28
Prolactin- secreting pituitary tumors Rosario Pivonello Department of Molecular and Clinical Endocrinology and Oncology, Federico II University, Naples, Italy
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | javier-spittle |
| View: | 218 times |
| Download: | 3 times |

Prolactin-secreting
pituitary tumorsRosario PivonelloDepartment of Molecular and Clinical
Endocrinology and Oncology, Federico II University, Naples, Italy

• Prolactinomas are the most frequent pituitary tumors,with an estimated prevalence in the adult population of 100 per million population
• Their frequency varies with age and sex, occurring most frequently in females between 20 and 50 yr old, when the ratio between the sexes is estimated to be 10:1.
• After the fifth decade of life, the frequency of prolactinomas is similar in both sexes.
• Prolactinomas account for approximately 40% of all pituitary adenomas and are an important cause of hypogonadism and infertility.
Epidemiology
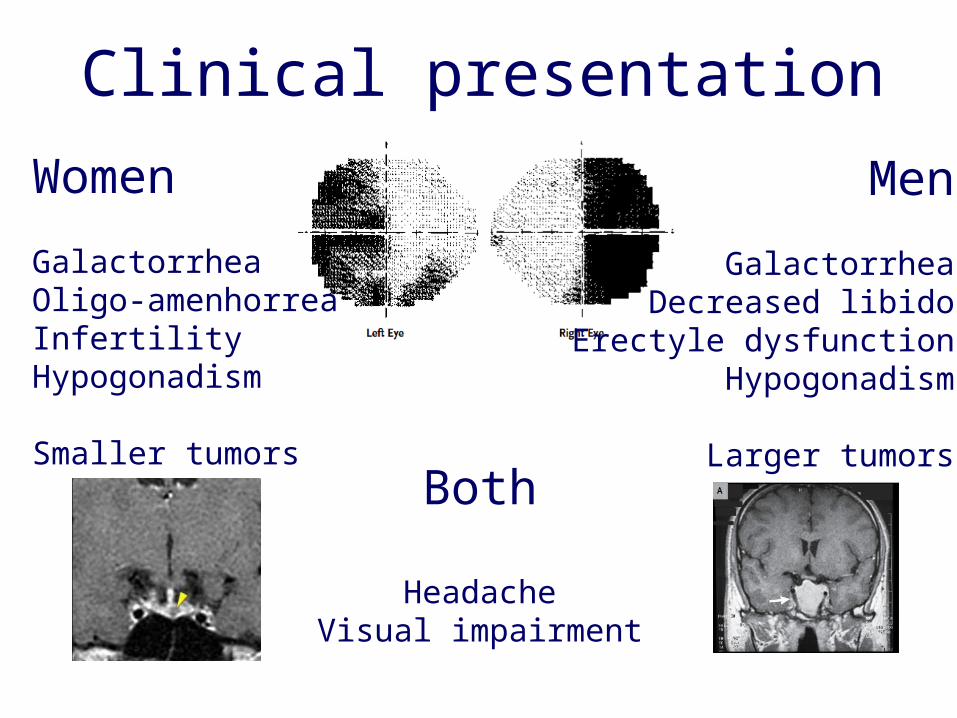
Clinical presentationWomen
GalactorrheaOligo-amenhorreaInfertilityHypogonadism
Smaller tumors
Men
GalactorrheaDecreased libido
Erectyle dysfunctionHypogonadism
Larger tumorsBoth
HeadacheVisual impairment
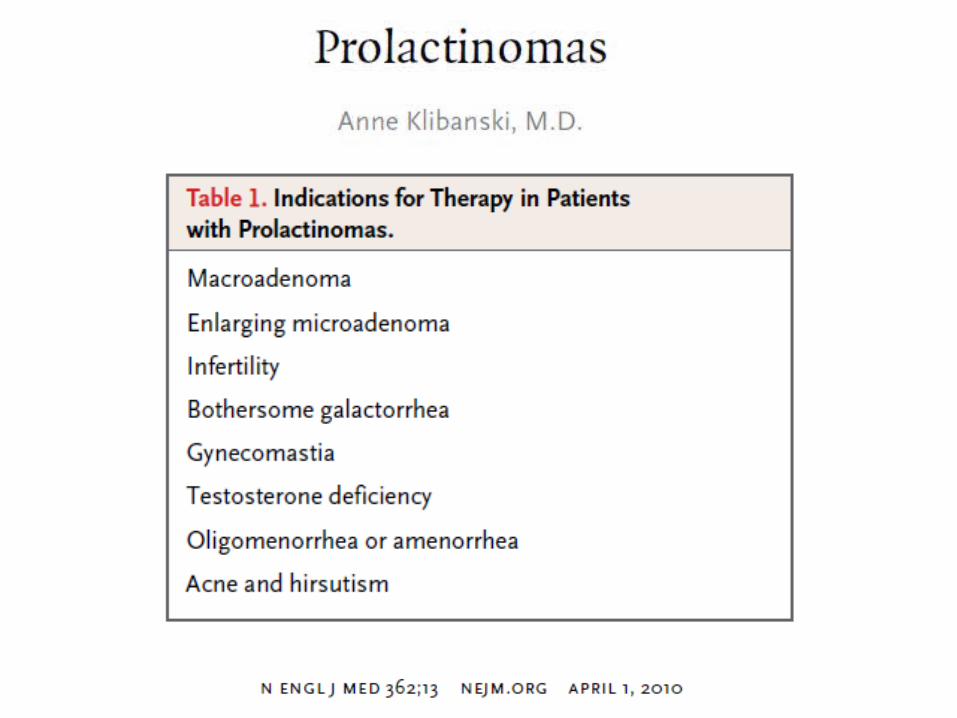


Tumor removal, preservation of normal residual function, and prevention of recurrences
Restoration of normal secretion
Relief of symptoms directly caused by PRL excess
Prevention of complications (hypogonadism, osteoporosis)
Colao and Lombardi. Lancet. 1998;352:1455.

Patients With Micro-, Macroadenomas, and Idiopathic Hyperprolactinemia Primarily Treated With Various Dopamine
Agonists
Dopamine Agonist Total
No. With Normal PRL
% With Normal PRL
Bromocriptine1 997 757 76
Pergolide2 98 85 87
Cabergoline3 612 544 89
1. Fossati, Friesen, Bergh, Badano, Crosignani, Horowitz, Molitch, Liuzzi, van der Heijden, Brue, Webster, Pascal-V, Pinzone, DiSarno, Sabuncu.
2. Horowitz, Kleinberg, L’Hermite, Freda.3. Ferrari, Ferrari, Webster, Pascal-V, Muratori, Verhelst, Pinzone, Di Sarno, Sabuncu.
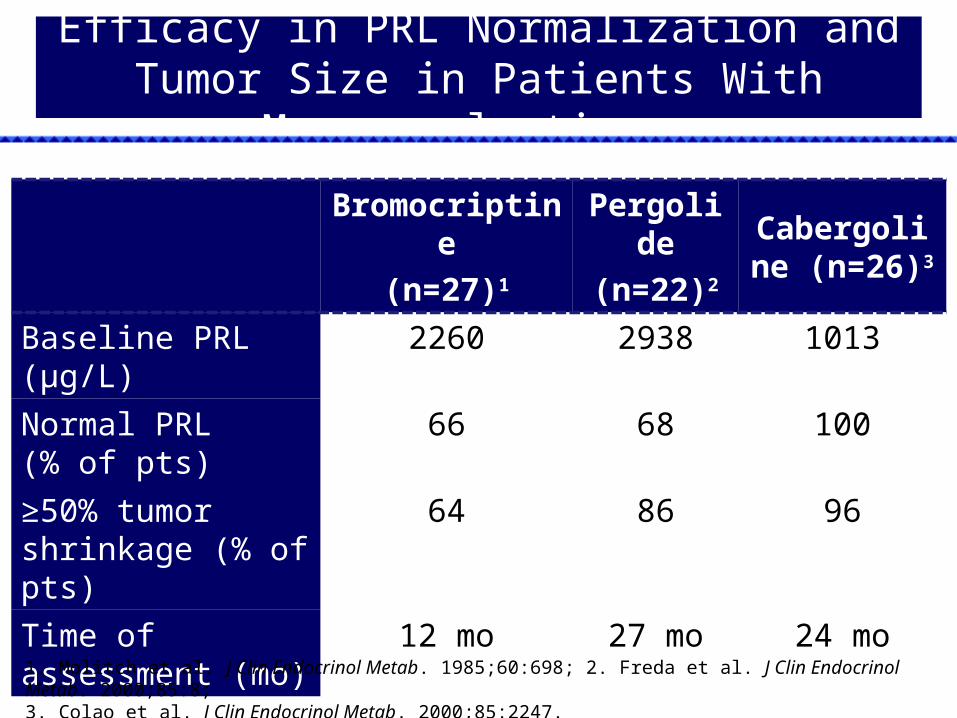
Efficacy in PRL Normalization and Tumor Size in Patients With Macroprolactinoma
Bromocriptine(n=27)1
Pergolide(n=22)2
Cabergoline (n=26)3
Baseline PRL(µg/L)
2260 2938 1013
Normal PRL (% of pts)
66 68 100
≥50% tumor shrinkage (% of pts)
64 86 96
Time of assessment (mo)
12 mo 27 mo 24 mo
1. Molitch et al. J Clin Endocrinol Metab. 1985;60:698; 2. Freda et al. J Clin Endocrinol Metab. 2000;85:8; 3. Colao et al. J Clin Endocrinol Metab. 2000;85:2247.

Basal1180 μg/L
1 week550 μg/L
4 weeks55 μg/L
Early Changes of Prolactinomas After Cabergoline

Basal
1 week
1 month

Remission after cabergoline withdrawal
32% (Koppelman et al. Ann Intern Med. 1984;100:115)
33% (Jeffcoate et al. Clin Endocrinol (Oxf). 1996;45:299)
35% (Schlechte et al. J Clin Endocrinol Metab. 1989;68:412)
>55% (Sisam et al. Fertil Steril. 1987;48:67)

Normalization of PRL levels Tumor size at MRI No tumor Residual tumor but ≥50% tumor reduction of baseline size in
presence of a ≥5 mm distance from optic chiasm and in the absence of invasion of one or both cavernous sinuses or any other cerebral area
Follow-up after withdrawal at least 24 months
Cabergoline Withdrawal: Inclusion Criteria
Colao et al. N Engl J Med. 2003;349:2023.
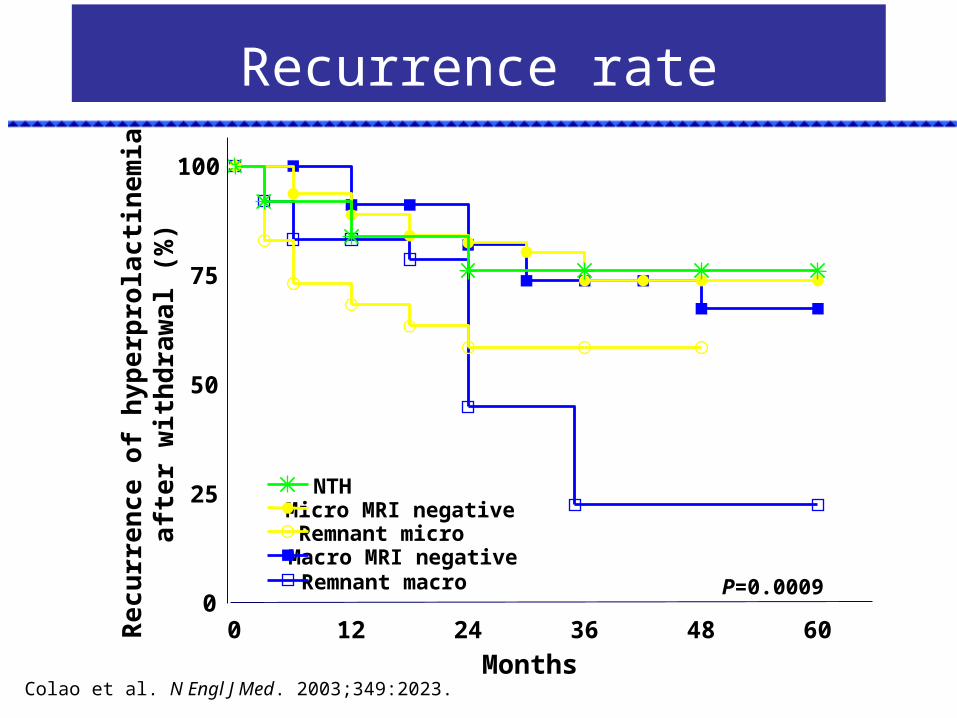
Recurrence rate
0 12 24 36 48 600
25
50
75
100
NTHMicro MRI negativeRemnant microMacro MRI negativeRemnant macro P=0.0009
Months
Recu
rren
ce o
f hyp
erpr
olac
tinem
iaaft
er w
ithdr
awal
(%)
Colao et al. N Engl J Med. 2003;349:2023.
SummarySummary
Recurrence after cabergoline withdrawal was low in patients achieving tumor disappearance and did not differ in NTH (24%), micro-(26.2%) and macroprolactinomas (32.6%)
Recurrence of hyperprolactinemia was higher in patients still presenting small remnant tumors at MRI (41.5% in micro- and 77.5% in macroprolactinomas)
In no case of recurrence of hyperprolactinemia did tumor regrow or symptoms reappear
Colao et al. N Engl J Med. 2003;349:2023.Colao et al. N Engl J Med. 2003;349:2023.

Cardiac valve regurgitation after cabergoline withdrawal


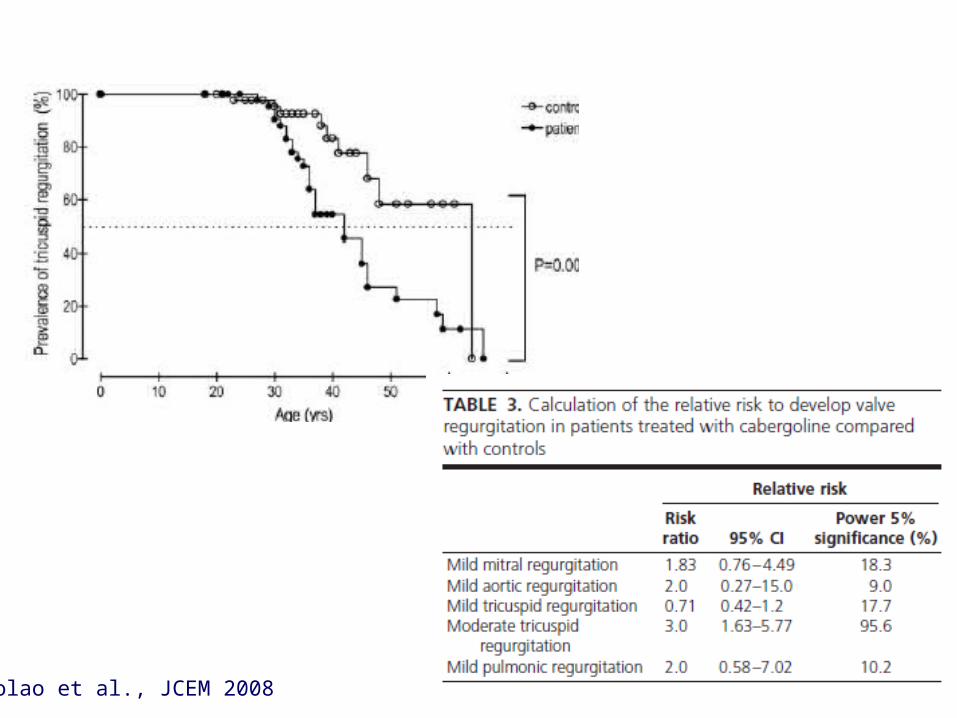
Colao et al., JCEM 2008

Colao et al., JCEM 2008


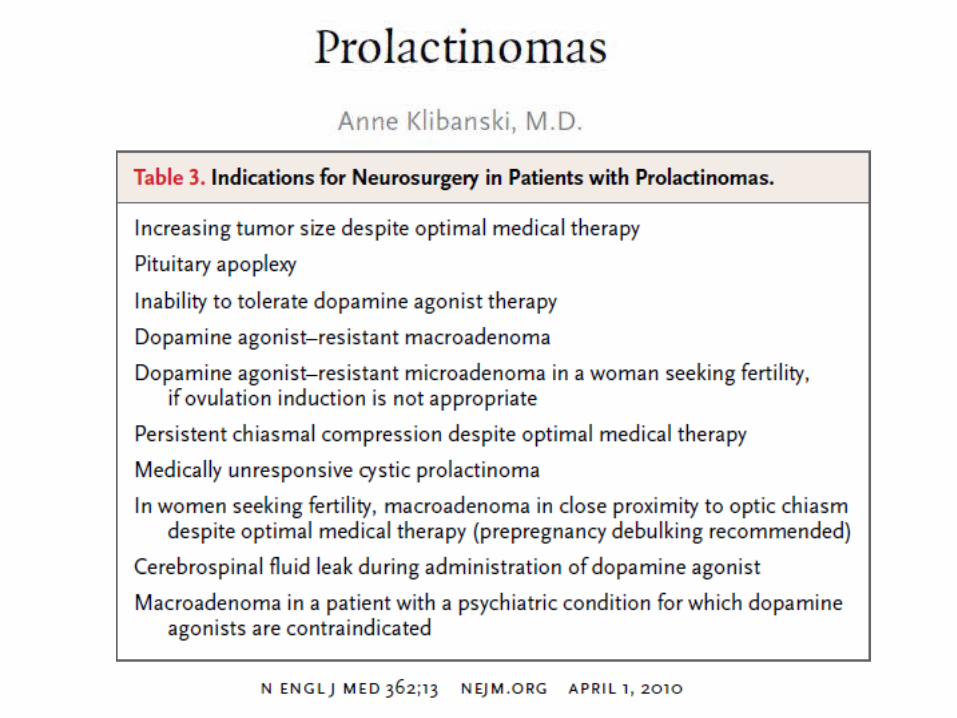
No controversies on macroprolactinomas: 1st treatment is pharmacotherapy (cabergoline). Surgery indicated in patients with resistant adenomas
In young patients with microprolactinoma, the surgical choice should be offered based on the high likelihood of definitive cure (risk of tricuspid regurgitation!)
Patients fully responsive to bromocriptine or cabergoline who showed the disappearance of the tumor in MRI could be withdrawn from the drug and followed up.
There is an increased risk for asymptomatic tricuspid regurgitation that should be investigated more carefully
Conclusions

Thanks

















