39
Maternal sepsis Marian Knight Professor of Maternal and Child Population Health National Perinatal Epidemiology Unit Nuffield Department of Population Health

Maternal sepsis
Marian KnightProfessor of Maternal and Child Population Health
National Perinatal Epidemiology Unit
Nuffield Department of Population Health

Objectives
• To describe the main causes of maternal
sepsis in the UK
• To identify women at greater risk of
maternal sepsis
• To highlight actions to prevent and treat
maternal sepsis

Anna’s story
Hinton L
Anna was 21 years old. She already had
one son at home. When she came home
with her new baby she started to feel
unwell.

Anna’s story
Hinton L

Maternal deaths from genital
tract sepsis
Test for trend p=0.01

Maternal deaths from genital
tract sepsis
0.0
0.5
1.0
1.5
1985-87 1988-90 1991-93 1994-96 1997-99 2000-02 2003-05 2006-08
Rate
per
100,0
00 m
ate
rnit
ies
Source: Lewis G et al. Saving Mothers Lives 2006-8. BJOG 2011
Test for trend p=0.01

UK national study of severe sepsis
associated with pregnancy
• Affected women were identified between
2011 and 2012
• Information collected on the source of
infection, management, and the
subsequent consequences to both mother
and baby
0.0
0.5
1.0
1.5
1985-87 1988-90 1991-93 1994-96 1997-99 2000-02 2003-05 2006-08
Rate
pe
r 1
00
,00
0 m
ate
rnit
ies

Sepsis morbidity
• 365 women diagnosed with severe sepsis
associated with pregnancy over one year
(47 per 100,000 maternities)
• 71 women developed septic shock
(9 per 100,000 maternities)
• 5 women died
• For every woman who dies, 14 have septic
shock; a further 60 have severe sepsisAcosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Sources of severe sepsis
Genital tract 31%
Urinary tract20%
Wound9%
Respiratory5%
Other9%
Unknown26%
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)
37% (N=134) before delivery
UTI (34%)
63% (N=231) after delivery
Genital-tract (37%)
(P<0.0001)

Sources of sepsis – intensive care
Pregnant or recently pregnant women admitted to
UK intensive care units 2008-2010 (ICNARC data) Source of infection
Number of women
(n=646) Pneumonia/ respiratory infection 257 (39.8)
Genital tract 157 (24.3)
Urinary tract/kidney 59 (9.1)
Surgical trauma 24 (3.7)
Septicaemia 20 (3.1)
Appendicitis 19 (2.9)
Other infection 62 (9.6)
Unknown 48 (7.4)
Acosta C et al. 2016 (BMJ Open; 6(8):e012323)

Sources of infection
• Genital tract infection (classic “puerperal
fever”) forms only a small proportion of
maternal morbidity from infectious disease
• Maternal sepsis should be considered as a
wider definition
• Consideration of all types of infection is
important in training, when planning
management and services

Causative organisms
Escherichia coli 21%
Group A streptococcus
9%
Group B streptococcus
8%
Other streptococcus
6%Staphylococcus6%
Mixed organisms5%
Other7%
Unknown2%
No laboratory confirmed infection
36%
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Causative organism by source
of infection
0
20
40
60
80
100
120
Nu
mb
er
of
ca
se
s
Source of infection
No Lab confirmed infection
Unknown
Other
Mixed
Staph
Other strep
Group B strep
Group A strep
E.coli
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)
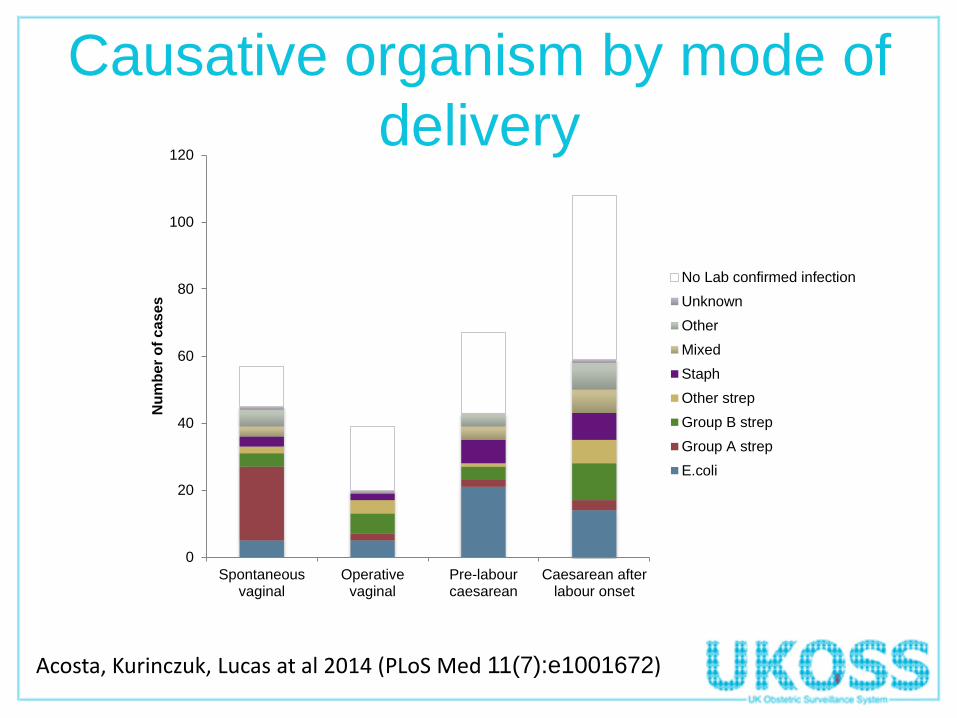
Causative organism by mode of
delivery
0
20
40
60
80
100
120
Spontaneousvaginal
Operativevaginal
Pre-labourcaesarean
Caesarean afterlabour onset
Nu
mb
er
of
ca
se
s
No Lab confirmed infection
Unknown
Other
Mixed
Staph
Other strep
Group B strep
Group A strep
E.coli
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Rapid progression to severe
sepsis
• <24 hours between the first signs of an inflammatory
response to infection and sepsis:
– 83% of cases and 85% of septic shock cases
• <48 hours between the first signs of an inflammatory
response to infection and sepsis:
– 89% of cases and 95% of septic shock cases
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Causative organism according to
whether septic shock diagnosed
0
5
10
15
20
25
30
35
40
45
50
E.coli Group Astrep
Group Bstrep
Other strep Staph Mixed Other Unknown No Labconfirmedinfection
Pro
po
rtio
n o
f w
om
en
(%
)
Septic shock No shock
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Rapid progression to severe
sepsis for women with Group A
streptococcal infection
• 50% <2 hours between the first signs of an inflammatory
response to infection and sepsis diagnosis
• 75% <9 hours between the first signs of an inflammatory
response to infection and sepsis diagnosis
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Significant medical risk factors
Cases n (%)
Controls n (%) aOR* 95% CI
n=365 n=757
Parity
0 197 (54) 330 (44) 1.6 (1.2-2.2)
≥1 167 (46) 427 (56) 1
Pre-existing medical problems
Yes 120 (33) 171 (23) 1.4 (1.0-1.9)
No 245 (67) 583 (77) 1
Febrile illness or antibiotics in 2 wks before delivery
Yes 153 (42) 42 (6) 12.1 (8.1-18.0)
No 212 (58) 715 (94) 1
*Adjusted for all other factors examined
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Significant delivery risk factors
Postpartum cases n (%)
Controls n (%) aOR* 95% CI
n=302 n=757
Mode of delivery
Spontaneous vaginal 57 (21) 443 (59) 1
Operative vaginal 39 (14) 100 (13) 3.4 (1.7-7.0)
Pre-labour caesarean 67 (25) 119 (16) 3.5 (2.0-6.1)
Caesarean after labour onset 108 (40) 92 (12) 6.7 (3.8-12.0)
Complications of delivery
Yes 103 (34) 279 (37) 1.7 (1.1-2.5)
No 199 (66) 478 (63) 1
*Adjusted for all other factors examined
Acosta, Kurinczuk, Lucas at al 2014 (PLoS Med 11(7):e1001672)

Significant factors associated
with mortality in intensive careSurvivors
n (%)Deaths n (%) aOR* 95% CI
n=610 n=29
Maternal age
<25 234 (38) 5 (17) 1
25-34 254 (42) 15 (52) 2.2 (0.7-7.0)
≥ 35 121 (20) 9 (31) 3.3 (0.9-11.0)
BMI
Unknown 317 (52) 13 (45) 1.2 (0.2-9.1)
<25 126 (21) 3 (10) 1
25-29.9 90 (15) 7 (24) 5.2 (1.4-18.9)
≥ 30 76 (13) 6 (21) 6.3 (1.5-27.0)
IMD Quintiles 4&5 354 (58) 17 (58) 2.6 (1.0-6.7)
*Adjusted for all other factors examined
Acosta C et al. 2016 (BMJ Open; 6(8):e012323)

Causes of maternal death
UK 2009-12

Causes of maternal death
UK 2009-12

Influenza deaths 2009-12

Causes of maternal death
2009-12• Major contribution from influenza and
other non-genital tract sepsis deaths
• Overall rate of maternal mortality from
infectious causes in 2009-12 was 2.0 per
100,000 maternities (95%CI 1.6-2.6)

Maternal sepsis deaths 2000-
2012
0.00
0.50
1.00
1.50
2.00
2.50
3.00
2000-02 2003-05 2006-08 2009-12
Rate
per
100,0
00 m
ate
rnit
ies
Sources: CMACE and MBRRACE-UK

Key actions in suspected sepsis
• The key actions for diagnosis
and management of sepsis
are:
1. Timely recognition
2. Fast administration of intravenous antibiotics
3. Quick involvement of experts - senior review is
essential
NHS England Patient Safety Alert NHS/PSA/R/2014/015 (NHS England 2014)

Vignette: sepsis
Two hours after delivery a woman became unwell on the
postnatal ward feeling faint. Her oxygen saturation was
65%. She was reviewed by junior staff and found to be
shocked, with moderate PV bleeding. Her temperature
was never measured. A diagnosis of haemorrhage was
made and she was treated with fluids. She failed to
improve and was taken to theatre where she had a cardiac
arrest. A laparotomy and hysterectomy were carried out but
resuscitation failed. The postmortem found an extensive
blistering skin rash, swollen labia and disseminated
intravascular coagulation all as a result of overwhelming
Group A Streptococcal sepsis.

Antibiotic administration among
women who died 2009-12
Symptom onset Diagnosis Antibiotics Death
43 40 37
3
<1 hour
3
1 – 2 hours
2 – 3 hours
3 – 24 hours
< 24 hours
(missing time)
> 24 hours
Death at home or on arrival
Never commenced on antibiotics
Progression of disease
Tim
e
14
7
4
4
3
5
Mohamed-Ahmed O et al. 2015 BJOG;122(11):1506-15.
43 women died
from bacterial
sepsis
14 (33%)
received
antibiotics within
one hour

Vignette; sepsis
A woman who was seven days post spontaneous vaginal
delivery became unwell at home with a fever. She was advised
to attend the maternity unit immediately. On admission she
was noted to be tachycardic, tachypnoeic and febrile. She
was prioritised for urgent medical review. A diagnosis of
acute sepsis from retained products was made and fluid
resuscitation started immediately. Intravenous antibiotics were
started within one hour of the diagnosis and she was transferred
to the high dependency unit. The retained products of
conception were removed promptly and she made a full
recovery. Blood culture subsequently grew Klebsiella. Early
recognition, clear advice and prompt treatment led to a good
outcome without any further complications.

Screening and action tools for women who
are pregnant or who have given birth within
the last six weeks
https://sepsistrust.org/education/clinical-tools/

MATERNAL DEATHS FROM
SEPSIS – WHERE ARE WE
NOW?

Maternal mortality rate due to sepsis per 100,000 maternities, UK 2013-15

But..A woman with a large for dates baby was admitted at term in early
labour. CTG abnormalities were not recognised or responded to and an intrauterine death occurred. She then developed signs of sepsis and
acute kidney injury during labour, which were not promptly recognised. A sepsis bundle was not initiated. After a prolonged second stage she
had a massive haemorrhage, developed coagulopathy and died. Although her death was probably multifactorial, sepsis was the
underlying cause of her deterioration. Reviewers noted several aspects of her resuscitation that could have been improved. Senior staff were
not involved until after her collapse.
After her death it was thought amniotic fluid embolus was implicated, although this was reported as a secondary phenomenon by the
pathologist at postmortem. This led to a superficial review of her care, significantly limiting the lessons that should have been learnt from her death. A pathologist, who would have provided a better understanding
of the post-mortem findings, was not involved in the review.

WHO Global maternal sepsis
study• Over one week in the West Midlands 93
women were identified across 8 hospitals
who were treated for infection associated
with pregnancy
• Nationally, 82 maternity units reported that
they had no women with suspected or
confirmed pregnancy-associated infection
in the same week

Key points
• Genital tract infection forms only a small
proportion of maternal mortality and morbidity
from infectious disease
• Women with pre-existing medical problems and
women undergoing operative delivery are at
higher risk of sepsis morbidity
• Obesity, older maternal age and deprivation are
associated with mortality
• Symptoms of sepsis, particularly postnatally,
may be interpreted as part of the norm

Anna’s story
Hinton L
Anna had a life-saving hysterectomy and
after several weeks in hospital, she came
home to her sons. But being the Mum she
wanted to be was hard after being so
gravely ill.
Anna’s story
Hinton L

Acknowledgements and funding
MBRRACE-UK•Department of Health, England
•NHSSPS Northern Ireland
•Scottish Government Health Department
•NHS Wales
•Channel Islands and the Isle of Man Government Offices
The contract is managed on behalf of the funding bodies by the
Healthcare Quality Improvement Partnership (HQIP)
ICNARC/UKOSS studies•NIHR PGfAR And thanks to numerous
co-authors and
collaborators!


















