Procedure: M15p National Early Warning Score (NEWS) Procedure Relates to Primary Policy: B4 – Basic Life Support policy Version: M15p/04.2 Approved by: Quality Matters Committee Date approved: 6 th September 2016 Title of Author: Nurse Consultant Physical Healthcare Responsible ED: Medical Director Date issued: 19th April 2018 Review date: September 2019 Target audience: All clinical staff trust-wide Disclosure Status (B) B Can be disclosed to patients and the public
Transcript
Procedure: M15p National Early Warning Score (NEWS)
Procedure Relates to Primary Policy: B4 – Basic Life Support policy
Version: M15p/04.2
Approved by: Quality Matters Committee
Date approved: 6th September 2016
Title of Author: Nurse Consultant Physical Healthcare
Responsible ED: Medical Director
Date issued: 19th April 2018
Review date: September 2019
Target audience: All clinical staff trust-wide
Disclosure Status (B) B Can be disclosed to patients and the public
West London Mental Health NHS Trust Page 2 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Equality & Diversity Statement The Trust strives to ensure its policies are accessible, appropriate and inclusive for all. Therefore all policies will be required to undergo an Equality Impact Assessment and will only be approved once this process has been completed.
The Trust aspires to: “Ensure the health and wellbeing of those we serve and be a leader in the development of
mental health care and treatment.”
To achieve such an aim, the Trust will need to address the issues raised by its stakeholders and deliver the kind of service developments and outcomes they describe.
Such an endeavour needs to be underpinned by a core set of values.
West London Mental Health NHS Trust Page 3 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Version Control Sheet
Version Date Title of Author Status Comment
0.01 Aug 10 Lynne Read, Assistant Director of Primary Care
Draft New Policy.
Circulated to key members of the Physical Healthcare Group for initial comment.
0.01 Sept 10 Lynne Read, Assistant Director of Primary Care
Draft Revised to incorporate comments. To go to the CSSC September 2010.
0.01 Oct 10 Lynne Read, Assistant Director of Primary Care
Final Draft To be approved as a working document at the October 2010 CSSC
0.01 Dec 10 Dr A Cohen, Director of Primary Care
Final Draft For debate/discussion at CSSC
0.01 Jan 11 Lynne Read, Assistant Director of Primary Care
Final Draft To PRG for approval and minor amendments made
0.02 Jan 12 Director of Primary Care Reviewed Procedure
Ratified by CEC
0.02 April 12 Director of Primary Care Reviewed Procedure
Implementation & monitoring Plans updated
02 May 12 Director of Primary Care Ratified Ratified by TMT 9th May 2012
03 April 15
Sept 15
Director of Primary Care Review
Reviewed Procedure
Approved at May CEC.
Minor amendments throughout procedure, 7.3 (removed), 9.1, 9.2, 11.2, 12.1, 12.2, Apps 1&2. No change to policy process. Re-issued 15.09.15
04
04.1
04.2
July 16
November 2017
April 2018
Nurse consultant physical healthcare
Reviewed and amended
Revised & issued
Revised & issued
Changes to escalation process to bring it in line with RCP guidance. Changes to NEWs chart to bring it in line with RCP guidance. Addition of local escalation processes to reflect practice.
Minor text amend to 6.2.1
Minor text amend to Appendix 11. Medium risk - Registered Nurse to escalate to doctor. Doctor to see patient within 30 minutes
West London Mental Health NHS Trust Page 4 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
5. What is NEWS ............................................................................................................... 7 6. Systems and recording .................................................................................................. 7 7. Recognising a physically deteriorating patient ............................................................... 9 8. When to use NEWS ..................................................................................................... 10 9. Observation chart ........................................................................................................ 10
Appendix 1 - NEWS observation chart– front page…………………………………………..15 Appendix 2 - NEWS observation chart instruction – back page…………………………….16 Appendix 3 – Escalation Flowchart - Local Services, Jubilee Ward……………...………...17 Appendix 4 – Escalation Flowchart - Local Services, the Limes……………………………18 Appendix 5 – Escalation Flowchart - Local Services, H&F…………………………………..19 Appendix 6 – Escalation Flowchart - Local Services, Ealing…………………...……………20 Appendix 7 – Escalation Flowchart - Local Services, Hounslow…………………………….21 Appendix 8 – Escalation Flowchart - Local Services, Homeward, Magnolia……………….22 Appendix 9 – Escalation Flowchart - High Secure Services, Broadmoor Hospital……….. 23 Appendix 10 - Guidance for use of NEWS in ECT …………………………………...………24 Appendix 11 – Escalation Flowchart – West London Forensic Services………………..… 25
West London Mental Health NHS Trust Page 5 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
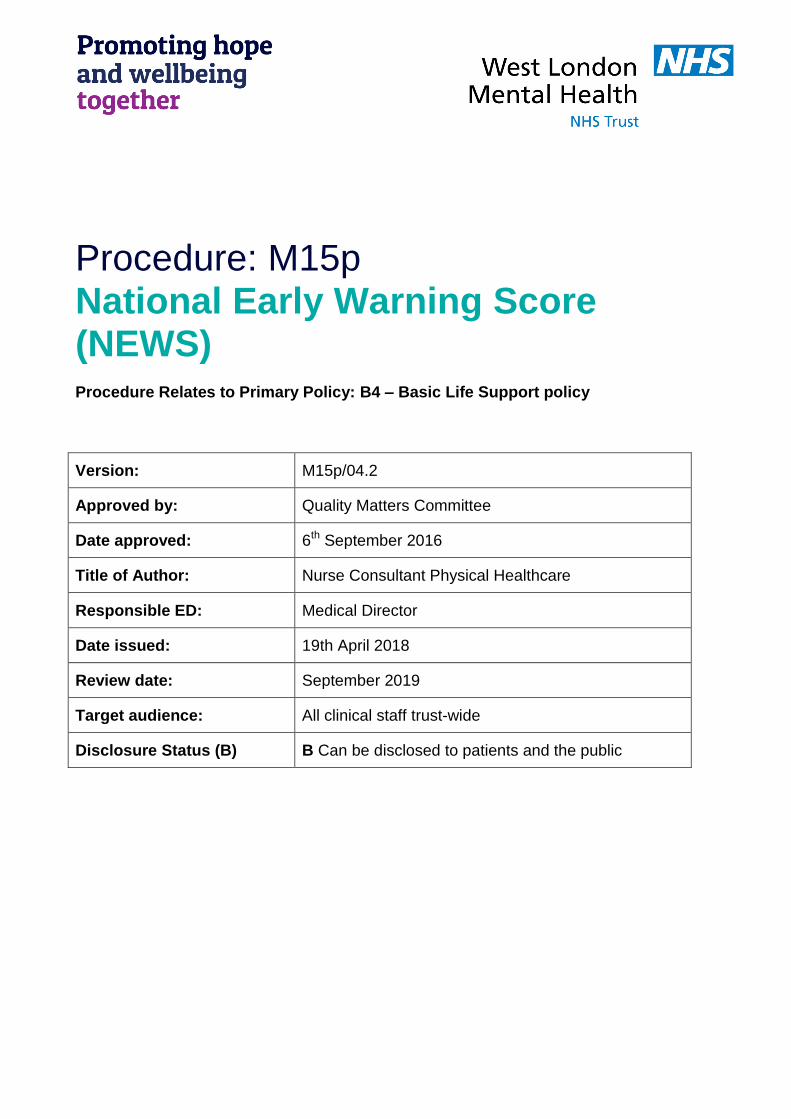
1. Flowchart
NEWS score of 1 - 4
Clinical risk:
LOW
NEWS score of 5 or more or 3 in one
parameter
Clinical risk: MEDIUM
NEWS score of 7 or
more
Clinical risk: HIGH
Complete NEWS Chart
Inform Nurse in Charge
Registered Nurse to decide if increased frequency of
monitoring and/or escalation of clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate to doctor. Doctor to see patient
within 30 minutes.
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
crash team or accident and emergency via ambulance service (see local escalation protocols)
Registered Nurse to immediately inform the medical team caring for
the patient.
Clinical priority safe transfer
Document action in notes. Complete IR1 if transferred Revise Care Plan as necessary
West London Mental Health NHS Trust Page 6 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
2 Introduction 2.1 Primary policy 2.1.1 The Trust’s Physical Healthcare Strategy describes the ‘interconnection between
mental and physical health’.
2.1.2 It states ‘having a mental problem increases mortality from heart disease1,2,3 coronary heart disease can increase the risk of depression. People with schizophrenia have a life expectancy that is significantly lower than that of the general population and have higher rates of serious long term conditions4,5,6People with mental health problems are also prone to factors that are damaging to overall health, such as poor diet, heavy smoking and drug and alcohol misuse7,8. Equally, people who smoke, are obese or take drugs or behave in other ways that put their health at risk are more likely to have mental health problems9,10 and may people in Mental Health Services will have co-morbid physical health problems such as long term conditions and complex end of life care needs11,12,13.
3 Purpose 3.1 The aim of this policy is to improve people’s outcomes by detecting and acting upon
early signs of deterioration in physical health of patients. This will be in part achieved through the implementation of the National Early Warning Score (NEWS) system that:
Identifies trends in patient observations;
Ensures that timely patient review and appropriate treatment occurs; and
Improves the documentation of patient observations.
3.2 Notification should also occur where clinical deterioration occurs other than that assessed by the NEWS criteria, or where sound clinical judgement would suggest that notification is in the best interests of patient care.
4 Scope 4.1 All staff are to record patient observations on the National Early Warning Scores
(NEWS) chart when are taken. Staff are to calculate and record score on the chart and escalate according to this policy.
4.2 It ONLY applies to people who are current in-patients of West London Mental Health NHS Trust
West London Mental Health NHS Trust Page 7 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
5 What is NEWS? 5.1 NEWS14 is an evidenced based system of care, used nationally in acute hospitals to
monitor the progress of patients, and to identify early deterioration in their health. It has been adopted by many Mental Health Trusts.
5.2 NEWS is a form of track and trigger scoring system. The triggers are based on
routine observations and are sensitive enough to detect subtle changes in a patient’s physiology which will be reflected in a change of score should the patient be improving or deteriorating.
5.3 All patients have their vital signs measured and these are converted into a score. The higher the score the more abnormal the vital signs are. If the scores reach above a certain threshold, staff must follow the escalation process
5.4 The system allows for the regular monitoring and recording of blood pressure, pulse, temperature, conscious state, oxygen saturation (pO2) and respiratory rate.
5.5 Early warning scoring systems were originally developed with 2 specific aims:
To facilitate timely recognition of the patients with established or impending critical illness; and
To empower nurses and junior medical staff to obtain experienced help through the operation of a trigger threshold which, if reached, required mandatory attendance by a more senior member of staff.
5.6 Use of a NATIONAL Early Warning Scoring system can also:
Improve the quality of patient observation and monitoring
Improve communication within the multidisciplinary team
Allow for timely admission to intensive care (acute hospital)
Support good medical judgement
Aid in securing appropriate assistance for sick patients
Give a good indication of physiological trends
Are a sensitive indicator of abnormal physiology NB – It is important that staff understand that NEWS does not replace clinical judgement
6 Systems and recording
6.1 The elements of the NEWS score, pulse, blood pressure, temperature, respiratory rate, oxygen saturation, and conscious state should be recorded in the patient’s electronic record, as well as the individual patient’s paper based record.
West London Mental Health NHS Trust Page 8 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
6.2 Frequency of recording 6.2.1 All patients who have returned to the ward following an attendance in accident and
emergency or who have been re-admitted to the ward following a stay in an acute hospital must have their NEWS score recorded immediately on return and escalated if any clinical concerns
6.2.2 All inpatients will have NEWS score recorded at least 12 hourly for the first three
days of admission. NEWS will normally be taken during the waking cycle. If there are clinical concerns follow NEWS score for more frequent monitoring or escalation as appropriate.
6.2.3 In Local Services in-patients with complex care needs i.e. patients on Meridian
Ward, the Limes, Jubilee and Magnolia ward the NEWS score will be recorded at least 12 hourly for the duration of admission. If there are clinical concerns follow NEWS score for more frequent monitoring or escalation as appropriate.
6.2.4 In local services other than those wards detailed above NEWS will after the first 72
hours be carried out at least once a week. If there are clinical concerns follow NEWS score for more frequent monitoring or escalation as appropriate.
6.2.5 In high secure and forensics services NEWS will after the first 72 hours be carried
out at least once a week. After one month NEWS will be carried out monthly. If there are clinical concerns follow NEWS score for more frequent monitoring or escalation as appropriate.
6.2.6 Rapid tranquilisation:
NEWS should be completed at least every 15 minutes following injectable Rapid tranquilisation for at least 1 hour. If no concerns this can be reduced to hourly until the patient is ambulatory. (See R10 Rapid Tranquilisation Restrictive Practice for further information including when more frequent monitoring is required).
6.2.7 Zuclopenthixol Acetate Administration:
NEWS should be completed at least every 4 hours following administration of zuclopenthixol acetate injection. Monitoring is recommended to be continued for 72 hours. (See Z1 Requesting a supply and the administration of Zuclopenthixol Acetate (Clopixol Acuphase®) for further information).
6.3 The NEWS score dictates the frequency of observations. 1-4 = 4-6 hourly
monitoring. 5 = hourly at least, 7 and above continuous whilst awaiting acute medical transfer/intervention. The frequency and specifications of all baseline observations should be written on the NEWS chart and prescribed in the Nursing Care plan.
6.4 Guidance for use of NEWS in ECT
Patients undergoing ECT treatment - please see Appendix 10 6.4.1 Undertake Physical Observations and NEW Score:
West London Mental Health NHS Trust Page 9 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Prior to ECT at the 'One Stop Clinic'
Prior to discharge following each ECT treatment 6.4.2 In acknowledgement that a service user’s physical observations are likely to be
volatile immediately prior to treatment and during recovery, there is no requirement to Score during this period, but to instead record the physical observations on the NEWS physical observation chart:
Prior to each ECT treatment
During ECT Recovery (recorded 3-4 times) 6.5 Reviewing NEWS 6.5.1 Ward rounds / clinical reviews and CPA meetings should routinely include review of
the service user’s physical observations that have occurred. This review should be recorded in the progress notes on RiO and within the CPA care plan.
6.6 Exceptions 6.6.1 If clinical teams decide that the routine recording of data for the NEWS is not
appropriate, for example, for people on an end-of-life care pathway, such decisions should be clearly documented in the progress notes and on the service user’s care plan on RiO.
6.7 Service user refusal 6.7.1 If it is not possible to measure a person’s physical observations, each attempt must
be recorded on the NEWS Physical Observation Chart as “Refused”. Staff must make repeated offers to undertake physical observations throughout a person’s stay in hospital.
7 Recognising a physically deteriorating patient 7.1 Clinical deterioration can occur at any stage of a patient’s illness, although there will
be certain periods during which a patients is more vulnerable such as at the onset of illness, during surgical or medical interventions and during recovery from critical illness.
7.2 Patients with a diagnosed physical health condition or illness must have a
secondary diagnosis recorded on RiO and agreed care plan must be written detailing the treatment plan including the signs and symptoms associated with deterioration.
West London Mental Health NHS Trust Page 10 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
8 When to use NEWS 8.1 NEWS relies on the routine recording and charting of the physiological status of the
patient however, the frequency of monitoring should be increased if abnormal physiology is observed. These are simple observations that can be performed by a nurse, doctor or other trained staff. These observations include:
Pulse
Respiratory rate
Temperature
Blood pressure
Oxygen saturation (pO2)
Conscious state (AVPU)
8.2 The NEWS evidence base does not apply to children or pregnant women – therefore this guidance is only applicable to adults.
9 Observation chart 9.1 The Trust will use the nationally recommended chart as the standard trust
document
10 NEWS score 10.1 Where there are concerns that a patient is unwell the NEWS observations are
carried out and the results used to gauge the severity of deterioration as indicated. Table 1
West London Mental Health NHS Trust Page 11 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
AVPU is a simple assessment where A = Alert V = Responds to verbal commands only P = Responds to Pain U = Completely Unresponsive A flow diagram for the use of NEWS is shown in Appendix A.
11 Trigger scores - definitions 11.1 A low score – NEWS 1 – 4 11.2 A medium score is NEWS greater than 5 and/or one parameter score of 3 11.3 A high score is NEWS of 7 or above
12 How to respond to news 12.1 A low score: The Senor Nurse will assess the patient and provide guidance to the
ward staff on the further frequency of recording of physical signs, and other action that may be appropriate, depending on the clinical state of the patient. If necessary, the senior nurse will also seek the opinion of the duty doctor, although it may only be telephone advice that is necessary. See Appendix 2
12.2 A medium score: The duty doctor will assess the patient, and arrange for the
appropriate care to be delivered. The assessment should take place within thirty minutes of the request being made by the ward staff. This may involve further monitoring, administration of medication, seeking specialist review, or transferring the patient to a more appropriate location depending on the clinical symptoms and signs. See Appendix 2
12.1 A high score: Staff will call for emergency assistance (see relevant appendices for
local protocols) and inform the duty doctor so that the duty doctor can assist in stabilising the patient prior to transfer to acute care
12.4 This response should be no different whether or not the recording takes place in
hours or out of hours and at weekends. N.B. A failure to attend a NEWS call within an acceptable timescale (<30 minutes) should result in the completion of an IR1.
12.5 A NEWS action plan must be agreed and documented for any patient reviewed.
West London Mental Health NHS Trust Page 12 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
13 Recording NEWS 13.1 Observations and NEWS Scores MUST be recorded on the National NEWS
Observation Chart – see Appendix 1. Observations should also be recorded on the patient electronic record.
13.2 The decision to seek medical advice as a result of a NEWS score should be
recorded on RiO and any advice or treatment provided should also be recorded on the patient’s electronic record.
13.3 The NEWS score and observations should also be recorded on the patient’s
electronic record
14 NEWS training 14.1 Medical staff will receive information, instruction and training on the NEWS system
on induction and within core-curriculum teaching, and BLS training.
Nursing staff will receive information, instruction and training on the NEWS system and accurate observations as part of BLS training.
NEWS training will be mandatory for registered nursing staff and incorporated within the BLS training.
14.2 Staff caring for patients with physical conditions should have competencies in
monitoring, measurement, interpretation and prompt response to the acutely ill patients appropriate to the level of care they are providing. Education and training should be provided to ensure staff have these competencies and they should be assessed to ensure they can demonstrate them.
14.3 Using the NEWS observation chart 14.3.1 The NEWS chart replaces previously used TPR charts. This provides a
standardised system for recording routine clinical data for all patients in hospital. This consistent format, provides familiarity in recognition of patient data and facilitates training in the measurement and recording of such data in a systematic and standardised way by all NHS staff.
14.3.2 The NEWS chart contains dedicated sections to record the frequency of monitoring
as defined by the score and the clinical response to a change in score, e.g. an escalation in acute care – this will facilitate tracking of the response to changes in the NEWS score. The NEWS chart also contains dedicated sections to record urine output and pain severity. These do not form part of the NEWS score.
Please note that when the measured physiological parameter exceeds the range on the chart, the actual value should be recorded on the chart.
14.3.3 Please also note that the NEWS is not designed to replace recognised generic
scoring systems such as the GCS or disease-specific systems.
West London Mental Health NHS Trust Page 13 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
14.3.4 Reproducing this chart: this chart must be reproduced in colour and in actual size,
and should not be modified or amended. 14.4 The NEWS educational tool 14.4.1 The Royal College of Physicians’ NEWS Development and Implementation Group
(NEWSDIG) commissioned the NHS Training for Innovation team to work with members of NEWSDIG, including representation from the Royal College of Nursing and the National Outreach Forum, to develop a standardised generic NEWS chart that would be suitable for downloading for use by clinical teams across the NHS. Alongside, an online training package focused on the use of NEWS has been developed to facilitate implementation (http://tfinews.ocbmedia.com).
15 Monitoring & audit
An audit of implementation of NEWS will be undertaken annually by the Clinical Service Units (CSU).
Results of the audit will be presented to the Physical Health Group and Clinical Effectiveness Group
16 Associated polices The Physical Healthcare Policy (P15) Physical Healthcare Strategy First Aid (F3) Slips, Trips and Falls (F8) Health and Safety (H3) Infection Control Policies (ICP1)
17 Glossary of Terms / Acronyms CSU Clinical Service Unit
NHS National Health Service
TPR Temperature, Pulse and Respiration
BLS Basic Life Support
CPA Care Programme Approach
RiO Records in Operation
ECT Electro-convulsive therapy
NEWS National Early Warning Scores
NEWSDIG The Royal College of Physicians’ NEWS Development and Implementation Group
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
18 Appendices
Appendix 1 - NEWS OBSERVATION CHART–front page Appendix 2 - NEWS OBSERVATION CHART INSTRUCTION – back page Appendix 3 – Escalation Flowchart - Local Services, Jubilee Ward Appendix 4 – Escalation Flowchart - Local Services, The Limes Appendix 5 – Escalation Flowchart - Local Services, H&F Appendix 6 – Escalation Flowchart - Local Services, Ealing Appendix 7 – Escalation Flowchart - Local Services, Hounslow Appendix 8 – Escalation Flowchart - Local Services, Homeward, Magnolia Appendix 9 – Escalation Flowchart - High Secure Services, Broadmoor Hospital Appendix 10 - Guidance for use of NEWS in ECT Appendix 11 – Escalation Flowchart – West London Forensic Services
West London Mental Health NHS Trust Page 15 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 1 NEWS OBSERVATION CHART – front page
West London Mental Health NHS Trust Page 16 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 2 NEWS OBSERVATION CHART INSTRUCTION- back page National early warning score (NEWS) threshold and triggers
Scores Clinical Risk
0
Total 1- 4 LOW
Individual parameter scoring 3
Total 5-6 Medium
Total 7 or more High
NEWS score of 1 - 4
Clinical risk:
LOW
NEWS score of 5 or more or 3 in one
parameter
Clinical risk:
MEDIUM
NEWS score of 7 or
more
Clinical risk:
HIGH
Complete NEWS Chart
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to crash team or accident and emergency via ambulance service (see local escalation protocols)
Registered Nurse to
immediately inform the medical team caring for the
patient. Clinical priority safe transfer
Document action in notes
Revise Care Plan as necessary
West London Mental Health NHS Trust Page 17 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 3
Escalation Flowchart – Local Services, Jubilee Ward
*Local escalation protocol: Call emergency services on ex 2222. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medial history, current medication, latest bloods.
Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk: LOW
NEWS score of 5 or more or 3 in one
parameter Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Complete NEWS Chart
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
accident and emergency via ambulance service (see local escalation protocols *)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 18 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 4
Escalation Flowchart – Local Services, The Limes
*Local escalation protocol: Call emergency services on ex 9999. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medial history, current medication, NEWS chart, latest
bloods. Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk: LOW
NEWS score of 5 or more or 3 in one
parameter Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Complete NEWS Chart
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
accident and emergency via ambulance service (see local escalation protocols)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 19 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
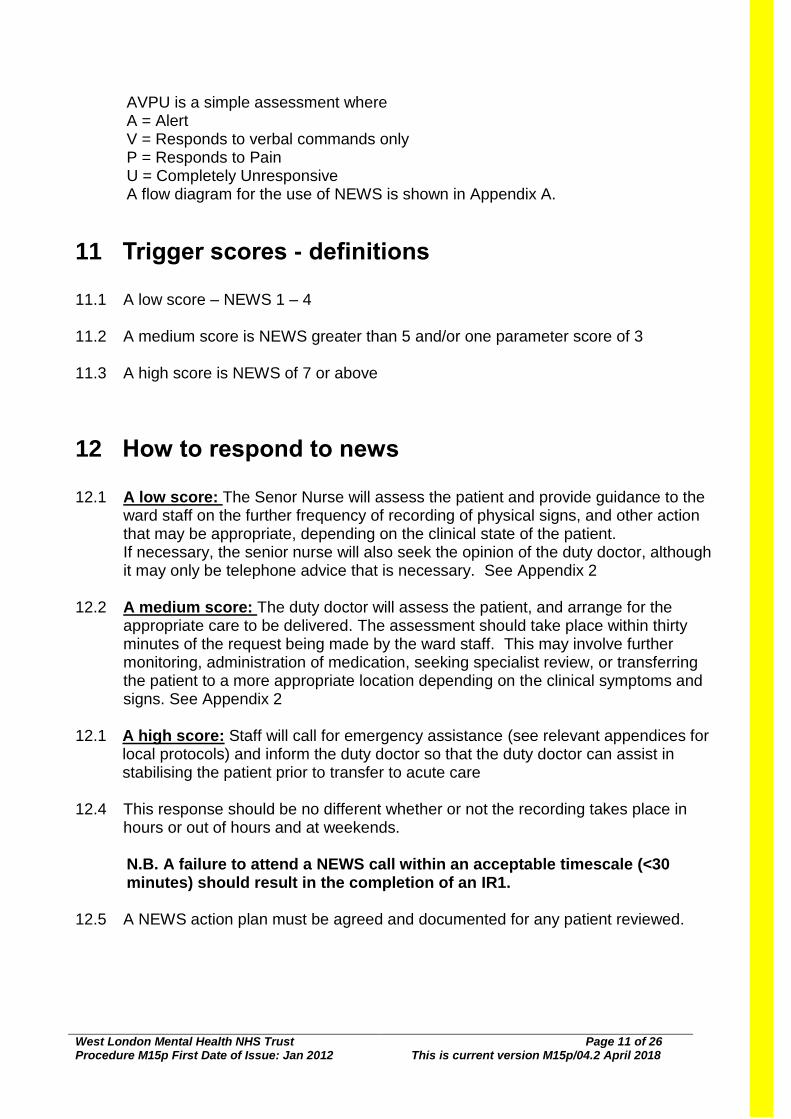
Appendix 5 Escalation Flowchart – Local Services, H&F
*Local escalation protocol: Call emergency services on ex 2222. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medial history, current medication, latest bloods.
Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk: LOW
NEWS score of 5 or more or 3 in one
parameter Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
accident and emergency via ambulance service (see local escalation protocols *)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 20 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 6 Escalation Flowchart – Local Services, Ealing
*Local escalation protocol: Call emergency services on ex 2222. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medial history, current medication, latest bloods.
Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk: LOW
NEWS score of 5 or more or 3 in one
parameter Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
accident and emergency via ambulance service (see local escalation protocols *)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 21 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
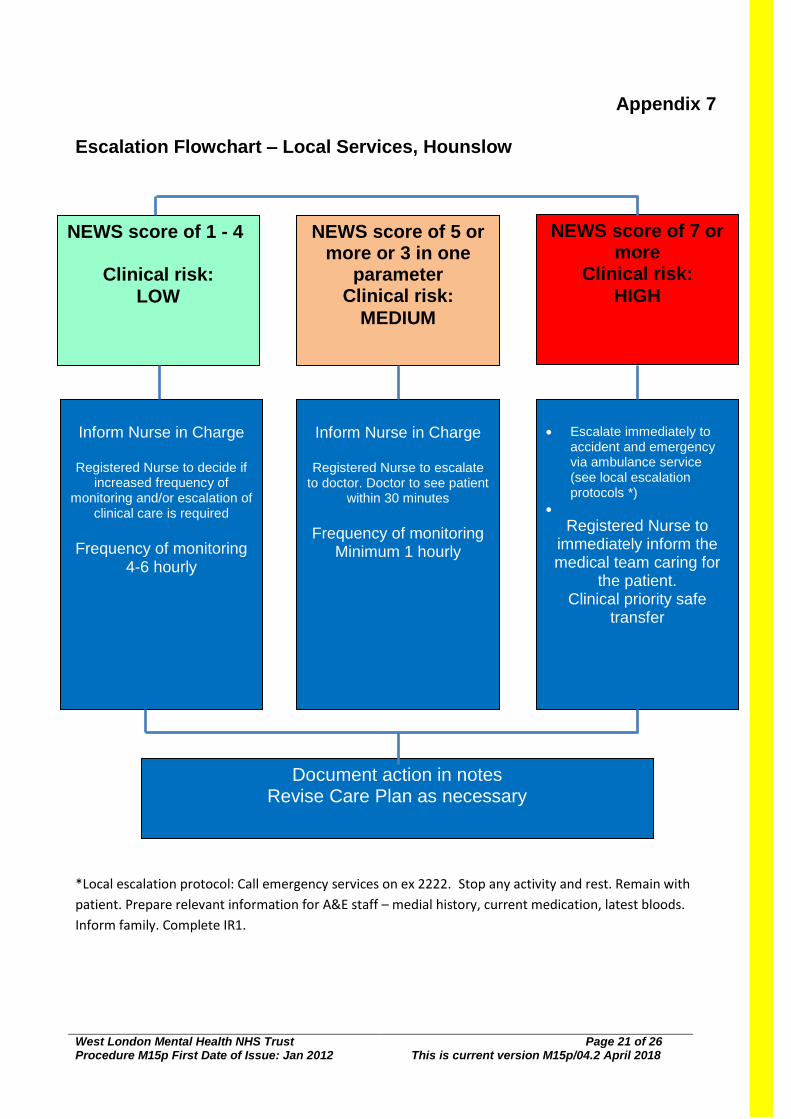
Appendix 7 Escalation Flowchart – Local Services, Hounslow
*Local escalation protocol: Call emergency services on ex 2222. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medial history, current medication, latest bloods.
Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk: LOW
NEWS score of 5 or more or 3 in one
parameter Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Inform Nurse in Charge
Registered Nurse to decide if
increased frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate
to doctor. Doctor to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to
accident and emergency via ambulance service (see local escalation protocols *)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 22 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 8 Escalation Flowchart – Local Services, Homeward & Magnolia
TOTAL
1-4
Minimum 4 hourly
Inform registered nurse who MUST assess the patient without delay. Registered nurse to decide if increased frequency of monitoring and/or escalation of clinical care is required, taking into account patient’s usual baseline.
If concerned about the patient escalate to appropriate clinician Inform the lead clinician of any deterioration
Total 5 or 6 or 3 in one parameter
Increased frequency to minimum 1 hourly
Registered nurse to seek urgent advice: Assessment by a clinician with core competencies to assess acutely ill patients; and decide if patient can still be managed safely within community hospital. Clinical care in an environment where observations can be regularly maintained
If on site, Advanced
Clinical Assessor or
doctor to assess patient.
If above not available,
registered nurse in
charge to discuss
patient’s condition with
Home ward doctor or
OOH doctor
(Home ward doctor via
020 8354 8354 / OOH
doctor: Primary care
advice (LCW) via 0300
0333444 (option 2) or On-
call SpR / Physician
(CWFT) via 020 3315
8000) as per ward
escalation protocol
Appropriate pathway for transfer to secondary care will be considered
Total 7 or more
Continuous monitoring of vital signs
Must inform the senior clinician – this may be the doctor or advanced nurse practitioner Arrange transfer to Emergency Department via LAS (999) Complete IR1 to document transfer
Wherever possible inform receiving emergency department of patients’ clinical history Contact next of kin at earliest opportunity
West London Mental Health NHS Trust Page 23 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 9
Escalation Flowchart – High Secure Services, Broadmoor Hospital
NEWS Score
Frequency of Monitoring
Clinical Response
0
As per Guidance for use of NEWS
Continue routine physical observations as set out in the Guidance
Total 1 - 4
As determined by the Medical Team
Call nurse in charge to assess They should assess within 30 mins
Plan of care recorded
Total 5 or more
or 3 in one
parameter
As determined by the Medical Team
Call doctor/on-call doctor to attend They should assess within 30 mins
Plan of care recorded
Total
7 or more
As determined by the Medical Team
Seek urgent assistance from ward team and Reassess using the NEWS scoring system
Provide BLS as required Call 222 request urgent doctor/on-call doctor assistance and ambulance providing a clear
description of the patient’s symptoms and the NEWS score
West London Mental Health NHS Trust Page 24 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 10 The Adapted National Early Warning Score (NEWS) threshold and triggers for ECT
NEWS Score
Frequency of Monitoring
Clinical Response
0
As per Guidance for use of NEWS in
ECT (see above)
Continue routine physical observations as set out in the Guidance for use of NEWS in ECT
(see above)
Total 1 - 4
As determined by the Medical Team
Registered Nurse to assess service user
Nursing team to discuss with Anaesthetist if review is required
For inpatient service users, ensure that ward team notified of score and any recommended
action by Medical Team in the ECT department.
For outpatient service users, the ECT Specialist Nurse / Lead should discuss with the Medical Team in the ECT department, whether they should notify the service users GP and the
urgency of this.
Total 5 or more
Or
3 in one
parameter
As determined by the Medical Team
Registered Nurse to immediately inform Anaesthetist
For inpatient service users, ensure that ward team notified of score and any recommended
action by Medical Team in the ECT department.
For outpatient service users, the ECT Specialist Nurse / Lead should discuss with the Medical Team in the ECT department, whether they should notify the service users GP and the
urgency of this.
Total
7 Or more
As determined by the Medical Team
Registered Nurse to immediately inform Anaesthetist
If required Call (9)999 call for ambulance to transfer service user to nearest Acute Hospital
Please refer to appropriate policies for patients who have been newly introduced to anti-psychotics.
West London Mental Health NHS Trust Page 25 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
Appendix 11 Escalation Flowchart – West London Forensic Services
*Local escalation protocol: Call emergency services on ex 2222. Stop any activity and rest. Remain with
patient. Prepare relevant information for A&E staff – medical history, current medication, latest bloods.
Inform family. Complete IR1.
NEWS score of 1 - 4
Clinical risk:
LOW
NEWS score of 5 or more or 3 in one
parameter
Clinical risk:
MEDIUM
NEWS score of 7 or more
Clinical risk:
HIGH
Inform Nurse in Charge
Registered Nurse to decide if increased
frequency of monitoring and/or escalation of
clinical care is required
Frequency of monitoring
4-6 hourly
Inform Nurse in Charge
Registered Nurse to escalate to doctor. Doctor
to see patient within 30 minutes
Frequency of monitoring
Minimum 1 hourly
Escalate immediately to accident and emergency via ambulance service (see local escalation protocols *)
Registered Nurse to immediately inform the medical team caring for
the patient. Clinical priority safe
transfer
Document action in notes Revise Care Plan as necessary
West London Mental Health NHS Trust Page 26 of 26
Procedure M15p First Date of Issue: Jan 2012 This is current version M15p/04.2 April 2018
19. References 1 Hennekens CH, Hennekens AR, Hollar D et al (2005). Schizophrenia and increased risks of cardiovascular disease.
Am Heart J 150:6:1115–1121
2 National Institute for Health and Clinical Excellence (2009) Schizophrenia: Core Interventions for the treatment and
Management of Schizophrenia in Primary and Secondary Care (Update).NICE, London.
https://www.nice.org.uk/guidance/cg82
Accessed 17th
July 2016
3 Osborn DPJ, King MN, Nazareth I (2006). Risk of cardiovascular disease in people with SMI: across sectional
comparative study in primary care. Br J Psychiatry 188: 271-277.
4 Rethink (2013) Lethal Discrimination: Why People with Mental Illness are Dying Needlessly and What Needs to
Change. Rethink, London
5 Department of Health (2012) No Health Without Mental Health: A Guide for Clinical Commissioning Groups.