13
Probiotics and IBS Gail A. Cresci, PhD, RD, LD, CNSC Associate Staff Gastroenterology/Nutrition Cleveland Clinic Cleveland, OH
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | kristin-ball |
| View: | 217 times |
| Download: | 2 times |

Probiotics and IBSGail A. Cresci, PhD, RD, LD, CNSC
Associate Staff
Gastroenterology/Nutrition
Cleveland Clinic
Cleveland, OH
Disclosures
• Scientific Advisory Board – Advocare• Scientific Advisory Board - Covidien• Research Funding, Speaker’s Bureau - Metagenics

Probiotic
“Live microorganisms which when administered in adequate amounts confer a health benefit on the host”.
Food and Agricultural Org., WHO, 2001
“Good Little Bugs”

Prebiotics• Three Necessary Criteria of Ingredient
• Must be non-digestible by host enzymes• Must be fermented in the GI tract by anaerobic endogenous
bacteria in colon• Must be selective in the stimulation of intestinal microbiota
and of metabolic activity• Demonstration of criterion is difficult
• A prebiotic is not available to all bacterial species that inhabit GI ecosystem• Lactobacillus and Bifidobacterium considered indicator
organisms• Simple, naturally occurring or synthetic sugars
• Used as a carbon source by certain colonic bacteria for growth and metabolism
• Examples: Inulin, fructooligosaccharides (FOS), galactooligosaccharides (GOS), lactulose

Synbiotic
• Combination of probiotic and prebiotic• Meets criteria of probiotic and prebiotic• The prebiotic selectively supports the growth of the probiotic
component
• General Aim: • Support the probiotic and other indigenous beneficial
organisms by providing a preferred carbon and energy source to promote its growth
• Provide substrate for optimal or desired fermentation byproducts of probiotic
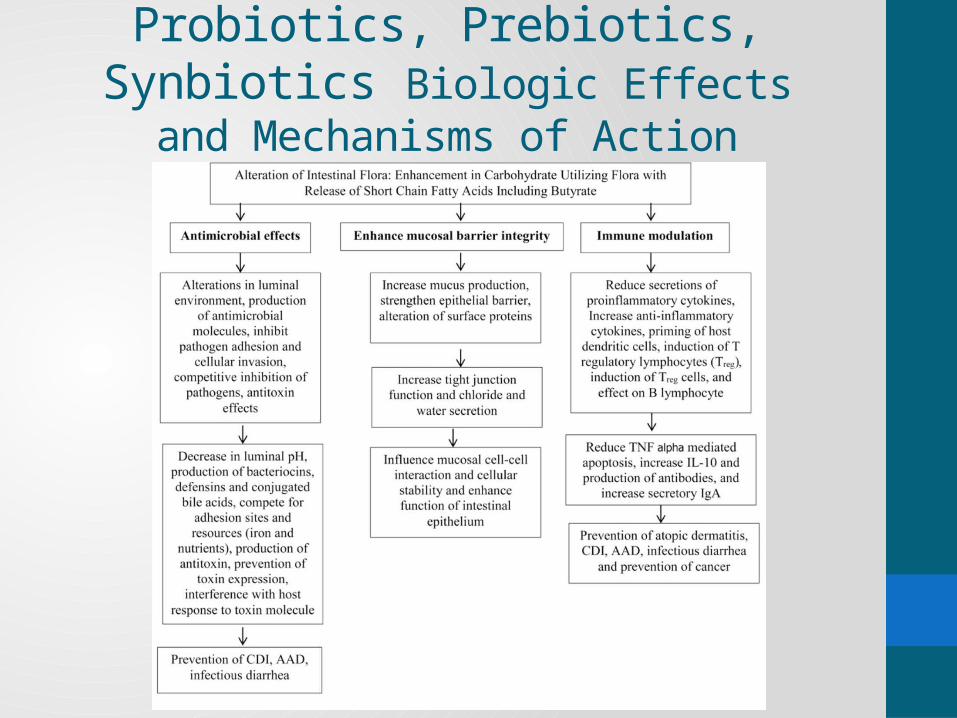
Probiotics, Prebiotics, Synbiotics Biologic Effects and Mechanisms of Action
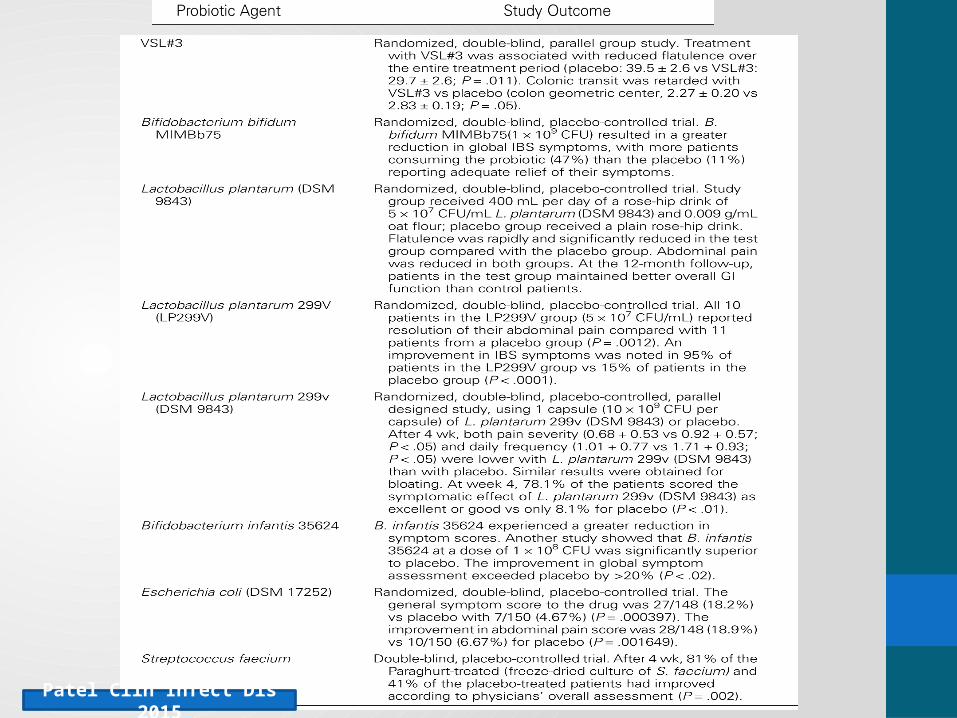
Patel Clin Infect Dis 2015

• Sept 2007-December 2013• 24 Clinical Trials [15 meta-analysis; 9 systematic review]• RCT, evaluating probiotic vs placebo in IBS improvement• Study quality evaluated
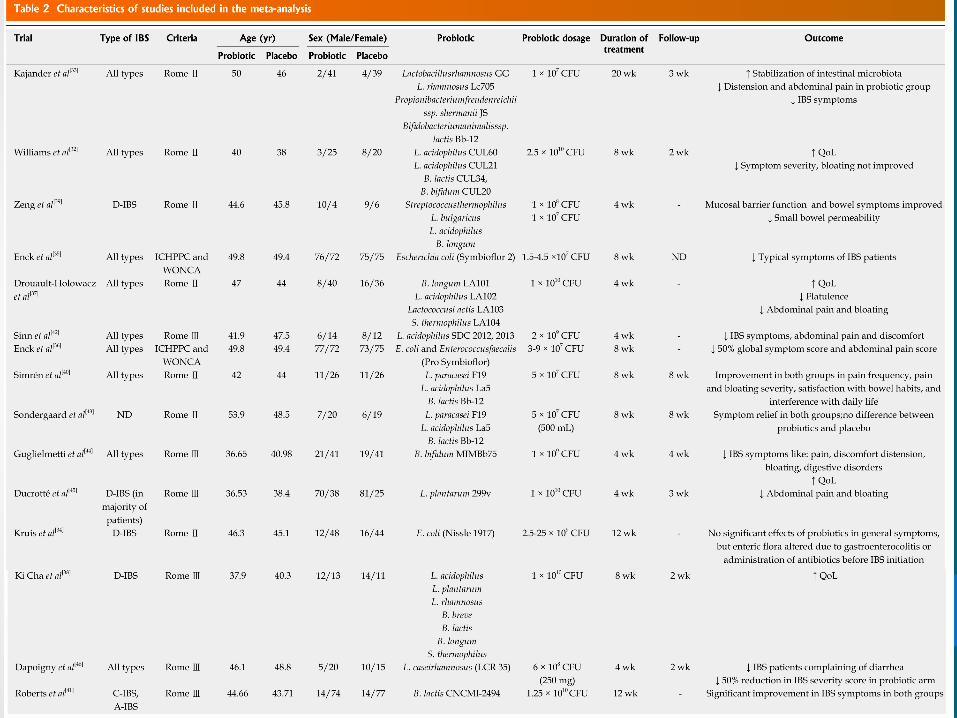

• Systematic review was performed to summarize non-eligible clinical trials for the meta-analysis that were excluded because of heterogeneity or different measurement scales for IBS symptoms
• All the nine studies were classified as randomized placebo-controlled trials. Four, six, and eight weeks of treatment with probiotics were reported.
Results
• 1793 patients in meta-analysis
• RR of responders to therapies:
• Abdominal pain score: two trials was 1.96 (95%CI: 1.14-3.36; P =
0.01)
• Global symptom score: two trials was 2.43 (95%CI: 1.13-5.21; P =
0.02)
• Adequate improvement of general symptoms: 7 trials (six studies)
was 2.14 (95%CI: 1.08-4.26; P = 0.03)
• Distension, bloating, and flatulence were evaluated using an IBS
severity scoring system in 3 trials (two studies)
• the standardized effect size of mean differences for probiotics therapy
was -2.57 (95%CI: -13.05--7.92)• Use of different scales to analyze mean differences of symptoms makes analysis difficult
• Further studies needed

Summary
• Probiotics reduce pain and symptom severity scores compared to placebo in IBS patients
• Studies inconsistent with design and outcome measurement
• Future studies needed with standardization• Longer treatment needed (8-12 week)• Ideal probiotic yet to be discovered

ReferencesPatel Clin Infect Dis 2015

















