45
Prognosticat ion After Brain Injury Organ Donation Midland Collaborative 7 th May 2015 Birmingham Maria Cartmill
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | oswald-barker |
| View: | 216 times |
| Download: | 1 times |

Prognostication After Brain
InjuryOrgan Donation Midland Collaborative
7th May 2015 Birmingham Maria Cartmill

Are we able to prognosticate?

No

..or not accurately for an individual patient…

Hippocratic aphorism
“No head injury is so serious that it
should be despaired of nor so trivial that it can be
ignored”
Inappropriately ambiguous
Unduly optimistic
Unnecessarily pessimistic
Just about right

• Experienced neurosurgeon assessed 100 patients; 56% correct prognosis (Kaufman)
• If the initial GCS is reliable, 20% with the worst initial score will survive; 8-10% with GOS 4-5

Probabilities not prophecies!

Glasgow Outcome Scale (GOS)
Unfavourable• 1 Death• 2 Persistent vegetative state• 3 Severe disability (dependent on daily support)
------------------------------------------Favourable
• 4 Moderate disability (disabled, independent)• 5 Good recovery (resumption of normal life)

Glasgow Coma Scale (GCS)

Brain Injuries• Traumatic • Aneurysmal subarachnoid haemorrhage• Hypoxia

Traumatic• IMPACT/CRASH/TRISS/APACHE 2• Early prognostic indicators• Age• Motor part of GCS• Pupils• Imaging findings

Age• Poor outcome increases with increasing age • Poor outcome increases significantly in patients
aged > 60y• Independent of the increased frequency of
complications in elderly

Age vs outcomeAge (y) GOS 1 (%) GOS 5 (%)1-4 17 175-9 22 6110-14 20 4015-19 25 4021-40 35 3341-60 55 1561-80 80 5
(Alberico. Class II)

Age vs mortalityAge (y) GOS 1 (%)11-20 3521-30 3931-40 4541-50 5551-60 6661-70 7771-80 8581-90 95
(Teasdale. Class I)

Recent studies
• No age threshold• 40-50% increase in poor outcome each additional
10y (Mukkelhoven 2003, 5600pts)

Pupils
• Post resuscitation responses• “> 4mm is a dilated pupil”• Bilateral absent pupil response > 70% PPV of
poor outcome

Pupils vs GOS 1-2 outcome
No of patients in study
Bilat reactive
%
Unilateral fixed
%
Bilat fixed
%600 42 - 95
305 29 54 90
213 36 - 91
746 32 34 74
Ave 35 44 88
(www.braintrauma.org)

GCS (Motor)• The motor component of GCS provides the best
predictive value
GCS (M)
GOS 1 (%)
1 88.92-4 56.25 12.56 0.4
(Colohan. Class II)

Imaging findings• Multiple lesions worse than single• Midline shift > 15 mm worse than < 5 mm• Basal cisterns compressed• Traumatic subarachnoid haemorrhage

Basal cisterns• Compressed basal cisterns x 3 increased risk of raised ICP• x 2-3 increased risk of mortality• Direct relationship with pupils

Herniation

GOS vs basal cisterns
Basal cisterns
GOS %
1 2 3 4 5
Normal 22 6 16 21 35
Compressed
39 7 18 17 19
Absent 77 2 6 4 11
(218 pts with GCS <8)

Traumatic subarachnoid haemorrhage (TrSAH)
• Present in severe TBI (26-53%)• Mortality increased x2• Extent of TrSAH related to outcome• TrSAH is significant independent prognostic
indicator

SAH gradeFisher Grade Unfavourabl
e (GOS 1-3)Favourable (GOS 4-5)
1 (no blood) 0 14 2 (diffuse/ <1mm)
6 13
3 (clot/ >1mm) 15 6 4 (ICH or IVH) 7 0
(Harders. Class II)

ICP monitoring• Helps manage ICP• Does it alter outcome?• Useful if ICP > MAP• Pressures can be very high in children with good
outcome

MRI
• Using conventional imaging, presence of bilateral lesions in the dorsolateral upper brainstem appears to be the factor of greatest adverse prognostic significance.
• With MRS, low NAA/creatine ratio in the hemispheres and in the pons predicts a poor outcome.
(Weiss et al, Crit Care 2007; 11(5): 230)

Neurosurger
y registrars’
3am
hopelessnes
s chart

Aneurysmal subarachnoid haemorrhage

Natural history• Peak incidence 55-60y• 10-20% die before reaching medical care• 30 day mortality 45%• Overall mortality 51%• 1/3 survivors remain dependent• Of the other 2/3 – only 30% patients achieve their
previous quality of life
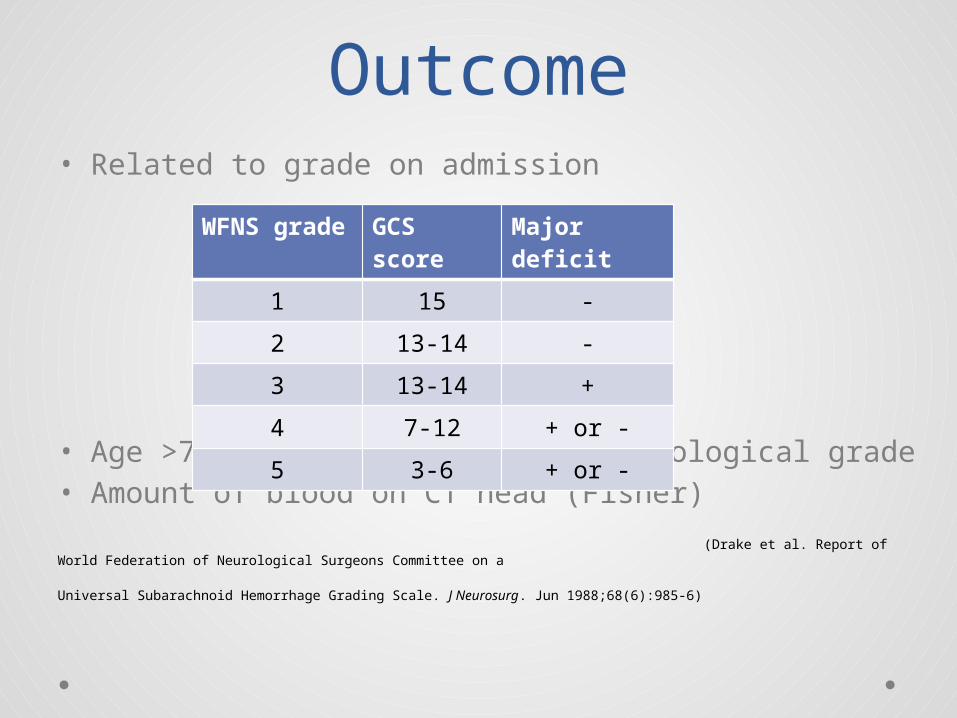
Outcome• Related to grade on admission
• Age >70y fare worse for each neurological grade• Amount of blood on CT head (Fisher)
(Drake et al. Report of World Federation of Neurological Surgeons Committee on a Universal Subarachnoid Hemorrhage Grading Scale. J Neurosurg. Jun 1988;68(6):985-6)
WFNS grade
GCS score
Major deficit
1 15 -
2 13-14 -
3 13-14 +
4 7-12 + or -
5 3-6 + or -

Physiology
• Average blood loss < 10mls• Rapid increase in ICP to > blood pressure• Cerebral stand still• Lose consciousness/ vomit/ severe headache• Possible seizure
• Permanent vs transient effect upon brain• Cerebral Stunning - “TIA of the midbrain”

When to prognosticate?
• Recommendation is to wait 6 hours to test• If diabetes insipidus/ hypothermia then likely
permanent• Keep assessing• Support in the interim• Allows for re-perfusion of central structures

Hypoxia

Pre-hospital• Poor outcome associated with:
• Type of arrhythmia: shockable >> non-shockable• Age > 70 years• Anoxia / no-flow time (witnessed) >25 mins• Duration of CPR• Co-morbidities
• Variable, with poor sensitivity / specificity• Cannot be used to reliably prognosticate

Clinical• Affected by therapeutic hypothermia (sedation) • GCS• Motor response to pain• Corneal reflexes
• Unaffected• Pupillary reflexes • Seizures / early myoclonus
(Cronberg et al. Recommendations from the Swedish Resuscitation Council. Resuscitation. 2013; 84(7): 867–72)

Imaging• MRI
• 4 stages• MRI sensitive but non-specific as single prognosticator • Grey-white-matter ratio (GWR)• Recent data suggests GWR <1.16 predicts poor
outcome (100% specific / 38% sensitive)
(Scheel et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2013; 21(1): 23)

Biomarkers• S-100B: calcium-binding astroglial protein• Neuron-specific enolase (NSE): isomer of enolase,
located in neurones• Ammonia & lactate
References
Intensive Care Society. Standards for the management of patients after cardiac arrest. 2008 Oct. http://www.ics.ac.uk/ics-homepage/guidelines-standards/ (accessed 12/09/2013)
Huntgeburth et al. Changes in neuron-specific enolase are more suitable than its absolute serum levels for the prediction of neurologic outcome in hypothermia-treated patients with out-of-hospital cardiac arrest. Neurocritical Care. 2014;20(3):358-366 Shinozaki et al. Blood ammonia and lactate levels on hospital arrival as a predictive biomarker in patients with out-of-hospitalcardiac arrest. Resuscitation. 2011; 82(4): 404–9.

Neurophysiology• SSEPs
• Bilateral median nerve stimulation• Measure cortical (N20) or shoulder (N9) potentials• Reliable specific test of neurological outcome (even with
hypothermia)
• EEG• Burst suppression / generalised epileptiform discharge
predict poor outcome• Issues of accuracy (not recommended)


Seizures• Seizures / myoclonus post-arrest + during cooling
associated with poor outcome• Myoclonic jerks on day 3, or after warming, do not
predict poor outcome• Lance-Adams, action-induced myoclonus without LOC
(Yadavmali et al. The Lance-Adams syndrome: helpful or just hopeful, after cardiopulmonary arrest. Journal of the Intensive Care Society. 2011; 12(4): 324 – 328)

Can we prognosticate?
Good Bad
EarlyReaction to pain (GCS M ≥ 5)Normal CTReactive EEG
Myoclonic status (+/- EEG)Reduced GWRIncrease in biomarkers
Late
Reaction to pain (GCS M ≥ 5)Normal CTLow biomarkersReactive EEG
GCS M 1 – 2Pupils / cornea unreactiveSSEP: bilateral lack of N20Abnormal CT / MRIHigh levels of biomarker
(Recommendations from the Swedish Resuscitation Council. Resuscitation. 2013; 84(7): 867–72)

When to prognosticate?
• Traditional guidance• 72 hours after arrest/event
• If cooled• 72 hours after reaching normothermia
(Wijdickset al. Neurology. 2006; 67(2): 203–10)

Are we able to prognosticate in patients with brain injury?

Conclusion• Not early
• We can give an early probability
• MDT approach recommended
• Time

















