88
Product Monograph Prescribing information can be found on the back cover

Product Monograph
Developed by Astellas Pharma Europe Limited*, Lovett House, Lovett Road, Staines, TW18 3AZ. Registered in England and Wales under Registered no. 2486792Date of Preparation: 03/2012. Item Code: FDX/11/0002/EUl*Astellas Pharma Europe Limited, located in the UK, is a European subsidiary of Tokyo-based Astellas Pharma Inc. ASTELLAS, LEADING LIGHT FOR LIFE, CHANGING TOMORROW and the Star logo are trademarks of Astellas Pharma Inc. and its related entities.
DificlirTM (fidaxomicin) Prescribing Information
Presentation: Dificlir™ tablets contain 200 mg fidaxomicin. Indication: The treatment of Clostridium difficile infections (CDI) also known as C. difficile-associated diarrhoea (CDAD) in adults. Consideration should be given to official guidelines on the appropriate use of antibacterial agents. Posology and method of administration: Adults and elderly (≥ 65 years of age): The recommended dose is one 200 mg tablet to be administered twice daily (once every 12 hours) for 10 days and can be taken with or without food. Paediatrics: The safety and efficacy of fidaxomicin in children aged below 18 years has not yet been established. Renal impairment: No dose adjustment is considered necessary. Use with caution in patients with severe renal impairment. Hepatic impairment: No dose adjustment is considered necessary. Use with caution with in patients with moderate to severe hepatic impairment. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Warnings and Precautions: Due to limited clinical data, fidaxomicin should be used with caution in patients with severe renal impairment or moderate to severe hepatic impairment. Fidaxomicin should also be used with caution in patients with pseudomembranous colitis, fulminant or life threatening CDI. No data is available in patients with concomitant bowel disease, caution should be used in these patients due to a risk of enhanced absorption and a potential risk for systemic adverse reactions. Co-administration of potent P-glycoprotein inhibitors such as cyclosporine, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and
amiodarone is not recommended. Drug interactions: Fidaxomicin is a substrate of P-gp and may be a mild to moderate inhibitor of intestinal P-gp. Co-administration of potent inhibitors of P-gp, such as cyclosporine, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and amiodarone are not recommended. Fidaxomicin had a small but not clinically relevant effect on digoxin exposure and a larger effect on P-gp substrates with lower bioavailability more sensitive to intestinal P-gp inhibition such as dabigatran etexilat cannot be excluded. Undesirable effects: Common (≥ 1/100 to < 1/10): vomiting, nausea, constipation. Uncommon (≥ 1/1,000 to < 1/100): decreased appetite, dizziness, headache, dysgeusia, abdominal distension, flatulence, dry mouth, increased alanine aminotransferase. Consult SmPC for complete information on side effects. Packs and Cost: 200 mg tablet x 20, £1,350.00. Legal Classification: POM. Marketing authorisation number: EU/1/11/733/001-004 Date of Preparation of PI: March 2012. Further information available from: Astellas Pharma Ltd, Future House, 3rd Floor, The Glanty, Egham, Surrey TW20 9AH. For Medical Information phone 0800 783 5018
Prescribing information can be found on the back cover
Adverse events should be reported. Reporting forms and information can be found at
www.mhra.gov.uk/yellowcard.
Adverse events should also be reported to Astellas Pharma Ltd. Please contact 0800 783 5018

© March 2012 Astellas Pharma Europe Ltd.
All Trade Marks, unless third party trademarks, are owned by Astellas Pharma Inc and/or its related entities. Third party trademarks, where referred to, are owned by originator companies and are represented here under license and/or with permission and/or with acknowledgement of their ownership.
Note: For non-English language versions of this Product Monograph
Figure 3 is translated with permission. The Canadian Medical Association is the copyright owner of “Figure 1: pathogenesis of Clostridium difficile-associated diarrhea in adults”, originally published in the CMAJ. The limited permission granted to translate into the French/German/Spanish/Portuguese/Greek/Italian/Czechoslovakian/Danish/Swedish/Finish/Norwegian/Hungarian/Russian/Dutch language does not extend to any other organization or person. The Canadian Medical Association and the authors of the original work are not responsible for the translation and do not necessarily endorse the accuracy or quality of the translation.
1
Table of contents
List of tables ........................................................................................................................................................................5
List of figures ......................................................................................................................................................................7
List of abbreviations.....................................................................................................................................................8
1. Introduction ............................................................................................................................................................... 11
1.1. Introduction ............................................................................................................................................................11
1.2. Overview of Clostridium difficile infection .............................................................................................12
1.3. Benefits of DIFICLIR – a targeted therapy for CDI .............................................................................13
1.4. Summary ...................................................................................................................................................................14
1.5. References ................................................................................................................................................................15
2. Microbiology, epidemiology and management of CDI ...................................................... 17
2.1. Clostridium difficile ..............................................................................................................................................17
2.1.1. History and classification ...........................................................................................................................17
2.1.2. Life cycle ...........................................................................................................................................................17
2.1.3. Pathogenesis of CDI .....................................................................................................................................18
2.1.4. Clinical presentation of infection with C. difficile .............................................................................20
2.1.4.1. Clinical presentation of CDI ......................................................................................................................20
2.1.4.2. Complications of CDI .................................................................................................................................20
2.1.5. Morbidity, mortality and burden of CDI................................................................................................21
2.1.5.1. Morbidity and mortality ............................................................................................................................21
2.1.5.2. Burden of CDI ..............................................................................................................................................21
2.1.6. Risk factors for development of CDI ......................................................................................................22
2.1.7. Recurrence of CDI .........................................................................................................................................23
2.1.7.1. Recurrence ..................................................................................................................................................23
2.1.7.2. Risk factors for recurrent CDI ....................................................................................................................23
2.2. Epidemiology of CDI ...........................................................................................................................................23
2.2.1. Epidemiology of CDI in Europe ................................................................................................................23
2.2.2. Changing epidemiology: increasing incidence and disease severity ..........................................24
2.2.3. Hypervirulent strains of C. difficile ..........................................................................................................25
2
2.3. Current management of CDI ..........................................................................................................................26
2.3.1. Diagnosis of CDI .............................................................................................................................................26
2.3.1.1. Signs and symptoms of CDI .......................................................................................................................26
2.3.1.2. Laboratory tests for CDI ............................................................................................................................27
2.3.2. Treatment of CDI ...........................................................................................................................................28
2.3.2.1. Pharmacotherapy of an initial episode of CDI and treatment guidelines ..............................................28
2.3.2.2. Pharmacotherapy of recurrent CDI and treatment guidelines ................................................................29
2.3.2.3. Pharmacotherapy for CDI: summary of ESCMID treatment guidelines ..................................................29
2.3.2.4. Management of complications of CDI and treatment guidelines ..........................................................30
2.3.2.5. Deficiencies associated with current management .................................................................................30
2.4. Rationale for a new treatment ......................................................................................................................32
2.5. Summary ...................................................................................................................................................................33
2.6. References ................................................................................................................................................................34
3. Pharmacology and pharmacokinetics of DIFICLIR ................................................................ 37
3.1. Chemical structure ..............................................................................................................................................37
3.2. Mechanism of action ..........................................................................................................................................37
3.3. Pharmacokinetics .................................................................................................................................................38
3.3.1. Absorption .......................................................................................................................................................38
3.3.1.1. Plasma levels ...............................................................................................................................................38
3.3.1.2. Effect of food on absorption .....................................................................................................................39
3.3.2. Distribution, metabolism and excretion ................................................................................................40
3.3.2.1. Metabolism of DIFICLIR ..............................................................................................................................40
3.3.2.2. Excretion of DIFICLIR ..................................................................................................................................40
3.4. Drug–drug interactions ......................................................................................................................................41
3.5. Use of DIFICLIR in specific patient groups .............................................................................................41
3.5.1. Pregnancy and breastfeeding ....................................................................................................................41
3.5.2. Paediatric population ....................................................................................................................................41
3.5.3. Use in elderly patients (aged ≥65 years) ................................................................................................41
3.6. Summary ...................................................................................................................................................................42
3.7. References ................................................................................................................................................................42
3
4. Antimicrobial profile of DIFICLIR ........................................................................................................... 43
4.1. Spectrum of antibacterial activity ...............................................................................................................43
4.1.1. Activity against C. difficile ...........................................................................................................................43
4.1.2. Activity against other Gram-positive bacteria .....................................................................................43
4.1.3. Low risk of acquisition of VRE ...................................................................................................................44
4.1.4. Activity against Gram-negative bacteria ................................................................................................44
4.2. Pharmacodynamic effects of DIFICLIR in vitro .....................................................................................44
4.2.1. Bactericidal action ..........................................................................................................................................45
4.2.2. Post-antibiotic effect ...................................................................................................................................47
4.2.3. Inhibition of C. difficile sporulation and toxin production ...............................................................48
4.3. In vitro activity of DIFICLIR ..............................................................................................................................49
4.3.1. Epidemiological cut-off value for DIFICLIR and C. difficile ..............................................................49
4.3.2. Resistance .........................................................................................................................................................49
4.4. In vivo activity in animal models ...................................................................................................................49
4.5. Summary ...................................................................................................................................................................50
4.6. References ................................................................................................................................................................50
5. Use, posology and administration........................................................................................................ 53
5.1. Indication ...................................................................................................................................................................53
5.2. Posology and method of administration .................................................................................................53
5.3. Use in specific patient populations ............................................................................................................53
5.3.1. Pregnancy and breastfeeding ....................................................................................................................53
5.3.2. Paediatric population ....................................................................................................................................53
5.3.3. Elderly patients (aged ≥65 years) ..............................................................................................................53
5.3.4. Renal impairment ...........................................................................................................................................53
5.3.5. Hepatic impairment .......................................................................................................................................53
5.4. Overdose ...................................................................................................................................................................53
5.5. References ...............................................................................................................................................................53
4
6. Clinical efficacy of DIFICLIR in CDI ...................................................................................................... 55
6.1. Overview of phase 2A proof-of-concept study ..................................................................................55
6.1.1. Primary efficacy analysis .............................................................................................................................56
6.1.2. Secondary efficacy analysis .......................................................................................................................56
6.1.3. Summary of phase 2A study observations ...........................................................................................56
6.2. Overview of phase 3 registration trials .....................................................................................................56
6.2.1. Trial objectives and analysis populations...............................................................................................59
6.2.2. Primary efficacy analysis .............................................................................................................................60
6.2.3. Secondary efficacy analysis ........................................................................................................................60
6.3. Efficacy in specific subpopulations ............................................................................................................62
6.3.1. Patients aged ≥65 years and ≥75 years ..................................................................................................63
6.3.2. Severity of CDI ................................................................................................................................................63
6.3.3. Infection with hypervirulent C. difficile ..................................................................................................64
6.3.4. Concomitant antibacterial therapy ..........................................................................................................65
6.3.5. Patients with renal impairment .................................................................................................................67
6.3.6. Recurrent CDI ..................................................................................................................................................68
6.4. Summary ...................................................................................................................................................................68
6.5. References ................................................................................................................................................................69
7. Safety and tolerability of DIFICLIR ....................................................................................................... 71
7.1. Overview of safety data from phase 3 trials .........................................................................................71
7.2. DIFICLIR – GI safety profile .............................................................................................................................74
7.3. DIFICLIR – cardiac safety profile ..................................................................................................................76
7.4. DIFICLIR – renal safety profile .......................................................................................................................77
7.5. DIFICLIR – clinical chemistry parameters and vital signs ...............................................................77
7.6. Summary ...................................................................................................................................................................77
7.7. References ...............................................................................................................................................................78
8. Summary and key points............................................................................................................................... 79
8.1. Summary ...................................................................................................................................................................79
8.2. Key points .................................................................................................................................................................81
8.3. References ................................................................................................................................................................82

5
List of tables
Table 1. Clinical experience with DIFICLIR in patients with CDI ...........................................................................................13
Table 2. Asymptomatic carriage and clinical manifestations of CDI ....................................................................................20
Table 3. Age-specific incidence of CDI and attributable mortality ......................................................................................21
Table 4. Antibacterials and risk of colonisation with C. difficile ..........................................................................................22
Table 5. Risk factors associated with the development of nosocomial CDI ........................................................................22
Table 6. Risk factors associated with the development of recurrent CDI ............................................................................23
Table 7. Factors associated with increased incidence of CDI in hospitalised patients ......................................................24
Table 8. Characteristics of epidemic C. difficile ribotype 027 .............................................................................................25
Table 9. Clinical signs and symptoms and findings from radiographic and laboratory examination that are suggestive of CDI ........................................................................................................................................................26
Table 10. Advantages and disadvantages of diagnostic tests for C. difficile........................................................................27
Table 11. European (ESCMID) guidelines for pharmacotherapy of CDI ...................................................................................30
Table 12. Clinical experience with DIFICLIR in patients with CDI ...........................................................................................32
Table 13. Mean peak plasma concentrations following a single oral dose of DIFICLIR 100–450 mg to healthy volunteers (n=16) .......................................................................................................................................................38
Table 14. Pharmacokinetic profile of DIFICLIR and OP-1118 following administration of an oral dose of 200 mg to fasted healthy volunteers .......................................................................................................................39
Table 15. Mean plasma concentrations of DIFICLIR and OP-1118 following oral doses of DIFICLIR 200 mg bid for up to 10 consecutive days in phase 3 trials ........................................................................................................39
Table 16. Faecal concentrations of DIFICLIR and OP-1118 following daily oral administration of DIFICLIR 150 mg, 300 mg or 450 mg to healthy volunteers for 10 consecutive days .........................................................................40
Table 17. Faecal concentrations of DIFICLIR and OP-1118 following administration of DIFICLIR 200 mg bid to CDI patients in the phase 3 trials .........................................................................................................................40
Table 18. Plasma concentrations of DIFICLIR and OP-1118 in CDI patients treated with DIFICLIR 200 mg bid in the phase 3 trials, stratified by age ......................................................................................................................42
Table 19. Compilation of in vitro activity of DIFICLIR against clinical isolates of C. difficile ..............................................43
Table 20. Activity of DIFICLIR in vitro against 792 strains of C. difficile isolated from patients enrolled in phase 3 trials (pooled analysis) .................................................................................................................................43
Table 21. Isolates of C. difficile used in time-kill experiments ..............................................................................................45
Table 22. Effect of exposure to DIFICLIR and vancomycin on C. difficile toxin production .................................................49
Table 23. Inclusion criteria in the open-label phase 2A proof-of-concept study .................................................................55
Table 24. Primary and secondary outcome measures in the phase 2A proof-of-concept study .........................................56
Table 25. Main criteria for inclusion in the phase 3 registration trials ...................................................................................57
Table 26. Demographic and baseline clinical characteristics of patients enrolled in the phase 3 registration trials (mITT population) ........................................................................................................................58
6
Table 27. Representation of patients in relation to CDI severity in the phase 3 registration trials (mITT population) .....58
Table 28. Definition of efficacy analysis populations and outcome measures in the phase 3 registration trials ...............60
Table 29. Treatment outcome in relation to age in the phase 3 registration trials (mITT population; a priori analysis) ...63
Table 30. Treatment outcome in relation to disease severity in the phase 3 registration trials (mITT population; a priori analysis) ..........................................................................................................................64
Table 31. Outcomes in DIFICLIR- versus vancomycin-treated patients in relation to isolate ribotype in the phase 3 registration trials (PP population; a priori analysis) ................................................................................................65
Table 32. Summary of adverse reactions with DIFICLIR by MedDRA system organ class .....................................................71
Table 33. Frequency of AEs in patients treated with DIFICLIR and vancomycin in phase 3 trials (pooled data) ..................72
Table 34. AEs occurring in ≥5% of patients in the DIFICLIR and vancomycin treatment arms ..............................................72
Table 35. AEs reported by >1 patient for which study medication was stopped permanently or patient was withdrawn from the study ..................................................................................................................................73
Table 36. Frequency of SAEs in patients treated with DIFICLIR or vancomycin .....................................................................73
Table 37. Frequency of AEs, SAEs and deaths in patients treated with DIFICLIR or vancomycin according to age .............74
Table 38. Frequency of GI-TEAEs and deaths from GI-TEAEs in patients treated with DIFICLIR or vancomycin .................74
Table 39. Frequency and nature of GI bleeding events in patients treated with DIFICLIR or vancomycin ...........................75
Table 40. Frequency of changes from baseline in QTc interval and QTc intervals at end of the study in patients treated with DIFICLIR or vancomycin .........................................................................................................76
Table 41. Frequency of deaths from cardiac AEs in patients treated with DIFICLIR or vancomycin .....................................76

7
List of figures
Figure 1. Life cycle of C. difficile ..............................................................................................................................................17
Figure 2. Coloured scanning electron micrographs of the vegetative form and endospores of C. difficile .......................17
Figure 3. Cycle of infection with C. difficile ............................................................................................................................18
Figure 4. Key steps in the pathogenesis of CDI .......................................................................................................................19
Figure 5. Model for the acquisition of CDI ...............................................................................................................................19
Figure 6. Images obtained from endoscopic examination of a healthy colon (left-hand picture) and from a patient with pseudomembranous colitis (right-hand picture) in which the characteristic inflamed mucosa studded with adherent white plaques (pseudomembranes) can be seen ............................................................................20
Figure 7. Distribution of C. difficile PCR ribotypes across Europe ........................................................................................25
Figure 8. Diagnostic algorithm for CDI .....................................................................................................................................28
Figure 9. Comparative efficacy of vancomycin and metronidazole for treatment of patients stratified by CDI severity ...29
Figure 10. Rates of treatment failure (A) with metronidazole and disease recurrence (B) with vancomycin and metronidazole .....................................................................................................................................................31
Figure 11. Chemical structure of DIFICLIR .................................................................................................................................37
Figure 12. Illustrated model of the initiation of clostridial messenger RNA synthesis showing the stages that are inhibited by DIFICLIR, myxopyronin and the rifamycins ..........................................................................................38
Figure 13. Comparative effects of DIFICLIR and vancomycin on acquisition of VRE ...............................................................44
Figure 14. Colonic levels of B. fragilis before (Day 0) and after treatment (Day 10) with DIFICLIR or vancomycin ...............44
Figure 15. Bactericidal effects of DIFICLIR, OP-1118 and vancomycin against five strains of C. difficile, including two laboratory-generated mutant strains to which DIFICLIR exhibited reduced activity ............................................46
Figure 16. Recovery kinetics of C. difficile strains ATCC 9689 (A), LC3 (B) and ATCC 43255 (C) following 1-hour exposure to DIFICLIR (with or without transferred cells), vancomycin or no-drug control ..................................47
Figure 17. Effect of exposure to DIFICLIR and vancomycin on sporulation by C. difficile strain ATCC 43255 ......................48
Figure 18. Design of the phase 3 DIFICLIR registration trials ...................................................................................................57
Figure 19. Disposition of patients in the two phase 3 registration trials ...............................................................................59
Figure 20. Rates of clinical cure in the mITT and PP populations of phase 3 trials (studies 003 and 004) ............................61
Figure 21. Rates of recurrence among clinically cured patients in the mITT and PP populations of phase 3 trials (studies 003 and 004) ..................................................................................................................................................61
Figure 22. Rates of sustained clinical cure in the mITT and PP populations of phase 3 trials (studies 003 and 004) ..........62
Figure 23. Rates of recurrence of CDI among the cohorts of patients with and without any concomitant antibacterial therapy (post hoc analysis) .................................................................................................................66
Figure 24. Rates of sustained clinical cure among the cohorts of patients with and without concomitant antibacterial therapy (post hoc analysis) .................................................................................................................67

8
List of abbreviations
AE adverse event
ATCC American Type Culture Collection
AUC area under the plasma concentration–time curve
BI restriction-endonuclease analysis group BI strain of C. difficile (also known as NAP1/027)
bid twice daily
bm bowel movements
CA concomitant antibacterials
CCA cell-culture cytotoxic assay
CDAD Clostridium difficile-associated diarrhoea
CDI Clostridium difficile infection
CFU colony forming unit
CLSI Clinical Laboratory Standards Institute
Cmax maximum plasma concentration
CYP450 cytochrome P450
DNA deoxyribonucleic acid
ECDC European Centre for Disease Control and Prevention
ECG electrocardiogram
EIA enzyme immunoassay
EOS end of study
EOT end of treatment
ESCMID European Society of Clinical Microbiology and Infectious Diseases
FDA United States Food and Drug Administration
FSR frequency of spontaneous resistance
GDH glutamate dehydrogenase
GI gastrointestinal
GI-TEAE gastrointestinal treatment-emergent adverse event
HIV human immunodeficiency virus
HPA United Kingdom’s Health Protection Agency
ICU intensive care unit
IDSA Infectious Diseases Society of America

9
IgG immunoglobulin G antibody
INF interferon
IV intravenous
LLOQ lower limit of quantification
MedDRA Medical Dictionary for Regulatory Activities
MIC minimum inhibitory concentration
MIC50 minimum concentration required to inhibit growth of 50% of organisms
MIC90 minimum concentration required to inhibit growth of 90% of organisms
mITT modified intent-to-treat
mRNA messenger ribonucleic acid
MRSA methicillin-resistant Staphylococcus aureus
NADPH nicotinamide adenine dinucleotide phosphate
NAP1 North American pulsed-field gel electrophoresis type 1 strain of C. difficile (also known as REA group BI/027)
NC not calculated
ND no data
NS not significant
PAE post-antibiotic effect
PCR polymerase chain reaction
PFGE pulsed-field gel electrophoresis
P-gp P-glycoprotein
PP per protocol
qid four-times daily
QTc QT interval corrected for heart rate
REA restriction-endonuclease analysis
RNA ribonucleic acid
SAE serious adverse event
SD standard deviation
SHEA Society for Healthcare Epidemiology of America
spp. species
t1/2 terminal elimination half-life
TEAE treatment-emergent adverse event

10
tid three-times daily
Tmax time to peak concentration
UBM unformed bowel movements
VRE vancomycin-resistant enterococci
WBC white blood cell
λz terminal rate disposition constant

11
Chapter 1: Introduction
1.1 IntroductionClostridium difficile is the leading cause of infectious nosocomial diarrhoea in industrialised countries1 and the incidence and severity of C. difficile infection (CDI) are increasing.2–6 CDI is associated with significant morbidity and represents a large clinical burden due to the resultant diarrhoea and potentially life-threatening complications, including pseudomembranous colitis, toxic megacolon, perforations of the colon and sepsis.7–9 The clinical burden of CDI is compounded by the fact that as many as 25% of patients with CDI suffer a recurrence of infection within 30 days following treatment.10–12 In a recent European survey of patients with suspected CDI or diarrhoea that developed ≥3 days after hospital admission, C. difficile was the attributive cause of mortality in 2% of patients and was contributory in a further 7% of cases.2
The intrinsic ability of C. difficile to produce spores that are resistant to standard sanitary procedures, and which can persist both in patients and in the environment, is a major factor associated with its transmission.7,13,14 Once ingested, the dormant spores can enter the active vegetative state if conditions are favourable. For example, in conditions where the protective effects of the normal gut microflora are disrupted, such as in patients who are taking or have recently taken broad-spectrum antibiotics, the vegetative C. difficile bacteria may be able to colonise the gut.14 From there, C. difficile produces toxins that injure the lining of the colon, leading to diarrhoea, inflammation and, in severe cases, pseudomembranous colitis.14 Following antibacterial therapy for CDI, spores may persist within the intestines of patients, leading to relapse.7,13–15
In hospitalised or vulnerable patients, such as those with an already compromised gut microflora or patients whose immune function is reduced (e.g. those receiving immunosuppressive therapy), a cycle of infection and recurrence can ensue, triggering repeated episodes of diarrhoea and a downward spiral of decline.15 A patient may gradually become weaker, exhausted and less able to recover to their previous health status. Since CDI and recurrent CDI commonly affect vulnerable patients, such as those who are immunocompromised,16 on certain antibiotics,2,17–20 who are renally impaired,21,22 or patients aged over 65 years,2,19,20 the consequences can be severe, potentially culminating in a permanent reduction in function and/or death.8,23
As well as the significant personal and clinical burden they are associated with, both CDI and recurrent CDI have an important economic impact due to an increased length and cost of hospitalisation.24–26 Furthermore, since CDI is a disease that affects a high proportion of patients aged ≥65 years, its economic burden is expected to increase over the coming years as the world’s population ages.27
Up until now, the treatment of CDI has relied on oral and intravenous (IV) metronidazole and oral vancomycin.28 Both agents are initially effective in treating mild-to-moderate CDI, with cure rates of 84–97%;29 but among patients with severe disease, response rates for vancomycin have been reported to be significantly greater versus metronidazole (97% vs. 76%; p=0.02). The recurrence of CDI is a serious and difficult-to-treat problem,28 occurring in up to 25% of patients within 30 days of the cessation of treatment.10–12 Some patients may even suffer repeated recurrences for years following their initial infection.15 Vancomycin and, to a lesser extent, metronidazole have non-selective antibacterial activity, suppressing many of the gut bacteria including the commensal microflora that compete with C. difficile for nutrients and other resources.30–32
The European Society of Clinical Microbiology and Infectious Diseases (ESCMID) has highlighted recurrence as the most important problem in the management of CDI.28 New treatment options are needed that specifically target C. difficile, while having minimal impact on the normal bowel microflora, which help prevent further colonisation and growth of the bacteria.33
DIFICLIR™ (fidaxomicin) is a novel oral macrocyclic antibacterial agent with bactericidal activity specifically targeted against C. difficile.34 Unlike other agents used in the treatment of CDI, DIFICLIR has limited activity against the commensal gut microflora.35–37
DIFICLIR has been evaluated in studies involving >1,000 patients with CDI.11,38,39 In the pivotal phase 3 trials, DIFICLIR met its primary endpoint of non-inferiority to oral vancomycin with respect to clinical cure at end of therapy.11,39 DIFICLIR significantly reduced the rate of recurrence, leading to rates of sustained clinical cure (defined as clinical cure with no recurrence during the 30-day follow-up period) that were superior to vancomycin.11,39
The systemic absorption of DIFICLIR is low, enabling it to act locally at the gut level where CDI arises, with minimal risk of systemic adverse events.40 DIFICLIR has a favourable safety profile that is comparable to that seen with oral vancomycin.11,39
1

12
This monograph provides an overview of the microbiology, epidemiology and management of CDI. It also reviews the preclinical profile of DIFICLIR, and reports the efficacy and safety data from its pivotal clinical studies.
1.2. Overview of Clostridium difficile infectionA number of patients are at increased risk of CDI including:
• Patients who are immunocompromised,41 such as those with human immunodeficiency virus (HIV)42 or who are receiving chemotherapy43
• Those currently receiving or who recently received broad-spectrum antibiotic therapy2,17,44
• Individuals/patients aged over 65 years2,17
• Those receiving gastric acid suppression therapy17,45
• Those with serious underlying diseases2
• Those in intensive care units (ICUs)17
• Patients who have recently undergone non-surgical gastrointestinal procedures or those being tube-fed.17
Although CDI often occurs in hospitalised patients, it may also occur and spread within nursing and care homes. Recently, CDI has been reported in the community as well as in patients considered to be at lesser risk of infection.2
Since 2003, there has been a rise in the prevalence of CDI.2 The reasons for this increase are multifactorial and may include an increasingly aging population,27 increased numbers of immunocompromised patients,27 hospital overcrowding,46 inadequate infection control practices46 and the presence of more virulent strains of the bacteria.47,48
CDI is associated with high morbidity as well as mortality and frequently recurs, with up to 25% of patients suffering a recurrence of CDI within 30 days of the initial infection.10–12
CDI also imposes a significant economic burden on European healthcare systems. The length of hospital stay as a result of the infection can be increased by approximately 7–21 days versus uninfected patients25,26 and there are significant costs associated with treating recurrent infections. Together, both metronidazole and vancomycin are initially effective in treating mild-to-moderate CDI, with cure rates of 84–97%.29 However, among patients with severe disease, response rates for vancomycin have been reported to be significantly greater versus metronidazole (97% vs. 76%; p=0.02). Furthermore, these agents act non-selectively and hence can produce gut conditions that could favour
overgrowth of C. difficile. More effective treatments are needed to selectively target C. difficile while having a minimal impact on the normal gut microflora, which compete with C. difficile in the intestines to inhibit colonisation.28 Such agents could have a significant clinical and economic impact.
For mild cases of CDI, cessation of the antibacterial therapy that may have precipitated the infection may be the only action required.28 However, most patients with CDI require more intensive therapy. This includes patients in whom symptoms persist despite cessation of concomitant antibiotics, those in whom symptoms worsen, or those who have a high risk of recurrence. A number of risk factors for recurrence have been identified. These include patients who are immunocompromised,16 on certain concomitant antibiotics,2,18–20 who are renally impaired,21,22 or patients aged 65 years or over.2,19,20
Oral and IV metronidazole and oral vancomycin have been the mainstays of treatment for CDI to date.28 Metronidazole is currently recommended for the treatment of non-severe disease, with vancomycin being recommended, either alone or in combination with metronidazole, in cases of severe CDI.28 Both agents are effective in treating CDI;29 however, up to 25% of patients experience recurrence within 30 days following treatment.10–12 Patients with a recurrent episode of CDI are at an increased risk of subsequent recurrences.15 Approximately 45% of patients with recurrent CDI experience a subsequent episode.15
ESCMID has identified recurrence as being the most important problem in the treatment of CDI.28 A lack of effective treatments for recurrence has prompted the use of alternative therapies such as faecal bacteriotherapy to help restore the normal colonic microflora in patients with refractory and recurrent CDI.49 Reducing the incidence of recurrence could potentially reduce the clinical burden, lower the economic impact of treating additional episodes of CDI, and reduce the rate of person-to-person transmission.11
The high rate of recurrent infection following treatment with vancomycin and metronidazole (up to 25%),10–12 is among the most significant drawbacks to these therapeutic options. This limitation is particularly apparent for patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic, such as patients who are immunocompromised,16 receiving concomitant antibiotics,2,18–20 who are renally impaired,21,22 or those aged 65 years or over.2,19,20 In addition, there are high rates of treatment failure with metronidazole (approximately 18%)50 and a tendency for both vancomycin
ESCMID has identified recurrence as being the most important problem in the treatment of CDI
Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic include those who:
• Are immuno-compromised
• Are receiving concomitant antibiotics
• Are renally impaired• Are aged 65 years
or over
13
and metronidazole to promote overgrowth of vancomycin-resistant enterococci (VRE) in patients already colonised with VRE.51 While rare, enterococcal infections, such as VRE bacteraemia, can be potentially fatal.52 These drawbacks demonstrate the need for innovative treatments for CDI, especially at a time of increasing incidence.
The ideal treatment for CDI should be effective against C. difficile and achieve high rates of clinical cure that are at least equivalent to vancomycin. It should also reduce the risk of recurrence, as well as being well tolerated.33 The inhibition of spore and toxin production, and minimal effects on the normal bowel microflora, would also be desirable properties.
1.3. Benefits of DIFICLIR – a targeted therapy for CDIDIFICLIR is a novel oral macrocyclic antibacterial agent with targeted activity against C. difficile and minimal impact on the normal colonic microflora.53 By having a minimal impact on the normal colonic microflora, DIFICLIR has the potential to positively impact recurrence rates since the normal colonic microflora can compete at the mucosal surface with C. difficile. Furthermore, DIFICLIR inhibits C. difficile spore production, as well as toxin production,37,54–56 which are important in the pathogenesis of CDI, recurrent CDI and transmission of the infection.
DIFICLIR is a locally acting drug.34 DIFICLIR and its main active metabolite (OP-1118) undergo negligible systemic absorption following oral administration and are detectable only at very low levels in plasma.34,40
Low systemic exposure to DIFICLIR34 minimises the risk of systemic adverse events (AEs), giving DIFICLIR a tolerability profile similar to oral vancomycin.11,39 High faecal levels,42 a long post-antibiotic effect (PAE)57 and the low likelihood of resistance development58 provide further clinical benefits.
The recommended dose of DIFICLIR for adults, including those aged ≥65 years, is 200 mg administered twice daily for 10 days.34
The efficacy and safety of DIFICLIR in patients with CDI were first investigated in a phase 2A proof-of-concept study.38 This was subsequently confirmed in two phase 3 registration studies,*11,39 the largest comparative studies with vancomycin in CDI conducted to date (Table 1) enrolling more than 1,000 patients, over half of whom were aged ≥65 years.
There is an urgent need for new, innovative treatments for CDI to address deficiencies with current therapies, particularly the risk of recurrence
Table 1. Clinical experience with DIFICLIR in patients with CDI11,38,39
Trial Description DIFICLIR Vancomycin
Phase 2A38 Randomised, open-label, dose-ranging study of 10 days’ duration
50 mg bid; 100 mg bid; 200 mg bid
n=48
None
Phase 3 (003)11 North American multicentre, double-blind, randomised, parallel-group study of 10 days’ duration
200 mg bidn=302
125 mg qidn=327
Phase 3 (004)39 Multinational, multicentre, double-blind, randomised, parallel-group study of 10 days’ duration
200 mg bidn=270
125 mg qidn=265
bid, twice daily; qid, four-times daily
*Note: The two phase 3 trials of DIFICLIR versus vancomycin (studies OPT-80-003 and OPT-80-004)11,39 will be referred to from this point onwards as study 003 and study 004, respectively.
14
The results from the pivotal phase 3 studies in CDI demonstrated that treatment with DIFICLIR was comparable to vancomycin in respect of clinical cure (primary endpoint). Additionally, patients treated with DIFICLIR showed a significantly reduced rate of recurrence compared with those treated with vancomycin, resulting in a significantly higher sustained clinical cure (defined as clinical cure plus no relapse within 30 days). Further analyses of results from the phase 3 studies revealed other potential advantages with DIFICLIR, including:
• Significant reductions in recurrence of CDI among patients who had experienced a previous episode within 3 months of entering the study (a priori analysis, data not collected as a pre-defined endpoint)59
• Potentially improved clinical cure and reduced likelihood of recurrence in patients requiring concomitant antibacterial therapy in one analysis (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint).60
All these topics are discussed in further detail in the following chapters of this monograph.
DIFICLIR has been evaluated in studies involving >1,000 patients with CDI, where it was comparable to oral vancomycin in terms of clinical cure and superior in terms of recurrence and sustained clinical cure
1.4. Summary
Key points
• C. difficile is the leading cause of nosocomial diarrhoea in industrialised countries and the incidence of CDI is increasing
• In a European survey, C. difficile was the attributive cause of mortality in 2% of patients and was contributory in a further 7% of cases
• Recurrence of CDI is a serious and difficult-to-treat problem
• ESCMID has identified recurrence as being the most important problem in the treatment of CDI
• Up to 25% of CDI patients suffer a recurrence within 30 days following treatment with metronidazole or vancomycin, highlighting the need for an antibiotic that can offer an improved sustained clinical cure rate
• Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic include those who:
o Are immunocompromisedo Are receiving concomitant antibioticso Are renally impairedo Are aged 65 years or over
• Oral and IV metronidazole or oral vancomycin have been the mainstays of CDI treatment to date, with vancomycin being recommended in more severe cases
• DIFICLIR is an oral macrocyclic antibacterial indicated for the treatment of CDI, with targeted activity that kills C. difficile and inhibits spore and toxin production
• DIFICLIR causes minimal disruption to the normal colonic microflora and it may preserve colonisation resistance and thereby could restrict opportunities for C. difficile overgrowth
• DIFICLIR has proven efficacy with a clinical cure rate comparable to that of vancomycin
• DIFICLIR is superior to vancomycin in reducing the rate of CDI recurrence
• DIFICLIR is superior to vancomycin in terms of sustained clinical cure rate due to its high rate of clinical cure and low rate of recurrence
• In a subpopulation analysis of patients who received concomitant systemic antibacterials, significantly greater rates of clinical cure were observed in DIFICLIR- versus vancomycin-treated patients (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
o Rates of recurrence were significantly lower among DIFICLIR-treated versus vancomycin-treated patients
o Rates of sustained clinical cure were also significantly better among DIFICLIR-treated versus vancomycin-treated patients
• The safety profile of DIFICLIR is comparable to that of oral vancomycin
• DIFICLIR has low levels of systemic absorption, providing:o A low risk of systemic toxicityo Action at the site of infection
• DIFICLIR is available as a convenient twice-daily tablet.

15
1.5. References1. Crobach MJ, Dekkers OM, Wilcox MH, et al. European
Society of Clinical Microbiology and Infectious Diseases (ESCMID): data review and recommendations for diagnosing Clostridium difficile-infection (CDI). Clin Microbiol Infect 2009;15:1053–66.
2. Bauer MP, Notermans DW, van Benthem BH, et al. Clostridium difficile infection in Europe: a hospital-based survey. Lancet 2011;377:63–73.
3. Lyytikäinen O, Turunen H, Sund R, et al. Hospitalizations and deaths associated with Clostridium difficile infection, Finland, 1996–2004. Emerg Infect Dis 2009;15:761–5.
4. Søes L, Mølbak K, Strøbaek S, et al. The emergence of Clostridium difficile PCR ribotype 027 in Denmark – a possible link with the increased consumption of fluoroquinolones and cephalosporins? Euro Surveill 2009;14:pii-19176.
5. Soler P, Nogareda F, Cano R. Rates of Clostridium difficile infection in patients discharged from Spanish hospitals, 1997–2005. Infect Control Hosp Epidemiol 2008;29:887–9.
6. Vonberg RP, Schwab F, Gastmeier P. Clostridium difficile in discharged inpatients, Germany. Emerg Infect Dis 2007;13:179–80.
7. Mylonakis E, Ryan ET, Calderwood SB. Clostridium difficile-associated diarrhea. Arch Intern Med 2001;161:525–33.
8. Rubin MS, Bodenstein LE, Kent KC. Severe Clostridium difficile colitis. Dis Colon Rectum 1995;38:350–4.
9. Triadafilopoulos G, Hallstone AE. Acute abdomen as the first presentation of pseudomembranous colitis. Gastroenterology 1991;101:685–91.
10. Bouza E, Dryden M, Mohammed R, et al. Results of a phase III trial comparing tolevamer, vancomycin and metronidazole in patients with Clostridium difficile-associated diarrhoea. Clin Microbiol Infect 2008;14 (Suppl 7):S103–4.
11. Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
12. Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med 2010;362:197–205.
13. Hurley BW, Nguyen CC. The spectrum of pseudomembranous enterocolitis and antibiotic-associated diarrhea. Arch Intern Med 2002;162:2177–84.
14. Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ 2004;171:51–8.
15. McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol 2002;97:1769–75.
16. Cohen MB. Clostridium difficile infections: emerging epidemiology and new treatments J Ped Gastroenterol Nutr 2009;48:63–5.
17. Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect 1998;40:1–15.
18. Hu MY, Katchar K, Kyne L, et al. Prospective derivation and validation of a clinical prediction rule for recurrent Clostridium difficile infection. Gastroenterology 2009;136: 1206–14.
19. Kyne L, Warny M, Qamar A, et al. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet 2001;357:189–93.
20. Pépin J, Alary M-E, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis 2005;40:1591–7.
21. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis 1998;26:954–9.
22. Bauer MP, Miller M, Gerding DN, et al. Renal failure, fever, and leukocytosis all predict treatment failure in Clostridium difficile infection (CDI), but renal failure is the only predictor of recurrent CDI. Clin Microbiol Infect 2011;17(Suppl 4):A1–4.
23. Pépin J, Valiquette L, Alary M-E, et al. Clostridium difficile-associated diarrhea in a region of Quebec from 1991 to 2003: a changing pattern of disease severity. CMAJ 2004;171:466–72.
24. Dubberke ER, Wertheimer AI. Review of current literature on the economic burden of Clostridium difficile infection. Infect Control Hosp Epidemiol 2009;30:57–66.
25. Vonberg RP, Reichardt C, Behnke M, et al. Costs of nosocomial Clostridium difficile-associated diarrhoea. J Hosp Infect 2008;70:15–20.
26. Wilcox MH, Cunniffe JG, Trundle C, et al. Financial burden of hospital-acquired Clostridium difficile infection. J Hosp Infect 1996;34:23–30.
27. Kuijper EJ, Coignard B, Tüll P, et al. Emergence of Clostridium difficile–associated disease in North America and Europe. Clin Microbiol Infect 2006;12(Suppl 6):2–18.
28. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clin Microbiol Infect 2009;15:1067–79.
29. Zar FA, Bakkanagari SR, Moorthi SR, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium-associated diarrhea, stratified by disease severity. Clin Infect Dis 2007;45:302–7.
30. Bjørneklett A, Midtvedt T. Influence of three antimicrobial agents – penicillin, metronidazole, and doxycycline – on the intestinal microflora of healthy humans. Scand J Gastroenterol 1981;16:473–80.
31. Edlund C, Barkolt L, Liljequist BO, et al. Effect of vancomycin on intestinal flora of patients who previously received antimicrobial therapy. Clin Infect Dis 1997;25:729–32.
32. Löfmark S, Edlund C, Nord CE. Metronidazole is still the drug of choice for treatment of anaerobic infections. Clin Infect Dis 2010;50 (Suppl 1):S16–23.
33. DuPont HL. The search for effective treatment of Clostridium difficile infection. N Engl J Med 2011;364:473–5.
34. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
35. Credito KL, Appelbaum PC. Activity of OPT-80, a novel macrocycle, compared with those of eight other agents against selected anaerobic species. Antimicrob Agents Chemother 2004;48:4430–4.
36. Finegold SM, Molitoris D, Vaisanen ML, et al. In vitro activities of OPT-80 and comparator drugs against intestinal bacteria. Antimicrob Agents Chemother 2004;48:4898–902.
16
37. Louie TJ, Emery J, Krulicki W, et al. OPT-80 eliminates Clostridium difficile and is sparing of Bacteroides species during treatment of C. difficile infection. Antimicrob Agents Chemother 2009;53:261–3.
38. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety, and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
39. Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;doi:10.1016/S1473-3099(11)70374-7.
40. Shue YK, Sears PS, Shangle S, et al. Safety, tolerance, and pharmacokinetic studies of OPT-80 in healthy volunteers following single and multiple oral doses. Antimicrob Agents Chemother 2008;52:1391–5.
41. Barbut F, Corthier G, Charpak Y, et al. Prevalence and pathogenicity of Clostridium difficile in hospitalized patients. A French multicenter study. Arch Intern Med 1996;156:1449–54.
42. Sanchez TH, Brooks JT, Sullivan PS, et al. Bacterial diarrhea in persons with HIV infection, United States, 1992–2002. Clin Infect Dis 2005;41:1621–7.
43. Bilgrami S, Feingold JM, Dorsky D, et al. Incidence and outcome of Clostridium difficile infection following autologous peripheral blood stem cell transplantation. Bone Marrow Transplant 1999;23:1039–42.
44. Cohen SH, Gerding DN, Johnson S et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidem 2010;31:431–55.
45. Aseeri M, Schroeder T, Kramer J, et al. Gastric acid suppression by proton pump inhibitors as a risk factor for Clostridium difficile-associated diarrhea in hospitalized patients. Am J Gastroenterol 2008;103:2308–13.
46. Health Protection Agency. Investigation into outbreaks of Clostridium difficile at Maidstone and Tunbridge Wells NHS Trust. Commission for Healthcare Audit and Inspection, 2007.
47. Kuijper EJ, Barbut F, Brazier JS, et al. Update of Clostridium difficile infection due to PCR ribotype 027 in Europe, 2008. Euro Surveill 2008;13ii:18942.
48. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multiinstitutional outbreak of Clostridium difficile–associated diarrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–9.
49. Yoon SS, Brandt L. Treatment of refractory/recurrent C. difficile-associated disease by donated stool transplanted via colonoscopy: a case series of 12 patients. J Clin Gastroenterol 2010;44:562–6.
50. Aslam S, Hamill RJ, Musher DM. Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 2005;5:549–57.
51. Al-Nassir WN, Sethi AK, Li Y, et al. Both oral metronidazole and oral vancomycin promote persistent overgrowth of vancomycin-resistant enterococci during treatment of Clostridium difficile-associated disease. Antimicrob Agents Chemother 2008;52:2403–6.
52. Olivier CN, Blake RK, Steed LL, et al. Risk of vancomycin-resistant enterococcus (VRE) bloodstream infection among patients colonized with VRE. Infect Control Hosp Epidemiol 2008;29:404–9.
53. Sullivan KM, Spooner LM. Fidaxomicin: a macrocyclic antibiotic for the management of Clostridium difficile infection. Ann Pharmacother 2010;44:352–9.
54. Bouillaut L, Babakhani F, Sonenshein A. Inhibition of Clostridium difficile toxin synthesis and sporulation by fidaxomicin. Presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy; 18–21 September 2011, Chicago, IL, USA.
55. Gomez A, Sears P, Nguyen L, et al. Fidaxomicin inhibits spore production in C. difficile 027/NAP1/BI. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-632.
56. Sims C, Gomez A, Sears P, et al. Fidaxomicin inhibits production of toxin A and toxin B in C. difficile. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-634.
57. Babakhani F, Gomez A, Robert N, et al. Postantibiotic effect of fidaxomicin and its major metabolite, OP-1118, against Clostridium difficile. Antimicrob Agents Chemother 2011;55:4427–9.
58. Swanson RN, Hardy DJ, Shipkowitz NL, et al. In vitro and in vivo evaluation of tiacumicins B and C against Clostridium difficile. Antimicrob Agents Chemother 1991;35:1108–11.
59. Cornely OA, Miller M, Louie T, et al. Randomized controlled trial (RCT) of fidaxomicin (FDX) versus vancomycin (VAN) in treatment of recurrent Clostridium difficile infection (CDI). Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 12–15 September 2010; Boston, MA, USA. Abstract L1-1305.
60. Mullane KM, Miller MA, Weiss K, et al. Efficacy of fidaxomicin versus vancomycin as therapy for Clostridium difficile infection in patients taking concomitant antibiotics for other concurrent infections. Clin Infect Dis 2011;53:440–7.
17
Chapter 2: Microbiology, epidemiology and management of CDI
2.1. Clostridium difficile2.1.1. History and classificationC. difficile is a Gram-positive, spore-forming, anaerobic bacillus that was first identified in 1935 following isolation from the faecal microflora of healthy neonates and babies.1 C. difficile is rarely found in the healthy adult gut.2 Although C. difficile is now known to produce several potent toxins, its pathogenic potential was not recognised until 1978, when it was identified as being the causative agent of antibiotic-associated pseudomembranous colitis.3,4
Today, it is the leading cause of nosocomial diarrhoea in industrialised countries,5 and the incidence of C. difficile infection (CDI) is increasing in Europe.6–9
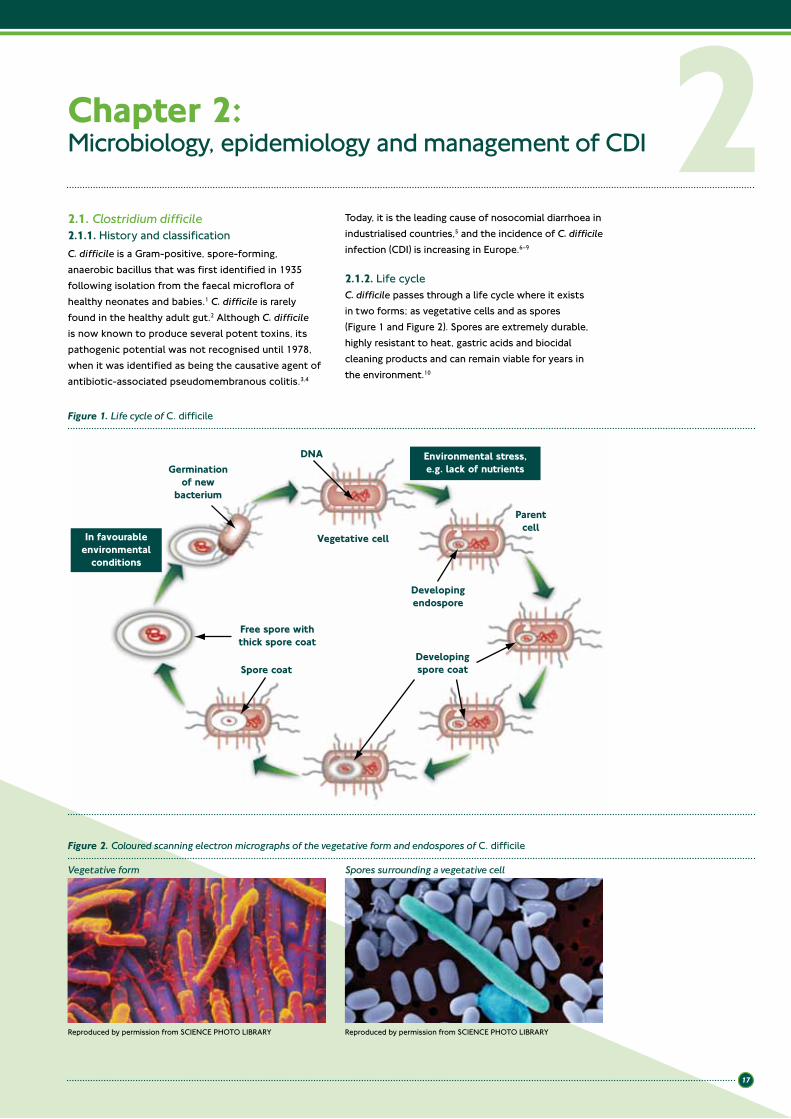
2.1.2. Life cycleC. difficile passes through a life cycle where it exists in two forms; as vegetative cells and as spores (Figure 1 and Figure 2). Spores are extremely durable, highly resistant to heat, gastric acids and biocidal cleaning products and can remain viable for years in the environment.10
2Figure 1. Life cycle of C. difficile
Figure 2. Coloured scanning electron micrographs of the vegetative form and endospores of C. difficile
Vegetative form Spores surrounding a vegetative cell
Reproduced by permission from SCIENCE PHOTO LIBRARY Reproduced by permission from SCIENCE PHOTO LIBRARY
DNA
Vegetative cell
Germinationof new
bacterium
Developingendospore
Free spore withthick spore coat
Developingspore coat
Parentcell
Spore coat
In favourableenvironmental
conditions
Environmental stress,e.g. lack of nutrients
18
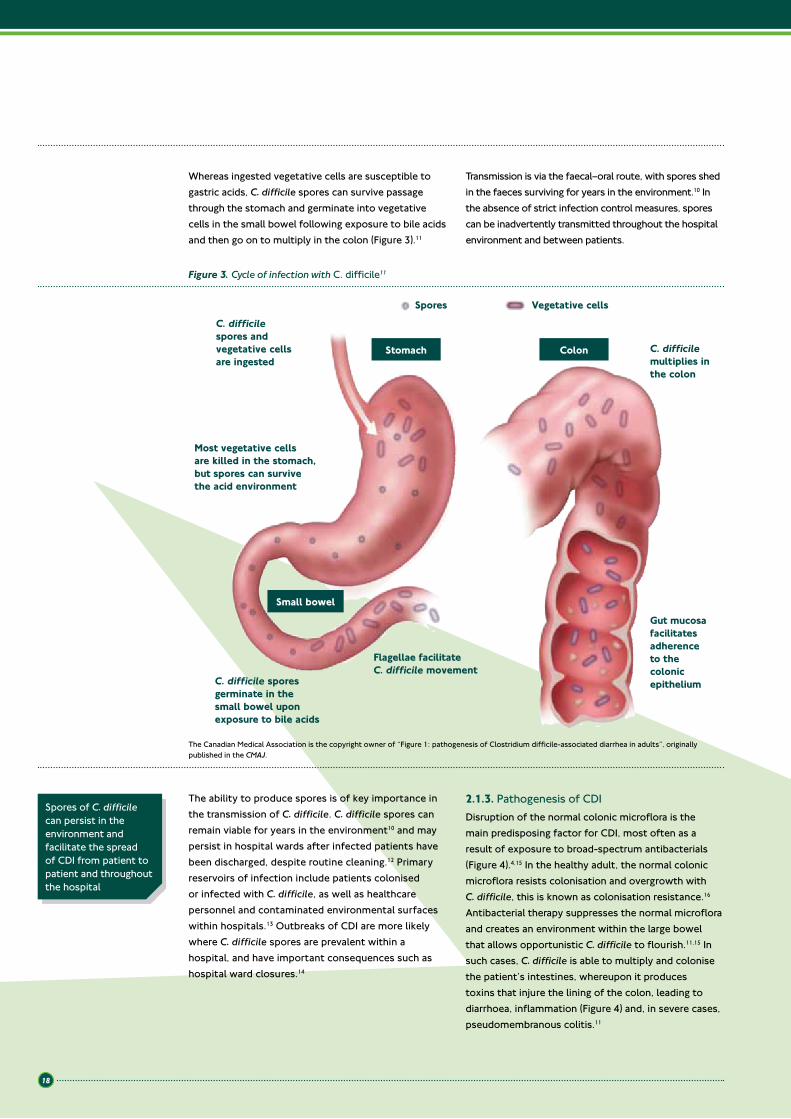
Whereas ingested vegetative cells are susceptible to gastric acids, C. difficile spores can survive passage through the stomach and germinate into vegetative cells in the small bowel following exposure to bile acids and then go on to multiply in the colon (Figure 3).11
Transmission is via the faecal–oral route, with spores shed in the faeces surviving for years in the environment.10 In the absence of strict infection control measures, spores can be inadvertently transmitted throughout the hospital environment and between patients.
The ability to produce spores is of key importance in the transmission of C. difficile. C. difficile spores can remain viable for years in the environment10 and may persist in hospital wards after infected patients have been discharged, despite routine cleaning.12 Primary reservoirs of infection include patients colonised or infected with C. difficile, as well as healthcare personnel and contaminated environmental surfaces within hospitals.13 Outbreaks of CDI are more likely where C. difficile spores are prevalent within a hospital, and have important consequences such as hospital ward closures.14
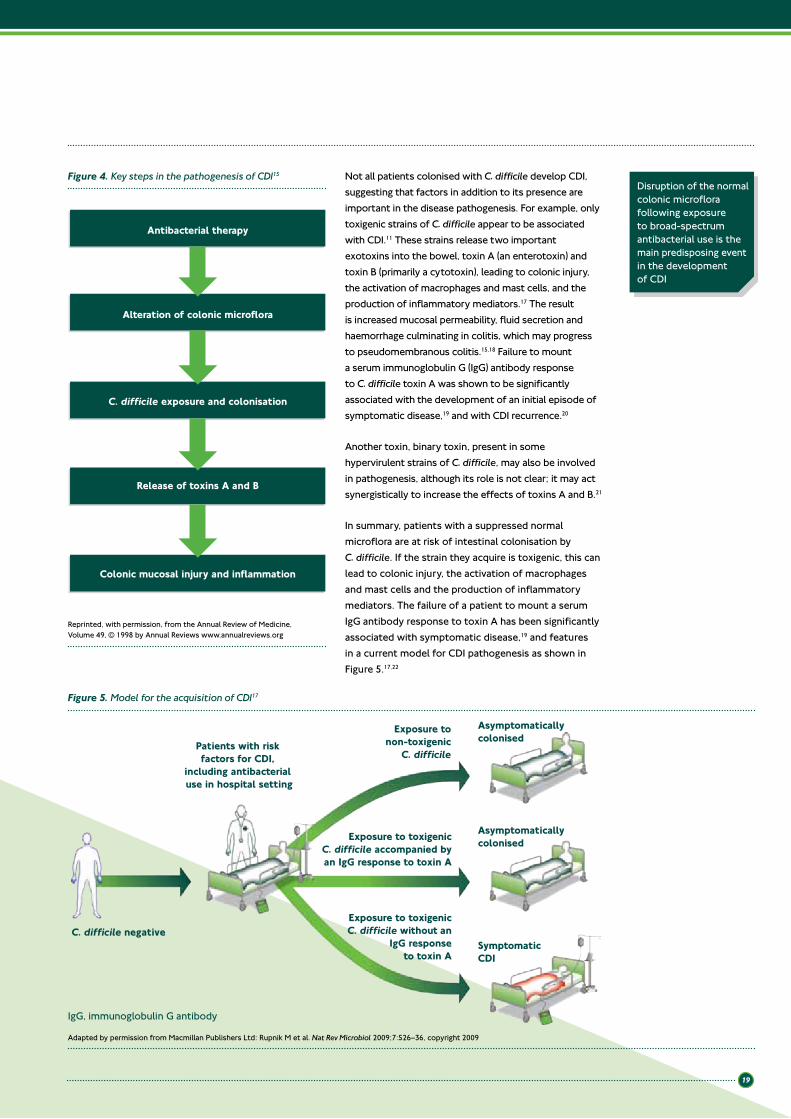
2.1.3. Pathogenesis of CDIDisruption of the normal colonic microflora is the main predisposing factor for CDI, most often as a result of exposure to broad-spectrum antibacterials (Figure 4).4,15 In the healthy adult, the normal colonic microflora resists colonisation and overgrowth with C. difficile, this is known as colonisation resistance.16 Antibacterial therapy suppresses the normal microflora and creates an environment within the large bowel that allows opportunistic C. difficile to flourish.11,15 In such cases, C. difficile is able to multiply and colonise the patient’s intestines, whereupon it produces toxins that injure the lining of the colon, leading to diarrhoea, inflammation (Figure 4) and, in severe cases, pseudomembranous colitis.11
Spores of C. difficile can persist in the environment and facilitate the spread of CDI from patient to patient and throughout the hospital
Figure 3. Cycle of infection with C. difficile11
C. difficile spores andvegetative cellsare ingested
Spores Vegetative cells
Most vegetative cells are killed in the stomach, but spores can survive the acid environment
C. difficile spores germinate in the small bowel upon exposure to bile acids
Flagellae facilitate C. difficile movement
C. difficile multiplies in the colon
Gut mucosa facilitates adherence to the colonic epithelium
Stomach Colon
Small bowel
The Canadian Medical Association is the copyright owner of “Figure 1: pathogenesis of Clostridium difficile-associated diarrhea in adults”, originally published in the CMAJ.
19
Disruption of the normal colonic microflora following exposure to broad-spectrum antibacterial use is the main predisposing event in the development of CDI
Not all patients colonised with C. difficile develop CDI, suggesting that factors in addition to its presence are important in the disease pathogenesis. For example, only toxigenic strains of C. difficile appear to be associated with CDI.11 These strains release two important exotoxins into the bowel, toxin A (an enterotoxin) and toxin B (primarily a cytotoxin), leading to colonic injury, the activation of macrophages and mast cells, and the production of inflammatory mediators.17 The result is increased mucosal permeability, fluid secretion and haemorrhage culminating in colitis, which may progress to pseudomembranous colitis.15,18 Failure to mount a serum immunoglobulin G (IgG) antibody response to C. difficile toxin A was shown to be significantly associated with the development of an initial episode of symptomatic disease,19 and with CDI recurrence.20
Another toxin, binary toxin, present in some hypervirulent strains of C. difficile, may also be involved in pathogenesis, although its role is not clear; it may act synergistically to increase the effects of toxins A and B.21
In summary, patients with a suppressed normal microflora are at risk of intestinal colonisation by C. difficile. If the strain they acquire is toxigenic, this can lead to colonic injury, the activation of macrophages and mast cells and the production of inflammatory mediators. The failure of a patient to mount a serum IgG antibody response to toxin A has been significantly associated with symptomatic disease,19 and features in a current model for CDI pathogenesis as shown in Figure 5.17,22
Figure 4. Key steps in the pathogenesis of CDI15
Antibacterial therapy
Alteration of colonic microflora
C. difficile exposure and colonisation
Release of toxins A and B
Colonic mucosal injury and inflammation
Figure 5. Model for the acquisition of CDI17
Patients with risk factors for CDI,
including antibacterial use in hospital setting
C. difficile negative
Asymptomaticallycolonised
Exposure tonon-toxigenic
C. difficile
Exposure to toxigenicC. difficile accompanied byan IgG response to toxin A
Exposure to toxigenicC. difficile without an
IgG responseto toxin A
Asymptomaticallycolonised
SymptomaticCDI
Adapted by permission from Macmillan Publishers Ltd: Rupnik M et al. Nat Rev Microbiol 2009;7:526–36, copyright 2009
Reprinted, with permission, from the Annual Review of Medicine, Volume 49, © 1998 by Annual Reviews www.annualreviews.org
IgG, immunoglobulin G antibody
20
2.1.4. Clinical presentation of infection with C. difficile2.1.4.1. Clinical presentation of CDI
The clinical presentation arising from colonisation and infection with C. difficile ranges from asymptomatic carriage to CDI, which itself varies in severity from mild-to-moderate watery diarrhoea with a distinctive odour to potentially life-threatening disease (Table 2).23,24
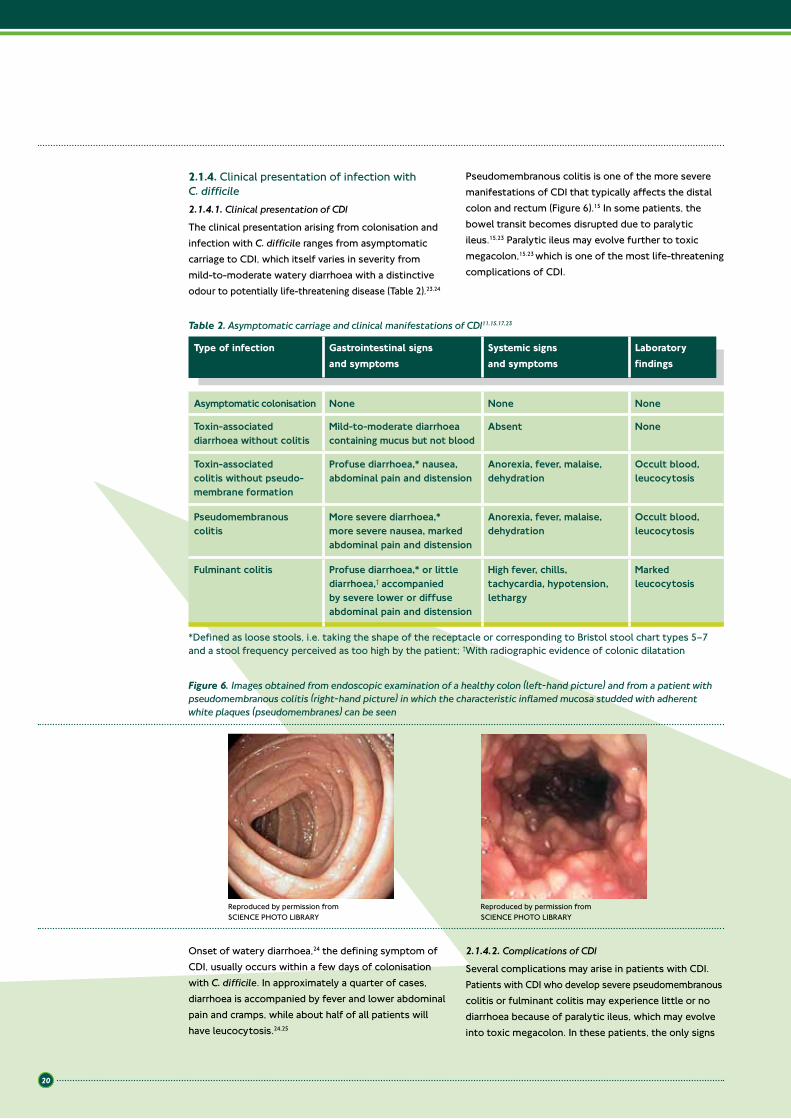
Pseudomembranous colitis is one of the more severe manifestations of CDI that typically affects the distal colon and rectum (Figure 6).15 In some patients, the bowel transit becomes disrupted due to paralytic ileus.15,23 Paralytic ileus may evolve further to toxic megacolon,15,23 which is one of the most life-threatening complications of CDI.
Onset of watery diarrhoea,24 the defining symptom of CDI, usually occurs within a few days of colonisation with C. difficile. In approximately a quarter of cases, diarrhoea is accompanied by fever and lower abdominal pain and cramps, while about half of all patients will have leucocytosis.24,25
2.1.4.2. Complications of CDI
Several complications may arise in patients with CDI.Patients with CDI who develop severe pseudomembranous colitis or fulminant colitis may experience little or no diarrhoea because of paralytic ileus, which may evolve into toxic megacolon. In these patients, the only signs
Table 2. Asymptomatic carriage and clinical manifestations of CDI11,15,17,23
Type of infection Gastrointestinal signs and symptoms
Systemic signs and symptoms
Laboratory findings
Asymptomatic colonisation None None None
Toxin-associated diarrhoea without colitis
Mild-to-moderate diarrhoea containing mucus but not blood
Absent None
Toxin-associated colitis without pseudo-membrane formation
Profuse diarrhoea,* nausea, abdominal pain and distension
Anorexia, fever, malaise, dehydration
Occult blood, leucocytosis
Pseudomembranous colitis
More severe diarrhoea,* more severe nausea, marked abdominal pain and distension
Anorexia, fever, malaise, dehydration
Occult blood, leucocytosis
Fulminant colitis Profuse diarrhoea,* or little diarrhoea,† accompanied by severe lower or diffuse abdominal pain and distension
High fever, chills, tachycardia, hypotension, lethargy
Marked leucocytosis
*Defined as loose stools, i.e. taking the shape of the receptacle or corresponding to Bristol stool chart types 5–7 and a stool frequency perceived as too high by the patient; †With radiographic evidence of colonic dilatation
Figure 6. Images obtained from endoscopic examination of a healthy colon (left-hand picture) and from a patient with pseudomembranous colitis (right-hand picture) in which the characteristic inflamed mucosa studded with adherent white plaques (pseudomembranes) can be seen
Reproduced by permission from SCIENCE PHOTO LIBRARY
Reproduced by permission from SCIENCE PHOTO LIBRARY

21
of disease may be abdominal distension, marked leucocytosis and a dilated and inflamed colon on abdominal X-ray or computed tomography scan.26 In one small study of 13 patients with severe CDI, complicated by systemic toxic effects and peritonitis requiring surgical intervention, mortality was observed to approach 40%.27 Rarely, the presence of colitis may allow bacteraemia to develop.28
2.1.5. Morbidity, mortality and burden of CDI2.1.5.1. Morbidity and mortality
CDI can lead to significant morbidity and mortality. Patients with CDI may suffer significant pain and discomfort as a result of CDI. The patients most at risk of CDI or recurrent CDI tend to be more vulnerable individuals, including those who are immunocompromised,29 on certain concomitant antibiotics,20,30–33 who are renally impaired,34,35 or patients who are aged 65 years or over.20,30,31,33
Recurrence is common (up to 25%) following treatment with metronidazole and vancomycin16,36,37 and recurrent cycles of CDI may result in a spiral of clinical decline which, in some cases, may even culminate in death.
Mortality rates of 2–7% have been reported in CDI patients in several studies.30,38 One such study was a recent pan-European hospital-based survey conducted over 1 month, in a population of patients mostly fitting the known risk profile for colonisation with C. difficile; almost two-thirds were aged ≥65 years, approximately two-fifths had a severe comorbidity and almost all had received prior antibacterial therapy in the 3 months before their infection.30 Among the entire cohort, the incidence of CDI was 4.1 cases per 10,000 patient days (range 0–36.3). Approximately 2% of patients died as a result of their infection, and CDI was considered contributory to mortality in a further 7% of cases.30 After a 3-month follow-up period, 22% of patients who had been diagnosed with CDI in the study had died, and infection with C. difficile was implicated in 40% of all deaths. All seven patients for whom CDI was attributed to be the main cause of death were aged ≥75 years.30 In a case control study of 1,703 patients with CDI in Canada, approximately 7% of patients died as a result of CDI, and their infection was considered contributory to mortality in a further 8% of cases.38
Older age is a major risk factor for the acquisition of C. difficile and development of CDI, and this is reflected in age-related incidence data and attributable mortality (Table 3).38
Mortality rates of 2–7% have been reported in CDI patients in several studies
The cost of CDI within the EU is estimated at €3,000 million per year and is expected to increase in line with the growing proportion of people aged over 65 years
Table 3. Age-specific incidence of CDI and attributable mortality38
Age, years CDI rate per 1,000 admissions, (%)
Attributable 30-day mortality rate, (%)
<40 3.5 2.6
41–50 11.2 1.2
51–60 20.0 3.2
61–70 24.4 5.1
71–80 38.3 6.2
81–90 54.5 10.2
>90 74.4 14.0
2.1.5.2. Burden of CDI
As well as causing significant morbidity and mortality, CDI imposes a significant economic burden on healthcare systems across Europe. Patients who develop CDI require isolation and therapy for their underlying disease as well as their CDI. Additional costs can accrue from the need for rigorous hygiene in patient care, environmental decontamination and, when outbreaks occur, potential cohort isolation and ward closure.
Patients with CDI spend on average an extra 7–21 days in hospital, compared with non-infected controls, which is a contributor to increased costs for healthcare systems.39–41
The potential cost of CDI within the European Union (EU) is estimated to be €3,000 million per year, and this is expected to rise over the next four decades42 as the proportion of people aged over 65 years in the population grows. By 2050, estimates suggest that
Reproduced by permission from Massachusetts Medical Society (“MMS”): New England Journal of Medicine, Loo VG, Poirier L, Miller MA, et al;353:2442–9. Copyright 2005

22
134.5 million Europeans will be aged over 65 years, which is one of the populations at greatest risk of developing CDI.42
In a recent study, the median cost to treat CDI was €33,840 per patient.40 The difference in the cost per patient showed that the cost for CDI patients was significantly more than for their non-infected matched controls (median €7,147; 95% confidence interval: €4,067–9,276).40
2.1.6. Risk factors for development of CDIC. difficile is primarily a nosocomial pathogen and, although cases of community-acquired CDI are increasing,43 these are currently less common than hospital-acquired infections.30
Exposure to antibacterial therapy, most notably broad-spectrum agents, is the main risk factor for the development of CDI.44 Most classes of antibacterial agents are associated with CDI to a greater or lesser extent, with the highest risk associated with clindamycin, certain fluoroquinolones and third-generation cephalosporins (Table 4).26,44
While exposure to antibacterial therapy is the main event predisposing to colonisation with C. difficile, the duration of this therapy and the use of multiple antibacterial agents are compounding factors.30,31,44,45 In addition, patients who are immunocompromised, such as those receiving immunosuppressive drugs or who are infected with human immunodeficiency virus (HIV),45,46 are also predisposed to C. difficile colonisation and subsequent development of CDI.31 The presence of severe underlying disease is also a risk factor. A more extensive list of patients at risk of an initial episode of CDI is given in Table 5.
Rates of infection are also increasing in populations previously considered at low risk.47 Such patients include pregnant women, who can develop CDI just before delivery,47,48 or new mothers in the first months after delivery.48 CDI arising in these patients may necessitate hospitalisation and, in some cases, colectomy, as shown in a study conducted in the USA.48
• Immunocompromised patientso Immunosuppressive drugs45,46
o HIV infection46
• Antibacterial therapy30,31,44,45
o Treatment during the previous 3 monthso Multiple antibacterial agents
• Older age (≥65 years)30,31
• Severe underlying illness30,31
• Tube-feeding and gastrointestinal surgery31,49,50
• Gastrointestinal medications, including gastric acid reduction therapy, e.g. antacids; histamine H2 blockers; proton pump inhibitors31
• ICU stay31
• Prolonged hospitalisation (median periods of 20 days)*51
• Antineoplastic agents45,46
Table 5. Risk factors associated with the development of nosocomial CDI30,31,44–46,49–51
Risk factors
*Versus 16 days for matched controls without CDI HIV, human immunodeficiency virus; ICU, intensive care unit
CDI is associated with antibacterial use, especially broad-spectrum fluoroquinolones and cephalosporins
Table 4. Antibacterials and risk of colonisation with C. difficile26,44
Risk for colonisation with C. difficile Antibacterials
High Clindamycin; second- and third-generation cephalosporins; fluoroquinolones*
Medium Macrolides; amoxicillin/ampicillin; amoxicillin/clavulanic acid
Low Aminoglycosides; vancomycin; trimethoprim; tetracyclines; benzylpenicillin; piperacillin/tazobactam
Reproduced by permission from the British Medical Journal (“BMJ”): Monaghan et al. Gut; 2008;57:850–860. Copyright 2008
*Data taken during a 027 ribotype CDI outbreak

23
2.1.7. Recurrence of CDI2.1.7.1. Recurrence
Recurrence of CDI has been identified by ESCMID as being the most important problem in the treatment of CDI.23 In their treatment guidelines, ESCMID defines recurrent CDI as being an increase in stool frequency for two consecutive days, looser stools or the development of new signs of severe colitis following an initial response to treatment. There will also be microbiological evidence of toxin-producing C. difficile in stools.23 In one study, CDI was considered recurrent if it arose within 8 weeks of a previous episode;30 however, there is no wider consensus on such a time frame. CDI recurrence and reinfection are common, occurring in up to 25% of cases within 30 days following treatment,16,36,37 highlighting the need for an antibacterial agent that can offer a sustained clinical cure.
The reasons for recurrence are not well understood. However, recurrence appears to be related to a combination of a failure to re-establish the colonic microflora, the presence in the intestines of spores of C. difficile, and a sub-optimal host immune response to the infecting organism and its toxins.52 Reinfection can also occur when an individual is exposed to a subsequent source of C. difficile.
In some individuals, a repetitive cycle of recurrence may ensue10 resulting in protein-losing enteropathy.
Recurrent CDI has an important clinical impact and is associated with sequelae that can have serious consequences for the patient’s well-being and longevity.
2.1.7.2. Risk factors for recurrent CDI
Risk factors for recurrent infection are shown in Table 6. Patients at high risk of recurrence or those for whom the impact of recurrence would be most dramatic include patients who are immunocompromised,29 on certain concomitant antibiotics,20,30,32,33 who are renally impaired,34,35 or patients aged 65 years or over.20,30,33
Treatment guidelines currently focus on treating patients on the basis of disease severity;23 however, there is growing awareness of the importance of the need to identify and manage those at high risk of recurrent CDI or those for whom the impact of recurrence would be most dramatic.
Recurrence of CDI is a serious and difficult-to-treat problem,23 impacting on the length and overall cost of hospitalisation.40,41 Reduction of recurrence could potentially reduce the costs of treating additional episodes of CDI and may also reduce the rate of person-to-person transmission.16 The introduction of an antibacterial agent which could reduce the rate of recurrent infection could warrant a change in the way that CDI is managed.
Patients who are immunocompromised, on certain concomitant antibiotics, who are renally impaired, and who are aged 65 years or over are at risk for recurrence of CDI
Table 6. Risk factors associated with the development of recurrent CDI10,20,23,29,30,32–35
Risk factors for recurrence
• Immunocompromised patients29
• Exposure to other antibacterial agents that disrupt the normal colonic microflora20,23,30,32
• Previous episode of CDI10,20,30
• Renal impairment34,35
• Aged 65 years or over20,30,33
• Impaired immune response to C. difficile toxin A20
• Severe underlying disease20
• Prolonged hospitalisation33
• ICU stay32
ICU, intensive care unit
2.2. Epidemiology of CDI2.2.1. Epidemiology of CDI in EuropeIn the last decade, rising rates of CDI, more severe and fulminant CDI and more recurrent CDIs have been observed in Europe,6–9 the USA30,53 and Canada.30,54,55 However, gaining an accurate picture of the prevalence of CDI throughout Europe is difficult because of marked variations in reporting.56 In a recent pan-European hospital-based survey the incidence of C. difficile infection varied across hospitals with an overall rate of 4.1 cases per 10,000 patient days (range 0–36.3).30
Reported prevalence rates across Europe often more accurately reflect the surveillance and reporting regulations in a particular country than the true prevalence of the disease itself. In some countries, such as the UK, Belgium, France and Germany, reporting of CDI is now mandatory, while a voluntary surveillance scheme has been in operation since 2009 in The Netherlands.
In other countries where there is no mandatory reporting, the prevalence of CDI, and its true burden, may be underestimated. An increase in testing and

24
While attention has focused predominantly on ribotype 027, this hypervirulent strain is relatively less prevalent in Europe compared with other ribotypes (Figure 7).30 In a pan-European hospital-based survey conducted in November 2008, the overall prevalence of ribotype 027 was approximately 5%; whereas it accounted for 25% of all strains isolated in the UK.30
This same survey also showed that ribotype 014/020 (ribotypes 014 and 020 were considered nearly identical and reported together) was the most predominantly isolated strain in Europe.30 The third most frequently isolated strain from hospitalised patients was the hypervirulent ribotype 078, which accounted for 8% of all typeable isolates.
reporting of CDI in these countries would therefore enable its epidemiology to be more accurately assessed.
2.2.2. Changing epidemiology: increasing incidence and disease severityThe past decade has seen rising rates of CDI worldwide, together with increased morbidity and mortality from CDI. Increases in incidence have been reported in many European countries, including Finland,6 Denmark,7 Spain8 and Germany.9 However in some countries, such as the UK, the incidence has decreased over the last few years.56,57 There are several possible reasons for the decline, including improved infection control and surveillance within hospitals, such as the mandatory reporting of all cases of CDI.58
Despite C. difficile primarily being a nosocomial pathogen,30 cases of community-acquired CDI, while currently less common, are increasing.43 For example, in a recent survey of CDI conducted across Europe, 80% of cases were nosocomial, 14% were community-acquired, and the remaining 6% were indeterminate.30
Many factors have contributed to the rise in incidence of CDI, including the emergence of hypervirulent strains, such as polymerase chain reaction (PCR) ribotype 027 (Table 7).59 In Europe ribotype 027 first appeared in the UK in 2003 and subsequently in The Netherlands in 2005.44 Multiple outbreaks and sporadic cases have since occurred in a number of European countries.30
Table 7. Factors associated with increased incidence of CDI in hospitalised patients14,42,55,60
Contributory factors
• Increasing numbers of patients who are aged ≥65 years,14,42 immunocompromised42,55 or who have other comorbidities14
• Use of high-risk antibacterials55
• Overburdened healthcare workers and reduced compliance with hand hygiene14
• Cost constraints leading to inadequate environmental disinfection14
• Rapid turnover in hospital beds55
• Overcrowding in hospitals14
• Prolonged periods of hospitalisation14
• Shared toilet facilities between patients55
• Inadequate isolation facilities for infected patients14,55
• Emergence of epidemic strains60
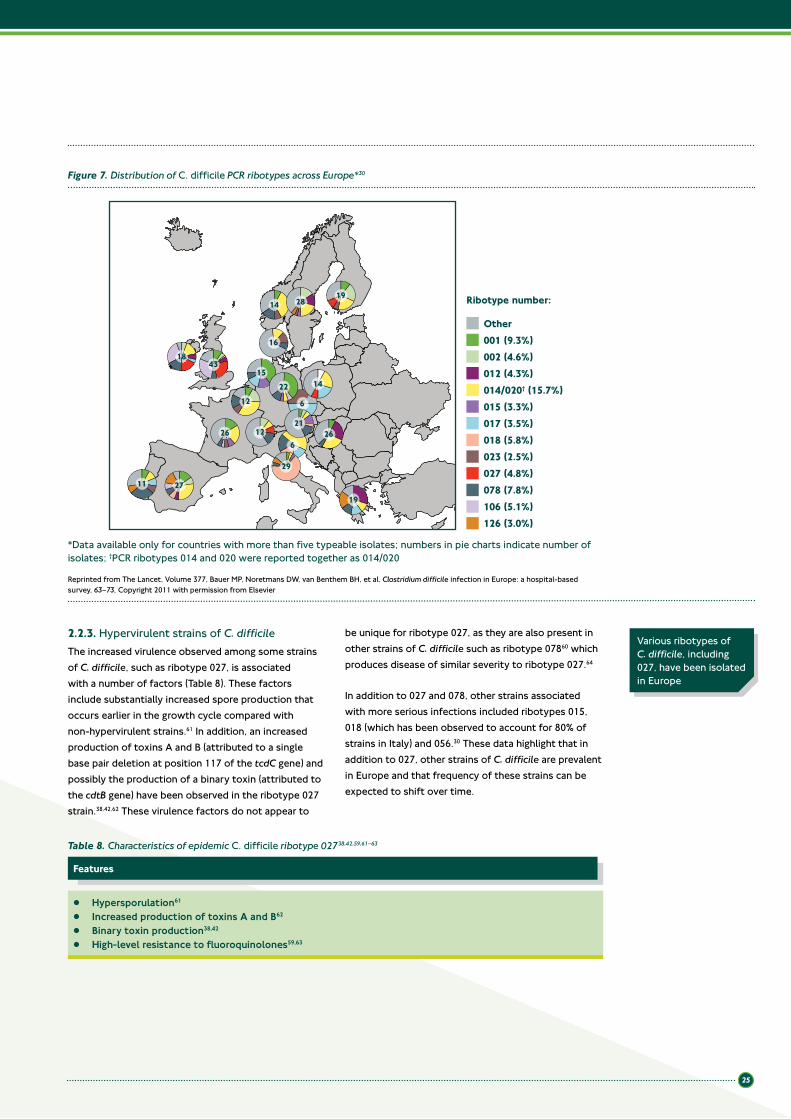
25
Figure 7. Distribution of C. difficile PCR ribotypes across Europe*30
Ribotype number:
Other001 (9.3%)002 (4.6%)012 (4.3%)014/020† (15.7%)015 (3.3%)017 (3.5%)018 (5.8%)023 (2.5%)027 (4.8%)078 (7.8%)106 (5.1%)126 (3.0%)
1843
11 27
266
12
16
14 2819
12 6
19
26
14
21
29
1522
*Data available only for countries with more than five typeable isolates; numbers in pie charts indicate number of isolates; †PCR ribotypes 014 and 020 were reported together as 014/020
Reprinted from The Lancet, Volume 377, Bauer MP, Noretmans DW, van Benthem BH, et al. Clostridium difficile infection in Europe: a hospital-based survey, 63–73, Copyright 2011 with permission from Elsevier
2.2.3. Hypervirulent strains of C. difficileThe increased virulence observed among some strains of C. difficile, such as ribotype 027, is associated with a number of factors (Table 8). These factors include substantially increased spore production that occurs earlier in the growth cycle compared with non-hypervirulent strains.61 In addition, an increased production of toxins A and B (attributed to a single base pair deletion at position 117 of the tcdC gene) and possibly the production of a binary toxin (attributed to the cdtB gene) have been observed in the ribotype 027 strain.38,42,62 These virulence factors do not appear to
be unique for ribotype 027, as they are also present in other strains of C. difficile such as ribotype 07860 which produces disease of similar severity to ribotype 027.64
In addition to 027 and 078, other strains associated with more serious infections included ribotypes 015, 018 (which has been observed to account for 80% of strains in Italy) and 056.30 These data highlight that in addition to 027, other strains of C. difficile are prevalent in Europe and that frequency of these strains can be expected to shift over time.
Table 8. Characteristics of epidemic C. difficile ribotype 02738,42,59,61–63
Features
• Hypersporulation61
• Increased production of toxins A and B62
• Binary toxin production38,42
• High-level resistance to fluoroquinolones59,63
Various ribotypes of C. difficile, including 027, have been isolated in Europe
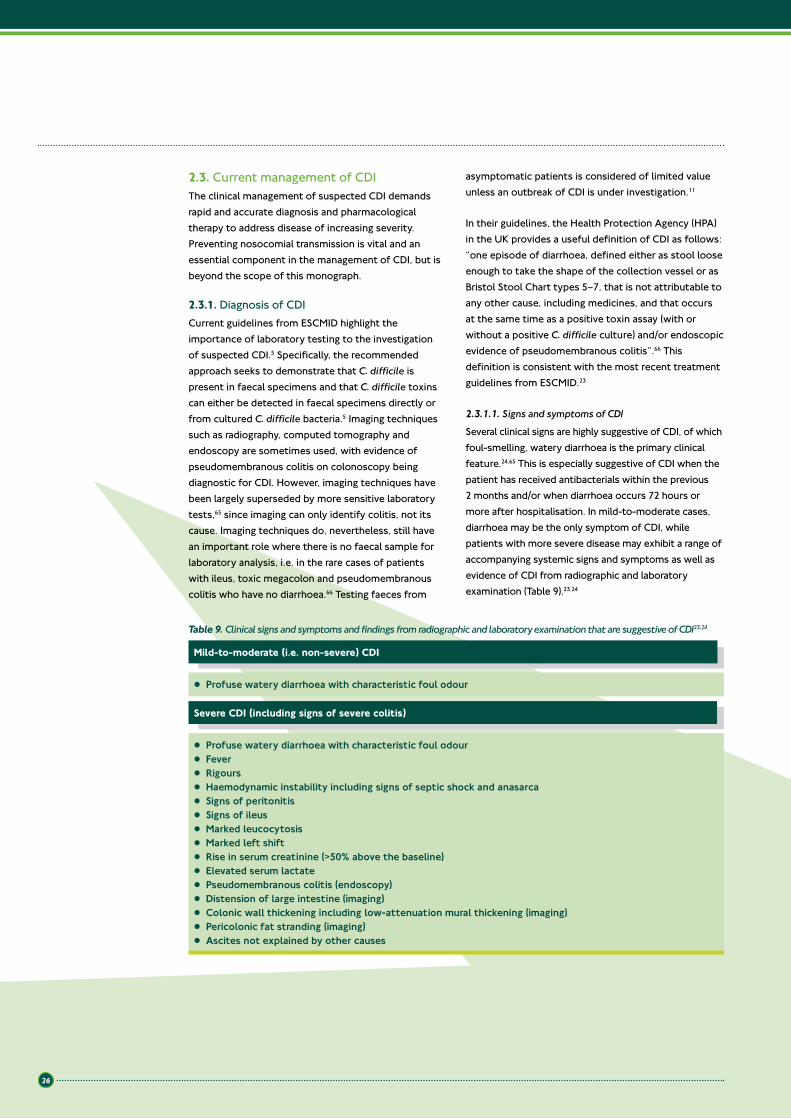
26
2.3. Current management of CDIThe clinical management of suspected CDI demands rapid and accurate diagnosis and pharmacological therapy to address disease of increasing severity. Preventing nosocomial transmission is vital and an essential component in the management of CDI, but is beyond the scope of this monograph.
2.3.1. Diagnosis of CDICurrent guidelines from ESCMID highlight the importance of laboratory testing to the investigation of suspected CDI.5 Specifically, the recommended approach seeks to demonstrate that C. difficile is present in faecal specimens and that C. difficile toxins can either be detected in faecal specimens directly or from cultured C. difficile bacteria.5 Imaging techniques such as radiography, computed tomography and endoscopy are sometimes used, with evidence of pseudomembranous colitis on colonoscopy being diagnostic for CDI. However, imaging techniques have been largely superseded by more sensitive laboratory tests,65 since imaging can only identify colitis, not its cause. Imaging techniques do, nevertheless, still have an important role where there is no faecal sample for laboratory analysis, i.e. in the rare cases of patients with ileus, toxic megacolon and pseudomembranous colitis who have no diarrhoea.66 Testing faeces from
asymptomatic patients is considered of limited value unless an outbreak of CDI is under investigation.11
In their guidelines, the Health Protection Agency (HPA) in the UK provides a useful definition of CDI as follows: “one episode of diarrhoea, defined either as stool loose enough to take the shape of the collection vessel or as Bristol Stool Chart types 5–7, that is not attributable to any other cause, including medicines, and that occurs at the same time as a positive toxin assay (with or without a positive C. difficile culture) and/or endoscopic evidence of pseudomembranous colitis”.66 This definition is consistent with the most recent treatment guidelines from ESCMID.23
2.3.1.1. Signs and symptoms of CDI
Several clinical signs are highly suggestive of CDI, of which foul-smelling, watery diarrhoea is the primary clinical feature.24,65 This is especially suggestive of CDI when the patient has received antibacterials within the previous 2 months and/or when diarrhoea occurs 72 hours or more after hospitalisation. In mild-to-moderate cases, diarrhoea may be the only symptom of CDI, while patients with more severe disease may exhibit a range of accompanying systemic signs and symptoms as well as evidence of CDI from radiographic and laboratory examination (Table 9).23,24
Table 9. Clinical signs and symptoms and findings from radiographic and laboratory examination that are suggestive of CDI23,24
Mild-to-moderate (i.e. non-severe) CDI
Severe CDI (including signs of severe colitis)
• Profuse watery diarrhoea with characteristic foul odour
• Profuse watery diarrhoea with characteristic foul odour• Fever • Rigours • Haemodynamic instability including signs of septic shock and anasarca• Signs of peritonitis• Signs of ileus• Marked leucocytosis• Marked left shift• Rise in serum creatinine (>50% above the baseline)• Elevated serum lactate• Pseudomembranous colitis (endoscopy)• Distension of large intestine (imaging)• Colonic wall thickening including low-attenuation mural thickening (imaging)• Pericolonic fat stranding (imaging)• Ascites not explained by other causes

27
2.3.1.2. Laboratory tests for CDI
A number of laboratory tests are available today to confirm a putative clinical diagnosis of CDI. However, all have limitations (Table 10).5,15
The cell-culture cytotoxic assay (CCA) and toxigenic stool culture are considered the reference standard methods for the diagnosis of CDI.5 However, while these methods are sensitive and specific for the detection of CDI, they are labour intensive and slow.74
Table 10. Advantages and disadvantages of diagnostic tests for C. difficile5,15,23,24,67–73
Diagnostic test
Turnaround time
Sensitivity Advantages Disadvantages
Endoscopy 2 hours 51%24 • Diagnostic of pseudomembranous colitis23
• Low sensitivity;24 may require laboratory investigations23
Anaerobic culture
48 hours69,70 93–100%69,70 • Direct detection68
• High sensitivity68,69
• Slow68
• Does not distinguish toxin-producing strains68
CCA ≥24 hours67,71 97–100%71 • Gold standard5
• Detects A and B strains71
• Highly specific (99%)71
• Long turnaround time67,68
• Labour intensive15
EIA-GDH (common antigen) test
7 hours*72 80–97%†5 • Easy to use15
• Detects a C. difficile-specific enzyme67
• Highly specific (89–100%)†5,67
• Does not distinguish toxin-producing strains67
EIA-toxin A 2–6 hours68,72 49–93%†5 • Easy to use15
• Highly specific (83–100%)†5
• Suboptimal sensitivity when used alone5
EIA-toxins A and B
2–6 hours68,72 75–99%†5 • Easy to use15
• Detects A and B strains5
• Highly specific (94–100%)†5
• Suboptimal sensitivity when used alone5
Real-time PCR
<1 hour73 87–100%†5 • Rapid72
• Highly specific (94–100%)†5
• Detects toxin genes, but not toxin production73
• Higher cost73
CCA, cell-culture cytotoxic assay; EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; PCR, polymerase chain reaction; *Turnaround time for two-step assay (comprising EIA-GDH first, followed by PCR); †Relative to CCA
Most laboratories today use enzyme immunoassays (EIAs) to detect C. difficile toxins.15 These assays are highly specific (high positive predictive value) and are available as easy-to-use commercial kits which can be run in a matter of hours and batch processed.5,15,72 However, they are less sensitive than CCA, so further testing (e.g. toxigenic culture) may be needed if an initial test is negative.5 Some laboratories use tests against the common C. difficile antigen, glutamate dehydrogenase (GDH). Although highly specific, which is significant, since these assays detect both toxigenic and non-toxigenic organisms, they can detect GDH from other organisms and therefore lack sensitivity.5 GDH assays have therefore been recommended as a first step to rule out C. difficile, as this technique has a high negative predictive value; however, such tests need to be followed by another test when they are positive to determine if the strain is toxigenic.5,67 Commercial real-time PCR assays represent the most recent additions to the range of diagnostic procedures for C. difficile.74 Of comparable sensitivity and specificity to CCA,5 PCR offers
similar advantages to EIA, including a rapid turnaround.75 However, real-time PCR can result in false positives as it does not discriminate between toxigenic and non-toxigenic strains (it only detects the presence of the genes), therefore a secondary confirmatory test is recommended.5,75 While the role of real-time PCR in routine clinical practice merits further examination,74 its advantages could enable this technique to replace CCA as the reference diagnostic test for C. difficile.
Current guidelines from ESCMID recommend a two-step approach for accurate microbiological diagnosis of CDI (Figure 8).5 Specifically, these tests must demonstrate that C. difficile is present in faecal specimens and that C. difficile toxins can either be detected in faecal specimens directly or from cultured C. difficile bacteria.5 This two-step approach improves diagnostic accuracy in microbiological laboratories that use diagnostic tests with a lower sensitivity and specificity than the CCA (the reference standard test).5
ESCMID recommends a two-step approach to laboratory diagnosis of CDI to improve diagnostic accuracy
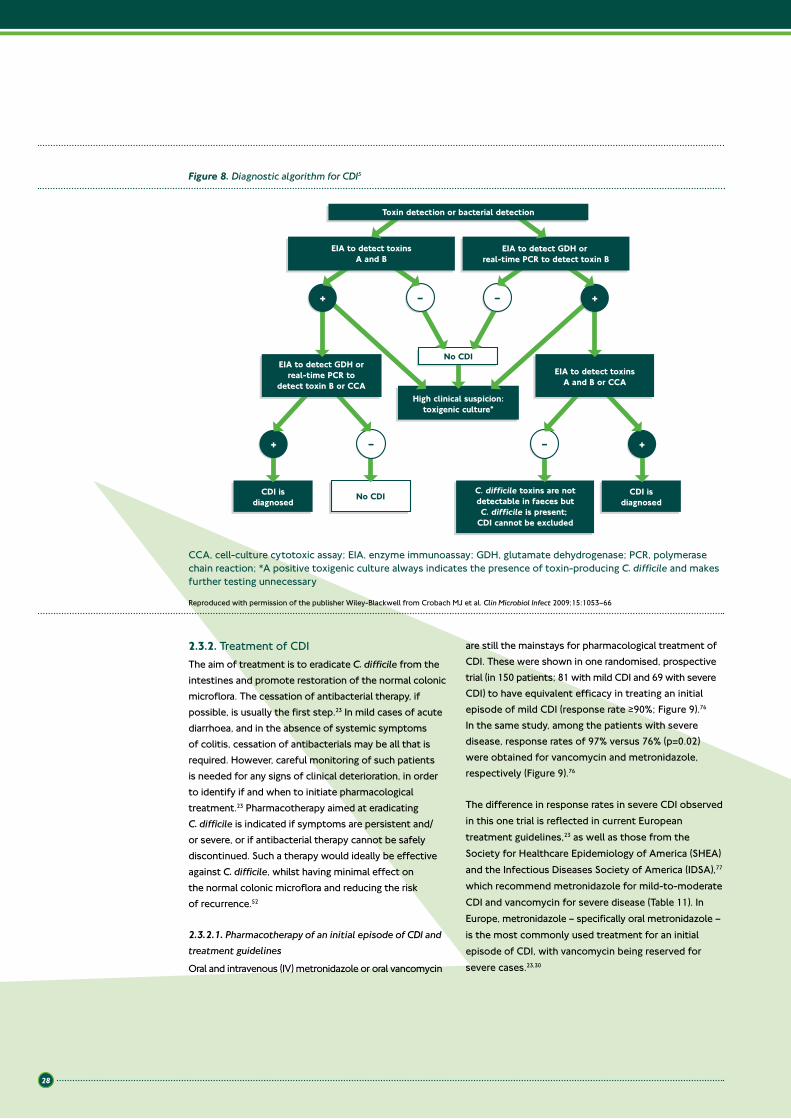
28
2.3.2. Treatment of CDIThe aim of treatment is to eradicate C. difficile from the intestines and promote restoration of the normal colonic microflora. The cessation of antibacterial therapy, if possible, is usually the first step.23 In mild cases of acute diarrhoea, and in the absence of systemic symptoms of colitis, cessation of antibacterials may be all that is required. However, careful monitoring of such patients is needed for any signs of clinical deterioration, in order to identify if and when to initiate pharmacological treatment.23 Pharmacotherapy aimed at eradicating C. difficile is indicated if symptoms are persistent and/or severe, or if antibacterial therapy cannot be safely discontinued. Such a therapy would ideally be effective against C. difficile, whilst having minimal effect on the normal colonic microflora and reducing the risk of recurrence.52
2.3.2.1. Pharmacotherapy of an initial episode of CDI and treatment guidelines
Oral and intravenous (IV) metronidazole or oral vancomycin
are still the mainstays for pharmacological treatment of CDI. These were shown in one randomised, prospective trial (in 150 patients; 81 with mild CDI and 69 with severe CDI) to have equivalent efficacy in treating an initial episode of mild CDI (response rate ≥90%; Figure 9).76 In the same study, among the patients with severe disease, response rates of 97% versus 76% (p=0.02) were obtained for vancomycin and metronidazole, respectively (Figure 9).76
The difference in response rates in severe CDI observed in this one trial is reflected in current European treatment guidelines,23 as well as those from the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA),77 which recommend metronidazole for mild-to-moderate CDI and vancomycin for severe disease (Table 11). In Europe, metronidazole – specifically oral metronidazole – is the most commonly used treatment for an initial episode of CDI, with vancomycin being reserved for severe cases.23,30
Figure 8. Diagnostic algorithm for CDI5
C. difficile toxins are notdetectable in faeces butC. difficile is present;
CDI cannot be excluded
EIA to detect toxinsA and B or CCA
EIA to detect GDH orreal-time PCR to
detect toxin B or CCA
No CDICDI isdiagnosed
CDI isdiagnosed
EIA to detect toxinsA and B
Toxin detection or bacterial detection
EIA to detect GDH or real-time PCR to detect toxin B
++ ––
++ ––
No CDI
High clinical suspicion:toxigenic culture*
CCA, cell-culture cytotoxic assay; EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; PCR, polymerase chain reaction; *A positive toxigenic culture always indicates the presence of toxin-producing C. difficile and makes further testing unnecessary
Reproduced with permission of the publisher Wiley-Blackwell from Crobach MJ et al. Clin Microbiol Infect 2009;15:1053–66

29
*Patients were stratified by mild or severe disease based on a severity assessment score developed for this study. Patients received one point each for age >60 years, temperature >38.3°C, albumin level <2.5 mg/dL, or peripheral white blood cell count >15,000 cells/mm3 within 48 hours of enrolment. Two points were given for endoscopic evidence of pseudomembranous colitis or treatment in an intensive care unit. Patients with ≥2 points were considered to have severe CDI
Figure 9. Comparative efficacy of vancomycin and metronidazole for treatment of patients stratified by CDI severity*76
Resp
onse
rate
(%)
Mild infection Severe infection
100
90
80
70
60
50
40
30
20
10
0
90%
97%98%
76%
Vancomycin Metronidazole
2.3.2.2. Pharmacotherapy of recurrent CDI and treatment guidelines
ESCMID has identified recurrence as being the most important problem in the treatment of CDI.23 After initially responding to treatment, evidence of disease recurrence is usually manifest as an increase in stool frequency for two consecutive days, looser stools or the development of new signs of colitis. There will also be microbiological evidence of toxin-producing C. difficile in stools following an initial response to treatment.23 In these cases, the guidelines recommend treating a first recurrence as a first episode unless the disease has progressed from non-severe to severe (Table 11).23
Treatment recommendations for second and later recurrences are summarised in Table 11.23
2.3.2.3. Pharmacotherapy for CDI: summary of ESCMID treatment guidelines
To summarise, the European (ESCMID) guidelines recommend that patients with an initial episode of CDI and a first recurrence are managed in the same way, with pharmacotherapy tailored to reflect disease severity (Table 11).23 For patients with second or later recurrences, these can be treated in the same way as a severe first recurrence or with the option of using tapered or pulsed dosing regimens (Table 11).
ESCMID has identified recurrence as being the most important problem in the treatment of CDI
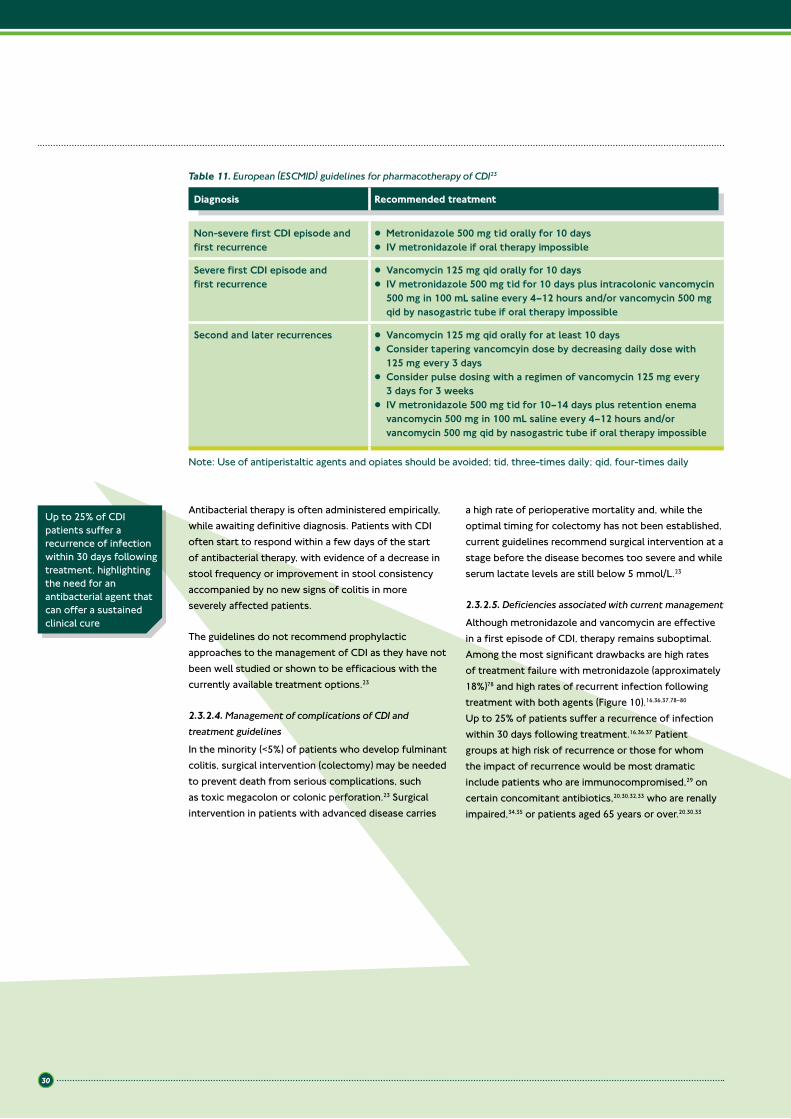
30
Antibacterial therapy is often administered empirically, while awaiting definitive diagnosis. Patients with CDI often start to respond within a few days of the start of antibacterial therapy, with evidence of a decrease in stool frequency or improvement in stool consistency accompanied by no new signs of colitis in more severely affected patients.
The guidelines do not recommend prophylactic approaches to the management of CDI as they have not been well studied or shown to be efficacious with the currently available treatment options.23
2.3.2.4. Management of complications of CDI and treatment guidelines
In the minority (<5%) of patients who develop fulminant colitis, surgical intervention (colectomy) may be needed to prevent death from serious complications, such as toxic megacolon or colonic perforation.23 Surgical intervention in patients with advanced disease carries
a high rate of perioperative mortality and, while the optimal timing for colectomy has not been established, current guidelines recommend surgical intervention at a stage before the disease becomes too severe and while serum lactate levels are still below 5 mmol/L.23
2.3.2.5. Deficiencies associated with current management
Although metronidazole and vancomycin are effective in a first episode of CDI, therapy remains suboptimal. Among the most significant drawbacks are high rates of treatment failure with metronidazole (approximately 18%)78 and high rates of recurrent infection following treatment with both agents (Figure 10).16,36,37,78–80 Up to 25% of patients suffer a recurrence of infection within 30 days following treatment.16,36,37 Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic include patients who are immunocompromised,29 on certain concomitant antibiotics,20,30,32,33 who are renally impaired,34,35 or patients aged 65 years or over.20,30,33
Up to 25% of CDI patients suffer a recurrence of infection within 30 days following treatment, highlighting the need for an antibacterial agent that can offer a sustained clinical cure
Non-severe first CDI episode and first recurrence
• Metronidazole 500 mg tid orally for 10 days• IV metronidazole if oral therapy impossible
Severe first CDI episode and first recurrence
• Vancomycin 125 mg qid orally for 10 days • IV metronidazole 500 mg tid for 10 days plus intracolonic vancomycin
500 mg in 100 mL saline every 4–12 hours and/or vancomycin 500 mg qid by nasogastric tube if oral therapy impossible
Second and later recurrences • Vancomycin 125 mg qid orally for at least 10 days• Consider tapering vancomcyin dose by decreasing daily dose with
125 mg every 3 days• Consider pulse dosing with a regimen of vancomycin 125 mg every
3 days for 3 weeks• IV metronidazole 500 mg tid for 10–14 days plus retention enema
vancomycin 500 mg in 100 mL saline every 4–12 hours and/or vancomycin 500 mg qid by nasogastric tube if oral therapy impossible
Table 11. European (ESCMID) guidelines for pharmacotherapy of CDI23
Diagnosis Recommended treatment
Note: Use of antiperistaltic agents and opiates should be avoided; tid, three-times daily; qid, four-times daily
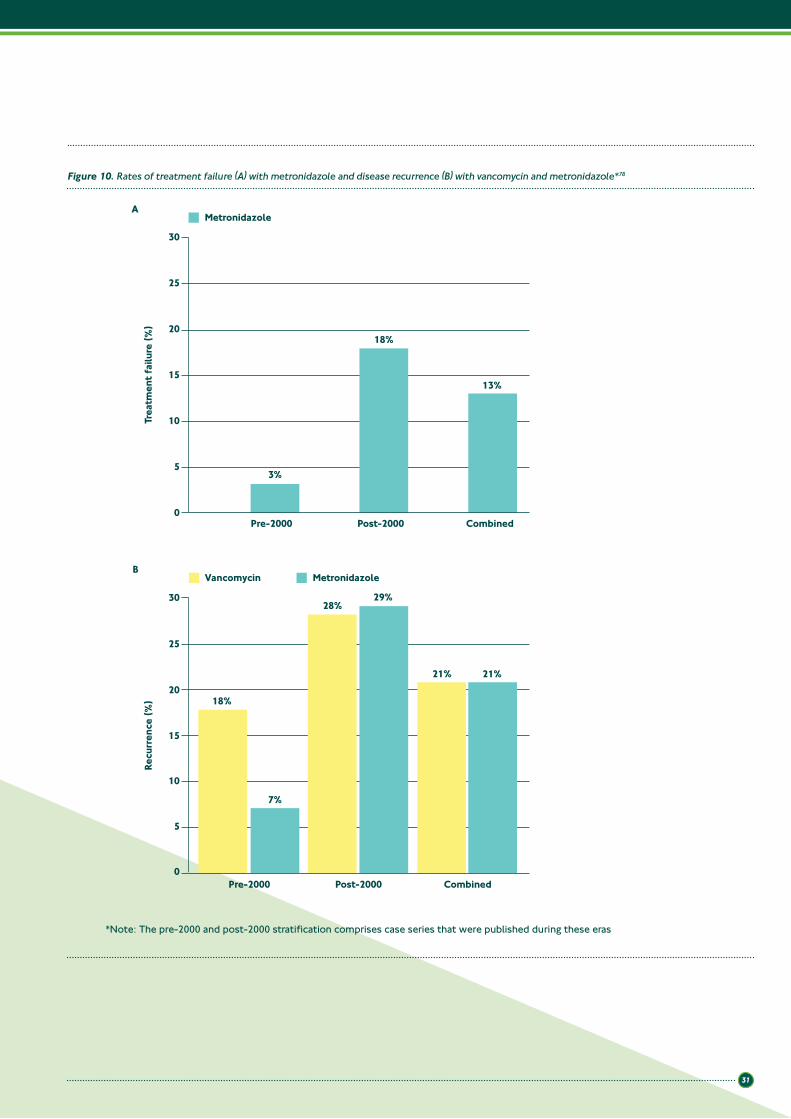
31
*Note: The pre-2000 and post-2000 stratification comprises case series that were published during these eras
Figure 10. Rates of treatment failure (A) with metronidazole and disease recurrence (B) with vancomycin and metronidazole*78
A
Recu
rren
ce (%
)
Pre-2000 Post-20000
5
10
15
20
25
30
Combined
7%
29%
21%
28%
18%
21%
Vancomycin Metronidazole
Metronidazole
B
Pre-2000 Post-2000 Combined
Trea
tmen
t fai
lure
(%)
0
5
10
15
20
25
30
18%
3%
13%
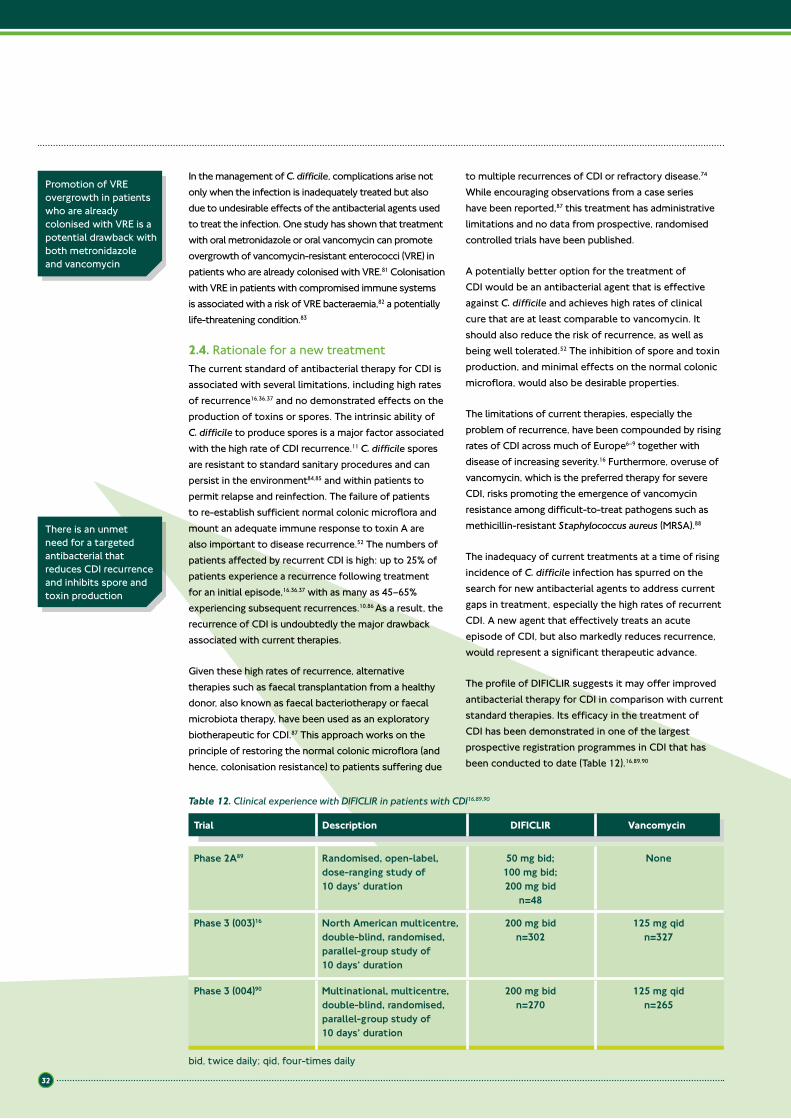
32
In the management of C. difficile, complications arise not only when the infection is inadequately treated but also due to undesirable effects of the antibacterial agents used to treat the infection. One study has shown that treatment with oral metronidazole or oral vancomycin can promote overgrowth of vancomycin-resistant enterococci (VRE) in patients who are already colonised with VRE.81 Colonisation with VRE in patients with compromised immune systems is associated with a risk of VRE bacteraemia,82 a potentially life-threatening condition.83
2.4. Rationale for a new treatmentThe current standard of antibacterial therapy for CDI is associated with several limitations, including high rates of recurrence16,36,37 and no demonstrated effects on the production of toxins or spores. The intrinsic ability of C. difficile to produce spores is a major factor associated with the high rate of CDI recurrence.11 C. difficile spores are resistant to standard sanitary procedures and can persist in the environment84,85 and within patients to permit relapse and reinfection. The failure of patients to re-establish sufficient normal colonic microflora and mount an adequate immune response to toxin A are also important to disease recurrence.52 The numbers of patients affected by recurrent CDI is high: up to 25% of patients experience a recurrence following treatment for an initial episode,16,36,37 with as many as 45–65% experiencing subsequent recurrences.10,86 As a result, the recurrence of CDI is undoubtedly the major drawback associated with current therapies.
Given these high rates of recurrence, alternative therapies such as faecal transplantation from a healthy donor, also known as faecal bacteriotherapy or faecal microbiota therapy, have been used as an exploratory biotherapeutic for CDI.87 This approach works on the principle of restoring the normal colonic microflora (and hence, colonisation resistance) to patients suffering due
to multiple recurrences of CDI or refractory disease.74 While encouraging observations from a case series have been reported,87 this treatment has administrative limitations and no data from prospective, randomised controlled trials have been published.
A potentially better option for the treatment of CDI would be an antibacterial agent that is effective against C. difficile and achieves high rates of clinical cure that are at least comparable to vancomycin. It should also reduce the risk of recurrence, as well as being well tolerated.52 The inhibition of spore and toxin production, and minimal effects on the normal colonic microflora, would also be desirable properties.
The limitations of current therapies, especially the problem of recurrence, have been compounded by rising rates of CDI across much of Europe6–9 together with disease of increasing severity.16 Furthermore, overuse of vancomycin, which is the preferred therapy for severe CDI, risks promoting the emergence of vancomycin resistance among difficult-to-treat pathogens such as methicillin-resistant Staphylococcus aureus (MRSA).88
The inadequacy of current treatments at a time of rising incidence of C. difficile infection has spurred on the search for new antibacterial agents to address current gaps in treatment, especially the high rates of recurrent CDI. A new agent that effectively treats an acute episode of CDI, but also markedly reduces recurrence, would represent a significant therapeutic advance.
The profile of DIFICLIR suggests it may offer improved antibacterial therapy for CDI in comparison with current standard therapies. Its efficacy in the treatment of CDI has been demonstrated in one of the largest prospective registration programmes in CDI that has been conducted to date (Table 12).16,89,90
There is an unmet need for a targeted antibacterial that reduces CDI recurrence and inhibits spore and toxin production
Promotion of VRE overgrowth in patients who are already colonised with VRE is a potential drawback with both metronidazole and vancomycin
Table 12. Clinical experience with DIFICLIR in patients with CDI16,89,90
Trial Description DIFICLIR Vancomycin
Phase 2A89 Randomised, open-label, dose-ranging study of 10 days’ duration
50 mg bid; 100 mg bid; 200 mg bid
n=48
None
Phase 3 (003)16 North American multicentre, double-blind, randomised, parallel-group study of 10 days’ duration
200 mg bidn=302
125 mg qidn=327
Phase 3 (004)90 Multinational, multicentre, double-blind, randomised, parallel-group study of 10 days’ duration
200 mg bidn=270
125 mg qidn=265
bid, twice daily; qid, four-times daily

33
Overall, the results from these studies showed that DIFICLIR was non-inferior to vancomycin in the treatment of acute CDI but, additionally, was significantly more effective than vancomycin in reducing disease recurrence and therefore
significantly more effective in terms of sustained clinical response.16,90 DIFICLIR was generally well tolerated with a safety profile that was comparable to oral vancomycin.16,90,91 These findings are discussed in detail in Chapters 6 and 7.
A new agent that effectively treats an acute episode of CDI but also markedly reduces recurrence would represent a significant therapeutic advance
2.5. Summary
Key points
• C. difficile is the leading cause of nosocomial infectious diarrhoea in industrialised countries, and the incidence of CDI is increasing
• The ability to produce spores and their persistent nature is a key factor in the transmission of C. difficile to patients• Exposure to antibacterial therapy that reduces colonisation resistance is the main predisposing event in the
acquisition of CDI• Older age and being immunocompromised are thought to be key risk factors in the development of CDI• The number of reported cases of CDI has increased dramatically in the past decade, together with increased
morbidity and mortality from CDI• The emergence of epidemic strains has been a significant factor in outbreaks and is associated with increased
morbidity and mortality from CDI• CDI imposes a substantial burden on healthcare systems (length of hospital stay, morbidity, mortality)• Surveillance and reporting are inconsistent across Europe, with varying levels of knowledge and awareness of
the disease and its impact• The recommended approach for diagnosis of CDI is a two-step process• As treatment of CDI is often empirical, rapid diagnostic tests with improved sensitivity and specificity are
needed to facilitate early treatment• For patients with mild CDI, without systemic symptoms, discontinuation of the antibacterial therapy may be
sufficient to resolve diarrhoea• Oral or IV metronidazole has been the usual first-line treatment for CDI, with oral (or enteral) vancomycin
being reserved for severe and recurrent CDI• Up to 25% of CDI patients suffer a recurrence of infection within 30 days following treatment• Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic
include those who:o Are immunocompromisedo Are receiving concomitant antibioticso Are renally impairedo Are aged 65 years or over
• ESCMID has identified recurrence as being the most important problem in the treatment of CDI• CDI remains a disease for which there are significant unmet needs, e.g.:
o Therapy to provide sustained clinical cure (defined as clinical cure without recurrence)o Therapy to reduce recurrence (relapse and/or reinfection)o Better identification of patients at risk of recurrence or those for whom the impact of recurrence
would be most dramatic• A new agent that effectively treats an acute episode of CDI but also markedly reduces recurrence would
represent a significant therapeutic advance• DIFICLIR has a clinical profile that offers improved therapy for CDI compared with current treatments
o Results from phase 3 studies showed that DIFICLIR was comparable to vancomycin in the treatment of acute CDI and was significantly more effective than vancomycin at reducing the likelihood of disease recurrence (i.e. providing a sustained clinical cure)
• DIFICLIR was well tolerated with a safety profile that was comparable to oral vancomycin.
34
2.6. References1. Hall IC, O’Toole E. Intestinal flora in newborn infants with a
description of a new pathogenic anaerobe, Bacillus difficilis. Am J Dis Child 1935;49:390–402.
2. Riley TV. Clostridium. Chapter 22 in Medical Microbiology. Eds: D Greenwood, R Slack, J Peutherer, M Barer. 17th Ed: Churchill Livingstone, 2007.
3. Larson HE, Price AB, Honour P, et al. Clostridium difficile and the aetiology of pseudomembranous colitis. Lancet 1978;1:1063–6.
4. Bartlett JG, Taylor NS, Chang T, et al. Clinical and laboratory observations in Clostridium difficile colitis. Am J Clin Nutr 1980;33(11 Suppl):2521–6.
5. Crobach MJ, Dekkers OM, Wilcox MH, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): data review and recommendations for diagnosing Clostridium difficile-infection (CDI). Clin Microbiol Infect 2009;15:1053–66.
6. Lyytikäinen O, Turunen H, Sund R, et al. Hospitalizations and deaths associated with Clostridium difficile infection, Finland, 1996–2004. Emerg Infect Dis 2009;15:761–5.
7. Søes L, Mølbak K, Strøbaek S, et al. The emergence of Clostridium difficile PCR ribotype 027 in Denmark – a possible link with the increased consumption of fluoroquinolones and cephalosporins? Euro Surveill 2009;14:pii-19176.
8. Soler P, Nogareda F, Cano R. Rates of Clostridium difficile infection in patients discharged from Spanish hospitals, 1997–2005. Infect Control Hosp Epidemiol 2008;29:887–9.
9. Vonberg RP, Schwab F, Gastmeier P. Clostridium difficile in discharged inpatients, Germany. Emerg Infect Dis 2007;13:179–80.
10. McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol 2002;97:1769–75.
11. Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ 2004;171:51–8.
12. Verity P, Wilcox MH, Fawley W, et al. Prospective evaluation of environmental contamination by Clostridium difficile in isolation side rooms. J Hosp Infect 2001;49:204–9.
13. McFarland LV, Mulligan ME, Kwok RY, et al. Nosocomial acquisition of Clostridium difficile infection. N Engl J Med 1989;320:204–10.
14. Health Protection Agency. Investigation into outbreaks of Clostridium difficile at Maidstone and Tunbridge Wells NHS Trust. Commission for Healthcare Audit and Inspection, 2007.
15. Kelly CP, LaMont JT. Clostridium difficile infection. Annu Rev Med 1998;49:375–90.
16. Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
17. Rupnik M, Wilcox MH, Gerding DN. Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat Rev Microbiol 2009;7:526–36.
18. Triadafilopoulos G, Hallstone AE. Acute abdomen as the first presentation of pseudomembranous colitis. Gastroenterology 1991;101:685–91.
19. Kyne L, Warny M, Qamar A, et al. Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A. N Engl J Med 2000;342:390–7.
20. Kyne L, Warny M, Qamar A, et al. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhea. Lancet 2001;357:189–93.
21. Barbut F, Decré D, Lalande V, et al. Clinical features of Clostridium difficile-associated diarrhoea due to binary toxin (actin-specific ADP-ribosyltransferase)-producing strains. J Med Microbiol 2005;54:181–5.
22. Wilcox M, Minton J. Role of antibody response in outcome of antibiotic-associated diarrhoea. Lancet 2001;357:158–9.
23. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clin Microbiol Infect 2009;15:1067–79.
24. Bartlett JG, Gerding DN. Clinical recognition and diagnosis of Clostridium difficile. Clin Infect Dis 2008;46:S12–8.
25. Mogg GA, Keighley MR, Burdon DW, et al. Antibiotic-associated colitis – a review of 66 cases. Br J Surg 1979;66:738–42.
26. Monaghan T, Boswell T, Mahida YR. Recent advances in Clostridium difficile-associated disease. Gut 2008;57:850–60.
27. Lipsett PA, Samantaray DK, Tam ML, et al. Pseudomembranous colitis: a surgical disease? Surgery 1994;116:491–6.
28. Feldman RJ, Kallich M, Weinstein MP. Bacteremia due to Clostridium difficile: case report and review of extraintestinal C. difficile infections. Clin Infect Dis 1995;20:1560–2.
29. Cohen MB. Clostridium difficile infections: emerging epidemiology and new treatments. J Ped Gastroenterol Nutr 2009;48:63–5.
30. Bauer MP, Noretmans DW, van Benthem BH, et al. Clostridium difficile infection in Europe: a hospital-based survey. Lancet 2011;377:63–73.
31. Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect 1998;40:1–15.
32. Hu MY, Katchar K, Kyne L, et al. Prospective derivation and validation of a clinical prediction rule for recurrent Clostridium difficile infection. Gastroenterology 2009;136: 1206–14.
33. Pépin J, Alary M-E, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis 2005;40:1591–7.
34. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis 1998;26:954–9.
35
35. Bauer MP, Miller M, Gerding DN, et al. Renal failure, fever, and leukocytosis all predict treatment failure in Clostridium difficile infection (CDI), but renal failure is the only predictor of recurrent CDI. Clin Microbiol Infect 2011;17(Suppl 4):A1–4.
36. Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med 2010;362:197–205.
37. Bouza E, Dryden M, Mohammed R, et al. Results of a phase III trial comparing tolevamer, vancomycin and metronidazole in patients with Clostridium difficile-associated diarrhoea. Clin Microbiol Infect 2008; 14(Suppl 7):S103–4.
38. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multiinstitutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–9.
39. Dubberke ER, Wertheimer AI. Review of current literature on the economic burden of Clostridium difficile infection. Infect Control Hosp Epidemiol 2009;30:57–66.
40. Vonberg RP, Reichardt C, Behnke M, et al. Costs of nosocomial Clostridium difficile-associated diarrhoea. J Hosp Infect 2008;70:15–20.
41. Wilcox MH, Cunniffe JG, Trundle C, et al. Financial burden of hospital-acquired Clostridium difficile infection. J Hosp Infect 1996;34:23–30.
42. Kuijper EJ, Coignard B, Tull P. ESCMID study group for Clostridium difficile. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin Microbiol Infect 2006;12:2–18.
43. Kuijper EJ, van Dissel JT. Spectrum of Clostridium difficile infections outside health care facilities. CMAJ 2008;179:747–8.
44. Bartlett JG. Historical perspectives on studies of Clostridium difficile and C. difficile infection. Clin Infect Dis 2008;46:S4–11.
45. Bilgrami S, Feingold JM, Dorsky D, et al. Incidence and outcome of Clostridium difficile infection following autologous peripheral blood stem cell transplantation. Bone Marrow Transplant 1999;23:1039–42.
46. Barbut F, Corthier G, Charpak Y, et al. Prevalence and pathogenicity of Clostridium difficile in hospitalized patients. A French multicenter study. Arch Intern Med 1996;156:1449–54.
47. Centers for Disease Control and Prevention. Severe Clostridium difficile-associated disease in populations previously at low risk – four states, 2005. MMWR Weekly 2005;54:1201–5.
48. Rouphael NG, O’Donnell JA, Bhatnagar J, et al. Clostridium difficile-associated diarrhea: an emerging threat to pregnant women. Am J Obstet Gynecol 2008;198:635.e1–635.e6.
49. Bliss DZ, Johnson S, Savik K, et al. Acquisition of Clostridium difficile and Clostridium difficile–associated diarrhea in hospitalized patients receiving tube feeding. Ann Intern Med 1998;129:1012–9.
50. Thibault A, Miller MA, Gaese C. Risk factors for the development of Clostridium difficile-associated diarrhea during a hospital outbreak. Infect Control Hosp Epidemiol 1991;12:345–8.
51. Gerding DN, Olson MM, Peterson LR, et al. Clostridium difficile-associated diarrhea and colitis in adults. A prospective case-controlled epidemiologic study. Arch Intern Med 1986;146:95–100.
52. DuPont HL. The search for effective treatment of Clostridium difficile infection. N Engl J Med 2011;364:473–4.
53. Archibald LK, Banerjee SN, Jarvis WR. Secular trends in hospital-acquired Clostridium difficile disease in the United States, 1987–2001. J Infect Dis 2004;189:1585–9.
54. Pépin J, Valiquette L, Alary ME, et al. Clostridium difficile-associated diarrhea in a region of Quebec from 1991 to 2003: a changing pattern of disease severity. CMAJ 2004;171:466–72.
55. Loo VG, Libman MD, Miller MA, et al. Clostridium difficile: a formidable foe. CMAJ 2004;71:47–8.
56. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev 2010;23:529–49.
57. Health Protection Agency. Health protection report. Weekly report, 18 February 2011.
58. Walker AS, Spiegelhalter D, Crook DW, et al. Fairness of financial penalties to improve control of Clostridium difficile. BMJ 2008;337:a2097.
59. McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med 2005;353:2433–41.
60. Kuijper EJ, Barbut F, Brazier JS, et al. Update of Clostridium difficile infection due to PCR ribotype 027 in Europe, 2008. Euro Surveill 2008;13ii:18942.
61. Merrigan M, Venugopal A, Mallozzi M, et al. Human hypervirulent Clostridium difficile strains exhibit increased sporulation as well as robust toxin production. J Bacteriol 2010;192:4904–11.
62. Warny M, Pépin J, Fang A, et al. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North America and Europe. Lancet 2005;366:1079–84.
63. Pépin J, Saheb N, Coulombe MA, et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a cohort study during an epidemic in Quebec. Clin Infect Dis 2005;41:1254–60.
64. Goorhuis A, Bakker D, Corver J, et al. Emergence of Clostridium difficile infection due to a new epidemic strain, polymerase chain reaction ribotype 078. Clin Infect Dis 2008;47:1162–70.
65. Bartlett JG. Antibiotic associated diarrhoea. N Engl J Med 2002;346:334–9.
66. Health Protection Agency. Clostridium difficile infection: how to deal with the problem. Department of Health and Health Protection Agency, 2008.
36
67. Shetty N, Wren MW, Coen PG. The role of glutamate dehydrogenase for the detection of Clostridium difficile in faecal samples: a meta-analysis. J Hosp Infect 2011;77:1–6.
68. Barbut F, Kajzer C, Planas N, et al. Comparison of three enzyme immunoassays, a cytotoxicity assay, and toxigenic culture for diagnosis of Clostridium difficile-associated diarrhea. J Clin Microbiol 1993;31:963–7.
69. Shanholtzer CJ, Willard KE, Holter JJ, et al. Comparison of the VIDAS Clostridium difficile toxin A immunoassay with C. difficile culture and cytotoxin and latex tests. J Clin Microbiol 1992;30:1837–40.
70. De Girolami PC, Hanff PA, Eichelberger K, et al. Multicenter evaluation of a new enzyme immunoassay for detection of Clostridium difficile enterotoxin A. J Clin Microbiol 1992;30:1085–8.
71. Doern GV, Coughlin RT, Wu L. Laboratory diagnosis of Clostridium difficile-associated gastrointestinal disease: comparison of a monoclonal antibody enzyme immunoassay for toxins A and B with a monoclonal antibody enzyme immunoassay for toxin A only and two cytotoxicity assays. J Clin Microbiol 1992;30:2042–6.
72. Goldenberg SD, Price NM, Tucker D, et al. Mandatory reporting and improvements in diagnosing Clostridium difficile infection: an incompatible dichotomy? J Infect 2011;62:363–70.
73. Goldenberg SD, Cliff PR, Smith S, et al. Two-step glutamate dehydrogenase antigen real-time polymerase chain reaction assay for detection of toxigenic Clostridium difficile. J Hosp Infect 2010;74:48–54.
74. Ananthakrishnan AN. Clostridium difficile infection: epidemiology, risk factors and management. Nat Rev Gastroenterol Hepatol 2011;8:17–26.
75. van den Berg RJ, Vaessen N, Endtz HP, et al. Evaluation of real-time PCR and conventional diagnostic methods for the detection of Clostridium difficile-associated diarrhoea in a prospective multicentre study. J Med Microbiol 2007;56:36–42.
76. Zar FA, Bakkanagari SR, Moorthi SR, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium-associated diarrhea, stratified by disease severity. Clin Infect Dis 2007;45:302–7.
77. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 2010;31:431–55.
78. Aslam S, Hamill RJ, Musher DM. Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 2005;5:549–57.
79. McFarland LV. Renewed interest in a difficult disease: Clostridium difficile infections – epidemiology and current treatment strategies. Curr Opin Gastroenterol 2009;25:24–35.
80. Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis 2005;40:1586–90.
81. Al-Nassir WN, Sethi AK, Li Y, et al. Both oral metronidazole and oral vancomycin promote persistent overgrowth of vancomycin-resistant enterococci during treatment of Clostridium difficile-associated disease. Antimicrob Agents Chemother 2008;52:2403–6
82. Butler AM, Olsen MA, Merz LR, et al. Attributable costs of enterococcal bloodstream infections in a nonsurgical hospital cohort. Infect Control Hosp Epidemiol 2010;31:28–35.
83. Olivier CN, Blake RK, Steed LL, et al. Risk of vancomycin-resistant enterococcus (VRE) bloodstream infection among patients colonized with VRE. Infect Control Hosp Epidemiol 2008;29:404–9.
84. Mylonakis E, Ryan ET, Calderwood SB. Clostridium difficile-associated diarrhea. Arch Intern Med 2001;161:525–33.
85. Hurley BW, Nguyen CC. The spectrum of pseudomembranous enterocolitis and antibiotic-associated diarrhea. Arch Intern Med 2002;162:2177–84.
86. McFarland LV, Surawicz CM, Greenberg RN, et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913–8.
87. Yoon SS, Brandt LJ. Treatment of refractory/recurrent C. difficile-associated disease by donated stool transplanted via colonoscopy: a case series of 12 patients. J Clin Gastroenterol 2010;44:562–6.
88. Centers of Disease Control and Prevention. Investigation and control of vancomycin intermediate and resistant Staphylococcus aureus (VISA/VRSA). A Guide for Health Departments and Infection. September 2006.
89. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety, and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
90. Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;doi:10.1016/S1473-3099(11)70374-7.
91. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
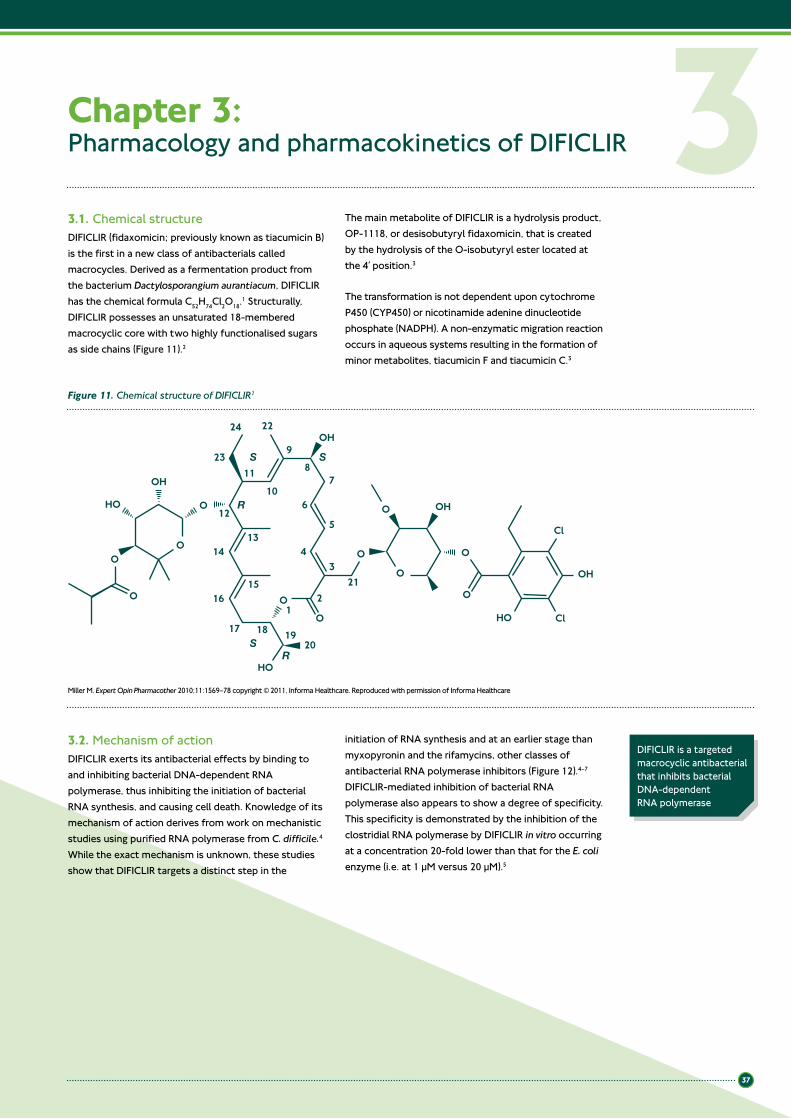
37
Chapter 3: Pharmacology and pharmacokinetics of DIFICLIR
3.1. Chemical structureDIFICLIR (fidaxomicin; previously known as tiacumicin B) is the first in a new class of antibacterials called macrocycles. Derived as a fermentation product from the bacterium Dactylosporangium aurantiacum, DIFICLIR has the chemical formula C52H74Cl2O18.1 Structurally, DIFICLIR possesses an unsaturated 18-membered macrocyclic core with two highly functionalised sugars as side chains (Figure 11).2
The main metabolite of DIFICLIR is a hydrolysis product, OP-1118, or desisobutyryl fidaxomicin, that is created by the hydrolysis of the O-isobutyryl ester located at the 4′ position.3
The transformation is not dependent upon cytochrome P450 (CYP450) or nicotinamide adenine dinucleotide phosphate (NADPH). A non-enzymatic migration reaction occurs in aqueous systems resulting in the formation of minor metabolites, tiacumicin F and tiacumicin C.3
3OH
HO
O
O OH
OOH
O
O
O
O HO
Cl
Cl
O
O
O
O
HO
OH
24 22
98
7
5
321
6
4
23
12
14
16
17 18S
S S
R
R
1920
21
15
13
10
11
Figure 11. Chemical structure of DIFICLIR1
3.2. Mechanism of actionDIFICLIR exerts its antibacterial effects by binding to and inhibiting bacterial DNA-dependent RNA polymerase, thus inhibiting the initiation of bacterial RNA synthesis, and causing cell death. Knowledge of its mechanism of action derives from work on mechanistic studies using purified RNA polymerase from C. difficile.4 While the exact mechanism is unknown, these studies show that DIFICLIR targets a distinct step in the
initiation of RNA synthesis and at an earlier stage than myxopyronin and the rifamycins, other classes of antibacterial RNA polymerase inhibitors (Figure 12).4–7 DIFICLIR-mediated inhibition of bacterial RNA polymerase also appears to show a degree of specificity. This specificity is demonstrated by the inhibition of the clostridial RNA polymerase by DIFICLIR in vitro occurring at a concentration 20-fold lower than that for the E. coli enzyme (i.e. at 1 µM versus 20 µM).5
Miller M. Expert Opin Pharmacother 2010;11:1569–78 copyright © 2011, Informa Healthcare. Reproduced with permission of Informa Healthcare
DIFICLIR is a targeted macrocyclic antibacterial that inhibits bacterial DNA-dependent RNA polymerase

38
3.3. PharmacokineticsThe pharmacokinetic properties of DIFICLIR have been determined from a series of phase 1 studies in 126 healthy volunteers, a phase 2A proof-of-concept study in 48 patients infected with C. difficile, as well as a subset of the patients included in the two phase 3 clinical trials. A total of six studies examined the pharmacokinetics of DIFICLIR at single and multiple doses up to 450 mg.8 The studies also assessed the effect of food on plasma concentrations and the potential for interactions with concomitantly administered drugs.
3.3.1. Absorption3.3.1.1. Plasma levels
In healthy adult volunteers, oral administration of DIFICLIR at doses in the range 100–450 mg resulted in negligible systemic absorption of drug with plasma levels often below quantifiable limits (Table 13).8 Even at the highest doses, multiple dosing over 10 consecutive days showed no evidence of drug accumulation. Plasma levels of OP-1118 were about 2-fold higher than those of the parent drug but still close to quantifiable limits of 5 ng/mL.9
Table 13. Mean peak plasma concentrations following a single oral dose of DIFICLIR 100–450 mg to healthy volunteers (n=16)8
Dose of DIFICLIR
100 mg 200 mg 300 mg 450 mg
Plasma concentration (range), ng/mL
7.1 (5.2–9.7)
8.1 (5.2–10.6)
9.9 (5.1–16.9)
23.9 (13.8–37.8)
Figure 12. Illustrated model of the initiation of clostridial messenger RNA synthesis showing the stages that are inhibited by DIFICLIR, myxopyronin and the rifamycins7
*s subunit interacts with promoter DNA; mRNA, messenger ribonucleic acid; RNA, ribonucleic acid
Reproduced with permission
s subunit*
Core RNA polymerase
RNA polymerase holoenzyme
Activesite
+ Nucleotidetriphosphates
Elongation of mRNA
Myxopyronin
DIFICLIR
Rifamycins
+1
+1
+1
-10-35
-10-35
PromoterDNA
Open complex
Second intermediatecomplex
First intermediatecomplex
Closed complex
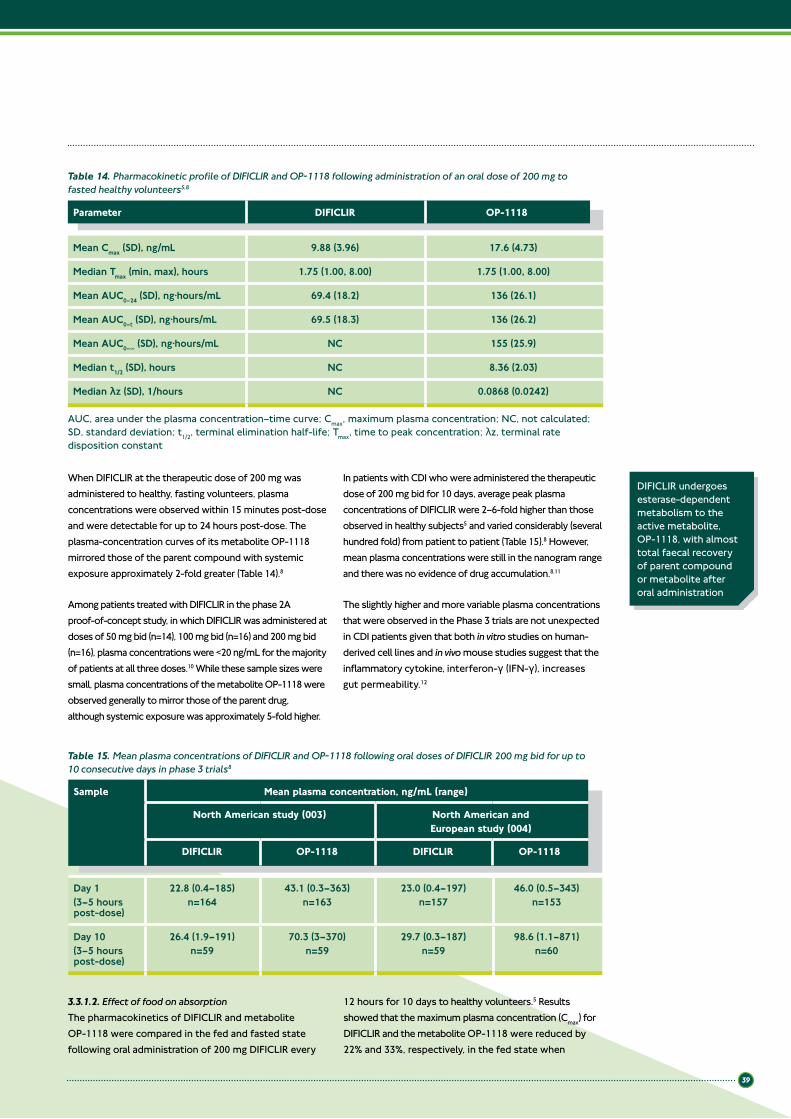
39
Parameter DIFICLIR OP-1118
Mean Cmax (SD), ng/mL 9.88 (3.96) 17.6 (4.73)
Median Tmax (min, max), hours 1.75 (1.00, 8.00) 1.75 (1.00, 8.00)
Mean AUC0–24 (SD), ng·hours/mL 69.4 (18.2) 136 (26.1)
Mean AUC0–t (SD), ng·hours/mL 69.5 (18.3) 136 (26.2)
Mean AUC0–∞ (SD), ng·hours/mL NC 155 (25.9)
Median t1/2 (SD), hours NC 8.36 (2.03)
Median λz (SD), 1/hours NC 0.0868 (0.0242)
AUC, area under the plasma concentration–time curve; Cmax, maximum plasma concentration; NC, not calculated; SD, standard deviation; t1/2, terminal elimination half-life; Tmax, time to peak concentration; λz, terminal rate disposition constant
Table 14. Pharmacokinetic profile of DIFICLIR and OP-1118 following administration of an oral dose of 200 mg to fasted healthy volunteers5,8
When DIFICLIR at the therapeutic dose of 200 mg was administered to healthy, fasting volunteers, plasma concentrations were observed within 15 minutes post-dose and were detectable for up to 24 hours post-dose. The plasma-concentration curves of its metabolite OP-1118 mirrored those of the parent compound with systemic exposure approximately 2-fold greater (Table 14).8
Among patients treated with DIFICLIR in the phase 2A proof-of-concept study, in which DIFICLIR was administered at doses of 50 mg bid (n=14), 100 mg bid (n=16) and 200 mg bid (n=16), plasma concentrations were <20 ng/mL for the majority of patients at all three doses.10 While these sample sizes were small, plasma concentrations of the metabolite OP-1118 were observed generally to mirror those of the parent drug, although systemic exposure was approximately 5-fold higher.
In patients with CDI who were administered the therapeutic dose of 200 mg bid for 10 days, average peak plasma concentrations of DIFICLIR were 2–6-fold higher than those observed in healthy subjects5 and varied considerably (several hundred fold) from patient to patient (Table 15).8 However, mean plasma concentrations were still in the nanogram range and there was no evidence of drug accumulation.8,11
The slightly higher and more variable plasma concentrations that were observed in the Phase 3 trials are not unexpected in CDI patients given that both in vitro studies on human-derived cell lines and in vivo mouse studies suggest that the inflammatory cytokine, interferon-γ (IFN-γ), increases gut permeability.12
DIFICLIR undergoes esterase-dependent metabolism to the active metabolite, OP-1118, with almost total faecal recovery of parent compound or metabolite after oral administration
Day 1 (3–5 hours post-dose)
22.8 (0.4–185)n=164
43.1 (0.3–363)n=163
23.0 (0.4–197)n=157
46.0 (0.5–343)n=153
Day 10 (3–5 hours post-dose)
26.4 (1.9–191)n=59
70.3 (3–370)n=59
29.7 (0.3–187)n=59
98.6 (1.1–871)n=60
Table 15. Mean plasma concentrations of DIFICLIR and OP-1118 following oral doses of DIFICLIR 200 mg bid for up to 10 consecutive days in phase 3 trials8
Sample Mean plasma concentration, ng/mL (range)
North American study (003) North American and European study (004)
DIFICLIR OP-1118 DIFICLIR OP-1118
3.3.1.2. Effect of food on absorptionThe pharmacokinetics of DIFICLIR and metabolite OP-1118 were compared in the fed and fasted state following oral administration of 200 mg DIFICLIR every
12 hours for 10 days to healthy volunteers.5 Results showed that the maximum plasma concentration (Cmax) for DIFICLIR and the metabolite OP-1118 were reduced by 22% and 33%, respectively, in the fed state when
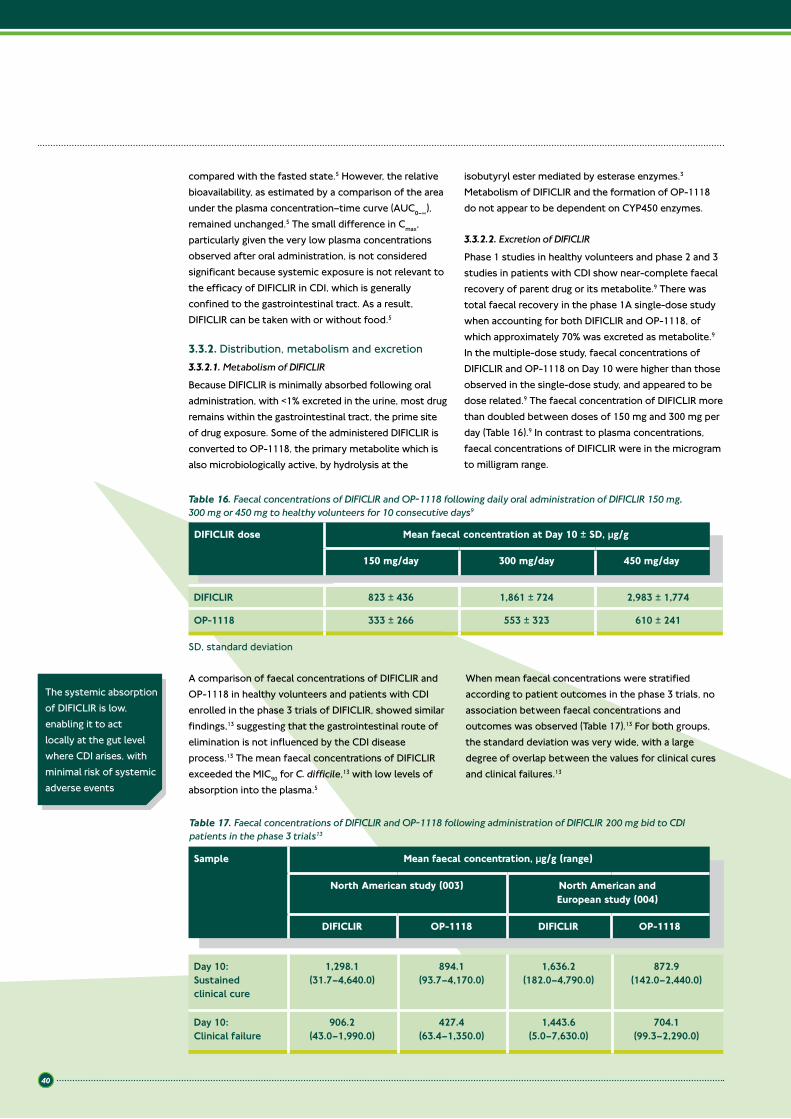
40
A comparison of faecal concentrations of DIFICLIR and OP-1118 in healthy volunteers and patients with CDI enrolled in the phase 3 trials of DIFICLIR, showed similar findings,13 suggesting that the gastrointestinal route of elimination is not influenced by the CDI disease process.13 The mean faecal concentrations of DIFICLIR exceeded the MIC90 for C. difficile,13 with low levels of absorption into the plasma.5
When mean faecal concentrations were stratified according to patient outcomes in the phase 3 trials, no association between faecal concentrations and outcomes was observed (Table 17).13 For both groups, the standard deviation was very wide, with a large degree of overlap between the values for clinical cures and clinical failures.13
The systemic absorption of DIFICLIR is low, enabling it to act locally at the gut level where CDI arises, with minimal risk of systemic adverse events
Table 17. Faecal concentrations of DIFICLIR and OP-1118 following administration of DIFICLIR 200 mg bid to CDI patients in the phase 3 trials13
Day 10:Sustained clinical cure
1,298.1(31.7–4,640.0)
894.1(93.7–4,170.0)
1,636.2(182.0–4,790.0)
872.9(142.0–2,440.0)
Day 10: Clinical failure
906.2(43.0–1,990.0)
427.4(63.4–1,350.0)
1,443.6(5.0–7,630.0)
704.1(99.3–2,290.0)
Sample Mean faecal concentration, µg/g (range)
North American study (003) North American and European study (004)
DIFICLIR OP-1118 DIFICLIR OP-1118
compared with the fasted state.5 However, the relative bioavailability, as estimated by a comparison of the area under the plasma concentration–time curve (AUC0–∞), remained unchanged.5 The small difference in Cmax, particularly given the very low plasma concentrations observed after oral administration, is not considered significant because systemic exposure is not relevant to the efficacy of DIFICLIR in CDI, which is generally confined to the gastrointestinal tract. As a result, DIFICLIR can be taken with or without food.5
3.3.2. Distribution, metabolism and excretion3.3.2.1. Metabolism of DIFICLIR
Because DIFICLIR is minimally absorbed following oral administration, with <1% excreted in the urine, most drug remains within the gastrointestinal tract, the prime site of drug exposure. Some of the administered DIFICLIR is converted to OP-1118, the primary metabolite which is also microbiologically active, by hydrolysis at the
isobutyryl ester mediated by esterase enzymes.3 Metabolism of DIFICLIR and the formation of OP-1118 do not appear to be dependent on CYP450 enzymes.
3.3.2.2. Excretion of DIFICLIR
Phase 1 studies in healthy volunteers and phase 2 and 3 studies in patients with CDI show near-complete faecal recovery of parent drug or its metabolite.9 There was total faecal recovery in the phase 1A single-dose study when accounting for both DIFICLIR and OP-1118, of which approximately 70% was excreted as metabolite.9 In the multiple-dose study, faecal concentrations of DIFICLIR and OP-1118 on Day 10 were higher than those observed in the single-dose study, and appeared to be dose related.9 The faecal concentration of DIFICLIR more than doubled between doses of 150 mg and 300 mg per day (Table 16).9 In contrast to plasma concentrations, faecal concentrations of DIFICLIR were in the microgram to milligram range.
DIFICLIR 823 ± 436 1,861 ± 724 2,983 ± 1,774
OP-1118 333 ± 266 553 ± 323 610 ± 241
DIFICLIR dose Mean faecal concentration at Day 10 ± SD, µg/g
150 mg/day 300 mg/day 450 mg/day
Table 16. Faecal concentrations of DIFICLIR and OP-1118 following daily oral administration of DIFICLIR 150 mg, 300 mg or 450 mg to healthy volunteers for 10 consecutive days9
SD, standard deviation

41
DIFICLIR and potent P-gp inhibitors should not be administered at the same time
3.4. Drug–drug interactionsDIFICLIR is metabolised primarily by esterase-dependent metabolism to OP-1118.3 Drug interactions are potentially possible with drugs that could increase absorption of DIFICLIR or inhibit its systemic clearance. However, at present there are no commercially available drugs that cause clinically relevant drug interactions by inhibiting esterases and, moreover, the absorption of DIFICLIR is very limited.5 Significant drug interactions by way of inhibition of metabolism of DIFICLIR are not anticipated.14
As many drugs are metabolised by the CYP450 system or actively excreted by drug transport systems such as P-glycoprotein (P-gp), studies were undertaken in healthy volunteers to assess the impact of DIFICLIR and OP-1118 on these systems. Although DIFICLIR and OP-1118 are weak inhibitors of CYP enzymes, clinical drug–drug interaction studies of DIFICLIR with a CYP substrate did not result in statistically significant changes in the pharmacokinetics of marker substrate drugs for CYP2C9 (warfarin), CYP2C19 (omeprazole) and CYP3A4/5 (midazolam).14 No dose adjustment is necessary when DIFICLIR is co-administered with drugs that are CYP substrates.
DIFICLIR and OP-1118 are substrates of the transporter P-gp and may be mild-to-moderate inhibitors of intestinal P-gp.5 The inhibition of P-gp may lead to higher systemic exposure to DIFICLIR and OP-1118. Co-administration of single doses of the P-gp inhibitor cyclosporin A and DIFICLIR in healthy volunteers were observed to result in a 4- and 2-fold increase in DIFICLIR Cmax and AUC, respectively, and in a 9.5- and 4-fold increase in Cmax and AUC, respectively, for OP-1118. The clinical relevance of this increase in exposure is unclear. Due to the pharmacodynamics of potent P-gp inhibitors such as cyclosporin, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and amiodarone, these medicines should not be administered at the same time as DIFICLIR.5
DIFICLIR (200 mg bid) had a small but not clinically relevant effect on digoxin exposure. However, a larger effect on P-gp substrates with lower bioavailability more sensitive to intestinal P-gp inhibition, such as dabigatran etexilate, cannot be excluded.5
Because the systemic exposure to DIFICLIR is low, the use of the product is not expected to lead to any clinically meaningful systemic drug interactions.
3.5. Use of DIFICLIR in specific patient groupsDIFICLIR is the first drug in its class to be investigated for use in humans and data on its use in specific patient groups are therefore limited. Given that DIFICLIR is eliminated in the faeces with barely detectable levels present in urine, no dose adjustment is considered necessary in patients with renal impairment.5 Due to limited clinical data, DIFICLIR should be used with caution in patients with severe renal impairment, moderate-to-severe hepatic impairment, pseudomembranous colitis, or fulminant or life-threatening CDI. There are no data describing the use of DIFICLIR in patients with concomitant inflammatory bowel disease. DIFICLIR should be used with caution in these patients due to the risk of enhanced absorption and potential risk of systemic adverse reactions.5 The use of DIFICLIR in other specific patient groups is described in this chapter.
3.5.1. Pregnancy and breastfeedingThere are no data available from the use of DIFICLIR in pregnant women. Animal studies did not indicate direct or indirect harmful effects with respect to reproductive toxicity. As a precautionary measure, it is preferable to avoid the use of DIFICLIR during pregnancy.5
It is unknown if DIFICLIR and its metabolites are excreted in human milk. Although no effects on breastfed newborns/infants are anticipated since the systemic exposure to DIFICLIR is low, a risk to
newborns/infants cannot be excluded. A decision must therefore be made whether to discontinue breastfeeding or to discontinue/abstain from DIFICLIR therapy, taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.5
3.5.2. Paediatric populationThe safety and efficacy of DIFICLIR in children aged below 18 years has not yet been established. No data are available.5
3.5.3. Use in elderly patients (aged ≥65 years)More than 50% of patients enrolled in the phase 3 randomised controlled trials comparing DIFICLIR with vancomycin were ≥65 years, while just under a third were aged ≥75 years. Pharmacokinetic analyses in these patients showed that plasma levels of DIFICLIR and its active metabolite OP-1118 were slightly elevated in patients ≥65 years (Table 18).3 However, they were still in the low nanogram range and not considered clinically meaningful.5 Moreover, subgroup safety and efficacy analyses that included patients ≥65 years showed that the advantages of DIFICLIR over vancomycin mirrored those seen for the study population as a whole (a priori analysis, data not collected as a pre-defined endpoint).11 These findings suggest that at the therapeutic dose of 200 mg bid, DIFICLIR is as appropriate for patients aged ≥65 years as it is for those aged <65 years. No dose adjustment is necessary in patients aged ≥65 years undergoing treatment with DIFICLIR for CDI.5
No dose adjustment of DIFICLIR is necessary in elderly patients

42
3.6. Summary
Key points
• DIFICLIR is the first member of the new class of macrocyclic antibacterials• DIFICLIR targets bacterial DNA-dependent RNA polymerase, thus inhibiting the initiation of bacterial
RNA synthesis• DIFICLIR can be administered to patients with or without food• The pharmacokinetic properties of DIFICLIR include minimal systemic absorption (ng/mL range) and high
faecal concentrations (in the microgram to milligram range) that far exceed the MIC90 for C. difficile• The systemic absorption of DIFICLIR is low, enabling it to act locally at the gut level where CDI arises, with
minimal risk of systemic adverse events• DIFICLIR metabolism is catalysed by esterase-dependent metabolism to the active metabolite OP-1118 • DIFICLIR is excreted in the faeces with near complete faecal recovery of parent drug or its metabolite OP-1118• No dose adjustment is necessary when DIFICLIR is co-administered with drugs that are CYP substrates• DIFICLIR should not be co-administered with drugs that are potent P-gp inhibitors• No dose adjustment is necessary in older patients (≥65 years) undergoing treatment for CDI with DIFICLIR.
3.7. References1. Miller M. Fidaxomicin (OPT-80) for the treatment of
Clostridium infection. Expert Opin Pharmacother 2010;11:1569–78.
2. Swanson RN, Hardy DJ, Shipkowitz NL, et al. In vitro and in vivo evaluation of tiacumicins B and C against Clostridium difficile. Antimicrob Agents Chemother 1991;35:1108–11.
3. Astellas Pharma Europe Ltd. Data on file, FDX/11/0003/EU.
4. Sergio S, Piralis R, White R, et al. Lipiarmycin, a new antibiotic from Actinoplanes. III mechanism of action. J Antibiotics 1975;XXVIII:543–9.
5. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
6. Mullane KM, Gorbach S. Fidaxomicin: first-in-class macrocyclic antibiotic. Expert Rev Anti Infect Ther 2011;9:767–77.
7. Astellas Pharma Europe Ltd. Data on file, FDX/11/0025/EU.
8. Astellas Pharma Europe Ltd. Data on file, FDX/11/0002/EU.
9. Shue YK, Sears PS, Shangle S, et al. Safety, tolerance, and pharmacokinetic studies of OPT-80 in healthy volunteers following single and multiple oral doses. Antimicrob Agents Chemother 2008;52:1391–5.
10. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety, and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
11. Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
12. Beaurepaire C, Smyth D, McKay D. Interferon-γ regulation of intestinal epithelial permeability. J Interferon Cytokine Res 2009;29:133–43.
13. Astellas Pharma Europe Ltd. Data on file, FDX/11/0005/EU.
14. Astellas Pharma Europe Ltd. Data on file, FDX/11/0006/EU.
15. Astellas Pharma Europe Ltd. Data on file, FDX/11/0007/EU.
Table 18. Plasma concentrations of DIFICLIR and OP-1118 in CDI patients treated with DIFICLIR 200 mg bid in the phase 3 trials, stratified by age15
Plasma(Day 1: 3–5 hours post-dose), ng/mL
N>LLOQMean (SD)MedianRange
16715.2 (20.7)
8.8(0.364–197)
16529.4 (33.6)
15.5(0.283–173)
14531.6 (29.9)
24.3(0.898–185)
15161.0 (59.8)
46.5(0.982–363)
Plasma(Day 10: 3–5 hours post-dose), ng/mL
N>LLOQMean (SD)MedianRange
4218.0 (19.4)
9.2(1.90–86.9)
4556.4 (130)
19.4(3.01–871)
5836.2 (39.0)
22.2(0.305–191)
58108 (129)
68.7(1.09–829)
Sample Measurement Age <65 years Age ≥65 years
DIFICLIR OP-1118 DIFICLIR OP-1118
LLOQ, lower limit of quantification; SD, standard deviation
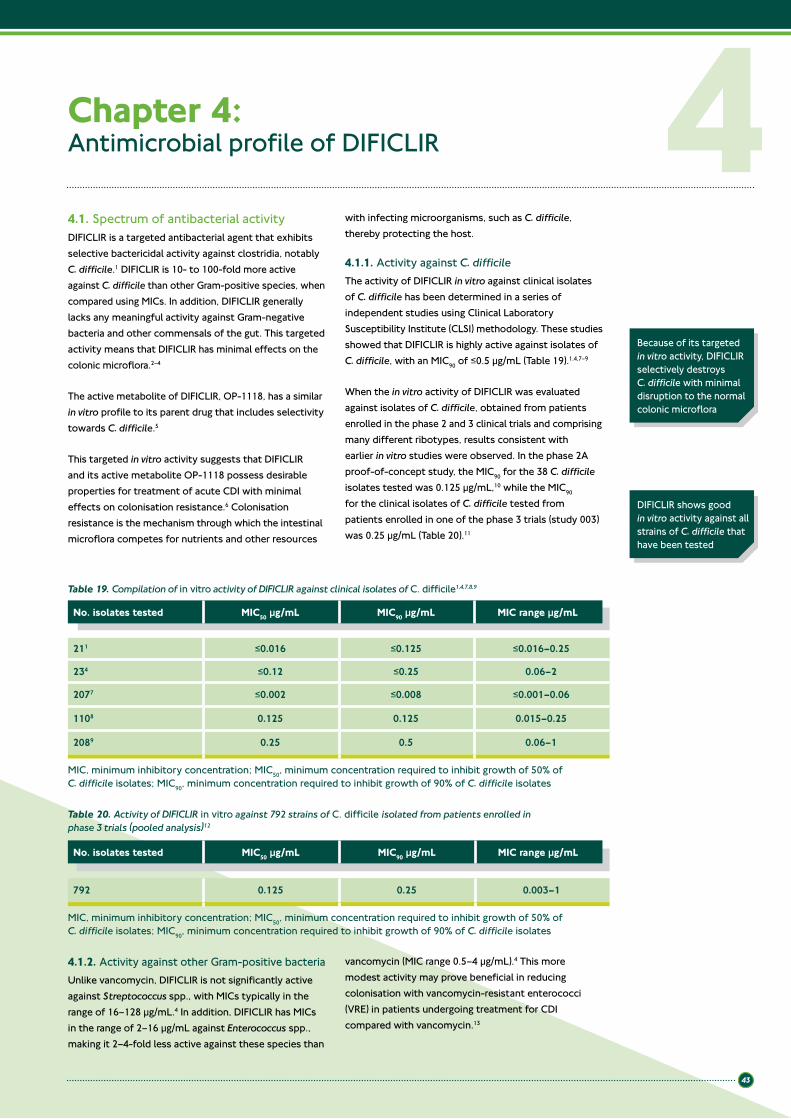
43
Chapter 4: Antimicrobial profile of DIFICLIR
4.1. Spectrum of antibacterial activityDIFICLIR is a targeted antibacterial agent that exhibits selective bactericidal activity against clostridia, notably C. difficile.1 DIFICLIR is 10- to 100-fold more active against C. difficile than other Gram-positive species, when compared using MICs. In addition, DIFICLIR generally lacks any meaningful activity against Gram-negative bacteria and other commensals of the gut. This targeted activity means that DIFICLIR has minimal effects on the colonic microflora.2–4
The active metabolite of DIFICLIR, OP-1118, has a similar in vitro profile to its parent drug that includes selectivity towards C. difficile.5
This targeted in vitro activity suggests that DIFICLIR and its active metabolite OP-1118 possess desirable properties for treatment of acute CDI with minimal effects on colonisation resistance.6 Colonisation resistance is the mechanism through which the intestinal microflora competes for nutrients and other resources
with infecting microorganisms, such as C. difficile, thereby protecting the host.
4.1.1. Activity against C. difficileThe activity of DIFICLIR in vitro against clinical isolates of C. difficile has been determined in a series of independent studies using Clinical Laboratory Susceptibility Institute (CLSI) methodology. These studies showed that DIFICLIR is highly active against isolates of C. difficile, with an MIC90 of ≤0.5 µg/mL (Table 19).1,4,7–9
When the in vitro activity of DIFICLIR was evaluated against isolates of C. difficile, obtained from patients enrolled in the phase 2 and 3 clinical trials and comprising many different ribotypes, results consistent with earlier in vitro studies were observed. In the phase 2A proof-of-concept study, the MIC90 for the 38 C. difficile isolates tested was 0.125 µg/mL,10 while the MIC90 for the clinical isolates of C. difficile tested from patients enrolled in one of the phase 3 trials (study 003) was 0.25 µg/mL (Table 20).11
4Because of its targeted in vitro activity, DIFICLIR selectively destroys C. difficile with minimal disruption to the normal colonic microflora
4.1.2. Activity against other Gram-positive bacteriaUnlike vancomycin, DIFICLIR is not significantly active against Streptococcus spp., with MICs typically in the range of 16–128 µg/mL.4 In addition, DIFICLIR has MICs in the range of 2–16 µg/mL against Enterococcus spp., making it 2–4-fold less active against these species than
vancomycin (MIC range 0.5–4 µg/mL).4 This more modest activity may prove beneficial in reducing colonisation with vancomycin-resistant enterococci (VRE) in patients undergoing treatment for CDI compared with vancomycin.13
DIFICLIR shows good in vitro activity against all strains of C. difficile that have been tested
Table 19. Compilation of in vitro activity of DIFICLIR against clinical isolates of C. difficile1,4,7,8,9
No. isolates tested MIC50 µg/mL MIC90 µg/mL MIC range µg/mL
211 ≤0.016 ≤0.125 ≤0.016–0.25
234 ≤0.12 ≤0.25 0.06–2
2077 ≤0.002 ≤0.008 ≤0.001–0.06
1108 0.125 0.125 0.015–0.25
2089 0.25 0.5 0.06–1
MIC, minimum inhibitory concentration; MIC50, minimum concentration required to inhibit growth of 50% of C. difficile isolates; MIC90, minimum concentration required to inhibit growth of 90% of C. difficile isolates
Table 20. Activity of DIFICLIR in vitro against 792 strains of C. difficile isolated from patients enrolled in phase 3 trials (pooled analysis)12
No. isolates tested MIC50 µg/mL MIC90 µg/mL MIC range µg/mL
792 0.125 0.25 0.003–1
MIC, minimum inhibitory concentration; MIC50, minimum concentration required to inhibit growth of 50% of C. difficile isolates; MIC90, minimum concentration required to inhibit growth of 90% of C. difficile isolates

44
Treatment with DIFICLIR may reduce acquisition of VRE compared with vancomycin
VancomycinDIFICLIR
Patie
nts
who
acq
uire
d VR
E (%
)
p<0.001
7%
33%
50
40
30
20
10
0
Figure 13. Comparative effects of DIFICLIR and vancomycin on acquisition of VRE13
VRE, vancomycin-resistant enterococci
Figure 14. Colonic levels of B. fragilis before (Day 0) and after treatment (Day 10) with DIFICLIR or vancomycin3
VancomycinDIFICLIR
Day 0 Day 10M
ean
CFU
per
gra
m o
f fae
ces
7.0 7.37.4
3.6
1 ¶ 1010
1 ¶ 108
1 ¶ 106
1 ¶ 104
1 ¶ 102
0
CFU, colony forming units
4.1.4. Activity against Gram-negative bacteriaSusceptibility studies in vitro show that DIFICLIR has very little activity against Gram-negative bacteria, with MIC90 values generally >128 µg/mL for a range of species that include important constituents of the normal colonic microflora, such as Bacteroides fragilis.1,4 These in vitro results are supported by data from clinical studies in which stool samples from patients treated with either DIFICLIR or vancomycin were subject to quantitative culture post-treatment. In the first study, in which B. fragilis was used as a marker of the anaerobic microflora, both drugs were effective in reducing C. difficile load. However, while vancomycin also had a markedly suppressive effect on levels of B. fragilis, treatment with DIFICLIR across a range of doses had no significant effect on levels of B. fragilis in faecal samples (Figure 14).3
In the second study, again in contrast to vancomycin, there were no significant effects of DIFICLIR on a wide range of colonic microflora that included: Gram-positive commensals (including members of clostridial clusters XIV and IV [common commensal clostridial] and bifidobacteria) and to Gram-negative organisms (such as the Enterobacteriaceae).2
Overall, these findings provide strong evidence that DIFICLIR causes minimal disruption to the colonic microflora when used as a treatment for CDI.
4.2. Pharmacodynamic effects of DIFICLIR in vitroDIFICLIR is a locally acting drug that cannot be used to treat systemic infections.14 As a result, the establishment of a clinical breakpoint is not relevant. Antibacterial susceptibility testing does not give a clear picture of the activity of DIFICLIR against C. difficile at the site of infection and is of limited clinical utility.
DIFICLIR exhibits bactericidal activity against C. difficile and also has a long post-antibiotic effect (PAE).15,16 This is in contrast to vancomycin, which is only bacteriostatic against C. difficile and has little or no PAE.17
4.1.3. Low risk of acquisition of VREA subgroup analysis of 302 CDI patients enrolled in the phase 3 trial of DIFICLIR, 248 of whom had a negative VRE stool sample upon entering the trial, showed that only 7% of patients treated with DIFICLIR acquired VRE compared with 33% of the vancomycin-treated patients (p<0.001) (Figure 13).13
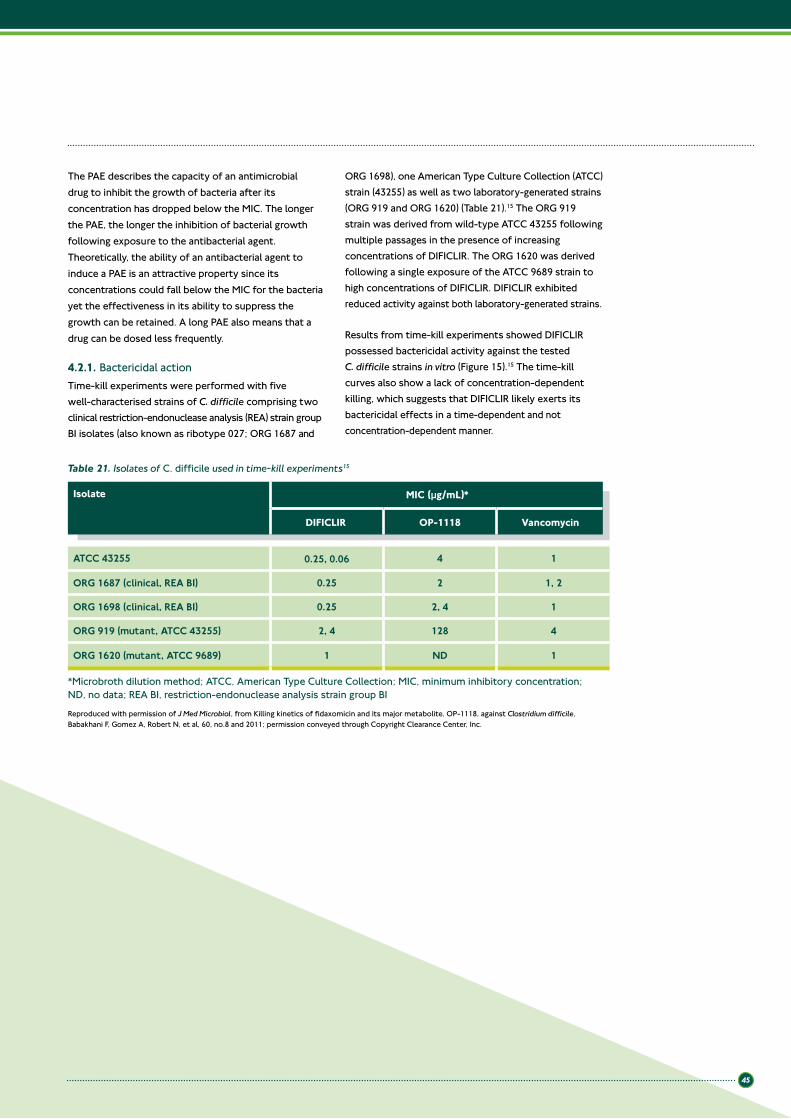
45
The PAE describes the capacity of an antimicrobial drug to inhibit the growth of bacteria after its concentration has dropped below the MIC. The longer the PAE, the longer the inhibition of bacterial growth following exposure to the antibacterial agent. Theoretically, the ability of an antibacterial agent to induce a PAE is an attractive property since its concentrations could fall below the MIC for the bacteria yet the effectiveness in its ability to suppress the growth can be retained. A long PAE also means that a drug can be dosed less frequently.
4.2.1. Bactericidal actionTime-kill experiments were performed with five well-characterised strains of C. difficile comprising two clinical restriction-endonuclease analysis (REA) strain group BI isolates (also known as ribotype 027; ORG 1687 and
ORG 1698), one American Type Culture Collection (ATCC) strain (43255) as well as two laboratory-generated strains (ORG 919 and ORG 1620) (Table 21).15 The ORG 919 strain was derived from wild-type ATCC 43255 following multiple passages in the presence of increasing concentrations of DIFICLIR. The ORG 1620 was derived following a single exposure of the ATCC 9689 strain to high concentrations of DIFICLIR. DIFICLIR exhibited reduced activity against both laboratory-generated strains.
Results from time-kill experiments showed DIFICLIR possessed bactericidal activity against the tested C. difficile strains in vitro (Figure 15).15 The time-kill curves also show a lack of concentration-dependent killing, which suggests that DIFICLIR likely exerts its bactericidal effects in a time-dependent and not concentration-dependent manner.
Table 21. Isolates of C. difficile used in time-kill experiments15
Isolate MIC (µg/mL)*
DIFICLIR OP-1118 Vancomycin
ATCC 43255 0.25, 0.06 4 1
ORG 1687 (clinical, REA BI) 0.25 2 1, 2
ORG 1698 (clinical, REA BI) 0.25 2, 4 1
ORG 919 (mutant, ATCC 43255) 2, 4 128 4
ORG 1620 (mutant, ATCC 9689) 1 ND 1
*Microbroth dilution method; ATCC, American Type Culture Collection; MIC, minimum inhibitory concentration; ND, no data; REA BI, restriction-endonuclease analysis strain group BI
Reproduced with permission of J Med Microbiol, from Killing kinetics of fidaxomicin and its major metabolite, OP-1118, against Clostridium difficile, Babakhani F, Gomez A, Robert N, et al, 60, no.8 and 2011; permission conveyed through Copyright Clearance Center, Inc.
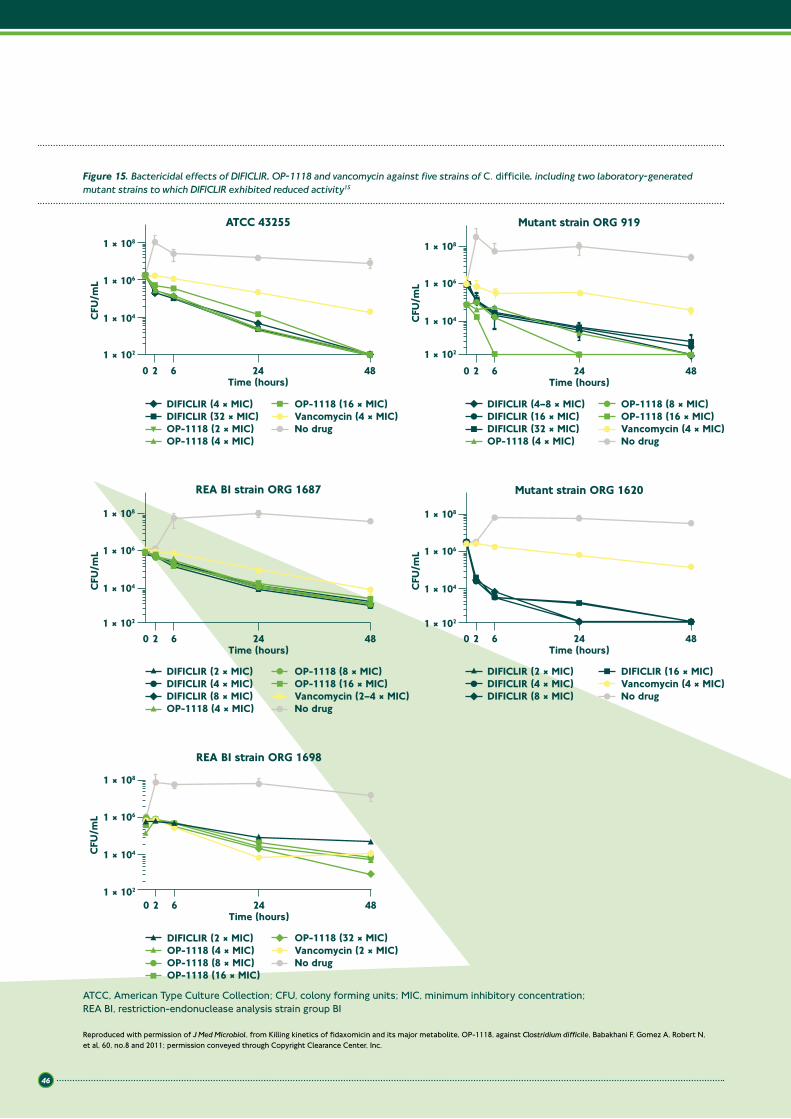
46
1 ¶ 108
1 ¶ 104
1 ¶ 102
1 ¶ 106
CFU
/mL
1 ¶ 108
1 ¶ 104
1 ¶ 102
20 6 24Time (hours)
48
1 ¶ 106
ATCC 43255
DIFICLIR (4 ¶ MIC)
CFU
/mL
20 6 24Time (hours)
48
REA BI strain ORG 1687
Vancomycin (2–4 ¶ MIC)
CFU
/mL
1 ¶ 108
1 ¶ 104
1 ¶ 102
20 6 24Time (hours)
48
1 ¶ 106
Mutant strain ORG 919
CFU
/mL
1 ¶ 108
1 ¶ 104
1 ¶ 102
20 6 24Time (hours)
48
1 ¶ 106
Mutant strain ORG 1620
DIFICLIR (16 ¶ MIC)
Vancomycin (4 ¶ MIC)DIFICLIR (4–8 ¶ MIC)DIFICLIR (16 ¶ MIC)DIFICLIR (32 ¶ MIC)
No drug
No drugNo drugVancomycin (4 ¶ MIC)
DIFICLIR (2 ¶ MIC)DIFICLIR (4 ¶ MIC)DIFICLIR (8 ¶ MIC)
DIFICLIR (2 ¶ MIC)DIFICLIR (4 ¶ MIC)DIFICLIR (8 ¶ MIC)
1 ¶ 108
1 ¶ 104
1 ¶ 102
1 ¶ 106
CFU
/mL
20 6 24Time (hours)
48
REA BI strain ORG 1698
DIFICLIR (2 ¶ MIC)OP-1118 (4 ¶ MIC)OP-1118 (8 ¶ MIC)OP-1118 (16 ¶ MIC)
OP-1118 (32 ¶ MIC)Vancomycin (2 ¶ MIC)No drug
OP-1118 (2 ¶ MIC)
OP-1118 (16 ¶ MIC)
OP-1118 (8 ¶ MIC)
OP-1118 (4 ¶ MIC)
OP-1118 (8 ¶ MIC)
OP-1118 (4 ¶ MIC)
DIFICLIR (32 ¶ MIC)
OP-1118 (4 ¶ MIC)
OP-1118 (16 ¶ MIC)
OP-1118 (16 ¶ MIC) Vancomycin (4 ¶ MIC)No drug
Figure 15. Bactericidal effects of DIFICLIR, OP-1118 and vancomycin against five strains of C. difficile, including two laboratory-generated mutant strains to which DIFICLIR exhibited reduced activity15
Reproduced with permission of J Med Microbiol, from Killing kinetics of fidaxomicin and its major metabolite, OP-1118, against Clostridium difficile, Babakhani F, Gomez A, Robert N, et al, 60, no.8 and 2011; permission conveyed through Copyright Clearance Center, Inc.
ATCC, American Type Culture Collection; CFU, colony forming units; MIC, minimum inhibitory concentration; REA BI, restriction-endonuclease analysis strain group BI
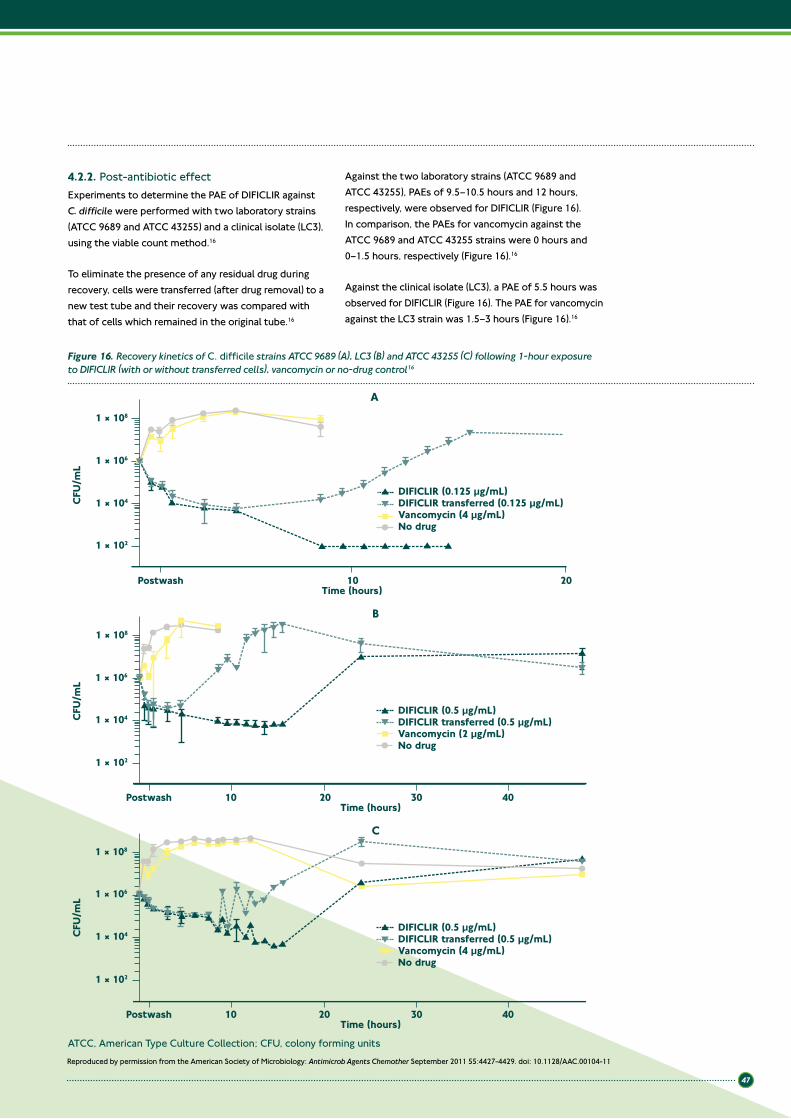
47
Figure 16. Recovery kinetics of C. difficile strains ATCC 9689 (A), LC3 (B) and ATCC 43255 (C) following 1-hour exposure to DIFICLIR (with or without transferred cells), vancomycin or no-drug control16
DIFICLIR (0.5 µg/mL)DIFICLIR transferred (0.5 µg/mL)Vancomycin (2 µg/mL)No drug
DIFICLIR (0.125 µg/mL)DIFICLIR transferred (0.125 µg/mL)Vancomycin (4 µg/mL)No drug
CFU
/mL
Time (hours)
1 ¶ 102
1 ¶ 104
1 ¶ 106
1 ¶ 108
Postwash 10 20
A
B
CFU
/mL
Time (hours)
1 ¶ 102
1 ¶ 104
1 ¶ 106
1 ¶ 108
Postwash 10 20 30 40
DIFICLIR (0.5 µg/mL)DIFICLIR transferred (0.5 µg/mL)Vancomycin (4 µg/mL)No drug
C
CFU
/mL
Time (hours)
1 ¶ 102
1 ¶ 104
1 ¶ 106
1 ¶ 108
Postwash 10 20 30 40
Reproduced by permission from the American Society of Microbiology: Antimicrob Agents Chemother September 2011 55:4427-4429. doi: 10.1128/ AAC.00104-11
4.2.2. Post-antibiotic effectExperiments to determine the PAE of DIFICLIR against C. difficile were performed with two laboratory strains (ATCC 9689 and ATCC 43255) and a clinical isolate (LC3), using the viable count method.16
To eliminate the presence of any residual drug during recovery, cells were transferred (after drug removal) to a new test tube and their recovery was compared with that of cells which remained in the original tube.16
Against the two laboratory strains (ATCC 9689 and ATCC 43255), PAEs of 9.5–10.5 hours and 12 hours, respectively, were observed for DIFICLIR (Figure 16). In comparison, the PAEs for vancomycin against the ATCC 9689 and ATCC 43255 strains were 0 hours and 0–1.5 hours, respectively (Figure 16).16
Against the clinical isolate (LC3), a PAE of 5.5 hours was observed for DIFICLIR (Figure 16). The PAE for vancomycin against the LC3 strain was 1.5–3 hours (Figure 16).16
ATCC, American Type Culture Collection; CFU, colony forming units

48
The long PAE observed for DIFICLIR against C. difficile may translate into clinical benefits in patients with CDI. Due to the rapid transit time in the bowel associated with severe diarrhoea there is a risk that a drug is eliminated from the bowel before the next dose is given. Antibacterials with a prolonged PAE may have the potential to provide antibacterial activity against C. difficile even in the absence of therapeutic concentrations and so may offer protection between doses. A prolonged PAE may also permit less frequent dosing.
4.2.3. Inhibition of C. difficile sporulation and toxin productionThe effects of DIFICLIR and vancomycin on C. difficile spore and toxin production have been evaluated. Recrudescence of C. difficile vegetative and/or spore
counts and re-expression of cytotoxin following treatment were compared in patients enrolled in a phase 2 study of DIFICLIR.3 Analysis of faecal samples from treated patients showed that while both treatments were effective at reducing C. difficile load, DIFICLIR was significantly more effective at inhibiting spore production than vancomycin (p=0.03). Re-expression of C. difficile cytotoxin B also occurred in significantly fewer patients treated with DIFICLIR than among vancomycin recipients (1/27 vs. 3/8, respectively; p=0.03).
In another study, DIFICLIR was shown to inhibit spore production by the C. difficile strain ATCC 43255 in vitro (Figure 17).18 In contrast, the comparator drug, vancomycin, had no discernable effect on spore production.
DIFICLIR kills C. difficile vegetative cells and inhibits spore and toxin production
Figure 17. Effect of exposure to DIFICLIR and vancomycin on sporulation by C. difficile strain ATCC 4325518
3
1 ¶ 103
1 ¶ 105
Detection limit
Drug added
1 ¶ 107
1 ¶ 109
23 48 72 96 120Time (hours)
DIFICLIR (1/4 ¶ MIC)Vancomycin (1/4 ¶ MIC)Control (no drug)
Spor
e CF
U/m
L
144 168 192 216
CFU, colony forming units; MIC, minimum inhibitory concentration
Reproduced with permission
Studies in vitro have also demonstrated that exposure to DIFICLIR can suppress production of C. difficile toxins A and B.19 Sub-MIC concentrations of DIFICLIR, its metabolite OP-1118 and vancomycin were added to C. difficile ATCC 43255 (a high-level toxin-producing strain) at the early stationary phase of growth. The cultures were then incubated for a period of at least 1 week. At different time intervals, samples were collected for quantification of secreted toxin A and B
levels in culture supernatants using a commercial enzyme immunoassay. Exposure to DIFICLIR resulted in marked, dose-dependent suppression of C. difficile toxin production (Table 22). By contrast, the results for vancomycin were no different to the untreated controls. Further investigations have found that in contrast to vancomycin, DIFICLIR and its metabolite OP-1118 inhibit the expression of the genes responsible for toxin production and sporulation.20
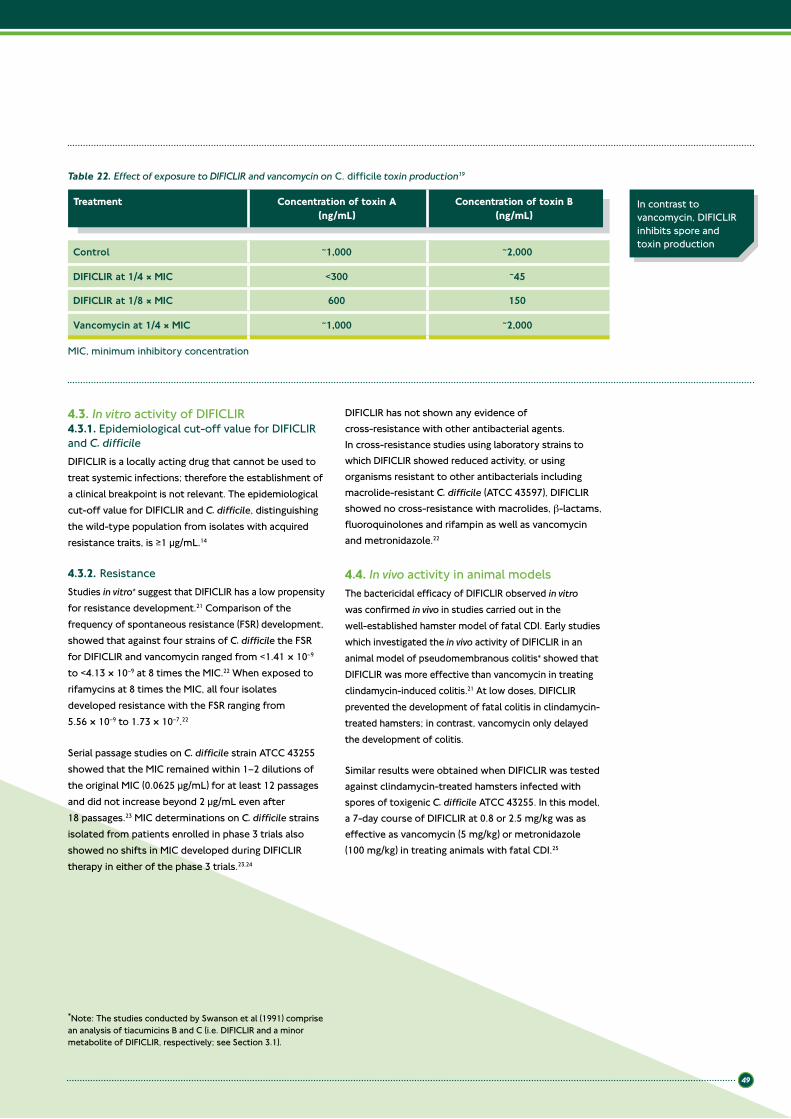
49
4.3. In vitro activity of DIFICLIR4.3.1. Epidemiological cut-off value for DIFICLIR and C. difficileDIFICLIR is a locally acting drug that cannot be used to treat systemic infections; therefore the establishment of a clinical breakpoint is not relevant. The epidemiological cut-off value for DIFICLIR and C. difficile, distinguishing the wild-type population from isolates with acquired resistance traits, is ≥1 µg/mL.14
4.3.2. ResistanceStudies in vitro* suggest that DIFICLIR has a low propensity for resistance development.21 Comparison of the frequency of spontaneous resistance (FSR) development, showed that against four strains of C. difficile the FSR for DIFICLIR and vancomycin ranged from <1.41 × 10–9 to <4.13 × 10–9 at 8 times the MIC.22 When exposed to rifamycins at 8 times the MIC, all four isolates developed resistance with the FSR ranging from 5.56 × 10–9 to 1.73 × 10–7.22
Serial passage studies on C. difficile strain ATCC 43255 showed that the MIC remained within 1–2 dilutions of the original MIC (0.0625 µg/mL) for at least 12 passages and did not increase beyond 2 µg/mL even after 18 passages.23 MIC determinations on C. difficile strains isolated from patients enrolled in phase 3 trials also showed no shifts in MIC developed during DIFICLIR therapy in either of the phase 3 trials.23,24
DIFICLIR has not shown any evidence of cross-resistance with other antibacterial agents. In cross-resistance studies using laboratory strains to which DIFICLIR showed reduced activity, or using organisms resistant to other antibacterials including macrolide-resistant C. difficile (ATCC 43597), DIFICLIR showed no cross-resistance with macrolides, β-lactams, fluoroquinolones and rifampin as well as vancomycin and metronidazole.22
4.4. In vivo activity in animal modelsThe bactericidal efficacy of DIFICLIR observed in vitro was confirmed in vivo in studies carried out in the well-established hamster model of fatal CDI. Early studies which investigated the in vivo activity of DIFICLIR in an animal model of pseudomembranous colitis* showed that DIFICLIR was more effective than vancomycin in treating clindamycin-induced colitis.21 At low doses, DIFICLIR prevented the development of fatal colitis in clindamycin-treated hamsters; in contrast, vancomycin only delayed the development of colitis.
Similar results were obtained when DIFICLIR was tested against clindamycin-treated hamsters infected with spores of toxigenic C. difficile ATCC 43255. In this model, a 7-day course of DIFICLIR at 0.8 or 2.5 mg/kg was as effective as vancomycin (5 mg/kg) or metronidazole (100 mg/kg) in treating animals with fatal CDI.25
Table 22. Effect of exposure to DIFICLIR and vancomycin on C. difficile toxin production19
Treatment Concentration of toxin A(ng/mL)
Concentration of toxin B(ng/mL)
Control ~1,000 ~2,000
DIFICLIR at 1/4 ¶ MIC <300 ~45
DIFICLIR at 1/8 ¶ MIC 600 150
Vancomycin at 1/4 ¶ MIC ~1,000 ~2,000
In contrast to vancomycin, DIFICLIR inhibits spore and toxin production
*Note: The studies conducted by Swanson et al (1991) comprise an analysis of tiacumicins B and C (i.e. DIFICLIR and a minor metabolite of DIFICLIR, respectively; see Section 3.1).
MIC, minimum inhibitory concentration

50
4.5. Summary
Key points
• DIFICLIR is a novel Gram-positive antibacterial agent with targeted activity against C. difficile and a minimal impact on the normal colonic microflora
• DIFICLIR is effective against all ribotypes of C. difficile tested with MIC90 values <1 µg/mL
• DIFICLIR exerts bactericidal activity against C. difficile in a time-dependent manner
• DIFICLIR is a locally acting drug that cannot be used to treat systemic infections
• DIFICLIR has a prolonged PAE resulting in antibacterial activity that persists at sub-therapeutic levels. This may be beneficial in CDI, a disease in which rapid intestinal transit due to diarrhoea may hasten faecal drug elimination
• DIFICLIR kills C. difficile vegetative cells and inhibits spore and toxin production
• DIFICLIR is significantly more effective than vancomycin at inhibiting C. difficile spore and toxin production in vitro
• DIFICLIR has a low propensity for resistance development and displays no cross-resistance with existing classes of antibacterial agents
• Treatment with DIFICLIR may reduce acquisition of VRE compared with vancomycin
• In vivo models show that DIFICLIR is effective in treating CDI.
4.6. References1. Credito KL, Appelbaum PC. Activity of OPT-80, a novel
macrocycle, compared with those of eight other agents against selected anaerobic species. Antimicrob Agents Chemother 2004;48:4430–4.
2. Tannock GW, Munro K, Taylor C, et al. A new macrocyclic antibiotic, DIFICLIR (OPT 80), causes less alteration to the bowel microbiota of Clostridium difficile-infected patients than does vancomycin. Microbiology 2010;156:3354–9.
3. Louie TJ, Emery J, Krulicki W, et al. OPT-80 Eliminates Clostridium difficile and is sparing of Bacteroides species during treatment of C. difficile infection. Antimicrob Agents Chemother 2009;53:261–3.
4. Finegold SM, Molitoris D, Vaisanen ML, et al. In vitro activities of OPT-80 and comparator drugs against intestinal bacteria. Antimicrob Agents Chemother 2004;48:4898–902.
5. Babakhani FK, Seddon J, Robert N, et al. Narrow spectrum activity and low fecal protein binding of OPT-80 and its major hydrolysis metabolite (OP-1118). Abstract presented at the Annual Interscience Conference on Antimicrobial Agents and Chemotherapy, 17–20 September 2007; Chicago, IL, USA. Abstract E-2076.
6. Sullivan KM, Spooner LM. DIFICLIR: A macrocyclic antibiotic for the management of Clostridium difficile infection. Ann Pharamacother 2010;44:352–9.
7. Ackermann G, Loffler B, Adler D, et al. In vitro activity of OPT-80 against Clostridium difficile. Antimicrob Agents Chemother 2004;48:2280–2.
8. Hecht DW, Galang MA, Sambol SP, et al. In vitro activities of 15 antimicrobial agents against 110 toxigenic Clostridium difficile clinical isolates collected from 1983 to 2004. Antimicrob Agents Chemother 2007;51:2716–9.
9. Karlowsky JA, Laing NM, Zhanel GG. In vitro activity of OPT-80 tested against clinical isolates of toxin-producing Clostridium difficile. Antimicrob Agents Chemother 2008;52:4163–5.
10. Citron D, Babakhani F, Goldstein EJC, et al. Typing and susceptibility of bacterial isolates from the DIFICLIR (OPT-80) phase II study for C. difficile infection. Anaerobe 2009;15:234–6.
11. Goldstein EJC, Citron DM, Sears P, et al. Comparative fidaxomicin susceptibilities of isolates collected at baseline, failure, and recurrence from subjects in a phase III trial of Clostridium difficile infection (CDI). Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 12–15 September 2009; San Francisco, CA, USA. Abstract L1-1641.
12. Astellas Pharma Europe Ltd. Data on file, FDX/11/0008/EU.
13. Nerandzic MM, Mullane K, Miller M, et al. Acquisition and overgrowth of vancomycin-resistant enterococci in patients treated with either DIFICLIR or vancomycin for C. difficile infection. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 12–15 September 2009; San Francisco, CA, USA. Abstract K-1915.
14. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
15. Babakhani F, Gomez A, Robert N, et al. Killing kinetics of fidaxomicin and its major metabolite, OP-1118, against Clostridium difficile. J Med Microbiol 2011;60:1213–7.
16. Babakhani F, Gomez A, Robert N, et al. Postantibiotic effect of fidaxomicin and its major metabolite, OP-1118, against Clostridium difficile. Antimicrob Agents Chemother 2011;55:4427–9.

51
17. Odenholt I, Walder M, Wullt M. Pharmacodynamic studies of vancomycin, metronidazole and fusidic acid against Clostridium difficile. Chemotherapy 2007;53:267–74.
18. Gomez A, Sears P, Nguyen L, et al. Fidaxomicin inhibits spore production in C. difficile 027/NAP1/BI. Poster presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Poster C1-632.
19. Sims C, Gomez A, Sears P, et al. Fidaxomicin inhibits production of toxin A and toxin B in C. difficile. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-634.
20. Bouillaut L, Babakhani F, Sonenshein A. Inhibition of Clostridium difficile toxin synthesis and sporulation by fidaxomicin. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-635.
21. Swanson RN, Hardy DJ, Shipkowitz NL, et al. In vitro and in vivo evaluation of tiacumicins B and C against Clostridium difficile. Antimicrob Agents Chemother 1991;35:1108–11.
22. Astellas Pharma Europe Ltd. Data on file, FDX/11/0024/EU.
23. Astellas Pharma Europe Ltd. Data on file, FDX/11/0009/EU.
24. Louie TJ, Miller MA, Mullane KM, et al. DIFICLIR versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
25. Astellas Pharma Europe Ltd. Data on file, FDX/11/0010/EU.

52

53
Chapter 5: Use, posology and administration
5.1. IndicationDIFICLIR is indicated in adults for the treatment of Clostridium difficile infections (CDI), also known as C. difficile-associated diarrhoea (CDAD).1
Consideration should be given to official guidelines on the appropriate use of antibacterial agents.
5.2. Posology and method of administrationDIFICLIR for oral administration is supplied as capsule-shaped, film-coated tablets containing 200 mg fidaxomicin.1
For adult and elderly (i.e. aged ≥65 years) patients, the recommended dose is 200 mg (one tablet) administered twice daily (once every 12 hours) for 10 days.1 Patients enrolled in the phase 2A proof-of-concept study experienced the highest rates of clinical cure with this dose regimen (compared with 50 mg and 100 mg bid) and also tolerated this dose well.2
5.3. Use in specific patient populations5.3.1. Pregnancy and breastfeedingThere are no data available regarding the use of DIFICLIR in pregnant women. Animal studies did not indicate any direct or indirect harmful effects with respect to reproductive toxicity. As a precautionary measure, it is preferable to avoid the use of DIFICLIR during pregnancy.1
It is unknown if DIFICLIR and its metabolites are excreted in human milk. Although no effects on breastfed newborns/infants are anticipated since the systemic exposure to DIFICLIR is low, a risk to newborns/infants cannot be excluded. A decision must be made whether to discontinue breastfeeding or to discontinue/abstain from DIFICLIR therapy, taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.1
5.3.2. Paediatric populationThe safety and efficacy of DIFICLIR in children aged below 18 years has not yet been established. No data are available.1
5.3.3. Elderly patients (aged ≥65 years)Despite greater exposures in elderly patients (i.e. those aged ≥65 years), DIFICLIR and OP-1118 plasma concentrations remained in the nanogram range. No dose adjustment is therefore considered necessary for patients aged ≥65 years.1
5.3.4. Renal impairmentNo dose adjustment is considered necessary in patients with renal impairment. Due to the limited clinical data in patients with severe renal impairment, DIFICLIR should be used with caution in this population.1
5.3.5. Hepatic impairmentNo dose adjustment is considered necessary in patients with hepatic impairment. Due to the limited clinical data in patients with moderate-to-severe hepatic impairment, DIFICLIR should be used with caution in this population.1
5.4. OverdoseNo cases of acute overdose have been reported in humans.1
5.5. References1. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary
of Product Characteristics, 19 December 2011.
2. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety, and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
5With only twice-daily oral dosing, DIFICLIR offers a more convenient treatment regimen compared with current standard therapies

54

55
Chapter 6: Clinical efficacy of DIFICLIR in CDI 66.1. Overview of phase 2A proof-of-concept studyEvidence of the efficacy of DIFICLIR in the treatment of CDI was first demonstrated in a phase 2A proof-of-concept study. In this open-label study, 48 subjects
meeting eligibility criteria (Table 23) were randomised to DIFICLIR at doses of 50 mg bid, 100 mg bid and 200 mg bid. Study medication, administered orally, was given every 12 hours for 10 consecutive days.1
The efficacy of DIFICLIR in this phase 2A proof-of-concept study was determined at the end of treatment in the modified intent-to-treat (mITT) population, which consisted of all randomised patients who had received at least one dose of study medication.1 Outcome measures included clinical assessment at end of treatment and recurrence of CDI among cured patients 6 weeks after the end of therapy (Table 24).
The study population was representative of patients infected with C. difficile, with the mean number of daily bowel movements being 6.7 ± 2.79.1
All patients had positive assay results for C. difficile toxin together with signs and symptoms consistent with infection such as elevated white blood cell (WBC) counts, elevated body temperature, and abdominal discomfort. Of the 48 patients entered into this study, 41 completed the study. All patients in the highest dose treatment group (200 mg bid) completed the study compared with 88% (14/16) and 94% (15/16) in the 50 mg bid and 100 mg bid groups, respectively. Treatment failure was the most common reason for study withdrawal and defined as the need for additional therapy during the treatment period.1
Inclusion criteria
• Adults (≥18 years)• Inpatient or outpatient• Confirmed diagnosis of CDI
o Diarrhoea defined as change in bowel habits with either ≥3 UBM in a 24-hour period or ≥6 UBM in a 36-hour period
o Presence of C. difficile toxins A or B in stool• Primary episode or first recurrence of CDI
Exclusion criteria
• >12 UBM/day• Vomiting• Presence of ileus• Abdominal tenderness• WBC >30 × 109/L• >1 recurrence or relapse within 3 months• Need for concurrent antibacterial therapy• Crohn’s disease or ulcerative colitis• Toxic megacolon• Potentially life-threatening CDI
Table 23. Inclusion criteria in the open-label phase 2A proof-of-concept study1
UBM, unformed bowel movements; WBC, white blood cell
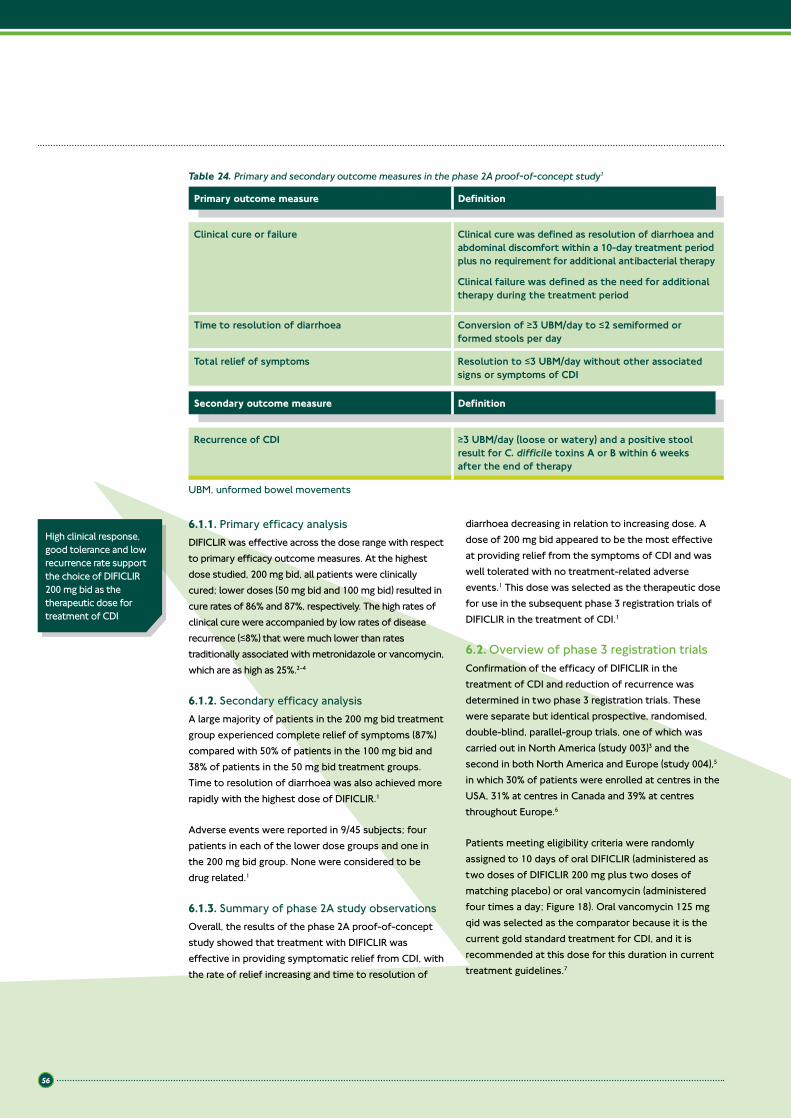
56
6.1.1. Primary efficacy analysisDIFICLIR was effective across the dose range with respect to primary efficacy outcome measures. At the highest dose studied, 200 mg bid, all patients were clinically cured; lower doses (50 mg bid and 100 mg bid) resulted in cure rates of 86% and 87%, respectively. The high rates of clinical cure were accompanied by low rates of disease recurrence (≤8%) that were much lower than rates traditionally associated with metronidazole or vancomycin, which are as high as 25%.2–4
6.1.2. Secondary efficacy analysisA large majority of patients in the 200 mg bid treatment group experienced complete relief of symptoms (87%) compared with 50% of patients in the 100 mg bid and 38% of patients in the 50 mg bid treatment groups. Time to resolution of diarrhoea was also achieved more rapidly with the highest dose of DIFICLIR.1
Adverse events were reported in 9/45 subjects; four patients in each of the lower dose groups and one in the 200 mg bid group. None were considered to be drug related.1
6.1.3. Summary of phase 2A study observationsOverall, the results of the phase 2A proof-of-concept study showed that treatment with DIFICLIR was effective in providing symptomatic relief from CDI, with the rate of relief increasing and time to resolution of
diarrhoea decreasing in relation to increasing dose. A dose of 200 mg bid appeared to be the most effective at providing relief from the symptoms of CDI and was well tolerated with no treatment-related adverse events.1 This dose was selected as the therapeutic dose for use in the subsequent phase 3 registration trials of DIFICLIR in the treatment of CDI.1
6.2. Overview of phase 3 registration trialsConfirmation of the efficacy of DIFICLIR in the treatment of CDI and reduction of recurrence was determined in two phase 3 registration trials. These were separate but identical prospective, randomised, double-blind, parallel-group trials, one of which was carried out in North America (study 003)3 and the second in both North America and Europe (study 004),5 in which 30% of patients were enrolled at centres in the USA, 31% at centres in Canada and 39% at centres throughout Europe.6
Patients meeting eligibility criteria were randomly assigned to 10 days of oral DIFICLIR (administered as two doses of DIFICLIR 200 mg plus two doses of matching placebo) or oral vancomycin (administered four times a day; Figure 18). Oral vancomycin 125 mg qid was selected as the comparator because it is the current gold standard treatment for CDI, and it is recommended at this dose for this duration in current treatment guidelines.7
Table 24. Primary and secondary outcome measures in the phase 2A proof-of-concept study1
Clinical cure or failure Clinical cure was defined as resolution of diarrhoea and abdominal discomfort within a 10-day treatment period plus no requirement for additional antibacterial therapy
Clinical failure was defined as the need for additional therapy during the treatment period
Time to resolution of diarrhoea Conversion of ≥3 UBM/day to ≤2 semiformed or formed stools per day
Total relief of symptoms Resolution to ≤3 UBM/day without other associated signs or symptoms of CDI
Primary outcome measure Definition
Secondary outcome measure Definition
Recurrence of CDI ≥3 UBM/day (loose or watery) and a positive stool result for C. difficile toxins A or B within 6 weeks after the end of therapy
High clinical response, good tolerance and low recurrence rate support the choice of DIFICLIR 200 mg bid as the therapeutic dose for treatment of CDI
UBM, unformed bowel movements
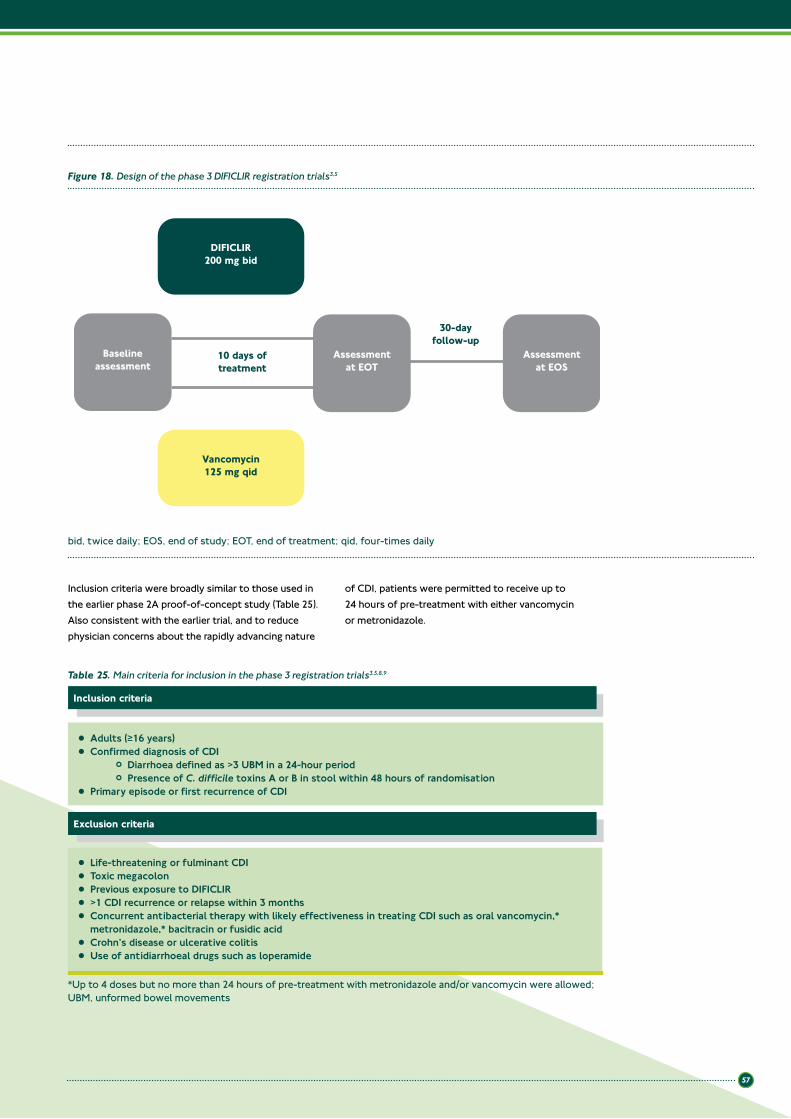
57
Baselineassessment
Assessmentat EOT
Assessmentat EOS
Vancomycin125 mg qid
DIFICLIR200 mg bid
10 days oftreatment
30-dayfollow-up
Figure 18. Design of the phase 3 DIFICLIR registration trials3,5
bid, twice daily; EOS, end of study; EOT, end of treatment; qid, four-times daily
Inclusion criteria were broadly similar to those used in the earlier phase 2A proof-of-concept study (Table 25). Also consistent with the earlier trial, and to reduce physician concerns about the rapidly advancing nature
of CDI, patients were permitted to receive up to 24 hours of pre-treatment with either vancomycin or metronidazole.
Table 25. Main criteria for inclusion in the phase 3 registration trials3,5,8,9
Inclusion criteria
• Adults (≥16 years)• Confirmed diagnosis of CDI
o Diarrhoea defined as >3 UBM in a 24-hour periodo Presence of C. difficile toxins A or B in stool within 48 hours of randomisation
• Primary episode or first recurrence of CDI
Exclusion criteria
• Life-threatening or fulminant CDI• Toxic megacolon• Previous exposure to DIFICLIR• >1 CDI recurrence or relapse within 3 months• Concurrent antibacterial therapy with likely effectiveness in treating CDI such as oral vancomycin,*
metronidazole,* bacitracin or fusidic acid• Crohn’s disease or ulcerative colitis• Use of antidiarrhoeal drugs such as loperamide
*Up to 4 doses but no more than 24 hours of pre-treatment with metronidazole and/or vancomycin were allowed; UBM, unformed bowel movements

58
The trials enrolled a population of predominantly older patients. In study 003, the mean age of patients in the DIFICLIR treatment arm was 60.3 years and in the vancomycin treatment arm the mean age was 62.9 years.3 In study 004, the mean age of patients
in the DIFICLIR treatment arm was 64.3 years and in the vancomycin treatment arm the mean age was 62.5 years (Table 26).5 The proportions of patients with mild, moderate and severe CDI were broadly equal between treatment arms (Table 27).
Table 26. Demographic and baseline clinical characteristics of patients enrolled in the phase 3 registration trials (mITT population)3,5,9
Mean age (SD), years 60.3 (± 16.9) 62.9 (± 16.9) 64.3 (± 17.9) 62.5 (± 18.4)
Female (%) 57.1 54.7 58.7 63.0
Mean number UBM per day (SD) 8.1 (± 4.2) 8.3 (± 5.4) 7.5 (± 4.4) 7.5 (± 4.3)
Inpatient (%) 58.2 60.5 69.0 67.3
Previous metronidazole failure (%) 4.5 5.5 4.8 3.1
Treatment for C. difficile in previous 24 hours (%) 38.3 39.8 38.5 38.1
Previous episode of CDI (%) 16.7 17.5 15.9 14.0
BI/NAP1/027 strain* (%) 37.5 38.6 33.2 33.1
Table 27. Representation of patients in relation to initial CDI severity in the phase 3 registration trials (mITT population)8,9
Mild 64 (22.3) 80 (25.9) 77 (30.6) 95 (37.0)
Moderate 111 (38.7) 106 (34.3) 82 (32.5) 73 (28.4)
Severe 112 (39.0) 123 (39.8) 90 (35.7) 88 (34.2)
Characteristic, n (%) Study 003 Study 004
DIFICLIRN=287
VancomycinN=309
DIFICLIRN=252
VancomycinN=257
Baseline disease severity categories defined as: Mild, 4–5 UBM per day or WBC ≤12,000/mm3; Moderate, 6–9 UBM per day or WBC 12,001–15,000 mm3; Severe, ≥10 UBM per day or WBC ≥15,001/mm3
*Percentages based on numbers of patients with C. difficile isolates that were typed (Study 003, n=415; Study 004, n=377); 027, polymerase chain reaction ribotype 027; BI, restriction-endonuclease analysis group BI strain of C. difficile; NAP1, North American pulsed-field gel electrophoresis type 1 strain of C. difficile; SD, standard deviation; UBM, unformed bowel movements
Reproduced by permission from Massachusetts Medical Society (“MMS”): New England Journal of Medicine, Louie TJ et al. 2001;364:422–31. Copyright 2011
Characteristic Study 003 Study 004
DIFICLIRN=287
VancomycinN=309
DIFICLIRN=252
VancomycinN=257
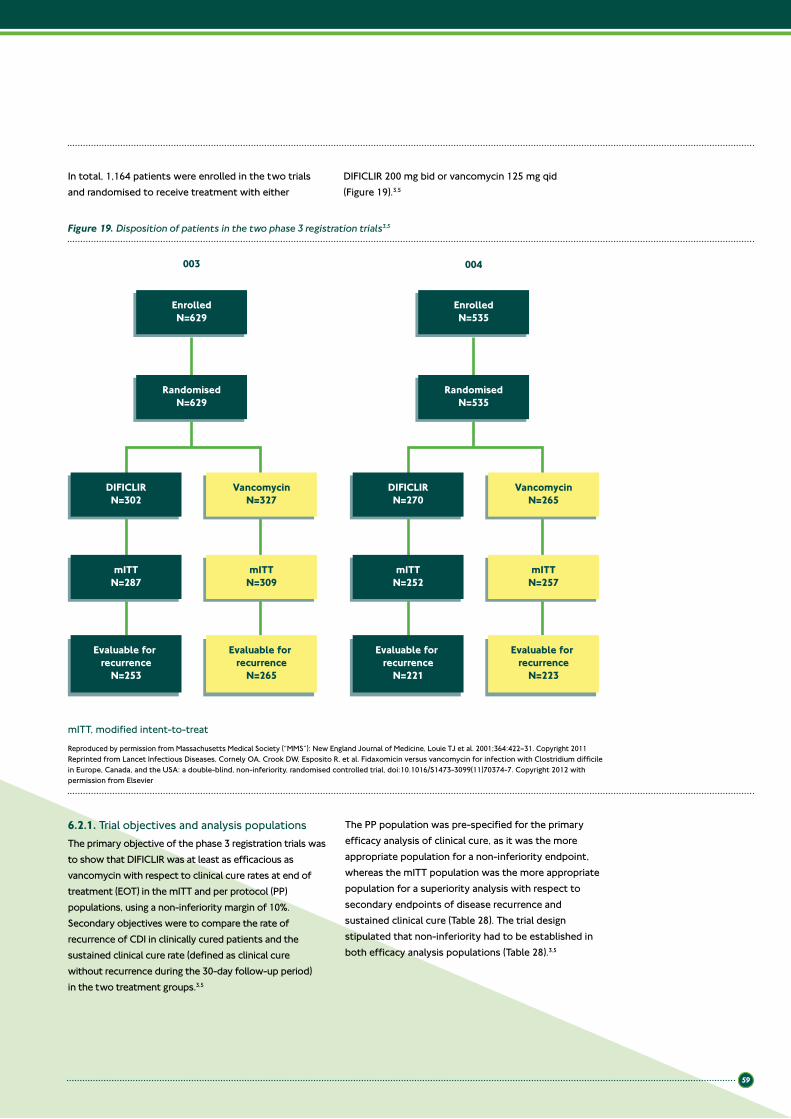
59
In total, 1,164 patients were enrolled in the two trials and randomised to receive treatment with either
DIFICLIR 200 mg bid or vancomycin 125 mg qid (Figure 19).3,5
003 004
EnrolledN=629
RandomisedN=629
DIFICLIRN=302
VancomycinN=327
mITTN=287
mITTN=309
Evaluable for recurrence
N=253
Evaluable for recurrence
N=265
EnrolledN=535
RandomisedN=535
DIFICLIRN=270
VancomycinN=265
mITTN=252
mITTN=257
Evaluable for recurrence
N=221
Evaluable for recurrence
N=223
Figure 19. Disposition of patients in the two phase 3 registration trials3,5
mITT, modified intent-to-treat
Reproduced by permission from Massachusetts Medical Society (“MMS”): New England Journal of Medicine, Louie TJ et al. 2001;364:422–31. Copyright 2011Reprinted from Lancet Infectious Diseases, Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial, doi:10.1016/S1473-3099(11)70374-7. Copyright 2012 with permission from Elsevier
6.2.1. Trial objectives and analysis populationsThe primary objective of the phase 3 registration trials was to show that DIFICLIR was at least as efficacious as vancomycin with respect to clinical cure rates at end of treatment (EOT) in the mITT and per protocol (PP) populations, using a non-inferiority margin of 10%. Secondary objectives were to compare the rate of recurrence of CDI in clinically cured patients and the sustained clinical cure rate (defined as clinical cure without recurrence during the 30-day follow-up period) in the two treatment groups.3,5
The PP population was pre-specified for the primary efficacy analysis of clinical cure, as it was the more appropriate population for a non-inferiority endpoint, whereas the mITT population was the more appropriate population for a superiority analysis with respect to secondary endpoints of disease recurrence and sustained clinical cure (Table 28). The trial design stipulated that non-inferiority had to be established in both efficacy analysis populations (Table 28).3,5

60
Table 28. Definition of efficacy analysis populations and outcome measures in the phase 3 registration trials3,5
mITT Patients with documented CDI who underwent randomisation and received at least one dose of study medication
PP Patients in the mITT population who received at least 3 days study medication in the case of treatment failure or 8 days in the case of clinical cure; had documented adherence to study protocol and underwent EOT evaluation
Study population Definition
Outcome measures
Clinical cure Resolution of diarrhoea (≤3 UBM/day for two consecutive days),with maintenance of resolution for the duration of therapy and no further requirement for therapy from Day 2 following EOT
Recurrence Reappearance of >3 diarrhoeal stools per 24-hour period within 30 days of cessation of therapy, the presence of C. difficile toxins A or B, or both, in stool, and the need for re-treatment for CDI
Time to resolutionof diarrhoea
Time elapsing from start of treatment to resolution of diarrhoea (first of two consecutive days of ≤3 UBM that are sustained through EOT)
Sustained clinical cure Clinical cure without recurrence during the 30-day follow-up period
6.2.2. Primary efficacy analysisBoth studies 003 and 004 met the primary efficacy endpoint of non-inferiority to vancomycin in clinical cure rate at EOT in the mITT and PP populations (Figure 20).3,5 As Figure 20 shows, a similar proportion of patients were cured in both the mITT and PP populations. In the two trials, the 95% confidence intervals of -2.6% and -3.1% for the mITT and PP populations, respectively, for study 0033 and of -4.3% and -4.9%, respectively, for study 0045 were well within the pre-defined non-inferiority margin of 10% (Figure 20).
6.2.3. Secondary efficacy analysisWith respect to the secondary efficacy endpoint of recurrence of CDI following successful treatment of an acute episode of CDI, significantly fewer patients in the DIFICLIR arms of the two trials experienced recurrent CDI within 30 days of the cessation of therapy (Figure 21). Recurrence rates in the DIFICLIR treatment group for the mITT population in studies 003 and 004 were 15.4% and 12.7%, respectively, compared with 25.3% and 26.9%, respectively, for vancomycin.3,5 The combined differences represent a 47% reduction in CDI recurrence (recurrence rates in the pooled PP population: DIFICLIR 13.04%, vancomycin 24.57%),10 which is statistically significant and clinically meaningful.
DIFICLIR has comparable efficacy to vancomycin in the treatment of CDI
DIFICLIR is significantly more effective than vancomycin in reducing recurrence of CDI, achieving a 47% reduction relative to vancomycin (recurrence rates in the pooled PP population: DIFICLIR 13.04%, vancomycin 24.57%)
EOT, end of treatment; mITT, modified intent-to-treat; PP, per protocol; UBM, unformed bowel movements

61
VancomycinDIFICLIR
003 004 003 004mITT PP
Clin
ical
cur
e (%
)
85.8% 86.8%88.2% 87.7%91.7%89.8% 90.6%92.1%
100
80
60
40
20
0
p=NS p=NS p=NS p=NS
Figure 20. Rates of clinical cure in the mITT and PP populations of phase 3 trials (studies 003 and 004)3,5
VancomycinDIFICLIR
003 004mITT
003 004PP
Recu
rren
ce (%
)
15.4%12.8%12.7%
25.3%26.9%
24.0%25.3%
13.3%
p=0.005 p=0.0002 p=0.004 p=0.002
50
40
30
20
10
0
Figure 21. Rates of recurrence among clinically cured patients in the mITT and PP populations of phase 3 trials (studies 003 and 004)3,5
mITT, modified intent-to-treat; NS, not significant; PP, per protocol
mITT, modified intent-to-treat; PP, per protocol

62
The high rates of clinical cure achieved with DIFICLIR when combined with significantly reduced rates of CDI recurrence, translated into significantly higher rates of sustained clinical cure (i.e. clinical cure without recurrence during the 30-day follow-up period) for DIFICLIR in comparison to vancomycin (Figure 22).
Across the two trials, more than 75% of DIFICLIR-treated patients achieved sustained clinical cure compared with approximately 65% of vancomycin-treated patients. This difference was statistically significant and clinically meaningful.3
VancomycinDIFICLIR
003 004
Sust
aine
d cl
inic
al c
ure
(%) 64.1% 63.4%
76.6%
67.1% 65.5%
77.7%74.6%
mITT003 004
PP
79.6%
p=0.0006 p=0.001 p=0.0006 p<0.001
100
80
60
40
20
0
Figure 22. Rates of sustained clinical cure in the mITT and PP populations of phase 3 trials (studies 003 and 004)3,5
In study 004, the median time to resolution of diarrhoea in the mITT population was 58 hours for vancomycin-treated patients compared with 56 hours for those on DIFICLIR.5
6.3. Efficacy in specific subpopulationsSeparate efficacy analyses were carried out in important subgroups within the population of patients enrolled in studies 003 and 004 to assess whether there were further potential advantages to treatment of CDI with DIFICLIR. Subanalyses examined the effects of age on treatment outcomes as well as the effect of clinical characteristics such as disease severity, infecting strain of C. difficile, use of concomitant antibacterial therapy and recurrent CDI.
DIFICLIR delivers a superior sustained clinical cure (clinical cure and no recurrence within 30 days) compared with vancomycin
mITT, modified intent-to-treat; PP, per protocol
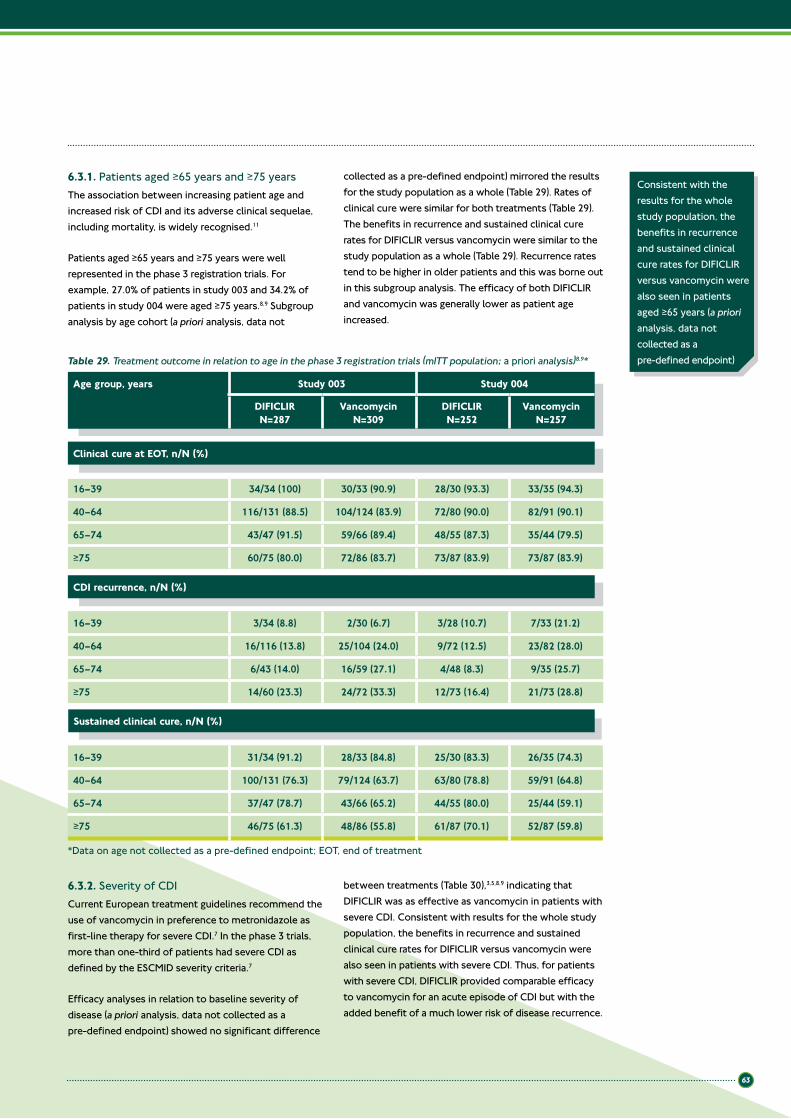
63
6.3.1. Patients aged ≥65 years and ≥75 yearsThe association between increasing patient age and increased risk of CDI and its adverse clinical sequelae, including mortality, is widely recognised.11
Patients aged ≥65 years and ≥75 years were well represented in the phase 3 registration trials. For example, 27.0% of patients in study 003 and 34.2% of patients in study 004 were aged ≥75 years.8,9 Subgroup analysis by age cohort (a priori analysis, data not
collected as a pre-defined endpoint) mirrored the results for the study population as a whole (Table 29). Rates of clinical cure were similar for both treatments (Table 29). The benefits in recurrence and sustained clinical cure rates for DIFICLIR versus vancomycin were similar to the study population as a whole (Table 29). Recurrence rates tend to be higher in older patients and this was borne out in this subgroup analysis. The efficacy of both DIFICLIR and vancomycin was generally lower as patient age increased.
Table 29. Treatment outcome in relation to age in the phase 3 registration trials (mITT population; a priori analysis)8,9*
16–39 34/34 (100) 30/33 (90.9) 28/30 (93.3) 33/35 (94.3)
40–64 116/131 (88.5) 104/124 (83.9) 72/80 (90.0) 82/91 (90.1)
65–74 43/47 (91.5) 59/66 (89.4) 48/55 (87.3) 35/44 (79.5)
≥75 60/75 (80.0) 72/86 (83.7) 73/87 (83.9) 73/87 (83.9)
Clinical cure at EOT, n/N (%)
Age group, years Study 003 Study 004
DIFICLIRN=287
VancomycinN=309
DIFICLIRN=252
VancomycinN=257
16–39 3/34 (8.8) 2/30 (6.7) 3/28 (10.7) 7/33 (21.2)
40–64 16/116 (13.8) 25/104 (24.0) 9/72 (12.5) 23/82 (28.0)
65–74 6/43 (14.0) 16/59 (27.1) 4/48 (8.3) 9/35 (25.7)
≥75 14/60 (23.3) 24/72 (33.3) 12/73 (16.4) 21/73 (28.8)
CDI recurrence, n/N (%)
16–39 31/34 (91.2) 28/33 (84.8) 25/30 (83.3) 26/35 (74.3)
40–64 100/131 (76.3) 79/124 (63.7) 63/80 (78.8) 59/91 (64.8)
65–74 37/47 (78.7) 43/66 (65.2) 44/55 (80.0) 25/44 (59.1)
≥75 46/75 (61.3) 48/86 (55.8) 61/87 (70.1) 52/87 (59.8)
Sustained clinical cure, n/N (%)
Consistent with the results for the whole study population, the benefits in recurrence and sustained clinical cure rates for DIFICLIR versus vancomycin were also seen in patients aged ≥65 years (a priori analysis, data not collected as a pre-defined endpoint)
6.3.2. Severity of CDICurrent European treatment guidelines recommend the use of vancomycin in preference to metronidazole as first-line therapy for severe CDI.7 In the phase 3 trials, more than one-third of patients had severe CDI as defined by the ESCMID severity criteria.7
Efficacy analyses in relation to baseline severity of disease (a priori analysis, data not collected as a pre-defined endpoint) showed no significant difference
between treatments (Table 30),3,5,8,9 indicating that DIFICLIR was as effective as vancomycin in patients with severe CDI. Consistent with results for the whole study population, the benefits in recurrence and sustained clinical cure rates for DIFICLIR versus vancomycin were also seen in patients with severe CDI. Thus, for patients with severe CDI, DIFICLIR provided comparable efficacy to vancomycin for an acute episode of CDI but with the added benefit of a much lower risk of disease recurrence.
*Data on age not collected as a pre-defined endpoint; EOT, end of treatment
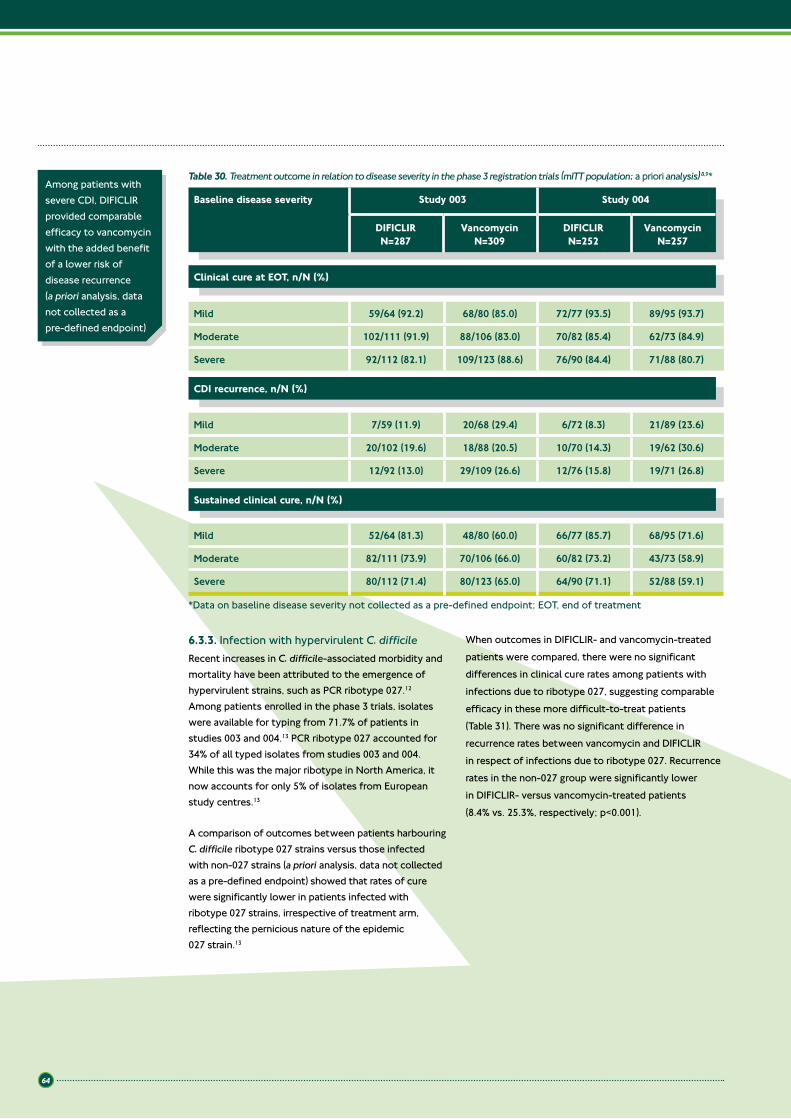
64
6.3.3. Infection with hypervirulent C. difficileRecent increases in C. difficile-associated morbidity and mortality have been attributed to the emergence of hypervirulent strains, such as PCR ribotype 027.12 Among patients enrolled in the phase 3 trials, isolates were available for typing from 71.7% of patients in studies 003 and 004.13 PCR ribotype 027 accounted for 34% of all typed isolates from studies 003 and 004. While this was the major ribotype in North America, it now accounts for only 5% of isolates from European study centres.13
A comparison of outcomes between patients harbouring C. difficile ribotype 027 strains versus those infected with non-027 strains (a priori analysis, data not collected as a pre-defined endpoint) showed that rates of cure were significantly lower in patients infected with ribotype 027 strains, irrespective of treatment arm, reflecting the pernicious nature of the epidemic 027 strain.13
When outcomes in DIFICLIR- and vancomycin-treated patients were compared, there were no significant differences in clinical cure rates among patients with infections due to ribotype 027, suggesting comparable efficacy in these more difficult-to-treat patients (Table 31). There was no significant difference in recurrence rates between vancomycin and DIFICLIR in respect of infections due to ribotype 027. Recurrence rates in the non-027 group were significantly lower in DIFICLIR- versus vancomycin-treated patients (8.4% vs. 25.3%, respectively; p<0.001).
Mild 52/64 (81.3) 48/80 (60.0) 66/77 (85.7) 68/95 (71.6)
Moderate 82/111 (73.9) 70/106 (66.0) 60/82 (73.2) 43/73 (58.9)
Severe 80/112 (71.4) 80/123 (65.0) 64/90 (71.1) 52/88 (59.1)
Sustained clinical cure, n/N (%)
Mild 7/59 (11.9) 20/68 (29.4) 6/72 (8.3) 21/89 (23.6)
Moderate 20/102 (19.6) 18/88 (20.5) 10/70 (14.3) 19/62 (30.6)
Severe 12/92 (13.0) 29/109 (26.6) 12/76 (15.8) 19/71 (26.8)
Mild 59/64 (92.2) 68/80 (85.0) 72/77 (93.5) 89/95 (93.7)
Moderate 102/111 (91.9) 88/106 (83.0) 70/82 (85.4) 62/73 (84.9)
Severe 92/112 (82.1) 109/123 (88.6) 76/90 (84.4) 71/88 (80.7)
CDI recurrence, n/N (%)
Clinical cure at EOT, n/N (%)
Table 30. Treatment outcome in relation to disease severity in the phase 3 registration trials (mITT population; a priori analysis) 8,9*
Baseline disease severity Study 003 Study 004
DIFICLIRN=287
VancomycinN=309
DIFICLIRN=252
VancomycinN=257
Among patients with severe CDI, DIFICLIR provided comparable efficacy to vancomycin with the added benefit of a lower risk of disease recurrence (a priori analysis, data not collected as a pre-defined endpoint)
*Data on baseline disease severity not collected as a pre-defined endpoint; EOT, end of treatment

65
6.3.4. Concomitant antibacterial therapyEvidence shows that patients receiving concomitant antibacterial therapy are more susceptible to CDI and often experience worse outcomes.14 The effect of concomitant antibacterial therapy on treatment outcomes in the phase 3 trials was investigated in a subgroup analysis with respect to its effect on resolution of CDI and on the risk of recurrence of symptomatic CDI (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint).14 Pooled data from studies 003 and 004 (N=999) showed that a total of 275 patients (27.5%) received antibacterial therapy for other infections during their 10-day treatment for CDI or during the 30-day follow-up. Of these, 192 patients (19.2%) received one or more other antibacterial agents during their treatment for CDI. Among patients who were evaluable for recurrence (N=794), a total of 185 (23.3%) received concomitant antibacterial therapy during treatment or follow-up.
An analysis of the results showed that among patients receiving concomitant antibacterial therapy during or following therapy, patients in the DIFICLIR treatment arm had better outcomes compared with vancomycin recipients.14
In the absence of concomitant antibacterial use, DIFICLIR and vancomycin were equivalent in their rates of clinical cure at EOT (92.3% vs. 92.8%, respectively; p=0.80). When subjects who received ≥1 concomitant antibacterial were analysed, DIFICLIR-treated patients had significantly better rates of clinical cure versus vancomycin-treated patients (90.0% vs. 79.4%, respectively; p=0.04).14
In patients who received ≥1 concomitant antibacterial, rates of recurrence at any time during their 10-day treatment period and 30-day follow-up were significantly better among DIFICLIR-treated versus vancomycin-treated patients (16.9% vs. 29.2%; p=0.048; Figure 23).14
In patients who received antibiotics only during the 30-day follow-up, rates of recurrence in DIFICLIR-treated patients were numerically, but not significantly, lower than those in vancomycin-treated patients (Figure 23).14
Among patients who received no concomitant antibacterial therapy during the trials, recurrence was twice as high in vancomycin-treated patients compared with those on DIFICLIR (23.9% vs. 11.5%, respectively; p<0.001; Figure 23).14
DIFICLIR is as effective as vancomycin in patients infected with the hypervirulent 027 strain of C. difficile (a priori analysis, data not collected as a pre-defined endpoint)
Table 31. Outcomes in DIFICLIR- versus vancomycin-treated patients in relation to isolate ribotype in the phase 3 registration trials (PP population; a priori analysis)13*
DIFICLIR Vancomycin p value
Ribotype 027 105/120 (87.5) 106/124 (85.4) NS
Non-027 strain 225/236 (95.3) 220/236 (93.2) NS
CDI recurrence, n/N (%)
Clinical cure, n/N (%)
Ribotype 027 21/90 (23.3) 29/93 (31.2) NS
Non-027 strain 17/203 (8.4) 49/194 (25.3) <0.001
*Data on isolate ribotype not collected as a pre-defined endpoint; NS, not significant
Reproduced with permission of the American Society for Microbiology
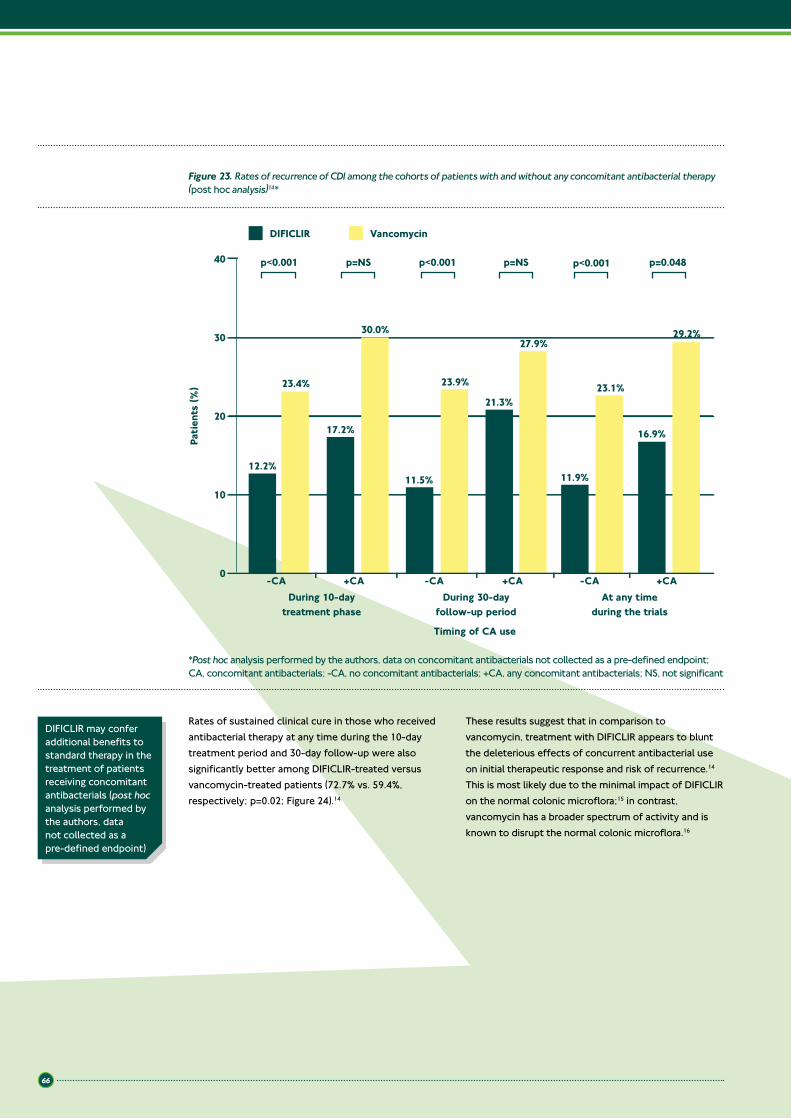
66
0
10
20
30
40
Patie
nts
(%)
Timing of CA use
VancomycinDIFICLIR
-CA +CA -CA +CA -CA +CA
12.2%
17.2%
11.5%
21.3%
11.9%
16.9%
23.4%
30.0%
23.9%
27.9%
23.1%
29.2%
During 10-daytreatment phase
During 30-dayfollow-up period
At any timeduring the trials
p<0.001 p<0.001p=NS p=NS p=0.048p<0.001
Figure 23. Rates of recurrence of CDI among the cohorts of patients with and without any concomitant antibacterial therapy (post hoc analysis)14*
*Post hoc analysis performed by the authors, data on concomitant antibacterials not collected as a pre-defined endpoint; CA, concomitant antibacterials; -CA, no concomitant antibacterials; +CA, any concomitant antibacterials; NS, not significant
Rates of sustained clinical cure in those who received anti bacterial therapy at any time during the 10-day treatment period and 30-day follow-up were also significantly better among DIFICLIR-treated versus vancomycin-treated patients (72.7% vs. 59.4%, respectively; p=0.02; Figure 24).14
These results suggest that in comparison to vancomycin, treatment with DIFICLIR appears to blunt the deleterious effects of concurrent antibacterial use on initial therapeutic response and risk of recurrence.14 This is most likely due to the minimal impact of DIFICLIR on the normal colonic microflora;15 in contrast, vancomycin has a broader spectrum of activity and is known to disrupt the normal colonic microflora.16
DIFICLIR may confer additional benefits to standard therapy in the treatment of patients receiving concomitant antibacterials (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)

67
6.3.5. Patients with renal impairmentA few studies have linked chronic renal disease to increased risk of, and poor outcomes from, CDI. As a result, a pooled analysis studied renal function and clinical outcomes in a large database of CDI patients treated with DIFICLIR or vancomycin (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint).17
Of the 1,031 patients treated with DIFICLIR or vancomycin, 57% had abnormal renal function. Renal impairment was mild in 27%, moderate in 21%, and severe in 9% of patients. Clinical cure rates (irrespective of treatment) were unaffected by mild renal impairment (91% for normal and 92% for mild), but declined to 80% for moderate and 74% for severe (p<0.001 for trend).17 Clinical cure rates were similar for DIFICLIR and vancomycin at each impairment level.
DIFICLIR was superior to vancomycin in reducing the risk of recurrence at all levels of renal function (p<0.05). The absolute difference in recurrence rates between treatments increased with level of renal impairment from 10% (11% DIFICLIR, 21% vancomycin) in patients with normal renal function to 21% (15% DIFICLIR, 35% vancomycin) in patients with severe renal impairment.17
Due to the limited clinical data in patients with severe renal impairment, DIFICLIR should be used with caution in this population.18
0
100
Patie
nts
(%)
-CA +CA
VancomycinDIFICLIR
10
20
30
40
50
60
70
80
9080.8%
p<0.001 p=0.02
72.7%69.0%
59.4%
Figure 24. Rates of sustained clinical cure among the cohorts of patients with and without concomitant antibacterial therapy (post hoc analysis)14*
*Post hoc analysis performed by the authors, data on concomitant antibacterials not collected as a pre-defined endpoint; concomitant antibacterials were prescribed to 27.5% of the 999 patients eligible for clinical cure and sustained clinical cure in the phase 3 trials; -CA, no concomitant antibacterials; +CA, any concomitant antibacterials
DIFICLIR delivers superior sustained clinical cure (clinical cure and no recurrence within 30 days) compared with vancomycin, irrespective of renal impairment (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
68
6.3.6. Recurrent CDIUp to 25% of patients with CDI experience disease recurrence within 30 days of treatment of a first acute episode with standard antibacterial therapy.2–4 Currently, management of recurrence is suboptimal and evidence from adequately powered prospective trials is lacking to guide treatment of recurrent CDI.
In planning the DIFICLIR phase 3 trials, a separate, pre-specified nested intervention population was constructed, consisting of patients who experienced a single prior episode of CDI within 3 months of entering the study (a priori analysis, data not collected as a pre-defined endpoint).19 Of the patients who met this
criterion and were randomised to treatment across the two studies, 128 were evaluable for recurrence. In this subgroup analysis, the primary endpoint was a second recurrence of CDI within 30 days of completing therapy, with recurrence defined by the same criteria as that used in the primary analysis (Table 28). Results showed that following treatment, 22 vancomycin-treated patients (35.5%) experienced another recurrence compared with 13 DIFICLIR-treated patients (19.7%; p=0.045), a difference that equates to a 45% reduction in repeat CDI recurrence.19 Consistent with other studies, patients aged ≥75 years had more than twice the risk of experiencing a second recurrence compared with younger patients (<55 years).20
Patients with recurrent CDI were significantly less likely to experience another recurrence when treated with DIFICLIR versus vancomycin (a priori analysis, data not collected as a pre-defined endpoint)
6.4. Summary
Key points
• DIFICLIR is non-inferior to vancomycin in the treatment of CDI and achieves similar clinical cure rates• High rates of clinical cure and low rates of recurrence with DIFICLIR translate into clinically significant
improvements in sustained clinical cure compared with vancomycin• DIFICLIR is significantly more effective than vancomycin in reducing recurrence of CDI, achieving a
47% reduction relative to vancomycin (recurrence rates in the pooled PP population: DIFICLIR 13.04%, vancomycin 24.57%)
• DIFICLIR is the first antibacterial to demonstrate lower recurrence rates for CDI versus vancomycin and corresponding improvements in sustained clinical cure
• Reduction of recurrence is not only of benefit to patients, but also potentially reduces the costs of treating additional episodes of CDI
• Consistent with the results for the whole study population, the benefits in recurrence and sustained clinical cure rates for DIFICLIR versus vancomycin were also seen in patients aged ≥65 years (a priori analysis, data not collected as a pre-defined endpoint)
• DIFICLIR is as effective as vancomycin in patients infected with the hypervirulent 027 strain of C. difficile (a priori analysis, data not collected as a pre-defined endpoint)
• In a subpopulation analysis of patients receiving concomitant antibacterial therapy, those treated with DIFICLIR exhibited significantly better rates of clinical cure for CDI versus those treated with vancomycin (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
• DIFICLIR treatment was associated with significantly lower rates of recurrence compared with vancomycin in patients who received concomitant antibacterials (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
• In one analysis, DIFICLIR achieved significantly greater rates of sustained clinical cure for CDI in patients who received concomitant antibacterial therapy (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
• Treatment with DIFICLIR was associated with significantly lower rates of recurrence of CDI than vancomycin in patients with renal impairment (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
• Patients with recurrent CDI treated with DIFICLIR were significantly less likely to experience another recurrence of CDI versus those treated with vancomycin (a priori analysis, data not collected as a pre-defined endpoint).

69
6.5. References1. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety,
and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
2. Bouza E, Dryden M, Mohammed R, et al. Results of a phase III trial comparing tolevamer, vancomycin and metronidazole in patients with Clostridium difficile-associated diarrhoea. Clin Microbiol Infect 2008;14 (Suppl 7):S103–4.
3. Louie TJ, Miller MA, Mullane KM, et al. DIFICLIR versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
4. Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med 2010;362:197–205.
5. Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;doi:10.1016/S1473-3099(11)70374-7.
6. Astellas Pharma Europe Ltd. Data on file, FDX/11/0023/EU.
7. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clin Microbiol Infect 2009;15:1067–79.
8. Astellas Pharma Europe Ltd. Data on file, FDX/11/0011/EU.
9. Astellas Pharma Europe Ltd. Data on file, FDX/11/0012/EU.
10. Mullane KM, Gorbach S. Fidaxomicin: first-in-class macrocyclic antibiotic. Expert Rev Anti Infect Ther 2011;9:767–77.
11. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multiinstitutional outbreak of Clostridium difficile–associated diarrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–9.
12. Kuijper EJ, Barbut F, Brazier JS, et al. Update of Clostridium difficile infection due to PCR ribotype 027 in Europe, 2008. Euro Surveill 2008;13ii:18942.
13. Gerding DN, Sambol SP, Nagaro K, et al. Clostridium difficile strain frequency as determined by restriction endonuclease analysis (REA) typing in two phase III trials of fidaxomicin vs vancomycin: treatment outcome for the epidemic BI/NAP/027 strain. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 12–15 September 2010; Boston, MA, USA. Abstract L1-1306.
14. Mullane KM, Miller MA, Weiss K, et al. Efficacy of fidaxomicin versus vancomycin as therapy for Clostridium difficile infection in patients taking concomitant antibiotics for other concurrent infections. Clin Infect Dis 2011;53:440–7.
15. Sullivan KM, Spooner LM. Fidaxomicin: a macrocyclic antibiotic for the management of Clostridium difficile infection. Ann Pharmacother 2010;44:352–9.
16. Finegold SM, Molitoris D, Vaisanen ML, et al. In vitro activities of OPT-80 and comparator drugs against intestinal bacteria. Antimicrob Agents Chemother 2004;48:4898–902.
17. Astellas Pharma Europe Ltd. Data on file, FDX/11/0013/EU.
18. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
19. Cornely OA, Miller M, Louie T, et al. Randomized controlled trial (RCT) of fidaxomicin (FDX) versus vancomycin (VAN) in treatment of recurrent Clostridium difficile infection (CDI). Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 12–15 September 2010; Boston, MA, USA. Abstract L1-1305.
20. Astellas Pharma Europe Ltd. Data on file, FDX/11/0014/EU.

70
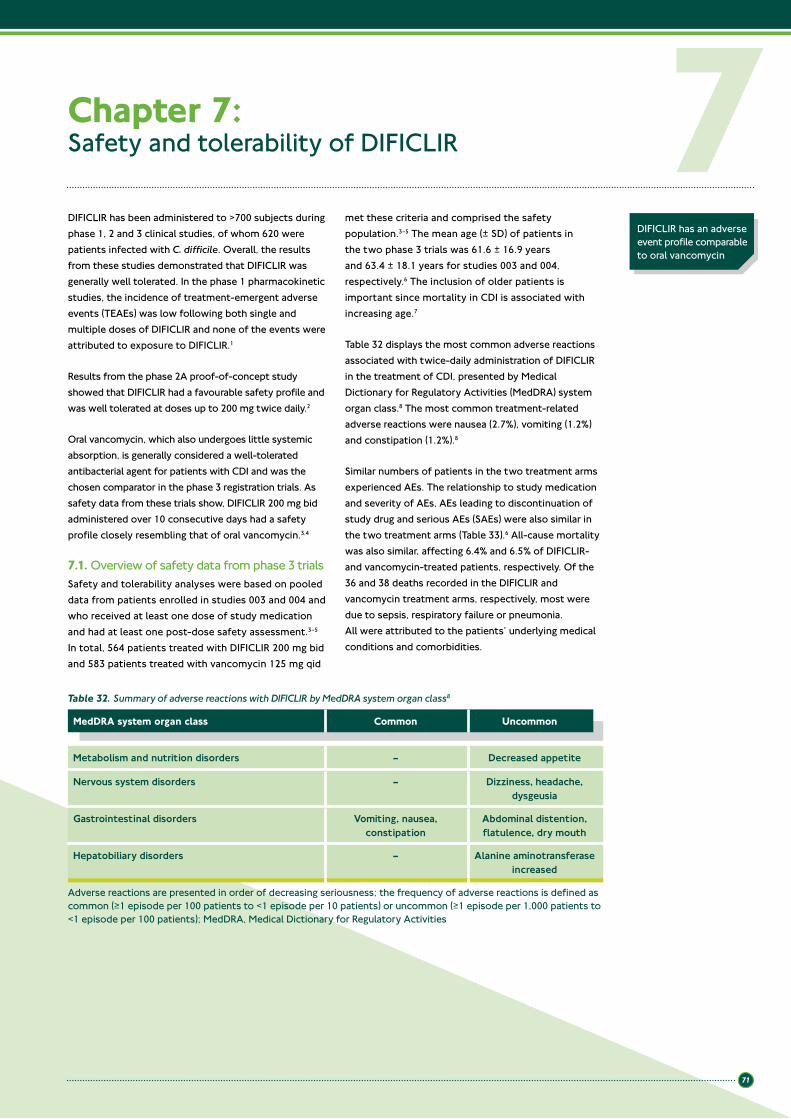
71
Chapter 7: Safety and tolerability of DIFICLIR
DIFICLIR has been administered to >700 subjects during phase 1, 2 and 3 clinical studies, of whom 620 were patients infected with C. difficile. Overall, the results from these studies demonstrated that DIFICLIR was generally well tolerated. In the phase 1 pharmacokinetic studies, the incidence of treatment-emergent adverse events (TEAEs) was low following both single and multiple doses of DIFICLIR and none of the events were attributed to exposure to DIFICLIR.1
Results from the phase 2A proof-of-concept study showed that DIFICLIR had a favourable safety profile and was well tolerated at doses up to 200 mg twice daily.2
Oral vancomycin, which also undergoes little systemic absorption, is generally considered a well-tolerated antibacterial agent for patients with CDI and was the chosen comparator in the phase 3 registration trials. As safety data from these trials show, DIFICLIR 200 mg bid administered over 10 consecutive days had a safety profile closely resembling that of oral vancomycin.3,4
7.1. Overview of safety data from phase 3 trialsSafety and tolerability analyses were based on pooled data from patients enrolled in studies 003 and 004 and who received at least one dose of study medication and had at least one post-dose safety assessment.3–5 In total, 564 patients treated with DIFICLIR 200 mg bid and 583 patients treated with vancomycin 125 mg qid
met these criteria and comprised the safety population.3–5 The mean age (± SD) of patients in the two phase 3 trials was 61.6 ± 16.9 years and 63.4 ± 18.1 years for studies 003 and 004, respectively.6 The inclusion of older patients is important since mortality in CDI is associated with increasing age.7
Table 32 displays the most common adverse reactions associated with twice-daily administration of DIFICLIR in the treatment of CDI, presented by Medical Dictionary for Regulatory Activities (MedDRA) system organ class.8 The most common treatment-related adverse reactions were nausea (2.7%), vomiting (1.2%) and constipation (1.2%).8
Similar numbers of patients in the two treatment arms experienced AEs. The relationship to study medication and severity of AEs, AEs leading to discontinuation of study drug and serious AEs (SAEs) were also similar in the two treatment arms (Table 33).6 All-cause mortality was also similar, affecting 6.4% and 6.5% of DIFICLIR- and vancomycin-treated patients, respectively. Of the 36 and 38 deaths recorded in the DIFICLIR and vancomycin treatment arms, respectively, most were due to sepsis, respiratory failure or pneumonia. All were attributed to the patients’ underlying medical conditions and comorbidities.
7DIFICLIR has an adverse event profile comparable to oral vancomycin
Table 32. Summary of adverse reactions with DIFICLIR by MedDRA system organ class8
MedDRA system organ class Common Uncommon
Metabolism and nutrition disorders – Decreased appetite
Nervous system disorders – Dizziness, headache, dysgeusia
Gastrointestinal disorders Vomiting, nausea, constipation
Abdominal distention, flatulence, dry mouth
Hepatobiliary disorders – Alanine aminotransferase increased
Adverse reactions are presented in order of decreasing seriousness; the frequency of adverse reactions is defined as common (≥1 episode per 100 patients to <1 episode per 10 patients) or uncommon (≥1 episode per 1,000 patients to <1 episode per 100 patients); MedDRA, Medical Dictionary for Regulatory Activities
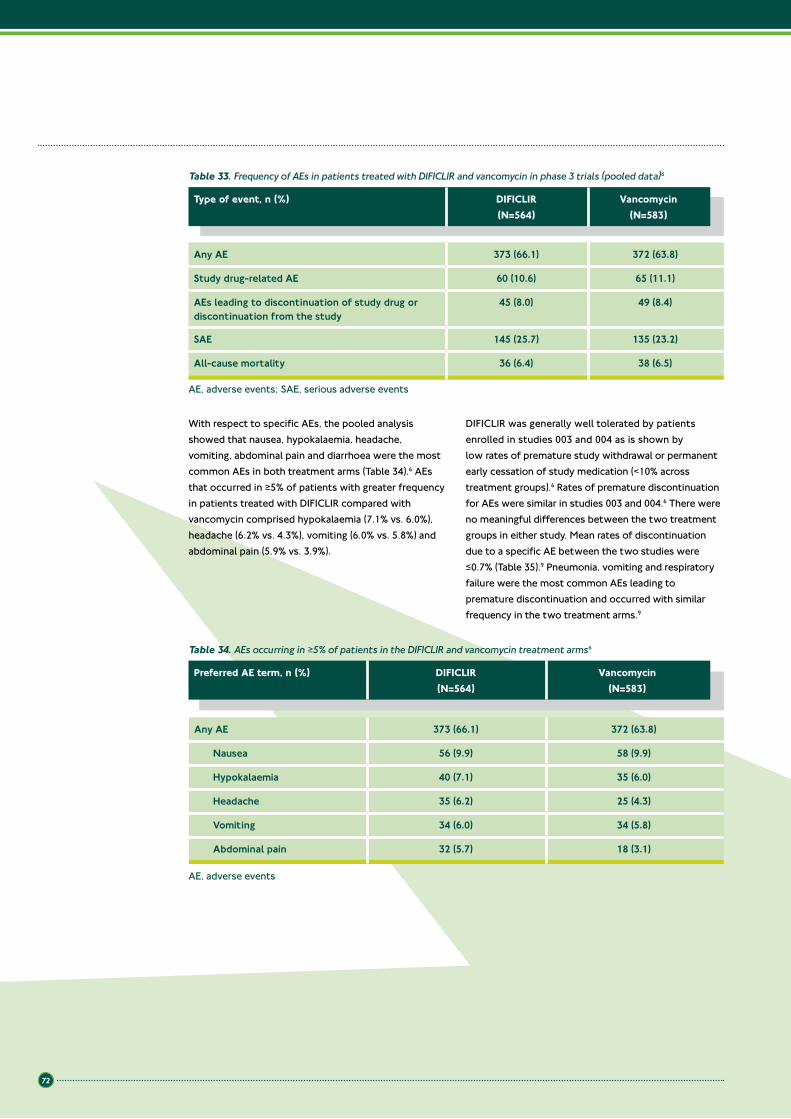
72
With respect to specific AEs, the pooled analysis showed that nausea, hypokalaemia, headache, vomiting, abdominal pain and diarrhoea were the most common AEs in both treatment arms (Table 34).6 AEs that occurred in ≥5% of patients with greater frequency in patients treated with DIFICLIR compared with vancomycin comprised hypokalaemia (7.1% vs. 6.0%), headache (6.2% vs. 4.3%), vomiting (6.0% vs. 5.8%) and abdominal pain (5.9% vs. 3.9%).
DIFICLIR was generally well tolerated by patients enrolled in studies 003 and 004 as is shown by low rates of premature study withdrawal or permanent early cessation of study medication (<10% across treatment groups).6 Rates of premature discontinuation for AEs were similar in studies 003 and 004.6 There were no meaningful differences between the two treatment groups in either study. Mean rates of discontinuation due to a specific AE between the two studies were ≤0.7% (Table 35).9 Pneumonia, vomiting and respiratory failure were the most common AEs leading to premature discontinuation and occurred with similar frequency in the two treatment arms.9
Table 33. Frequency of AEs in patients treated with DIFICLIR and vancomycin in phase 3 trials (pooled data)6
Type of event, n (%) DIFICLIR (N=564)
Vancomycin (N=583)
Any AE 373 (66.1) 372 (63.8)
Study drug-related AE 60 (10.6) 65 (11.1)
AEs leading to discontinuation of study drug or discontinuation from the study
45 (8.0) 49 (8.4)
SAE 145 (25.7) 135 (23.2)
All-cause mortality 36 (6.4) 38 (6.5)
AE, adverse events; SAE, serious adverse events
Table 34. AEs occurring in ≥5% of patients in the DIFICLIR and vancomycin treatment arms6
Preferred AE term, n (%) DIFICLIR (N=564)
Vancomycin (N=583)
Any AE 373 (66.1) 372 (63.8)
Nausea 56 (9.9) 58 (9.9)
Hypokalaemia 40 (7.1) 35 (6.0)
Headache 35 (6.2) 25 (4.3)
Vomiting 34 (6.0) 34 (5.8)
Abdominal pain 32 (5.7) 18 (3.1)
AE, adverse events
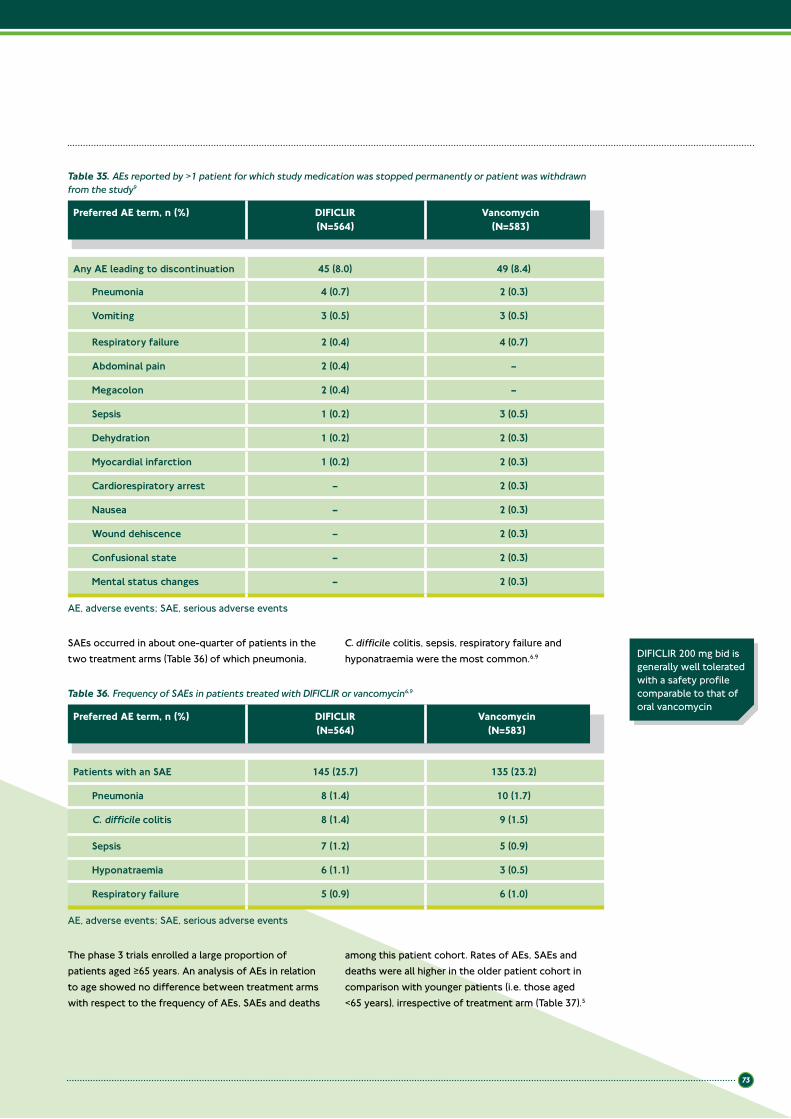
73
Table 35. AEs reported by >1 patient for which study medication was stopped permanently or patient was withdrawn from the study9
Preferred AE term, n (%) DIFICLIR (N=564)
Vancomycin (N=583)
Any AE leading to discontinuation 45 (8.0) 49 (8.4)
Pneumonia 4 (0.7) 2 (0.3)
Vomiting 3 (0.5) 3 (0.5)
Respiratory failure 2 (0.4) 4 (0.7)
Abdominal pain 2 (0.4) –
Megacolon 2 (0.4) –
Sepsis 1 (0.2) 3 (0.5)
Dehydration 1 (0.2) 2 (0.3)
Myocardial infarction 1 (0.2) 2 (0.3)
Cardiorespiratory arrest – 2 (0.3)
Nausea – 2 (0.3)
Wound dehiscence – 2 (0.3)
Confusional state – 2 (0.3)
Mental status changes – 2 (0.3)
DIFICLIR 200 mg bid is generally well tolerated with a safety profile comparable to that of oral vancomycin
SAEs occurred in about one-quarter of patients in the two treatment arms (Table 36) of which pneumonia,
C. difficile colitis, sepsis, respiratory failure and hyponatraemia were the most common.6,9
Table 36. Frequency of SAEs in patients treated with DIFICLIR or vancomycin6,9
Preferred AE term, n (%) DIFICLIR (N=564)
Vancomycin (N=583)
Patients with an SAE 145 (25.7) 135 (23.2)
Pneumonia 8 (1.4) 10 (1.7)
C. difficile colitis 8 (1.4) 9 (1.5)
Sepsis 7 (1.2) 5 (0.9)
Hyponatraemia 6 (1.1) 3 (0.5)
Respiratory failure 5 (0.9) 6 (1.0)
The phase 3 trials enrolled a large proportion of patients aged ≥65 years. An analysis of AEs in relation to age showed no difference between treatment arms with respect to the frequency of AEs, SAEs and deaths
among this patient cohort. Rates of AEs, SAEs and deaths were all higher in the older patient cohort in comparison with younger patients (i.e. those aged <65 years), irrespective of treatment arm (Table 37).5
AE, adverse events; SAE, serious adverse events
AE, adverse events; SAE, serious adverse events
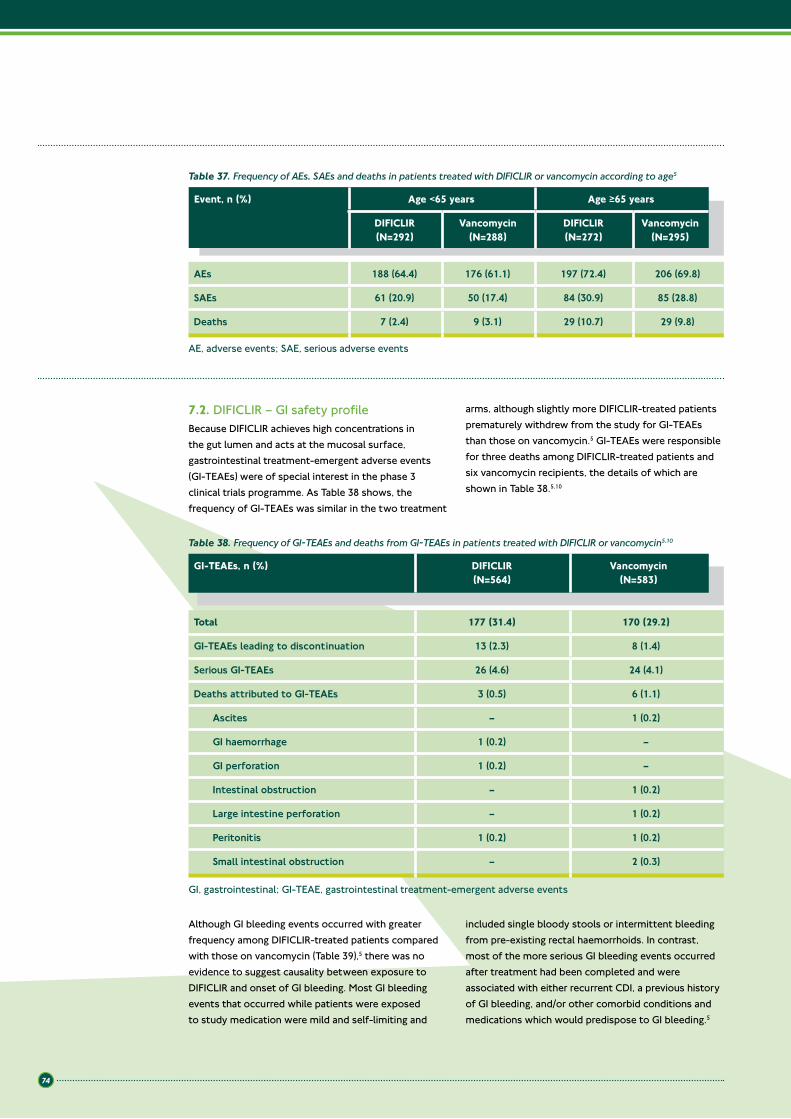
74
Event, n (%) Age <65 years Age ≥65 years
DIFICLIR(N=292)
Vancomycin(N=288)
DIFICLIR(N=272)
Vancomycin(N=295)
AEs 188 (64.4) 176 (61.1) 197 (72.4) 206 (69.8)
SAEs 61 (20.9) 50 (17.4) 84 (30.9) 85 (28.8)
Deaths 7 (2.4) 9 (3.1) 29 (10.7) 29 (9.8)
Table 37. Frequency of AEs, SAEs and deaths in patients treated with DIFICLIR or vancomycin according to age5
7.2. DIFICLIR – GI safety profileBecause DIFICLIR achieves high concentrations in the gut lumen and acts at the mucosal surface, gastrointestinal treatment-emergent adverse events (GI-TEAEs) were of special interest in the phase 3 clinical trials programme. As Table 38 shows, the frequency of GI-TEAEs was similar in the two treatment
arms, although slightly more DIFICLIR-treated patients prematurely withdrew from the study for GI-TEAEs than those on vancomycin.5 GI-TEAEs were responsible for three deaths among DIFICLIR-treated patients and six vancomycin recipients, the details of which are shown in Table 38.5,10
Although GI bleeding events occurred with greater frequency among DIFICLIR-treated patients compared with those on vancomycin (Table 39),5 there was no evidence to suggest causality between exposure to DIFICLIR and onset of GI bleeding. Most GI bleeding events that occurred while patients were exposed to study medication were mild and self-limiting and
included single bloody stools or intermittent bleeding from pre-existing rectal haemorrhoids. In contrast, most of the more serious GI bleeding events occurred after treatment had been completed and were associated with either recurrent CDI, a previous history of GI bleeding, and/or other comorbid conditions and medications which would predispose to GI bleeding.5
Table 38. Frequency of GI-TEAEs and deaths from GI-TEAEs in patients treated with DIFICLIR or vancomycin5,10
GI-TEAEs, n (%) DIFICLIR (N=564)
Vancomycin (N=583)
Total 177 (31.4) 170 (29.2)
GI-TEAEs leading to discontinuation 13 (2.3) 8 (1.4)
Serious GI-TEAEs 26 (4.6) 24 (4.1)
Deaths attributed to GI-TEAEs 3 (0.5) 6 (1.1)
Ascites – 1 (0.2)
GI haemorrhage 1 (0.2) –
GI perforation 1 (0.2) –
Intestinal obstruction – 1 (0.2)
Large intestine perforation – 1 (0.2)
Peritonitis 1 (0.2) 1 (0.2)
Small intestinal obstruction – 2 (0.3)
GI, gastrointestinal; GI-TEAE, gastrointestinal treatment-emergent adverse events
AE, adverse events; SAE, serious adverse events
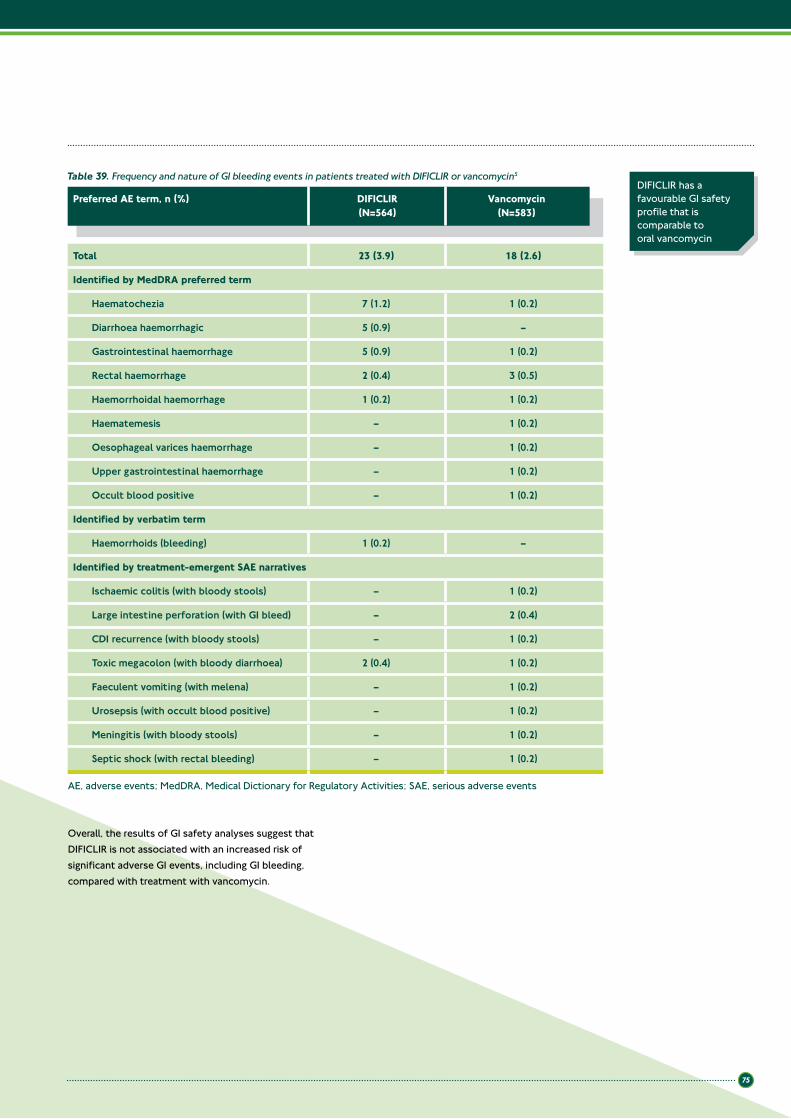
75
Overall, the results of GI safety analyses suggest that DIFICLIR is not associated with an increased risk of significant adverse GI events, including GI bleeding, compared with treatment with vancomycin.
Preferred AE term, n (%) DIFICLIR(N=564)
Vancomycin (N=583)
Total 23 (3.9) 18 (2.6)
Identified by MedDRA preferred term
Haematochezia 7 (1.2) 1 (0.2)
Diarrhoea haemorrhagic 5 (0.9) –
Gastrointestinal haemorrhage 5 (0.9) 1 (0.2)
Rectal haemorrhage 2 (0.4) 3 (0.5)
Haemorrhoidal haemorrhage 1 (0.2) 1 (0.2)
Haematemesis – 1 (0.2)
Oesophageal varices haemorrhage – 1 (0.2)
Upper gastrointestinal haemorrhage – 1 (0.2)
Occult blood positive – 1 (0.2)
Identified by verbatim term
Haemorrhoids (bleeding) 1 (0.2) –
Identified by treatment-emergent SAE narratives
Ischaemic colitis (with bloody stools) – 1 (0.2)
Large intestine perforation (with GI bleed) – 2 (0.4)
CDI recurrence (with bloody stools) – 1 (0.2)
Toxic megacolon (with bloody diarrhoea) 2 (0.4) 1 (0.2)
Faeculent vomiting (with melena) – 1 (0.2)
Urosepsis (with occult blood positive) – 1 (0.2)
Meningitis (with bloody stools) – 1 (0.2)
Septic shock (with rectal bleeding) – 1 (0.2)
Table 39. Frequency and nature of GI bleeding events in patients treated with DIFICLIR or vancomycin5
DIFICLIR has a favourable GI safety profile that is comparable to oral vancomycin
AE, adverse events; MedDRA, Medical Dictionary for Regulatory Activities; SAE, serious adverse events
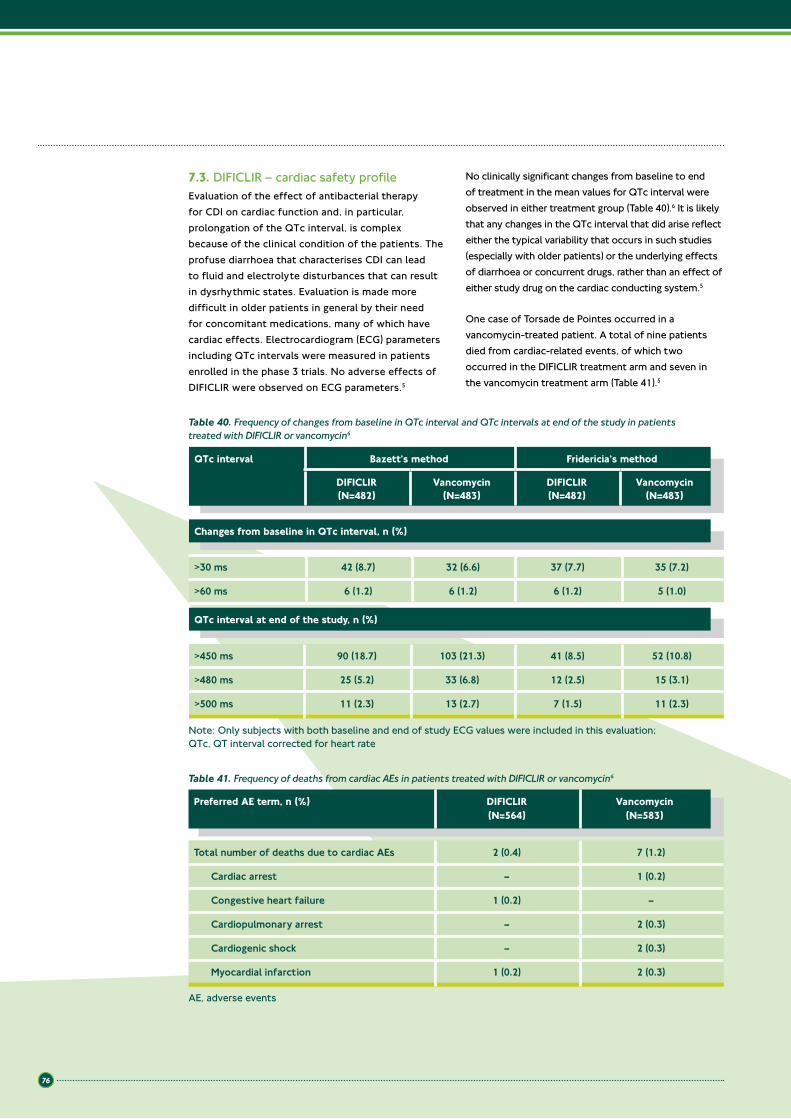
76
7.3. DIFICLIR – cardiac safety profileEvaluation of the effect of antibacterial therapy for CDI on cardiac function and, in particular, prolongation of the QTc interval, is complex because of the clinical condition of the patients. The profuse diarrhoea that characterises CDI can lead to fluid and electrolyte disturbances that can result in dysrhythmic states. Evaluation is made more difficult in older patients in general by their need for concomitant medications, many of which have cardiac effects. Electrocardiogram (ECG) parameters including QTc intervals were measured in patients enrolled in the phase 3 trials. No adverse effects of DIFICLIR were observed on ECG parameters.5
No clinically significant changes from baseline to end of treatment in the mean values for QTc interval were observed in either treatment group (Table 40).6 It is likely that any changes in the QTc interval that did arise reflect either the typical variability that occurs in such studies (especially with older patients) or the underlying effects of diarrhoea or concurrent drugs, rather than an effect of either study drug on the cardiac conducting system.5
One case of Torsade de Pointes occurred in a vancomycin-treated patient. A total of nine patients died from cardiac-related events, of which two occurred in the DIFICLIR treatment arm and seven in the vancomycin treatment arm (Table 41).5
>30 ms 42 (8.7) 32 (6.6) 37 (7.7) 35 (7.2)
>60 ms 6 (1.2) 6 (1.2) 6 (1.2) 5 (1.0)
Changes from baseline in QTc interval, n (%)
Table 40. Frequency of changes from baseline in QTc interval and QTc intervals at end of the study in patients treated with DIFICLIR or vancomycin6
QTc interval Bazett’s method Fridericia’s method
DIFICLIR (N=482)
Vancomycin(N=483)
DIFICLIR(N=482)
Vancomycin(N=483)
QTc interval at end of the study, n (%)
>450 ms 90 (18.7) 103 (21.3) 41 (8.5) 52 (10.8)
>480 ms 25 (5.2) 33 (6.8) 12 (2.5) 15 (3.1)
>500 ms 11 (2.3) 13 (2.7) 7 (1.5) 11 (2.3)
Note: Only subjects with both baseline and end of study ECG values were included in this evaluation; QTc, QT interval corrected for heart rate
Table 41. Frequency of deaths from cardiac AEs in patients treated with DIFICLIR or vancomycin6
Preferred AE term, n (%) DIFICLIR (N=564)
Vancomycin(N=583)
Total number of deaths due to cardiac AEs 2 (0.4) 7 (1.2)
Cardiac arrest – 1 (0.2)
Congestive heart failure 1 (0.2) –
Cardiopulmonary arrest – 2 (0.3)
Cardiogenic shock – 2 (0.3)
Myocardial infarction 1 (0.2) 2 (0.3)
AE, adverse events

77
7.4. DIFICLIR – renal safety profilePatients with renal impairment are a group of patients at risk of CDI recurrence.11,12 DIFICLIR was generally well tolerated by patients with mild, moderate or severe renal impairment with no clinically significant differences observed in frequency of AEs between treatment groups within each subpopulation of renal patients. Not unexpectedly, patients with severe renal impairment experienced the highest rate of SAEs in both treatment groups; these patients were usually patients aged ≥65 years with serious underlying illnesses.5
7.5. DIFICLIR – clinical chemistry parameters and vital signsLaboratory test abnormalities occurred with similar frequency in the two treatment arms, with the exception of decreases in WBC count. Decreases in WBC counts were more common in the DIFICLIR treatment arm, affecting 23 patients (4.1%) compared with 11 vancomycin recipients (1.9%).5 Almost all of the observed changes occurred in patients with
underlying haematological malignancies, prior bone marrow transplantation, and/or those undergoing chemotherapy. In addition, patients in the DIFICLIR treatment arm had a higher incidence of pre-existing active blood and lymphatic disorders at enrolment (38.7% vs. 32.6%, respectively). More patients assigned to DIFICLIR were concomitantly receiving treatment with antineoplastic or immunomodulatory agents than those in the vancomycin treatment arm (67 subjects [11.9%] vs. 48 subjects [8.2%], respectively).
Overall, laboratory measurements taken before and at the end of treatment showed that exposure to DIFICLIR had no clinically significant or meaningful effect on clinical chemistry parameters that included liver function tests.6 Similarly, there were no clinically significant changes in any vital signs in either of the phase 3 trials and no notable differences between the two treatment arms.6 These findings are consistent with a locally acting antibacterial agent that undergoes minimal systemic absorption.
DIFICLIR was generally well tolerated by patients with mild, moderate or severe renal impairment
Exposure to DIFICLIR 200 mg bid appeared to have no clinically significant effects on vital signs, clinical chemistry or ECG parameters
7.6. Summary
Key points
• DIFICLIR is a generally well-tolerated antibacterial agent with a safety profile that is comparable to oral vancomycin
• In phase 3 trials, frequency of AEs, serious TEAEs, drug-related TEAEs and discontinuations because of TEAEs were similar for DIFICLIR and vancomycin
• SAEs and deaths occurred with similar frequency in DIFICLIR- and vancomycin-treated patients and were consistent with the patients’ underlying medical conditions
• Although AEs and SAEs occurred more frequently in patients aged ≥65 years there was no difference in frequency of AEs between DIFICLIR and vancomycin treatment in the older patient cohort
• There was no evidence to suggest that DIFICLIR induces clinically relevant QTc prolongation• There are no specific safety concerns when administering DIFICLIR to patients with renal and hepatic impairment• There were no differences between DIFICLIR and vancomycin with respect to clinically significant changes
in clinical chemistry parameters and vital signs; where changes were observed these were attributed to underlying medical conditions including CDI.

78
7.7. References1. Shue YK, Sears PS, Shangle S, et al. Safety, tolerance, and
pharmacokinetic studies of OPT-80 in healthy volunteers following single and multiple oral doses. Antimicrob Agents Chemother 2008;52:1391–5.
2. Louie T, Miller M, Donskey C, et al. Clinical outcomes, safety, and pharmacokinetics of OPT-80 in a phase 2 trial with patients with Clostridium difficile infection. Antimicrob Agents Chemother 2009;53:223–8.
3. Louie TJ, Miller MA, Mullane KM, et al. DIFICLIR versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
4. Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;doi:10.1016/S1473-3099(11)70374-7.
5. Astellas Pharma Europe Ltd. Data on file, FDX/11/0016/EU.
6. Astellas Pharma Europe Ltd. Data on file, FDX/11/0015/EU.
7. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multiinstitutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–9.
8. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
9. Astellas Pharma Europe Ltd. Data on file, FDX/11/0027/EU.
10. Astellas Pharma Europe Ltd. Data on file, FDX/11/0026/EU.
11. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis 1998;26:954–9.
12. Bauer MP, Miller M, Gerding DN, et al. Renal failure, fever, and leukocytosis all predict treatment failure in Clostridium difficile infection (CDI), but renal failure is the only predictor of recurrent CDI. Clin Microbiol Infect 2011;17(Suppl 4):A1–4.

79
Chapter 8: Summary and key points
8.1. Summary C. difficile infection has been recognised as a significant cause of morbidity and mortality in hospitalised patients. In a recent European survey of patients with suspected CDI or diarrhoea that developed ≥3 days after hospital admission, CDI was the attributive cause of mortality in 2% of patients and was contributory in a further 7% of cases.1
The clinical importance of C. difficile has grown in the past decade because of rising incidence rates and increasing disease severity, mortality and rates of recurrence.2,3
The ability of C. difficile to produce spores is key in its transmission to vulnerable patients. C. difficile spores can remain viable in hospital environments despite routine cleaning.4 This persistence both in the environment, and within the intestines of patients, permits transmission and recurrence of CDI.5,6
Recurrence of CDI has been identified by ESCMID as being the most important problem in its treatment.7 Up to 25% of CDI patients suffer a recurrence within 30 days following treatment with metronidazole or vancomycin,2,8,9 highlighting the need for an antibiotic that can offer a sustained clinical cure.
Recurrence of CDI is a serious and difficult-to-treat problem,7 increasing the length and overall cost of hospitalisation.10,11 Reducing the recurrence of CDI could lower the costs of treating additional episodes and may reduce the rate of person-to-person transmission.2 Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most dramatic include those who are immunocompromised,12 receiving certain concomitant antibiotics,1,13–15 who are renally impaired,16,17 or who are aged 65 years or over.1,13,15
Despite the changing epidemiology of CDI, recommended treatment so far has been limited to metronidazole for non-severe cases and vancomycin for severe cases.7 However, because of the pressure to limit the use of vancomycin in general due to concerns around VRE and decreasing vancomycin susceptibility in Staphylococcus aureus, greater constraints on the use of vancomycin for CDI have arisen.
Vancomycin and, to a lesser extent, metronidazole have non-selective antibacterial activity, suppressing the normal colonic microflora that would otherwise compete for nutrients and other resources with
C. difficile.18–20 While the reasons for recurrence are not completely understood, the failure to re-establish the normal colonic microflora is understood to be an important factor.3
Other factors to which the high rates of CDI recurrence are attributed include the persistence of spores of C. difficile in the intestines of patients and the failure of the host to mount an appropriate immune response to its toxins.3 Inhibiting the production of spores may enable the risk of recurrence to be reduced; however, neither metronidazole nor vancomycin has been shown to exhibit such an effect. Metronidazole and vancomycin also require frequent dosing, with regimens of three- and four-times daily, respectively. Following administration, oral metronidazole is almost completely absorbed in the gut.3 This means that levels of metronidazole in the colon may be low, increasing the risk of treatment failure.3
In view of all these limitations, there is an urgent need for new treatments for CDI to improve outcomes and reduce over dependence on vancomycin, in light of the diminishing efficacy of metronidazole, and reduce the high rates of recurrence with both treatments.
An ‘ideal’ treatment for CDI should be effective against C. difficile and achieve high rates of clinical cure that are at least comparable to vancomycin. It should reduce the risk of recurrence, be well tolerated, and have a low potential for resistance development.3 Since recurrence is associated with a failure to re-establish the normal colonic microflora,3 an ideal treatment would offer minimal disruption to colonisation resistance. Also, as the persistence of C. difficile spores in patients’ intestines is regarded as another reason for recurrence,3 an ideal treatment would inhibit spore production. Furthermore, because the pathology of CDI is mediated by the toxins that are produced by C. difficile5 an ideal treatment would inhibit toxin production.
DIFICLIR, a convenient twice-daily tablet that is the first in a new class of antibacterial agents, called the macrocycles, developed for the treatment of CDI21 meets all of the above criteria. In the pivotal phase 3 trials, DIFICLIR met its primary endpoint of non-inferiority to oral vancomycin with respect to clinical cure at end of therapy, and significantly reduced the rate of recurrence, leading to sustained clinical cure rates that were superior to vancomycin.2,22
8

80
DIFICLIR exhibits targeted antibacterial activity and, as a result, causes minimal disruption to the normal colonic microflora23 that maintains colonisation resistance and restricts opportunities for C. difficile overgrowth.2 DIFICLIR also acts to inhibit the production of C. difficile spores and toxins.23–26
As clinical trials have shown, DIFICLIR-treated patients were significantly less likely to suffer a CDI recurrence than those treated with vancomycin. This included patients aged ≥65 years and those with severe CDI (both a priori analyses, data not collected as pre-defined endpoints) as well as those with renal impairment (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint). The reduced likelihood of recurrence with DIFICLIR relative to current therapies is partly due to its minimal effects on the normal colonic microflora, which reduce the opportunities for the overgrowth of C. difficile. The intrinsic ability of C. difficile to produce spores that can persist both in the intestines of patients and in the environment to permit relapse is a major factor associated with the high rate of disease recurrence.5 If spores remain in the gastrointestinal tract they can become a source of relapse once treatment is completed. In addition, by inhibiting spore production, DIFICLIR may further help reduce the risk of disease recurrence through reduced environmental contamination.
Resistance to DIFICLIR is not expected to emerge rapidly based on in vitro testing and analysis of samples taken during the clinical trials at baseline and at the point of failure or recurrence.
As a locally acting agent within the gastrointestinal tract, DIFICLIR undergoes minimal systemic absorption and, as such, is associated with low levels of systemic toxicity. Across the phase 3 trial populations, which included a high proportion of patients aged ≥65 years,2,22
DIFICLIR was well tolerated with a safety profile comparable to that of oral vancomycin.2,22 There is no requirement for dose adjustment in patients aged ≥65 years, or in patients with renal or hepatic impairment.21 This is important since many patients with CDI are aged 65 years or over.
There is no indication that DIFICLIR induces relevant prolongation of the QTc interval and an analysis of GI bleeding events, leucopenia and liver function in DIFICLIR-treated patients did not reveal any special concerns when underlying patient conditions and concomitant therapy were taken into consideration. DIFICLIR does not induce or inhibit cytochrome P450 enzymes in vitro, but is a substrate of the P-glycoprotein (P-gp) transporter and may be a mild-to-moderate inhibitor of intestinal P-gp.21 DIFICLIR and potent P-gp inhibitors such as cyclosporin, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and amiodarone, should not be administered at the same time.21
Overall, the results from clinical trials suggest that DIFICLIR has a favourable benefit-to-risk profile in the treatment of CDI. By significantly reducing the risk of recurrence after either an initial CDI episode or first recurrence, DIFICLIR has the potential to advance the treatment of CDI in at-risk patients, including those who are: immunocompromised, receiving concomitant antibacterials, renally impaired, or who are aged 65 years or over.
As the first new antibacterial for CDI to demonstrate lower recurrence rates and corresponding improvements in sustained clinical cure when compared to vancomycin, DIFICLIR provides clinicians with a first-line therapy for CDI which addresses many of the key unmet needs in the management of this debilitating disease.
81
8.2. Key points
Key points
• C. difficile is the leading cause of nosocomial diarrhoea in industrialised countries and the incidence of CDI is increasing
• In a European survey, C. difficile was the attributive cause of mortality in 2% of patients and was contributory in a further 7% of cases
• The ability to produce spores and their persistent nature is a key factor in the transmission of C. difficile to patients
• ESCMID has identified recurrence as being the most important problem in the treatment of CDI• Up to 25% of CDI patients suffer a recurrence of infection within 30 days following treatment with
metronidazole or vancomycin, highlighting the need for an antibiotic that can offer a sustained clinical cure• Patient groups at high risk of recurrence or those for whom the impact of recurrence would be most
dramatic include those who:o Are immunocompromisedo Are receiving concomitant antibioticso Are renally impairedo Are aged 65 years or over
• Recommended treatment options for CDI so far have been limited to metronidazole and vancomycin• An ideal treatment for CDI would be effective against C. difficile, reduce the risk of recurrence, inhibit the
production of spores and toxins, and have minimal effects on the normal colonic microflora• DIFICLIR is an oral macrocyclic antibacterial indicated for the treatment of CDI, with targeted activity that
kills C. difficile and inhibits spore and toxin production• As DIFICLIR causes minimal disruption to the normal colonic microflora, it preserves colonisation resistance
and thereby restricts opportunities for C. difficile re-emergence• DIFICLIR has proven efficacy against CDI with a clinical cure rate comparable to that of vancomycin• DIFICLIR is superior to vancomycin in reducing the rate of CDI recurrence
o Reduction of recurrence is not only of benefit to patients, but may also decrease the costs of treating additional episodes of CDI and may lower the risk of person-to-person transmission
• DIFICLIR is superior to vancomycin in terms of sustained clinical cure rates due to its high rate of clinical cure and low rate of recurrence
• In a subpopulation analysis of patients who received concomitant antibacterials, greater rates of clinical cure were observed in DIFICLIR- versus vancomycin-treated patients (post hoc analysis performed by the authors, data not collected as a pre-defined endpoint)
o Rates of recurrence were significantly lower among DIFICLIR- versus vancomycin-treated patientso Rates of sustained clinical cure were also significantly better among DIFICLIR-treated versus
vancomycin-treated patients• The safety profile of DIFICLIR is comparable to that of oral vancomycin• DIFICLIR has low levels of systemic absorption, providing:
o A low risk of systemic toxicityo Activity at the site of infection
• There is no need for dose adjustments in patients aged 65 years or over or those with renal and hepatic impairment
• DIFICLIR is the first new antibacterial for CDI to demonstrate lower recurrence rates for CDI, delivering superior rates of sustained clinical cure (clinical cure and no recurrence within 30 days) compared to vancomycin
• DIFICLIR is a convenient, twice-daily tablet that provides clinicians with a first-line therapy for CDI that addresses many of the key unmet needs in the management of this debilitating disease.
82
8.3. References1. Bauer MP, Notermans DW, van Benthem BH, et al.
Clostridium difficile infection in Europe: a hospital-based survey. Lancet 2011;377:63–73.
2. Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011;364:422–31.
3. DuPont HL. The search for effective treatment of Clostridium difficile infection. N Engl J Med 2011;364:473–4.
4. Verity P, Wilcox MH, Fawley W, et al. Prospective evaluation of environmental contamination by Clostridium difficile in isolation side rooms. J Hosp Infect 2001;49:204–9.
5. Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ 2004;171:51–8.
6. McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol 2002;97:1769–75.
7. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clin Microbiol Infect 2009;15:1067–79.
8. Lowy I, Molrine DC, Leav BA, et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N Engl J Med 2010;362:197–205.
9. Bouza E, Dryden M, Mohammed R, et al. Results of a phase III trial comparing tolevamer, vancomycin and metronidazole in patients with Clostridium difficile-associated diarrhoea. Clin Microbiol Infect 2008;14(Suppl 7):S103–4.
10. Vonberg RP, Reichardt C, Behnke M, et al. Costs of nosocomial Clostridium difficile-associated diarrhoea. J Hosp Infect 2008;70:15–20.
11. Wilcox MH, Cunniffe JG, Trundle C, et al. Financial burden of hospital-acquired Clostridium difficile infection. J Hosp Infect 1996;34:23–30.
12. Cohen MB. Clostridium difficile infections: emerging epidemiology and new treatments. J Ped Gastroenterol Nutr 2009;48:63–5.
13. Kyne L, Warny M, Qamar A, et al. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet 2001;357:189–93.
14. Hu MY, Katchar K, Kyne L, et al. Prospective derivation and validation of a clinical prediction rule for recurrent Clostridium difficile infection. Gastroenterology 2009;136:1206–14.
15. Pépin J, Alary M-E, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis 2005;40:1591–7.
16. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for early recurrent Clostridium difficile-associated diarrhea. Clin Infect Dis 1998;26:954–9.
17. Bauer MP, Miller M, Gerding DN, et al. Renal failure, fever, and leukocytosis all predict treatment failure in Clostridium difficile infection (CDI), but renal failure is the only predictor of recurrent CDI. Clin Microbiol Infect 2011;17(Suppl 4):A1–4.
18. Edlund C, Barkolt L, Liljequist BO, et al. Effect of vancomycin on intestinal flora of patients who previously received antimicrobial therapy. Clin Infect Dis 1997;25:729–32.
19. Löfmark S, Edlund C, Nord CE. Metronidazole is still the drug of choice for treatment of anaerobic infections. Clin Infect Dis 2010;50(Suppl 1):S16–23.
20. Bjørneklett A, Midtvedt T. Influence of three antimicrobial agents – penicillin, metronidazole, and doxycycline – on the intestinal microflora of healthy humans. Scand J Gastroenterol 1981;16:473–80.
21. Astellas Pharma Europe Ltd. DIFICLIR (fidaxomicin). Summary of Product Characteristics, 19 December 2011.
22. Cornely OA, Crook DW, Esposito R, et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;doi:10.1016/S1473-3099(11)70374-7.
23. Louie TJ, Emery J, Krulicki W, et al. OPT-80 Eliminates Clostridium difficile and is sparing of Bacteroides species during treatment of C. difficile infection. Antimicrob Agents Chemother 2009;53:261–3.
24. Gomez A, Sears P, Nguyen L, et al. Fidaxomicin inhibits spore production in C. difficile 027/NAP1/BI. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-632.
25. Sims C, Gomez A, Sears P, et al. Fidaxomicin inhibits production of toxin A and toxin B in C. difficile. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-634.
26. Bouillaut L, Babakhani F, Sonenshein A. Inhibition of Clostridium difficile toxin synthesis and sporulation by fidaxomicin. Abstract presented at the Interscience Conference on Antimicrobial Agents and Chemotherapy, 18–21 September 2011, Chicago, IL, USA. Abstract C1-635.

83

84

© March 2012 Astellas Pharma Europe Ltd.
All Trade Marks, unless third party trademarks, are owned by Astellas Pharma Inc and/or its related entities. Third party trademarks, where referred to, are owned by originator companies and are represented here under license and/or with permission and/or with acknowledgement of their ownership.
Note: For non-English language versions of this Product Monograph
Figure 3 is translated with permission. The Canadian Medical Association is the copyright owner of “Figure 1: pathogenesis of Clostridium difficile-associated diarrhea in adults”, originally published in the CMAJ. The limited permission granted to translate into the French/German/Spanish/Portuguese/Greek/Italian/Czechoslovakian/Danish/Swedish/Finish/Norwegian/Hungarian/Russian/Dutch language does not extend to any other organization or person. The Canadian Medical Association and the authors of the original work are not responsible for the translation and do not necessarily endorse the accuracy or quality of the translation.

Product Monograph
Developed by Astellas Pharma Europe Limited*, Lovett House, Lovett Road, Staines, TW18 3AZ. Registered in England and Wales under Registered no. 2486792Date of Preparation: 03/2012. Item Code: FDX/11/0002/EUl*Astellas Pharma Europe Limited, located in the UK, is a European subsidiary of Tokyo-based Astellas Pharma Inc. ASTELLAS, LEADING LIGHT FOR LIFE, CHANGING TOMORROW and the Star logo are trademarks of Astellas Pharma Inc. and its related entities.
DificlirTM (fidaxomicin) Prescribing Information
Presentation: Dificlir™ tablets contain 200 mg fidaxomicin. Indication: The treatment of Clostridium difficile infections (CDI) also known as C. difficile-associated diarrhoea (CDAD) in adults. Consideration should be given to official guidelines on the appropriate use of antibacterial agents. Posology and method of administration: Adults and elderly (≥ 65 years of age): The recommended dose is one 200 mg tablet to be administered twice daily (once every 12 hours) for 10 days and can be taken with or without food. Paediatrics: The safety and efficacy of fidaxomicin in children aged below 18 years has not yet been established. Renal impairment: No dose adjustment is considered necessary. Use with caution in patients with severe renal impairment. Hepatic impairment: No dose adjustment is considered necessary. Use with caution with in patients with moderate to severe hepatic impairment. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Warnings and Precautions: Due to limited clinical data, fidaxomicin should be used with caution in patients with severe renal impairment or moderate to severe hepatic impairment. Fidaxomicin should also be used with caution in patients with pseudomembranous colitis, fulminant or life threatening CDI. No data is available in patients with concomitant bowel disease, caution should be used in these patients due to a risk of enhanced absorption and a potential risk for systemic adverse reactions. Co-administration of potent P-glycoprotein inhibitors such as cyclosporine, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and
amiodarone is not recommended. Drug interactions: Fidaxomicin is a substrate of P-gp and may be a mild to moderate inhibitor of intestinal P-gp. Co-administration of potent inhibitors of P-gp, such as cyclosporine, ketoconazole, erythromycin, clarithromycin, verapamil, dronedarone and amiodarone are not recommended. Fidaxomicin had a small but not clinically relevant effect on digoxin exposure and a larger effect on P-gp substrates with lower bioavailability more sensitive to intestinal P-gp inhibition such as dabigatran etexilat cannot be excluded. Undesirable effects: Common (≥ 1/100 to < 1/10): vomiting, nausea, constipation. Uncommon (≥ 1/1,000 to < 1/100): decreased appetite, dizziness, headache, dysgeusia, abdominal distension, flatulence, dry mouth, increased alanine aminotransferase. Consult SmPC for complete information on side effects. Packs and Cost: 200 mg tablet x 20, £1,350.00. Legal Classification: POM. Marketing authorisation number: EU/1/11/733/001-004 Date of Preparation of PI: March 2012. Further information available from: Astellas Pharma Ltd, Future House, 3rd Floor, The Glanty, Egham, Surrey TW20 9AH. For Medical Information phone 0800 783 5018
Prescribing information can be found on the back cover
Adverse events should be reported. Reporting forms and information can be found at
www.mhra.gov.uk/yellowcard.
Adverse events should also be reported to Astellas Pharma Ltd. Please contact 0800 783 5018

















