Primary Care and ACOs: From Medical Homes to Medical Neighborhoods National ACO Congress November 2, 2011 David Nace, MD McKesson Corporation/Relay Health Patient Centered Primary Care Collaborative Kevin Grumbach, MD UCSF Department of Family and Community Medicine
Transcript
Primary Care and ACOs: From Medical Homes
to Medical Neighborhoods
National ACO Congress November 2, 2011
David Nace, MDMcKesson Corporation/Relay Health
Patient Centered Primary Care Collaborative
Kevin Grumbach, MDUCSF Department of Family and Community Medicine
PatientPatient
Health Care: A Perilous Journey*Health Care: A Perilous Journey*
OrthopedistCardiologist
Radiologist
Gastroenterologist
Chestpain
Stomach
Ache
Knee
ache
Physical Therapist
SNF
*From Tom Bodenheimer, NEJM 2008;358(10):1064
The Delivery System Reform Imperative
•
Patients need–
A medical home
•
High performing, patient-centered primary care
–
A cohesive medical neighborhood•
Care integrated across the diverse components of the health delivery system
Primary Care: The Cardinal 4 C’s
first ContactComprehensive
Continuity
Coordination
–
“Ample research concludes in recent years that the nation’s over
reliance on specialty care services at the expense of primary care leads to a health system that is less efficient…research shows that preventive care, care coordination for the chronically ill, and continuity of care—all hallmarks of primary care medicine—can achieve better health outcomes and cost savings.”
But the Primary Care Foundation in the US is Crumbling
•
Plummeting numbers of new physicians entering primary care and burnout among PCPs
•
Growing problems of access to primary care and “medical homelessness”
•
Dysfunctional systems that are not delivering the goods in primary care
Bodenheimer T. N Engl J Med 2006;355:861-864
Family Medicine Residency Positions and Number Filled by U.S. Medical School Graduates
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
$450,000A
nnua
l Inc
ome
Year
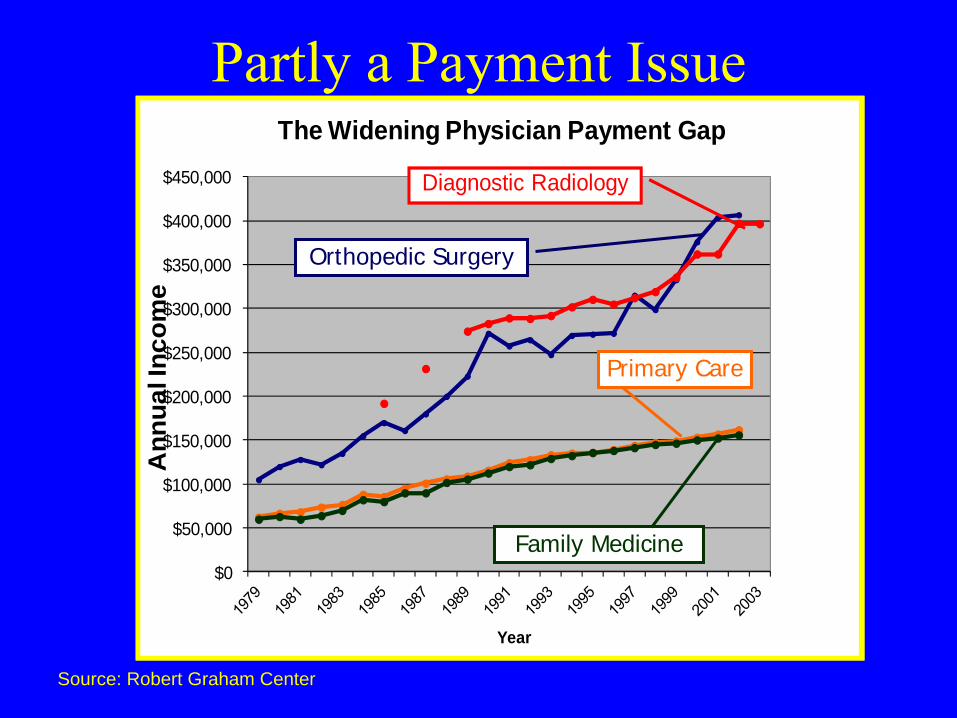
The Widening Physician Payment Gap
Diagnostic Radiology
Orthopedic Surgery
Primary Care
Family Medicine
Source: Robert Graham Center
Partly a Payment Issue
Partly a Systems Issue
•
A primary care physician with a panel of 2500 average patients would spend:
–
7.4 hours per day to deliver all recommended preventive care (Yarnall et al. Am J Public Health 2003;93:635)
–
10.6 hours per day to deliver all recommended chronic care services (Ostbye et al. Annals of Fam Med 2005;3:209)
Tom Daschle, Health Policy Advisor to Barack Obama, testifying to Senate Health Committee, Jan 2009: “Every country starts at the base of the pyramid with primary care, and they work their way up until the money runs out.”
3°
Care
1°
Care
2°
Care
3°
Care
2°
Care
1°
Care
… “We start at the top of the pyramid, and we work our way down until the money runs out…And so we have to change the pyramid. We have to start at the base.”
Senator Orrin Hatch Senate Finance Committee Roundtable
Reforming America’s Health Care Delivery System April 21, 2009
•
“The US is first in providing rescue care, but this care has little or no impact on the general population. We must put more focus on primary care and preventive medicine. How do we transform the system to do this?”
Randy MacDonald, Sr VP House Ways and Means Hearing April 29, 2009
•
“I will start with the very last question asked by the committee--what is the single most important thing to fix in healthcare? Primary care. Strengthen primary care --
transform it and pay differently using a model like the Patient Centered Medical Home.”
•
Congressman: “And the second issue?”
•
“Well, if you don't fix the first issue and do not have a foundation of powerful primary care then you can do nothing else. You have to fix primary care before you can even begin to address a second issue.”
The Multistakeholder The Multistakeholder Movement for Renewal and Movement for Renewal and
Reform of Primary CareReform of Primary Care•
Large employers/private purchasers
•
Consumers/patients/the public•
Government
•
Health professionals
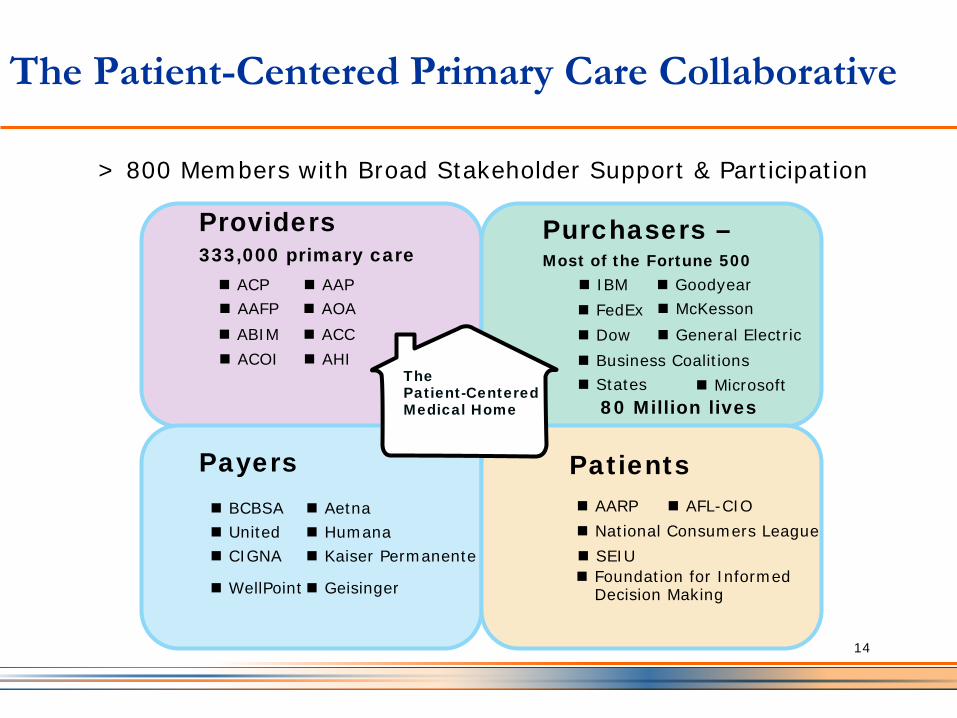
The Patient-Centered Primary Care Collaborative
ACP
Providers 333,000 primary care
Purchasers –Most of the Fortune 500
Payers Patients
AAPAAFP AOAABIM ACCACOI AHI
IBM Goodyear
General ElectricFedEx
Microsoft
Dow
StatesBusiness Coalitions
BCBSAUnited
Aetna
CIGNAHumana
WellPoint
Kaiser Permanente
AARP AFL-CIONational Consumers LeagueSEIUFoundation for Informed Decision Making
> 800 Members with Broad Stakeholder Support & Participation
The Patient-Centered Medical Home 80 Million lives
14
Geisinger
McKesson
Where we are and why primary care mattersUS Healthcare system
fraught with issues
Uncontrollable Spending $2.4 trillion (17% of GDP)
Low Quality compared with EU
Counterparts
Poor Access to PCPs Due to worsen in 2014 with expansion of Medicaid and Exchanges
Below average Population
Health judged by life expectancy
and mortality rates
PPACA and ARRA legislationQuality Reporting InitiativesValue Based Reimbursement Patient Centered Medical HomeEHR/HIE InvestmentDisease Management PilotsAlternate Care SettingsPatient EngagementCare Coordination PilotsHealth Insurance ExchangesTop of License PracticeTelemedicine Pilots
Many experiments underway in an
attempt to improve system
Primary Care has the single‐most
ability to deliver the quality, cost
and population health ambitions
embedded within the IHI’s Triple
Aim
Primary Care centric projects
have proven results
Government financial crisis, an aging population, an already‐high and growing incidence of chronic disease and an expanding
physician shortage (primary care and specialists) only make matters worse
15
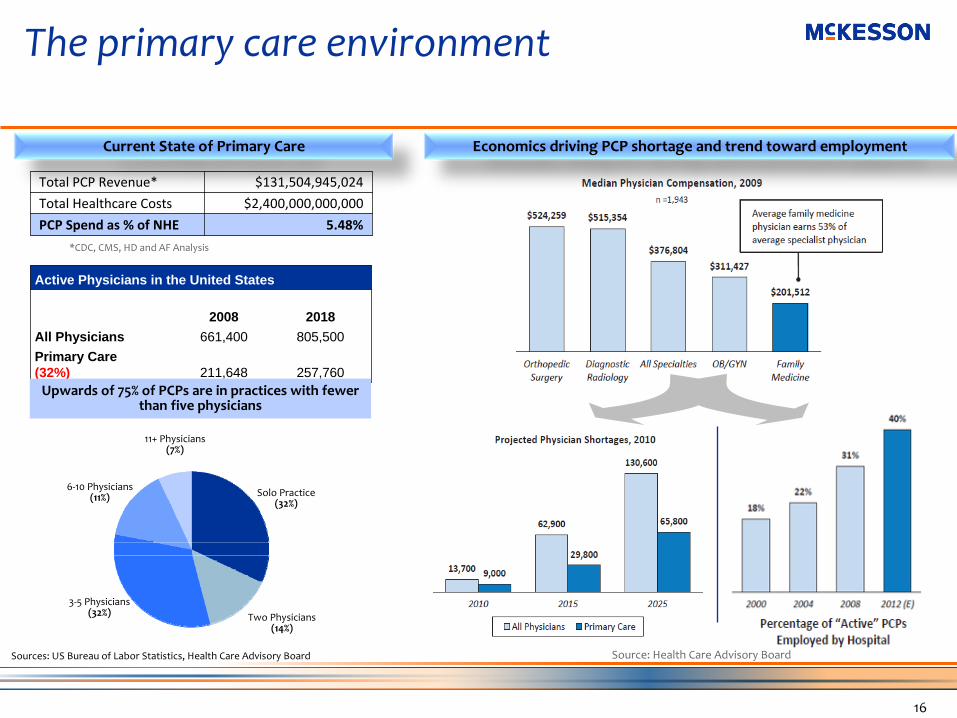
The primary care environment
Active Physicians in the United States
2008 2018All Physicians 661,400 805,500Primary Care (32%) 211,648 257,760
Sources: US Bureau of Labor Statistics, Health Care Advisory Board
Current State of Primary Care
*CDC, CMS, HD and AF Analysis
Source: Health Care Advisory Board
Solo Practice (32%)
3‐5 Physicians (32%) Two Physicians
(14%)
6‐10 Physicians (11%)
11+ Physicians (7%)
Upwards of 75% of PCPs are in practices with fewer
than five physicians
Total PCP Revenue* $131,504,945,024
Total Healthcare Costs $2,400,000,000,000
PCP Spend as % of NHE 5.48%
Economics driving PCP shortage and trend toward employment
16
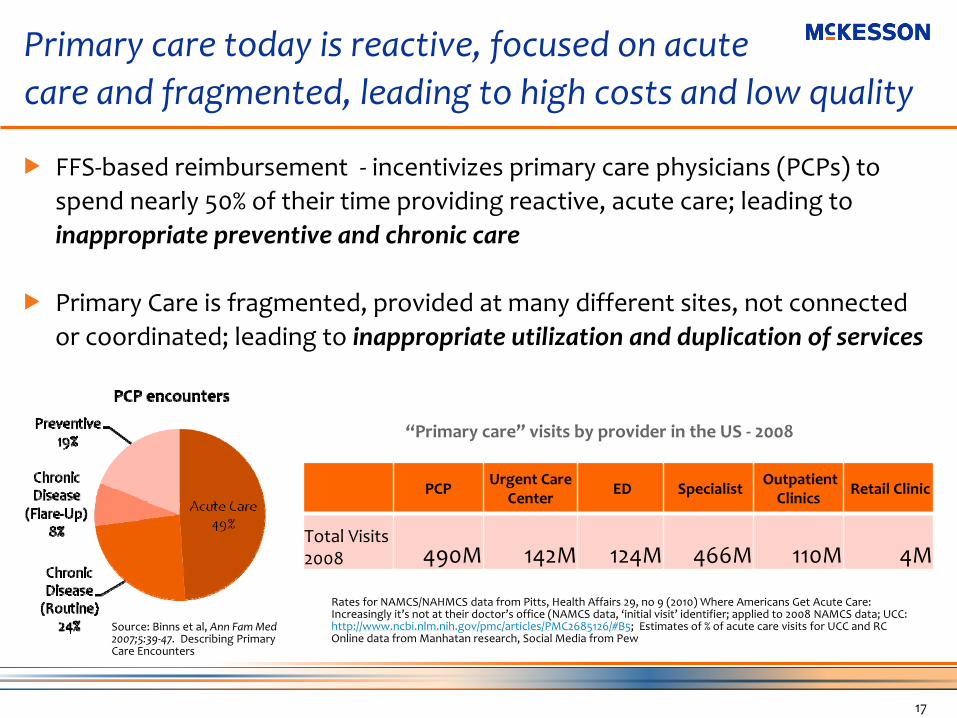
Primary care today is reactive, focused on acute care and fragmented, leading to high costs and low quality
17
Rates for NAMCS/NAHMCS data from Pitts, Health Affairs 29, no 9 (2010) Where Americans Get Acute Care:
Increasingly it’s not at their doctor’s office (NAMCS data, ‘initial visit’
identifier; applied to 2008 NAMCS data; UCC:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2685126/#B5; Estimates of % of acute care visits for UCC and RCOnline data from Manhatan research, Social Media from Pew
“Primary care”
visits by provider in the US ‐
2008
Source: Binns et al, Ann Fam Med
2007;5:39‐47.
Describing Primary
Care Encounters
PCPUrgent Care
Center ED Specialist Outpatient
Clinics Retail Clinic
Total Visits
2008 490M 142M 124M 466M 110M 4M
FFS‐based reimbursement ‐ incentivizes primary care physicians (PCPs) to spend nearly 50% of their time providing reactive, acute care; leading to inappropriate preventive and chronic care
Primary Care is fragmented, provided at many different sites, not connected or coordinated; leading to inappropriate utilization and duplication of services
American Academy of Pediatrics (1967) – first documentation of the “medical home” ‐ One central source of a child’s pediatric records”History of the Medical Home Concept Calvin Sia, Thomas F. Tonniges, Elizabeth Osterhus and Sharon Taba Pediatrics 2004;113;1473‐1478
Patient Centered – introduced by the Institute of Medicine
Karen Davis (Commonwealth Fund) – urges adoption of the Danish model of the Patient Centered Medical Home
18
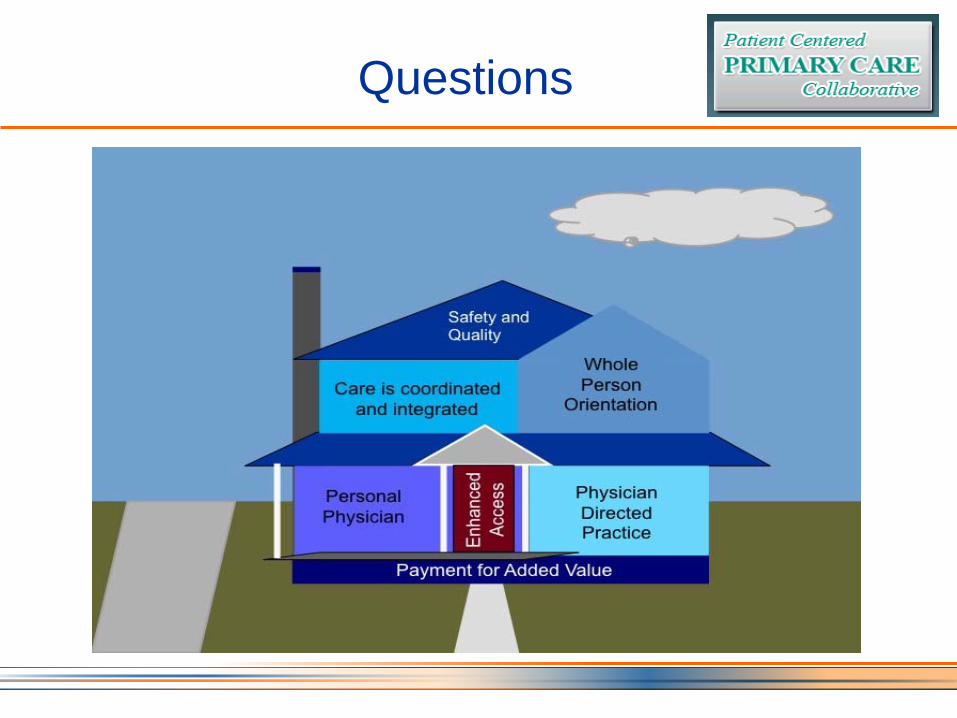
Joint principles of the Patient‐Centered Medical Home (2007)
The following principles were written and agreed upon by the four Primary Care
Physician Organizations – the American Academy of Family Physicians, the
American Academy of Pediatrics, the American College of Physicians, and the
American Osteopathic Association.
Principles:
Ongoing relationship with personal physicianPhysician directed medical practiceWhole person orientationCoordinated care across the health systemQuality and safety Enhanced access to carePayment recognizes the value added
19
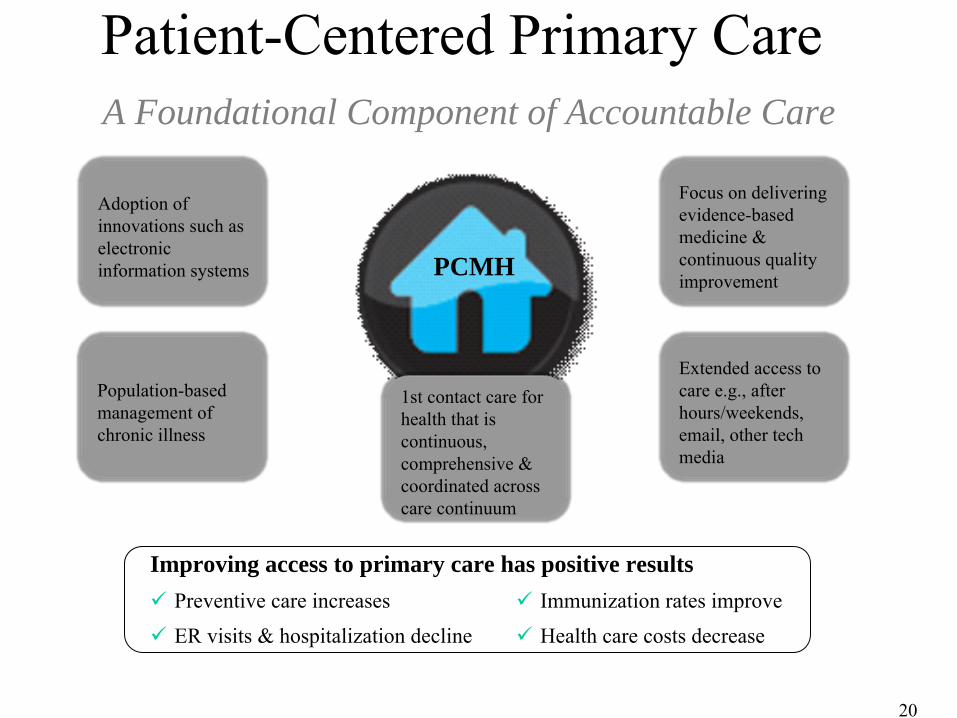
Patient-Centered Primary Care A Foundational Component of Accountable Care
1st contact care for health that is continuous, comprehensive & coordinated
across care continuum
Adoption of innovations such as electronic information systems
Population-based management of chronic illness
Focus on delivering evidence-based medicine
& continuous quality improvement
Extended access
to care e.g., after hours/weekends, email, other tech media
PCMH
Improving access to primary care has positive resultsPreventive care increases Immunization rates improve
ER visits & hospitalization decline Health care costs decrease
20
Case Study: Group Health Cooperative of Puget Sound
•
Patient Centered Medical Home model piloted at one site in 2007–
Avg PCP panel size reduced from 2327 to 1800
–
Longer face-to-face visits and scheduled time for phone and email encounters
–
Increased team staffing and teamwork–
HIT
–
Panel management
Group Health PCMH Pilot: Controlled Evaluation 12 Month Outcomes
•
Improved continuity of care•
Better patient experiences (6 of 7 measures)
•
Better composite quality of care score•
Reductions in ED visits and Ambulatory Care Sensitive Hospitalizations
•
No difference in total costs at year 1 (lower total costs by year 2)
Source: R Reid et al. Am J Managed Care 2009;15:e71
North Carolina Medicaid/SCHIP: Cumulative savings of $974.5 million over 6 years (2003-2008)
•
Colorado Medicaid: $215 ↓
cost per child per year
From Medical Homes to Medical Neighborhoods
•
High performing primary care necessary but not sufficient
•
Accountable Care Organizations as an approach to integrated medical neighborhoods
The Concept of Integrated CareIntegrated Care
•
Ann Beal, Aetna Foundation:–
“
Integrated health care starts with good primary
care and refers to the delivery of comprehensive health care services that are well coordinated with good communication among providers; includes informed and involved patients; and leads to high-quality, cost-effective care. At the center of integrated health care delivery is a high-performing primary care provider who can serve as a medical home for patients.”
Hospital Payer
Other
Caregivers
Pharmacies
Nurse
Specialists
Social Worker
PCMH
Primary Care Team
Patient
Workplace
Home and
Family
Patients Need a Good Home and a Good Neighborhood
Community
What is Accountable Care?
Accountable care requires physicians to change how they deliver care
and to work with other providers and payors in collaborative ways
Significant care coordination between providers caring for a patientAbility to collect and share information across care givers and patientsPerformance transparency across the system and stakeholdersShifting to a primary focus on patient health & care outcomes rather than on transactions/intensity of services
Accountable care is a term that is often a proxy for the desired outcome of health reform efforts: high quality care at the best possible cost
Key Elements to Achieve Accountable Care
30
Health IT Framework
Accountable Care and PCMHTwo Sides of the Same Coin
PCMH
PCMH
PCMH
PCMHHospitals
Public Health
Community Care TeamCare CoordinatorCase Managers
Behavioral Health SpecialistCommunity Health Workers
Specialists
A Coordinated Health System
PCMH
PCMHs require resources that enable care coordination, includingAdequate primary care workforceHealth information technologyInnovative team-based care coordination models with appropriately-trained staffPayment models that compensate PCMHs for care coordination activities that fall outside the in-person, patient visit
PCMH Have a Critical Role in Care Coordination in ACOs
Care Coordination An Essential Function of Accountable Care
Targeted care coordination may involve assigning a care coordinator to specific cases, including face-to-face patient contact
Care coordination using team-based primary care models has been shown to improve health outcomes and/or reduce hospitalizations, readmissions and costs
Care coordination using team-based primary care models has been shown to improve health outcomes and/or reduce hospitalizations, readmissions and costs
33
Health Information Technology Enabling Practice Transformation
To support PCMH (practice) and ACO (enterprise) practice transformation, an interconnected HIT network with key capabilities acts to optimize
engagement and coordinate care
HIT as an enabler of Access, Care Coordination, and Care Integration
A foundational shift in Health Information Technology (HIT) must occur in order to drive widespread adoption of the Patient Centered Medical Home (PCMH) model, and support the Accountable Care Organization (ACO)
- “Better to Best : Value Driving Elements of the Patient Centered Medical Home and Accountable Care Organizations”, March 2011, Health2Resources, Washington, D.C.
What we are now learning……
System Level Interventions to Enhance Integration
•
eReferral in the San Francisco General Hospital clinic system as an example of a disruptive HIT-enabled innovation to promote a better functioning medical neighborhood
San Francisco General HospitalSan Francisco General Hospital
Reengineering Specialty Referrals at SFGH
•
EHR-embedded “eReferral”
system
•
Home grown product developed by SFGH- UCSF gastroenterologist, Hal Yee, MD,
expanded by Alice Chen, MD, Gen Int Med
•
Chen AH, Kushel, Yee, Grumbach. Health Affairs 2010 May;29(5):969-71.
Description of eReferral____________________________
•
HIPAA compliant web-based referral system–Linked to EHR, with auto-
population of relevant EHR data –Free text referral questions–Mandatory use for enrolled specialty
clinics and certain imaging studies
Description of eReferral____________________________
•
Individualized review and response by specialist–
Specialists can: •
Request clarification of question or additional work-up prior to specialty appointment
•
Provide information for PCP management of condition, with or without an appointment
•
Overbook appointment if clinically warranted–
Ability for iterative communication between referring and reviewing clinicians
Improved Timing of Consultations Resulting in Reduced Waiting Times
Mixed payment model (Medicaid, Medicare fee for service payments + block funding from City for uninsured)
•
Capacity constrained system•
Network-wide EHR
•
Culture of collaboration, multispecialty medical group
Regional HIE Collaboration Northern California Market
Six Health Organizations Collaborating in the SF Bay Area
•Over 3,000 connected physicians
•Over 1,000,000 connected patients
•More than 150,000 actively connected individuals
•Providers and hospital information exchange
•Reference lab collaboration
•Coordinated care across community
•Interoperability with 5 different vendors (Cerner, GE, NextGen, McKesson, Dynamic Business Solutions)
44
SpecialtyProviders
Primary Care Providers
Consumer PHRs
Loca
l Clin
ical
Inte
grat
ion
Loca
l Clin
ical
Inte
grat
ion
Reg
iona
lly C
onne
cted
Reg
iona
lly C
onne
cted
Patient Centric Platform
HospitalsHospital Lab & Radiology Centers
Home Health Services
Community Labs
Nat
iona
lly C
onne
cted
Nat
iona
lly C
onne
cted
Payers
NHIN
Regional Health Systems
State RHIOs
Patients
Extending from the Practice ……. to the Community
45
46
Internet based networks can deliver immediate value through a patient-centered strategy
Patient centricity is a paradigm shift, that can catalyze structural changes in the delivery system…….
11/1/2011 46
Patient Centricity Critical to Driving Value
PCMH is foundational for Patient Centered ACO’s
Source: Premier Healthcare Alliance 47
4 Key Pillars of Competency
I. Consumer Engagement and PCMHthe ability to actively engage patients in their care process, provide patients with access to their pertinent information, and enable a range of personal health management and health information tools.
II. Analyticsthe ability to identify and stratify populations for management, manage cost and quality, address PMPM spend, generate and act upon care gaps, understand and optimize provider performance, and support stakeholder and regulatory reporting.
III. Care Managementthe ability to leverage evidence based decisions in the delivery of care, create efficient and effective utilization management programs, and establish an integrated medical management workflow system for utilization and disease management.
IV. Financial Managementthe ability to leverage analytics to define and support care bundles and identify network / provider efficiency in preparation for undertaking bundled payment and support for additional payment mechanics.
48
The Medical Home financial rewards model
FEE FOR SERVIC E
PAY FOR PERFORMANCE
(BONUS)
SHARED INCENTIVES
FOR MEDICAL NEIGHBORHOOD
PATIENT CENTERED MEDICAL HOME ---- ACCOUNTABLE CARE ORGANIZATION
CARE MGMTFEE
(PMPM)
49
The Challenge to PCMHs and ACOs
• PCMHs - Expand care teams, conduct non-visit based care coordination, utilize health IT, focus on assuring needs assessment, goal setting, and respecting patient values and preferences
• ACOs - Invest in a solid foundation of primary care, build an HIT infrastructure, focus on care integration and care transitions, align governance and incentives to hold members of the medical neighborhood accountable to each other




















































![Acos postcard[final]](https://static.documents.pub/doc/80x56/568c55701a28ab4916c2c624/acos-postcardfinal.jpg)








