147
Professional Development Programme for Organ Donation Diagnosis of Death Masterclass Alex Manara Dale Gardiner Paul Murphy 31 March 2010 “Improving organ donation within your hospital” 1
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | thomasine-george |
| View: | 216 times |
| Download: | 2 times |
Professional Development Programme for Organ Donation
Diagnosis of Death Masterclass
Alex ManaraDale GardinerPaul Murphy
31 March 2010
“Improving organ donation within your hospital”
1

Professional Development Programme for Organ Donation2
Professional Development Programme for Organ Donation3
Diagnosis of Death MasterclassThe six big wins

Professional Development Programme for Organ Donation4
Diagnosis of Death Masterclass
2. Increased diagnosis of brain stem death
3. Increased donation after cardiac death
Professional Development Programme for Organ Donation
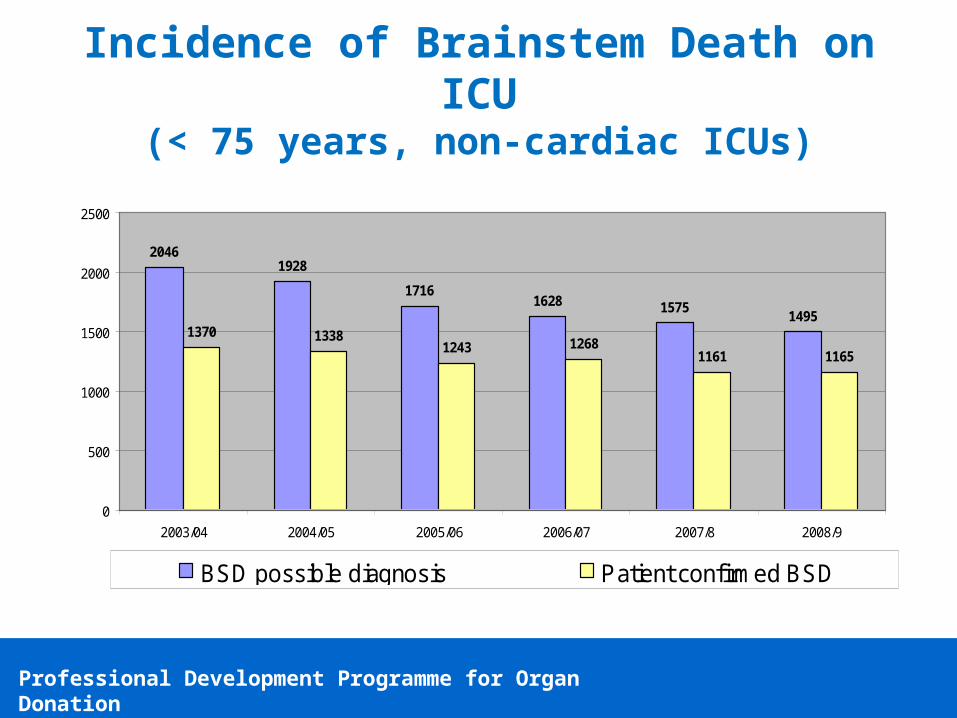
20461928
17161628 1575
14951370 1338
1243 12681161 1165
0
500
1000
1500
2000
2500
2003/04 2004/05 2005/06 2006/07 2007/8 2008/9
BSD possible diagnosis Patient confirmed BSD
Incidence of Brainstem Death on ICU(< 75 years, non-cardiac ICUs)
Professional Development Programme for Organ Donation
20461928
17161628 1575
14951370 1338
1243 12681161 1165
0
500
1000
1500
2000
2500
2003/04 2004/05 2005/06 2006/07 2007/8 2008/9
BSD possible diagnosis Patient confirmed BSD
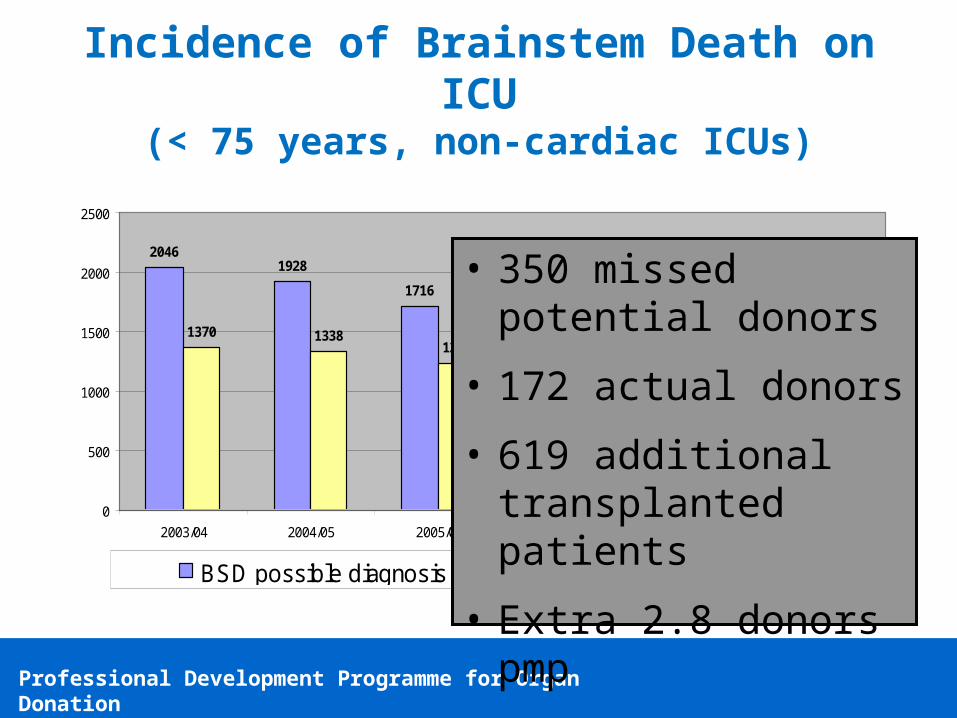
Incidence of Brainstem Death on ICU(< 75 years, non-cardiac ICUs)
• 350 missed potential donors
• 172 actual donors
• 619 additional transplanted patients
• Extra 2.8 donors pmp

Professional Development Programme for Organ Donation
Diagnosis of Brainstem Death
Reasons for not testing (approx 650 / year)
30.4
28.1
14.6
11
8.4
6.1
0.7
0.7
0 10 20 30 40
cardiovascular instability
unknow n
residual neurological function
family-related
problems w ith testing
contra-indication to donation (including age)
coroner
others
% total
Reasons for not testing (approx 350 / year)
Professional Development Programme for Organ Donation
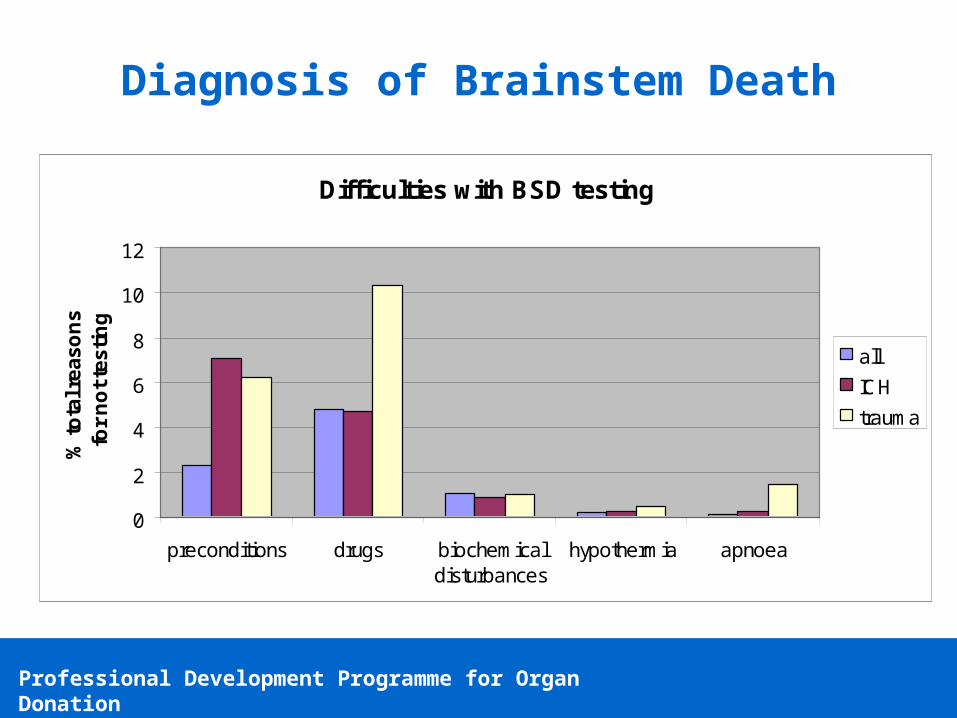
Diagnosis of Brainstem Death
Difficulties with BSD testing
0
2
4
6
8
10
12
preconditions drugs biochemicaldisturbances
hypothermia apnoea
% t
ota
l re
as
on
s f
or
no
t te
sti
ng
all
ICH
trauma
Professional Development Programme for Organ Donation
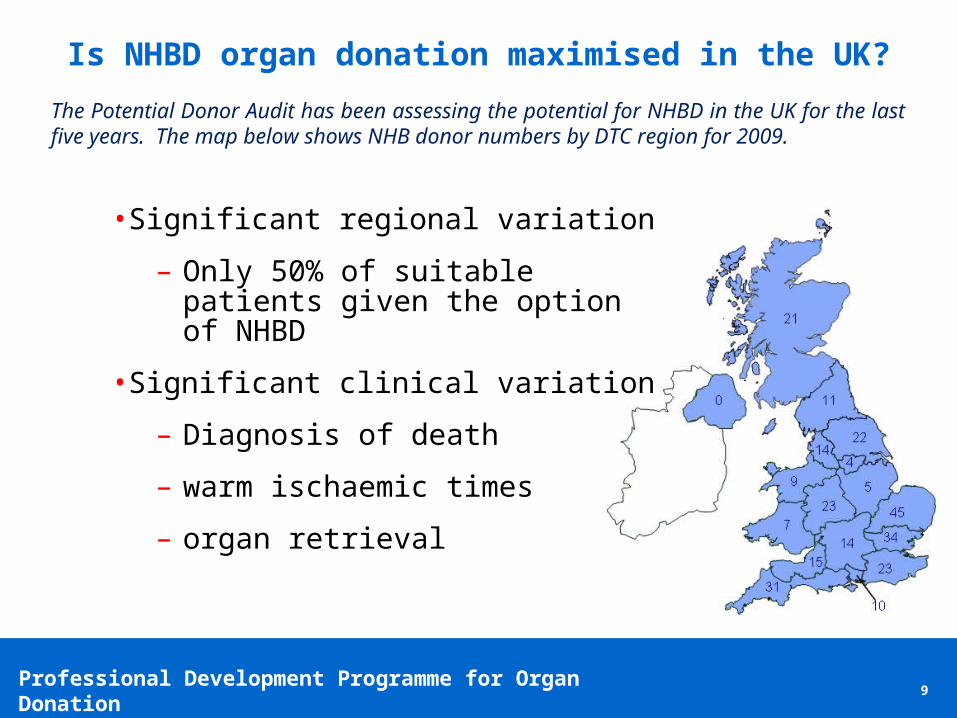
• Significant regional variation
– Only 50% of suitable patients given the option of NHBD
• Significant clinical variation
– Diagnosis of death
– warm ischaemic times
– organ retrieval
Is NHBD organ donation maximised in the UK?
9
The Potential Donor Audit has been assessing the potential for NHBD in the UK for the last five years. The map below shows NHB donor numbers by DTC region for 2009.
Professional Development Programme for Organ Donation10
Aims:
1. Promote national consistency in the use of the criteria used to diagnose death.
2. You to feel confident in the criteria used to diagnose death whilst being alert to potential pitfalls.
3. For you to be aware of potential criticisms by colleagues and the literature and have thought about possible counter arguments.

Professional Development Programme for Organ Donation
Agenda
1 Introduction 09.30-09.45
2 Diagnosis of Death: A defence of the British criteria 09.45-10.15
3 Quiz: Dead or not dead? 10.15-10.30
Break 10.30-10.40
4 The confirmation of death 10.40-11.15
5 Case study activity 11.15-12.15
6 Questions 12.15-12.25
7 Summary & close 12.25-12.30
11

A Defence of the British Criteria
Dale Gardiner
12

Professional Development Programme for Organ Donation13
30 years on…
Professional Development Programme for Organ Donation
UK criticsDavid EvansDavid HillPhilip Keep
Critics
Rinaldo Bellomo
Margaret Lock
Alan Shewmon
14
Edmund Pellegrino
Peter Singer

Professional Development Programme for Organ Donation15
Professional Development Programme for Organ Donation16
Criteria for Human Death
= The irreversible cessation of brain-stem function
=> Irreversible unconsciousness + Irreversible apnoea
=> intra-cranial or extra-cranial cause
DO NOT restore Cerebral Circulation
=> 5 mins absent cerebral circulation
Professional Development Programme for Organ Donation17
Professional Development Programme for Organ Donation18
Professional Development Programme for Organ Donation19
Transplant Technique• Split livers• Marginal Donors
Immunosuppressants• Tacrolimus• Mycophenolate
Professional Development Programme for Organ Donation20
Professional Development Programme for Organ Donation21
Brain Death
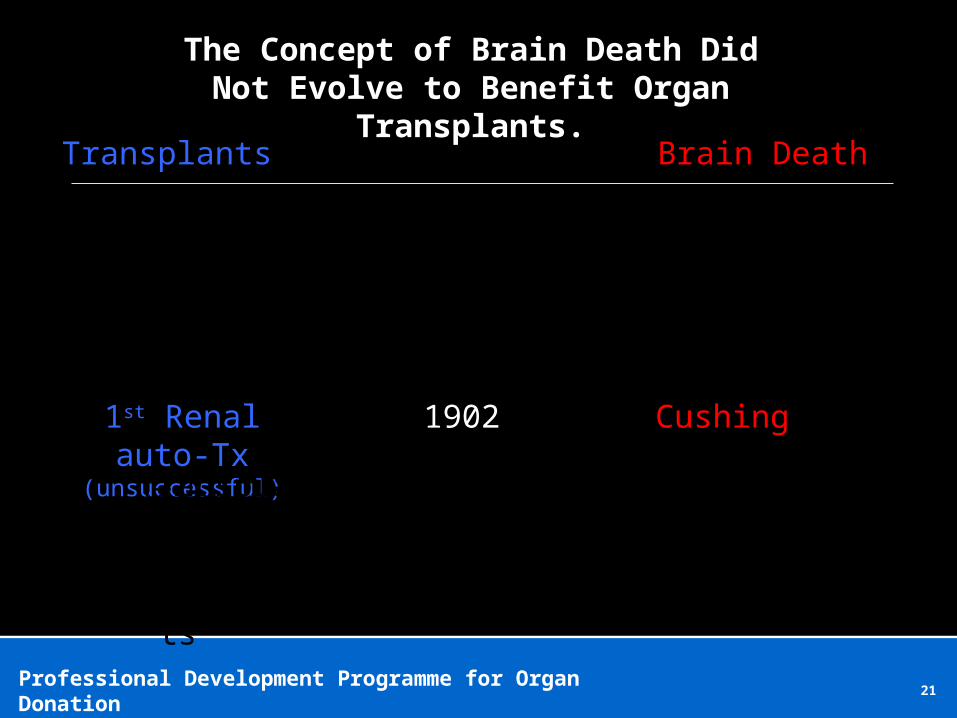
Cushing1st Renal auto-Tx(unsuccessful)
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplantsTransplantsTransplants
Transplants
1902
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.

Professional Development Programme for Organ Donation22
Brain Death
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplantsTransplants
Transplants
1902
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.
1st xeno-Tx (unsuccessful)
EEG discovered In electric potential =
Death
Loss cortical potentials seen in ischaemia1st Renal cadaveric Tx
(unsuccessful)1950
Professional Development Programme for Organ Donation23
Brain Death
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplants
Transplants
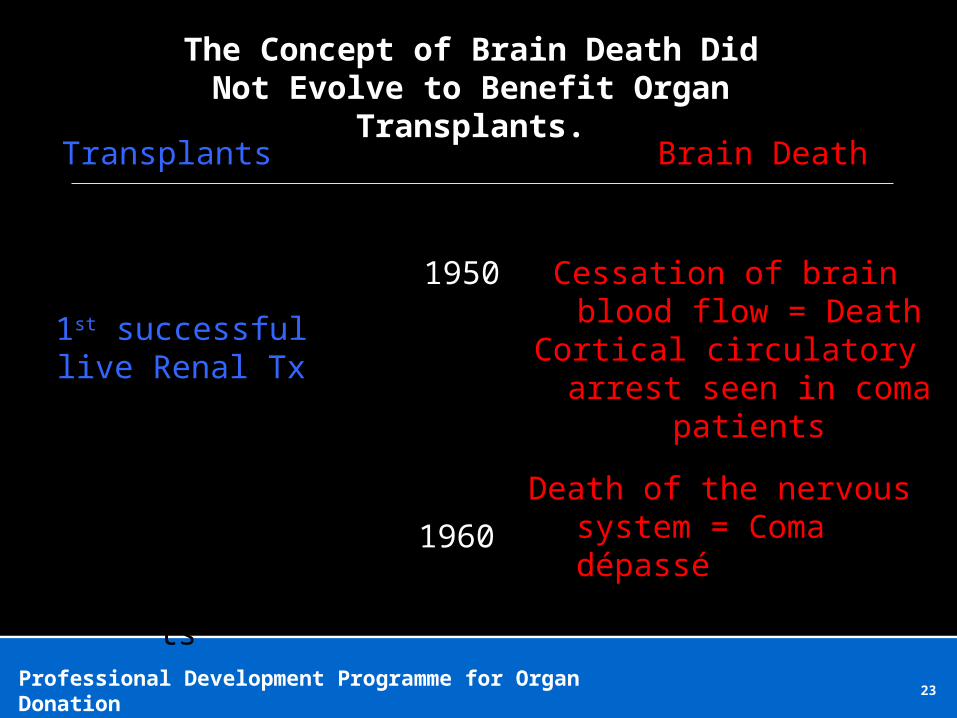
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.
1950 Cessation of brain blood flow = Death
Cortical circulatory arrest seen in coma patients
1st successful live Renal Tx
1960Death of the nervous system
= Coma dépassé
Professional Development Programme for Organ Donation24
Brain Death
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplants
Transplants
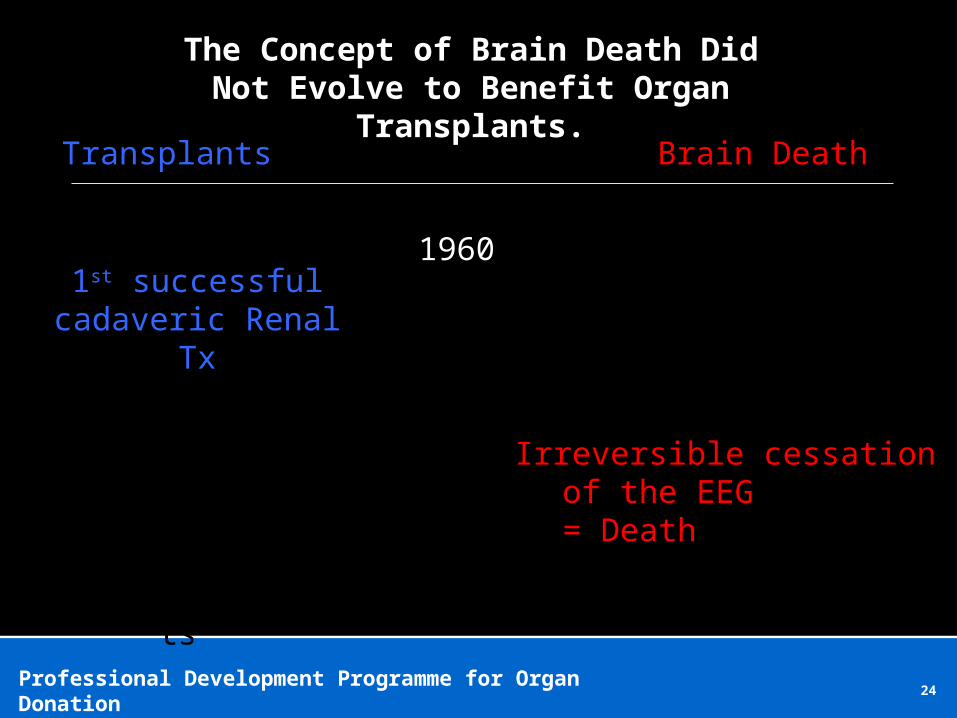
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.
19601st successful
cadaveric Renal Tx
Irreversible cessation of the EEG= Death

Professional Development Programme for Organ Donation25
Brain Death
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplants
Transplants
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.
1967-68
1st successful Heart Tx
Harvard CriteriaBrain Death = DEATH
Professional Development Programme for Organ Donation26
3rd December 1967

Professional Development Programme for Organ Donation27
Ad Hoc Committee of the Harvard Medical SchoolJAMA
5th Aug 1968
Professional Development Programme for Organ Donation28

Professional Development Programme for Organ Donation29
‘Our Primary purpose is to define irreversible coma as a new criterion for death…
…Obsolete criteria for the definition of death can lead to controversy in obtaining organs for transplantation.’
Professional Development Programme for Organ Donation30
Brain Death
TransplantsTransplantsTransplants
Transplants
TransplantsTransplantsTransplantsTransplantsTransplants
Transplants
The Concept of Brain Death Did Not Evolve to Benefit Organ Transplants.
Future
1st xeno Tx
1st lab grown organ Tx
Brain Death = DEATH

Professional Development Programme for Organ Donation31

Professional Development Programme for Organ Donation32

Professional Development Programme for Organ Donation33
diagnosis decision
Professional Development Programme for Organ Donation34

Professional Development Programme for Organ Donation35
Brain Stem Death
UK
Whole Brain Death
Rest of the World
Higher Brain DeathPhilosophers

Professional Development Programme for Organ Donation36
Higher Brain DeathPhilosophers
Peter Singer
Professional Development Programme for Organ Donation37
Whole Brain Death
Rest of the World
Rinaldo BellomoICM 2004

Professional Development Programme for Organ Donation38
Brain Stem Death UK

Professional Development Programme for Organ Donation39
Whole Brain DeathRest of the World
Professional Development Programme for Organ Donation40
Whole Brain DeathRest of the World
Professional Development Programme for Organ Donation41
Whole Brain DeathRest of the World
Professional Development Programme for Organ Donation42
Brain Stem Death UK
Professional Development Programme for Organ Donation43

Professional Development Programme for Organ Donation44
NEJM 2010
Professional Development Programme for Organ Donation45

Professional Development Programme for Organ Donation46
ALIVE DEAD
Professional Development Programme for Organ Donation47
Brain Stem DeathUK
Professional Development Programme for Organ Donation48
Brain Stem DeathUK

Professional Development Programme for Organ Donation49
Brain Stem DeathUK
Professional Development Programme for Organ Donation50
Professional Development Programme for Organ Donation51
Professional Development Programme for Organ Donation52
D. Alan Shewmon, MD

Professional Development Programme for Organ Donation53
Professional Development Programme for Organ Donation54
Professional Development Programme for Organ Donation55
Professional Development Programme for Organ Donation56
Doctors fight to save brain-dead mom’s foetus...
… for 3½ months

Professional Development Programme for Organ Donation57
Professional Development Programme for Organ Donation58
Whole Brain DeathRest of the World

Professional Development Programme for Organ Donation59
Brain Stem Death UK

Professional Development Programme for Organ Donation60
The inferior hypophysial artery is an artery supplying the posterior pituitary gland. It is a branch of the cavernous carotid artery (internal carotid artery) which is extradural at this point.
Professional Development Programme for Organ Donation61

Professional Development Programme for Organ Donation62
Professional Development Programme for Organ Donation63
Whole Brain DeathRest of the World
Professional Development Programme for Organ Donation64
Criteria for Human Death
= The irreversible cessation of brain-stem function
=> Irreversible unconsciousness + Irreversible apnoea

Professional Development Programme for Organ Donation65
Alan Shewmon MD

Professional Development Programme for Organ Donation66
‘Although we were unable to restore his consciousness or spontaneous breathing, the boy lived several more years.’
(page 195)

Professional Development Programme for Organ Donation67
Brain Stem DeathUK

Professional Development Programme for Organ Donation68
Professional Development Programme for Organ Donation69
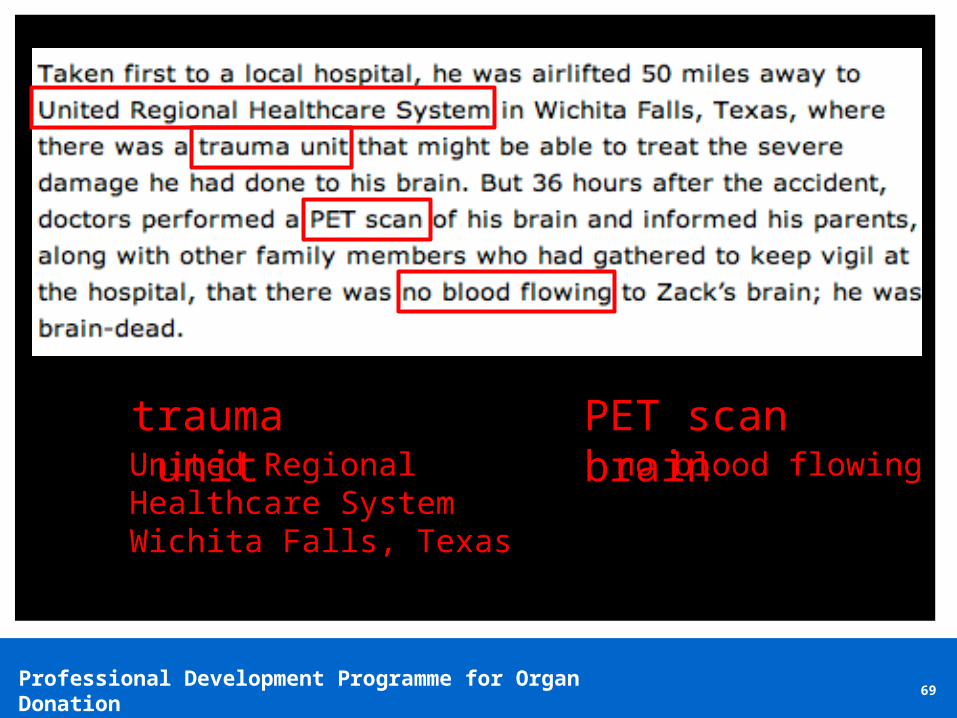
trauma unit PET scan brainno blood flowingUnited Regional
Healthcare System Wichita Falls, Texas
Professional Development Programme for Organ Donation70
Professional Development Programme for Organ Donation71
Regions only Level III Trauma Centre

Professional Development Programme for Organ Donation72
USA Trauma Center Level I - Highest toLevel III - Lowest

Professional Development Programme for Organ Donation73

Professional Development Programme for Organ Donation74

Professional Development Programme for Organ Donation75

Professional Development Programme for Organ Donation76
Professional Development Programme for Organ Donation77
Criteria for Human Death
= The irreversible cessation of brain-stem function
=> Irreversible unconsciousness + Irreversible apnoea
=> intra-cranial or extra-cranial cause
DO NOT restore Cerebral Circulation
=> 5 mins absent cerebral circulation
Professional Development Programme for Organ Donation78
75 seconds, 2 minutes, 5 minutes
2 minutes
5 minutes

Professional Development Programme for Organ Donation79
Dr Michael DeVitaUniversity of Pittsburgh
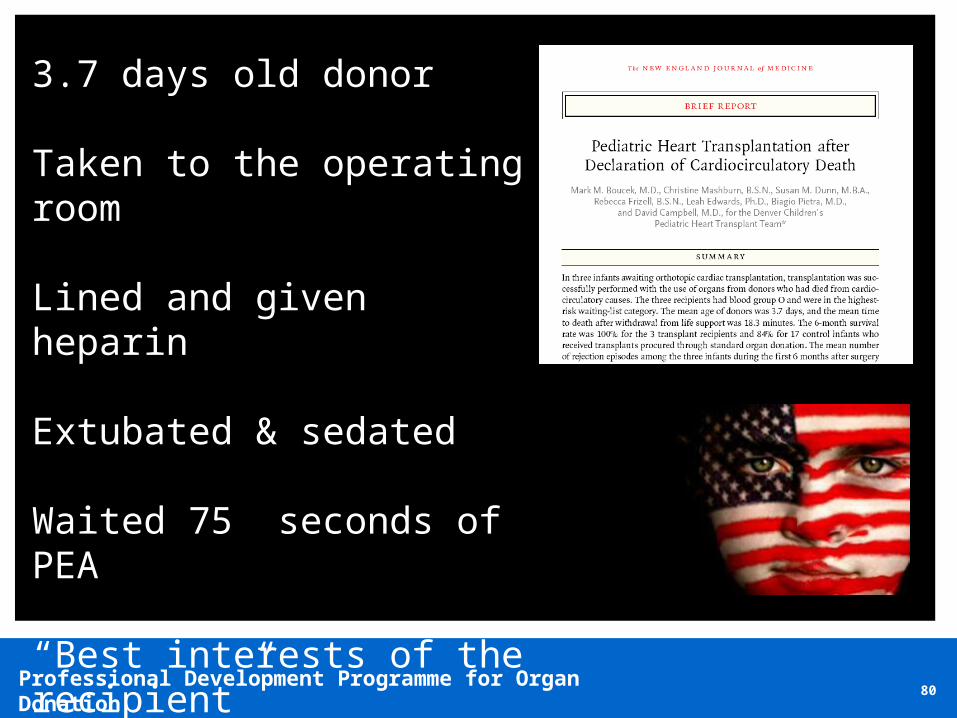
Professional Development Programme for Organ Donation80
3.7 days old donor
Taken to the operating room
Lined and given heparin
Extubated & sedated
Waited 75 seconds of PEA
“Best interests of the recipient”
Professional Development Programme for Organ Donation81

Professional Development Programme for Organ Donation82
Professional Development Programme for Organ Donation83
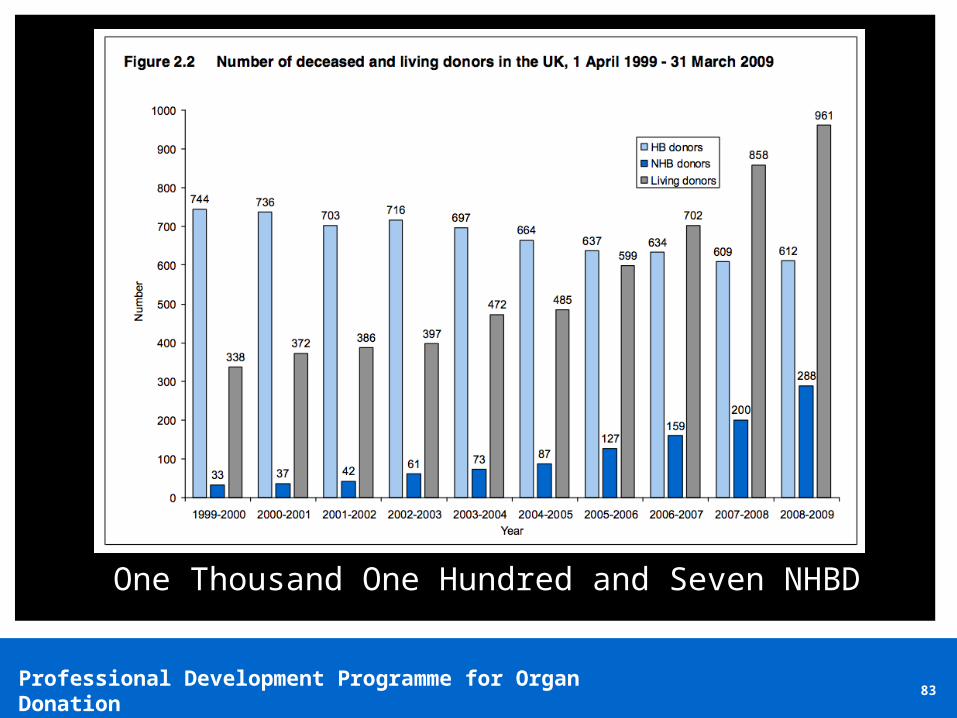
One Thousand One Hundred and Seven NHBD

Professional Development Programme for Organ Donation84
ALIVE DEAD
Professional Development Programme for Organ Donation85

Professional Development Programme for Organ Donation86
Questions?
Quiz: Dead or not Dead?
87
Professional Development Programme for Organ Donation8888
Question 1
1. The patient flexes their arm at the elbow following
imposition of a painful stimulus to the nail bed on that
side?
Dead - May represent a spinal reflex
Professional Development Programme for Organ Donation8989
Question 2
2. The ventilator registers the patient as making
spontaneous respirations?
Dead - May represent the heart beat creating flow
that is triggering ventilation
Professional Development Programme for Organ Donation9090
Question 3
3. The patient has a generalised tonic clonic seizure?
NOT brain stem dead – the patient must have intact
neural connections to have a grand mal fit
Professional Development Programme for Organ Donation9191
Question 4
4. The patient’s pulse increases from 70bpm to 110 bpm
during apnoea testing?
Dead - Hypercarbia (which occurs during apnoea
testing) results in endogenous adrenaline release.

Professional Development Programme for Organ Donation9292
Question 5
5. There is slow drift of one eye away from the ear in which
cold water is injected?
NOT brain stem dead – any eye movements in
response to caloric testing signifies the presence of
some reflex brain stem arc function.

Professional Development Programme for Organ Donation9393
Question 6
6. The patient sits up during apnoea testing (Lazarus sign)?
Dead - A spinal reaction to the acidosis which
follows hypercarbia. Very unsettling and disturbing!

Professional Development Programme for Organ Donation9494
How are you going?
These six questions were asked in the Australian JFICM
exam 2008 and the pass rate was only 65%!

Professional Development Programme for Organ Donation9595
Question 7
7. During an apnoea test on a mechanical ventilator after
20 seconds the patient starts to breathe and then
continues to breathe at 16 breaths per minute?
Dead – ventilator apnoea ventilation has kicked in.
Are you convinced not to do your apnoea tests still
connected to the ventilator?
Professional Development Programme for Organ Donation9696
Question 8
8. Supra-orbital painful stimulus leads to movement in one
of the arms?
Not dead – although one primarily looks for
movement in the cranial nerve distribution one must
actively ensure (by repetition) that this was a
coincidental spinal reflex but until proven this may
represent the patient is not brain stem dead.

Professional Development Programme for Organ Donation9797
Question 9
9. During the second set of brain stem testing the second
clinician finds the ears full of wax and can't visualise the
drum?
Not dead – this finding may invalidate the first
oculovestibular test and thus the patient may not be
dead.

Professional Development Programme for Organ Donation9898
Question 10
10.Due to left orbital trauma you can't visualise or observe
the left eye?
Dead – may still be dead even if one can’t carry out
the full test. Some of the options we discuss in our
case based discussions after morning tea.

Professional Development Programme for Organ Donation9999
Question 11
10.After a complete set of brain stem tests, confirming
clinical brain stem death, your colleague organises a CT
angiogram which reveals persisting intracerebral blood
flow?
Dead – Brain Stem Death is the UK Criteria
The Confirmation of Death
Alex ManaraICU Frenchay Hospital
100
Professional Development Programme for Organ Donation101101
Confirmation vs. Certification

Professional Development Programme for Organ Donation102102
600,000 UK deaths per annum

Professional Development Programme for Organ Donation103103
Confirming Death
• Cessation of heart beat
• Cessation of breathing
• Unresponsiveness
• Relatively easy to make
• Reproducible
• Recognizable
Professional Development Programme for Organ Donation104104
Confirming Death

Professional Development Programme for Organ Donation105105
Confirming Death: Most doctors.
Professional Development Programme for Organ Donation106106
Confirming Death: Neurosurgeons...

Professional Development Programme for Organ Donation107107
Confirming Death: Orthopods...
Professional Development Programme for Organ Donation108108
Confirming Death: What the public think...

Professional Development Programme for Organ Donation109109
The Law
• There is no statutory definition of death in the United Kingdom
(Unlike USA)
• The determination of death using neurological criteria has been
accepted by the courts of England and Wales.
• Otherwise you’re dead when a doctor says so = accepted medical
practice

Professional Development Programme for Organ Donation110110
Variation in Practice
Professional Development Programme for Organ Donation111111
What is accepted medical practice?
Professional Development Programme for Organ Donation112112
Definition of death
“The irreversible loss of those essential characteristics which are necessary to the existence of a living human person”
=
“The irreversible loss of the capacity for consciousness, combined with the irreversible loss of the capacity to breathe”
Professional Development Programme for Organ Donation113113
All Death is Brain Death
1. Cardio-respiratory determination of death
2. Neurological determination of death
3. Somatic determination of death
Professional Development Programme for Organ Donation114114
Cardio-respiratory criteria
“The heart and lung are not important as basic prerequisites to continue
life but rather because the irreversible cessation of their functions shows
that the brain has ceased functioning”
Professional Development Programme for Organ Donation115115
Cardio-respiratory criteria
• Need to be applicable to primary care / out of hospital setting
• Simultaneous and irreversible onset of apnoea, and
unconsciousness in the absence of a circulation.
• Irreversible cessation of brain stem function rapidly follows
Professional Development Programme for Organ Donation116116
Preconditions for cardiac criteria
• Decision made to abandon CPR
• The individual meets the criteria for not attempting CPR (ROLE)
• Active treatment is being withdrawn as declared not in the patient’s
best interests
• Patient has an advance directive refusing CPR

Professional Development Programme for Organ Donation117117
At “asystole”
• Person confirming death present and continuously observes apnoea,
asystole and unresponsiveness for a minimum of 5 minutes
• Absent circulation confirmed clinically or with monitors
• Return of circulation or respiration prompts start of a further 5
minutes from point of next cardio-respiratory arrest
• Confirm absent pupillary and corneal reflexes and no central
response to pain
Professional Development Programme for Organ Donation118118
At “asystole”
• Person confirming death present and continuously observes apnoea,
asystole and unresponsiveness for a minimum of 5 minutes
• Absent circulation confirmed clinically or with monitors
• Return of circulation or respiration prompts start of a further 5
minutes from point of next cardio-respiratory arrest
• Confirm absent pupillary and corneal reflexes and no central
response to pain

Professional Development Programme for Organ Donation119119
Irreversibility
• Heart will not be restarted because patient not for CPR
• Cardiac activity will not resume spontaneously
• Cannot be restarted even with CPR
No post-mortem procedures that have the potential to restore cerebral perfusion

Professional Development Programme for Organ Donation120120
Post mortem Interventions
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_108827.pdf

Professional Development Programme for Organ Donation121121
Post Mortem Interventions
Anything that places the person at risk of serious harm or distress is
unlikely ever to be in the person’s best interests. (CPR, femoral
cannulation, heparinisation)

Professional Development Programme for Organ Donation122122
International Differences
• 2 minutes
Pittsburgh protocol 1993
ANZICS
• Minimum of 2 minutes, no more than 5 minutes recommended
Society of Critical Care Medicine, USA
• Minimum of 5 minutes:
Academy of Medical Royal Colleges UK
Intensive Care Society, UK
Institute of Medicine, USA
Canadian Council for Donation and Transplantation
• Minimum of 10 minutes
Maastricht Conference, Holland
Professional Development Programme for Organ Donation123123
Professional Development Programme for Organ Donation124124
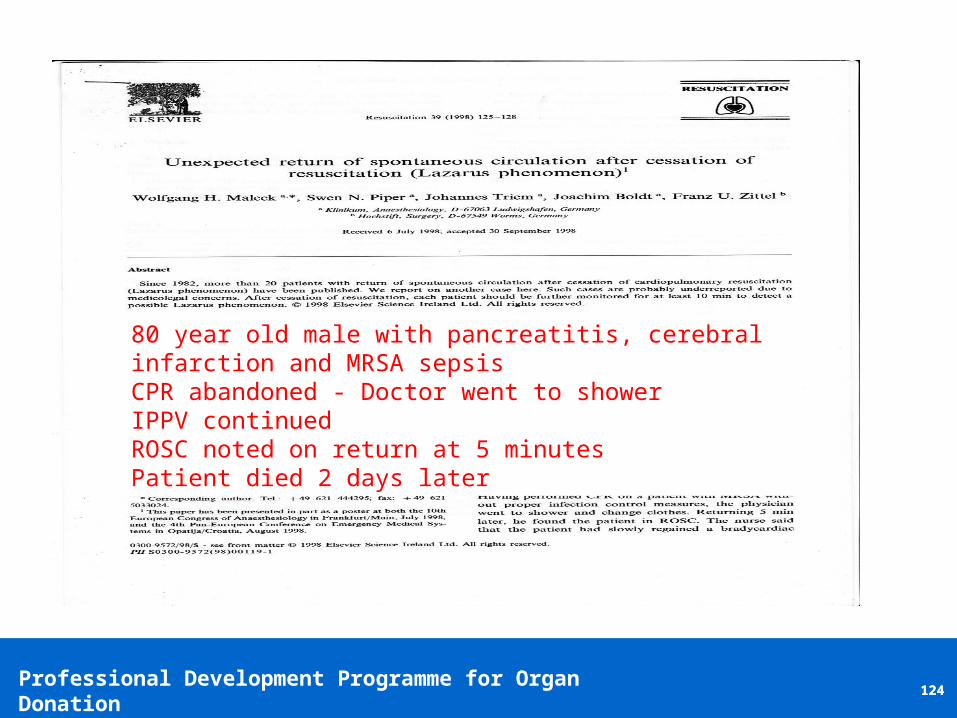
80 year old male with pancreatitis, cerebral infarction and MRSA sepsisCPR abandoned - Doctor went to showerIPPV continuedROSC noted on return at 5 minutesPatient died 2 days later

Professional Development Programme for Organ Donation125125
UK Deceased Organ Donors
Professional Development Programme for Organ Donation126126
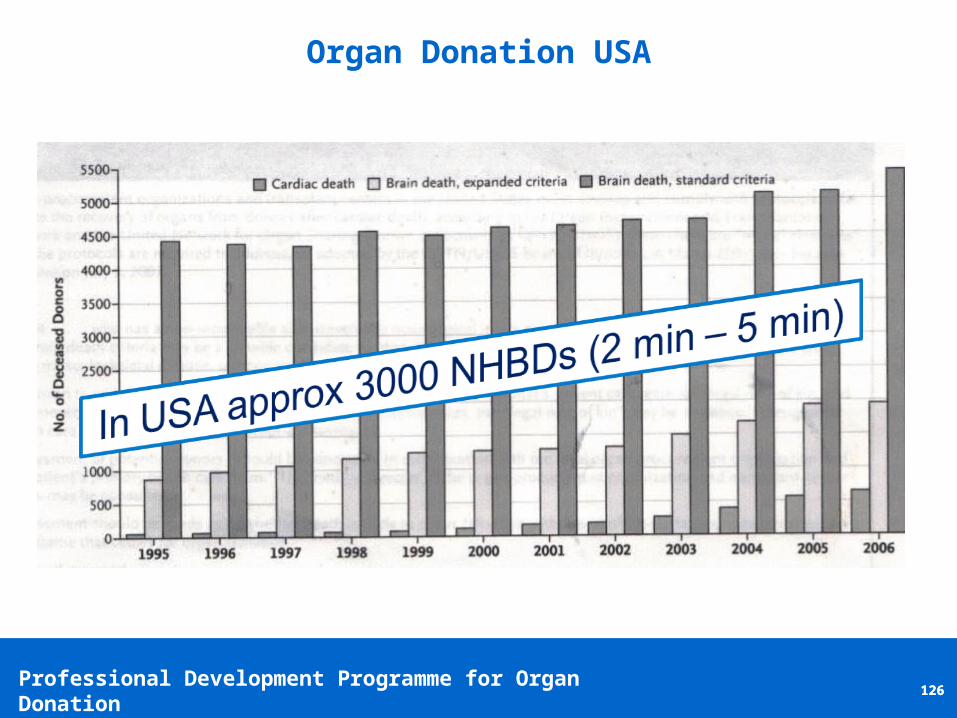
Organ Donation USA

Professional Development Programme for Organ Donation127127
Lazarus?
Is auto-resuscitation a result of not having a standardised way of
confirming death and also defining what can and cannot happen after
death?
Professional Development Programme for Organ Donation128128
Neurological Determination of Death in UK
Professional Development Programme for Organ Donation129129
History
• Improved ICU care of comatose
patients
• Coma depassé described in
Paris in 1959
• Deep irreversible coma
• Nearly always followed by
cardiac arrest

Professional Development Programme for Organ Donation130130
Cardiac Prognosis After NDD
Pallis 1987:
1300 patients all developed cardiorespiratory arrest even with full
support
Hung et al 1995:
•73 adults and children
• Full and continued CVS support
• All became asystolic; within 10 days

Professional Development Programme for Organ Donation131131
Rationale for New Guidelines
• Variable practice when
guidelines not specific
• Guidelines not always followed
even when specific

Professional Development Programme for Organ Donation132132
New Guidelines
• Published 2008
• Attempts further standardisation
• Primarily a clinical diagnosis
• Clinical judgement still required

Professional Development Programme for Organ Donation133133
Neurological Determination of Death in UK
1. Patient in deep apnoeic coma
Professional Development Programme for Organ Donation134134
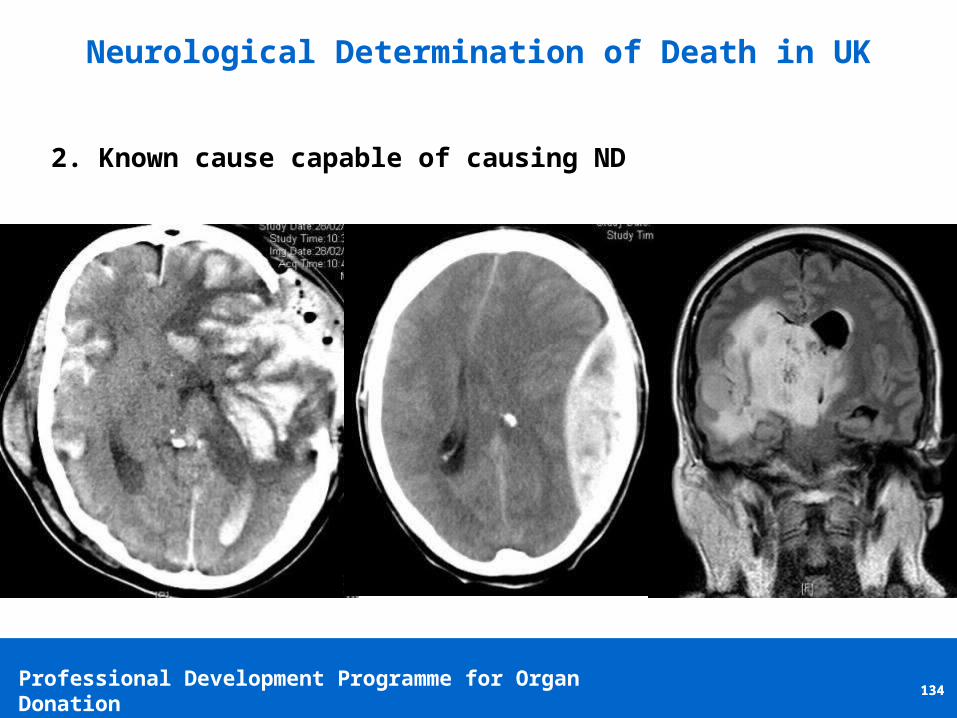
Neurological Determination of Death in UK
2. Known cause capable of causing ND
Professional Development Programme for Organ Donation135135
Neurological Determination of Death in UK
• Primary hypothermia
• Metabolic disturbances
• Alcohol
• Depressant drugs
• Muscle relaxants
3. No reversible causes / confounding factors
Professional Development Programme for Organ Donation136136
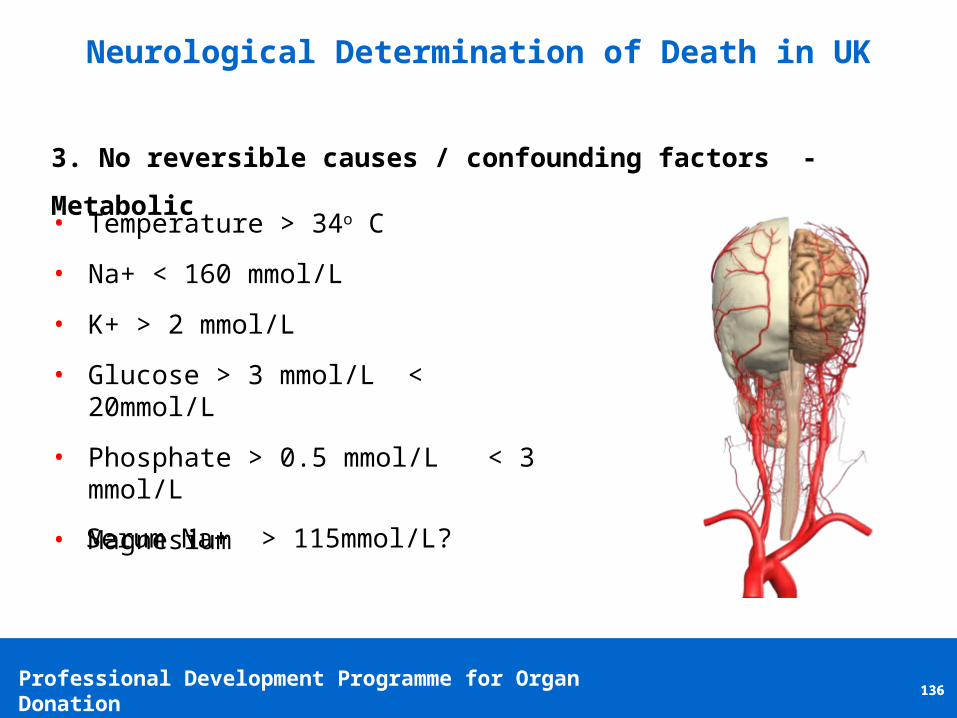
Neurological Determination of Death in UK
• Temperature > 34o C
• Na+ < 160 mmol/L
• K+ > 2 mmol/L
• Glucose > 3 mmol/L < 20mmol/L
• Phosphate > 0.5 mmol/L < 3 mmol/L
• Magnesium
3. No reversible causes / confounding factors - Metabolic
Serum Na+ > 115mmol/L?

Professional Development Programme for Organ Donation137137
Neurological Determination of Death in UK
• Clinical judgement essential
• Impossible to create rules covering every situation
• Difficulties mainly with thiopentone and midazolam
• Plasma concentrations not good predictors of effect
• Use of antagonists may help
• Ideally use non cumulative drugs – propofol, remifentanil
3. No reversible causes / confounding factors - Sedatives
Professional Development Programme for Organ Donation138138
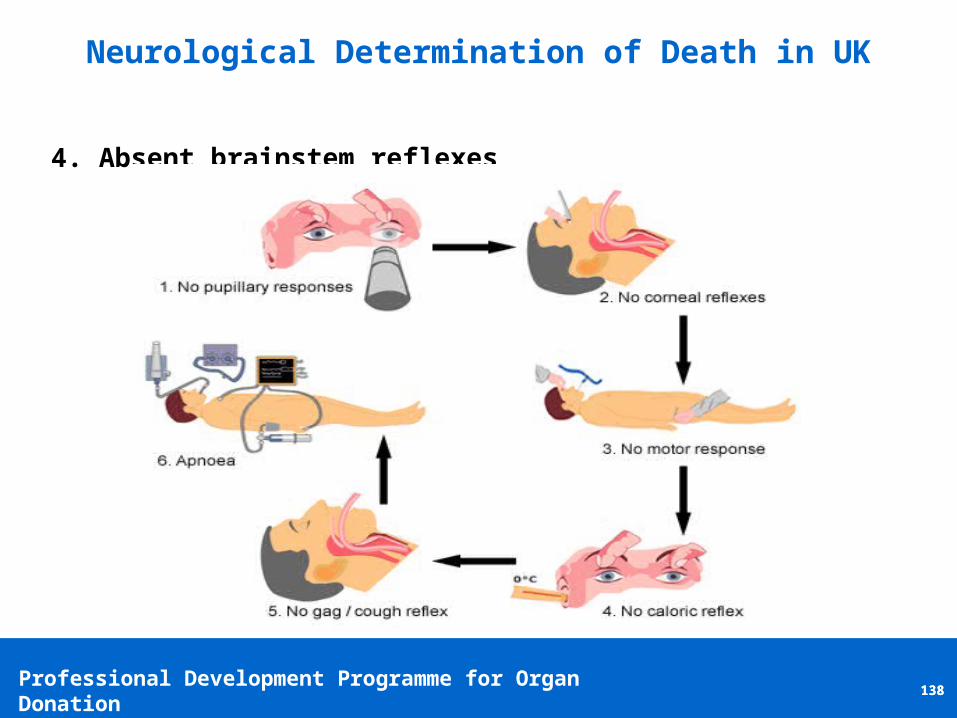
Neurological Determination of Death in UK
4. Absent brainstem reflexes
Professional Development Programme for Organ Donation139139
Neurological Determination of Death in UK
• Must be done last after other reflexes absent
• Undertaken no more than twice
• Achieve CVS stability at PaCO2 > 6kPa before disconnection
• Disconnect for 5 minutes
• Return PaCO2 to normal on reconnection
Apnoea Test

Professional Development Programme for Organ Donation140140
Neurological Determination of Death in UK
• 4 vessel cerebral angiography
• CT angiography
• MRI angiography
• EEG
• TCD
• SPECT
• Brain stem evoked potentials
• Response to 2mg atropine
• ICP > MAP
5. Ancillary Tests
Professional Development Programme for Organ Donation141141
Whole Brain Death ?
http://video.bloodservices.ca/Streaming/nddvideo/
Professional Development Programme for Organ Donation142142
Reducing Variability in Practice
• Guidelines – Helpful but limited value
• CLODs – Professional Development Programme
• Development of international approach to confirmation
• Prospective observational studies on onset of asystole

Case Study Activity
143
Professional Development Programme for Organ Donation144144
Case Study Exercise
• We have 2 case studies which we would like you to discuss and
respond to in your table groups
• You each have a handout of the 2 case studies which provide a case
context and a series of questions
• We will spend 30 mins total on each case study, 15mins to discuss &
answer questions and15 mins to feedback as a wider group
• This part of the session will take an hour to complete and will be
followed by a more general Q&A

Professional Development Programme for Organ Donation145145
Case Study 1
A middle-aged woman presents to your Emergency Department at 1600
after collapsing at home. She has fixed pupils and is intubated without
drugs. CT head reveals catastrophic subarachnoid haemorrhage.
Neurosurgical opinion is that this is an unsurvivable situation and
withdrawal of life sustaining treatment is advised. The family approach
the ED staff suggesting their relative would wish to be an organ donor.
Brain death is suspected.
Professional Development Programme for Organ Donation146146
Case Study 2
A young man is admitted to your neuro-critical care unit with severe
traumatic brain injury. Despite aggressive treatment his pupils fix after
four days and irreversible cessation of brain stem function (brain stem
death) is suspected.
He has received substantial doses of sedatives (midazolam, alfentanil
and propofol).

Questions???
147
















