82
Principle of Pharmacology Higher Diploma in Nursing – Year 1 Pathophysiology and Pharmacology
| Date post: | 16-Mar-2018 |
| Category: |
Documents |
| Upload: | phungduong |
| View: | 227 times |
| Download: | 1 times |

Principle of Pharmacology
Higher Diploma in Nursing – Year 1Pathophysiology and Pharmacology

Speaker
• Dr Edgar Liu
• PhD in Pharmacology
• Program Director of Pharmaceutical Studies in
HKU SPACE
• Contact: [email protected]

Topics to cover in this session
• Absorption, distribution, bio-transformation and
elimination of drugs
• Drug interactions
• Drug tolerance and dependency

What is Pharmacology?• Greek: pharmakon
• the Science that deals with the fate of drugs in
the body and their actions on the body
Drug Nomenclature
• Chemical name
• Generic name (or official name)
• Trade name
• Common name
N-(4-hydroxyphenyl)acetamide
Paracetamol / acetaminophen
Panadol, tylenol….etc.

Sources: IntegratedPharmacology, 3rd edition.Mosby 2006
Definitions used in pharmacology• Pharmacokinetics: how the body absorbs, distributes,
metabolizes and excretes drugs
• Pharmacodynamics: how the body responds to drugs:
the interaction between drug and receptor
• Pharmacogenetics: how genetics alters responses to
drugs
• Pharmacoeconomics: cost-effectiveness of drug
treatments

Pharmacokinetics
bsorptionistribution
etabolism
limination
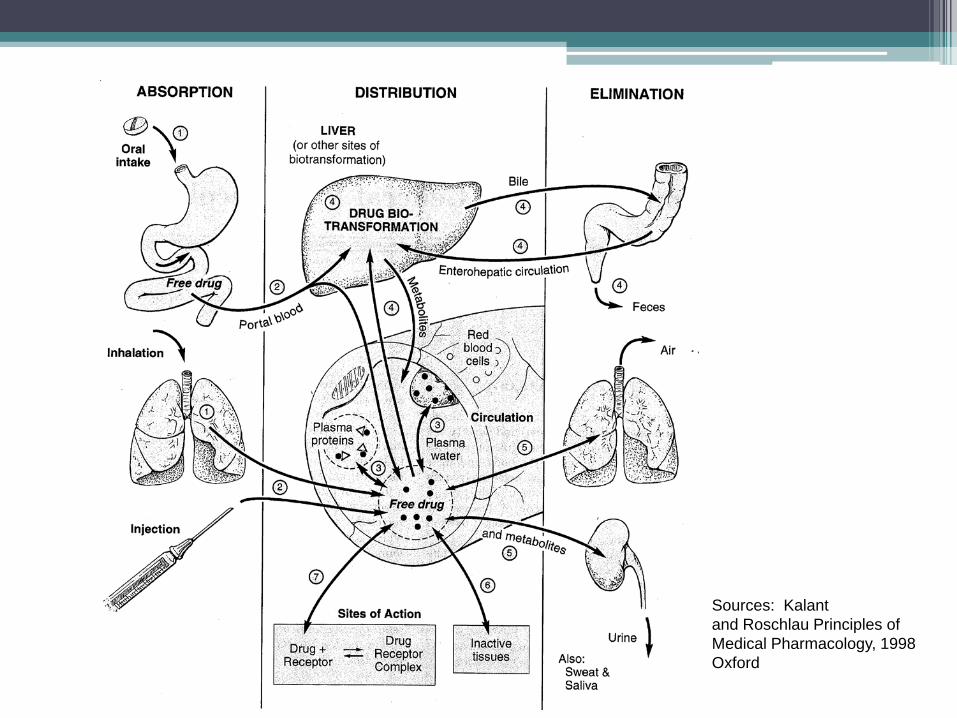
Sources: Kalantand Roschlau Principles ofMedical Pharmacology, 1998Oxford

Routes of drug administration• Topical (e.g. eye, skin)• Sublingual• Oral (p.o. per os)• Rectal mucosa (suppositories)• Pulmonary epithelium (inhalation)• Injection▫ subcutaneous (s.c.)▫ intramuscular (i.m.)▫ intravenous (i.v.)▫ intra-arterial (i.a.)▫ intrathecal (i.t.)▫ intraperitoneal (i.p.)

Drug dosage• Commonly used: mg, ml (cc)• Frequency:
qd: once dailybd (or bid): twice dailytds (or tid): three times dailyqds (or qid) : four times daily

Drug formulation• Tablets, capsules, solutions and suspensions• Controlled-release formulation• Patches• Ointments, creams• Injectable solutions• Suppositories• Inhalers

Scored tablet: the indentation may be used to divide the doseEnteric-coated tablet: coating resists dissolution in the acidTimed-release capsule: the granules in the capsule dissolve at different rates
Medication order• Standing order▫ The patient is to receive the prescribed drug on a regular basis.
e.g. Aricept 10mg PO qd• Single order▫ To administer the drug one time only. e.g. Valium 10mg IV at
9:00pm• PRN order▫ To administer the drug as needed. e.g. Demerol 100mg IM q4h
PRN for pain• STAT order▫ A one-time order given as soon as possible e.g. Losec 40mg IV
STAT
Site of absorption• p.o. : stomach, small intestine• inhalation: pulmonary epithelium• sublingual epithelium• injection: blood circulation• rectal mucosa
Factors affecting absorption• Chemical properties:▫ Chemical nature▫ Lipid partition coefficient (permeability)
• Physical properties:▫ Drug formulations▫ Gastric motility▫ pH at the absorption site▫ Ingestion with or without food▫ Area of absorbing surface

Examples in absorption in G.I.
Highly permeableHighly impermeable
Highly impermeableHighly permeable
1) A tertiary amine
2) An acid

Oral drug absorption
• When the drug is administered in dissolved solution:
easiest to be absorbed

Pathways of Drug Distribution
DRUG DOSAGE
Absorption
Free drug in extracellular water
metabolitesDRUG at the site of action
ExcretionBinding to:serum proteins
tissue fat, proteins

Volume of distribution• 70 kg man • Blood volume: 4-5 L• Total body water: 50-70% of weight = ~40 liters• 40 L = extracellular + intracellular
(13L) (27L)
Plasma concentration = Mass (g) / Volume of distribution (L)

Simple calculationA 70kg lean man takes 15g of alcohol:Total body water= 70% of weight = 50LConcentration of drug in TBW = 15g/50L = 0.3g/LSince alcohol does not bind to plasma proteins,and plasma contains 93% waterConc. in plasma = 0.28 g/LConc. in blood = 0.24 g/L (conversion factor 1.16)Alcohol limit in Hong Kong: 0.5g/L
log
conc
.
time
C0
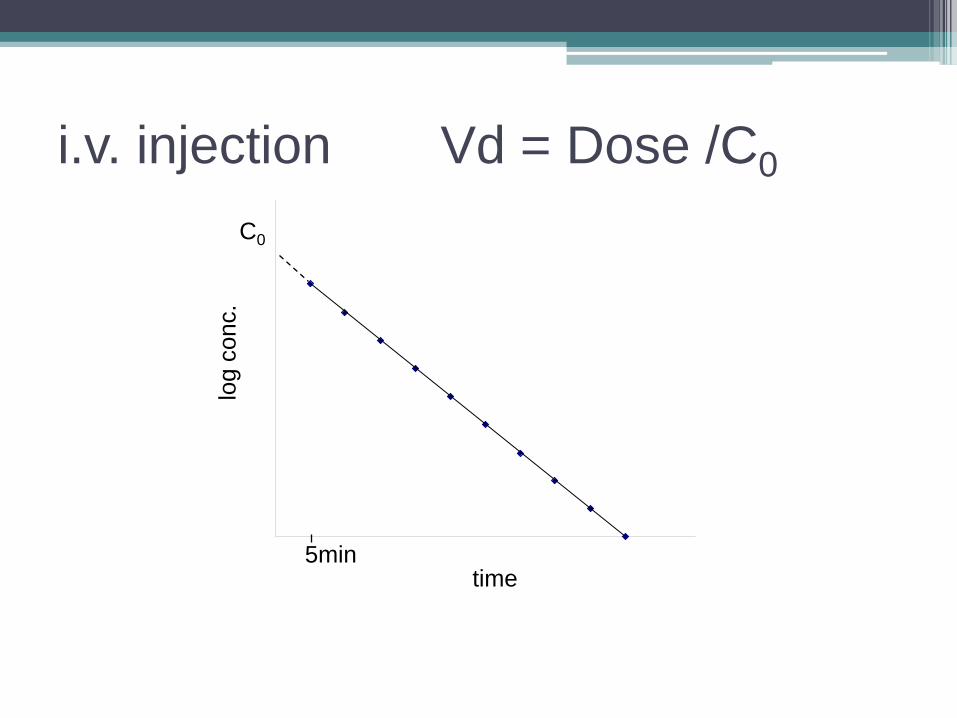
i.v. injection Vd = Dose /C0
5min

Tissue and plasma protein binding• Tissues: fat and protein
e.g. DDT stored in fat
• Plasma protein bindinge.g. diazepam or propanolol (over 90% bound)- albumin protein: acidic drug- globulin protein: basic drug
A A+

Importance of plasma protein binding
• free drug conc., pharmacological activity
• clearance by glomerular fitration in kidney
• Prolong half life of drug in the body
• Highly protein bound drug interactions
• Competition binding with endogenous substance
e.g. bilirubin, fatty acids

Conc. ofhalothanein eachtissuegroup
Vessel-rich group
Time
Tissue distribution of halothane

Blood brain barrier• Only capillaries in the body that have their
intercellular spaces completely occluded.• Only lipid-soluble drugs normally get into the
cerebral spinal fluid (CSF) from the blood• Once the drug get to CSF, they can permeate
into the brain cells freely.

Metabolism (or biotransformation)
Background
• Intake may contain traces of potential toxic chemicals
• Conversion of lipid-soluble xenobiotics into more polar and water soluble products
more efficient excretion
Parent Drug
Excreted
Product
Phase I
Phase II
reactions
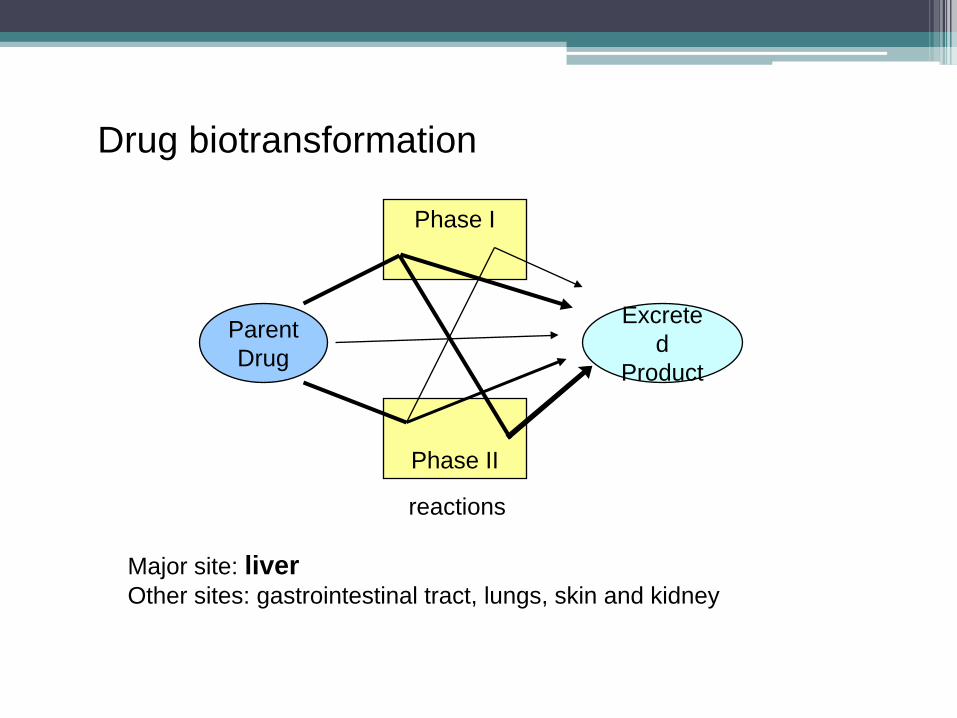
Drug biotransformation
Major site: liverOther sites: gastrointestinal tract, lungs, skin and kidney

Phase I reactions• Oxidation, reduction and hydrolysis
Phase II reactions• Coupling of a drug or drug metabolite with an
endogenous substance
• Epoxide hydration, glucuronidation, glutathione conjugation, sulphation, acetylation, methylation, glycine conjugation

Biotransformation of paracetamol in liver
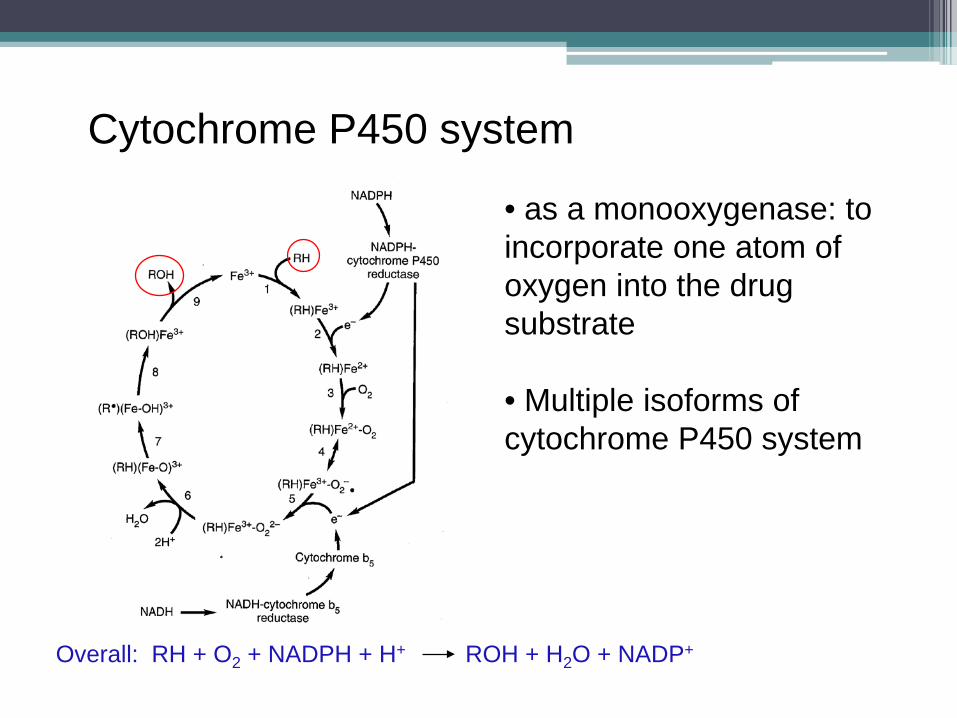
Cytochrome P450 system
• as a monooxygenase: to incorporate one atom of oxygen into the drug substrate
• Multiple isoforms of cytochrome P450 system
Overall: RH + O2 + NADPH + H+ ROH + H2O + NADP+
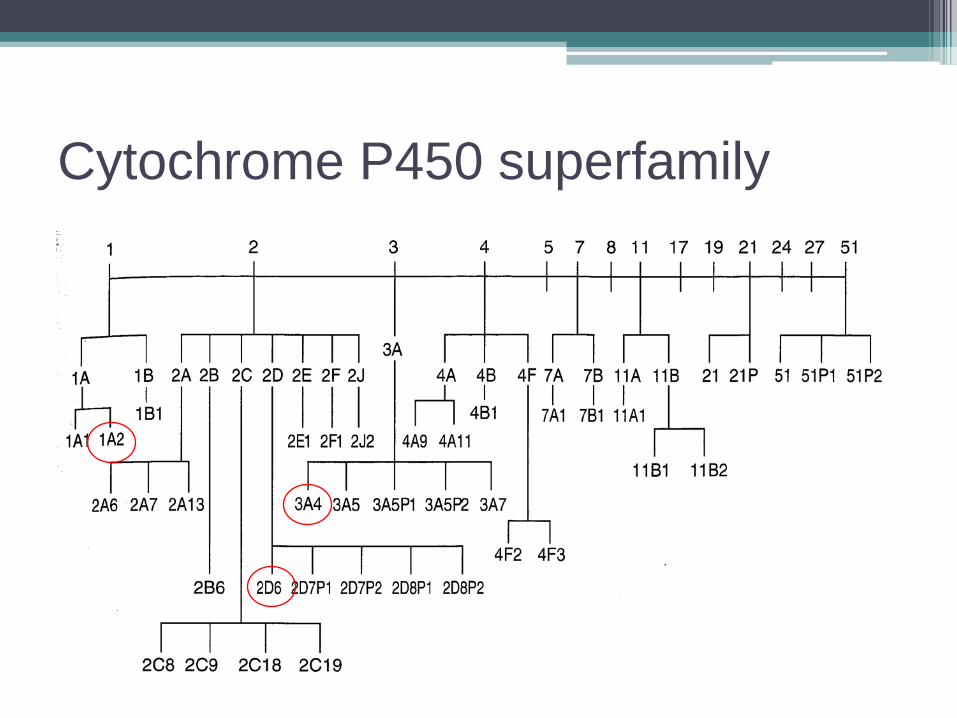
Cytochrome P450 superfamily

Common P450 cytochromes CYP isoforms
Drug substrates
CYP 1A2 Caffeine, tricyclic antidepressants
CYP 2D6 Beta blockers, class I antiarrhythmics, antidepressants (TCA, SSRI, SNRI), antipsychotics
CYP 3A4 acetaminophen, codeine, cyclosporin A, diazepam, erythromycin, statins, calcium channel blockers, steroids, antidepressants and carcinogens
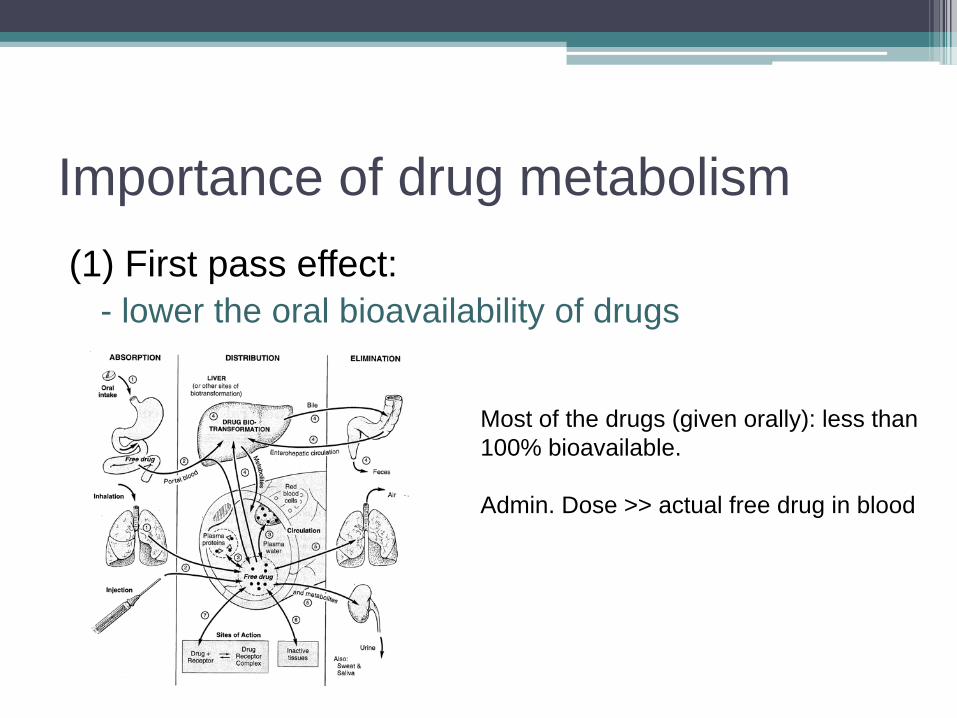
Importance of drug metabolism(1) First pass effect:
- lower the oral bioavailability of drugs
Most of the drugs (given orally): less than100% bioavailable.
Admin. Dose >> actual free drug in blood

2. Activation- An inactive precursor (pro-drug) can be converted
into a pharmacologically active drug
e.g. L-dopa to dopamine (Parkinson’s)sulfasalazine to 5-aminosalicylic acid (5-ASA)
Importance of drug metabolism

3. Individual difference- Impaired enzyme functions may result in poor
detoxification, leading to overdose toxicity
4. Drug-drug interaction
Importance of drug metabolism
Elimination• Drugs are excreted from the body by:▫ Kidneys (urine)▫ Intestinal tract (bile and feces)▫ Lungs (exhaled air)▫ Breast milk▫ Sweat

- Drugs are eliminated regardless of how it is administered
Time course of drugconcentration following i.v. injection
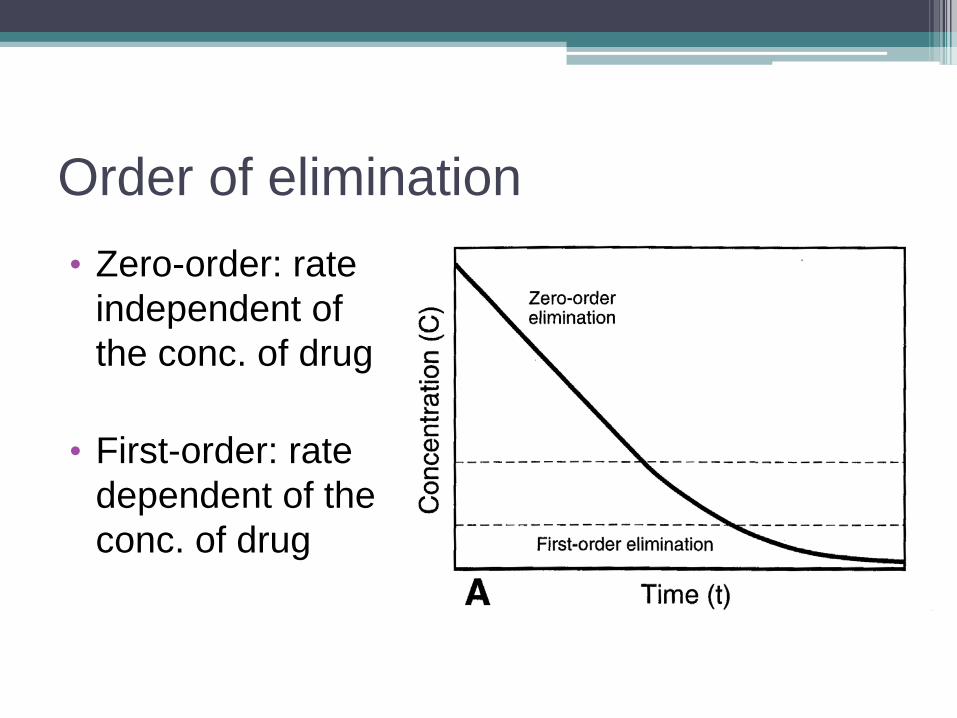
Order of elimination• Zero-order: rate
independent of the conc. of drug
• First-order: rate dependent of the conc. of drug

C=C0e-kt
log10C=log10C0-kt/2.303
Time course of drugconcentration following i.v. injection
t1/2
C0/2
Half life eliminationt1/2= 0.693/kwhere k is the elimination constant
Slope = - k/2.303
Sample calculation• 10mg dose of a drug (i.v.)• Its plasma concentration is recorded repeatedly• The logarithms of the conc. have been plotted against times (hr)
• A straight line: slope: -0.0751 and intercept: 0.301
∴ k= -2.303×(-0.0751) = 0.173 hr-1
C0 = antilog 0.301 = 100.301 = 2mg/Lt1/2= 0.693/k = 0.693/0.173 = 4.0 hrsVolume of distribution = 10mg/2mg/L = 5L
Duration of Drug Action• proportional to half life of elimination
• Pharmacological effect is attained if the conc. of the drug in the central compartment is higher than a minimal threshold
• the duration is extended by one half life if the dose is doubled.

Effect of doses on the duration of drug action
i.v. administration
oral administration
Common phenomenon:
Why we should keep taking the drug three/ four times a day even the half life of the drug is more than 18 hours?
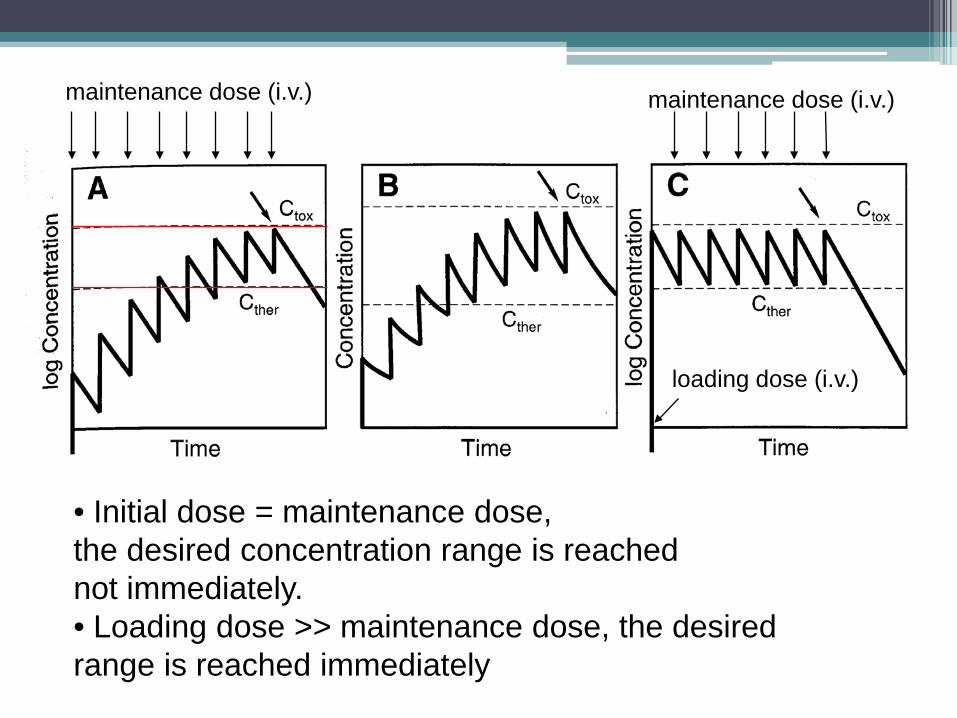
• Initial dose = maintenance dose, the desired concentration range is reachednot immediately.• Loading dose >> maintenance dose, the desired range is reached immediately
loading dose (i.v.)
maintenance dose (i.v.) maintenance dose (i.v.)

Clearance• A quantitative measure characterizing the rate of
removal of drugs from the body, as a result of ADME.
• Cl = kVd (where k is the elimination constant, Vdis the volume of distribution) (mL/min)
• The amount of drug in the body at any time is VdC; therefore the rate of elimination is a function of VdC, which is kVdC

• At steady state, the rate of input (Q) is equal to the rate of elimination
Q = k Vd Css where Css is the steady state conc.
= Cl × Css
Css
Rate of input
Rate of elimination

Calculation of the rate of drug infusion (i.v.)
Given: 70kg manCther = 2.0mg/Lt1/2 = 80 minVd = 49 L (70% of BW for TBW)
k = 0.693 / 80min = 0.0087 min-1
Desired infusion rate = kVC = 0.087×49×2 = 0.85mg/minClearance = kV = 0.43 L/minLoading dose = VCss = 49×2 = 98mg

• Bioavailability factor F =
•Calculation of the rate of drug oral intakemultiplied by bioavailability factor F
Drug conc. in plasma followinga single i.v. injection Drug conc. in plasma following
a single oral administration
AUC (oral)AUC (i.v.)
Drug interactions

Drug interactions• Most notable in elderly, due to polypharmacy,
multiple diseases
• Patients with chronic disorders or chronic use of drugs: hypertension, diabetes
• Specific drug classes: e.g. anticoagulants

Classification of Drug Interactions
• Consequence: beneficial or adverse
• Site: external or internal
• Mechanism: pharmacodynamic,
pharmacokinetic, physiological

Consequence• Beneficial:▫ Enhancing therapeutic effectiveness; or▫ Lowering toxicity or side effect▫ e.g. cancer therapy, infection, hypertension
therapy
• Adverse:▫ Reducing therapeutic effectiveness; or▫ Increasing toxicity or side effect▫ e.g. antidepressants + alcohol
vasodilator + beta blocker
Site of interaction• External:▫ Physicochemical incompatible: precipitation or
inactivation may occur if the drugs are mixed
• Internal:▫ Receptor level▫ DNA, RNA,▫ Cell membrane▫ E.g. metoprolol blocks β1-adrenoceptor agonists,
such as isoproterenol

Mechanism of pharmacodynamic interaction
• Response related• Barbiturates + alcohol: death rate due to
enhancing the CNS effects (hynopsis)
• Hydralazine: peripheral resistanceβ-blockers: can block reflex tachycardia induced by fall in peripheral resistanceOverall, augmenting the antihypertensive effect of hydralazine
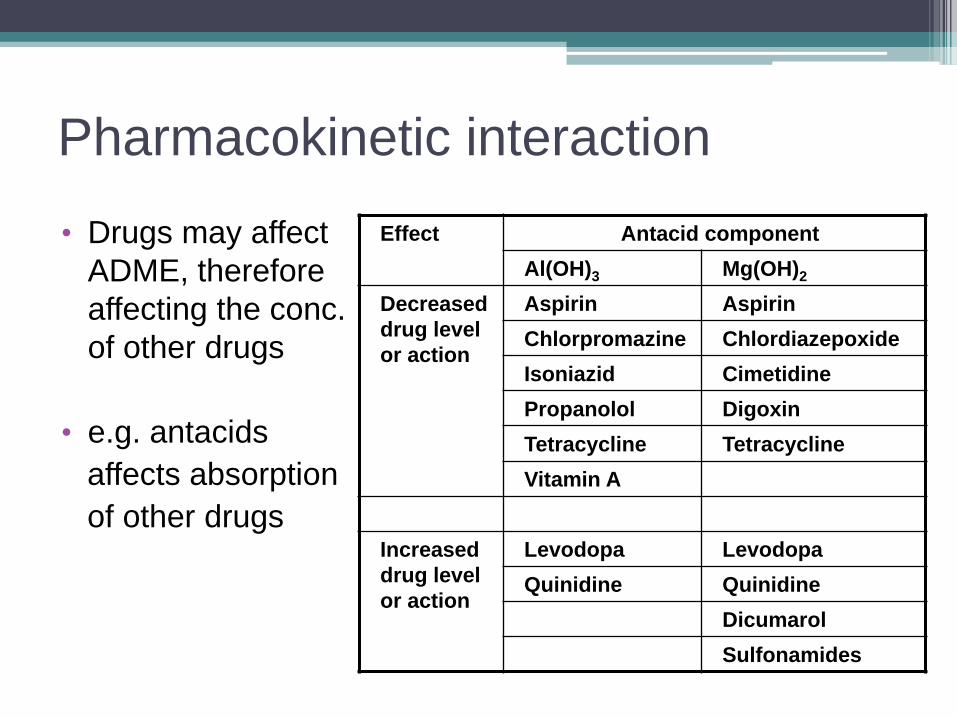
Pharmacokinetic interaction• Drugs may affect
ADME, therefore affecting the conc. of other drugs
• e.g. antacidsaffects absorptionof other drugs
Effect Antacid componentAl(OH)3 Mg(OH)2
Decreased drug level or action
Aspirin AspirinChlorpromazine ChlordiazepoxideIsoniazid CimetidinePropanolol DigoxinTetracycline TetracyclineVitamin A
Increased drug level or action
Levodopa LevodopaQuinidine Quinidine
DicumarolSulfonamides

Drugs affecting absorption and distribution• Changes in gastrointestinal motility▫ gastric emptying▫ intestinal motility
• Serum protein binding▫ Highly bound drugs may be displaced by other
high bound drugs:∴ higher level of free drug (may become toxic) ;
faster action; shorter half life

Drugs affecting biotransformation of other drugs• Cytochrome P450 enzymes• Drugs may induce enzymes:▫ Increases the rate of biotransformation of other drugs▫ Increases the rate of production of metabolites▫ Increases hepatic clearance▫ Decreases the drug half life▫ Decreases serum total and free drug concentrations▫ Decreases pharmacological effect▫ e.g. phenobarbital affects biotransformation of warfarin

Drugs affecting biotransformation of other drugs
• Drugs may inhibit enzymes:▫ Decreases the rate of biotransformation of other
drugs▫ Decreases the rate of production of metabolites▫ Decreases hepatic clearance▫ Increases the drug half life▫ Increases serum total and free drug
concentrations▫ Increases pharmacological effect▫ e.g. ethanol affects the biotransformation of
propranolol, amitriptyline, diazepam….etc.

Examples of drugs and specific isoforms of cytochrome P-450 which require adjustment of medication to prevent metabolic interaction

Notable drug-drug interactionsAlcohol
• affect absorption and metabolism of many drugse.g. anti-anxiety drugs, antidepressants (dangerous), narcotics, sleeping pills, antihistamines…etc.
Notable drug-drug interactionsContraceptives
• may interact with barbiturates, antibiotics, asthma medicine

Notable drug-drug interactionsNSAIDs
• NSAIDs impair control of coagulation in patients on oral anticoagulant therapye.g. aspirin on effect of warfarin
• NSAID counteracts hypotensive effect by some diuretics

Notable drug-drug interactionsAnticoagulant:
• interacts with antibiotics, aspirin, anticonvulsants, antidepressants, antifungal drugs, NSAIDS.

Notable drug-nutrient interactionsGrapefruit juice
• Naringen in converted to naringenin, and it appears to be the inhibitor of CYP3A4, CYP1A2 and CYP2A6.
• affects calcium channel blockers, statins, cyclosporine, caffeine

Drug tolerance and dependency

Tolerance• Need for increased amounts of the drug to
achieve the desired effect, or markedly decreased effect with the same amount of the substance

Pharmacodynamics:Drug action onreceptors


A graph of dose-response curve

Mechanism of tolerance• Reduction of the number of receptors• Reduction in the affinity of drugs on receptors• Increase in receptor internalization

More drug is needed to produce the same response

Example of tolerance
• Use of analgesics (e.g. morphine)
• Use of hypnotics (e.g. benzodiazepines)
• Use of alcohol

Drug dependence• Use of larger amount, over a long period, than intended
• Tolerance developed
• Withdrawal syndrome occur if the administration stops
• Unsuccessful effort to cut down and control its use
• Spending of a great deal of time/money getting and using the substance, or recovering from its effects
• Continuation of the use despite having persistent or recurrent physical or psychological problems.

Substance (drug) dependence
• Common motives: REWARDING
• Producing pleasure
• Relieving displeasure
• Winning approval of the user’s peers (friends, working partners, spouse)

Common drug dependence• Benzodiazepines (anxiolytics, hypnotics)• Ethanol• Opioids (morphine, heroin, fentanyl)• Cocaine• Amphetamines (methamphetamine, ecstasy)• Nicotine (tobacco in cigarettes, cigars)• Caffeine

Consequence of drug dependence
• Risk of overdose
• Risk of dangerous drug-drug interactions: effects on CNS
• Liver or kidney or lung damage
• Personal problem: economic, familial, social

Treatment of Drug Dependence• The goal: to stop the undesired drug-taking response from
continuing to be self-reinforcing
• Psychological and social therapy• Pharmacotherapy:▫ Use of specific blockers▫ Non-specific blockade of reinforcement (e.g.
antidepressants)▫ Substituting a less reinforcing and legally available drug
(e.g. methadone)▫ Aversive agents to produce an unpleasant effect (e.g.
disulfiram)• Exercising
Useful websites for drug search• Latest Publication: Pubmed
http://www.ncbi.nlm.nih.gov/pubmed/
• Hong Kong drug registrationhttp://www.psdh.gov.hk/eps/productSearchSimpleAction.do
Six Rights• RIGHT PATIENT• RIGHT DRUG• RIGHT DOSE• RIGHT ROUTE OF ADMINISTRATION• RIGHT TIME• RIGHT DOCUMENTATION

End

















