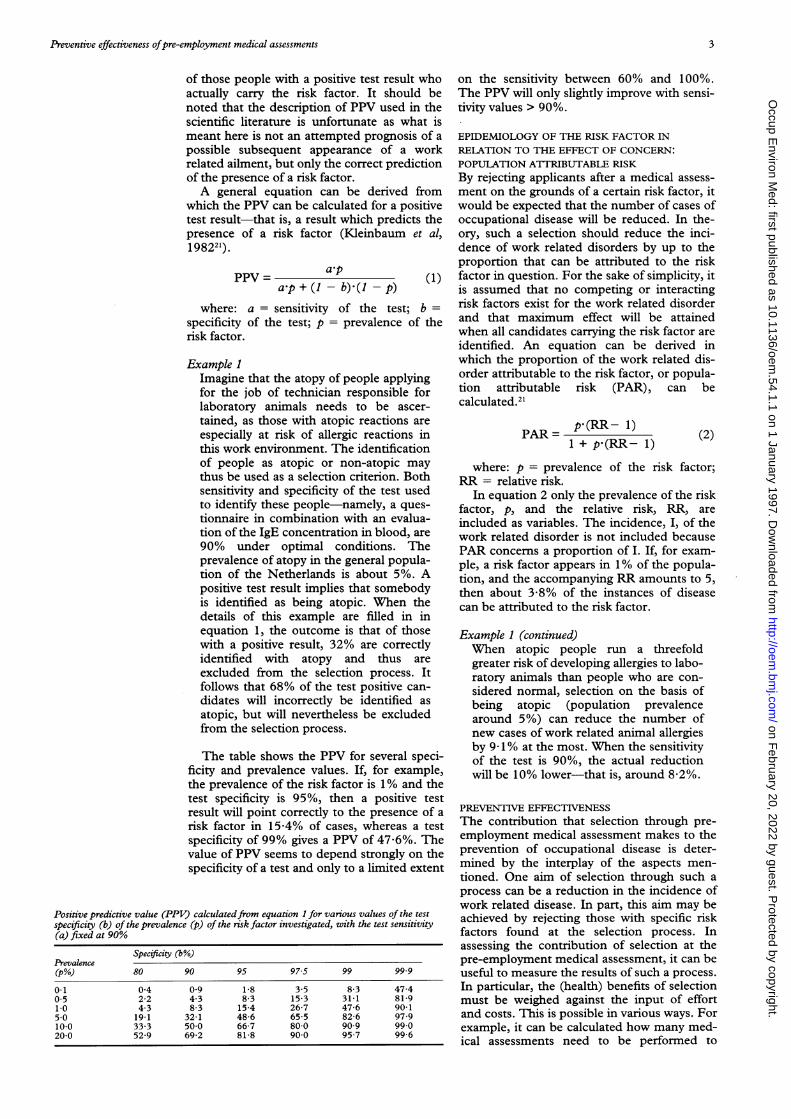
The table shows the PPV for several speci-ficity and prevalence values. If, for example,the prevalence of the risk factor is 1% and thetest specificity is 95%, then a positive testresult will point correctly to the presence of arisk factor in 15-4% of cases, whereas a testspecificity of 99% gives a PPV of 47-6%. Thevalue of PPV seems to depend strongly on thespecificity of a test and only to a limited extent
Positive predictive value (PPV) calculatedfrom equation 1 for various values of the testspecificity (b) of the prevalence (p) of the risk factor investigated, with the test sensitivity(a) fixed at 90%
on the sensitivity between 60% and 100%.The PPV will only slightly improve with sensi-tivity values > 90%.
EPIDEMIOLOGY OF THE RISK FACTOR INRELATION TO THE EFFECT OF CONCERN:POPULATION ATTlRIBUTABLE RISKBy rejecting applicants after a medical assess-ment on the grounds of a certain risk factor, itwould be expected that the number of cases ofoccupational disease will be reduced. In the-ory, such a selection should reduce the inci-dence of work related disorders by up to theproportion that can be attributed to the riskfactor in question. For the sake of simplicity, itis assumed that no competing or interactingrisk factors exist for the work related disorderand that maximum effect will be attainedwhen all candidates carrying the risk factor areidentified. An equation can be derived inwhich the proportion of the work related dis-order attributable to the risk factor, or popula-tion attributable risk (PAR), can becalculated.21
PAR = p*(RR- 1)1 + p-(RR- 1)
(2)
where: p = prevalence of the risk factor;RR = relative risk.
In equation 2 only the prevalence of the riskfactor, p, and the relative risk, RR, areincluded as variables. The incidence, I, of thework related disorder is not included becausePAR concerns a proportion of I. If, for exam-ple, a risk factor appears in 1% of the popula-tion, and the accompanying RR amounts to 5,then about 3-8% of the instances of diseasecan be attributed to the risk factor.
Example 1 (continued)When atopic people run a threefoldgreater risk of developing allergies to labo-ratory animals than people who are con-sidered normal, selection on the basis ofbeing atopic (population prevalencearound 5%) can reduce the number ofnew cases of work related animal allergiesby 9-1% at the most. When the sensitivityof the test is 90%, the actual reductionwill be 10% lower-that is, around 8 2%.
PREVENTIVE EFFECTIENESSThe contribution that selection through pre-employment medical assessment makes to theprevention of occupational disease is deter-mined by the interplay of the aspects men-tioned. One aim of selection through such aprocess can be a reduction in the incidence ofwork related disease. In part, this aim may beachieved by rejecting those with specific riskfactors found at the selection process. Inassessing the contribution of selection at thepre-employment medical assessment, it can beuseful to measure the results of such a process.In particular, the (health) benefits of selectionmust be weighed against the input of effortand costs. This is possible in various ways. Forexample, it can be calculated how many med-ical assessments need to be performed to
3
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D
reduce the number of new cases of a specificoccupational disease by one. How many can-didates need to be rejected to reduce the num-ber of new cases of a certain work relatedailment by one can also be calculated. Theappendix shows a derivation of the equationsused in these calculations. With formula (8')from the appendix, the necessary number ofmedical assessments to reduce the number ofnew cases by one, K, amounts to:
1aKPAR-I (8')
and the necessary number of rejections,Krejectedl amounts to:
Kr,jCWd = -(1PPV.PARI (9)Where a = sensitivity of the applied test;
PAR = population attributable risk; I =(cumulative) incidence of the disease oradverse career outcome; p = prevalence of therisk factor; PPV = positive predictive value.The equations can be calculated quickly andeasily.
Example 1 (continued)The cumulative incidence I for the acqui-sition of an allergy to laboratory animalsamounts in some investigations to around100/1000 animal technicians. With valuesfor p, PAR, and PPV it can be calculatedby means of equations 8' and 9' that foreach avoided case of allergy 122 medicalassessments must be performed and 17candidates must be rejected. Twelve ofthe group of 17 rejected candidates willhave been diagnosed incorrectly as beingatopic.
Example 2When appointing nurses for a generalhospital the occupational physicianwishes to prevent sick leave periods due tolow back pain lasting four weeks or moreduring the 10 years after the health assess-ment. Previous chronic episodes of backpain are regarded as a valid predictor.Therefore, the use of a questionnaire ask-ing for absence due to back pain for atleast four weeks in the past is considered.To apply equations 8' and 9', some criti-cal values have to be estimated.
In a first estimation, values close toreality will be used. Also, more or lessextreme estimations will be presented tostimulate the discussion.
Firstly, sensitivity of the question onsickness absence in the past is expected tobe low, 0 70, as some applicants will denyproblems. Being a rather straightforwardquestion, a high specificity of 0-95 is pre-sumed. In this mostly young populationthe prevalence of an absence for fourweeks or more due to back pain in thepast has been reported to be 3%. Peoplewith such absence in the past may show arelative risk for three for future periods ofsickness absence of four weeks or more.
The cumulative incidence of sicknessabsence for four weeks or more during 10years has been estimated to be 10% of theapplicant population.The results of the calculations are a K
value of 252 and a Krejected value of 18. Inother words, to prevent one case 252examinations have to be organised with18 candidates rejected, including 12incorrectly diagnosed risk carriers.
In a second estimation, a situationmore favourable for pre-employmentmedical assessments is presented. Here, asensitivity of 0 90, a specificity of 0-975,and a prevalence of the personal risk fac-tor of 6% are assumed. As some publica-tions report a high relative risk, wedecided for this example on a relative riskof five in combination with a cumulativeincidence of 20%. Now, 29 pre-employ-ment assessments are necessary and twocandidates have to be rejected for everyprevented case. In a third estimation, amore extreme situation in the oppositedirection has been chosen with a sensitivityof 0 70, a specificity of 0-80, a prevalencevalue of 2%, a relative risk of two, and acumulative incidence of 5%. From this, Kis 1457 and Keected is 306, including 286incorrectly diagnosed risk carriers.
Preventive effectiveness of pre-employmentmedical assessments is not restricted to pre-venting work related diseases but can be gen-eralised to other goals. Subsequently, theresults of the calculated preventive effective-ness can be applied to estimate the extent ofthe anticipated avoidance of economic risk.However, it is necessary to keep in mind thesubstantial social influences on outcomes suchas sickness absence. Moreover, the pre-employment medical itself is likely to onlymake a small (if any) contribution to safeworking practices, hazard control, and indeed,sickness absence during the course of employ-ment.
Example 3Assume that 5% of the population of can-didates run a twofold risk of health relatedsick leave or some other health relatedadverse career outcome-such as prema-ture retirement for health reasons-whichwould occur in 5% of the working popu-lation. Given these assumptions, the riskcarrying candidates account for about4-8% additional sick leaves or prematureretirements for health reasons. Assumealso that sensitivity and specificity areboth 90% with the available methods ofidentifying the risk carriers. Then 467candidates must be examined, of whichabout 65 (14%, including about 44 non-risk carriers) must be rejected to preventone person from experiencing the adverseoutcome of concern. The justification ofadopting such a selection policy could bethat it is considered more profitable toexamine 467 candidates and to reject 65(including 44 non-risk carriers) than to
4
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D
Preventive effectiveness ofpre-employment medical assessments
accept one person who will experience anadverse outcome, presupposing that theadverse outcome could not have beenprevented otherwise.
Decision makingThe previous section should offer a rationalefor the use of a test in a pre-employment med-ical assessment but also for use of all the pre-employment medical assessments as a meansof personnel selection. Thus it is crucial todevelop assessments of job specific pre-employment medicals. Job demands shoulddictate the contents of the medical assessment.In our view, this automatically leads to the set-ting of conditions on the contents of a pre-employment medical assessment.
Firstly, the medical assessment should con-sist of no more questions and tests than areneeded. This implies that the preventive effec-tiveness of the questions or tests must beknown or be estimated from available knowl-edge. If the preventive effectiveness is consid-ered to be too low, then the question or testshould not be incorporated for selection pur-poses-for example, questions involving the"general impression" of the physician in deci-sion making, a medical test that cannot bereproduced, should be avoided. Moreover, thegeneral impression of the physician involved isunlikely to be an appropriate selection crite-rion for any job. Ultimately, if no acceptablemedical questions or tests are at hand, thereshould not be a pre-employment medicalassessment to select personnel. During thisdecision making process a wide range ofKval-ues may occur that are highly dependent onthe estimation of some basic values. Someresults may not indicate the adoption of thepre-employment medical examination toselect personnel, but others would stronglysupport it. One possible solution for narrowingthe wide range ofK values is to ask a profes-sional panel to present an evidence based(more narrow) range of K and Krejected valuesfor several common situations. To foster effi-ciency and to stimulate implementation, theseactivities can be incorporated in the develop-ment of professional guidelines.
Secondly, criteria for rejection must be setin advance. If set afterwards, criteria may easilybe distorted by personal views and subjectiveand variable standards. As a corollary, testvalidity decreases, thus lowering preventiveeffectiveness, simply because the reproducibil-ity of the test will be lower.
Thirdly, although emphasis on preventiveeffectiveness remains of utmost importance, alow preventive effectiveness can be acceptablewhenever the impact of the risk to be avoided isconsidered large-for example, if the safety ofcolleagues, customers, or the public in generalis at stake-or if the health effect is very seri-ous. As a matter of course, serious risks do notimprove preventive effectiveness. However,the benefit of reducing the incidence of a seri-ous adverse event by one may outweigh thecosts of rejecting many candidates-for exam-ple, in the selection of aircrew.
Fourthly, it is unlikely that experience andknowledge of the individual occupationalphysician will not play a part in performingpre-employment medical assessments andthus in the outcome. This unavoidable "expertjudgment", notwithstanding its subjectivenature, can be considered justified in situa-tions where general guidelines are not applica-ble or simply not available because of theuniqueness of the situation. If such a situationoccurs, the preventive effectiveness cannot becalculated or estimated. The use of expertjudgment, therefore, remains a decisive tool inassessing medical fitness for a job. The appli-cation of expert judgment should be based onprofessional guidelines wherever possible andshould be made clear. An unequivocal regis-tration of the results of the medical assessmentis required for evaluation. Therefore, the argu-ments for the decision must be made explicit.
Fifthly, unexpected or coincidental findingsmust be treated properly. That is, serendipi-tous discoveries should not be denied andmust be treated carefully. However, findingsuch cases cannot justify the use of pre-employment medical assessments to selectpersonnel although, in individual cases, rejec-tion of the candidate involved might just bethe actual outcome of the procedure.
ConclusionThe pre-employment medical assessment aimsat reducing adverse health related career out-comes and job related safety risks by identifyingrisk carriers and taking subsequent appropriatemeasures. From a different point of view, itmay sometimes be used for lowering absen-teeism, long term disablement, or financialrisks to the health insurance company or thepension fund.We suggest that a balanced policy in occu-
pational medicine should be pursued and thatthe concept of preventive effectiveness may behelpful in attaining evidence based occupa-tional medicine, which starts at the pre-employment medical assessment.
Appendix: Derivation of equations for thenumber ofmedical assessments and rejectionsneeded to reduce the number of adverse careeroutcomes by oneSuppose, a company needs Z new employees for a par-ticular type of job within a given time span. Withoutselection, it can be expected that ultimately a propor-tion I of the employees will contract a certain occupa-tional disease-that is, the cumulative incidence of thisdisorder is I. From equation 2, it follows that, in thissituation, in the group of Z employees there are:
Nfactor= PAR-I-Z (3)employees who will get this disorder and for whom
the disorder can be attributed to the fact that theseemployees have a certain risk factor. With the risk factoras a selection criterion, the number of cases of this par-ticular occupational disease should decline. If a is thetest sensitivity, then by means of the pre-employmentmedical policy there are:
Navoided= a-PAR-I-Z (4)less new cases of the work related disease. As this
risk factor is used as a selection criterion at the medicalassessment, several candidates will be rejected from the
5
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D
selection process. If Z new workers are ultimatelyrequired to be taken into service, then more than Zcandidates must be screened, namely Z' candidates. Z'can be determined as follows.The expected proportion with a positive test result,
and therefore the expected proportion to be rejected bythe medical assessment, Frej,,ted amounts to (equation1):
Frejected = a-p + (1 - b) (l -P) = ap (5)PPV
It holds that:
Z- Frjcted Z =Z (6)
From equation 6 it follows that:
Z'= z 7( 1 Frejected)
candidates must be subjected to a pre-employmentmedical assessment to eventually appoint Z newemployees. The number of medical assessments toavoid one case, K (equations 4 and 7), then amountsto:
NK- ided a-PAR-I(l - Frejecred)By multiplying equation 8 by equation 5 it is possible
to calculate the number of rejections per case avoided,Krejected:
Rejected = KFrejected = (9)PPV-PARI(l - Fmimed)(9If Freje:,,d is very small, then equations 8 and 9 can be
reduced to:
K Zt 1(8')Navoided a-PAR-I
and:
Krejected = K Frejected p-P (9-I=E,,5=PPV-PARI ('
We thank Jos Verbeek and Willeke van der Weide for theirassistance in preparing the manuscript, in particular, for theinformation needed to elaborate examples.
1 Van Dijk FJH, De Kort WLAM, Verbeek JHAM. Qualityassessment of occupational health services instruments.Occup Med 1993;43(suppl 1):S28-33.
2 Whitaker S, Aw TC. Audit of pre-employment assessmentsby occupational health departments in the NationalHealth Service. Occup Med 1995;45:75-80.
3 Hendriks A, Gevers JKM. (Pre-)employment medicalexaminations and the law, with particular reference to theEuropean Union. European Journal of Health Law 1994;1:229-64.
4 Wilson JMG, Jungner G. Principles and practice of screeningfor disease. Geneva: World Health Organisation, 1968.(Public health papers 34.)
5 Halperin WE, Ratcliffe J, Frazier TF, Wilson L, Becker SP,Schulte PA. Medical screening in the workplace: pro-posed principles. J OccupMed 1986;28:547-52.
6 Atherley G. Human rights versus occupational medicine.IntrHealth Serv 1983;13:265-75.
7 Hogan JC, Bernacki EJ. Developing job-related preplace-ment medical examinations. J Occup Med 1981;23:469-76.
8 Schilling RSF. The role of medical examination in protect-ing worker health. J Occup Med 1986;28:553-7.
9 Cox RAF, Edwards FC. Introduction. In: Cox RAF,Edwards FC, McCallum RI, eds. Fitness for work. Themedical aspects. Oxford, Oxford University Press, 1995.
10 Harber P, Herzstein J. Impairment and disability. Con-siderations of susceptible populations. In: Rosenstock L,Cullen MR, eds. Textbook of clinical occupational and envi-ronmental medicine. Philadelphia, WB Saunders, 1994.
11 Rothstein MA. Medical screening of workers. Washington,DC: Bureau of National Affairs, 1984.
12 International Commission on Occupational Health. Inter-national code of ethics for occupational health professionals.Singapore: International Commission on OccupationalHealth, 1992.
13 Hauptverband der gewerblichen BerufsgenossenschaftenArbeitsmedizinische Vorsorgeuntersuchungen bei Ein-wirkung krebserzeugender Arbeitsstoffe. ArbeitsmedizinSozialmedizin Prciventivmedizin 1982;17:228-35.
14 Health and Safety Executive. Pre-employment health screen-ing. London: HSE, 1982. (Guidance note MS20.)
15 International Labour Organisation. Convention concerningoccupational health services. Geneva: ILO, 1985. (Conven-tion 161.)
16 International Labour Organisation. Recommendation con-cerning occupational health services. Geneva: ILO, 1985.(Recommendation 171.)
17 World Health Organization. Early detection of occupationaldiseases. Geneva: WHO, 1986:1-5.
18 KNMG (Royal Dutch Medical Association). Een protocolten behoeve van werkgevers en arbodiensten betrokken bijaanstellingskeuringen. (A protocol for the benefit of employersand occupational health services involved in pre-employmentmedical assessments). Utrecht, the Netherlands: KNMG,1995.
19 De Kort WLAM, Fransman LG, Van Dijk FJH. Pre-employment medical examinations in a large occupa-tional health service. ScandJ Work Environ Health 1991;17:392-7.
20 De Kort WIAM, Post Uiterweer HW, Van Dijk FJH.Agreement on fitness for a job. Scand J Work EnvironHealth 1992;18:246-51.
21 Kleinbaum DG, Kupper LL, Morgenstern H. Epidemio-logical research. Principles and quantitative methods. NewYork: Van Nostrand Reinhold, 1982.
6
on February 20, 2022 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.1.1 on 1 January 1997. D