ALBURY WODONGA HEALTH © PRO1483 – Page 1
Procedure
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR
X-RAY EXAMINATIONS
Definition / Description:
In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging, Albury Wodonga
Health Wodonga Campus (AWHWC) requires all medical imaging referrals that will use medical
radiation, to be justified and optimised.
Personnel Able to Perform or Assist with Procedure:
Radiation Medical Practitioner.
Operators
Expected Outcomes:
To assist in implementation of the As Low As Reasonably Achievable (ALARA) principle.
To reduce inappropriate or over irradiation of patients.
To provide guidelines for appropriate investigations.
To comply with requirements of the Victorian Radiation Act 2005.
Equipment:
N/A.
Process Standards:
WHY ARE GUIDELINES AND REFERRAL CRITERIA REQUIRED?
A useful investigation is one in which the result – positive or negative – will alter management or add
confidence to the clinician’s diagnosis. A significant number of radiological investigations do not fulfil
these aims and may add unnecessarily to patient irradiation. The chief causes of this are:
Repeating investigations which have already been performed.
Investigating when the results are unlikely to affect patient management.
Investigating too often.
Requesting the wrong investigation.
Failing to provide appropriate clinical information and questions that the investigation should
answer.
Over-investigating.
SCOPE:
This document provides specific protocols that should be applied to medical imaging referrals prior to
any X-ray examination or procedure.
ROLES AND RESPONSIBILITIES:
It is the responsibility of the Radiation Medical Practitioner to define whether an X-ray examination is
justified. It is the role of the Operator to assess a referral and determine whether the X-ray falls within
the criteria of the generic justification protocol or whether it should be justified on an individual basis.
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 2
DEFINITION OF JUSTIFICATION:
A radiation procedure is justified when it is determined that the radiation exposure will produce
sufficient benefit to the exposed individual to offset the risk associated with the radiation exposure. In
determining the net benefit from a radiation procedure, the Radiation Medical Practitioner must take
into account clause 3.2.2 of the Code.
JUSTIFICATION PROCESS:
Justification of X-ray examinations and procedures can be on the basis of generic justification
OR on an individual basis. In both cases the definitions are determined by the Radiation Medical
Practitioner.
As part of the justification process the Radiation Medical Practitioner should:
Communicate directly with the referrer to seek clarification if the referral is:
Inappropriate.
Ambiguous.
Would lead to a radiation exposure that does answer the clinical question being posed.
The Radiation Medical Practitioner should where it is clinically appropriate:
Substitute other imaging tests that do not use ionizing radiation.
Modify the examination.
Cancel the examination.
Limit the procedure scope, eg: limit number of phases.
Communicate decisions with the referrer.
ABBREVIATIONS:
AEC Automatic Exposure Control
AP Anteroposterior
COPD Chronic Obstructive Pulmonary Disease
DP Dorsiplantar
GI Gastrointestinal
kV Kilo Voltage
mAs Milliamps per second
NOF Neck of Femur
# Fracture
SCN Special Care Nursery
TMJ Temporomandibular Joint
OPG Orthopantomogram
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 3
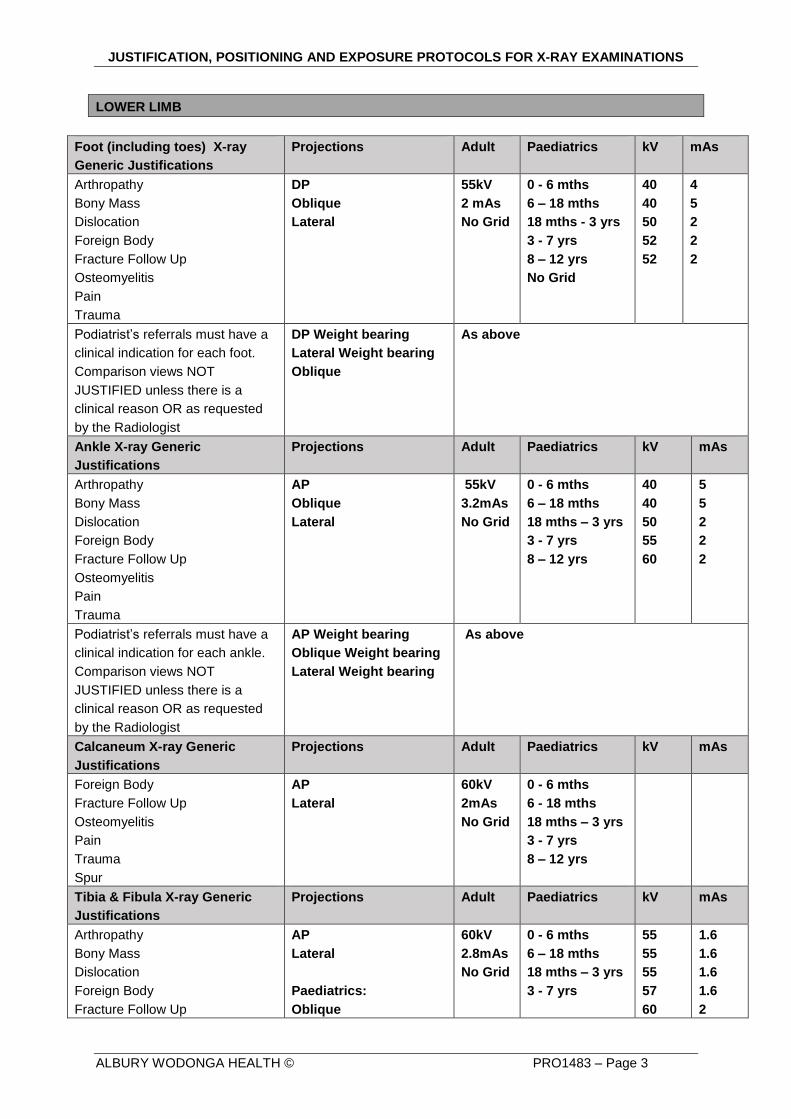
LOWER LIMB
Foot (including toes) X-ray
Generic Justifications
Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture Follow Up
Osteomyelitis
Pain
Trauma
DP
Oblique
Lateral
55kV
2 mAs
No Grid
0 - 6 mths
6 – 18 mths
18 mths - 3 yrs
3 - 7 yrs
8 – 12 yrs
No Grid
40
40
50
52
52
4
5
2
2
2
Podiatrist’s referrals must have a
clinical indication for each foot.
Comparison views NOT
JUSTIFIED unless there is a
clinical reason OR as requested
by the Radiologist
DP Weight bearing
Lateral Weight bearing
Oblique
As above
Ankle X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture Follow Up
Osteomyelitis
Pain
Trauma
AP
Oblique
Lateral
55kV
3.2mAs
No Grid
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
40
40
50
55
60
5
5
2
2
2
Podiatrist’s referrals must have a
clinical indication for each ankle.
Comparison views NOT
JUSTIFIED unless there is a
clinical reason OR as requested
by the Radiologist
AP Weight bearing
Oblique Weight bearing
Lateral Weight bearing
As above
Calcaneum X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Foreign Body
Fracture Follow Up
Osteomyelitis
Pain
Trauma
Spur
AP
Lateral
60kV
2mAs
No Grid
0 - 6 mths
6 - 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
Tibia & Fibula X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture Follow Up
AP
Lateral
Paediatrics:
Oblique
60kV
2.8mAs
No Grid
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
55
55
55
57
60
1.6
1.6
1.6
1.6
2
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 4
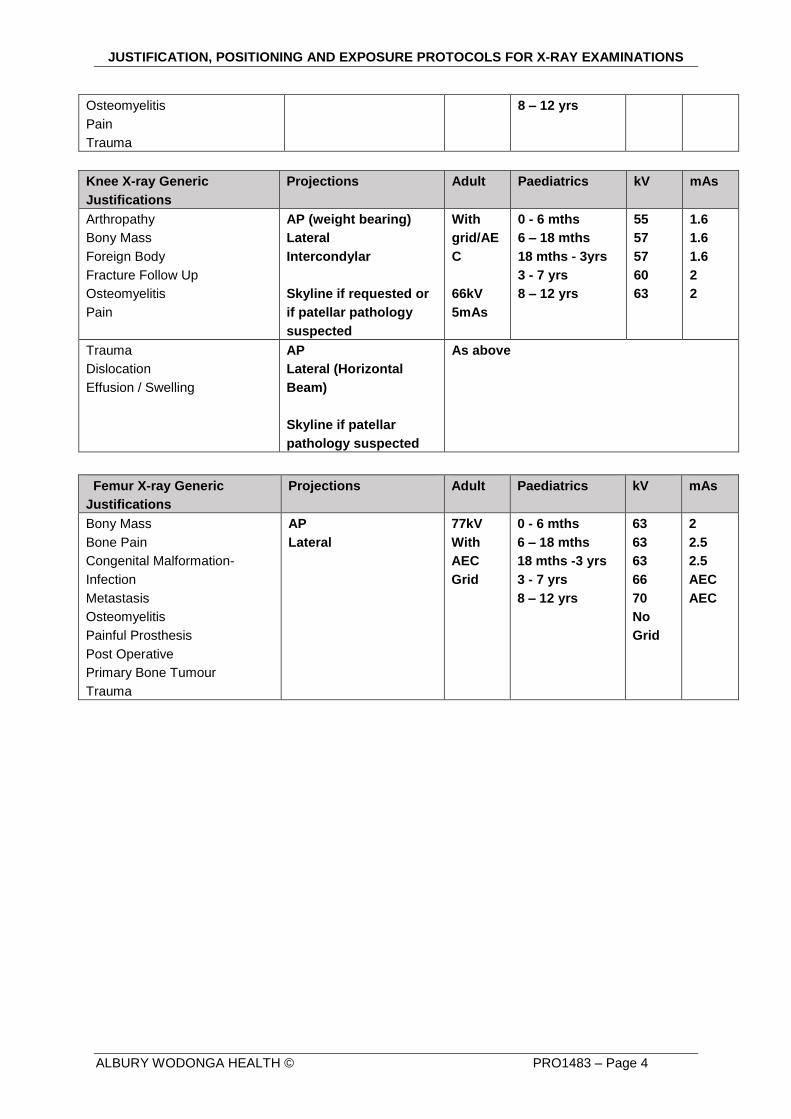
Osteomyelitis
Pain
Trauma
8 – 12 yrs
Knee X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Foreign Body
Fracture Follow Up
Osteomyelitis
Pain
AP (weight bearing)
Lateral
Intercondylar
Skyline if requested or
if patellar pathology
suspected
With
grid/AE
C
66kV
5mAs
0 - 6 mths
6 – 18 mths
18 mths - 3yrs
3 - 7 yrs
8 – 12 yrs
55
57
57
60
63
1.6
1.6
1.6
2
2
Trauma
Dislocation
Effusion / Swelling
AP
Lateral (Horizontal
Beam)
Skyline if patellar
pathology suspected
As above
Femur X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Bony Mass
Bone Pain
Congenital Malformation-
Infection
Metastasis
Osteomyelitis
Painful Prosthesis
Post Operative
Primary Bone Tumour
Trauma
AP
Lateral
77kV
With
AEC
Grid
0 - 6 mths
6 – 18 mths
18 mths -3 yrs
3 - 7 yrs
8 – 12 yrs
63
63
63
66
70
No
Grid
2
2.5
2.5
AEC
AEC
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 5
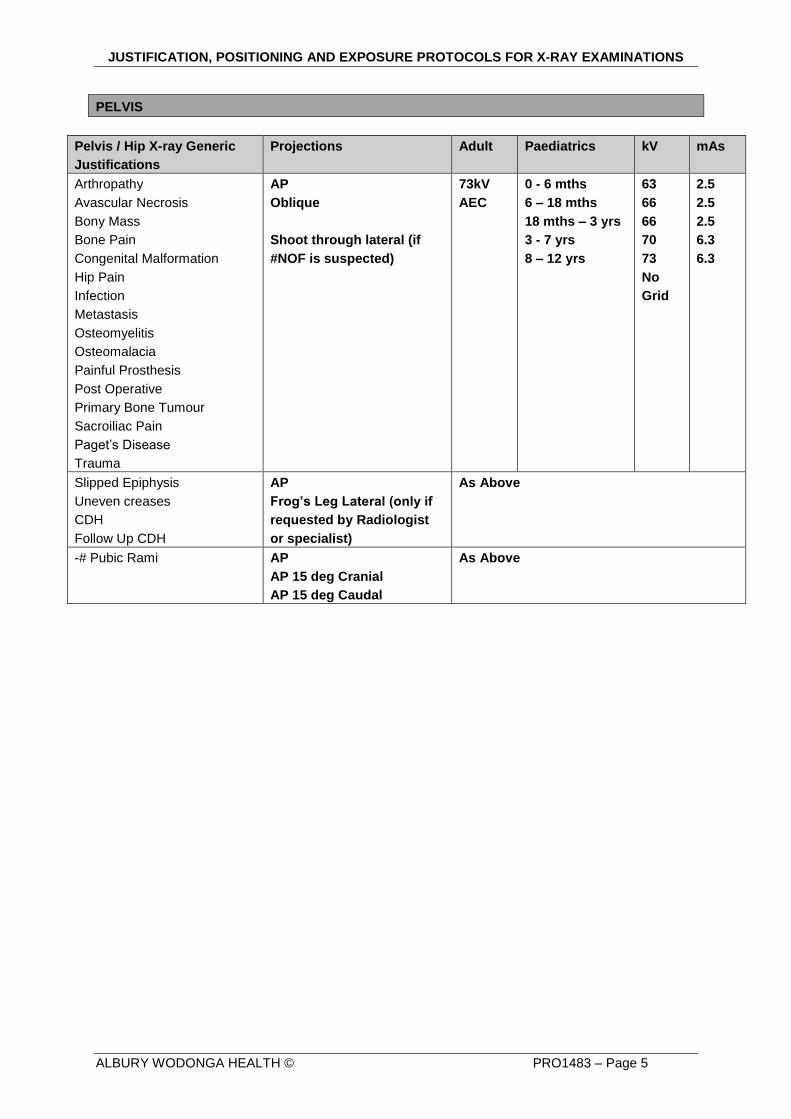
PELVIS
Pelvis / Hip X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Arthropathy
Avascular Necrosis
Bony Mass
Bone Pain
Congenital Malformation
Hip Pain
Infection
Metastasis
Osteomyelitis
Osteomalacia
Painful Prosthesis
Post Operative
Primary Bone Tumour
Sacroiliac Pain
Paget’s Disease
Trauma
AP
Oblique
Shoot through lateral (if
#NOF is suspected)
73kV
AEC
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
63
66
66
70
73
No
Grid
2.5
2.5
2.5
6.3
6.3
Slipped Epiphysis
Uneven creases
CDH
Follow Up CDH
AP
Frog’s Leg Lateral (only if
requested by Radiologist
or specialist)
As Above
-# Pubic Rami AP
AP 15 deg Cranial
AP 15 deg Caudal
As Above
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 6
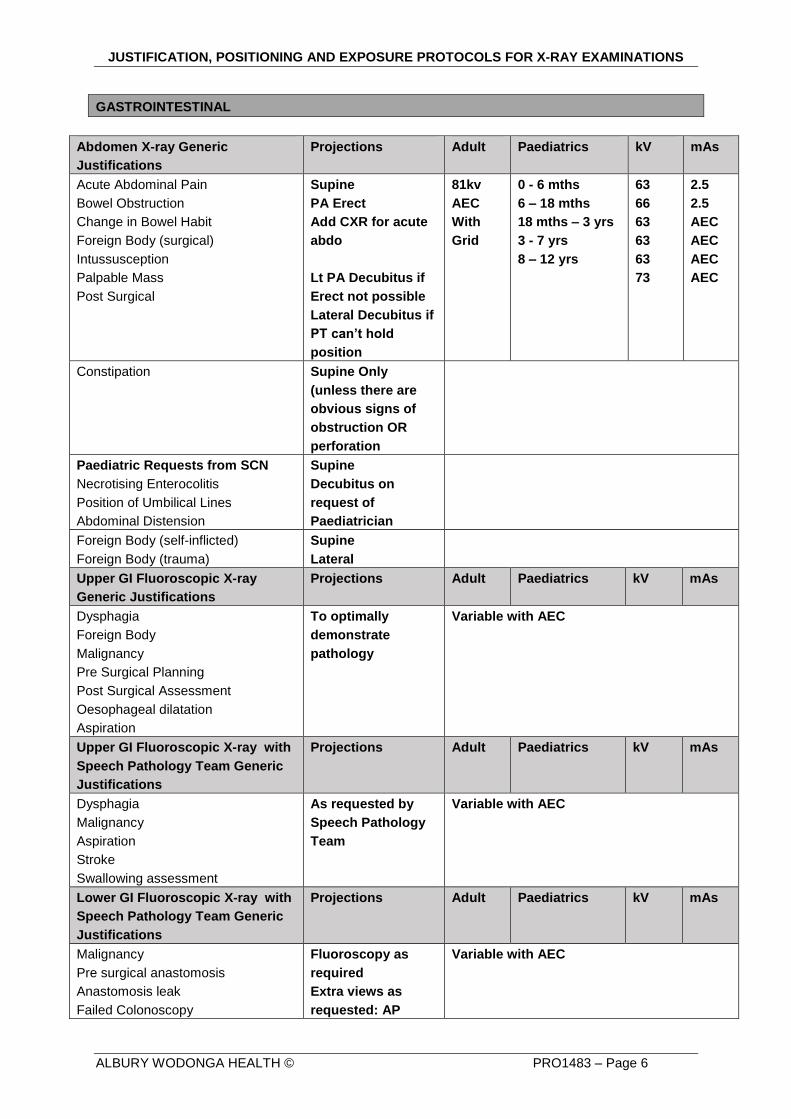
GASTROINTESTINAL
Abdomen X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Acute Abdominal Pain
Bowel Obstruction
Change in Bowel Habit
Foreign Body (surgical)
Intussusception
Palpable Mass
Post Surgical
Supine
PA Erect
Add CXR for acute
abdo
Lt PA Decubitus if
Erect not possible
Lateral Decubitus if
PT can’t hold
position
81kv
AEC
With
Grid
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
63
66
63
63
63
73
2.5
2.5
AEC
AEC
AEC
AEC
Constipation Supine Only
(unless there are
obvious signs of
obstruction OR
perforation
Paediatric Requests from SCN
Necrotising Enterocolitis
Position of Umbilical Lines
Abdominal Distension
Supine
Decubitus on
request of
Paediatrician
Foreign Body (self-inflicted)
Foreign Body (trauma)
Supine
Lateral
Upper GI Fluoroscopic X-ray
Generic Justifications
Projections Adult Paediatrics kV mAs
Dysphagia
Foreign Body
Malignancy
Pre Surgical Planning
Post Surgical Assessment
Oesophageal dilatation
Aspiration
To optimally
demonstrate
pathology
Variable with AEC
Upper GI Fluoroscopic X-ray with
Speech Pathology Team Generic
Justifications
Projections Adult Paediatrics kV mAs
Dysphagia
Malignancy
Aspiration
Stroke
Swallowing assessment
As requested by
Speech Pathology
Team
Variable with AEC
Lower GI Fluoroscopic X-ray with
Speech Pathology Team Generic
Justifications
Projections Adult Paediatrics kV mAs
Malignancy
Pre surgical anastomosis
Anastomosis leak
Failed Colonoscopy
Fluoroscopy as
required
Extra views as
requested: AP
Variable with AEC
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 7
Supine, PA 40 deg
Caudal, Right
Decubitus, Left
Decubitus
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 8
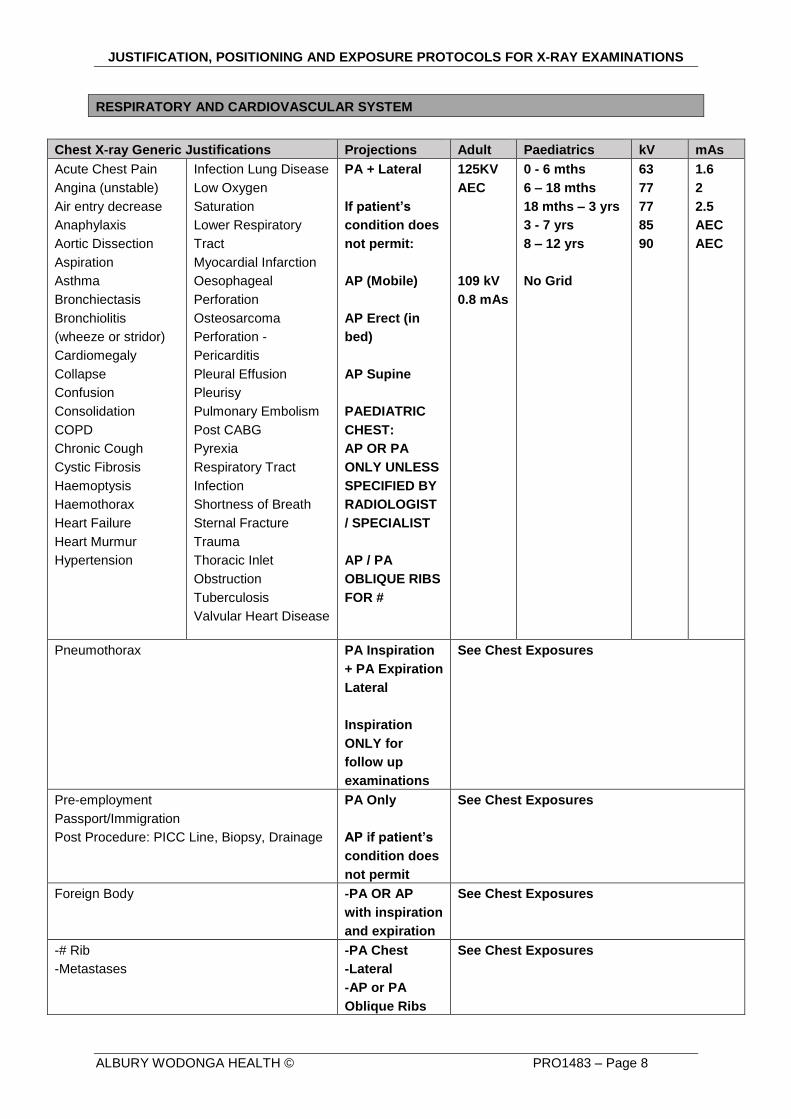
RESPIRATORY AND CARDIOVASCULAR SYSTEM
Chest X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Acute Chest Pain
Angina (unstable)
Air entry decrease
Anaphylaxis
Aortic Dissection
Aspiration
Asthma
Bronchiectasis
Bronchiolitis
(wheeze or stridor)
Cardiomegaly
Collapse
Confusion
Consolidation
COPD
Chronic Cough
Cystic Fibrosis
Haemoptysis
Haemothorax
Heart Failure
Heart Murmur
Hypertension
Infection Lung Disease
Low Oxygen
Saturation
Lower Respiratory
Tract
Myocardial Infarction
Oesophageal
Perforation
Osteosarcoma
Perforation -
Pericarditis
Pleural Effusion
Pleurisy
Pulmonary Embolism
Post CABG
Pyrexia
Respiratory Tract
Infection
Shortness of Breath
Sternal Fracture
Trauma
Thoracic Inlet
Obstruction
Tuberculosis
Valvular Heart Disease
PA + Lateral
If patient’s
condition does
not permit:
AP (Mobile)
AP Erect (in
bed)
AP Supine
PAEDIATRIC
CHEST:
AP OR PA
ONLY UNLESS
SPECIFIED BY
RADIOLOGIST
/ SPECIALIST
AP / PA
OBLIQUE RIBS
FOR #
125KV
AEC
109 kV
0.8 mAs
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
No Grid
63
77
77
85
90
1.6
2
2.5
AEC
AEC
Pneumothorax PA Inspiration
+ PA Expiration
Lateral
Inspiration
ONLY for
follow up
examinations
See Chest Exposures
Pre-employment
Passport/Immigration
Post Procedure: PICC Line, Biopsy, Drainage
PA Only
AP if patient’s
condition does
not permit
See Chest Exposures
Foreign Body -PA OR AP
with inspiration
and expiration
See Chest Exposures
-# Rib
-Metastases
-PA Chest
-Lateral
-AP or PA
Oblique Ribs
See Chest Exposures
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 9
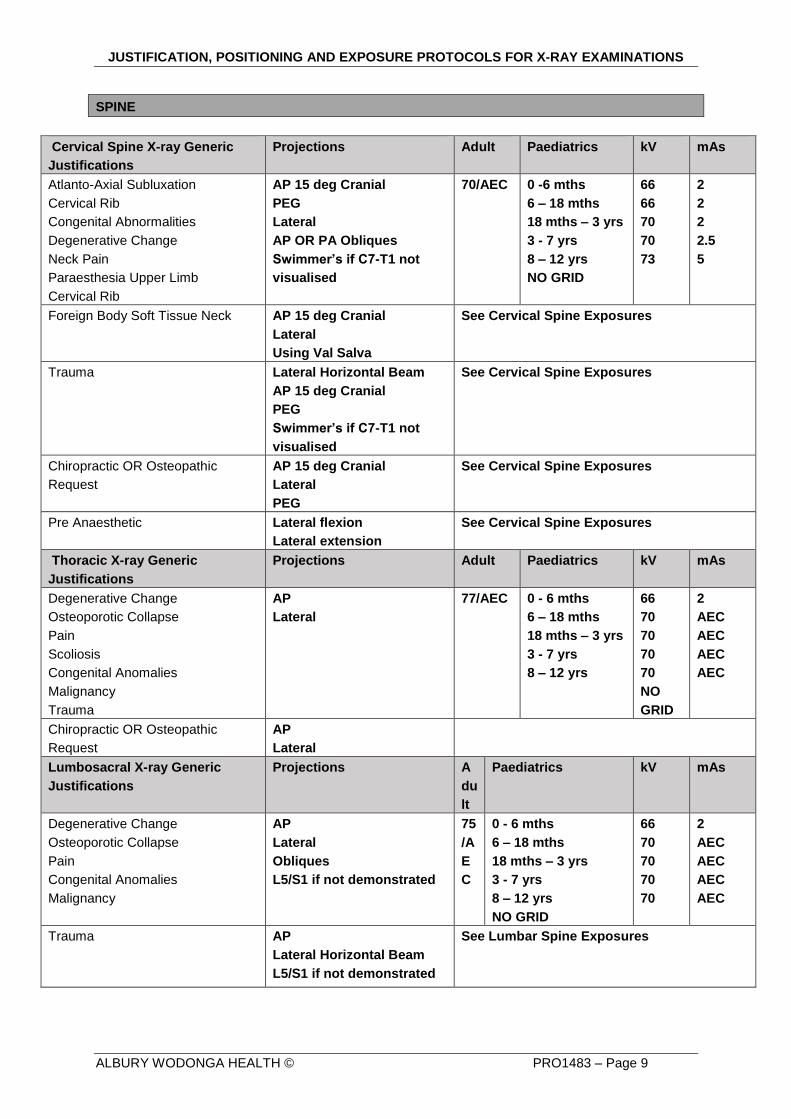
SPINE
Cervical Spine X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Atlanto-Axial Subluxation
Cervical Rib
Congenital Abnormalities
Degenerative Change
Neck Pain
Paraesthesia Upper Limb
Cervical Rib
AP 15 deg Cranial
PEG
Lateral
AP OR PA Obliques
Swimmer’s if C7-T1 not
visualised
70/AEC 0 -6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
NO GRID
66
66
70
70
73
2
2
2
2.5
5
Foreign Body Soft Tissue Neck AP 15 deg Cranial
Lateral
Using Val Salva
See Cervical Spine Exposures
Trauma Lateral Horizontal Beam
AP 15 deg Cranial
PEG
Swimmer’s if C7-T1 not
visualised
See Cervical Spine Exposures
Chiropractic OR Osteopathic
Request
AP 15 deg Cranial
Lateral
PEG
See Cervical Spine Exposures
Pre Anaesthetic Lateral flexion
Lateral extension
See Cervical Spine Exposures
Thoracic X-ray Generic
Justifications
Projections Adult Paediatrics kV mAs
Degenerative Change
Osteoporotic Collapse
Pain
Scoliosis
Congenital Anomalies
Malignancy
Trauma
AP
Lateral
77/AEC 0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
66
70
70
70
70
NO
GRID
2
AEC
AEC
AEC
AEC
Chiropractic OR Osteopathic
Request
AP
Lateral
Lumbosacral X-ray Generic
Justifications
Projections A
du
lt
Paediatrics kV mAs
Degenerative Change
Osteoporotic Collapse
Pain
Congenital Anomalies
Malignancy
AP
Lateral
Obliques
L5/S1 if not demonstrated
75
/A
E
C
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
NO GRID
66
70
70
70
70
2
AEC
AEC
AEC
AEC
Trauma AP
Lateral Horizontal Beam
L5/S1 if not demonstrated
See Lumbar Spine Exposures
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 10
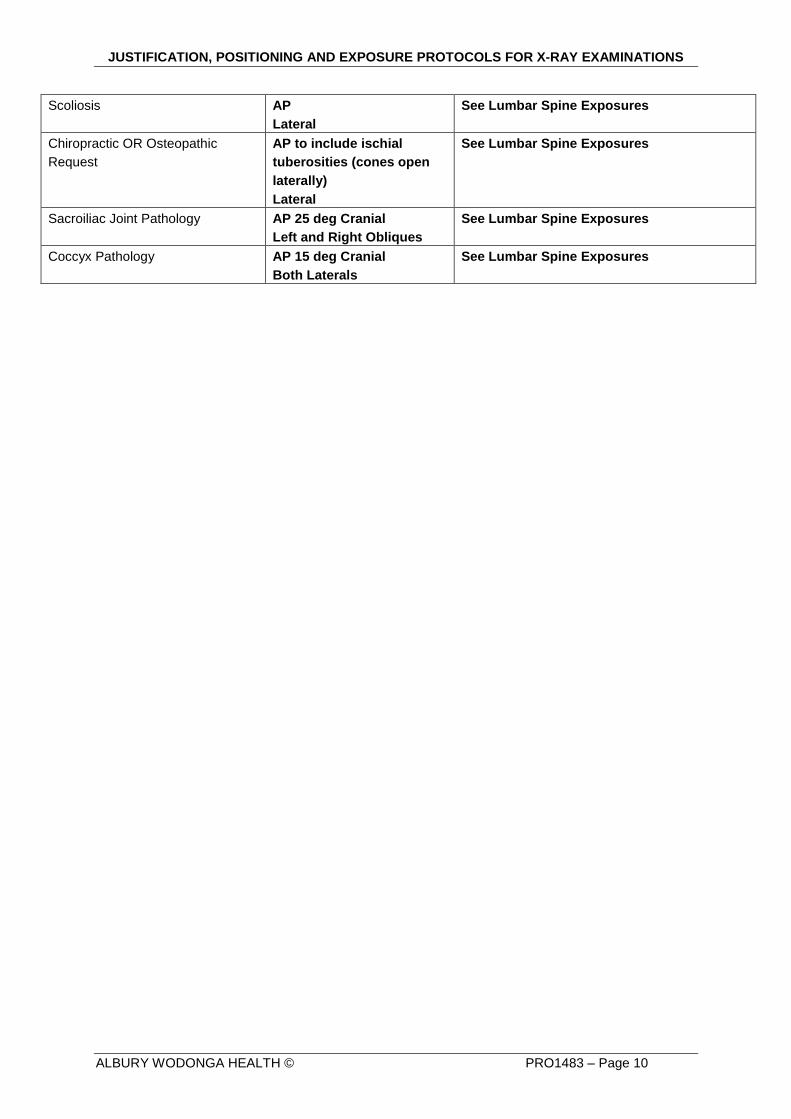
Scoliosis
AP
Lateral
See Lumbar Spine Exposures
Chiropractic OR Osteopathic
Request
AP to include ischial
tuberosities (cones open
laterally)
Lateral
See Lumbar Spine Exposures
Sacroiliac Joint Pathology AP 25 deg Cranial
Left and Right Obliques
See Lumbar Spine Exposures
Coccyx Pathology AP 15 deg Cranial
Both Laterals
See Lumbar Spine Exposures
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 11
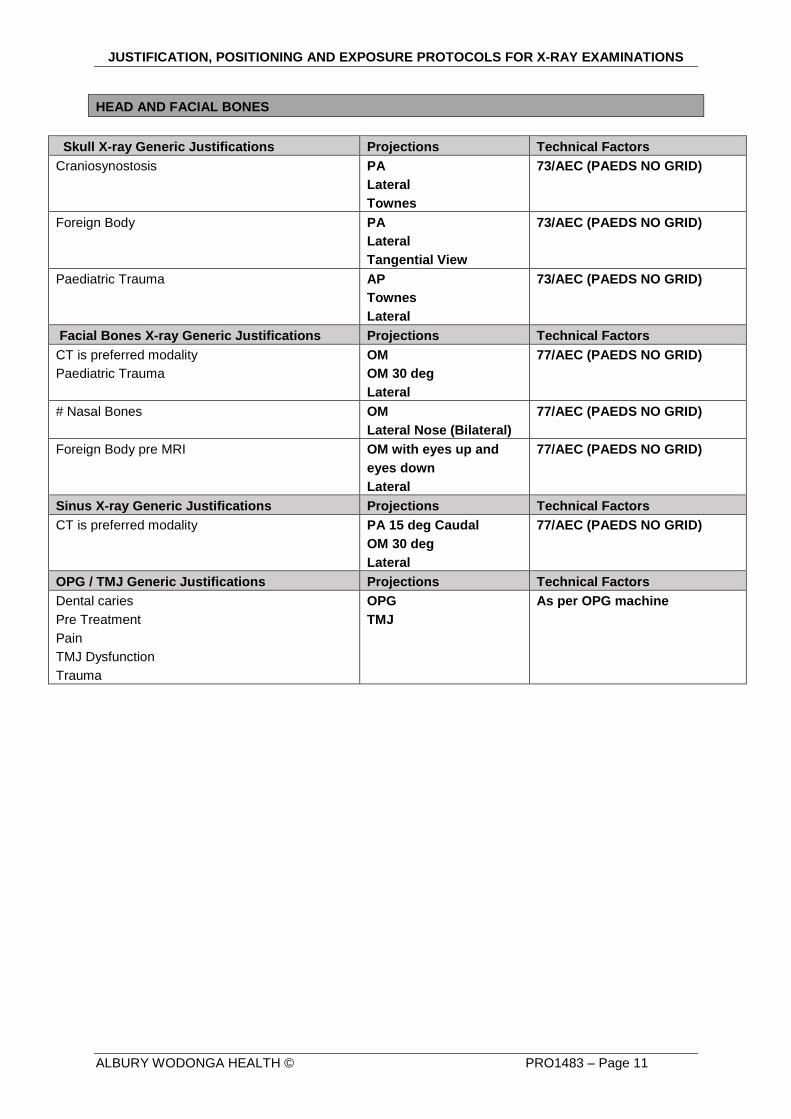
HEAD AND FACIAL BONES
Skull X-ray Generic Justifications Projections Technical Factors
Craniosynostosis PA
Lateral
Townes
73/AEC (PAEDS NO GRID)
Foreign Body PA
Lateral
Tangential View
73/AEC (PAEDS NO GRID)
Paediatric Trauma AP
Townes
Lateral
73/AEC (PAEDS NO GRID)
Facial Bones X-ray Generic Justifications Projections Technical Factors
CT is preferred modality
Paediatric Trauma
OM
OM 30 deg
Lateral
77/AEC (PAEDS NO GRID)
# Nasal Bones OM
Lateral Nose (Bilateral)
77/AEC (PAEDS NO GRID)
Foreign Body pre MRI OM with eyes up and
eyes down
Lateral
77/AEC (PAEDS NO GRID)
Sinus X-ray Generic Justifications Projections Technical Factors
CT is preferred modality PA 15 deg Caudal
OM 30 deg
Lateral
77/AEC (PAEDS NO GRID)
OPG / TMJ Generic Justifications Projections Technical Factors
Dental caries
Pre Treatment
Pain
TMJ Dysfunction
Trauma
OPG
TMJ
As per OPG machine
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 12
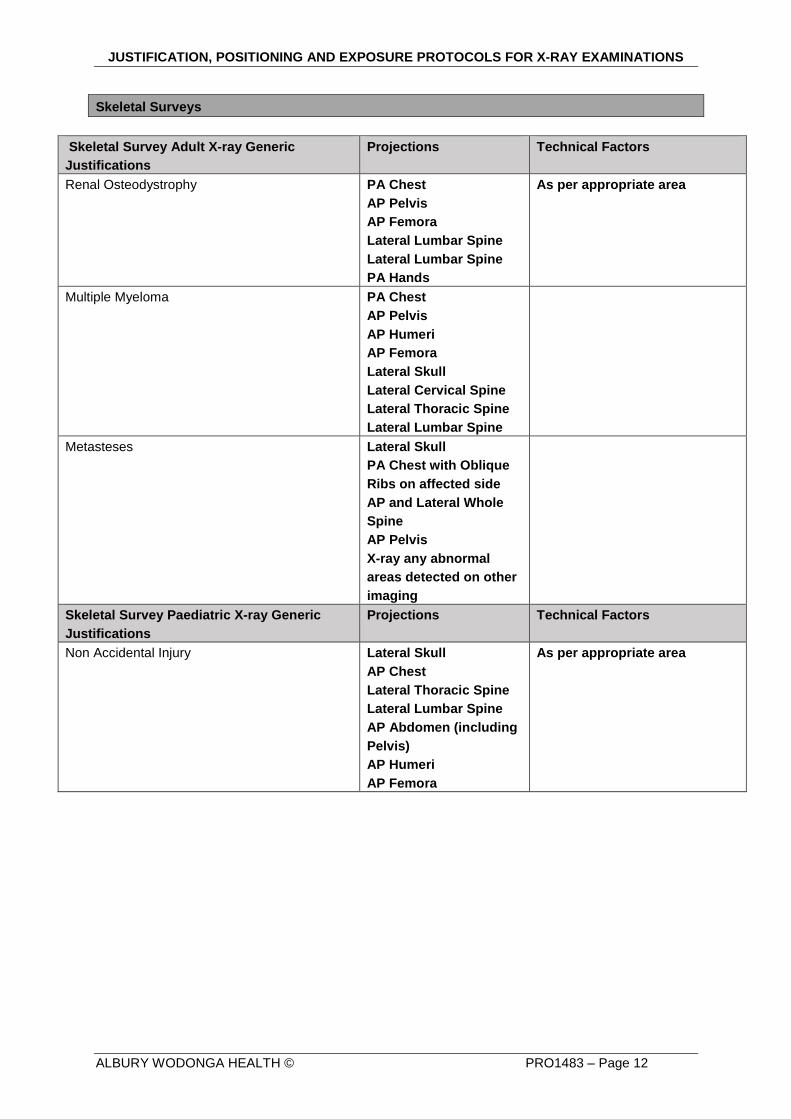
Skeletal Surveys
Skeletal Survey Adult X-ray Generic
Justifications
Projections Technical Factors
Renal Osteodystrophy PA Chest
AP Pelvis
AP Femora
Lateral Lumbar Spine
Lateral Lumbar Spine
PA Hands
As per appropriate area
Multiple Myeloma PA Chest
AP Pelvis
AP Humeri
AP Femora
Lateral Skull
Lateral Cervical Spine
Lateral Thoracic Spine
Lateral Lumbar Spine
Metasteses Lateral Skull
PA Chest with Oblique
Ribs on affected side
AP and Lateral Whole
Spine
AP Pelvis
X-ray any abnormal
areas detected on other
imaging
Skeletal Survey Paediatric X-ray Generic
Justifications
Projections Technical Factors
Non Accidental Injury Lateral Skull
AP Chest
Lateral Thoracic Spine
Lateral Lumbar Spine
AP Abdomen (including
Pelvis)
AP Humeri
AP Femora
As per appropriate area
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 13
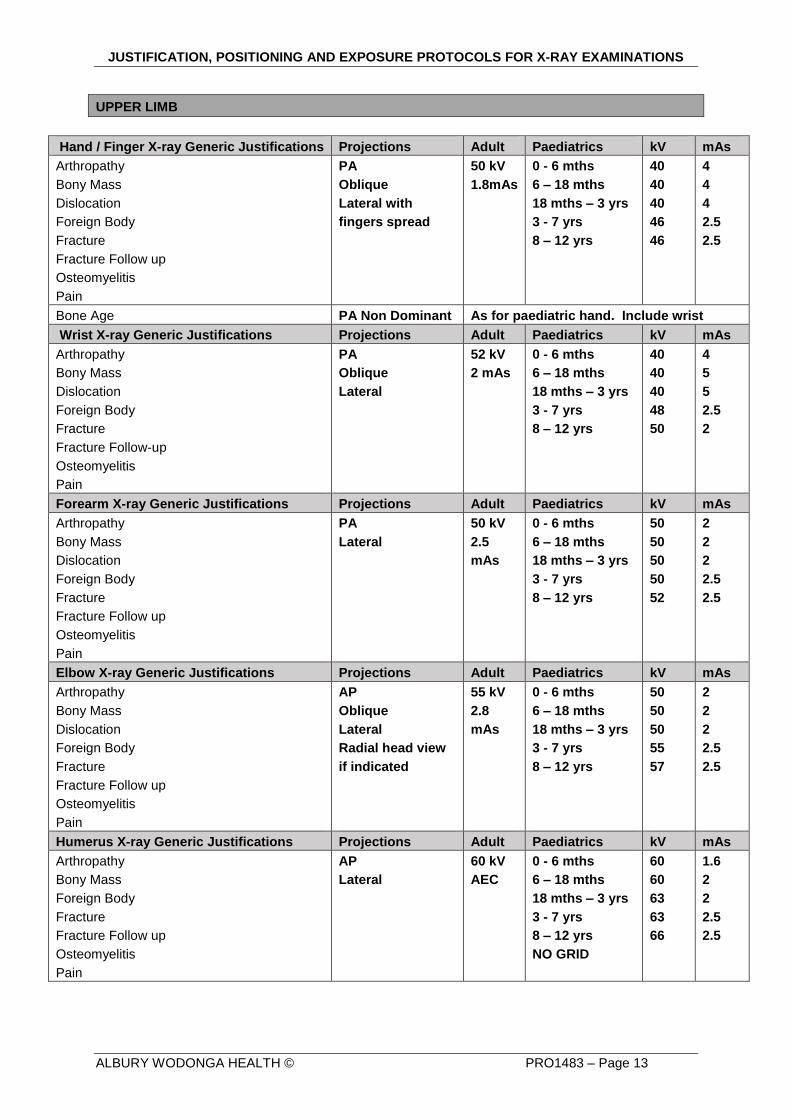
UPPER LIMB
Hand / Finger X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture
Fracture Follow up
Osteomyelitis
Pain
PA
Oblique
Lateral with
fingers spread
50 kV
1.8mAs
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
40
40
40
46
46
4
4
4
2.5
2.5
Bone Age PA Non Dominant As for paediatric hand. Include wrist
Wrist X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture
Fracture Follow-up
Osteomyelitis
Pain
PA
Oblique
Lateral
52 kV
2 mAs
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
40
40
40
48
50
4
5
5
2.5
2
Forearm X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture
Fracture Follow up
Osteomyelitis
Pain
PA
Lateral
50 kV
2.5
mAs
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
50
50
50
50
52
2
2
2
2.5
2.5
Elbow X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Dislocation
Foreign Body
Fracture
Fracture Follow up
Osteomyelitis
Pain
AP
Oblique
Lateral
Radial head view
if indicated
55 kV
2.8
mAs
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
50
50
50
55
57
2
2
2
2.5
2.5
Humerus X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Foreign Body
Fracture
Fracture Follow up
Osteomyelitis
Pain
AP
Lateral
60 kV
AEC
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
NO GRID
60
60
63
63
66
1.6
2
2
2.5
2.5
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 14
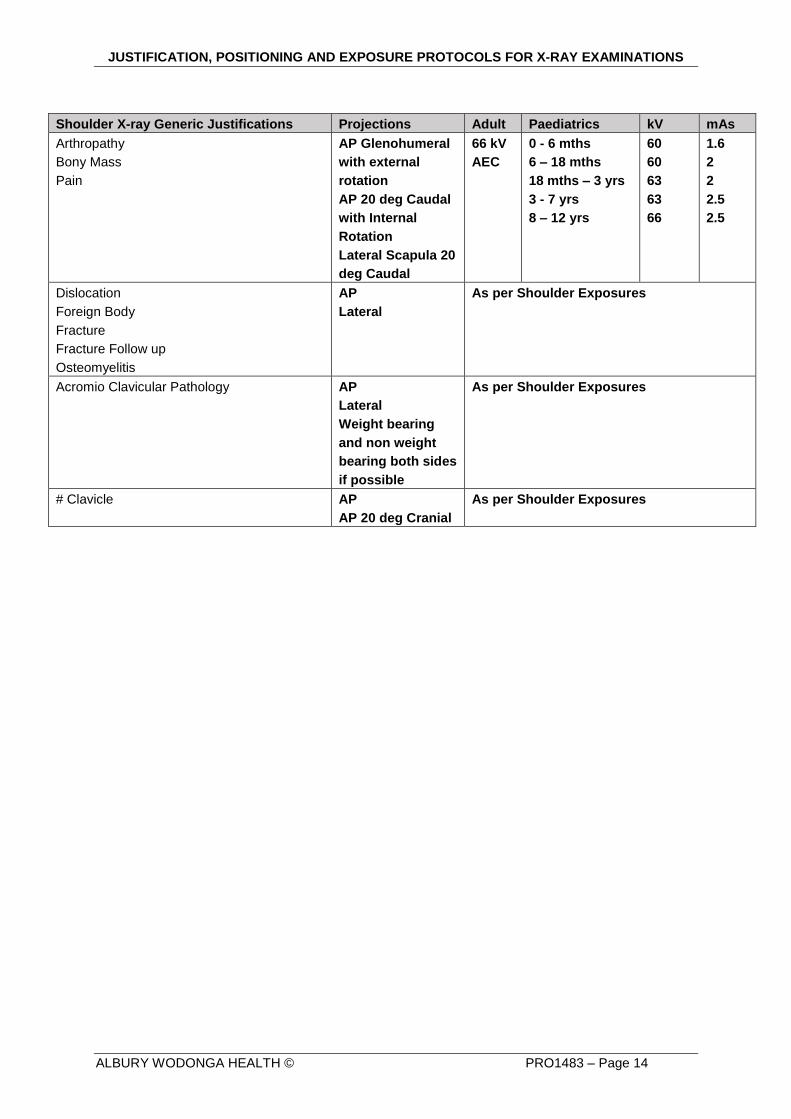
Shoulder X-ray Generic Justifications Projections Adult Paediatrics kV mAs
Arthropathy
Bony Mass
Pain
AP Glenohumeral
with external
rotation
AP 20 deg Caudal
with Internal
Rotation
Lateral Scapula 20
deg Caudal
66 kV
AEC
0 - 6 mths
6 – 18 mths
18 mths – 3 yrs
3 - 7 yrs
8 – 12 yrs
60
60
63
63
66
1.6
2
2
2.5
2.5
Dislocation
Foreign Body
Fracture
Fracture Follow up
Osteomyelitis
AP
Lateral
As per Shoulder Exposures
Acromio Clavicular Pathology AP
Lateral
Weight bearing
and non weight
bearing both sides
if possible
As per Shoulder Exposures
# Clavicle AP
AP 20 deg Cranial
As per Shoulder Exposures
JUSTIFICATION, POSITIONING AND EXPOSURE PROTOCOLS FOR X-RAY EXAMINATIONS
ALBURY WODONGA HEALTH © PRO1483 – Page 15
Annexes:
Related AWH Documents:
Accreditation Standards:
Other Relevant Information:
References:
Contact Point: Medical Imaging Manager.
In consultation with:
TITLE / POSITION
THIS SECTION FOR QUALITY & CLINICAL GOVERNANCE OFFICE USE ONLY
Approved by Executive / Delegate: Date Approved: SharePoint Location:
Executive Director of Medical Services
and Clinical Governance
7 October 2015 Procedures…
Responsible Department: Date for Review: Linked Documents:
Medical Imaging 7 October 2018
Version No: Original Approval Date: Previously Named As:
1 7 October 2015