P ulmonary artery (PA) stenosis is common inpatients with congenital heart disease, andinvasive PA procedures may account for up
to 20% of all catheter-based interventions in thispopulation (1–4). Despite the relative frequency ofPA interventions, little is known about how oftenthey yield a successful outcome. Although pro-cedural success rates remain unclear, there is
m the aDivision of Cardiology, Department of Medicine, Schneeweiss A
dical Center, New York, New York; bMid-America Heart Institute, Kansa
logy, Department of Pediatrics, Columbia University Medical Center, New
erican College of Cardiology’s National Cardiovascular Data Registry. Th
ips relevant to the contents of this paper to disclose. The views expressed
t necessarily represent the official views of the National Cardiovascular D
ntified at www.CVQuality.ACC.org/NCDR.
nuscript received November 17, 2015; revised manuscript received Decem
increasing evidence that adverse events may becommon (3,5–8). In one of the few multicenterstudies of PA interventions, 22% of patients experi-enced an adverse event and 10% experienced ahigh severity event (4). Given the high rates of pro-cedural complications and poorly defined metrics ofprocedural success, additional data are needed toimprove patient selection.
dult Congenital Heart Center, Columbia University
s City, Missouri; and the cDivision of Pediatric Car-
York, New York. This research was supported by the
e authors have reported that they have no relation-
in this paper represent those of the authors and do
ata Registry or its associated professional societies
Lewis et al. J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6
Success and Complication Rates in PA Stenting M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5
1328
Optimizing patient selection for PA stent-ing is obscured by a lack of a standardizeddefinition of procedural success, the pluralityof indications, and the paucity of multi-institutional studies. Although previousstudies have classified successful outcomes ofPA stenosis treatment as a >50% increase inPA diameter post-procedure and/or >20%
decrease in the ratio of subpulmonic to aortic pres-sure, this definition has never been validated and maynot apply to patients with a single ventricle (9). Theheterogeneity of indications also complicates com-parisons between patients, especially in the setting ofsmall, single-center studies in which lesion locationand morphological severity are not standardized. As aresult, it remains challenging to define the patientparameters that provide the greatest probability of asuccessful outcome while minimizing the risk ofcomplication.
TABLE 1 Adverse Events Considered “Major”
� Cardiac arrest
� Unplanned surgery
� Major bleeding event
� Device embolization
� Cardiac tamponade
� Event requiring left ventricular assist device/extracorporealmembrane oxygenation (nonelective)
� Embolic stroke
� Air embolus
� Airway event requiring intubation
SEE PAGE 1336
The IMPACT (Improving Pediatric and AdultCongenital Treatment) Registry is a multi-institutional initiative to develop performance andquality metrics for patients with congenital heartdisease undergoing diagnostic catheterizations andcatheter-based interventions (10). In participationwith the IMPACT Registry, the goal of the presentstudy was to determine the rate of procedural successand adverse events for PA stenting according toindication and procedural characteristic.
METHODS
Data for this study were obtained from the NationalCardiovascular Data Registry–IMPACT Registry,which comprises data on pediatric and adultcongenital heart disease catheterizations obtainedfrom centers that have agreed to enrollment. Specificdetails regarding the registry have been publishedpreviously (10,11). Definitions for exposures and out-comes of interest were pre-specified and collected inaccordance with a strict quality program previouslydescribed for the National Cardiovascular Data Reg-istry (12). For the purposes of the present study, allpertinent data related to PA procedures werereviewed before formulation of the analytic plan.Endpoints were pre-specified as defined later.
STUDY POPULATION AND EXPOSURES OF INTEREST. Thestudy assessed IMPACT data collected during cardiaccatheterizations for PA stenting in patients enrolledfrom January 2011 to January 2014. All patientswho underwent PA stenting were eligible for inclu-sion. Demographic, procedural, and historical data
were available for each visit. Procedure status wasdefined to indicate if a procedure was performedemergently, urgently, electively, or as a salvage pro-cedure. Patients were grouped into 1 of 5 diagnosticcategories. Group 1 included all patients with tetral-ogy of Fallot (TOF) and TOF-like anatomy (includingpatients with pulmonary atresia, “hemitruncus,” or aTOF-type double outlet right ventricle); group 2comprised all patients with a primary PA abnormality;group 3 included all nongroup 1 patients with a con-otruncal abnormality; group 4 comprised all patientswith a single ventricle; and group 5 included allother patients. Procedural indication was defined byeach patient’s treating physician and included PAgradient, PA flow discrepancy, right ventricularhypertension/dysfunction, angiographic narrowing,and pulmonary insufficiency. Procedure-specific data,including defect location and type, pre- andpost-procedure proximal and distal PA systolic pres-sures, and pre- and postprocedure PA diameter, werealso collected. Data pertaining to stent type were notstandardized and incomplete, and they were not usedin the analysis. Data on adverse events, includingmortality, were collected per admission and sub-divided into major adverse events (MAEs) based onseverity (Table 1).
OUTCOMES AND DEFINITIONS OF PROCEDURAL
SUCCESS. Given the lack of a standardized definitionfor PA stenting procedural success, 2 definitions werepre-specified for patients with biventricular hearts,and a separate definition was pre-specified for pa-tients with a single ventricle (Table 2). The first defi-nition for patients with a biventricular heart wasextracted from previous studies; it represented ahistorical definition of procedural success and con-sisted of improvements in subpulmonic ventricularpressure and PA diameter.
A second definition of procedural success wascreated and implemented to account for potentialdeficits in the historical definition. In addition tometrics based on changes in ventricular pressure andPA size, definition 2 also included a >50% gradient
TABLE 2 Definitions of Procedural Success
Biventricular hearts
Definition 1:� >50% increase in pre-procedure diameter and/or� >20% decrease in subpulmonic ventricular pressure
Definition 2:� Post-stent PA vessel diameter/pre-stent distal PA
diameter $0.8 and/or� >50% decrease in gradient across the stenosis and/or� >25% decrease in subpulmonic ventricular pressure
Single ventricle palliation
� Post-stent PA vessel diameter/pre-stent distal PA diameter $1
PA ¼ pulmonary artery.
TABLE 3 Patient Demographic and Procedure Characteristics
(N ¼ 1,183)
Male 663 (57)
Age
<30 days 25 (2)
30 days to <1 yr 212 (18)
1 yr to <18 yrs 787 (67)
$18 yrs 150 (13)
Missing data 9 (1)
Weight, kg
2.5–4 49 (4)
>4–10 240 (21)
>10–169 882 (75)
Missing data 12 (1)
Prior catheterization 902 (77)
Prior cardiac surgery 1,050 (90)
>1 Cardiac surgeries 580 (67)
Syndromes
Alagille 15 (2)
Noonan 3 (0.3)
Williams-Beuren 6 (0.6)
Congenital rubella 2 (0.2)
Procedure indications
PA gradient 412 (35)
RV hypertension 175 (15)
Pulmonary insufficiency 41 (4)
PA flow discrepancy 195 (17)
Angiographic narrowing 360 (30)
Procedure status
Elective 1,024 (88)
Urgent 108 (9)
Emergency 28 (2)
Salvage 8 (1)
Pre-procedure creatinine, mg/ml 0.5 � 0.4
Pre-procedure hemoglobin, g/dl 13 � 2.1
Coagulation disorder 16 (2)
Renal insufficiency 17 (2)
Systemic ventricular systolic pressure, mm Hg 86.0 � 14.5
PA systolic pressure, mm Hg 37.3 � 20.3
Pulmonary ventricular systolic pressure, mm Hg 56.4 � 21.8
Pulmonary vascular resistance, WU 2.5 � 2.3
Values are n (%) or mean � SD. All listed values are per-procedure.
PA ¼ pulmonary artery; RV ¼ right ventricular.
J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6 Lewis et al.M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5 Success and Complication Rates in PA Stenting
1329
reduction across the stenosis to identify proceduralsuccess in patients with elevated pressure in thecontralateral lung. In addition, the ratio of the post-procedure in-stent diameter to the pre-proceduredistal diameter was used as a metric to characterizeimprovement in PA size. This metric was establishedin place of a 50% increase in stenotic diameter toclarify situations in which improvements in post-procedure PA vessel diameter may overestimate im-provements in PA vessel size. Because of the low-flowstate across the pulmonary arteries in patients with asingle ventricle, only procedures with normalizationof the vessel diameter (i.e., a ratio $1.0) wereconsidered a success. To account for possible post-stenotic dilation in patients with biventricular circu-lation, a ratio of the post-procedure in-stent diameterto pre-procedure distal diameter >0.8 was considereda success.
COVARIATES. Patient factors that could affect pro-cedural success were identified based on clinicalrationale and previous studies. Specific covariatespre-specified for inclusion in multivariate models ofprocedural success were patient weight, age, proce-dural indication, and procedure status. Additionalcovariates were included in multivariate models toinclude any variables that reached a p value <0.20 inthe analysis (13). For multivariate models of adverseevents, pre-specified variables included patientweight, age, procedural indication, procedural status,single ventricle status, and procedural success.Separate multivariate models for adverse events weremade for each procedural definition of success inpatients with biventricular hearts.
STATISTICAL ANALYSIS. Data are presented as mean� SD for continuous data and number (%) for cate-gorical data. Given the nature of the database, pro-cedures were used as the unit of analysis. Unadjustedcomparisons were made with either the chi-squaretest or the Student t test. Modified hierarchical Pois-son regression was used to estimate the risk ratio (RR)
of covariates predicting the adverse events or successendpoints. We used a random intercept model to ac-count for the clustering of patients in hospitals, withno additional corrections for multiple procedureswithin patients or admissions. A p value of 0.05 wasused to determine statistical significance. SAS version9.3 (SAS Institute, Inc., Cary, North Carolina) wasused for all analyses.
RESULTS
Between January 2011 and January 2014, data werecollected on 1,183 PA stenting procedures at 59
TABLE 4 Univariate
Ostial stenosis
Procedure status
Elective
Urgent
Emergency
Salvage
Distal obstruction
Pre-procedure distaldiameter, mm
Prior catheterization
Diagnosis
TOF/TOF-like
Primary PA abnorma
Conotruncal abnorm
Other
No diagnosis
Values are n (%) or meanincluded, but were not sig
PA ¼ pulmonary artery;
FIGURE 1 Procedural Success Rates
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Proc
edur
e Su
cces
s Rat
es
Overall PA Gradient Right VentricularDysfunction
PA Flowdiscrepancy
Angiographicnarrowing
PulmonaryInsufficiency
Definition 1 Definition 2 Single Ventricle
75%
84%
75% 74%
85%
70%
78%85%
64%
81%
88%
77%
70%
79%78%
70%76%
There was no significant difference between success rates for pulmonary artery (PA) stenting according to procedure indication for
any definition.
Lewis et al. J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6
Success and Complication Rates in PA Stenting M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5
1330
institutions across 1,001 unique admissions and 974patients. Table 3 presents demographic data andbaseline characteristics. Mean patient age was 8.6 �9.8 years, and mean patient weight was 28.7 � 26.2kg. Twenty patients (2%) had planned cardiac surgeryduring their admission. Overall, 211 (18%) procedureswere performed in patients with TOF or TOF-like
Comparison of Definitions of Procedural Success
Definition 1* Definition 2* Single Ventricle*
Success(n ¼ 689) p Value
Success(n ¼ 774) p Value
Success(n ¼ 196) p Value
349 (81) <0.001 379 (88) 0.002 NS
0.02 0.01 NS
631 (76) 707 (85)
47 (77) 52 (85)
5 (42) 7 (58)
1 (33) 1 (33)
133 (75) 0.02 NS NS
9.3 � 4.6 0.04 NS 7.5 � 3.3 0.02
490 (72) 0.001 NS NS
0.03 NS
155 (74)
lity 146 (78)
ality 99 (85)
100 (68)
109 (75)
� SD. *Age, sex, weight, prior cardiac surgery, indication, and defect location werenificant, in each model.
TOF ¼ tetralogy of Fallot.
diagnoses (group 1); 182 (15%) procedures were per-formed in patients with a primary PA stenosis (group2); 110 (9%) procedures were performed in patientswith conotruncal abnormalities (group 3); 262 (22%)procedures were performed in patients with a singleventricle (group 4); and 234 (20%) procedures wereperformed in patients with a different diagnosis(group 5). Diagnoses were not available for 184patients.
Data on PA stenting location were available for1,182 procedures with PA stenting in the right PA in395 lesions (33%) and in the left PA in 787 lesions(67%). A total of 510 (43%) procedures were per-formed on an ostial PA stenosis, whereas a distalobstruction was present in 188 (16%) procedures. Themean pre-procedure PA diameter of the stenoticsegment was 5.4 � 3.4 mm, and the mean pre-procedure distal diameter was 9.0 � 4.0 mm. Themean post-procedure PA in-stent diameter was 9.5 �4.0 mm.
The overall rate of procedural success for pro-cedures in biventricular hearts was 76% (95% confi-dence interval [CI]: 73% to 79%) for definition 1 and84% (95% CI: 82% to 86%) for definition 2. There wasa significant difference in the number of proceduresclassified as successful for each definition (p < 0.001).Patients with a single ventricle had a successfulintervention in 75% (95% CI: 70% to 80%) of cases.Procedural success rates according to definition andindication are shown in Figure 1. Notably, there wasno significant difference in procedural success by
PA gradient vs. RV hypertension 1.24 (0.78–1.95) 0.36
PA flow discrepancy vs. RV hypertension 1.31 (0.71–2.42) 0.40
Angiographic narrowing vs. RV hypertension 1.38 (0.87–2.18) 0.17
*Weight, age at procedure, procedure status, prior cardiac catheterizations, and diagnosis were included, but notsignificant, in this model. †Weight, sex, and multiple cardiac surgeries were included, but not significant, in thismodel. ‡Weight, age at procedure, procedure status, and right versus left PA were included, but not significant, inthis model.
CI ¼ confidence interval; PI ¼ pulmonary insufficiency; RR ¼ risk ratio; other abbreviations as in Table 3.
J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6 Lewis et al.M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5 Success and Complication Rates in PA Stenting
1331
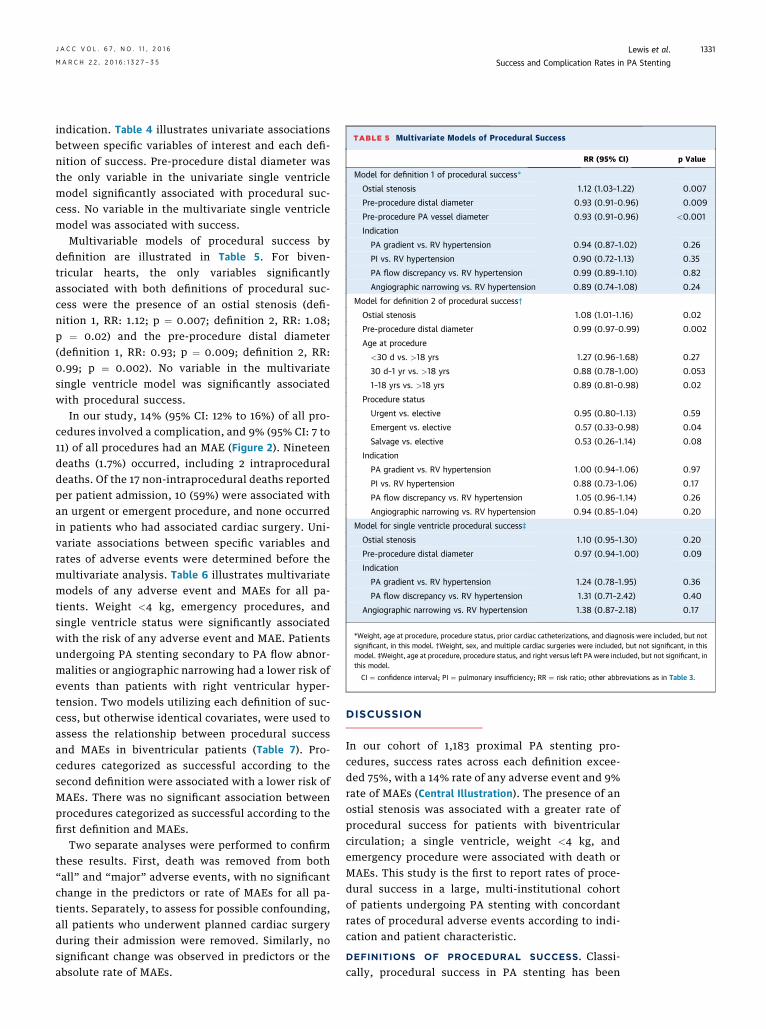
indication. Table 4 illustrates univariate associationsbetween specific variables of interest and each defi-nition of success. Pre-procedure distal diameter wasthe only variable in the univariate single ventriclemodel significantly associated with procedural suc-cess. No variable in the multivariate single ventriclemodel was associated with success.
Multivariable models of procedural success bydefinition are illustrated in Table 5. For biven-tricular hearts, the only variables significantlyassociated with both definitions of procedural suc-cess were the presence of an ostial stenosis (defi-nition 1, RR: 1.12; p ¼ 0.007; definition 2, RR: 1.08;p ¼ 0.02) and the pre-procedure distal diameter(definition 1, RR: 0.93; p ¼ 0.009; definition 2, RR:0.99; p ¼ 0.002). No variable in the multivariatesingle ventricle model was significantly associatedwith procedural success.
In our study, 14% (95% CI: 12% to 16%) of all pro-cedures involved a complication, and 9% (95% CI: 7 to11) of all procedures had an MAE (Figure 2). Nineteendeaths (1.7%) occurred, including 2 intraproceduraldeaths. Of the 17 non-intraprocedural deaths reportedper patient admission, 10 (59%) were associated withan urgent or emergent procedure, and none occurredin patients who had associated cardiac surgery. Uni-variate associations between specific variables andrates of adverse events were determined before themultivariate analysis. Table 6 illustrates multivariatemodels of any adverse event and MAEs for all pa-tients. Weight <4 kg, emergency procedures, andsingle ventricle status were significantly associatedwith the risk of any adverse event and MAE. Patientsundergoing PA stenting secondary to PA flow abnor-malities or angiographic narrowing had a lower risk ofevents than patients with right ventricular hyper-tension. Two models utilizing each definition of suc-cess, but otherwise identical covariates, were used toassess the relationship between procedural successand MAEs in biventricular patients (Table 7). Pro-cedures categorized as successful according to thesecond definition were associated with a lower risk ofMAEs. There was no significant association betweenprocedures categorized as successful according to thefirst definition and MAEs.
Two separate analyses were performed to confirmthese results. First, death was removed from both“all” and “major” adverse events, with no significantchange in the predictors or rate of MAEs for all pa-tients. Separately, to assess for possible confounding,all patients who underwent planned cardiac surgeryduring their admission were removed. Similarly, nosignificant change was observed in predictors or theabsolute rate of MAEs.
DISCUSSION
In our cohort of 1,183 proximal PA stenting pro-cedures, success rates across each definition excee-ded 75%, with a 14% rate of any adverse event and 9%rate of MAEs (Central Illustration). The presence of anostial stenosis was associated with a greater rate ofprocedural success for patients with biventricularcirculation; a single ventricle, weight <4 kg, andemergency procedure were associated with death orMAEs. This study is the first to report rates of proce-dural success in a large, multi-institutional cohortof patients undergoing PA stenting with concordantrates of procedural adverse events according to indi-cation and patient characteristic.
DEFINITIONS OF PROCEDURAL SUCCESS. Classi-cally, procedural success in PA stenting has been
FIGURE 2 Major Adverse Events
70
60
50
40
30
20
10
0
Num
ber o
f Eve
nts
(% T
otal
)
16%
17
57%
62
7%
8
7%
85
5%3
3%3
3%1
1%1
1% 0 0
Death
Bleeding Eve
nt
Device
Embolizati
on
Airway
Event R
equirin
g Intubati
on
Event r
equirin
g ECMO
Cardiac
Arrest
Unplanned
Cardiac
Surgery
Other Surgery
Due to Cath
Complicati
on
Air Embolus
Tamponad
e
Embolic Stro
ke
Of all procedures performed, 9% were associated with a major adverse event; bleeding was the most common, followed by death.
TABLE 6 Multivariate Model of Adverse Events: All Patients
Major Adverse Events Any Adverse Event
RR(95% CI) p Value
RR(95% CI) p Value
Weight
$4 kg vs. <4 kg 0.34 (0.14–0.83) 0.018 0.48 (0.24–0.96) 0.037
Age at procedure
$30 d vs. <30 d 0.79 (0.27–2.31) 0.67 0.84 (0.36–1.96) 0.68
Indication
PA gradient vs. RVhypertension
0.83 (0.49–1.39) 0.47 0.96 (0.63–1.47) 0.88
PI vs. RV hypertension 1.19 (0.51–2.75) 0.69 0.88 (0.39–2.0) 0.77
PA flow discrepancy vs. RVhypertension
0.48 (0.25–0.91) 0.025 0.62 (0.37–1.04) 0.07
Angiographic narrowingvs. RV hypertension
0.43 (0.25–0.76) 0.004 0.66 (0.41–1.04) 0.07
Procedure status
Emergency vs. others 4.0 (2.31–6.92) <0.001 3.21 (1.99–5.20) <0.001
Single ventricle status 2.26 (1.54–3.33) <0.001 1.51 (1.09–2.09) 0.013
Abbreviations as in Tables 3 and 5.
Lewis et al. J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6
Success and Complication Rates in PA Stenting M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5
1332
defined by an improvement in PA diameter, a decreasein right ventricular pressure, or an improvement inpulmonary blood flow (7,9,14). These criteria may notapply equally to all patients with congenital heartdisease undergoing PA rehabilitation. In patients witha single ventricle, for example, the goal of PA stentingis generally normalization of the PA diameter relativeto nonstenotic segments. In addition, by failing toinclude a change in PA gradient, the standard defini-tion might not account for lesions stented to diminishpulmonary hypertension in the contralateral lung. Insuch cases, treating improvements in vessel diameteras a ratio relative to the unaffected segment or asan improvement in pressure gradient may provide amore accurate assessment of post-procedure success.Because the optimal definition of procedural success isnot known, we added an additional definition of suc-cess to account for these considerations. In so doing,we were able to select for covariates that met bothdefinitions of success, minimizing the contribution ofprocedures that increased PA diameter but failed to
TABLE 7 Multivariate Model of Major Adverse Events: Biventricular Patients
PA gradient vs. RV hypertension 0.87 (0.49–1.54) 0.62
PI vs. RV hypertension 1.34 (0.52–3.47) 0.54
PA flow discrepancy vs. RV hypertension 0.30 (0.12–0.75) 0.011
Angiographic narrowing vs. RV hypertension 0.11 (0.03–0.48) 0.003
*Age and weight were included, but were not significant, in each model.
Abbreviations as in Tables 3 and 5.
J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6 Lewis et al.M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5 Success and Complication Rates in PA Stenting
1333
improve PA gradient, the ratio of the stenotic segmentto the distal segment, or the subpulmonic ventricularpressure.
The majority of covariates did not have a significantassociation with procedural success according toeither definition. Although certainmetrics of PA vesselsize, such as pre-procedure distal diameter, were sig-nificant, the magnitude of the effect was sufficientlysmall that it is unlikely that these results were clini-cally meaningful. The presence of an ostial stenosiswas significantly associated with higher odds of asuccessful procedure according to both definitions.Because an ostial lesion may affect a larger vascularbed, successful stenting may have a more pronouncedeffect on reducing elevated right ventricular pres-sures. Ostial lesions are also generally easier to access,and operators may feel more comfortable using higherpressures during dilation and stent deployment. As aresult, successful stenting of ostial lesions may besimpler technically and therefore less affected by theheterogeneity of this cohort. Finally, because vesselangulation contributes to narrowing in ostial lesions,they may be intrinsically more amenable to stentingthan mid- and distal-PA lesions, which are more likelyto be scar related.
Indication was not a statistically significant predic-tor of procedural success; however, patients who un-derwent stenting secondary to an angiographicnarrowing or PA flowdiscrepancywere at lower risk foran MAE. Unfortunately, the lack of a clear, standard-ized definition for indication complicates interpreta-tion of these findings and may have led tomisclassification bias. In addition, the unequal distri-bution of patients in each category and the heteroge-neous nature of each group increase the probability ofconfounding, further limiting our ability to infer as-sociations between indication and outcome. There-fore, although these results were the first to suggest apossible association between indication and adverseevents in PA stenting, future studies with standard-ized indications are needed to validate our findings.
PREDICTORS OF ADVERSE EVENTS AND PROCEDURAL
SUCCESS. In our cohort of patients undergoing PAstenting, 14% of procedures were associated with anadverse event, and 9% were associated with eitherdeath or an MAE. These rates are similar to those re-ported in previous studies of outcomes in PA rehabil-itation (4) but are the first to confirm such high rates forPA stenting alone. Similar to earlier studies, we foundthat low patient weight and nonelective status wereassociated with a higher rate of adverse events. How-ever, our study was the first to identify single ventriclestatus as an independent risk factor. We found that
patients with a single ventricle were 2.3 times morelikely to have an MAE than patients with biventricularcirculation, even after controlling for procedure sta-tus, patient age, and patient weight. These resultssuggest that additional measures should be used tomitigate risk in patients with a palliated singleventricle. Prospective studies designed to identifymodifiable risk factors and the impact of balloon type,stent type, operator experience, and center volume areneeded in this population.
Successful interventions did not increase the riskfor adverse events. Instead, we found that patientswho had a procedural success according to the seconddefinition were significantly less likely to have anMAE. Anatomic factors that decrease the probabilityof a successful outcome may also play a role indefining which patients are at highest risk for anMAE. Long-term follow-up is necessary to validatethese results and to further inform how successful PAinterventions are classified in this population.
In this study, current practice standards for PAstenting resulted in successful procedures 75% to 84%of the time. These findings are consistent with thosereported in previous studies, in which success rateshave varied from 70% to 98% (14–17). We also found anassociated rate of 9% for death or MAE. Because ourresults did not account for adverse events that occurafter the index hospitalization, the relative rate ofsuccessful procedures to adverse events may be evenlower. Although long-term follow-up is necessary torefine these data, our results suggest that PA stenting
CENTRAL ILLUSTRATION PA Stenting: Rates and Predictors of Procedural Success and Adverse Events
Lewis, M.J. et al. J Am Coll Cardiol. 2016; 67(11):1327–35.
Rates and significant multivariate predictors of successful pulmonary artery (PA) stenting are displayed for each definition of success. Rates of “any” and “major” adverse
events are shown, in addition to significant predictors of major adverse events.
Lewis et al. J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6
Success and Complication Rates in PA Stenting M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5
1334
is associated with significant risk. Furthermore, giventhat PA stenting can complicate subsequent cardiacsurgery, an improved understanding of optimal pa-tient selection is needed. Although lesion locationseemed to play a larger role than demographic,
clinical, or historical covariates in defining which pa-tients were mostly likely to benefit from PA stenting,the presence of an ostial stenosis was associated withonly a modest improvement in the rate of proceduralsuccess. These results highlight the need for
PERSPECTIVES
COMPETENCY IN PATIENT CARE AND PROCEDURAL
SKILLS: PA stenting can be successfully achieved in most cases,
but adverse events are common. Patients with ostial PA stenosis
have a higher probability of successful outcomes than those with
more distal PA lesions, and patients undergoing emergency
procedures, those with a single ventricle, and those with low
weight will face a higher risk of MAEs.
TRANSLATIONAL OUTLOOK: Additional research is neces-
sary to define the rate of late adverse events after PA stenting
and the influence of stent type on procedural outcomes.
J A C C V O L . 6 7 , N O . 1 1 , 2 0 1 6 Lewis et al.M A R C H 2 2 , 2 0 1 6 : 1 3 2 7 – 3 5 Success and Complication Rates in PA Stenting
1335
additional, prospective research powered to ascertainmodifiable risk factors in patients undergoing PAstenting.
STUDY LIMITATIONS. This study did not addresslong-term outcomes of PA stenting. In addition, wewere limited to data made available through theregistry and were unable to risk-stratify patientsbased on pre-procedure indices of ventricular andpulmonary function. Given the nature of the registry,limited data were available regarding stent andballoon type, and data pertaining to MAEs could notbe further adjudicated. Furthermore, we were unableto assess for changes in pulmonary blood flow fordefining successful interventions and were unable todiscern between mortality from procedures and thehospitalization. Nonetheless, this study is the largestto assess the rates of procedural success and adverseevents exclusively in patients with congenital heartdisease undergoing PA stenting.
CONCLUSIONS
In our study, PA stenting had a success rate >75%with a 14% risk of any adverse event and a 9% risk ofdeath or MAE. Biventricular patients with an ostialstenosis have a higher probability of a successfuloutcome; patients with a single ventricle, weight<4 kg, or emergency procedure have a higher risk ofdeath or MAE. In addition, patients with a post-procedure ratio of in-stent minimum to distal PAdiameter $0.8, a >50% decrease in gradient across
the stenosis, or >25% decrease in subpulmonic ven-tricular pressure were less likely to incur an MAE.These findings should inform referring physiciansand operators regarding patient selection before PAstenting. Given the high rate of adverse events,further study is necessary to elucidate mechanisms tominimize patient risk and further validate definitionsof procedural success.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Matthew J. Lewis, Division of Cardiology, ColumbiaUniversity Medical Center, Herbert Irving Pavilion, 161Fort Washington Avenue, Suite 627, New York, NewYork 10032. E-mail: [email protected].
RE F E RENCE S
1. Rothman A, Perry SB, Keane JF, Lock JE. Balloondilation of branch pulmonary artery stenosis.Semin Thorac Cardiovasc Surg 1990;2:46–54.
2. Rocchini AP, Kveselis D. The use of balloonangioplasty in the pediatric patient. Pediatr ClinNorth Am 1984;31:1293–305.
3. Shaffer KM, Mullins CE, Grifka RG, et al. Intra-vascular stents in congenital heart disease: short-and long-term results from a large single-centerexperience. J Am Coll Cardiol 1998;31:661–7.
4. Holzer RJ, Gauvreau K, Kreutzer J, et al. Balloonangioplasty and stenting of branch pulmonaryarteries: adverse events and procedural charac-teristics: results of a multi-institutional registry.Circ Cardiovasc Interv 2011;4:287–96.
5. Bergersen L, Marshall A, Gauvreau K, et al.Adverse event rates in congenital cardiaccatheterization—a multi-center experience. Cath-eter Cardio Interv 2010;75:389–400.
6. Law MA, Shamszad P, Nugent AW, et al. Pul-monary artery stents: long-term follow-up. Cath-eter Cardiovasc Interv 2010;75:757–64.
7. Kenny D, Amin Z, Slyder S, Hijazi ZM. Medium-term outcomes for peripheral pulmonary artery
stenting in adults with congenital heart disease.J Interv Cardiol 2011;24:373–7.
8. McMahon CJ, El Said HG, Vincent JA, et al.Refinements in the implantation of pulmonaryarterial stents: impact on morbidity and mortalityof the procedure over the last two decades. Car-diol Young 2002;12:445–52.
9. Gentles TL, Lock JE, Perry SB. High pressureballoon angioplasty for branch pulmonary arterystenosis: early experience. J Am Coll Cardiol 1993;22:867–72.
10. Martin GR, Beekman RH, Ing FF, et al. TheIMPACT registry: improving pediatric and adultcongenital treatments. Semin Thorac CardiovascSurg Pediatr Card Surg Annu 2010;13:20–5.
11. O’Byrne ML, Glatz AC, Shinohara RT, et al. Ef-fect of center catheterization volume on risk ofcatastrophic adverse event after cardiac cathe-terization in children. Am Heart J 2015;169:823–32.e5.
12. Messenger JC, Ho KK, Young CH, et al. TheNational Cardiovascular Data Registry (NCDR) dataquality brief: the NCDR data quality program in2012. J Am Coll Cardiol 2012;60:1484–8.
13. Maldonado G, Greenland S. Simulation study ofconfounder-selection strategies. Am J Epidemiol1993;138:923–36.
14. Ing FF, Khan A, Kobayashi D, et al. Pulmonaryartery stents in the recent era: immediate and in-termediate follow-up. Catheter Cardiovasc Interv2014;84:1123–30.
15. O’Laughlin MP, Slack MC, Grifka RG, et al.Implantation and intermediate-term follow-up ofstents in congenital heart disease. Circulation1993;88:605–14.
16. Bergersen L, Jenkins KJ, Gauvreau K, Lock JE.Follow-up results of cutting balloon angioplastyused to relieve stenoses in small pulmonary ar-teries. Cardiol Young 2005;15:605–10.
17. Fogelman R, Nykanen D, Smallhorn JF, et al.Endovascular stents in the pulmonary circul-ation. Clinical impact on management andmedium-term follow-up. Circulation 1995;92:881–5.
KEY WORDS cardiac catheterization,congenital heart disease, pulmonary arterystenosis, success rates