Prostate Total Tumor Extent Versus Index Tumor Extent—Which
is Predictive of Biochemical Recurrence Following
Radical Prostatectomy?
Athanase Billis,* Luciana R. Meirelles, Leandro L. L. Freitas, Aline S. Polidoro,Hamilton A. Fernandes, Mariana M. Padilha, Luis A. Magna and Ubirajara Ferreira
From the Departments of Pathology (AB, LRM, LLLF, ASP, HAF, MMP), Medical Genetics/Biostatistics (LAM) and Urology (UF), School ofMedicine, University of Campinas, São Paulo, Brazil
Purpose: It is controversial whether tumor extent in radical prostatectomiespredicts biochemical recurrence following surgery. We compared the predictivevalue of total tumor extent vs dominant nodule (index tumor) extent.Materials and Methods: A mean of 32 paraffin blocks was processed from pros-tate surgical specimens step sectioned at 3 to 5 mm intervals from 300 patientstreated with radical retropubic prostatectomy. Each transverse section was sub-divided into 2 anterolateral and 2 posterolateral quadrants. Tumor extent wasevaluated by a semiquantitative point count method. Dominant nodule extent wasrecorded as the maximal number of positive points of the largest single focus ofcancer in the quadrants. Time to biochemical recurrence was analyzed by Kaplan-Meier product limit analysis. Prediction of shorter time to biochemical recurrencewas determined by univariate and multivariate Cox proportional hazards models.Results: Except for age and race, total and index tumor extent was significantlyassociated with higher preoperative prostate specific antigen, clinical stage T2,pathological stage greater than T2, positive surgical margins and higher radicalprostatectomy Gleason score. Total and index tumor extent was significantlyassociated with time to biochemical recurrence in Kaplan-Meier estimates. Totaland index tumor extent significantly predicted shorter time to biochemical recur-rence on univariate analysis but only index tumor extent was an independentpredictor of time to biochemical recurrence on multivariate analysis.Conclusions: The study indicates that any tumor extent estimate in surgicalspecimens should be related to the dominant nodule (index tumor) and not tototal tumor extent.
Accepted for publication July 3, 2012.Study received institutional committee of eth-
ics approval.Supplementary material for this article can be
obtained at http://jurology.com.* Correspondence: Department of Pathology,
School of Medicine, University of Campinas (Uni-camp), Rua Tessália Vieira de Camargo, 126, CEP13083-887 Campinas, São Paulo, Brazil (FAX:�55 19 3289-38-97; e-mail: [email protected]).
For another article on a related
topic see page 329.
antigen; pathology, surgical
THERE is no controversy that prostatetumor extent on needle biopsy shouldbe reported.1–4 The only controversyis related to which method of tumorquantification should be adopted.3,5–7
However, it is controversial whethertumor extent on RP specimens is anindependent prognostic factor of BCR
Because prostate cancer grows irreg-ularly, volume measurement is techni-cally much more difficult than in otherorgans. The most accurate method is touse computer assisted image analysissystems, which is not feasible for rou-tine clinical practice. Other alternative,simpler methods have been proposed,
including the diameter of the largest
http://dx.doi.org/10.1016/j.juro.2012.08.179Vol. 189, 99-104, January 2013
PROSTATE TOTAL TUMOR EXTENT VERSUS INDEX TUMOR EXTENT100
tumor focus, the number of tumor foci, the numberor percent of involved blocks, a grid with 3.0 mmsquares, the semiquantitative point count methodand even eye examination of the glass slides.9–16
Several groups reported that tumor extent on RP isan independent predictor of disease recurrence.14–16
However, others were unfavorable, arguing that tu-mor extent does not provide additional informationbeyond that of Gleason score and surgical margin sta-tus.17–19 Alternatively, in other studies the extent ofthe dominant nodule (index tumor) was an indepen-dent risk factor for PSA recurrence after RP.13,20,21
We compared total tumor extent vs dominantnodule (index tumor) extent as independent predic-tors of BCR following RP.
MATERIALS AND METHODS
This retrospective study was based on 300 consecutivepatients with clinical stage T1c (144) and T2 (156) treatedwith retropubic RP by 1 surgeon (UF). Several clinicopath-ological variables were studied.
After RP serum PSA was measured every 3 monthsduring year 1, every 6 months during year 2 and annuallythereafter. No patient in this series received radiotherapyor androgen manipulation before or after surgery. Totalserum PSA was measured using the previously validatedImmulite® PSA kit. Postoperative BCR was consideredPSA 0.2 ng/ml or greater according to the American Uro-logical Association recommendation.22 Patients withoutevidence of BCR were censored at last followup. The studywas approved by our institutional committee of ethics.
Surgical specimens were step sectioned at 3 to 5 mmintervals and embedded in paraffin. A mean of 32 paraffinblocks was processed. Sections (6 �m) of each block werestained with hematoxylin and eosin. Each transverse sectionof the prostate was subdivided into 2 anterolateral and 2posterolateral quadrants. Using the cone method 8 sectionsfrom the bladder neck and 8 from the apex were obtained.
PSM was defined as cancer cells in contact with theinked specimen surface. Extraprostatic extension was di-agnosed when cancer was seen in adipose tissue, and incase of a desmoplastic response when a protuberance cor-responding to tumor extension into periprostatic tissuewas seen. Seminal vesicle invasion occurred when therewas involvement of the muscular coat.
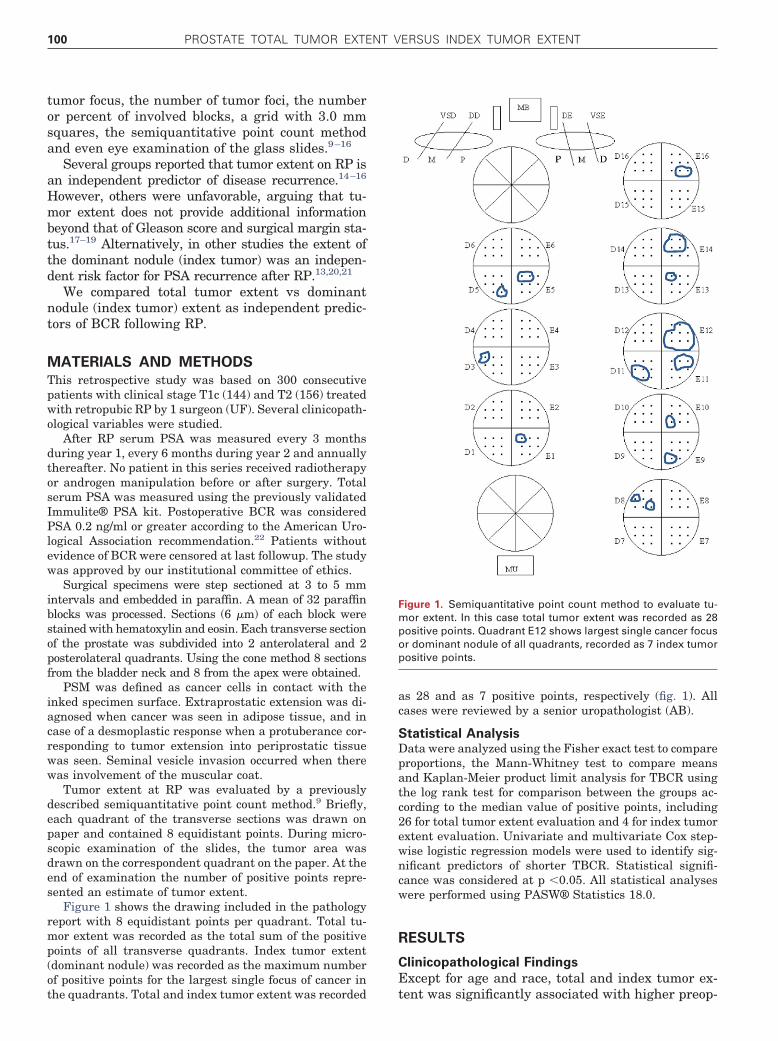
Tumor extent at RP was evaluated by a previouslydescribed semiquantitative point count method.9 Briefly,each quadrant of the transverse sections was drawn onpaper and contained 8 equidistant points. During micro-scopic examination of the slides, the tumor area wasdrawn on the correspondent quadrant on the paper. At theend of examination the number of positive points repre-sented an estimate of tumor extent.
Figure 1 shows the drawing included in the pathologyreport with 8 equidistant points per quadrant. Total tu-mor extent was recorded as the total sum of the positivepoints of all transverse quadrants. Index tumor extent(dominant nodule) was recorded as the maximum numberof positive points for the largest single focus of cancer in
the quadrants. Total and index tumor extent was recorded
as 28 and as 7 positive points, respectively (fig. 1). Allcases were reviewed by a senior uropathologist (AB).
Statistical AnalysisData were analyzed using the Fisher exact test to compareproportions, the Mann-Whitney test to compare meansand Kaplan-Meier product limit analysis for TBCR usingthe log rank test for comparison between the groups ac-cording to the median value of positive points, including26 for total tumor extent evaluation and 4 for index tumorextent evaluation. Univariate and multivariate Cox step-wise logistic regression models were used to identify sig-nificant predictors of shorter TBCR. Statistical signifi-cance was considered at p �0.05. All statistical analyseswere performed using PASW® Statistics 18.0.
RESULTS
Clinicopathological Findings
Except for age and race, total and index tumor ex-
Figure 1. Semiquantitative point count method to evaluate tu-mor extent. In this case total tumor extent was recorded as 28positive points. Quadrant E12 shows largest single cancer focusor dominant nodule of all quadrants, recorded as 7 index tumorpositive points.
tent was significantly associated with higher preop-
(4–9)
PROSTATE TOTAL TUMOR EXTENT VERSUS INDEX TUMOR EXTENT 101
erative PSA, clinical stage T2, pathological stagegreater than T2, PSM and higher RP Gleason score(supplementary table, jurology.com and table 1).
Time to BCR
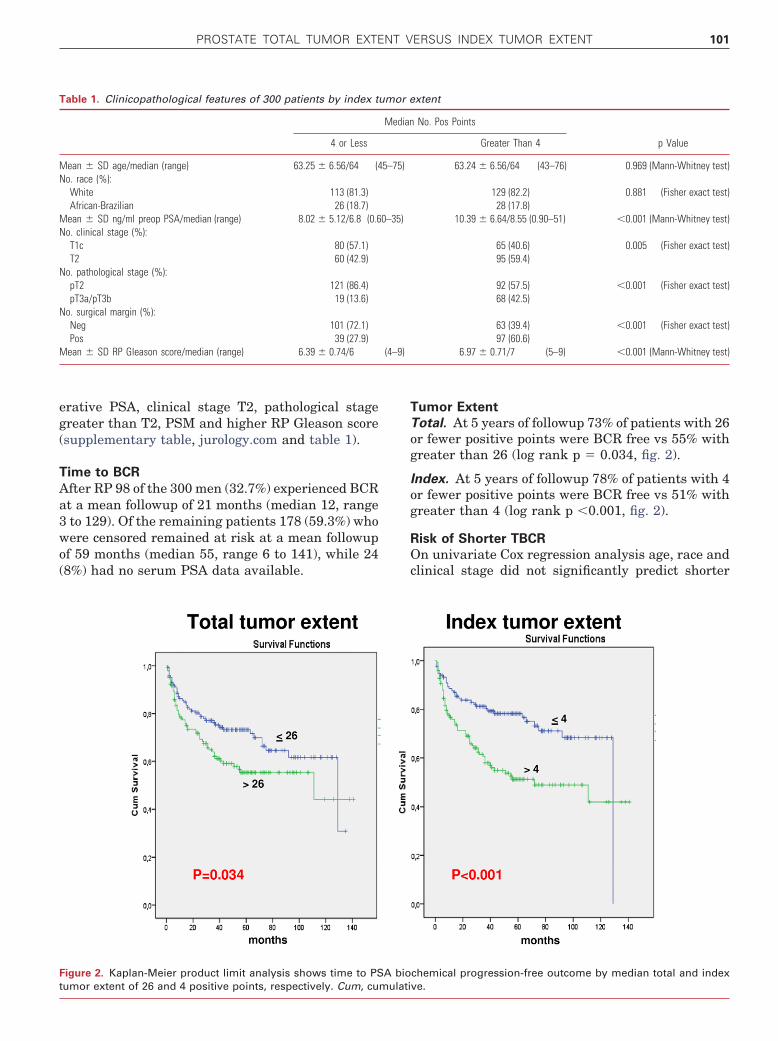
After RP 98 of the 300 men (32.7%) experienced BCRat a mean followup of 21 months (median 12, range3 to 129). Of the remaining patients 178 (59.3%) whowere censored remained at risk at a mean followupof 59 months (median 55, range 6 to 141), while 24(8%) had no serum PSA data available.
Table 1. Clinicopathological features of 300 patients by index t
PROSTATE TOTAL TUMOR EXTENT VERSUS INDEX TUMOR EXTENT102
TBCR (table 2). Pathological stage greater than T2,preoperative PSA, Gleason score on RP, PSM andtotal tumor extent as well as index tumor extentwere significantly predictive of shorter TBCR.
Two multivariate analysis models were used(table 2). In model 1 we included total tumor extent,pathological stage greater than T2, preoperativePSA, Gleason score on RP and PSM. In model 2 weincluded index tumor extent, pathological stagegreater than T2, preoperative PSA, Gleason score onRP and PSM. In all models we used the backwardstepwise logistic regression method. Only index tu-mor extent was an independent predictor of shorterTBCR.
DISCUSSION
Several studies favor tumor extent as a prognosticindicator. Humphrey and Vollmer determined tu-mor extent in 117 prostatectomy specimens by a gridmethod.14 They recommended reporting histologicalgrade and tumor extent in the prostate gland sinceeach appears to be important for identifying pa-tients at risk for a poor outcome after prostatectomyfor prostatic carcinoma.
Stamey et al studied RP specimens from 379 mentreated from 1983 to 1992 with surgical excisiononly.15 Percent Gleason grade 4/5, cancer volume,positive lymph nodes and intraprostatic vascularinvasion were independently associated with pros-
Table 2. Cox univariate and multivariate proportional hazard anto biochemical recurrence after radical prostatectomy
tate cancer progression, as indicated by serum PSA0.07 ng/ml. Using a visual estimate of the percent ofcarcinoma in prostatic tissue from RP specimens,Carvalhal et al found that the percent of carcinoma,preoperative PSA, Gleason grade and pathologicalstage were significant predictors of disease recur-rence.16
However, other studies do not indicate that tumorextent is an independent prognostic indicator. Ep-stein et al analyzed 185 men who underwent retro-pubic RP for clinical stage T2 adenocarcinoma of theprostate.17 Although extraprostatic extension, tu-mor volume and percent of prostate involved by tu-mor each predicted progression, on stepwise regres-sion analysis they did not provide independentprognostic information. On multivariate analysisGleason score was the best predictor of progression.Surgical margin was the only variable that en-hanced prediction, although it was less influentialthan grade. They concluded that although an accu-rate preoperative assessment of tumor volume re-mains desirable for managing prostate cancer, tu-mor volume measurement in RP specimens does notprovide additional information beyond that of Glea-son score and surgical margin status.
Salomon et al analyzed 200 consecutive RP spec-imens.18 On univariate analysis tumor progressioncorrelated with final Gleason score, PSM, tumor vol-ume and stage. On multivariate analysis tumor pro-
of several clinicopathological factors predicting shorter time
PROSTATE TOTAL TUMOR EXTENT VERSUS INDEX TUMOR EXTENT 103
gression correlated only with final Gleason score andstage. They concluded that Gleason score and path-ological stage are independent factors for predictingprostate cancer progression after RP. When theseparameters are known, tumor volume does not pro-vide additional information. Wolters et al analyzed344 participants in the ERSPC (European Random-ized Study of Screening for Prostate Cancer).19 Afterassessing tumor volume in an accurate manner bycomputer assisted morphometric analysis, they con-cluded that it does not add prognostic value to rou-tine pathological parameters and there seems to belittle reason to routinely include tumor volume inRP specimens in the pathology report.
These groups evaluated the prognostic value oftotal tumor extent. Alternatively, in other studiestumor extent was an independent risk factor forPSA recurrence following RP when the dominanttumor (index tumor) was evaluated. Renshaw et aldetermined whether maximum tumor diameter wasan independent predictor of PSA failure in a seriesof 434 men who underwent RP.13 Maximum tumordiameter was an independent risk factor for PSAfailure along with preoperative serum PSA andGleason score 8 or greater. They concluded thatprostate carcinoma maximum diameter is a simple,inexpensive, independent predictor of PSA failure.
Eichelberger et al studied specimens evaluated bywhole mount processing from 364 patients who un-derwent RP.20 The greatest diameter of the largestsingle focus of tumor was determined by a rulermarked in mm. Cox multiple regression was per-formed to test the prognostic value of maximumtumor diameter, adjusting for pathological stage,Gleason score and surgical margin status. Maxi-mum tumor diameter was associated with preoper-ative PSA, prostate weight, tumor volume, Gleasonscore and pathological stage. On multivariate anal-ysis increased maximum tumor diameter was anindependent predictor of shorter time to PSA recur-rence in a model including Gleason score and surgi-cal margin status. They concluded that maximumtumor diameter is a significant predictor of BCR inpatients with prostate cancer.
Dvorak et al studied 781 men with clinical stageT1c-T2 prostate cancer who underwent RP.21 Maxi-mum tumor diameter was recorded as the maximaldimension of the largest single focus of cancer in all3 mm step sections. Cox regression analysis wasused to determine predictors of time to postoperativePSA failure and Kaplan-Meier estimates of PSA fail-ure-free survival dichotomized by median maximumtumor diameter. On multivariate analysis not in-cluding surgical margin status increased maximumtumor diameter was an independent predictor ofshorter time to PSA recurrence (p � 0.004). How-
ever, when margin status was added to the model,
maximum tumor diameter approached but did notattain statistical significance (p � 0.07).
We evaluated total tumor and dominant nodule(index tumor) extent as predictors of BCR after RP.Except for age and race, each tumor extent evalua-tion was significantly associated with preoperativePSA, clinical stage T2, pathological stage greaterthan T2, PSM and RP Gleason score (supplementarytable, jurology.com and table 1). Total and indextumor extent were significantly associated withTBCR (p � 0.034 and �0.001, respectively). On Coxunivariate analysis, except for age, race and clinicalstage, shorter TBCR was significantly predicted bypathological stage greater than T2, preoperativePSA, Gleason score on RP, PSM, and total and indextumor extent. However, on multivariate analysisonly index tumor extent was an independent predic-tor of shorter TBCR.
The method that we used to evaluate dominantnodule extent is similar to that of Eichelberger20 andDvorak21 et al. They measured the largest diameterof the largest single focus in mm. We counted thenumber of positive points using the semiquantita-tive point count method. A drawback to the 2 meth-ods is that they underestimate the real extent of thedominant nodule, which may be greater if the quad-rants preceding or following the quadrant with thelargest focus are also measured. The positive pointsin quadrants E10, E14 and E16 could also becounted (fig. 1). However, considering that eachquadrant is 3 to 5 mm thick and prostate cancergrows irregularly and is essentially multifocal, weare not sure whether all of these quadrants repre-sent a single nodule. In favor of this is that consis-tent reproducibility was obtained when measuringthe largest focus in only 1 quadrant.
Some study limitations warrant discussion. Fol-lowup was relatively brief. Johansson et al reportedthat local tumor progression and distant metastasesdeveloped even after 15 years of followup.23 However,more than 90% of patients who undergo RP experiencerelapse within 5 years postoperatively.23,24 Therefore,it is likely that most biochemical progression caseswere already identified in our study.
Also, if we had incorporated additional variablesin the Cox model, such as tumor extent on biopsy,preoperative PSA velocity and others, results couldhave been different. Therefore, other studies areneeded that incorporate these variables.
Computer assisted analysis is the most precisemethod for tumor volume evaluation. However, it istime-consuming and not adopted in routine practice.Our point count method may not be accurate fortotal or index tumor extent evaluation because itignores vertical tumor dimension but is equivalent
to other methods that can be used by the pathologist
PROSTATE TOTAL TUMOR EXTENT VERSUS INDEX TUMOR EXTENT104
in routine practice. It is also controversial whetherthe largest tumor represents the index tumor. Thereis no consensus on the defining feature of an indextumor nodule in an RP specimen. Voting results on thedefinition of an index tumor among pathologists in aconsensus meeting favored largest size (24%), size andgrade (29%), and stage and grade (28%).25 We consid-ered the index tumor to be the largest focus size.
At the International Society of Urological Pathol-ogy consensus conference on handling and stagingRP specimens a recommendation was made that somequantitative estimate of cancer volume should be per-formed, of which the nature depends on routine prac-tice at the pathology laboratory.25 If this recommen-
dation is accepted, our study favors that any kind of
REFERENCES
tween tumor extent in radical prostatectomies and tivariate analysis of 185 c
estimate should be related to the dominant nodule(index tumor) and not to total tumor extent.
CONCLUSIONS
Total and index tumor extent is significantly associ-ated with higher preoperative PSA, clinical stageT2, pathological stage greater than T2, PSM andhigher RP Gleason score. Total and index tumorextent predicted TBCR following RP on univariateanalysis. However, only dominant nodule (index tu-mor) extent was an independent predictor of TBCRon multivariate analysis. The study suggests thatany type of tumor extent estimate in surgical spec-imens should be related to the dominant nodule
(index tumor) and not to total tumor extent.
1. Antunes AA, Srougi M, Dall=Oglio MF et al:Preoperative determination of prostate cancertumor volume: analysis through biopsy frag-ments. Int Braz J Urol 2007; 33: 477.
2. Briganti A, Chun FK, Hutterer GC et al: System-atic assessment of the ability of the number andpercentage of positive biopsy cores to predictpathologic stage and biochemical recurrence af-ter radical prostatectomy. Eur Urol 2007; 52: 733.
3. Brimo F, Vollmer RT, Corcos J et al: Prognosticvalue of various morphometric measurements oftumor extent in prostate needle core tissue. His-topathology 2008; 53: 177.
4. D’Amico AW, Whittington R, Malkowicz SB et al:The combination of preoperative prostate specificantigen and postoperative pathological findingsto predict prostate specific antigen outcome inclinically localized prostate cancer. J Urol 1998;160: 2096.
5. Epstein JI and Potter SR: The pathological inter-pretation and significance of prostate needle bi-opsy findings: implications and current controver-sies. J Urol 2001; 166: 402.
6. Bismar TA, Ewis JS Jr, Vollmer RT et al: Multiplemeasures of carcinoma extent versus perineuralinvasion in prostate needle biopsy tissue in pre-diction of pathologic stage in a screening popu-lation. Am J Surg Pathol 2003; 27: 432.
7. Quintal MM, Meirelles LR, Freitas LL et al: Var-ious morphometric measurements of cancer ex-tent on needle prostatic biopsies: which is pre-dictive of pathologic stage and biochemicalrecurrence following radical prostatectomy? IntUrol Nephrol 2011; 43: 697.
8. Epstein JI: Prognostic significance of tumor vol-ume in radical prostatectomy and needle biopsyspecimens. J Urol 2011; 186: 790.
9. Billis A, Magna LA and Ferreira U: Correlation be-
preoperative PSA, histological grade, surgicalmargins, and extraprostatic extension: Applicationof a new practical method for tumor extentevaluation. Int Braz J Urol 2003; 29: 113.
10. Cantrell BB, DeKlerk DP, Eggleston JC et al:Pathologic factors that influence prognosis instage A prostatic cancer: the influence of extentversus grade. J Urol 1981; 125: 516.
11. Humphrey PA and Vollmer RT: Percentage carci-noma as a measure of prostatic tumor size inradical prostatectomy tissues. Mod Pathol 1997;10: 326.
12. Renshaw AA, Chang H and D’Amico AV: Estima-tion of tumor volume in radical prostatectomyspecimens in routine clinical practice. Am J ClinPathol 1997; 107: 704.
13. Renshaw AA, Richie JR, Loughlin KR et al: Max-imum diameter of prostatic carcinoma is a sim-ple, inexpensive, and independent predictor ofprostate-specific antigen failure in radical prosta-tectomy specimens. Am J Clin Pathol 1999; 111:641.
14. Humphrey PA and Vollmer RT: Intraglandular tu-mor extent and prognosis in prostatic carcinoma:application of a grid method to prostatectomyspecimens. Hum Pathol 1990; 21: 799.
15. Stamey TA, McNeal JE, Yemoto CM et al: Bio-logical determinants of cancer progression inmen with prostate cancer. JAMA 1999; 281:1395.
16. Carvalhal GF, Humphrey PA, Thorson P et al:Visual estimate of the percentage of carcinoma isan independent predictor of prostate carcinomarecurrence after radical prostatectomy. Cancer2000; 89: 1308.
17. Epstein JI, Carmichael M, Partin AW et al: Istumor volume an independent predictor of pro-gression following radical prostatectomy? A mul-
linical stage B adeno-
carcinomas of the prostate with 5 years offollowup. J Urol 1993; 149: 1478.
18. Salomon L, Levrel O, Anastasiadis AG et al:Prognostic significance of tumor volume afterradical prostatectomy: a multivariate analysis ofpathological prognostic factors. Eur Urol 2003;43: 39.
19. Wolters T, Roobol MJ, van Leeuwen PJ et al:Should pathologists routinely report prostate tu-mour volume? The prognostic value of tumourvolume in prostate cancer. Eur Urol 2010; 57: 821.
20. Eichelberger LE, Koch MO, Eble JN et al: Maxi-mum tumor diameter is an independent predictorof prostate-specific antigen recurrence in pros-tate cancer. Mod Pathol 2005; 18: 886.
21. Dvorak T, Chen MH, Renshaw AA et al: Maximaltumor diameter and the risk of PSA failure in menwith specimen-confined prostate cancer. Urology2005; 66: 1024.
22. Cookson MS, Aus G, Burnett AL et al: Variation inthe definition of biochemical recurrence in pa-tients treated for localized prostate cancer: theAmerican Urological Association Prostate Guide-lines for Localized Prostate Cancer Update Panelreport and recommendations for a standard in thereporting of surgical outcomes. J Urol 2007; 177:540.
23. Johansson JE, Andrén O, Andersson SO et al:Natural history of early, localized prostate cancer.JAMA 2004; 291: 2713.
24. Kattan MW, Eastham JA, Stapleton AM et al: Apreoperative nomogram for disease recurrencefollowing radical prostatectomy for prostate can-cer. J Natl Cancer Inst 1998; 90: 766.
25. Van der Kwast TH, Amin MB, Billis A et al:International Society of Urological Pathology(ISUP) consensus conference on handling andstaging of RP specimens. Working Group 2: T2substaging and prostate cancer volume. Mod