34
PROJECT HEART END-OF-PROJECT REPORT CÔTE D'IVOIRE TOWARD AN HIV-FREE GENERATION: EIGHT YEARS OF IMPLEMENTING PROJECT HEART
| Date post: | 13-Mar-2018 |
| Category: |
Documents |
| Upload: | nguyendiep |
| View: | 215 times |
| Download: | 2 times |

PROJECT HEART END-OF-PROJECT REPORT
CÔTE D'IVOIRETOWARD AN HIV-FREE GENERATION:
EIGHT YEARS OF IMPLEMENTING PROJECT HEART

PROJECT HEART END-OF-PROJECT REPORT: CÔTE D'IVOIRETOWARD AN HIV-FREE GENERATION: EIGHT YEARS OF IMPLEMENTING PROJECT HEART
Project HEART was made possible through the generous support of the U.S. Centers for Disease Control and Prevention (CDC) under Cooperative Agreement U62/CCU123541. We are especially grateful for our close collaboration with the Ministry of Health in Côte d’Ivoire and for its tireless dedication to caring for and improving the lives of people living with HIV. We would also like extend our deep appreciation to our global and in-country implementing partners for their significant contributions. Additionally, we want to thank all of EGPAF’s sub-grantees, the health care professionals and EGPAF staff in Côte d’Ivoire who fight against HIV/AIDS every day, for their inspiring commitment to the Foundation’s mission of eliminating pediatric HIV.
AUTHORS: Dr. Joseph Diby, Director, Monitoring and Evaluation and Health Systems Strengthening, EGPAF/Côte d'Ivoire Shobana Ramachandran, Strategic Information and Evaluation Officer, EGPAF/Global Shauna Eisenberg, Associate Technical Officer, EGPAF/Global
WITH SUPPORT FROM STAFF FROM EGPAF/CÔTE D'IVOIRE AND FONDATION ARIEL GLASER POUR LA
LUTTE CONTRE LE SIDA PÉDIATRIQUE: Dr. Joseph Essombo, Country Director, EGPAF Dr Patricia Fassinou, Technical Director, EGPAF Dr. Clement Adjé, Technical Advisor for Care and Support, EGPAF Dr. Joseph Attiah, Senior Technical Advisor for Capacity Building and Transition, EGPAF Charles Boitini, Senior Monitoring and Evaluation Officer, Fondation Ariel Glaser Ali Coulibaly, Database Administrator, Fondation Ariel Glaser Jacqueline Dreesen, Transition Coordinator, EGPAF Dr. Joseph Kouakou, Senior Advisor, Program Evaluation, EGPAF Dr. Ebah Laurence, Technical Advisor, Monitoring and Evaluation, Fondation Ariel Glaser Dr. Eliane Leunkeu, Technical Advisor, PMTCT and Pediatrics, EGPAF Nda Jean Paul Kouadio, Technical Advisor, Monitoring and Evaluation, EGPAF Dr. Marc N’goran, Technical Advisor, Treatment, EGPAF Justine Pango, Monitoring and Evaluation Officer, EGPAF Katherine Warminsky, Graphic Designer, EGPAF
ADDRESS: Elizabeth Glaser Pediatric AIDS Foundation in Côte d'Ivoire Cocody, 2 Plateaux les Vallons Rue J50, Immeuble Avodiré 08 BP 2678 Abidjan 08 République de Côte d'Ivoire +225 22 41 45 05
DISCLAIMER: This publication was supported by Cooperative Agreement Number U62/CCU123541 from the U.S. Centers for Disease Control and Prevention (CDC) under the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC, PEPFAR, or the United States government.

TABLE OF CONTENTS
ACKNOWLEDGMENTS ........................................................................................................... ii
ABBREVIATIONS AND ACRONYMS ...................................................................................4
EXECUTIVE SUMMARY ...........................................................................................................5
INTRODUCTION ........................................................................................................................6
COUNTRY CONTEXT ...............................................................................................................7
EXPANSION OF ACCESS TO HIV SERVICES ...................................................................8
DELIVERING HIV CARE AND TREATMENT .....................................................................9
PREVENTING THE TRANSMISSION OF HIV FROM MOTHERS TO THEIR INFANTS ............................................................................17
STRATEGIC APPROACHES TO HIV SERVICE DELIVERY ...........................................20
CONTRIBUTIONS TO STRENGTHENING OF NATIONAL HEALTH SYSTEMS AND ENSURING PROGRAM SUSTAINABILITY ..............................................................................................23
TRANSITION: FROM PROJECT HEART TO LOCAL PROGRAM OWNERSHIP ......................................................................................23
CONCLUSION .........................................................................................................................25
ANNEX A: LIST OF SUB-GRANTEES ...............................................................................26
ALL PHOTOS OLIVIER ASSELIN

2 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 3
PROJECT HEART: CÔTE D'IVOIRE
4 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
LIST OF ABBREVIATIONS AND ACRONYMS
AIS AIDS Indicator Survey
AIDS acquired immune deficiency syndrome
ART antiretroviral treatment
ARV antiretroviral
CDC U.S. Centers for Disease Control and Prevention
CTX cotrimoxazole
DIPE Directorate for Information, Planning, and Evaluation (Direction de l'Information de la Planification et de l'Evaluation)
EID early infant diagnosis
EGPAF Elizabeth Glaser Pediatric AIDS Foundation
Fondation Ariel Glaser Ariel Glaser Pediatric AIDS Foundation (Fondation Ariel pour la Lutte contre le Sida Pédiatrique)
GLASER Global AIDS System for Evaluation and Reporting
GroForMéd Medical Training Group (Groupe de Formation Médicale)
HIV human immunodeficiency virus
HSS health systems strengthening
INFS National Institute for Training of Social Workers (Institut National de Formation Sociale)
JSI John Snow, Inc.
MOH Ministry of Health and the Fight Against HIV/AIDS (Ministère de la Santé et de la Lutte contre le Sida)
NGO non-governmental organization
OI opportunistic infection
OVC orphans and vulnerable children
PBF performance-based financing
PEPFAR U.S. President’s Emergency Plan for AIDS Relief
PMTCT prevention of mother-to-child transmission of HIV
PNLT National TB Program (Programme National de Lutte contre la Tuberculose)
PNPEC National Program for Care and Treatment of People Living with HIV (Programme National de Prise en Charge Médicale des PVVIH)
Project HEART Help Expand Antiretroviral Treatment to Children and Families
PSP National Pharmacy for Public Health (Pharmacie de la Santé Publique)
QI quality improvement
SIP Ivorian Pediatric Society (Société Ivoirienne de Pédiatrie)
TB tuberculosis
UNAIDS Joint United Nations Programme on HIV/AIDS
UFRSM University of Abidjan-Cocody Faculty of Medicine
UFRSPB University of Abidjan-Cocody Faculty of Pharmacy

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 5
PROJECT HEART: CÔTE D'IVOIRE
EXECUTIVE SUMMARY
Throughout the past three decades, HIV has ravaged Côte d’Ivoire, and the country has struggled to cope with the dire repercussions of an epidemic that disproportionately affected the most productive members of its society. However, in recent years, the epidemic’s tide has turned. HIV prevalence in the country has decreased significantly: in 2004, the Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated Côte d’Ivoire’s HIV prevalence at 7%, but by the end of 2009 this figure had dropped to 3.4%. Nonetheless, even at this lower level, Côte d'Ivoire has one of the highest burdens of HIV in West Africa. The epidemic is generalized, and according to the latest data available, Côte d’Ivoire is home to approximately 450,000 people living with HIV, including 63,000 children under age 15.1
From 1998 to 2003, Côte d’Ivoire benefited from a treatment access initiative pioneered by UNAIDS. During this time, seven health facilities, all located in Abidjan, the country’s commercial capital, provided care and treatment to HIV-positive patients, and nearly 2,100 patients were initiated on treatment.2 Although this was an accomplishment in a country scrambling to provide even basic care for those infected with the disease, it did not come close to meeting the HIV care and treatment needs of its population. Hence, in 2004, the U.S. government, through the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), began providing financial support to the government of Côte d’Ivoire to fight the spread of HIV. At the time, the main objectives of PEPFAR in Côte d'Ivoire were twofold:
• To prevent 200,000 new infections in five years
• To provide treatment for 77,000 HIV-positive people in five years
Since that time, the Elizabeth Glaser Pediatric Aids Foundation (EGPAF, or the Foundation), one of PEPFAR’s main implementing partners in Côte d’Ivoire, has been at the forefront of the fight against HIV in the country. Through the implementation of Project HEART, funded by the U.S. Centers for Disease Control and Prevention (CDC) since 2004, the Foundation has provided technical assistance to the Côte d’Ivoire Ministry of Health (MOH) in scaling up HIV prevention, care, and treatment services across the country; since then, the Foundation’s programs have been integral to the
1 UNAIDS, Report on the Global AIDS Epidemic, 2010.
2 National Care and Treatment Program (PNPEC) of Ministry of Health, March 2004.
fight against HIV in Côte d’Ivoire. By the end of September 2011, the Foundation had provided support services in 43 districts out of a total of 101 in the country and 12 regions out of a total of 19. Specifically, Project HEART in Côte d’Ivoire had accomplished the following:
• Supporting more than 350 sites providing HIV prevention, care, and treatment services
• Initiated more than 76,000 patients on antiretroviral treatment (ART)
• Enrolled more than 154,000 patients into HIV care
• Provided almost 900,000 pregnant women with prevention of mother-to-child transmission (PMTCT) services
• Distributed antiretroviral (ARV) prophylaxis to approximately 30,000 HIV-positive pregnant women3
• Averted an estimated 5,550 infant HIV infections4
These achievements are the results of complementary approaches and strategies combining capacity building of health care providers; implementation of national and international standards in delivering services; strengthening of health infrastructure; improvement of national health information systems; and provision of strong and continuous technical support to sites, districts, and regions to improve the quality of the interventions.
In addition, the Foundation created an affiliated national organization named Fondation Ariel Glaser pour la Lutte contre le Sida Pédiatrique (Fondation Ariel Glaser). In accordance with the renewed vision of PEPFAR to make health systems sustainable and nationally owned, Fondation Ariel Glaser will take over EGPAF’s support to prevention, care, and treatment sites, carrying on the legacy of EGPAF’s work under Project HEART. EGPAF, on the other hand, while remaining a key HIV treatment partner, will focus its efforts on strengthening health systems, from regional health directorates to national institutions.
3 Data from GLASER, September 2011. EGPAF’s Global AIDS System for Evaluation and Reporting. (GLASER) is the Foundation’s customizable, web-based data entry and storage database.
4 Based on a calculation used by PEPFAR: “The estimated number of infant HIV infections averted is calculated by multiplying the total number of HIV-positive pregnant women receiving ARV prophylaxis by 19%, to represent regimen effectiveness. This is an approximation of infections averted using a single-dose nevirapine regimen, which is expected to reduce HIV transmission from about 35% to approximately 16%. However, this is likely a significant underestimate.” PEPFAR Seventh Annual Report to Congress, 2011.

6 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
INTRODUCTIONSince 2004 the Elizabeth Glaser Pediatric AIDS Foundation (EGPAF, or the Foundation) has been heavily involved in the fight against HIV in Côte d’Ivoire. As one of the major U.S. Centers for Disease and Prevention (CDC)-funded partners in helping to carry out prevention of mother-to-child transmission (PMTCT) and care and treatment programs in the country, the Foundation has been rapidly expanding its programmatic scope and geographic reach in Côte d’Ivoire for the last eight years.
Implemented by the Foundation, Project HEART was the first major U.S. government-supported care and treatment program in Côte d’Ivoire. As such, over the last eight years, the Foundation has been the largest implementing partner in the country, enrolling approximately 154,000 patients in HIV care, starting more than 76,000 patients on antiretroviral treatment (ART), and providing antiretroviral (ARV) prophylaxis to approximately 30,000 HIV-positive pregnant women to prevent the transmission of HIV by September 2011. The program uses a diverse array of implementation models, all of which rely on working closely with the Ivorian Ministry of Health and the Fight against AIDS (MOH) to support the delivery of HIV services via public and private partners.
PROJECT HEART IN CÔTE D’IVOIRE
•97 staff dedicated to decreasing the burden of HIV/
AIDS in Côte d’Ivoire
•359 sites supported, offering PMTCT and ART services
•More than 76,000 people initiated on ART
•More than 154,000 people enrolled in HIV care
•Almost 900,000 HIV-positive pregnant women
provided with PMTCT services
•30,000 HIV-positive pregnant women provided with
ARV prophylaxis
•24,000 HIV-exposed infants provided with ARV
prophylaxis
Source: GLASER. Data as of September 2011.

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 7
PROJECT HEART: CÔTE D'IVOIRE
nationwide were in need of ART in 2009.8 Among those in need, a total of 72,011 patients received ART in 2009, a significant increase from the 51,820 patients who received ART in 2008.9 Coverage of HIV treatment and prevention interventions drastically increased in the past decade: 40% of those in need of treatment have received it, and 50% of HIV-positive pregnant women have been provided with access to PMTCT services.10
8 UNAIDS Epidemiological Fact Sheet, 2010.
9 Côte d'Ivoire MOH/DIPE/PNPEC, Annual Report of HIV Indicators of the Health Sector in Côte d’Ivoire, 2009.
10 UNAIDS Epidemiological Fact Sheet, 2010.
YAMOUSSOUKRO
DENGUÉLÉSAVANES
AGNÉBY
BAFING
BAS-SASSANDRA
DIX-HUITMONTAGNES
FROMAGER
HAUT-SASSANDRA
LACS
LAGUNES
MARAHOUÉ
MOYEN CAVALLY
MOYEN-COMOÉ
N’ZI-COMOÉ
SUD-BANDAMA SUD-COMOÉ
VALLÉE DUBANDAMA
WORODOUGOU
ZANZAN
PMTCT- and C&T-supported districtsPMTCT- supported districtsC&T-supported districtsOther districts
Odienné
Tengréle
Boundiali
Korhogo
Ferkessédougou
Bouna
Katiola Dabakala
Bondoukou
TandaM’bahiakro
Daoukro Agnibilékro
Bongouanou
Adzopé
Abengourou
Agboville
Tiassalé
DivoSassandra
San Pédro
Tabou
Guiglo
Soubré
GagnoaLakota
Issia
Duékoué
Danané
Toulepleu
Man
Bangolo
Biankouma
Trouba
Séguéla Mankono
Zuénoula
Daloa
Vavous
Boua�é
OuméToumodi
Sinfra
Bouaké
Tiébissou
Sakassou
Dimbokro
Bocanda
Granc Lahou
DabouAbidjan
Jacqueville
Grand Bassam
Aléne
Aboisso
Adiaké
Yamoussoukro
COUNTRY CONTEXTWith an estimated population of 21 million people and an overall adult HIV prevalence of 3.4%, Côte d’Ivoire is among the most affected countries in sub-Saharan Africa with respect to the HIV pandemic. Approximately 450,000 people are currently living with HIV, and in 2009 alone, the most recent year for which estimates are available, 36,000 individuals died as a result of AIDS.5 Children under the age of 15 have been particularly vulnerable to the epidemic, with approximately 63,000 children testing HIV-positive and 440,000 children have lost at least one parent to AIDS in 2009.6
The most recent national data available are from the AIDS Indicator Survey (AIS),7 which describes a generalized epidemic in Côte d’Ivoire marked by important gender and regional divides. Women were more likely than men to have acquired HIV, with current estimates putting the number of adult women infected with the virus at 220,000. Gender differences were especially pronounced among those aged 20–24 years, with prevalence rates at 4.5% among women versus 0.3% among men. HIV prevalence peaked among women aged 30–34 years at 14.9%, while male prevalence peaked at ages 40–44 at 7%.
While HIV prevalence rates in urban settings as compared with rural settings only showed marginal differences (5.4 % versus 4.1%), the epidemic was especially severe in certain geographic pockets in the country. To illustrate, in the northwestern part of Côte d’Ivoire, prevalence is approximately 1.7%. However, prevalence is almost 5.5% in the southeastern part of the country, which includes the commercial capital of Abidjan, a major city with the highest prevalence rate in the country at 6.1%.
It was against this backdrop that the Foundation implemented Project HEART in Côte d’Ivoire over the last eight years. Armed with the knowledge that the epidemic was markedly concentrated in particular populations, Project HEART’s approach to delivering prevention, care, and treatment services has been tailored and specific to Côte d’Ivoire’s unique epidemic context. As a consequence, Project HEART, along with the projects of other implementing partners in conjunction with the government of Côte d’Ivoire, made momentous strides in delivering HIV support services to those in need. To illustrate, according to the latest Joint United Nations Programme on HIV/AIDS (UNAIDS) data, approximately 190,000 adults
5 UNAIDS, Report on the Global AIDS Epidemic, 2010.
6 UNICEF, Children and AIDS: Fifth Stocktaking Report, 2010.
7 National Institute of Statistics at Ministry of HIV/AIDS, Côte d’Ivoire, and ORC Macro, 2005 AIDS Indicator Survey (AIS).
CÔTE D'IVOIRE AT A GLANCE
•Adult HIV prevalence: 3.4%
•450,000 people living with HIV by end of 2009, including:
� 20,000 HIV-positive pregnant women
� 63,000 HIV-positive children under 15 years old
•440,000 children have lost one or both parents due to AIDS
Sources: UNAIDS. Report on the Global AIDS Epidemic, 2010; UNICEF. Children and AIDS: Fifth Stocktaking Report, 2010.
EGPAF SUPPORTED REGIONS AND DISTRICTS IN CÔTE D’IVOIRE

8 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
EXPANSION OF ACCESS TO HIV SERVICES
One of the major achievements of Project HEART in Côte d’Ivoire has been the rapid expansion of HIV services in terms of both the sheer number of sites and geographic reach. Between 2004 and 2011, the Foundation supported a total of 420 sites, which included a combination of sites providing PMTCT services and care and treatment services. At the conclusion of Project HEART, the Foundation was actively supporting 359 sites. Of these, 320 sites were providing PMTCT services and 156 sites were providing care and treatment services, with several of these sites offering both services (Figure 1). This scale-up of supported sites has increased access to health services significantly in the country. To put these figures in context, an Ivorian national 2009 HIV report revealed that 33% of sites offering care and treatment and 47% of those providing PMTCT services nationwide were supported by the Foundation through Project HEART.11
11 Côte d'Ivoire MOH/DIPE/PNPEC, Annual Report of HIV Indicators of the Health Sector in Côte d’Ivoire, 2009.
In an effort to ensure that HIV services reach rural areas and strengthen the MOH’s overall health care delivery system, the Foundation opened four sub-offices in 2009 in the southern (San Pédro, Abidjan), eastern (Abengourou), and central (Bouaké) regions of the country. Within their respective catchment areas, these sub-offices have been responsible for supporting the MOH in the delivery of HIV services, implementing quality improvement (QI) activities at site level, reinforcing the sites’ relationships with local health authorities (e.g., regional health directorates, district management staff), and improving the overall sustainability of services. By September 2011, Project HEART was supporting prevention, care, and treatment programs in 12 out of 19 regions and 43 out of 101 districts across the country (Figure 2). This has dramatically contributed to the expansion of coverage of HIV-related services nationwide.
FIGURE 1. TRENDS IN THE NUMBER OF FOUNDATION-SUPPORTED SITES FROM OCTOBER 2004 TO SEPTEMBER 2011
“Project HEART has been a life-saving program.”Dr. Joseph Essombo, Country Director, EGPAF Côte d'Ivoire
0
50
100
150
200
250
300
350
400
Total numberof sites
Sites offering bothPMTCT and C&T
Sites offeringC&T only
Sites offeringPMTCT only
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Ap
r-Ju
n 20
05
Jan-
Mar
200
5
Oct
-Dec
200
4
NU
MB
ER
OF
SITE
S

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 9
PROJECT HEART: CÔTE D'IVOIRE
DELIVERING HIV CARE AND TREATMENTEGPAF’S CONTRIBUTION TO PEPFAR AND NATIONAL
TARGETS FOR HIV CARE AND TREATMENT
Project HEART built on the results of the Ivorian government’s National Access to HIV/AIDS Care and Treatment Initiative, which began in 1998. During the course of Project HEART, more than 154,000 people were enrolled in HIV care and 76,000 started on ART. These achievements make up a significant proportion of PEPFAR’s global care and treatment objectives, as well as its country-specific goals for Côte d'Ivoire (Table 1). In addition, when evaluating these results through the lens of Côte d’Ivoire’s national accomplishments, Project HEART’s contributions continue to be substantial (Table 2). In 2009, the latest year for which national data are available, the Foundation provided support for approximately half of the cumulative number of patients who ever started on ART in the country. In 2009, the latest year for which national data are available, EGPAF provided support for approximately half of the cumulative number of patients who started on ART in the country. The same trend was seen among the total number of patients who were continuing on ART by the end of 2009.
OVERALL TRENDS IN THE HIV CARE
AND TREATMENT
As mentioned above, Project HEART made enormous strides in the provision of HIV care and treatment services in Côte
d’Ivoire. From October 2004 to September 2011, the total number of patients enrolled into HIV care rose from 2,928 to 154,000. In addition, the number of patients started on treatment increased from 1,158 in October 2004 to 76,000 by the end of September 2011 (Figure 3). It should be noted that the drop in the cumulative number of patients supported by the Foundation in July 2007 occurred due to the fact that 18 care and treatment sites were transferred to another PEPFAR partner, who then began to report the cumulative numbers for these sites. Then again in June 2010, the cumulative number of patients ever on care or ART dropped slightly, following ten quarters of progressive increase. Despite increased access to care and treatment services, the figures reported for most care and treatment indicators decreased during this quarter because a major EGPAF-supported site, SMIT, refused to report. In addition, a data quality assessment was conducted during the quarter, and the subsequent corrective data management activities implemented helped the program to more correctly report on the major care and treatment indicators.
Analysis of patients enrolled in HIV care in Foundation-supported sites from 2004 to 2011 illustrates that the ratio of children to adults has remained fairly constant for the majority of Project HEART. Out of the 154,800 patients who ever enrolled in HIV care via Project HEART, almost 7,868 of them are children, which constituted approximately 5.1% of all patients (Figure 4).
FIGURE 2. MAP SHOWING THE FOUNDATION’S EXPANSION IN CÔTE D’IVOIRE FROM APRIL 2005 TO SEPTEMBER 2011
April 2005 September 2011
Abidjan
YAMOUSSOUKRO
Abidjan
YAMOUSSOUKRO

10 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
TABLE 1. PROJECT HEART’S CONTRIBUTIONS TO GLOBAL AND NATIONAL PEPFAR GOALS
PEPFAR Global Goals (2008) PEPFAR Country Goal (2008)Project HEART Contributions
(2004-2011)
Support care for more than 12 million
people, including 5 million OVC
Care for 385,000 persons affected by
HIV/AIDS, including OVC
154,000 adults and children
ever enrolled in care (40% of total
national goal)
Provide direct support for at least 3
million people on treatment
Provide treatment for 77,000 Ivorians
living with HIV/AIDS
76,000 adults and children
ever started on ART (99% of total
national goal)
12 Côte d'Ivoire MOH/DIPE/PNPEC, Annual Report of HIV Indicators of the Health Sector in Côte d’Ivoire, 2009. It should be noted that 2009 data are being used in this table because is the latest year for which national data are available for comparison to EGPAF’s contributions.
TABLE 2. COMPARISON OF EGPAF’S ACCOMPLISHMENTS AS COMPARED TO THE NATIONAL ACCOMPLISHMENTS IN TREATMENT IN 200912
HIV Treatment
IndicatorEGPAF’s
contributions
National
accomplishments
% of national
accomplishments
contributed by EGPAF
Number of sites 135 404 33%
Patients ever
placed on ART
61,306 117,584 52%
Patients newly
started on ART
3,661 29,002 13%
Patients currently on ART 34,968 72,011 49%

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 11
PROJECT HEART: CÔTE D'IVOIRE
Despite the tremendous efforts made during the last three years of Project HEART, it should be noted that the proportion of HIV-infected children who are enrolled in care and treatment programs remains relatively low at approximately 5%. In response to this, the Foundation began implementing the following strategies under Project HEART:
• Promotion of provider-initiated testing and counseling as the main strategy of HIV testing at pediatric entry points (e.g., immunization visits, weighing stations, nutrition consultations, outpatient and pediatric wards) at site level
• Expansion of early infant diagnosis (EID) among HIV-exposed infants using dried blood spot polymerase chain reaction testing
• Provision of technical assistance to the MOH in producing a set of pediatric guidelines for HIV care and treatment
• Classroom and on-site training in the identification of HIV-exposed children for physicians and non-physicians working with pediatric patients
When stratifying the data by gender, the proportion of patients enrolled in HIV care who are women is larger, with women making up almost 60% of all patients in Foundation programs under Project HEART. This has been true throughout the entire duration of Project HEART and is in line with the features of the HIV epidemic in Côte d’Ivoire, where HIV is more prevalent among women. In addition, it is a result of the large number of Foundation-supported PMTCT sites, where more HIV-positive women than man are identified.
FIGURE 3. CUMULATIVE NUMBER OF PATIENTS EVER ENROLLED IN HIV CARE AND CUMULATIVE NUMBER OF PATIENTS EVER STARTED ON TREATMENT FROM OCTOBER 2004 TO SEPTEMBER 201113
13 By June 2007, EGPAF was supporting 77 care and treatment sites, 20 of which were supported through ACONDA-VS, a local sub-grantee, and 32,371 of 88,974 cumulative patients on care were in ACONDA-supported sites. In July 2007, ACONDA-VS became a PEPFAR prime partner, and EGPAF transferred 18 care and treatment sites to them. This explains the drop in patients ever in care from the April-June 2007 quarter to the July-September 2007 quarter.
“Today, I feel very good and I am in good health thanks to PEPFAR and EGPAF. I hope that other people can benefit from their support as well.”Kevin Kouassi, Project HEART beneficiary and community counselor at Foundation-supported Centre de Santé Urbain Notre Dame des Apôtres
0
50,000
100,000
150,000
200,000
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
HIV TreatmentHIV Care
NU
MB
ER
OF
PATI
EN
TS

12 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 13
PROJECT HEART: CÔTE D'IVOIRECÔTE D'IVOIRE STORY OF HOPE: KEVIN KOUASSI
Kevin, son of a chief in rural Côte d’Ivoire, was 32 years old and living in the capital city of Abidjan when the fevers
started, followed by diarrhea, typhoid, and anemia. Within months, his weight dropped to 114 pounds, and he
moved back to his family’s village. Kevin's story might have ended there, all too typically, but for a wise and caring
father’s advice: Get tested for HIV.
Kevin went to the Centre NDA in Dimbokro — a health center supported by the Elizabeth Glaser Pediatric AIDS
Foundation through the President’s Emergency Plan for AIDS Relief (PEPFAR) — where he took an HIV test. The nurse
who provided post-test counseling asked Kevin to identify someone to whom he could disclose his HIV-positive status.
With some trepidation, Kevin chose his father.
“I wondered how he would react. Would he reject me?” Kevin recalls. “When I told him, he said, ‘You’re my son, and
I’m not going to reject you because of an illness.’ From then on, I became more confident. My father accompanied me
to all my appointments, he made sure that I took my medications, he paid for my prescriptions.”
Kevin started on antiretroviral therapy (ART) at the Centre NDA, and as of September 2007, he was one of nearly
35,000 patients in Côte d’Ivoire receiving Foundation/PEPFAR-supported ART.
Fifteen months later, Kevin was free of HIV-related infections and his weight had rebounded to 140 pounds. And now,
four years since his diagnosis, Kevin is still healthy. He works full-time as a community HIV counselor at the Centre NDA,
helping other HIV-positive clients who are facing the same issues he faced a few years ago. Kevin's father remains one
of his strongest supporters.
Kevin is engaged to a young woman who manages a small restaurant. When they first began their relationship, Kevin
encouraged her to be tested: She learned that she is also HIV-positive. At that point, Kevin told her about his positive
status.
Kevin's message, based on his own experience, is that being tested is the first step toward transforming HIV/AIDS from
a death sentence into a positive life. Citing his father’s lifesaving role, Kevin urges families to support those with HIV/
AIDS and enable them to enjoy a normal life.
“My wish,” Kevin says, “is that everyone’s parents be like my father.”

14 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
consistent CTX supplies for the prevention of OIs in people living with HIV/AIDS.
Under Project HEART, the Foundation supported the provision of comprehensive HIV care and treatment services to secure the well-being of families affected by HIV, ensuring their long-term health and survival. In 2004, the Foundation began supporting the government of Côte d'Ivoire and a host of local organizations in the provision of adult and pediatric treatment services. After a rapid phase of expansion in the first few years, Project HEART shifted its focus to building local capacity to manage and provide quality HIV services through the successful district approach.
RETENTION OF PATIENTS IN CARE AND TREATMENT
One of the major objectives of any program aiming to improve the health of people living with HIV/AIDS is the retention of patients in care and treatment. In recent years, the Foundation has focused on improving program quality, reducing the number of patients lost to follow-up, and enrolling more families and children into care and treatment at existing sites. This has been done by building local capacity using a variety of innovative approaches, including the district approach, community
COTRIMOXAZOLE FOR PREVENTION OF
OPPORTUNISTIC INFECTIONS
The delivery of cotrimoxazole (CTX) to patients responds to the need to curtail and prevent opportunistic infections (OIs) in people living with HIV/AIDS. In Côte d’Ivoire, the delivery of this medication has evolved over time, from being free to requiring that specific eligibility criteria be met according to national guidelines. In spite of numerous efforts and progress during the past four years, CTX delivery remains a challenge in Côte d'Ivoire.
This situation can be explained in part by the fact that the distribution of CTX to health facilities is conducted by Côte d’Ivoire’s National Pharmacy for Public Health (Pharmacie de la Santé Publique, or PSP). In Côte d'Ivoire, CTX is also used to treat common non-HIV-related infectious diseases. Thus the existence of two separate supply lines of CTX – from PEPFAR for the prevention of OIs in HIV-positive patients at no cost and from PSP for HIV-negative patients at a cost to patients – has often contributed to stockouts of the medicine and reduced access to CTX for people living with HIV/AIDS. The Foundation continues to work in close collaboration with PSP and the districts, as well as the health facilities, to ensure more
FIGURE 4. PERCENTAGE OF PATIENTS WHO ARE CHILDREN OUT OF ALL PATIENTS EVER ENROLLED IN HIV CARE AND INITIATED TREATMENT FROM JULY 2005 TO SEPTEMBER 2011
2%
4%
6%
8%
10%
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
HIV TreatmentHIV Care
PER
CE
NTA
GE
OF
PATI
EN
TS

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 15
PROJECT HEART: CÔTE D'IVOIRE
groups, and a QI approach using the EZ-QI tool,15 which was implemented at 124 Foundation-supported sites. In addition, in collaboration with John Snow, Inc. (JSI), the Foundation has developed and implemented approaches to quality of care that encourage the retention of patients in care and treatment services, including the following:
• Strengthening post-testing activities
• Completing the patient registration process, including all necessary contacts to reach the patient in case of missed appointment
• Involving community counselors in the care and treatment of patients, including psychosocial support and support groups – community-based organizations were active at 46 sites by the end of September 2011.)
• Reinforcing use of a database tool to allow for improved follow-up and tracking of patients enrolled in care and treatment
• Producing cohort data in care and treatment sites
• Implementing a phone tree and calling patients who missed appointments
• Searching for patients lost to follow-up through home visits and phone calls
• Continued assessment of quality of care and implementation of activities to improve quality of care in sites
• Organizing quarterly district meetings with all sites to assess and analyze their accomplishments
FIGURE 5. NUMBER AND PERCENTAGE OF PATIENTS RECEIVING COTRIMOXAZOLE PER QUARTER FROM JULY 200714 TO SEPTEMBER 2011
“Even more important than the treatment we provide, and more important than the prevention we provide, is our ability to involve the community in the fight against AIDS.”Dr. Anthony Tanoh, Executive Director, Fondation Ariel Glaser pour la Lutte contre le Sida Pédiatrique en Côte d'Ivoire
14 EGPAF-supported sites began reporting on cotrimoxazole data from July 2007.
15 The EZ-QI tool is a quality assessment and quality improvement initiative developed in collaboration with University Research Co., the National Program for Care and Treatment of PLWHA (People Living with HIV (Programme National de Prise en Charge Médicale des PVVIH, or PNPEC), and JSI.
0
4,000
16,000
14,000
12,000
10,000
8,000
6,000
2,000
18,000
20,000
22,000
0
20%
10%
30%
40%
50%
60%
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Number of patients who received CTX Percentage of children incare who received CTX
Percentage of adults in carewho received CTX
NU
MB
ER
OF
PATI
EN
TS
PER
CE
NTA
GE
OF
PATI
EN
TS

16 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
Together, these actions have contributed to helping the Foundation optimize proper support for patients currently on care and treatment. Nonetheless, crude retention rates for patients in HIV care and on treatment have had a downward slope over the course of Project HEART (Figure 6). On the one hand, this phenomenon can be attributed to the fact that the crude retention rates will naturally decline, because they are calculated using the total cumulative number of patients who ever enrolled in the program, so each patient that drops out reduces the percentage still in care.
On the other hand, keeping patients in care and treatment programs has been a struggle in Côte d’Ivoire (Figure 7). Specifically, EGPAF and other PEPFAR implementing partners have found the following particularly challenging:
• Prevention of loss to follow-up through complete registration of patients enrolled in care
• Continuous and routine follow-up of patients enrolled in care and treatment
• Task shifting through the effective integration of community workers and social workers into routine follow-up activities
• Active search for patients lost to follow-up through home visits and phone calls
• Effective quarterly and semiannual cohort studies and assessments using the EZ-QI tool to pinpoint areas for intervention based on data
Until June 2007, EGPAF supported the local NGO Aconda as sub-grantee, and data from Aconda sites were included in EGPAF global data. The retention rates in Aconda’s sites were much lower than EGPAF’s overall average. When Aconda became a prime PEPFAR partner in spring 2007, the denominator went down as well as the total number of attrition. That has led to an increase in the crude retention rate in Q3 2007.
In 2009, CDC, along with the National HIV Care and Treatment Program (Programme National de Prise en Charge Médicale des PVVIH, or PNPEC) and EGPAF, conducted an evaluation of 34 HIV care and treatment sites. Specifically, the evaluation looked at clinical characteristics and retention rates among
FIGURE 6. CRUDE RETENTION RATES AMONG PATIENTS WHO EVER ENROLLED IN HIV CARE FROM OCTOBER 2004 TO SEPTEMBER 201116
16 Crude retention rates were calculated by dividing the number of patients who were on ART during any given quarter by the cumulative number of patients who ever initiated ART during the life of the program. Data on the number of patients who were on ART during a given quarter were only collected from January 2005 onwards.
20%
10%
0%
40%
90%
80%
70%
60%
50%
30%
100%
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Adults Children
PER
CE
NTA
GE
OF
PATI
EN
TS
PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 17
PROJECT HEART: CÔTE D'IVOIRE
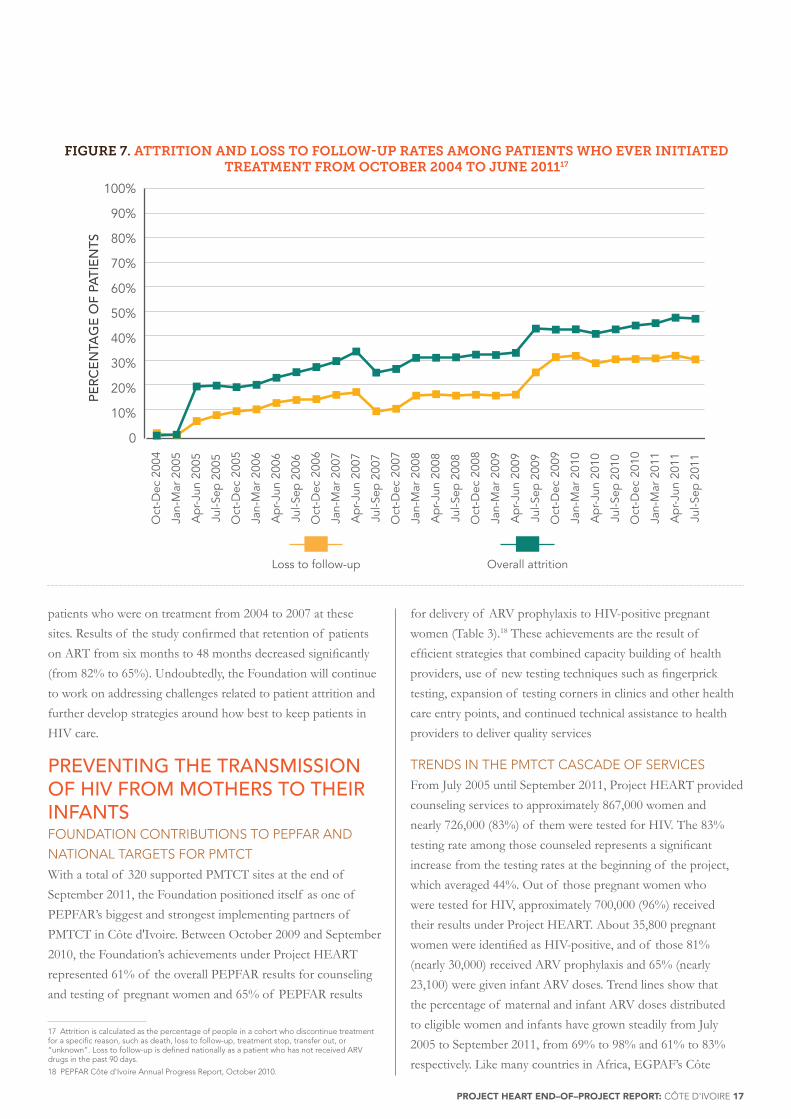
FIGURE 7. ATTRITION AND LOSS TO FOLLOW-UP RATES AMONG PATIENTS WHO EVER INITIATED TREATMENT FROM OCTOBER 2004 TO JUNE 201117
17 Attrition is calculated as the percentage of people in a cohort who discontinue treatment for a specific reason, such as death, loss to follow-up, treatment stop, transfer out, or “unknown”. Loss to follow-up is defined nationally as a patient who has not received ARV drugs in the past 90 days.
18 PEPFAR Côte d'Ivoire Annual Progress Report, October 2010.
patients who were on treatment from 2004 to 2007 at these sites. Results of the study confirmed that retention of patients on ART from six months to 48 months decreased significantly (from 82% to 65%). Undoubtedly, the Foundation will continue to work on addressing challenges related to patient attrition and further develop strategies around how best to keep patients in HIV care.
PREVENTING THE TRANSMISSION OF HIV FROM MOTHERS TO THEIR INFANTSFOUNDATION CONTRIBUTIONS TO PEPFAR AND
NATIONAL TARGETS FOR PMTCT
With a total of 320 supported PMTCT sites at the end of September 2011, the Foundation positioned itself as one of PEPFAR’s biggest and strongest implementing partners of PMTCT in Côte d'Ivoire. Between October 2009 and September 2010, the Foundation’s achievements under Project HEART represented 61% of the overall PEPFAR results for counseling and testing of pregnant women and 65% of PEPFAR results
for delivery of ARV prophylaxis to HIV-positive pregnant women (Table 3).18 These achievements are the result of efficient strategies that combined capacity building of health providers, use of new testing techniques such as fingerprick testing, expansion of testing corners in clinics and other health care entry points, and continued technical assistance to health providers to deliver quality services
TRENDS IN THE PMTCT CASCADE OF SERVICES
From July 2005 until September 2011, Project HEART provided counseling services to approximately 867,000 women and nearly 726,000 (83%) of them were tested for HIV. The 83% testing rate among those counseled represents a significant increase from the testing rates at the beginning of the project, which averaged 44%. Out of those pregnant women who were tested for HIV, approximately 700,000 (96%) received their results under Project HEART. About 35,800 pregnant women were identified as HIV-positive, and of those 81% (nearly 30,000) received ARV prophylaxis and 65% (nearly 23,100) were given infant ARV doses. Trend lines show that the percentage of maternal and infant ARV doses distributed to eligible women and infants have grown steadily from July 2005 to September 2011, from 69% to 98% and 61% to 83% respectively. Like many countries in Africa, EGPAF’s Côte
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Jan-
Mar
201
1
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Ap
r-Ju
n 20
05
Jan-
Mar
200
5
Oct
-Dec
200
4
Overall attritionLoss to follow-up
PER
CE
NTA
GE
OF
PATI
EN
TS

18 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
FIGURE 8: NUMBER OF WOMEN WHO WERE COUNSELED AND TESTED FOR HIV AND RECEIVED THEIR TEST RESULTS FROM JULY 2005 TO SEPTEMBER 2011
TABLE 3: COMPARISON OF EGPAF TO NATIONAL ACCOMPLISHMENTS IN PMTCT IN 200919
PMTCT
Indicator EGPAF’s contribution National accomplishments
% of national
accomplishments
contributed by EGPAF
Number of sites 260 554 47
Pregnant women
counseled
185,960 396,958 47
Pregnant women tested 168,780 342,698 49
Pregnant women who
received results
164,532 325,411 51
Pregnant women who
received ARVs for
prophylaxis
5,802 9,320 62
19 Côte d'Ivoire MOH/DIPE/PNPEC, Annual Report of HIV Indicators of the Health Sector in Côte d’Ivoire, 2009. It should be noted that 2009 data are being used in this table because is the latest year for which national data are available for comparison to EGPAF’s contributions.
0
10,000
20,000
30,000
40,000
50,000
60,000
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Tested for HIV Recieved resultsCounseled
NU
MB
ER
OF
WO
ME
N

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 19
PROJECT HEART: CÔTE D'IVOIRE
FIGURE 9: NUMBER OF WOMEN WHO TESTED HIV-POSITIVE AND RECEIVED ARV PROPHYLAXIS AND ESTIMATED NUMBER OF INFANT INFECTIONS AVERTED FROM JULY 2005 TO SEPTEMBER 2011
FIGURE 10: PERCENTAGE OF HIV-POSITIVE PREGNANT WOMEN AND INFANTS WHO RECEIVED ARV PROPHYLAXIS OUT OF ALL WOMEN IDENTIFIED AS HIV-POSITIVE ATTENDING FOUNDATION-
SUPPORTED SITES FROM JULY 2005 TO SEPTEMBER 2011
TABLE 3: COMPARISON OF EGPAF TO NATIONAL ACCOMPLISHMENTS IN PMTCT IN 200919
0
500
1,000
1,500
2,000
2,500
Jul-S
ep 2
011
Ap
r-Ju
n 20
11
Oct
-Dec
201
0
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Infant ARV prophylaxisWomen ARV ProphylaxisTotal Identi�ed HIV PositiveTested HIV Positive Infections averted
NU
MB
ER
OF
WO
ME
N
0
30%
20%
10%
90%
80%
70%
60%
50%
40%
100%Ju
l-Sep
201
1
Ap
r-Ju
n 20
11
Oct
-Dec
201
0
Jan-
Mar
201
1
Jul-S
ep 2
010
Ap
r-Ju
n 20
10
Jan-
Mar
201
0
Oct
-Dec
200
9
Jul-S
ep 2
009
Ap
r-Ju
n 20
09
Jan-
Mar
200
9
Oct
-Dec
200
8
Jul-S
ep 2
008
Ap
r-Ju
n 20
08
Jan-
Mar
200
8
Oct
-Dec
200
7
Jul-S
ep 2
007
Ap
r-Ju
n 20
07
Jan-
Mar
200
7
Oct
-Dec
200
6
Jul-S
ep 2
006
Ap
r-Ju
n 20
06
Jan-
Mar
200
6
Oct
-Dec
200
5
Jul-S
ep 2
005
Maternal ARV prophylaxisInfant ARV prophylaxis
PER
CE
NTA
GE
OF
WO
ME
N/C
HIL
DR
EN

20 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
d'Ivoire PMTCT program started by providing single-dose nevirapine to HIV-infected women. In 2006, the country adopted a policy of combination prophylaxis, and EGPAF shifted progressively from provision of the single dose to a complex regimen to HIV-positive pregnant women. Since early 2009, only the combination prophylaxis has been used in Foundation-supported sites. In all, using conservative measures, it is estimated that EGPAF’s programs under Project HEART averted at least 5,550 new HIV infections.20
Over the course of Project HEART, the Foundation has worked with maternal and child health clinics to integrate HIV care and treatment services into maternal and infant care to allow for continuity of care. However, the part of the PMTCT cascade relating to follow-up of the mother-child pair remains a challenge in Côte d'Ivoire, both for the Foundation and at the national level. Under the guidance of CDC and PEPFAR through follow-on projects in Côte d'Ivoire, the Foundation will continue to contribute to the improvement of this part of the PMTCT cascade through the following:
• Initiation of CD4 count for HIV-positive pregnant women;
• Increased efforts for enrollment in ART of eligible HIV-positive pregnant women;
• Increased efforts for identification and testing of HIV-exposed infants in order to initiate treatment for HIV-positive children; and
• Establishment of a link between the maternal departments and the pediatric services in health facilities, which will be an essential step toward meeting the objectives of the PMTCT program.
Côte d’Ivoire has adopted the 2010 WHO guidelines and has opted for Option A – treating all HIV-positive pregnant women. However, this strategy has not yet been implemented in the country. Over the course of Project HEART, the Foundation has supported the MOH at the national level to adopt and plan for implementation of the guidelines.
STRATEGIC APPROACHES TO HIV SERVICE DELIVERY DISTRICT APPROACH
The district approach is an integral pillar in the Foundation’s health systems strengthening (HSS) strategy in Côte d’Ivoire, as well as in other countries where the Foundation works. Since the beginning of Project HEART in 2004, the Foundation has worked hand-in-hand with the MOH to plan, implement, and monitor quality prevention, care, and treatment interventions. The district approach, first implemented in one region in 2007, was designed to improve efficiency and sustainability in scaling up HIV/AIDS services by building ownership and capacity 20 See footnote 4.

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 21
PROJECT HEART: CÔTE D'IVOIRE
at the health district level. The close partnership between the Foundation, the MOH, regional directorates, and district health management teams offered an opportunity to transfer good governance values such as accountability and participation. The results of the district approach speak for themselves. The introduction of the district approach in Abengourou in 2007 quadrupled the number of people on ART in the region within a year, from 260 to 1,024, and the number of people tested for HIV quadrupled as well.22 The model was expanded to all Foundation-supported districts by the end of Project HEART.
Using this model, the Foundation made health districts the cornerstone of the health care service delivery system. This resulted in increased ownership by the districts on activities ranging from the opening of new HIV care and treatment sites to the provision of technical assistance to sites. By empowering health districts in HIV service delivery, Project HEART has led to a rapid increase in access to HIV services within the district catchment areas and thus has directly contributed to the significant increase in the number of people enrolled into care and treatment programs in Côte d’Ivoire.
PERFORMANCE-BASED FINANCING
To address the discrepancy that sometimes exists between the provision of financial resources to sites and their performance, the Foundation piloted a performance-based financing (PBF) model at four Foundation-supported private clinics in 2006. The PBF model includes a systematic measurement of a predefined class of indicators. Support to the sites was then preconditioned on the results achieved in these indicators, thereby establishing a direct link between the funding of sites and their accomplishments in terms of services delivered to patients. This effort was intended to increase service utilization by patients and improve and strengthen the capacity of health care providers in HIV service delivery. In comparing sites employing this model with ones not employing the PBF model, EPGAF demonstrated that the model served to motivate health workers to reach their site-level targets. In addition, the PBF model was proven effective in increasing the uptake of PMTCT services and enhancing the accountability of the sub-awardees. By September 2011, the PBF model had expanded to 32 sites in 21 districts using 20 indicators linked to Project HEART’s and PEPFAR’s programmatic priorities.22
EARLY INFANT DIAGNOSIS (EID)
In line with its mission to eliminate pediatric HIV, the Foundation, through Project HEART, has substantially improved EID among HIV-exposed infants using dried blood spot polymerase chain reaction testing. By the end of September 2011, EID was part of routine HIV services offered at 268 Foundation-supported sites. This has dramatically improved provision of HIV care to infants and thus resulted in earlier treatment of HIV-positive children.
INTEGRATION OF TUBERCULOSIS (TB) AND HIV
SERVICES
Since 2007, the Foundation has identified TB/HIV management as a top priority to be part of the care package offered to all HIV-positive patients. By the end of September 2011, 50% (61) of the 121 sites providing TB services nationally were supported by the Foundation. During the last five years, the Foundation has worked closely with the National TB Program (Programme National de Lutte contre la Tuberculose, or PNLT) to build the capacity of care providers in TB/HIV management and to refurbish and provide equipment to sites providing TB/HIV services (Figure 11).
In addition, Foundation staff continuously provided technical assistance to care providers offering TB/HIV services and periodically conducted joint supportive supervisory visits to sites with PNLT staff in an effort to improve the quality of the services delivered. Under Project HEART, the Foundation has continued to work with PNLT to implement TB infection control plans and improve the management of multi-drug-resistant TB cases at Foundation-supported sites.
21 PEPtalk, PEPFAR Côte d’Ivoire Newsletter, No. 3, July 2008
22 EGPAF, Technical Issue Brief: Performance-Based Financing: A Promising Strategy to Improving HIV Service Delivery, 2010.
“During the past 6 years, we put in place the foundation. That foundation is skilled care providers; the foundation is laboratories that we equipped; and the foundation is the improvement of physical infrastructure.”Dr. Joseph Essombo, Country Director, EGPAF Côte d'Ivoire

22 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
TABLE 4: KEY RESULTS OF HSS ACTIVITIES UNDERTAKEN THROUGH PROJECT HEART
Domain Key Results
Human resources
development
through pre-service
training
In 2007, EGPAF developed a pre-service training program with the University of Abidjan-Cocody, Faculty of Medicine (UFRSM) and Faculty of Pharmacy (UFRSPB), and in 2009, expanded it to the National Institute for Training of Social Workers (INFS).The program prepares and assigns students for three- to six-month placements at underserved and rural EGPAF-supported locations offering HIV, TB, and malaria services. Through Project HEART, 245 students participated in this program and received an infectious disease certificate at the end of the placement. About half of the student doctors and social workers have requested to remain at their placement sites.•At UFRSM, 69 doctors were trained in care and treatment of HIV/AIDS, malaria, and TB.
In addition, 19 doctors received a netbook computer. These doctors received ongoing training via the internet, and a network was set up for communication and sharing of knowledge and experiences between doctors who have been trained through the initiative.
•At UFSSBP, 25 pharmacists were trained in laboratory and strategic supply management.
•At INFS, 151 social workers were trained to provide support and follow-up to people living with HIV/AIDS.
Human resources
development
through on-site
training to improve
quality of care
Partnerships with the Medical Training Group (GroForMéd) and the Ivorian Pediatric Society (SIP) focused on in-service training and mentorship in sites. •With GroForMéd, the Foundation produced a curriculum for refresher training and a
guide for trainers. Deliverables included:•Training manual for site support and on-site mentoring •Refresher training for 32 health care providers involved in the care and treatment of
people living with HIV/AIDS •SIP developed several training and capacity building resources, including:
•An information repository for pediatric care and treatment focal points •A job aid for pediatric care and treatment •Refresher training manuals for pediatric care and treatment•An internship manual • Investigation to determine conditions for provider-initiated counseling and testing
in pediatric sites •Conducted 32 technical assistance missions in pediatric sites
Improvement of
quality of care and
treatment
EGPAF worked with the General Inspectorate for Health and the Fight Against AIDS to
strengthen operational capacity, and provided support for the development of a procedure
document to control the quality of service and support for inspectors.
Improvement of data
quality management
EGPAF worked extensively with DIPE to strengthen operational capacities, and assisted
them with the recruitment of 41 data managers to ensure timely completion of data
collection and analysis
Health system
financing
EGPAF provided PBF to more than 30 private sites, often with admirable results. Some major achievements include:
•PMTCT: Organizations receiving PBF, making up only 8% of supported PMTCT sites (24 out of 297 sites), contributed up to 26% to the entire results of EGPAF/Côte d'Ivoire between January and June 2010.
•Counseling and testing: PBF organizations – 10% of supported testing sites (33 of 327 sites) – contributed to 60% of all results between January and March 2010.
•Care and treatment: PBF organizations – 24% of supported care and treatment sites (33 of 135) – contributed to 38% of the results between January and June 2010.
Support for
decentralization:
The district approach
Networks of care were implemented in two health districts, Aboisso and Yamoussoukro. Networking of the health facilities helps to improve access and continuity of care and services, increase geographic coverage, and ultimately increase the overall number of beneficiaries reached.
PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 23
PROJECT HEART: CÔTE D'IVOIRE
CONTRIBUTIONS TO STRENGTHENING NATIONAL HEALTH SYSTEMS AND ENSURING PROGRAM SUSTAINABILITY One of the Foundation’s strategies in the response to the HIV/AIDS epidemic in Côte d’Ivoire was to engage the MOH and other government agencies and non-governmental organizations (NGOs) in a process of HSS. The majority of HSS activities completed under Project HEART (Table 4) worked toward close collaboration and building relationships with local government agencies and NGOs to:
• Reverse the deficit in human resources in the health sector by developing various worker training programs
• Increase the quality of services offered in health facilities by fostering country ownership at the central level, in accordance with the national, organizational, and structural guidelines of the MOH
• Improve data quality through the strengthening of human and operational capacity of selected health facilities in collaboration with the national Directorate for Information, Planning, and Evaluation (DIPE)
• Support the decentralization and expansion of care and support services for people living with HIV/AIDS
Project HEART has greatly contributed to strengthening the capacities of the health providers to implement activities and to the administrative and technical capacity of local government
agencies and NGOs to implement those activities. These activities were conducted in collaboration with the MOH, the technical teams of CDC and PEPFAR, and other technical implementing partners working with PEPFAR.
TRANSITION: FROM PROJECT HEART TO LOCAL PROGRAM OWNERSHIPIn January 2008, CDC requested that the Foundation, along with all other PEPFAR 1.0 partners, transition existing Project HEART services to locally owned and operated organizations over the course of three years. The Foundation responded by implementing transition plans aimed at meeting this goal to realize long-term sustainability of HIV services in Côte d'Ivoire. The goal of the Project HEART transition was to support the strengthening of capacity of local government, health care institutions, and civil society to manage comprehensive HIV/AIDS programs in Côte d’Ivoire. The Foundation’s transition plan contained three main elements.
1. Strengthening of the national health system through expanded collaboration with pre-service training institutions and capacity building of the regional and district health systems to establish ownership and sustainability of high quality HIV prevention, care, and treatment services
2. Establishment of an independent, Ivorian NGO empowered to support continuity of high quality HIV/AIDS prevention, care, and treatment service delivery and to compete for and directly manage U.S. government and/or other available funds
3. Strengthening of the capacity and leadership of other local organizations and existing partners, such as private volunteer organizations, community-based organizations, and faith-based organizations
EGPAF HSS ACCOMPLISHMENTS 2005-2011 BY THE NUMBERS
•2,024 health providers trained in care and treatment of people living with HIV/AIDS
•1,913 health providers trained in PMTCT
•47 laboratories performing biological tests for people living with HIV/AIDS (hematology, biochemistry, and CD4)
•73 care and treatment sites with an information system for data management
•91 care and treatment sites with SIMPLE1 software for management and dispensation of ARVs
•More than 100 health facilities renovated
“Until now, the push has come directly from international organizations. We have now arrived at a moment where it is important for national organizations to involve themselves in the fight against AIDS at all levels.”Dr. Anthony Tanoh, Executive Director, Fondation Ariel Glaser pour la Lutte contre le Sida Pédiatrique en Côte d'Ivoire

24 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
These activities complemented the programmatic work that involved collaboration with district health management teams to strengthen technical capacity and the ability to oversee and coordinate HIV service delivery at clinical sites.
Consequently, under Project HEART, EGPAF established the Fondation Ariel Glaser pour la Lutte contre le Sida Pédiatrique en Côte d’Ivoire (Fondation Ariel Glaser). As an independent, locally owned and governed organization, Fondation Ariel Glaser will fill a gap in the current NGO landscape by serving as a national leader and expert in HIV service delivery with a focus on children and partnering with the Ivorian government for systems strengthening (Figure 12). To ensure that the transition process to Fondation Ariel Glaser is thorough and the new organization is robust, EGPAF also implemented a comprehensive transition monitoring plan, which included the development and implementation of several tools to assess
organizational capacity and viability, site capacity to provide high quality services, and the availability and access to services at the community level.
Under the affiliation model, EGPAF and Fondation Ariel Glaser will share common elements such as the logo, the mission, the bonds of governance, and the principles and standards of affiliation. This model of affiliation makes it possible for Fondation Ariel Glaser to access EGPAF’s technical and organizational resources to ensure, among other things, high standards of quality for the programs and service delivery upon transition. The affiliation relationship in Côte d'Ivoire was motivated by:
• Promotion of local sustainability and ownership of programs
• Ensured high standards for programs and operational accountability for the global organization and brand
FIGURE 12. MODEL FOR TRANSITION OF PROJECT HEART ACTIVITIES
In spring 2011, EGPAF and Fondation Ariel Glaser applied separately to CDC for funds to continue the successful and extensive work completed by EGPAF under Project HEART in a complementary way, and both were successful in their applications. Under its new project, Project Djidja, EGPAF will continue to do some HIV service delivery work and will begin to focus more on HSS and capacity building of Fondation Ariel Glaser. EGPAF has transitioned a number of sites and districts to Fondation Ariel Glaser, which will provide high quality service delivery under its new CDC-funded Project Cœur d’Ariel. Both organizations will work in close collaboration with districts, regions, and appropriate national organizations to build local health systems and increase country ownership of HIV service delivery programs.
Before Transition
Do
no
rU
SC
ôte
d’I
vo
ire
Districts,Region, CBOs
Districts,Region, CBOs
Districts,Region, CBOs
After Transition

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 25
PROJECT HEART: CÔTE D'IVOIRE
• Promotion of viability through local ownership
• Maintenance of partnership with EGPAF to ensure strong support for capacity building and fundraising
In spring 2011, EGPAF and Fondation Ariel Glaser applied separately to CDC for funds to continue the successful and extensive work completed by EGPAF under Project HEART in a complementary way, and both were successful in their applications. Under its new project, Project Djidja, EGPAF will continue to do some HIV service delivery work and will begin to focus more on HSS and capacity building of Fondation Ariel Glaser. EGPAF has transitioned a number of sites and districts to Fondation Ariel Glaser, which will provide high quality service delivery under its new CDC-funded Project Cœur d’Ariel. Both organizations will work in close collaboration with districts, regions, and appropriate national organizations to build local health systems and increase country ownership of HIV service delivery programs.
CONCLUSIONProject HEART has been instrumental in slowing the spread of HIV within the Ivorian population in an environment of great need, only exacerbated by the political and military crisis since 2002. It is clear that Project HEART has helped break the chain of HIV transmission and enabled more than 5,800 children to be born HIV-free. It has also helped tens of thousands of people to know their HIV status and to adopt safer behaviors.
Finally, Project HEART has contributed to prolonging the lives of tens of thousands of HIV-positive people and keeping families healthy by making ARV drugs and cotrimoxazole available for protection against opportunistic infections and disease progression.
In the recent past, PEPFAR has adapted its support of HIV programs in sub-Saharan Africa: it has gone from sponsoring emergency service delivery programs to advocating for sustainable approaches that include the strengthening of health systems for improved country ownership of interventions by national institutions. With this in perspective, EGPAF and Fondation Ariel Glaser, through Project Djidja and Project Cœur d’Ariel respectively will continue to deliver quality services to the Ivorian people and will work in line with the priorities expressed by the government of Côte d'Ivoire and PEPFAR to strengthen overall health systems. The term djidja in Dioula, one of Côte d’Ivoire’s many national languages, translates to “perseverance,” and it is in this spirit that the Foundation will carry forth the legacy left by Project HEART and work toward elimination of pediatric AIDS in Côte d’Ivoire and worldwide.

26 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE
1. ACONDA
2. Association de Soutien a L'Autopromotion Sanitaire Urbaine (ASAPSU)
3. Association des Eglises Chretiennes de Côte d'Ivoire
4. Association des Gestionnaires de Centre de Santé a Base Communautaire
5. Association Ivoirienne pour Le Bien-Être Familial
6. Association pour la Promotion de la Santé de la Femme (APROSAM)
7. Association pour la Santé Communautaire de Kennedy-Clouetcha
8. Association Saint Camille de Lellis
9. Center for Intergrated Bioclinical Research in Abidjan (CIRBA)
10. Centre Congregation des Sœurs de l'Ange Gardien
11. Centre de Santé La Providence
12. Centre de Santé Urbain Communautaire d'Abidjan Agban
13. Centre de Santé Urbain Communautaire Cocody Anono
14. Centre de Santé Urbain de Komborodougou
15. Centre Hospitalier et Universitaire de Treichville
16. Centre Médical Mère Maria Elisa Andreoli
17. Centre Médico Social Walé (AIFUP)
18. Centre Solidarité Action Sociale (CSAS)
19. Côte d'Ivoire Prosperité
20. Dispensaire Baptiste de Torgo
21. Dispensaire Foyer de Charité de Kotobi
22. Dispensaire Urbain Confessionnel Sainte Anne de Bocanda
23. District de Yamoussoukro
24. El Rapha Healthcare Center
25. Espace Confiance
26. Formation Sanitaire Urbaine Communautaire d'Abobo Sagbé
27. Fondation Ariel Glaser pour la Lutte contre le Sida Pédiatrique en Côte d'Ivoire
28. Groupe Biblique de Hôpitaux Cote d'Ivoire
29. HOPE Worldwide Côte d'Ivoire
30. Hôpital Baptiste de Ferkessédougou
31. Hôpital General D'Ayame (Mission Catholique)
32. Centre de Santé Urbain Confessional Notre Dame des Apôtres
33. Centre de Santé Communautaire Pianzola Lab of the Catholic Mission
34. Renaissance Santé Bouaké
35. Ruban Rouge Côte d'Ivoire
36. Centre de Santé Urbain Sainte Thérèse de l'Enfant Jésus
37. Amis des Hommes
38. Association Bouaké Eveil
39. Association de Cooperation Internationale et de Developpement
40. Association des Jeunes Patriotes pour la Santé et le Developpement
41. Association des Tresseuses Contre le Sida (ATRECSI)
42. CERAB
43. Cocody Cite d'Espoir
44. Foundation Djigui la Grande Esperance
45. Initiative Plus
46. Notre Grenier
47. ONG Agnintie Nitche
APPENDIX A: LIST OF SUB-GRANTEES AND PARTNERS
PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 27
PROJECT HEART: CÔTE D'IVOIRE
48. ONG Elan d'Amor
49. ONG Femmes Actives
50. ONG Fraternité
51. ONG Ko'Kohoua
52. ONG la Manne du Jour
53. ONG Manasse
54. ONG M'Bade Victoire
55. ONG Ruban Rouge Abengourou
56. ONG Solidarité Plus
57. ONG Tous Pour le Taukpé
58. GroForMéd
59. Helen Keller International
60. Inspection Générale de la Santé et de l'Hygiène Publique
61. Institut National de Formation Sociale
62. Institut Pasteur Côte d'Ivoire
63. JHPIEGO
64. Ministère de la Santé et de l'Hygiène Publique/DIPE
65. Ministère de la Santé et de l'Hygiène Publique/IGSLS
66. Ministère de la Santé et de l'Hygiène Publique/PNSR
67. Société Ivoirienne de Pédiatrie (SIP)
68. University of Abidjan-Cocody Faculty of Medicine (UFRSM)
69. University of Abidjan-Cocody Faculty of Pharmacy (UFRSPB)
70. University of California, San Francisco

28 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 29
PROJECT HEART: CÔTE D'IVOIRE

30 ELIZABETH GLASER PEDIATRIC AIDS FOUNDATION | PEDAIDS.ORG
PROJECT HEART: CÔTE D'IVOIRE

PROJECT HEART END–OF–PROJECT REPORT: CÔTE D'IVOIRE 31
PROJECT HEART: CÔTE D'IVOIRE
The Elizabeth Glaser Pediatric AIDS Foundation is
a nonprofit organization dedicated to preventing
pediatric HIV infection and eliminating pediatric
AIDS through research, advocacy, and prevention,
care, and treatment programs. Founded in 1988, the
Foundation works in 16 countries around the world.
Elizabeth Glaser acquired HIV through a blood
transfusion and unknowingly passed the virus on to
her daughter, Ariel, and her son, Jake. Following
Ariel’s death in 1988, Elizabeth joined with close
friends Susie Zeegen and Susan DeLaurentis to
create a foundation with one mission: to bring
hope to children with AIDS. Elizabeth lost her own
battle with AIDS in 1994, but thanks to the work of
the Elizabeth Glaser Pediatric AIDS Foundation,
Jake is now a healthy young adult, and hundreds of
thousands of other children have a chance to lead
longer, more vibrant lives.

1140 Connecticut Avenue NW, Suite 200Washington, D.C. 20036
t 202.296.9165f 202.296.9185e [email protected]
www.pedaids.org
facebook.com/hivfree @EGPAF

















