Proliferative verrucous leukoplakia of the gingiva Adam Fettig, DMD,a M. Anthony Pogrel, DDS, MD, a Sol Silverman Jr, MA, DDS,b Thomas E. Bramanti, DDS, PhD,c Maria DaCosta, MS,b and Joseph A. Regezi, DDS, MS,b San Francisco, Calif UNIVERSITY OF CALIFORNIA
Objective. The purpose of this study was to describe the clinical-pathologic features of what appears to be a gingival form of proliferative verrucous leukoplakia. Study design. Ten adult patients with recurrent and histologically progressive gingival leukoplakias who were diagnosed and treated at the University of California, San Francisco between 1994 and 1999, comprised the subject group for this investigation. Clinical and microscopic features were reviewed. Proliferation indices and p53 expression were evaluated immunohistochemically, and the presence of human papillomavirus (HPV) DNA was determined by using polymerase chain reaction (PCR) amplification. Results. Lesions presented as solitary or regional flat/papillary/verrucal leukoplakias of the free and attached gingiva (toothbearing areas only). With time, flat lesions developed a papillary or verruciform profile. Although lesions were recurrent, they were confined to the gingiva, and multiple lesions did not develop. Half the patients used tobacco, and HPV could not be detected by using PCR. Microscopically, 6 cases began as hyperkeratotic lesions, and 4 initially exhibited a psoriasiform pattern with a marked inflammatory component. With recurrences, the lesions became progressively atypical histologically. The proliferation indices for these lesions showed modest increases over normal epithelium, and positive p53 staining was evident in 4 of 1 0 cases, indicating a disruption of the keratinocyte cell cycle in these lesions. The mechanism associated with the positive p53 staining (protein binding to wild type p53 versus mutation of the p53 gene) was not determined. Lesions recurred after conservative scalpel or laser excision, and many developed into verrucous or squamous cell carcinoma. Conclusions. Proliferative verrucous leukoplakia of the gingiva (PVLG) appears to be a subset of oral proliferative verrucous leukoplakia. It can be characterized as a solitary, recurring, progressive white patch that develops a verruciform architecture and may not be associated with HPV. PVLG has an unpredictable course and is at risk for development into verrucous or squamous cell carcinoma. Currently, there is no way to determine or predict which gingival white lesions will follow the clinical course described for this group of patients with PVLG. (Oral Surg Oral Med Oral Pathol Oral Radio! Endod 2000;90:723-30)
Idiopathic leukoplakias of the oral cavity can arise from either keratinized or nonkeratinized epithelium. Although this lesion is often associated with a tobacco habit, many times an etiologic factor cannot be identified. Although most lesions follow a benign course, some transform into squamous cell carcinoma. A highrisk type of oral leukoplakia, known as proliferative verrucous leukoplakia (PVL), develops in multiple oral sites and progresses from hyperkeratosis, to verrucous hyperplasia, to verrucous or squamous cell carcinoma.1.2 Human papillomavirus (HPV), subtype 16, appears to be a possible etiologic factor in PVL,3.4 whereas tobacco seems to play only a minor role.5 The diagnosis is made by a combination of clinical and microscopic findings.
We have seen a number of adult patients who have PVL-Iike lesions of the gingiva. These lesions appear as solitary white lesions and are confined to the free or attached gingiva (buccal, lingual, interdental), although direct extension into adjacent tissue has occurred.
· Lesions have been recurrent and progressive, and many have developed into verrucous carcinoma or papillary squamous cell carcinoma. Microscopy has been deceptively bland in early stages. Laser ablation and surgical stripping typically have been ineffective at controlling this process.
The purpose of this investigation is to present a series of patients with recurrent proliferative verrucous leukoplakia of the gingiva (PVLG). Clinical-pathologic parameters are defined, tissue is analyzed for evidence of HPV DNA by using polymerase chain reaction (PCR)-based technology, and cell cycle is assessed through immunohistochemical staining for p53 and Ki-67 proteins.
MATERIAL AND METHODS Sequential patients (n = l 0) with recurrent papil
lary/verruciform leukoplakias of the gingiva who have
723
724 Fettig et a/
been treated at the University of California, San Francisco from 1995 through 1999 were included in this study. The first lesions in these patients were white keratotic plaques or papillary/verruciform lesions, initially exhibiting benign microscopic features. The various histologic diagnoses used in this series of patients are defined as follows: Psoriasiform hyperplasia-an epithelial pattern that shows elongated rete ridges with extreme thinning between ridges without evidence of keratinocyte atypia; verrucous hyperplasia- hyperkeratosis with a verrucous/papillary profile without epithelial atypia or expansion into submucosa; verrucous hyperplasia with dysplasiahyperkeratosis with a verrucous/papillary profile, but with atypical keratinocytes or an atypical rete ridge pattern; verrucous carcinoma-a robust papillaryverruciform proliferation showing definitive expansion into submucosa in the form of broad "pushing" rete ridges, and with no greater than slight keratinocyte atypia. A diagnosis of verrucous carcinoma was supported by an aggressive or recurrent clinical course.
Excluded were patients with multiple nongingival mucosal lesions diagnosed as proliferative verrucous leukoplakia, patients with multiple oral warts, patients whose initial lesions were microscopically dysplastic (moderate to severe) or malignant, and patients who are known to be human immunodeficiency virusinfected.
Polymerase chain reaction for HPV DNA Because the papillary-verruca! appearance of these
lesions suggested the possibility of an association with HPV, representative patient specimens were assessed for the presence of HPV DNA by using PCR. Four normal mucosal specimens (2 tongue, buccal mucosa, gingiva) and 1 gingival wart were also included with the patient samples.
DNA preparations were prepared from oral biopsy specimens by methods described previously.6 Briefly, sections cut from paraffin-embedded blocks were placed in sterile microfuge tubes. Paraffin was dissolved from sections and samples were suspended in 50 ).lL Sample Transport Medium (Digene Diagnostics, Silver Springs, Md). Samples were digested overnight at 55°C with 0.4 mg/mL proteinase K (Life Technologies, Gaithersburg, Md). Proteinase K was inactivated the next morning by boiling.
PCR and hybridization HPV testing was performed by using PCR with L I
consensus primers as described previously.7
Amplification of p-globin DNA was performed as a positive control for the presence of amplifiable DNA in the specimens. Briefly, 5 ).lL of sample was added to tubes containing 10 mmol/L tris-hydrochloric acid, 50 mmol/L potassium chloride, 4 mmol/L magnesium
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY December 2000
chloride, 200 ).lmol/L of each deoxyribonucleotide triphosphate, 2.5 units of AmpliTaq (PE Biosystems Foster City, Calif), 0.5 ).lmol/L of HPV primers MY09 and MY II, and 0.2 ).lmoi/L p-globin primers GH20 and PC04. PCR was performed on a Biometra Uno II Thermocycler (Tampa, Fla) : conditions were 95°C/3 minutes hotstart, 40 cycles of 95°C/30 s, 55°C/30 s, and 72°C/1 m, and a terminal extension of 72°C/5 m. After amplification, 6 ).lL of amplicon was applied to a nylon membrane and probed with a biotin-labeled HPV-Ll consensus probe mixture consisting of full-length HPV-11, HPV-16, HPV-18, and HPV-51 Ll DNA. A separate membrane was hybridized with biotin-labeled oligo probes to the human P-globin gene.
HPV typing If a sample was positive for the presence of HPV, it
was typed by restriction enzyme digestion. 8
Specifically, the PCR amplicon was digested with BamHI, Ddel, Haeiii, HinFI, Pstl, Rsal, and Sau3AI and run on a 4% 3: I NuSeive:Agarose gel. The restriction patterns were compared with those of known HPV types.
were subjected to a standard immunohistochemical staining protocol. Briefly, slides were microwaved in 0.1 mol/L citrate buffer (pH 6.0) for I 0 minutes for antigen enhancement. They were then incubated for I hour with anti-p53 (clone D0-7, dilution 1:50, Novacastra, Burlingame, Calif) or anti-Ki-67 (clone MIB-1, dilution 1:100, Immunotech, Westbrook, Me). Incubation with reagents of the Ultratech HRP Universal Detection System (lmmunotech) followed. Antigen-antibody reactions were visualized with aminoethylcarbazole chromogen. Normal mouse serum was used as a negative control. Positive controls consisted of 8 mucosal specimens of normal-appearing epithelium surfacing mild focal fibrous hyperplasia. Scoring was done in a semiquantitatively method in which epithelium was assessed in 5 consecutive fields at 200x magnification. The following scale was used: Jess than I 0% positive-staining nuclei were considered negative or within the range of control tissues; 10% to 25% keratinocyte nuclei positive were considered 1 +; 25% to 50% nuclei positive were considered 2+; >50% nuclei positive were considered 3+. The score recorded for each slide was the mean for the 5 fields assessed.
RESULTS Lesions were seen in 6 men and 4 women with an
average age of 65 years and a range of 51 to 82 years (Table 1). Three patients had a regular cigarettesmoking history (information on duration and amount unavailable), 5 patients did not smoke, and data were
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 90, Number 6
B
/.
' .· · ... · I ,
-·
Fettig et a/ 725
~ ~~-· .. ,, · ... ~ : .,.
:· ~',~:.}i\' ·i' .... ~-
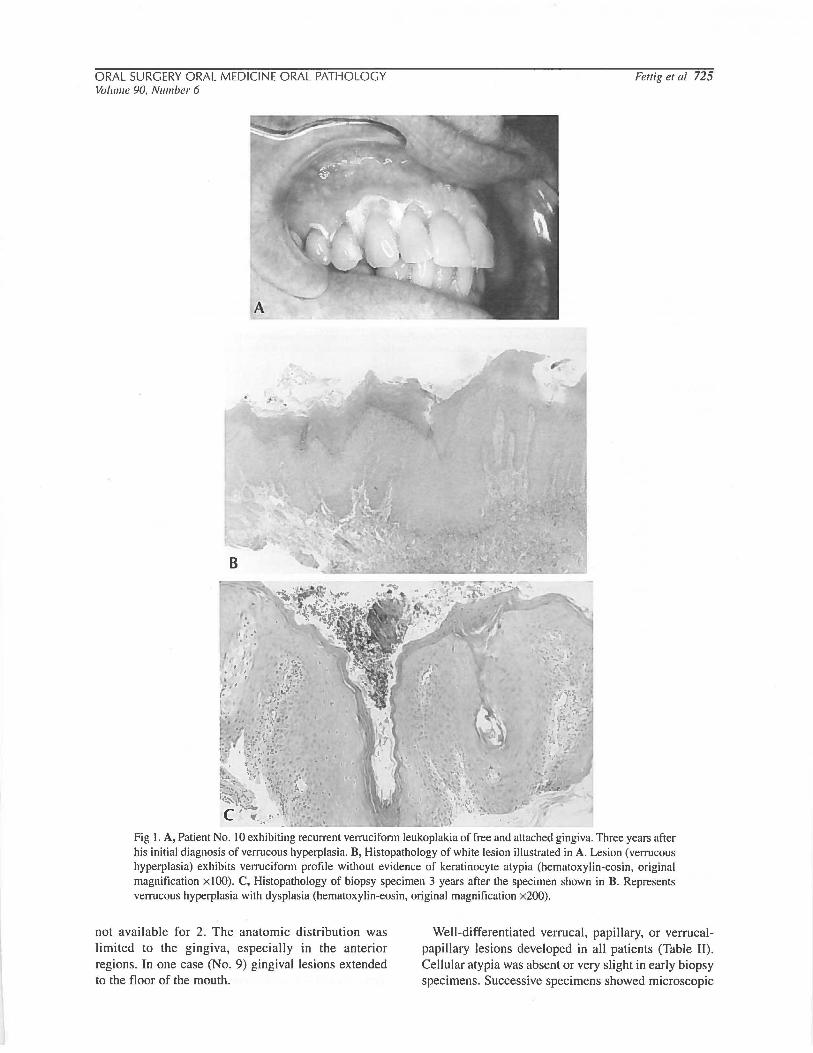
....,....;.~-------~-· ~-Fig I. A, Patient No. I 0 exhibiting recurrent verruciform leukoplakia of free and attached gingiva. Three years after his initial diagnosis of verrucous hyperplasia. B, Histopathology of white lesion illustrated in A. Lesion (verrucous hyperplasia) exhibits verruciform profile without evidence of keratinocyte atypia (hematoxylin-eosin, original magnification x!OO). C, Histopathology of biopsy specimen 3 years after the specimen shown in B. Represents verrucous hyperplasia with dysplasia (hematoxylin-eosin, original magnification x200).
not available for 2. The anatomic distribution was limited to the gingiva, especially in the anterior regions. In one case (No. 9) gingival lesions extended to the floor of the mouth.
Well-differentiated verruca), papillary, or verrucalpapillary lesions developed in all patients (Table II). Cellular atypia was absent or very slight in early biopsy specimens. Successive specimens showed microscopic
726 Fettig et a/ ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY December 2000
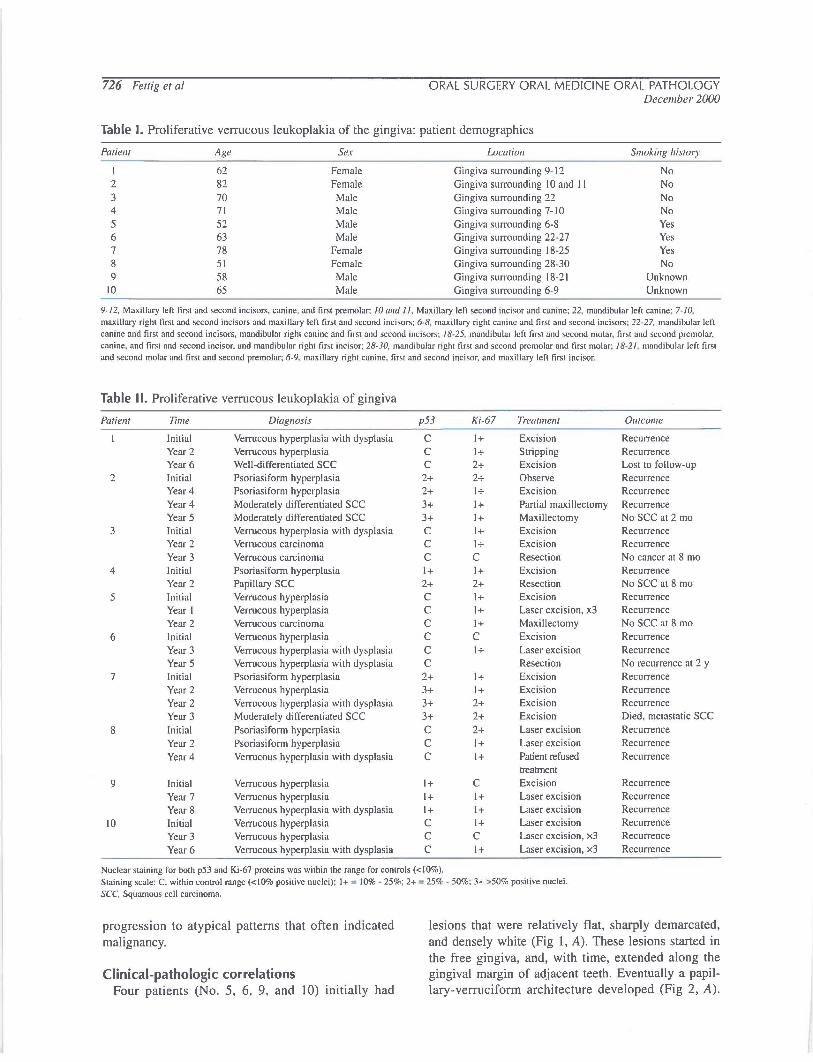
Table I. Proliferative verrucous leukoplakia of the gingiva: patient demographics
Patielll Age Sex Location Smoking histoJ)'
I 62 Female Gingiva surrounding 9- 12 No 2 82 Female Gingiva surrounding I 0 and II No 3 70 Male Gingiva surrounding 22 No 4 71 Male Gingiva surrounding 7-10 No 5 52 Male Gingiva surrounding 6-8 Yes 6 63 Male Gingiva surrounding 22-27 Yes 7 78 Female Gingiva surrounding 18-25 Yes 8 51 Female Gingiva surrounding 28-30 No 9 58 Male Gingiva surrounding 18-21 Unknown
10 65 Male Gingiva surrounding 6-9 Unknown
9-I2, Maxillary left first and second incisors, canine, and first premolar; IO and II, Maxillary left second inc1sor and canine; 22, mandibular left canine; 7-IO, maxillary right first and •econd incisors and maxillary left first and second incisors; 6-8, maxillary right canine and first and second incisors; 22·27, mandibular left canine and first and second incisors, mandibular right canine and first and •econd inc1so"; I8-25, mandibular left fi"t and 'econd molar, first and second premolar, canine, and first and second incisor, and mandibular nght fi"t inciSor; 28-30, mandibular nght fi"t and second premolar and first molar; I8-2I. mandibular left fi"t and •econd molar and first and second premolar; 6-9, maxillary right canine, first and second incisor, and maxillary left first incisor.
Table II. Proliferative verrucous leukoplakia of gingiva
Patielll Time Diagnosis p53 Ki-67 Treatment Outcome
Initial Verrucous hyperplasia with dysplasia c I+ Excision Recurrence
Year2 Verrucous hyperplasia c I+ Stripping Recurrence Year6 Well-differentiated SCC c 2+ Excision Lost to follow-up
2 Initial Psoriasiform hyperplasia 2+ 2+ Observe Recurrence Year4 Psoriasiform hyperplasia 2+ I+ Excision Recurrence Year4 Moderately differentiated SCC 3+ I+ Partial maxillectomy Recurrence Year 5 Moderately differentiated SCC 3+ I+ Maxillectomy No SCC at 2 mo
3 Initial Verrucous hyperplasia with dysplasia c I+ Excision Recurrence Year 2 Verrucous carcinoma c I+ Excision Recurrence
Year 3 Verrucous carcinoma c c Resection No cancer at 8 mo 4 Initial Psoriasiform hyperplasia I+ I+ Excision Recurrence
Year 2 Papillary sec 2+ 2+ Resection No SCC at 8 mo
5 Initial Verrucous hyperplasia c I+ Excision Recurrence
Year I Verrucous hyperplasia c I+ Laser excision, x3 Recurrence
Year 2 Verrucous carcinoma c I+ Maxillectomy No SCC at 8 mo
6 Initial Verrucous hyperplasia c c Excision Recurrence
Year 3 Verrucous hyperplasia with dysplasia c I+ Laser excision Recurrence
Year 5 Verrucous hyperplasia with dysplasia c Resection No recurrence at 2 y
8 Initial Psoriasiform hyperplasia c 2+ Laser excision Recurrence
Year 2 Psoriasiform hyperplasia c I+ Laser excision Recurrence
Year4 Verrucous hyperplasia with dysplasia c I+ Patient refused Recurrence treatment
9 Initial Verrucous hyperplasia I+ c Excision Recurrence
Year 7 Verrucous hyperplasia I+ I+ Laser excision Recurrence
Year 8 Verrucous hyperplasia with dysplasia I+ I+ Laser excision Recurrence
10 Initial Verrucous hyperplasia c I+ Laser excision Recurrence
Year 3 Verrucous hyperplasia c c Laser excision, x3 Recurrence
Year6 Verrucous hyperplasia with dysplasia c I+ Laser excision, x3 Recurrence
Nuclear staining for both p53 and Ki-67 proteins was within the range for controls ( < 10% ). Staining scale: C, within control range (<10% positive nuclei); I+ = 10% - 25%; 2+ = 25o/r - 50%; 3+ >50% positive nuclei. SCC, Squamous cell carcinoma.
progression to atypical patterns that often indicated malignancy.
Clinical-pathologic correlations Four patients (No. 5, 6, 9, and 10) initially had
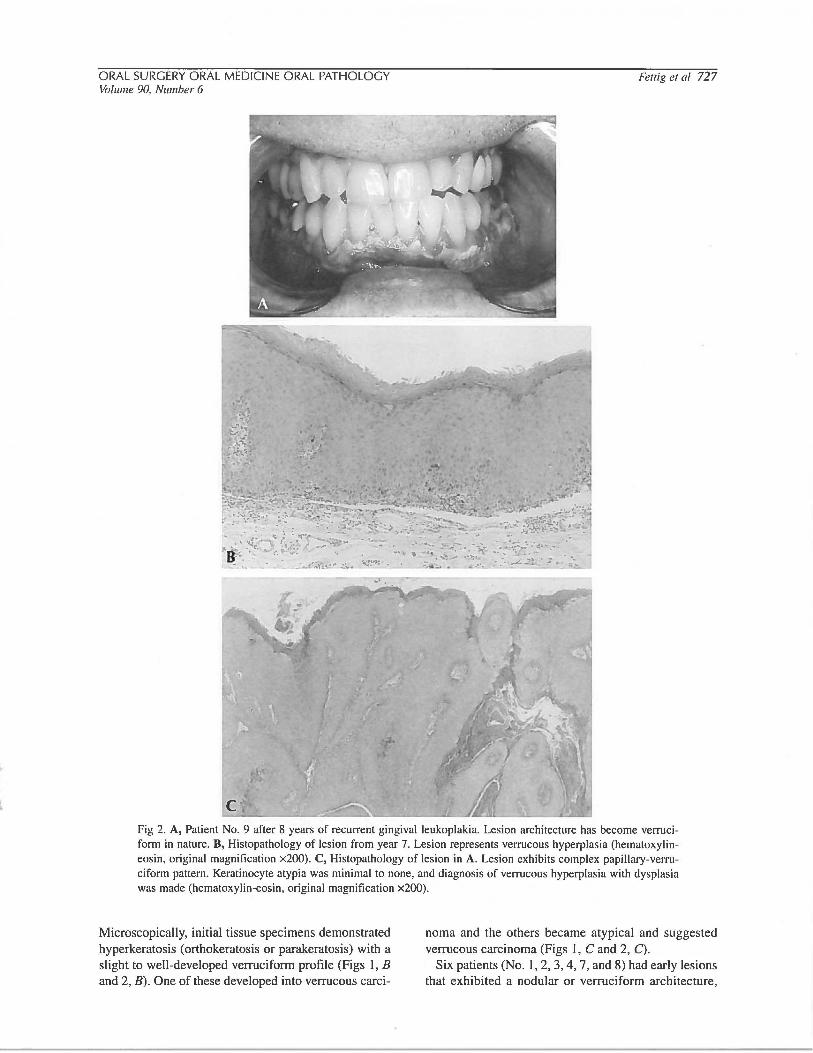
lesions that were relatively flat, sharply demarcated, and densely white (Fig I, A). These lesions started in the free gingiva, and, with time, extended along the gingival margin of adjacent teeth. Eventually a papillary-verruciform architecture developed (Fig 2, A).
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 90, Number 6
.~.i;,. :4;. o~··.
c
Fettig eta! 727
Fig 2. A, Patient No. 9 after 8 years of recurrent gingival leukoplakia. Lesion architecture has become verruciform in nature. B, Histopathology of lesion from year 7. Lesion represents verrucous hyperplasia (hematoxylineosin, original magnification x200). C, Histopathology of lesion in A. Lesion exhibits complex papillary-verruciform pattern. Keratinocyte atypia was minimal to none, and diagnosis of verrucous hyperplasia with dysplasia was made (hematoxylin-eosin, original magnification x200).
Microscopically, initial tissue specimens demonstrated hyperkeratosis (orthokeratosis or parakeratosis) with a slight to well-developed verruciform profile (Figs I, B and 2, B). One of these developed into verrucous carci-
noma and the others became atypical and suggested verrucous carcinoma (Figs I, C and 2, C).
Six patients (No. I, 2, 3, 4, 7, and 8) had early lesions that exhibited a nodular or verruciform architecture,
728 Fettig eta/ ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY December 2000
'f" -·--·-:·· . ... -.. ..... ~ .,~ ....... ..
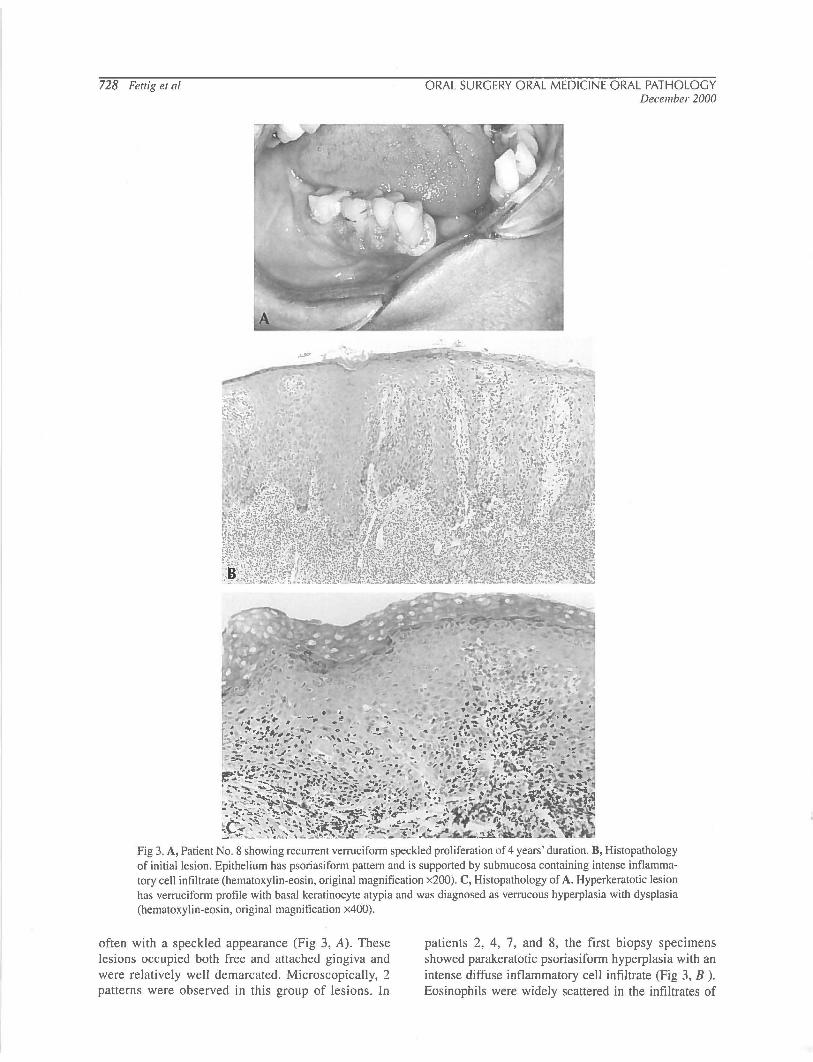
Fig 3. A, Patient No.8 showing recurrent verruciform speckled proliferation of 4 years' duration. B, Histopathology of initial lesion. Epithelium has psoriasiform pattern and is supported by submucosa containing intense inflammatory cell infiltrate (hematoxylin-eosin, original magnification x200). C, Histopathology of A. Hyperkeratotic lesion has verruciform profile with basal keratinocyte atypia and was diagnosed as verrucous hyperplasia with dysplasia (hematoxylin-eosin, original magnification x400).
often with a speckled appearance (Fig 3, A). These lesions occupied both free and attached gingiva and were relatively well demarcated. Microscopically, 2 patterns were observed in this group of lesions. In
patients 2, 4, 7, and 8, the first biopsy specimens showed parakeratotic psoriasiform hyperplasia with an intense diffuse inflammatory cell infiltrate (Fig 3, B ). Eosinophils were widely scattered in the infiltrates of
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 90, Number 6
all 4 cases. Occasionally, neutrophils were present in the epithelium. There was no evidence of foreign material (polarized light) or microorganisms in the early psoriasiform lesions. Either there was no nuclear atypia, or there was slight nuclear hyperchromasia and crowding of basal and parabasal keratinocytes. In these 4 patients, recurrences were keratotic with papillary or verruciform architecture (Fig 3, C); 3 were diagnosed as squamous cell carcinoma (moderately differentiated and papillary) and I as verrucous hyperplasia with dysplasia that suggested verrucous carcinoma. In 2 other patients (I and 3), the first biopsy specimens showed hyperkeratosis (ortho or para) with a combined papillary and verrucous architecture. Both cases developed into carcinoma (well differentiated and verrucous) in 6 and 2 years, respectively.
Successful PCR was performed with all biopsy specimens as determined by the presence of ~-globin PCR product. Only I sample (oral wart) contained HPV. It was typed by restriction fragment length polymorphism and was determined to be the low-risk type II. Normal mucosal specimens were negative for HPV.
Immunohistochemical stains for p53 protein showed positive nuclear staining of biopsy specimens from patients No. 2, 4, 7, and 9 (Table II). In these cases, specimens were positive in the first biopsies. Three of 4 cases, which showed psoriasiform hyperplasia initially, were positive. Stains for Ki-67 protein were generally moderately elevated in this series of I 0 PVLGs. Infrequently, the percentage of positive keratinocytes was not elevated above that associated with normal mucosa. Control specimens stained for p53 showed negative or weak staining of less than I 0% of basal keratinocyte nuclei. Control specimens stained for Ki-67 showed 5% to I 0% positive staining basal and parabasal keratinocyte nuclei.
Treatment Both simple excision and laser excision were inef
fective in eradicating premalignant lesions. Ultimately, local block resections were required to prevent recurrences. The block resections were done by removal of teeth adjacent to the process without extraction of teeth within the diseased field. By using reciprocal and oscillating saws, we removed the block of bone containing the teeth and gingiva. Immediate reconstruction was by direct apposition of the lingual to the buccal mucosa.
DISCUSSION Proliferative verrucous leukoplakia of the gingiva
can be described as a persistent or recurrent progressive condition occurring in tooth-bearing areas, especially in the anterior jaws. Initially, it presents as an asymptomatic benign-appearing solitary white patch
Fettig er a/ 729
that may have a flat, papillary, or verruca! architecture. It does not have the distribution (vestibule) or the microscopy (simple hyperkeratosis) of white lesions associated with the use of sanguinaria-containing oral hygiene products.9 It has no distinguishing features that can be used to separate it from other gingival idiopathic Ieukoplakias, making it incumbent on the clinician to perform a biopsy on the lesion and follow the patient indefinitely. PVLG is generally slow-growing, typically taking months to years to become histologically atypical. Progression to verrucous or squamous cell carcinoma appears to be a significant risk for affected patients.
The cause of PVLG is undetermined. Based on patient history, tobacco use (3 of I 0 patients) may be of minor importance. Also, based on the negative PCR results, a role for human papillomavirus in PVLG could not be demonstrated. Because both Ki-67 and p53 are overexpressed, the pathogenesis of PVLG appears to be related, at least in part, to a dysfunctional acceleration of the keratinocyte cell cycle. The 00-7 p53 antibody cannot distinguish between wildtype and mutant proteins, indicating that the positive staining may be caused by binding of wild-type p53 by protein of intrinsic origin (eg, MDM2) or viral origin (eg, HPV-E6), or mutation of the p53 gene.IO Molecular studies will be required to resolve this pathogenetic issue.
This is not a report of all patients with white gingival lesions, but an analysis of a selected collection of patients who had white lesion that followed an unexpected progressive course. Currently, there is no way to determine or predict which gingival white lesions will follow the clinical path described for this group of PVLGs.
Microscopically, unimpressive hyperkeratosis, psoriasiform hyperplasia, or verrucous hyperplasia characterize the initial disease phase, and carcinoma may be the ultimate outcome. The lesions are typically underdiagnosed, and the seriousness of the condition may not be suspected until the lesion becomes recurrent or begins to show atypical histologic features. The complex morphology of advanced lesions, which often makes tissue orientation very difficult, can contribute to diagnostic timidity. Microscopic interpretation is subjective and should be correlated with clinical behavior. When a bland microscopy is correlated with what appears to be an aggressive clinical behavior, PVLG should be entertained as a possible diagnosis.
Neither scalpel nor laser excision appears to be effective in ablating these lesions. This may be related, in part, to tumor extension through the embrasures of adjacent teeth and down the gingival sulcus or periodontal pocket. A localized block resection, although seemingly aggressive for a verrucous leukoplakia, has
730 Fettig et a/
been the only curative procedure. Block tissue removal includes the gingival sulcus and the periodontal ligament. Subsequent reconstruction can be with bone grafts, vestibular extensions, skin grafts, and osseointegrated implants.
PVLG shares many clinical and histologic features with proliferative verrucous leukoplakia in other sites. The progression and prognosis of PVLG appear to be consistent with previous reports of proliferative verrucous leukoplakia.1,5 However, the previously described oral proliferative verrucous leukoplakia affects multiple oral sites and, according to some reports, is strongly associated with oncogenic human papillomavirus, type 16.3 PVLG should be considered a subset of the better understood proliferative verrucous leukoplakia, at least until more is learned of this gingival phenomenon.
We thank Daniel Felmlee for his assistance in the PCR component of this study and Nusi P. Dekker for doing the immunohistochemical stains in this series.
REFERENCES I. Hansen LS, Olson JA, Silverman S. Proliferative verrucous
leukoplakia. Oral Surg Oral Med Oral Pathol 1985;60:285-98. 2. Zakrzewska JM, Lopes V, Speight P, Hopper C. Proliferative
verrucous leukoplakia: a report of ten cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:396-401.
3. Palefsky JM, Silverman S, Abdel-Salaam M, Daniels TE,
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY December 2000
Greenspan JS. Association between proliferative verrucous leukoplakia and infection with human papillomavirus type 16. J Oral Pathol Med 1995;24: 193-7.
4. Gopalakrishnan R, Weghorst CM, Lehman TA, Calvert RJ, Bijur G, Sabourin CL, et al. Mutated and wild-type p53 expression and HPV integration in proliferative verrucous leukoplakia and oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:471-7.
5. Silverman S, Gorsky M. Proliferative verrucous leukoplakia: a follow-up study of 54 cases. Oral Surg Oral Med Oral Pathol Oral Radio! Endod 1997;84:154-7.
6. Wright DK, Manos MM. Sample preparation from paraffinembedded tissues. In: Innis MA, Gelfand DH, Sninsky JJ, White TJ, editors. PCR protocols: a guide to methods and applications. Berkeley: Academic Press; 1990. p. 153-8.
7. Ting Y, Manos MM. Detection and typing of genital human papillomaviruses. In: Innis MA, Gelfand DH, Sninsky JJ, White TJ, editors. PCR protocols and applications. San Diego: Academic Press; 1990. p. 356-67.
8. Bernard H-U, Chan S-Y, Manos MM, Ong CK, Villa LL, Delius H, et al. Identification and assessment of known and novel human papillomaviruses by polymerase chain reaction amplification, restriction fragment length polymorphisms, nucleotide sequence, and phylogenetic algorithms. J Infect Dis 1994;170: 1077-85.
9. Damm DD, Curran A, White DK, Drummond JF. Leukoplakia of the maxillary vestibule- an association with Viadent? Oral Surg Oral Med Oral Pathol Oral Radio! Endod 1999;87:61-6.
10. Prives C, Hall PA. The p53 pathway. J Pathol199;187:112-26.
Reprint requests:
Joseph A Regezi, DDS, MS 513 Parnassus, S-512 University of California San Francisco, CA 94143-0424 [email protected]