26
Production of Health FGS - Chapter 5
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | amelia-sims |
| View: | 216 times |
| Download: | 3 times |
Production of Health
FGS - Chapter 5

General Formulation
HS = f (Health Care, Environment, Human Biology, Life Style)
HS = f (HC, Env, HB, LS)
If we’re concentrating on health care,
Total Product: HS = f (HC, Env, HB, LS)
Marginal Product: MP = HS/HC
Average Product: AP = HS/HC
(Excel Spreadsheet - Ch 5.xls)
What are these?
What are these?

HS = HCaAE1-a
a 0.1
All Else HC HP Ave. Pr. Mgl. Pr.
100 1 63.1 63.1100 2 67.6 33.8 4.5100 3 70.4 23.5 2.8100 4 72.5 18.1 2.1100 5 74.1 14.8 1.6100 6 75.5 12.6 1.4100 7 76.6 10.9 1.2100 8 77.7 9.7 1.0100 9 78.6 8.7 0.9100 10 79.4 7.9 0.8100 11 80.2 7.3 0.8100 12 80.9 6.7 0.7100 13 81.5 6.3 0.7100 14 82.2 5.9 0.6100 15 82.7 5.5 0.6100 16 83.3 5.2 0.5100 17 83.8 4.9 0.5100 18 84.2 4.7 0.5100 19 84.7 4.5 0.5100 20 85.1 4.3 0.4
Total, Average, and Marginal Products
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
0 5 10 15 20
Health Care
Prod
ucts
HS
Ave. Pr.
Mgl. Pr.
Measures of Health Status
• Death rates (easiest to measure)• Healthy days• Morbidity rates
It may be critical to distinguish between total and marginal contributions, since low marginals may accompany high totals.
Think about longevity.

Total v. Marginal
• It is critical to distinguish between total and marginal contributions. It may turn out that although the total contribution may be substantial, the marginal contribution may be very small. Why do we care?
• Because many decisions are made at the margin. Additions to the amount spent, may not be “worth it.”

Marginal Products
Under most conditions, marginal products are always going to be non-negative. Why?
Can ΔH/Δx (where x = health care) be negative?
<A> Yes! 2 Possibilities

Iatrogenic (physician caused) disease
Iatrogenic (physician caused) disease. All procedures have their risks. For example, in anesthesia, you kill someone a little bit -- You may do it too much.
Suppose, that the more we do, the higher the risk.
More care gives lower marginal product, higher risk.
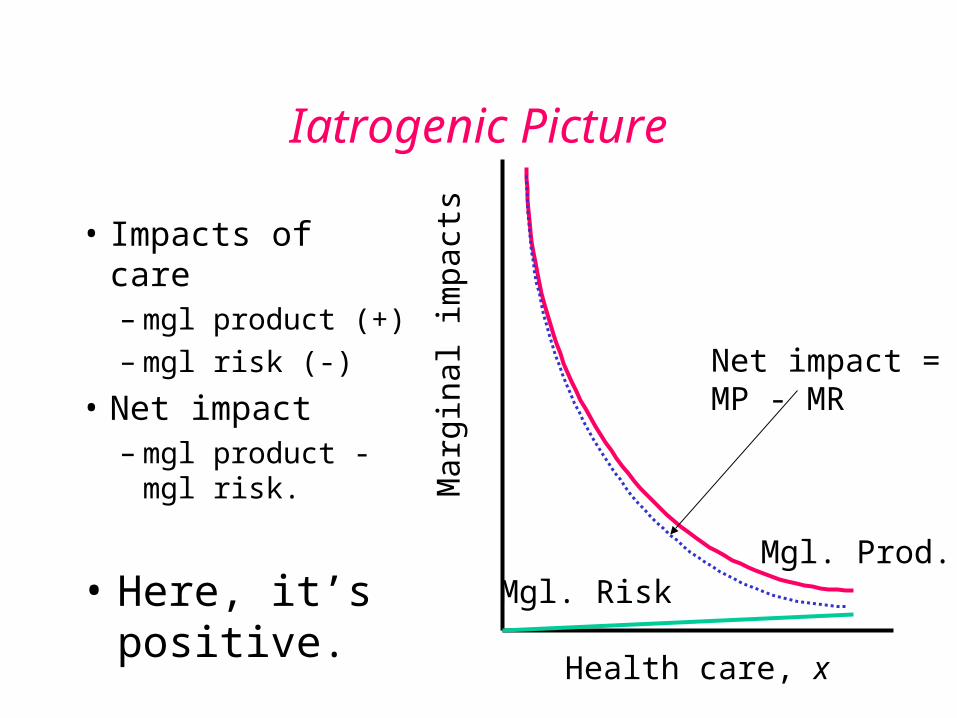
Iatrogenic Picture
• Impacts of care– mgl product (+)– mgl risk (-)
• Net impact– mgl product -
mgl risk.
Health care, x
Mar
gina
l im
pact
s
Mgl. Prod.Mgl. Risk
Net impact =MP - MR
• Here, it’s positive.
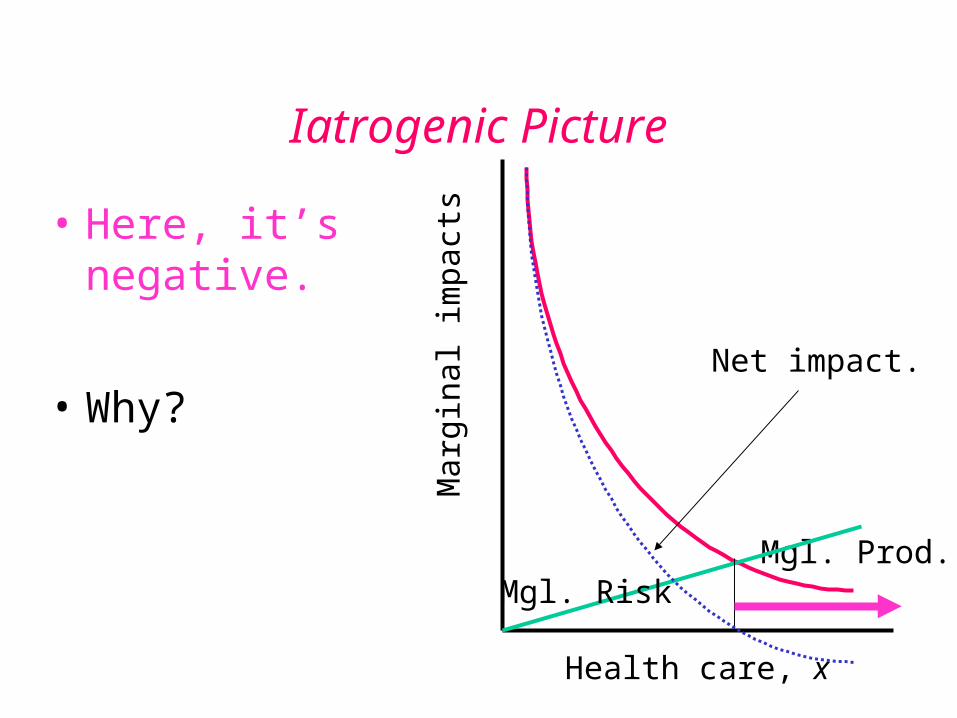
Iatrogenic Picture
Health care, x
Mar
gina
l im
pact
s
Mgl. Prod.Mgl. Risk
Net impact.
• Here, it’s negative.
• Why?
Examples of Iatrogenic (physician caused) disease
Examples: smallpox vaccine is a prime example;
Medical malpractice may be a another (i.e. the more done, the more possible mistakes).
Medicalization of Health Care
Ivan Illich has argued that the medicalization (substituting medical for home care) of health care could effectively lead to less personal consumer effort to produce health.
How would this work?Can you think of an example?
On the Historical Role of Medicine and Health Care
McKeown focused on dramatic rise in population in England and Wales since 1750.
It seems that world population rose and fell without any upward trend, up until that time.
How does population increase? (Discuss)
<A> Increased births
Decreased deaths
Increased in-migration
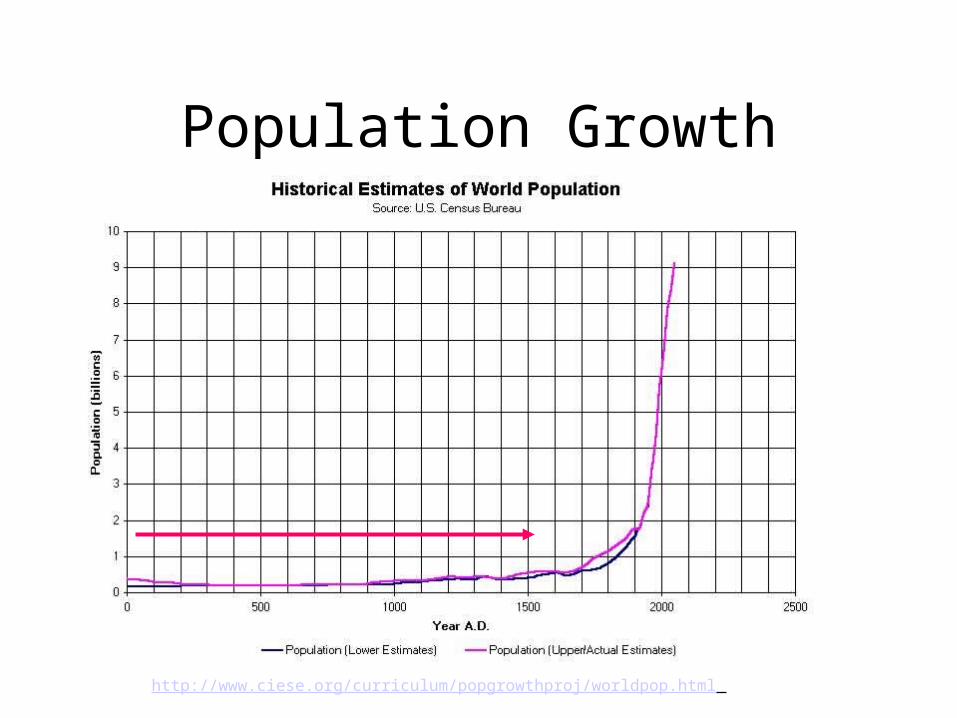
Population Growth
http://www.ciese.org/curriculum/popgrowthproj/worldpop.html
KEY !!!
Decreased deaths due to:
1. airborne causes -- tuberculosis, bronchitis, pneumonia, and influenza
2. waterborne causes
[Table 5.1].
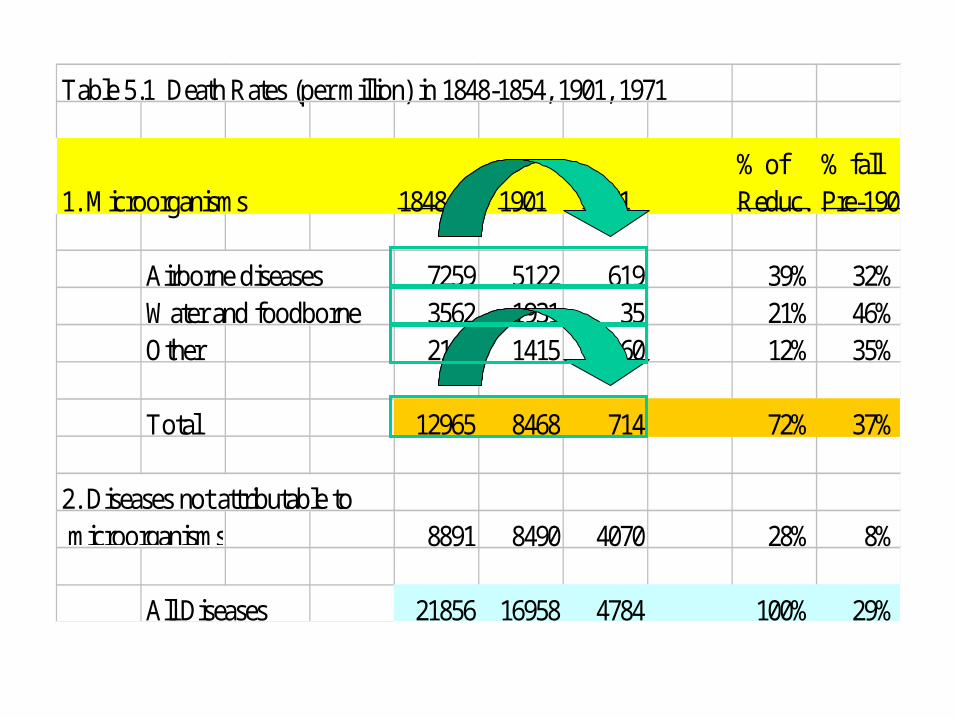
Table 5.1 Death Rates (per million) in 1848-1854, 1901, 1971
% of % fall1. Microorganisms 1848-54 1901 1971 Reduc. Pre-1901
Airborne diseases 7259 5122 619 39% 32%Water and foodborne 3562 1931 35 21% 46%Other 2144 1415 60 12% 35%
Total 12965 8468 714 72% 37%
2. Diseases not attributable to microorganisms 8891 8490 4070 28% 8%
All Diseases 21856 16958 4784 100% 29%
Public Health
If not medical care, than what?
McKeown argues that it’s public health
Immunization of populations
Quarantines
Sanitary standards for water and sewage
Sanitary standards for food handling and treatment
Key point, though is increased nutrition
Fogel - Increased Nutrition
“Infectious disease creates a relationship between host and parasite. While control of the parasite is directly helpful in reducing disease incidence, the condition of the host helps to determine its resistance to disease. A person who is better housed, better rested, and ... better fed, will be more resistant and less likely to die subsequent to exposure.” [FGS/4, Ch. 5]
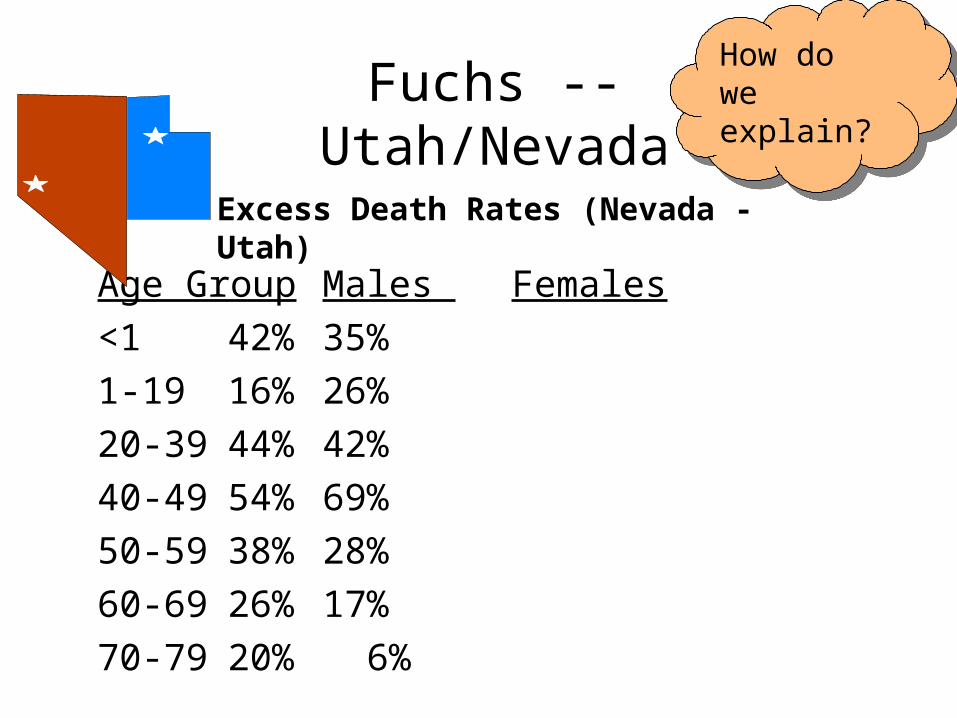
Age Group Males Females
<1 42% 35%
1-19 16% 26%
20-39 44% 42%
40-49 54% 69%
50-59 38% 28%
60-69 26% 17%
70-79 20% 6%
Fuchs -- Utah/Nevada
Excess Death Rates (Nevada - Utah)
How do we explain?
How do we explain?
Neonate Mortality• Table 5.3 looks at neonate mortality. Rate is the ratio of
infant deaths aged 1 month or less per thousand live births. It fell 1964-1982 from 17.9 to 7.7. Corman, Joyce, and Grossman were able to estimate the contributions of specific types of medical care and specific types of neonate-related programs.
• WIC - Women, Infants and Children (improved nutrition program) is means tested, directed toward the poor.
• For whites - 25% of the reduction can be explained
• For blacks - 56% can be explained.
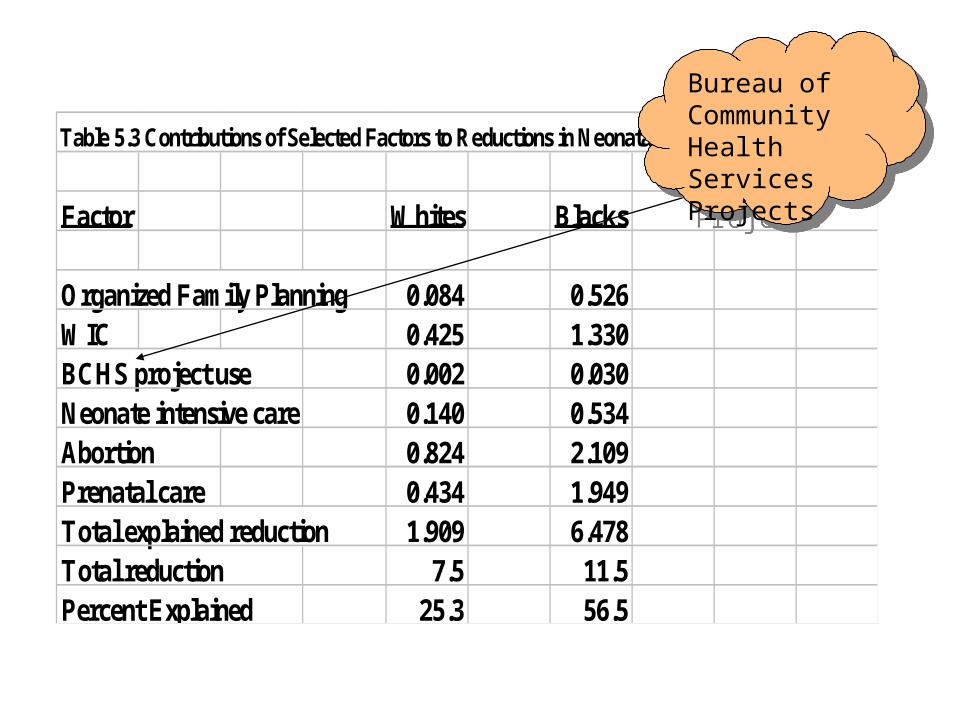
Table 5.3 Contributions of Selected Factors to Reductions in Neonatal Mortality Rates
Factor Whites Blacks
Organized Family Planning 0.084 0.526WIC 0.425 1.330BCHS project use 0.002 0.030Neonate intensive care 0.140 0.534Abortion 0.824 2.109Prenatal care 0.434 1.949Total explained reduction 1.909 6.478Total reduction 7.5 11.5Percent Explained 25.3 56.5
Bureau of Community Health Services Projects
Bureau of Community Health Services Projects

Morbidity
Mortality is useful because it is easy to measure. Morbidity refers to illness.
What might we expect? If most diseases are either self-limiting, or irreversible, the possibilities for additional medical services to reverse morbidity are small. May work for some services (hypertension, periodontal disease), and not for others. That's about what is found.
Schooling - Two Different Theories
• Grossman - Educated people produce health more efficiently. Why? If so, it makes sense to transfer resources from medical care to education.
• Fuchs - Education is an investment with a long time horizon. So is health! Since individuals with low time discount rates, or “long time horizons” will tend to invest both in education and health, the two (health and education) will be correlated. No explicit link.
• This debate has been around for a while, and they’re still arguing about it.

MC
CutlerStarts with a simple model:
U = V(q) – C(q), where q = health output
To maximize total utility
Mgl. Value = Mgl. Cost
Nothing profound here.
What we’ve done thus far in all of our analyses today is Mgl cost. What about Mgl value?
$
q
TC
TB
MB
q*
Increasing MC Δs
Decreasing MB Δs

Example
Studies have shown that we’re willing to pay $300 (MC) for an air bag. What are MB?
Air bag will save life of 1 in 10,000. So:MC for airbags ≤ MB for airbags$300 ≤ probability of dying * Value of life
.0001 * Value of lifeValue of life ≥ $300/0.0001 = $3,000,000Depending on how we discount it, this is worth
about $100,000 per year.
Look at Cardiovascular Care
Cutler asserts that “average 45 year old” will spend $30,000 in present value on CV care.
Average person will live 3 years longer because of the medical advance? Is it worth it? Who is average?
Turns out that average discounted benefit is $120,000.
Yes, it is worth it!
B/C=120/30 = 4!
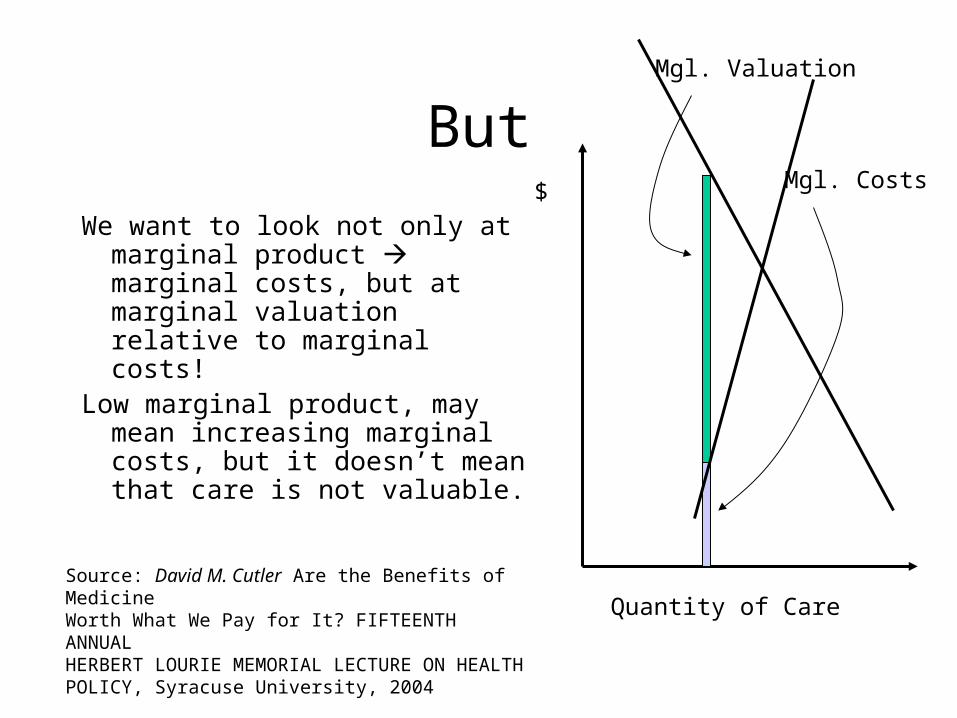
But
We want to look not only at marginal product marginal costs, but at marginal valuation relative to marginal costs!
Low marginal product, may mean increasing marginal costs, but it doesn’t mean that care is not valuable.
$
Quantity of Care
Mgl. Valuation
Mgl. Costs
Source: David M. Cutler Are the Benefits of MedicineWorth What We Pay for It? FIFTEENTH ANNUALHERBERT LOURIE MEMORIAL LECTURE ON HEALTH POLICY, Syracuse University, 2004







![Owner's Manual – MAGURA HS...Type name HS 11 HS 22 HS 33 Clamping Ø brake lever(E) [TD] mm 22+0.3/-0.1 Cantilever socket distance(F) 80±.2.0 Cantilever socket brake track area](https://static.documents.pub/doc/80x56/61176bf6c9c8cd257f121f33/owners-manual-a-magura-hs-type-name-hs-11-hs-22-hs-33-clamping-brake-levere.jpg)








