84
Prolonged Labour – CPD, Fetal Malposition and Malpresentation Tanan G.
| Date post: | 21-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | arsenic-halcyon |
| View: | 1,241 times |
| Download: | 2 times |
Prolonged Labour – CPD, Fetal Malposition and Malpresentation
Tanan G.

Prolonged Labour
The onset of labor is defined as the period when the uterine contraction activity is regular and cervical dilatation is present.The progress of labor can be divided into three stages which are preceded by the latent phase.The labour is considered to be prolonged if it exceeds the combined duration of 18 hrs of the 1st and 2nd stage.

The Friedman Curve for normal labour

Latent Phase
Preparatory stage of uterus and cervix before the onset of labour.8 hrs in primi4 hrs in multiIf it exceeds 20 hrs in primi, 14 hrs in multi it is abnormal and is considered to be prolonged latent phase.Labour should be considered prolonged once it lags behind the normal partogram by 2-3 hrs.

Partogram
Managerial tool used to record all observations made on a woman and fetus in labour in one chart.
Partogram helps to identify at an early stage those women whose labour is slow.
A managerial tool for prevention of prolonged labour.

Partograph
ALERT LINE – represent the mean rate of slowest progress of labour
ACTION LINE – appropriate action should be taken

DYSTOCIA
Labor abnormalities that may interfere with the orderly progression to spontaneous delivery
Abnormalities:• Powers (abnormal contractility, maternal
expulsive effort)• Passenger (abnormal descent of the presenting
part of the fetus)• Passage (delayed cervical dilatation, CPD)

Cephalopelvic Disproportion (CPD)
Obstructed labor resulting from disparity between the fetal head size and maternal pelvis.
Absolute CPD (true mechanical obstruction)
Permanent (maternal):• Contracted pelvis• Pelvic exostoses• Spondylolisthesis• Anterior sacrococcygeal
tumorsTemporary (fetal):• Hydrocephalus• Large infant
Relative CPD
• Brow presentation• Face presentation –
mentoposterior• Occipitoposterior
positions• Deflexed head

Contracted Pelvis
It is a pelvis in which one or more of its diameters is reduced below the normal ranges by 1-2 cm, so that it interferes with the normal mechanism of labour.
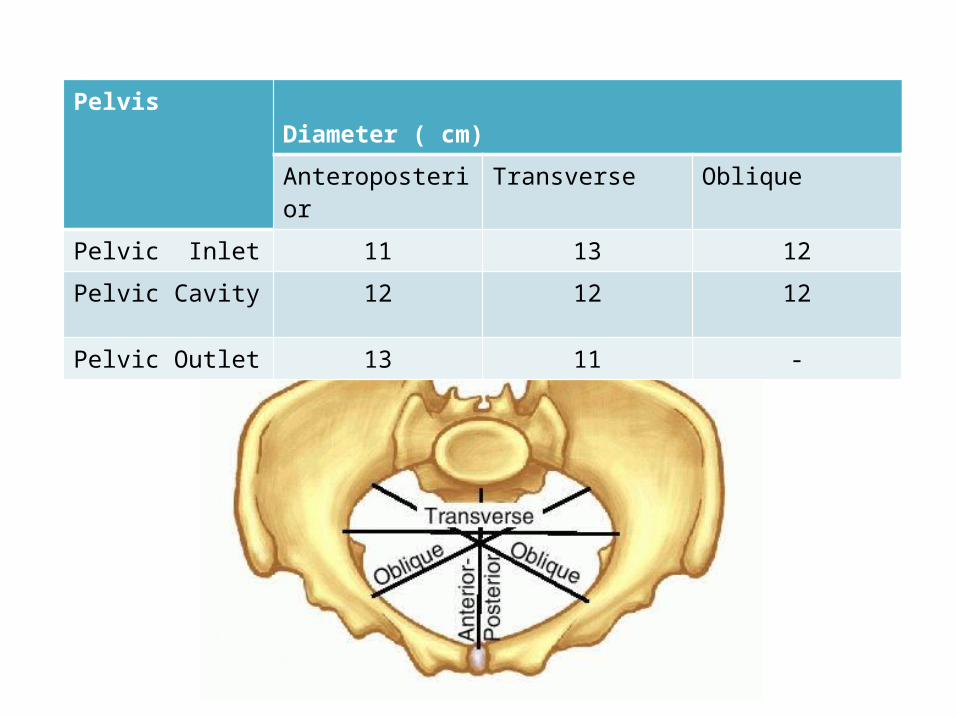
Pelvis Diameter ( cm)
Anteroposterior Transverse Oblique
Pelvic Inlet 11 13 12
Pelvic Cavity 12 12 12
Pelvic Outlet 13 11 -

Influencing Factors
• Developmental (hereditary, congenital disorders)
• Racial• Nutritional• Sexual (excessive production of androgen may
result in android pelvis)• Metabolic (rickets, osteomalacia)• Trauma, diseases or tumours
Developmental• Small gynaecoid pelvis• Small android pelvis• Small anthropoid pelvis• Small platypelloid pelvis• Naegele’s pelvis: absence of one sacral ala• Robert’s pelvis: absence of both sacral alae• High assimilation pelvis: The sacrum is composed of 6
vertebrae• Low assimilation pelvis: The sacrum is composed of 4 vertebrae• Split pelvis: splitted symphysis pubis

Classification by Pelvic Architecture
a. Pelvis aequabiliter justo minor• Characterized by general reduction of all
diameters; equally shortened usually by 1-2cm• Occurs in short women, also in women with
massive skeletal bones and developed muscles, the pelvis has masculine features such as narrow sacrum, narrow pubic outlet
b. Flat pelvis Reduced AP diameters with normal transverse and oblique diameters. Has 2 types:
Simple flat (or platypellic) pelvisEntire sacral platform is dislocated toward the symphysis hence all AP diameters of all pelvic planes are reduced
Flat rachiticOnly AP diameter of the pelvic inlet is reduced

c. Generally Contracted Pelvis• All diameters reduced, but the AP
diameters are shortened greater than the others
• Usually connected with the childhood history of rickets

Rare Forms• Otto’s pelvis – develop as result of inflammatory process in
the hip or knee•Beaked (rostrate) pelvis – under development of both
sacral wings•Spondylolisthetic pelvis – formed due to partial dislocation
of last lumbar vertebra in front of 1st sacral vertebra•Osteomalacic pelvis•Scoliotic pelvis – only the lumber region cause deformity of
the pelvis. The acetabulum is pushed inwards on the weight bearing side.





Classification by Degree of Contracture
I First degree: true conjugate <11cm but not <9cm, spontaneous delivery is possible
II Second degree: true conjugate equal to 9-7.5cm, spontaneous delivery possible but complications may arise
III Third degree: true conjugate 7.5-6cm spontaneous delivery impossible, use C-section
IV Fourth degree: true conjugate <6cm, impossible delivery, only way is C-section; also known as absolutely contracted pelvis

Diagnosis
History• Rickets (if there is a history of delayed walking and
dentition) • Trauma or diseases (previous tuberculosis of bones
and joints)• Infantilism• Bad obstetric history (prolonged labour ended by: difficult
forceps, caesarean section or still birth, evidence of maternal injuries: complete perineal tear, vesicovaginal fistula, rectovaginal fistula)

Examination
General examination:• Gait (suggestive of abnormalities in the pelvis,
spine or lower limbs)• Stature (women with less than 140-150 cm
height usually have contracted pelvis)• Spine and lower limbs (may have a disease or
lesion)

• Rickets manifestations (square shaped head, rosary beads in the costal ridges, pigeon chest, Harrison’s sulcus, bow legs)
• Dystocia dystrophia syndrome (the person is short, stocky, subfertile, has android pelvis and masculine hair distribution, with history of delayed menarche. Possibly may be more exposed to occipito-posterior position and dystocia)
• Solovjov’ index (estimated by the circumference of radiocarpal joint, if it exceeds 14-16 cm it indicates the thickness of the pelvic bones)

2 shapes of abdomen • Acuminate (pointed) abdomen in primigravida
with a resilient abdominal wall• Pendulous abdomen in multiparous women

Abdominal Examination
• Pendulous abdomen in primigravida • Positive Vasten’ sign (if disproportion between
fetal head and symphisis pubis is prominent - Vasten’ sign is positive, if disproportion between fetal head and symphisis pubis is absent - Vasten’ sign is negative)
• Non engagement in last 3-4 wks in primigravida

Degrees of Contracted Pelvis
1. Minor degree: The true conjugate is 9-10 cm. It corresponds to minor disproportion.
2.Moderate degree: The true conjugate is 8-9 cm. It corresponds to moderate disproportion.
3.Severe degree: The true conjugate is 6-8 cm. It corresponds to marked disproportion.
4.Extreme degree: The true conjugate is less than 6 cm. Vaginal delivery is impossible even after craniotomy as the bimastoid diameter (7.5 cm) is not crushed.

PelvimetryAssessment of the pelvic diameters and capacity done at 38-39weeks.• Clinical pelvimetry:
▫ Internal pelvimetry for: inlet, cavity, and outlet.
▫ External pelvimetry for: inlet and outlet
• Imaging pelvimetry:▫ X-ray▫ CT▫ MRI

Cephalometry
Ultrasonography is safe, accurate and easy. Can detect:
The biparietal diameter (BPD) The occipito-frontal diameter.The circumference of the head.

Mechanism of Labour in Contracted Pelvis
The process passes flat rachitic pelvis till the mid cavity, where internal rotation and further descent cannot occur due to persistence of flattening of the pelvis and contracted outlet. So, deep transverse arrest is common and vaginal delivery is obstructed.

Management
It depends mainly on the degree of disproportion.
• Minor disproportion: vaginal delivery• Moderate disproportion: trial labour, if failed
C-section• Marked disproportion: C-section

Indications of Caesarean Section
• Elective cesarean section:• Major degree of contraction• Major disproportion• Absolute contraction• Dead fetus• Patient not fit for trial labor
• During last week of pregnancy.• When trial labour has failed

Trial Labour
Conduction of spontaneous labour in a moderate degree of disproportion, in an institution under supervision with watchful expectancy for a vaginal delivery.

Suitable cases
• Young primigravida in good health• Moderate disproportion• Vertex presentation• No outlet contractions• Average sized baby
Termination
• Vaginal delivery (spontaneously or by forceps if the head was engaged)
• Caesarean section (failed trial of labour i.e. the head did not engage)
• Complications (foetal distress or prolapsed pulsating cord)

• Careful fetal and maternal monitoring by electronic fetal monitoring and non stress test
• Oral feeding remain suspended and hydration is maintained by intravenous drip
• Adequate analgesic is administered
• Augmentation of labor by pitocin
Successful trial - a healthy baby was born vaginally, spontaneously or by forcep, with the mother in good condition
Failure - delivery by cesarean section or delivery of a dead baby spontaneously or by craniotomy

• The progress of labor is mapped with partograph
• After the membrane rupture, pelvic examination is to be done:– to exclude cord prolapse– to note the color of liquor– to assess the pelvis once or more– to note the condition of the cervix

Complications
MaternalDuring pregnancy:• Incarcerated retroverted gravid uterus • Malpresentations• Pendulous abdomen • Nonengagement• Pyelonephritis (due to the compression of the
ureter)

During Labour:• Inertia, slow cervical dilatation and prolonged
labour• Premature rupture of membranes and cord
prolapse• Obstructed labour and ruptured uterus• Necrotic genito-urinary fistula• Injury to pelvic joints or nerves from difficult
forceps delivery• Postpartum haemorrhage

Foetal• Intracranial haemorrhage • Asphyxia • Fractured skull• Nerve injuries • Intra-amniotic infection
Malpositions and Malpresentations
Malpositions are abnormal positions of the vertex of the fetal head (with the occiput as the reference point) relative to the maternal pelvis. Malpresentations are all presentations of the fetus other than vertex.
Occipitoposterior positions
• Most common type• The vertex is presenting, but the occiput lies in
the posterior rather than the anterior part of the pelvis.
• As a consequence, the fetal head is deflexed and larger diameters of the fetal skull present.

There are three positions:• Right occipito-posterior position ROP (the
occiput directed to the right sacro-iliac joint)
• Left occipito-posterior position LOP ( the occiput directed to the left sacro-iliac joint)
• Direct occipitoposterior
Causes
• Anteriorly situated placenta
• Anthropoid pelvis
• Flat Sacrum
• Pundulous abdomen
• Chance
• R.O.P. three times as common as L.O.P.

Diagnosis
• Listen to the mother’s complaints (backaches, she may feel that her baby’s bottom is very high up against her ribs, feeling movements across both sides of her abdomen and etc.)
• Inspection (saucer-shaped depression at or just below the umbilicus, outline of the high, unengaged head can look like a full bladder)
• Palpation (the back is difficult to palpate as it is well out to the maternal side, limbs can be felt on both sides of the midline)
• Auscultation (the fetal back is not well flexed so the chest is thrust forward, therefore the fetal heart can be heard in the midline, the heart may be heard more easily at the flank on the same side as the back)

Management
• 12% will deliver spontaneously O.P.
• Transverse arrest may require operative intervention
• Lack of progress may warrant c-section
• Vacuum may be preferable to Forceps

FACE PRESENTATION
• Cephalic presentation where the attitude is one of complete extension, presenting part is face and denominator is the chin or mentum
• Engaging diameter is submentobregmatic-9.4cm• Primary face presentation are present before
onset of labour and are rare• Secondary caused by extension during labour
and is most common

Positions
• Left mentoanterior(LMA)• Right mentoanterior(RMA)• Right mentoposterior(RMP)• Left mentoposterior(LMP)
70% are mentoanterior and 30% posterior.

Causes
Maternal
• contracted pelvis• obliquity of uterus• multiparity or
pendulous abdomen
Fetal• anencephaly and
iniencephaly• cord around the neck• tumours of neck, like
congenital goiter• spasm of
sternocleidomatoid muscle

Diagnosis
• In mentoanterior, back is felt with difficulty as it is posterior and limbs anteriorly
• Head remains high• Cephalic prominence is the occiput and on the
same side as the back• Groove b/w the head and back is prominent• Fetal heart sounds are transmitted through the
chest and heard well anteriorly in mentoanterior
Management
• Mentoanterior, forward rotation in mentoposterior- labour allowed
• CPD, anencephaly, other anomalies, persistent mentoposterior, obstructed labour- C-section
• Dead baby- C-section or craniotomy

Brow Presentation
• Most unfavourable• Attitude is one of partial extension, presenting
part being the area between the ant. Fontanelle above and glabella and orbital ridges below and denominator is forehead or frontum
• Presenting diameter is verticomental- 13.5cm• Transitory presentation- flex or extend
Diagnosis
• High mobile head, which feels large from side to side
• Cephalic prominence is the occiput and is on same side as back and groove between cephalic prominence and back is less prominent than in face presentation

Management
• If membrane not ruptured wait for correction• After membrane ruptures, brow presentation
diagnosed and in persistent brow presentation –C-section
• Prologed labour with head high.. Brow presentation must be suspected
Shoulder Presentation
• Long axes of fetal and maternal ovoid are approximately at right angles to each other and shoulder is presenting in the pelvic inlet.
• Denominator- acromion
POSITIONS• Right acromial• Left acromial
Depending on the direstion of the back:• Dorsoanterior• Dorsoposterior• Dorsosuperior• Dorsoinferior

Causes
• Incidence- 1 in 500Maternal Factors• Multiparity• Contracted pelvis• Uterine anomalies like septate,bicornuate and
arcuate uterus• Placenta praevia• Fibroid in the lower segment

Fetal Factors
• Prematurity• Multiple pregnancy• Polyhydraminos• IUD
Diagnosis
• Transversely stretched• Fundal height less than period of gestation• No Fetal pole at fundus• Ballotable head in one flank & breech in the other• In dorsoanterior, back is felt a uniform reistance
acros the front of abdomen• In dorsoposterior, limbs are felt anteriorly• Empty pelvic grip

Vaginal Examination
• Hand/shoulder/elbow may be felt as a uniform resistance across the front of abdomen
• Shoulder can be identified by ribs running parallel to each other
• Late in labour, shoulder may be wedged in the pelvis and hand freequently prolapse into the vagina

Complications
Maternal• Increased chance of C-section• Obstructed labour or ruptured uterus
Fetal • Birth asphyxia due to cord prolapse and in
obstructed labour

Management
• External Cephalic Version• C-section best option• When ECV fails and CI• Transverse incision• If the fetus is dead – C-section or craniotomy
Breech Presentation
It is a polar alignment of the fetus in which the fetal buttocks present at the maternal pelvic inlet.
• 3 types: – Frank– Incomplete – Complete

Causes
• Polyhydramnios• Oligohydramnios• Uterine abnormalies
(bicornuate, uterus)• Pelvic tumour• Uterine surgery
• Prematurity• Multiple pregnancy• Fetal anomalies
(hydrocephalus, anencephaly

Frank/Extended
The fetal hips are flexed and the knees extended so that the thighs are apposed to the abdomen and the lower legs to the chest The buttocks are the most dependent part of the fetus.

Incomplete/FootlingIn incomplete breech presentation, the fetus has one or both hips incompletely flexed so that some part of the fetal lower extremity, rather than the buttocks, is the most dependent part (hence the terms single footling or double footling).

Complete/Flexed
The fetal hips and knees are both flexed so that the thighs are opposed to the abdomen and the legs lie on thighs.
Diagnosis
• A transverse groove may be seen above the umbilicus in sacro-anterior position. Corresponds to the neck.
• If the patient is thin, the head may be seen as a localised bulge in one hypochondrium.
Diagnosis
• Fundal grip. The head is felt as a smooth, hard, round ballottable mass which is often tender.
• Umbilical grip. The back is identified and a depression corresponds to the neck may be felt.
• First pelvic grip. The breech is felt as a smooth, soft mass continuous with the back. Trial to do ballottement to the breech shows that the movement is transmitted to the whole trunk.

Diagnosis
Fetal Heart Sound may be heard above the level of the umbilicus.

Diagnosis
Ultrasonography:• Diagnosis• Type of breech• Gestational age and foetal weight• Congenital anomalies

Management
• Vaginal breech delivery• External Cephalic Version (ECV)• Caesarian Section

ECV
• External cephalic version (ECV) is a third alternative to vaginal delivery or cesarean delivery for the breech fetus
• Success rate 60-75%• The mechanical goal is to squeeze the fetal
vertex gently out of the fundal area to the transverse and finally into the lower segment of the uterus.

ECV

Risks
• Placental abruption• Premature rupture of the membranes• Cord accident• Transplacental haemorrhage(remember anti-D
aministration in Rhesus-negative women)• Fetal bradycardia

Vaginal DeliveryThree types:• A spontaneous breech delivery is one in which the
entire infant delivers vaginally without manual aid. • The assisted breech delivery( partial breech
extraction.) In this delivery, the fetus is allowed to deliver by the forces of uterine contractions and maternal bearing-down efforts until the fetal umbilicus has passed over the mother's perineum. After this, delivery of the legs, trunk, and arms are assisted manually; the head may be delivered manually or with forceps.

• A complete breech extraction, in which manual assistance is applied by traction in the groins or on the lower extremities before delivery of the buttocks.

Pinard’s manoeuvre
• In breech with extended legs • once the groin is visible gentle pressure can be
applied to abduct the thigh and reach the knee.
• The knee can be flexed with pressure in the popliteal fossa and the leg delivered.
• Anterior leg is always delivered first.

Loveset’s manoeuvre
• This procedure automatically corrects any upward displacement of arms.
• In Lovset’s maneuver baby’s trunk is made to rotate with downward traction holding the baby at the iliac crest so that posterior shoulder comes below symphysis pubis and the arm is delivered by flexing the shoulder followed by hooking at the elbow and flexing it followed by bringing down the forearm ‘like a hand shake’.
• The same procedure is repeated by reverse rotation of 180 degree so that anterior shoulder comes below the symphysis pubis.

Mariceau-Smellie-Veit manoeuvre
• Here the baby is allowed to rest on the left supinated forearm of the obstetritian, with the limbs hanging on either side.
• Left index and middle finger is placed on the malar bones, while the right index and ring fingers are placed on the respective shoulders and the middle finger on the sub-occipital region.
• To achieve flexion, traction is now given in downward and backward direction and simultaneous suprapubic pressure is maintained by the assitant until the nape of the neck is visible.
• Thereafter, the baby is pulled in upward and forward direction so that the face is born and by depressing the trunk the head is born.

















