Professor David Williams, D.Sc.,F.R.Eng., Professor and Director of International Affairs, Wake Forest Institute of Regenerative Medicine, North Carolina, USA Editor-in-Chief, Biomaterials President-elect, Tissue Engineering & Regenerative Medicine Society International (TERMIS) Chairman and Director, Southern Access Technologies, South Africa Visiting Professor, Christiaan Barnard Department of Cardiothoracic Surgery, Cape Town, South Africa, Visiting Professor, Graduate School of Biomedical Engineering, University of New South Wales, Australia Guest Professor, Tsinghua University, Beijing and Visiting Professor, Shanghai Jiao Tong Medical University, China Emeritus Professor, University of Liverpool, UK
Transcript
Professor David Williams, D.Sc.,F.R.Eng., Professor and Director of International Affairs, Wake Forest Institute of
Regenerative Medicine, North Carolina, USA
Editor-in-Chief, BiomaterialsPresident-elect, Tissue Engineering & Regenerative Medicine Society International
(TERMIS)Chairman and Director, Southern Access Technologies, South Africa
Visiting Professor, Christiaan Barnard Department of Cardiothoracic Surgery, Cape Town,South Africa,
Visiting Professor, Graduate School of Biomedical Engineering, University of New SouthWales, Australia
Guest Professor, Tsinghua University, Beijing and Visiting Professor, Shanghai Jiao TongMedical University, China
Emeritus Professor, University of Liverpool, UK
Biocompatibility and War and Peace
Biocompatibility is a war zoneAnd war is a continuumConflict resolutionMay lead to quiescenceBut peaceLike biocompatibilityIs metastableInsurgencies, just as thrombus, can occurAt any timeIf defences are let downNew technologiesMaybe WMD at the nanoscaleLead to changes, andNew strategies of defence.
BiocompatibilityCan never be wonIt can be tamedAnd watched over, for ever
Williams D.F. On the mechanisms of biocompatibilityBiomaterials, 2008, 29, 2941
Williams D.F. On the nature of biomaterialsBiomaterials, 2009, 30, 5897
The Williams Definition ofBiocompatibility
‘The ability of a material toperform with an appropriate hostresponse in a specific application’
The Williams Dictionary of BiomaterialsLiverpool University Press, 1999
The Williams Definition of a Biomaterial
2009
A biomaterial is a substance that has been engineeredto take a form which, alone or as part of a complex system,
is used to direct, by control of interactions with components ofliving systems, the course of any therapeutic or diagnostic
procedure.
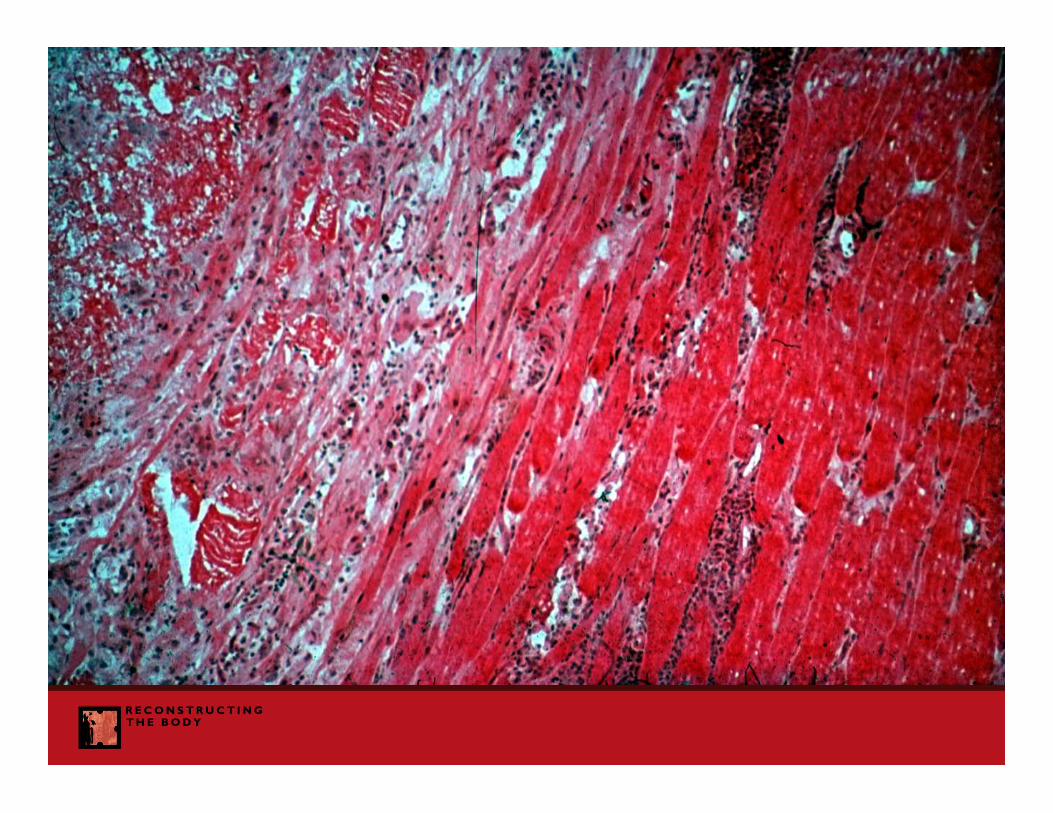
Implantable Medical Devices
Implantable Medical Devices•Long term biocompatibility and toxicology of metallic
systems are reasonably well known; do we need new alloys?
Implantable Medical Devices•Long term biocompatibility and toxicology of metallic
systems are reasonably well known; do we need new alloys?•Long term biocompatibility of biostable polymers isreasonably well known; do we need new polymers?
Implantable Medical Devices•Long term biocompatibility and toxicology of metallic
systems are reasonably well known; do we need new alloys?•Long term biocompatibility of biostable polymers isreasonably well known; do we need new polymers?•Long term response of bone to biomaterials is well
understood; do we need new bone-contacting surfaces?
Implantable Medical Devices
•Long term biocompatibility and toxicology of metallicsystems are reasonably well known; do we need new alloys?
•Long term biocompatibility of biostable polymers isreasonably well known; do we need new polymers?•Long term response of bone to biomaterials is well
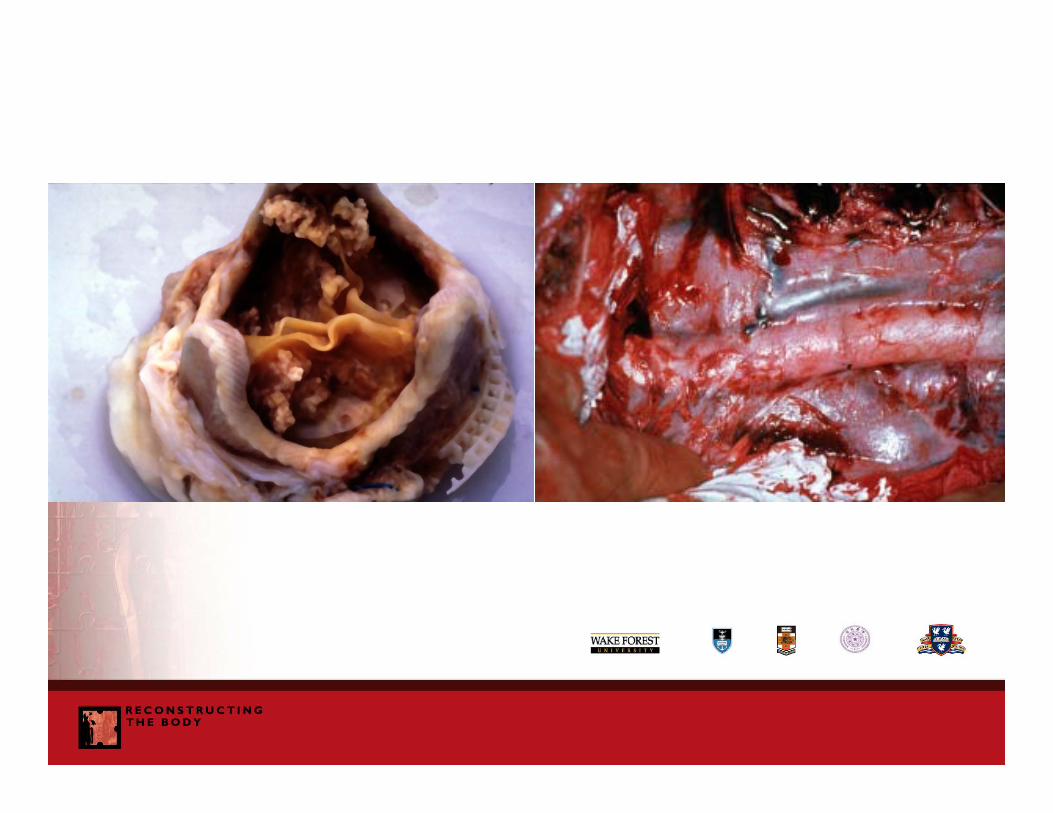
understood; do we need new bone-contacting surfaces?•Still have some issues with xenogeneic materials
•Still have some uncertainties over interactions with blood –endothelialization, thromboembolism etc
Biomaterial Performance
Always remember with the biocompatibility of medical devices, thethree most important mediators of clinical performance are, in this
order
• The Quality of the Surgery
• The Characteristics of the Patient
• The Inherent Biocompatibility of the Material
Implantable Degradable Systems
Implantable Device – Drug Combinations
Implantable Device – Drug Combinations
Drug – eluting stentsBMP releasing devices in the spine
Bisphosphonates in bone
Do we know sufficient about pharmacokinetics andpharmacodynamics in these systems to be sure of
mechanisms of action, efficacy and safety?
The ability of a material to perform with an appropriate hostresponse in a specific application
The scientific basis of biocompatibility involves theidentification of the causal relationships
between materials and host tissue such thatmaterials can be designed to elicit the
most appropriate response
This implies that it is possible to determineunequivocally the way in which material parameter X
influences host response Yand that knowing this, we can modify X in order to modulate Y
This is how we should determine the specifications for biomaterials
Material Variables
• Bulk material composition, microstructure, morphology,• Crystallinity and crystallography,• Elastic constants, compliance,• Surface chemical composition, chemical gradient, molecular
mobility,• Surface topography and porosity• Water content, hydrophobic – hydrophilic balance, surface
energy• Corrosion parameters, ion release profile, metal ion toxicity• Polymer degradation profile, degradation product toxicity• Leachables, catalysts, additives, contaminants• Ceramic dissolution profile• Wear debris release profile, particle size• Sterility and endotoxins
Host Response Characteristics
• Protein adsorption and desorption characteristics• Complement activation• Platelet adhesion, activation and aggregation• Activation of intrinsic clotting cascade• Neutrophil activation• Fibroblast behaviour and fibrosis• Microvascular changes• Macrophage activation, foreign body giant cell production• Osteoblast / osteoclast responses• Endothelial proliferation• Antibody production, lymphocyte behaviour• Acute hypersensitivity / anaphylaxis• Delayed hypersensitivity• Genotoxicity, reproductive toxicity• Tumour formation
The Reality for Implantable Devices
• The host response, involving both humoral and cellularcomponents is extremely complex,
• Several of these components involve amplification or cascadeevents,
• There is often a two-way relationship between the materialvariable and the host response e.g. a degradation process ispro-inflammatory and the products of inflammation enhance thedegradation process,
• Mechanical stability influences the host response, and in manysituations the host response determines the stability
• The host response is time dependent,• The host response is patient specific, depending on age,
gender, health status / concomitant disease, pharmacologicalstatus, lifestyle, etc.,
• Biocompatibility is species specific - testing materials in youngrats in Liverpool or Winston-Salem may be of no relevance tosenior citizens in Atlanta.
The Reality;Long-term Implantable Devices
It has proved impossible in virtually all situations topositively modulate the host response by
manipulation of the material variables.
In almost all situations, the practical consequence isthat we select devices that irritate the host the least,through the choice of the most inert and least toxic
materials and the most appropriate mechanicaldesign,
When selecting materials for long term implantabledevices, choose the material that optimises the
functional properties of the device, consistent withmaximum chemical and biological inertness
The biocompatibility of a long term implantablemedical device refers to the ability of the deviceto perform its intended function, with the desired
degree of incorporation in the host, withouteliciting any undesirable local or systemic effects
in that host.
Tissue Engineering
Tissue engineering is the creation of new tissue for thetherapeutic reconstruction of the human body, by the
deliberate and controlled stimulation of selectedtarget cells through a systematic combination of
molecular and mechanical signals
The Changing Nature of Biomaterials andMethods for their Evaluation
Tissue Engineering ProductsWe need to assess the intrinsic level of biological risk before a device is
used clinically We do not have high quality biomaterials for tissue engineering applications, and
we need new test procedures The failure to produce clinical success with tissue engineering products is partly
caused by the lack of standard testing and regulatory approval procedures Experience tells us the current pre-clinical test procedures are definitely not
predictive of clinical performance ISO 10993 is not a valid basis for testing new biomaterialsWe also need effective process validation systems for ensuring continuing
quality and safety Do we have the most effective procedures for quality control concerned with
biological safety?
Biocompatibility of Tissue EngineeringScaffolds and Matrices
The biocompatibility of a scaffold or matrix for a tissueengineering product refers to the ability to perform asa substrate that will support the appropriate cellularactivity, including the facilitation of molecular and
mechanical signalling systems, in order to optimisetissue regeneration, without eliciting any undesirable
local or systemic responses in the eventual host.
Previous FDA approval for the use of a biomaterial in a medical device is not anappropriate specification for a tissue engineering scaffold or matrix material
•Biocompatibility has to be determined in the context of theintended function of the product
•We need better systems for the determination of biologicalsafety
•We may have to re-define ‘surfaces’ in the new world ofnanostructured biomaterials
•We have to take the determination of biocompatibility out ofthe courtroom