Martin Koskas, M.D.,a,b,c,d Jennifer Uzan, M.D.,a Dominique Luton, M.D., Ph.D.,a,b
Roman Rouzier, M.D., Ph.D.,d,e and Emile Daraï, M.D., Ph.D.c,f
a Department of Obstetrics and Gynecology, Bichat University Hospital, Paris, France; b Paris Diderot University, Paris,France; c Unit�e Mixte de Recherche S938, Universit�e Pierre et Marie Curie, Paris, France; d Equipe d'accueil 7285,Universit�e de Versailles Saint-Quentin-en-Yvelines, Montigny-le-Bretonneux, France; e Department of Gynecology,Institut Curie, Paris, France; and f Department of Obstetrics and Gynecology, Tenon University Hospital, Paris, France
Objective: To evaluate the various possible prognostic factors on the fertility-sparing management of atypical hyperplasia andendometrial cancer; to generate survival curves to estimate remission and recurrence rates according to time.Design: Systematic review and meta-analysis. Registration number: CRD42013004557.Setting: University hospital.Patient(s): Patients who underwent fertility-sparing management for atypical hyperplasia and endometrial cancer.Intervention(s): All published studies were identified through MEDLINE and reported according to PRISMA guidelines.Main Outcome Measure(s): Remission, recurrence, progression, and pregnancy rates by age, obesity, infertility, previous pregnancy,histology, and medical treatment.Result(s): A total of 370 patients from 24 studies were included. The 12- and 24-month remission probabilities were 78.0% and 81.4%,respectively. In multivariate analysis, previous pregnancy (odds ratio [OR] 2.70, 95% confidence interval [CI] 1.23–5.89), infertility (OR2.26, 95% CI 1.05–4.87), and treatment with megestrol acetate (OR 2.70, 95% CI 1.20–6.02) were associated with higher remissionprobability. The 12- and 24-month recurrence probabilities were 9.6% and 29.2%, respectively. In multivariate analysis, none of thefactors studied was associated with higher recurrence probability. Twenty-two studies totaling 351 patients were used to assesspregnancy rate; 111 subjects (32%) had one pregnancy or more. In multivariate analysis, none of the factors were associated withpregnancy probability. Among the 263 patients used to assess progression rate, 39 (15%) had a tumor with at least myometrialinvasion on the hysterectomy specimen. Endometrial cancer and the use of other medical therapies (in comparison with megestrolacetate) were associated with an increased probability of progression.
Use your smartphone
Conclusion(s): Fertility-sparing management should not be contraindicated in older patientswith previous infertility or obesity. (Fertil Steril� 2014;101:785–94. �2014 by American Soci-ety for Reproductive Medicine.)Key Words: Fertility sparing, conservative, endometrial cancer, endometrial atypicalhyperplasia, systematic review
Discuss: You can discuss this article with its authors and with other ASRM members at http://fertstertforum.com/koskasm-fertility-sparing-endometrial-atypical-hyperplasia-cancer/
to scan this QR codeand connect to thediscussion forum forthis article now.*
* Download a free QR code scanner by searching for “QRscanner” in your smartphone’s app store or app marketplace.
Received July 14, 2013; revised November 15, 2013; accepted November 19, 2013; published onlineJanuary 2, 2014.
M.K. has nothing to disclose. J.U. has nothing to disclose. D.L. has nothing to disclose. R.R. has nothingto disclose. E.D. has nothing to disclose.
Reprint requests: Martin Koskas, M.D., Department of Gynecology, Bichat University Hospital, 46 rueHenri Huchard, 75018 Paris, France (E-mail: [email protected]).
(1). The classic treatment requires at least a hysterectomy witha bilateral salpingo-oophorectomy; however, the safety of aconservative approach has been confirmed in several cohortstudies that evaluated uterine preservation (2–4). Therefore,conservative treatment should be discussed in patients whowish to preserve their fertility.
For more than 40 years, the fertility-sparing managementof EC and AH and its oncologic and reproductive outcomeshave been reported in the literature. However, because thesestudies were performed on small patient cohorts, they lackthe statistical power to establish guidelines concerning themanagement and prognosis of conservative AH and ECtreatments.
Young women with AH or EC typically have a history ofinfertility, obesity, chronic anovulation, and polycysticovarian syndrome (PCOS), which are all conditions associatedwith prolonged unopposed estrogen (E) exposure (5). Howev-er, none of these characteristics have been studied as possibleprognostic factors for the oncologic and reproductive out-comes of fertility-sparing management.
Previous studies have shown reduced fertility in obesewomen (6), but the possibility of fertility-sparing manage-ment in obese women has never been evaluated. Similarly,in contrast to the study performed by Fauvet et al. (7), whichfocuses on ovarian borderline tumors, the impact of age hasnot been evaluated in terms of the reproductive outcome offertility-sparing management of AH and EC.
Hormone therapy is usually administered to promoteremission and allow pregnancy. Although several prospectivestudies have been conducted to evaluate the safety of thisapproach, none of these studies have compared differenttreatment or regimen protocols. Oral progestin has frequentlybeen evaluated, in particular 17-hydroxyprogesterones suchas medroxyprogesterone acetate (MPA) (4) and megestrol ac-etate (MA) (8). Other therapies that have been evaluated in alimited number of cases include GnRH agonist (9), intrauter-ine devices (IUDs) containing progestogen (10), or a combina-tion of these therapies (11).
A recent review (3) showed that AH has a significantlyhigher response rate than grade 1 EC, and a lower remissionrate is observed in women with carcinoma than in thosewith hyperplasia. Nonetheless, the reproductive outcomesdid not differ. This review focused on the outcomes and thecomparison of AH and EC for the fertility-sparing manage-ment of EC and AH. Notably, possible prognostic factorsthat may affect oncologic and reproductive outcomes werenot studied.
The aim of this review was to evaluate the impact of age,gravidity, obesity, fertility, histology, and hormonal treat-ments on reproductive and oncologic outcomes to better pre-dict the success of fertility-sparing management. Severalfactors need to be investigated to adequately assess theoptimal conditions for fertility-sparing treatment of AH andEC; these factors include timing, the optimal duration of treat-ment, and when to consider hysterectomy if the patient doesnot become pregnant. The duration of fertility-sparing treat-ment should be based on a balance between remission andpregnancy while avoiding recurrence and/or progression.For this reason, we have built survival curves. Moreover,
786
this approach allows for a better understanding of the evolu-tion of medically treated EC and AH.
MATERIALS AND METHODSStudies Eligible for Review
The population of interest in this systematic review waswomen with AH or EC that was limited to the endometrium(1988 International Federation of Gynecology and Obstetricsstage IA). The intervention queried was fertility-sparing ther-apies, and the outcomes were evidence of disease regression,relapse, pregnancy, and disease progression. We conducted aresearch with MEDLINE (1950 to 2011) using a combinationof medical subject headings. Text words were used to generatetwo subsets of citations: [1] studies of EC (‘‘endometri*cancer*,’’ ‘‘malignant endometri*,’’ ‘‘endometri* carcino*’’) orAH (‘‘endometr* atypical hyperplas*,’’ ‘‘premalignant endo-metr*,’’ ‘‘precancer* endometr*’’) and [2] studies of fertility-sparing therapies such as progestogens and IUDs or systems(‘‘intrauterine devices medicated,’’ ‘‘levonorgestrel,’’ ‘‘Mir-ena,’’ ‘‘intrauterine progest*,’’ ‘‘LNG-IU*,’’ ‘‘progest*,’’ ‘‘ges-tag,*’’ ‘‘fertility-sparing therapy,’’ ‘‘conservative therapy,’’‘‘hormon* therapy,’’ ‘‘conservative management’’). These sub-sets were combined with the word ‘‘and’’ and limited using theterms ‘‘humans’’ and ‘‘female’’ to generate a subset of cita-tions. The reference lists of all known primary and review ar-ticles were examined to identify cited articles that were notcaptured by electronic searches. Only articles published in En-glish and involving women between 19 and 44 years of agewere retrieved.
Inclusion and exclusion criteria for the selection of arti-cles were as follows. Inclusion criteria were studies includingpatients between 19 and 44 years of age; fertility-sparingmanagement; and histologic diagnosis of AH or stage Iadenocarcinoma of the endometrium. Exclusion criteriawere case reports and small study series with fewer thanfive patients; articles not written in English; patients with tu-mor invading the myometrium; conservation because of highrisk for perioperative morbidity; data not extractable; otheruterine neoplasia than endometrioid adenocarcinoma; pa-tients with simple hyperplasia; and redundant articles.
All studies obtained as a result of the search were re-viewed. The original portable document files of studies ob-tained from the search were located through direct onlinelinks to the files from the search results.
The complete review protocol can be accessed online(http://www.crd.york.ac.uk/prospero); the registration num-ber is CRD42013004557.
Data Abstraction
Each of the 24 articles were read by two different readers (J.U.and M.K.), and a database was created with the following twotypes of items: [1] the possible prognostic factors for fertilitypreservation management (because no standard guidelinesexist for this management, a control group could not beconstituted), and [2] four outcomes to assess the efficacy ofthis strategy. Studies containing original and detailed dataon the management and oncologic and reproductive
outcomes of patients in whom the uterus was preserved toobtain pregnancy were selected. Databases from these studieswere saved separately on a Microsoft Excel 2010 file for eacharticle. A line was created for each patient detailing thepossible prognostic factors for fertility preservation manage-ment and the four outcomes to assess the efficacy of this strat-egy. These results were then merged on a single MicrosoftExcel 2010 file and sorted to enable the identification of thepatient provenance. A study was included for the evaluationof one of the four outcomes only if the reported outcome wasavailable for all the patients included in the study. Forexample, studies were assessed for remission if response,delay for response, and follow-up were available for all thepatients included in the study. A study providing delay forremission only without providing the follow-up time for pa-tients who did not undergo remission was not used to estimateremission probability. The studies selected to assess the remis-sion probability are shown in Table 1 (‘‘Outcomes studied’’column). This strategy was applied for the four outcomesinvestigated in this meta-analysis.
The possible prognostic factors for fertility preservationmanagement success were age (evaluated as a continuousvariable), obesity, previous pregnancy, infertility, histology,and medical treatment. Concerning the definition of obesity,as widely accepted and as established by theWorld Health Or-ganization (www.who.int/mediacentre/factsheets/fs311/en),patients with bodymass index ofR30 kg/m2 were consideredobese. Concerning histology, because only 7 patients (2%)had grade 2 or 3 adenocarcinoma, and most studies did notdistinguish the various subtypes of AH (complex or simple),only the distinction between EC and AH was made. Atypicalhyperplasia was not divided into simple and complex AH.In none of the studies did the authors report cases of simpleAH managed conservatively. In four studies (9, 12–14) theauthors specified that all the cases of AH managed werecomplex, and in one study (15) the authors reported that thecases of AH managed were ‘‘severe.’’ In all the other studiesthe degree of AH was not reported. Treatments wereclassified into three categories: MA, MPA, and otherhormone therapy. This strategy was elected because itpermitted us to obtain three groups of patients with asufficient number of patients in each. Other hormonetherapy included hydroxyprogesterone caproate,norethisterone acetate, GnRH agonists, levonorgestrel IUD,combination of GnRH agonists and levonorgestrel IUD,bromicriptine, natural progesterone, ovulation induction,and oral contraceptives. Patients were considered to haveprevious infertility if this was stated in the original article.We assume that as stated by the World Health Organization,infertility was defined by ‘‘the failure to achieve a clinicalpregnancy after 12 months or more of regular unprotectedsexual intercourse.’’
The four outcomes used to assess the success of fertility-sparing management were remission, recurrence, progres-sion, and pregnancy. Remission was defined as absence ofAH or EC, and recurrence was defined as the reappearanceof AH or cancerous cells that had initially disappeared. Pro-gression was defined as histology upon hysterectomy thatwas classified as a minimal stage IB of the 1988 International
VOL. 101 NO. 3 / MARCH 2014
Federation of Gynecology and Obstetrics classification (i.e.,tumor extension beyond the endometrium), and pregnancywas defined as biological pregnancy. Biological pregnancywas defined by positive b hCG level.
To assess the remission rate according to time (Kaplan-Meier analysis), we selected only studies in which the delaybetween the beginning of medical treatment and the remis-sion or last follow-up was detailed for all patients. When sec-ondary remission (i.e., use of another medical treatmentbecause the first failed) was attained, we classified this asno remission; for Kaplan-Meier analysis we defined the delayas the time between the beginning of the first treatment andthe time of the last evidence of an endometrial tumor.
It was not possible to generate survival curves for thepregnancy rate because the delay between diagnosis andpregnancy was available for few patients. Similarly, it wasnot possible to generate survival curves for the progressionrate because the delay between diagnosis and progressionwas available for few patients. The articles selected for eachoutcome studied are detailed in Table 1.
Statistics and Data Analysis
The categoric and numeric variables were analyzed using thec2 t test and Student's t test, respectively. The differences wereconsidered to be significant at P< .05. Cox proportional haz-ards models were developed to examine survival. In the Coxproportional hazards analyses, we modeled the remissionand recurrence probabilities and studied the possible signifi-cant prognostic factors using the fast backward eliminationof factors based on the Lawless and Singhal method (16).Kaplan-Meier curves were generated to examine the remis-sion and recurrence probabilities. Logistic regression modelswere developed to describe the predictors of pregnancy andprogression. In the logistic regression analysis, we modeledall of the categories of each variable and controlled for allother variables in the model.
The data were analyzed with the R software package,version 2.13.0 in the Design, Hmisc, and Verification libraries(http://lib.stat.cmu.edu/R/CRAN/).
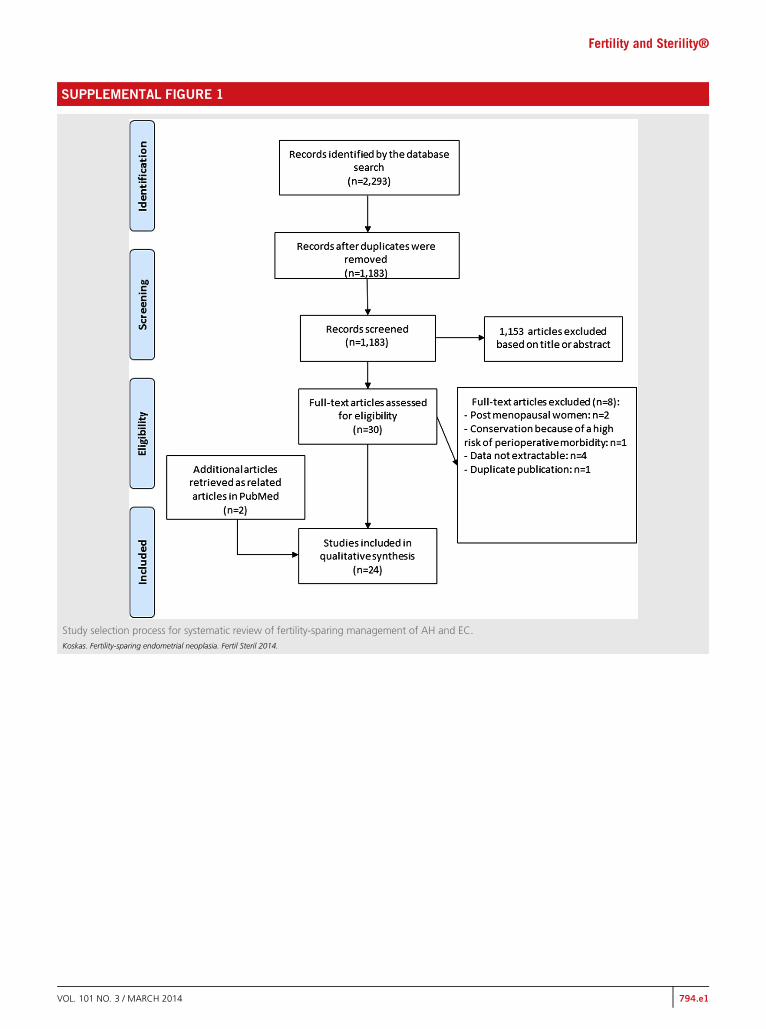
RESULTSOut of a total of 1,183 studies that were initially identified,1,153 were excluded after review of the title or the abstract.A total of 30 articles reporting medical treatment for AH orEC were therefore included for a thorough review. Afterdetailed review, 24 studies reporting conservative manage-ment of AH and EC in young patients who wished to preservetheir fertility were eligible for use in the meta-analysis (Fig. 1).Seven studies were prospective, and 16 were retrospective; thedistinction was not clear for 1 study. Pathologic review wasperformed in 17 studies, was not performed in 6 studies,and was not clearly stated in 1 study.
Patients, Tumor Characteristics, and Management
A total of 370 patients from 24 studies were included(Table 1). Patient characteristics are presented in Table 2.
Characteristics of studies included in the meta-analysis investigating oncologic and/or reproductive outcomes after fertility-sparing management for AH and EC.
First author, year(reference) Study size Participants Intervention Outcomes studied Design Follow-up
Pathologicreview
Duska, 2001 (29) 12 EC EC, age 40 y or younger,medical therapy anduterine conservation
Progestins not detailed Pregnancy Retrospective NA Yes
Minaguchi, 2007 (13) 31 (12 AH, 19 EC IAG1) EC or AH who wished topreserve fertility;however, one patientaged >40 y had toreceive conservativetherapy because ofcomplications
MPA Pregnancy Unclear Mean follow-up of 44 mo No
Minig, 2011 (11) 34 (20 AH, 14 EC G1) EC/AH, younger than 40 y,wish to preserve fertility
Kaplan-Meier analysis of remission probability of patients with AHand EC.Koskas. Fertility-sparing endometrial neoplasia. Fertil Steril 2014.
ORIGINAL ARTICLE: FERTILITY PRESERVATION
Median and mean follow-up were 42.00 and 48.86 months,respectively.
Remission
Fourteen studies with a total of 161 patients were used toassess remission probability and factors associated withremission. Median and mean follow-up were 46.5 and 53.3months, respectively. Among the 161 patients used to assessthe remission probability, 58 (36.0%) underwenthysterectomy.
The remission probability according to time is provided inFigure 1. The 3-, 6-, 12-, 18-, and 24-month remission prob-abilities based on the Kaplan-Meier curve were 30.4%, 72.4%,78.0%, 80%, and 81.4%, respectively. The Cox models of the
factors that were associated with remission are displayed inSupplemental Table 1 (available online). The univariate anal-ysis demonstrated that youngest patients, patients with previ-ous pregnancy, infertility, AH, and treatment with MA weremore likely to experience remission. The multivariate analysisincluded age, gravidity, previous infertility, histology, andhormonal therapy and found that patients with a previouspregnancy (odds ratio [OR] 2.70, 95% confidence interval[CI] 1.23–5.89), infertility (OR 2.26, 95% CI 1.05–4.87), andtreatment with MA (OR 2.70, 95% CI 1.20–6.02) were morelikely to experience remission.
Recurrence
Ten studies with a total of 100 patients were used to assess therecurrence probability and risk factors. Of these 100 patients,84 experienced remission after hormonal therapy, and 27(32.1%) experienced recurrence. The median and meanfollow-up were 47.5 and 55.1 months, respectively.
The recurrence probability according to time is providedin Figure 2. The 4-, 6-, 12-, 18-, and 24-month recurrenceprobabilities based on the Kaplan Meier curve were 3.6%,9.6%, 17.2%, 26.0%, and 29.2%, respectively. The Coxmodelsof the factors associated with recurrence are displayed inSupplemental Table 1. According to the univariate analysis,none of the factors studied was associated with an increasedrisk of recurrence.
Pregnancy
Twenty-two studies with a total of 351 patients were used toassess pregnancy rate and factors associated with pregnancy;111 (31.6%) of these patients had at least one pregnancy.Among those 111 patients, 60 (54.1%) obtained it with theuse of assisted reproductive technologies (ART), whereas in29 cases (26.1%), pregnancy was spontaneous. In the 22 re-maining cases (19.8%), this was not clearly stated. Meanage of patients who obtained pregnancy spontaneously was32.1 years (median 31.5 years, range 22–42 years). Meanage of patients who obtained pregnancy with the use ofART was 32.0 years (median 32.5 years, range 20–40 years).
FIGURE 2
Kaplan-Meier analysis of recurrence probability of patients with AHand EC.Koskas. Fertility-sparing endometrial neoplasia. Fertil Steril 2014.
VOL. 101 NO. 3 / MARCH 2014
Fertility and Sterility®
Among the 21 infertile women who obtained pregnancy andfor whom the conception method was detailed, 18 (85.7%)had pregnancy with the use of ART. To the contrary, amongthe eight fertile women who obtained pregnancy and forwhom the conception method was detailed, pregnancy wasspontaneous in four cases (P¼ .07). The logistic regressionmodels of the factors associated with pregnancy are displayedin Supplemental Table 2. Univariate analysis showed thatonly infertility was associated with an increased probabilityof pregnancy. Because of P values < .10, age (P¼ .09), previ-ous pregnancy (P¼ .07), obesity (P¼ .08), and previous infer-tility (P¼ .03) were included in the multivariate analysis. Themultivariate analysis showed that none of those factors wereassociated with pregnancy probability.
Progression
Nineteen studies with a total of 263 patients were used toassess the progression rate and factors associated with pro-gression; 39 of these patients (14.8%) had a tumor with myo-metrial invasion. Among those 263 patients, 87 (33.1%)underwent hysterectomy: this was performed because noremission occurred in 34 cases; because of recurrence withoutpregnancy in 24 cases; despite remission, without pregnancyand because of renunciation in 11 cases; after pregnancywithout recurrence in 9 cases; after pregnancy because ofrecurrence in 6 cases; and without clear reason in 3 cases.
The logistic regression models of the factors associatedwith progression are displayed in Supplemental Table 2.Endometrial cancer and the use of other medical therapies(in comparison with the use of MA) were associated with anincreased probability of progression. The multivariate anal-ysis showed that EC (OR 2.84, 95% CI 1.22–6.67) and theuse of other medical therapies (in comparison with the useof MA) (OR 3.95, 95% CI 1.44–10.81) were also associatedwith an increased probability of progression.
DISCUSSIONEndometrial cancer and AH are rarely encountered in youngwomen. Here we present a meta-analysis that investigatestwo major dimensions of the conservative, fertility-sparingmanagement of EC and AH. First we determined that theremission probability with conservative management reacheda plateau after 12 months, whereas the recurrence probabilityincreased continually over time for at least 5 years. Second,the meta-analysis identified prognosticators of oncologicand reproductive outcomes in the fertility-sparing manage-ment of AH and EC.
This was a novel study method that aimed to overcomethe lack of literature on fertility-sparing management for pa-tients with AH and EC. Using a meta-analysis, we created acohort with enough patients to permit the statistical analysisof four outcomes: remission probability, recurrence probabil-ity, pregnancy rate, and disease progression. Although thiscohort was retrospective and heterogeneous owing to theabsence of some data from the original articles, we can useour results to propose guidelines for the fertility-sparing man-agement of AH and EC. However, for a better interpretation ofthe results, several limitations must be discussed.
VOL. 101 NO. 3 / MARCH 2014
First, progression was defined as tumor extending intothe myometrium at the time of hysterectomy. Consequently,if a patient went from AH to EC that was limited to the endo-metrium at the time of hysterectomy, this would not havebeen considered progression. Because at the time of diagnosis,on the endometrial biopsy specimen, separating AH fromwell-differentiated EC is particularly difficult for the patholo-gist, we elected that evolution from AH to EC limited to theendometrium should not be considered a progression. InKaku et al.'s experience (17) reporting the results of a centralpathologic review to make definite diagnoses of 39 patientswith endometrioid EC and AH who received conservativetreatment, the diagnosis of EC in 29 cases was changed toAH in 10, complex hyperplasia in 3, and atypical polypoid ad-enomyoma in 3. Among the 10 cases of AH, 1 was changed toEC and 1 was changed to simple hyperplasia. Because centralpathologic review was not performed in all studies, it ispossible that in some cases, patients initially diagnosed withAH had well-differentiated EC limited to the endometrium.For such patients, considering that the diagnosis of well-differentiated EC on the hysterectomy specimen was a pro-gression would overestimate the progression risk. Moreover,because the prognosis of well-differentiated EC limited tothe endometrium is excellent, with a 3-year overall survivalclose to 100% (18) and the risk for lymph node metastasisclose to zero (19), it is not crucial to distinguish AH fromwell-differentiated EC limited to the endometrium for theevaluation of progression risk.
Second, we considered response rate to initial therapyrather than response rate to secondary therapy because inthe present meta-analysis we aimed to evaluate the impactof various therapies on oncologic and reproductive outcomes.It would not have been possible to perform such an evaluationby considering the cases of patients who underwent second-ary remission with the use of another therapy. However, if apatient was entered to have no remission after initial therapy,this was always because the original article stated that the pa-tient had no remission proven by pathologic evaluation of theendometrial specimen. In the present analysis, in only fourcases (patient 2 of the Kim et al. study [20], patient 4 of theMao et al. study [21], and patients 18 and 30 of the Randallet al. study [8]) included in this meta-analysis, the hormonaltherapy was changed or stopped because of secondary sideseffects.
Third, although some women may want to try conserva-tive management of their neoplasia to avoid surgery, some inthis situation could do so to maintain the option of havingchildren, and the pregnancy rate should be interpreted withcaution. However, to be selected in the present meta-analysis, studies had to include patients who underwent con-servative management for fertility-sparing managementonly. Conservation because of high risk for perioperativemorbidity was an exclusion criterion. Consequently, all thepatients desired pregnancy. It is not possible to assess whetherall patients tried to obtain pregnancy once remission was ob-tained, but we believe it important to remind the reader that inmany cases (when the fertility status was reported) endome-trial neoplasia was diagnosed during infertility investi-gations, and many patients were treated with ART.
791
ORIGINAL ARTICLE: FERTILITY PRESERVATION
Consequently, it is probable that most of the patients includedin this meta-analysis tried to obtain pregnancy. Moreover,uterine preservation is mainly proposed for young womenwho wish to achieve pregnancy after careful evaluation toexclude invasive proliferation or myometrial invasion.Consequently, it is likely that the vast majority of the patientswere counseled to obtain pregnancy once remission wasobtained.
Twelve months after medical treatment, the remissionprobability reached a plateau of approximately 80%; there-fore, fertility-sparing treatment should be reconsidered ifremission does not occur after 12 months. This robust findingfrom a methodologic and statistical point of view argues fordiscontinuing a conservative strategy after 2 years in patientswho did not experience remission. In contrast, because therecurrence probability increases continually with time, evenwhen remission is attained, close long-term surveillance ismandatory until the uterus is removed.
Multivariate analysis suggests that previous pregnancy,infertility, and treatment with MA increase the remissionprobability. A recent study has indicated an improved remis-sion rate with AH when compared with EC (3); however, amultivariate analysis was not performed in this study. Apossible explanation for the higher response probability ininfertile women is that in patients with PCOS, both serum Eand androgen levels are significantly elevated, whereas Plevels are chronically reduced (22). Unopposed E as found inchronic anovulatory women with PCOS promotes endome-trial growth and proliferation. Consequently, progestin ther-apy in such patients is likely to antagonize the mitoticactions of E on endometrial development and could be anexplanation for the better remission rate; however, the path-ophysiology of this mechanism is not clear. In patients withendometrial hyperplasia or adenocarcinoma, previous biolog-ical studies note that lesions with low bcl-2 expression or highp53 expression were more likely to respond to medical treat-ment (23). Therefore, in addition to routine histology, biolog-ical markers are required to better identify patients who maypotentially benefit from hormonal therapies. Previous preg-nancy was also associated with a higher remission probabil-ity. However, this finding needs to be confirmed at a largerscale because no pathophysiologic explanation is currentlyavailable to explain this phenomenon.
The use of MA in comparison with other hormonal treat-ments, including MPA, levonorgestrel IUD, and GnRHagonist, was also associated with a higher remission probabil-ity. Unfortunately, dosage as well as duration of treatmentwas not analyzable. Similarly, because of the retrospectivenature of most of the studies, other possible prognostic factors(e.g., histologic type, age, ART) were not controlled. Megestrolacetate and MPA are the most frequently evaluated treat-ments in the literature; both treatments are P agonists withantiandrogenic and antiestrogenic effects (24), but after oraladministration, the relative bioavailability of MA is signifi-cantly higher than that of MPA (25). However, in a previousstudy (26), MPA was evaluated in advanced and recurrentEC with the conclusion that 200 mg/d of oral MPA was anappropriate treatment for EC, particularly well-differentiated and/or P receptor–positive types. We could
792
extrapolate these results to MA because it is also a P receptoragonist. Treatment with MA is the most frequently evaluatedtreatment in the literature, and this meta-analysis found MAto be associated with a higher remission probability and lowerprogression probability. These data suggest that MA can be afirst-line agent for fertility-sparing treatment; however, wecannot recommend an appropriate dosage on the basis ofour results.
In contrast to the remission probability, the recurrenceprobability increases continually with time, even when remis-sion is attained; therefore, close long-term surveillance ismandatory until the uterus is preserved. In multivariate anal-ysis, no factors (age, obesity, infertility, gravidity, histologictype, or type of treatment) were statistically associated withthe recurrence probability. These results differ from a previousstudy (3), which concluded that EC was significantly associ-ated with a higher recurrence rate. In the present study the dif-ference likely did not reach statistical significance because weconducted a survival analysis instead of using the c2 test.However, in our meta-analysis EC was associated with anincreased disease progression risk compared with AH.Because of the persistence of risk factors (diabetes, obesity,high blood pressure) EC is likely to recur; therefore, a second-ary hysterectomy should be discussed once childbearing iscomplete.
The results of this meta-analysis for remission probabil-ity, recurrence probability, progression of disease, and preg-nancy probabilities revealed no association with age.Consequently we cannot recommend an age limit forfertility-sparing management of AH and EC. In particular,there was a tendency showing that age was associated witha lower pregnancy rate, but it did not reach statistical signif-icance. The paradoxical finding concerning the higher preg-nancy rate in patients with previous infertility on univariateanalysis may be related to a higher remission probability, aswell as the higher probability of ART use. Because infertilepatients were likely to have their endometrial tumor diag-nosed during infertility investigations, it is probable thatthe decision to undergo ART was made more frequentlyand rapidly in comparison with patients without prior infer-tility. This meta-analysis clearly suggests that in infertilewomen, pregnancy was the result of ART more frequentlywhen compared with pregnancies obtained in fertile women.However, these results should be interpreted with caution.For example, our analysis on pregnancy rates included allpregnancies, without differentiating the outcomes or the or-igins (spontaneous vs. ART). Because of missing data, ouranalysis could not precisely determine whether ART wasrequired for women in remission. It would be interesting todetermine exactly the rate of pregnancy attained by ARTand to determine whether ART made pregnancy attainablefor the oldest conservatively managed patients. Moreover,data evaluating ovarian reserve are also lacking. Antral fol-licle count by ultrasonography or antim€ullerian hormoneserum level determination could also help to distinguish pa-tients with a higher probability of spontaneous pregnancyfrom those requiring ART. This point is particularly impor-tant because there are few data available on the impact ofART on recurrence risk. In a recent meta-analysis evaluating
VOL. 101 NO. 3 / MARCH 2014
Fertility and Sterility®
the live birth rate after fertility-sparing management, the livebirth rate after ART (39.4%) was significantly higher than af-ter spontaneous pregnancy (14.9%) (P¼ .001) (27). In anobservational case series study, Elizur et al. (28) reported afertilization rate of 59% after IVF in eight infertile women,aged 35 years or younger, who were treated conservativelyfor EC: six women conceived, and four delivered six healthyinfants. Similarly, ART can be useful for obese patientsbecause this condition has been reported to be associatedwith difficulties in conception and implantation (6).
In the absence of data on ovarian reserve, the presentmeta-analysis does not permit us to decide when and in whichpatients ART should be decided once remission is attained.However, we recommend that ART should always be dis-cussed, especially in patients with a history of infertility,obesity, and/or greater ages. Although there is no direct evi-dence in this review or in publication that supports thisapproach to care, the implementation of ART not only in-creases the chance of conception but may also decrease theinterval to conception and consequently reduce the progres-sion risk.
In conclusion, the aim of this meta-analysis was to over-come the lack of significant literature; to evaluate the impactof age, gravidity, body mass index, fertility, histology, andhormonal treatments on fertility, and oncologic outcomes;and to predict the success of fertility-sparing management.On the basis of the results of both oncologic and reproductiveoutcomes, we find that conservative management should notbe restricted for obese or infertile patients. Megestrol acetateshould be the preferred treatment because it is associated witha better remission probability and a lower progression rate.Because the remission probability does not increase after 12months of treatment, the treatment period should not exceed12 months, and radical surgery should be discussed if noremission is attained within this time frame. The present re-sults also suggest that a close follow-up is mandatory forall patients managed conservatively, because the recurrenceprobability never reaches a plateau. Finally, except for thehistologic type of the tumor lesion, no factors were associatedwith a higher disease progression rate.
Acknowledgment: The authors thank Professor Serge Uzanfor expert analytical advice.
REFERENCES1. Navarria I, Usel M, Rapiti E, Neyroud-Caspar I, Pelte MF, Bouchardy C, et al.
Young patients with endometrial cancer: how many could be eligible forfertility-sparing treatment? Gynecol Oncol 2009;114:448–51.
2. KoskasM, Bendifallah S, Luton D, Darai E, Rouzier R. Safety of uterine and/orovarian preservation in young women with grade 1 intramucous endome-trial adenocarcinoma: a comparison of survival according to the extent ofsurgery. Fertil Steril 2012;98:1229–35.
3. Gunderson CC, Fader AN, Carson KA, Bristow RE. Oncologic and reproduc-tive outcomes with progestin therapy in women with endometrial hyperpla-sia and grade 1 adenocarcinoma: a systematic review. Gynecol Oncol 2012;125:477–82.
4. Ushijima K, Yahata H, Yoshikawa H, Konishi I, Yasugi T, Saito T, et al. Multi-center phase II study of fertility-sparing treatment with medroxyprogester-one acetate for endometrial carcinoma and atypical hyperplasia in youngwomen. J Clin Oncol 2007;25:2798–803.
VOL. 101 NO. 3 / MARCH 2014
5. Haoula Z, SalmanM,AtiomoW. Evaluating the association between endome-trial cancer and polycystic ovary syndrome. Hum Reprod 2012;27:1327–31.
6. Wise LA, Rothman KJ, Mikkelsen EM, Sorensen HT, Riis A, Hatch EE. Aninternet-based prospective study of body size and time-to-pregnancy.Hum Reprod 2010;25:253–64.
7. Fauvet R, Poncelet C, Boccara J, Descamps P, Fondrinier E, Darai E. Fertilityafter conservative treatment for borderline ovarian tumors: a French multi-center study. Fertil Steril 2005;83:284–90. quiz 525–6.
8. Randall TC, Kurman RJ. Progestin treatment of atypical hyperplasia andwell-differentiated carcinoma of the endometrium in women under age 40. Ob-stet Gynecol 1997;90:434–40.
9. Jadoul P, Donnez J. Conservative treatment may be beneficial for youngwomen with atypical endometrial hyperplasia or endometrial adenocarci-noma. Fertil Steril 2003;80:1315–24.
10. Laurelli G, Di Vagno G, Scaffa C, Losito S, Del Giudice M, Greggi S. Conser-vative treatment of early endometrial cancer: preliminary results of a pilotstudy. Gynecol Oncol 2011;120:43–6.
11. Minig L, Franchi D, Boveri S, Casadio C, Bocciolone L, Sideri M. Progestin in-trauterine device and GnRH analogue for uterus-sparing treatment of endo-metrial precancers and well-differentiated early endometrial carcinoma inyoung women. Ann Oncol 2011;22:643–9.
12. Han AR, Kwon YS, Kim DY, Kim JH, Kim YM, Kim YT, et al. Pregnancy out-comes using assisted reproductive technology after fertility-preserving ther-apy in patients with endometrial adenocarcinoma or atypical complexhyperplasia. Int J Gynecol Cancer 2009;19:147–51.
13. Minaguchi T, Nakagawa S, Takazawa Y, Nei T, Horie K, Fujiwara T, et al.Combined phospho-Akt and PTEN expressions associated with post-treatment hysterectomy after conservative progestin therapy in complexatypical hyperplasia and stage Ia, G1 adenocarcinoma of the endometrium.Cancer Lett 2007;248:112–22.
14. Signorelli M, Caspani G, Bonazzi C, Chiappa V, Perego P, Mangioni C.Fertility-sparing treatment in young women with endometrial cancer oratypical complex hyperplasia: a prospective single-institution experience of21 cases. BJOG 2009;116:114–8.
15. YuM, Yang JX,WuM, Lang JH, Huo Z, Shen K. Fertility-preserving treatmentin young womenwith well-differentiated endometrial carcinoma and severeatypical hyperplasia of endometrium. Fertil Steril 2009;92:2122–4.
16. Lawless JF, Singhal K. Efficient screening of nonnormal regression models.Biometrics 1978;34:318–27.
17. Kaku T, Yoshikawa H, Tsuda H, Sakamoto A, Fukunaga M, Kuwabara Y,et al. Conservative therapy for adenocarcinoma and atypical endometrial hy-perplasia of the endometrium in young women: central pathologic reviewand treatment outcome. Cancer Lett 2001;167:39–48.
18. Koskas M, Bendifallah S, Luton D, Darai E, Rouzier R. Independent externalvalidation of radiotherapy and its impact on the accuracy of a nomogram forpredicting survival of womenwith endometrial cancer. Gynecol Oncol 2011;123:214–20.
19. Bendifallah S, Genin AS, Naoura I, Chabbert Buffet N, Clavel Chapelon F,Haddad B, et al. A nomogram for predicting lymph node metastasis of pre-sumed stage I and II endometrial cancer. Am J Obstet Gynecol 2012;207:197.e1–8.
20. Kim YB, Holschneider CH, Ghosh K, Nieberg RK, Montz FJ. Progestinalone as primary treatment of endometrial carcinoma in premenopausalwomen. Report of seven cases and review of the literature. Cancer 1997;79:320–7.
21. Mao Y, Wan X, Chen Y, Lv W, Xie X. Outcomes of conservative therapy foryoungwomenwith early endometrial adenocarcinoma. Fertil Steril 2010;93:283–5.
23. Amezcua CA, ZhengW,Muderspach LI, Felix JC. Down-regulation of bcl-2 isa potential marker of the efficacy of progestin therapy in the treatment ofendometrial hyperplasia. Gynecol Oncol 1999;73:126–36.
24. Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR,Schweppe KW, et al. Classification and pharmacology of progestins. Matur-itas 2008;61:171–80.
25. Adlercreutz H, Eriksen PB, Christensen MS. Plasma concentrations ofmegestrol acetate and medroxyprogesterone acetate after single oral
administration to healthy subjects. J Pharm Biomed Anal 1983;1:153–62.
26. Thigpen JT, Brady MF, Alvarez RD, Adelson MD, Homesley HD, Manetta A,et al. Oral medroxyprogesterone acetate in the treatment of advanced orrecurrent endometrial carcinoma: a dose-response study by the GynecologicOncology Group. J Clin Oncol 1999;17:1736–44.
27. Gallos ID, Ganesan R, Gupta JK. Prediction of regression and relapse ofendometrial hyperplasia with conservative therapy. Obstet Gynecol 2013;121:1165–71.
28. Elizur SE, Beiner ME, Korach J, Weiser A, Ben-Baruch G, Dor J. Outcome ofin vitro fertilization treatment in infertile women conservatively treated forendometrial adenocarcinoma. Fertil Steril 2007;88:1562–7.
29. Duska LR, Garrett A, Rueda BR, Haas J, Chang Y, Fuller AF. Endometrial can-cer in women 40 years old or younger. Gynecol Oncol 2001;83:388–93.
30. Fujiwara H, Ogawa S, Motoyama M, Takei Y, Machida S, Taneichi A, et al.Frequency and characteristics of endometrial carcinoma and atypical hyper-plasia detected on routine infertility investigations in young women: a reportof six cases. Hum Reprod 2009;24:1045–50.
31. Gotlieb WH, Beiner ME, Shalmon B, Korach Y, Segal Y, Zmira N, et al.Outcome of fertility-sparing treatment with progestins in young patientswith endometrial cancer. Obstet Gynecol 2003;102:718–25.
32. Imai M, Jobo T, Sato R, Kawaguchi M, Kuramoto H. Medroxyprogesteroneacetate therapy for patients with adenocarcinoma of the endometrium whowish to preserve the uterus-usefulness and limitations. Eur J Gynaecol Oncol2001;22:217–20.
794
33. Mazzon I, Corrado G, Masciullo V, Morricone D, Ferrandina G, Scambia G.Conservative surgical management of stage IA endometrial carcinoma forfertility preservation. Fertil Steril 2009;93:1286–9.
34. Niwa K, Tagami K, Lian Z, Onogi K, Mori H, Tamaya T. Outcome of fertility-preserving treatment in young women with endometrial carcinomas. BJOG2005;112:317–20.
35. Ota T, Yoshida M, Kimura M, Kinoshita K. Clinicopathologic study of uterineendometrial carcinoma in young women aged 40 years and younger. IntJ Gynecol Cancer 2005;15:657–62.
36. Stanosz S. An attempt at conservative treatment in selected cases of type Iendometrial carcinoma (stage I a/G1) in youngwomen. Eur J Gynaecol Oncol2009;30:365–9.
37. Wang CB,Wang CJ, Huang HJ, Hsueh S, Chou HH, Soong YK, et al. Fertility-preserving treatment in young patients with endometrial adenocarcinoma.Cancer 2002;94:2192–8.
38. Yahata T, Fujita K, Aoki Y, Tanaka K. Long-term conservative therapy forendometrial adenocarcinoma in young women. Hum Reprod 2006;21:1070–5.
39. Yamazawa K, Hirai M, Fujito A, Nishi H, Terauchi F, Ishikura H, et al. Fertility-preserving treatment with progestin, and pathological criteria to predict re-sponses, in young women with endometrial cancer. Hum Reprod 2007;22:1953–8.
40. Yang YC, Wu CC, Chen CP, Chang CL, Wang KL. Reevaluating the safety offertility-sparing hormonal therapy for early endometrial cancer. Gynecol On-col 2005;99:287–93.
Study selection process for systematic review of fertility-sparing management of AH and EC.Koskas. Fertility-sparing endometrial neoplasia. Fertil Steril 2014.
Fertility and Sterility®
VOL. 101 NO. 3 / MARCH 2014 794.e1
SUPPLEMENTAL TABLE 1
Cox model of factors associated with remission and recurrence.
Variable
Remission Recurrence
Probability OR 95% CI P Probability OR 95% CI P
Age at diagnosis, per year – 0.96 0.94–0.98 .024 – 1.01 0.97–1.05 .820Gravidity