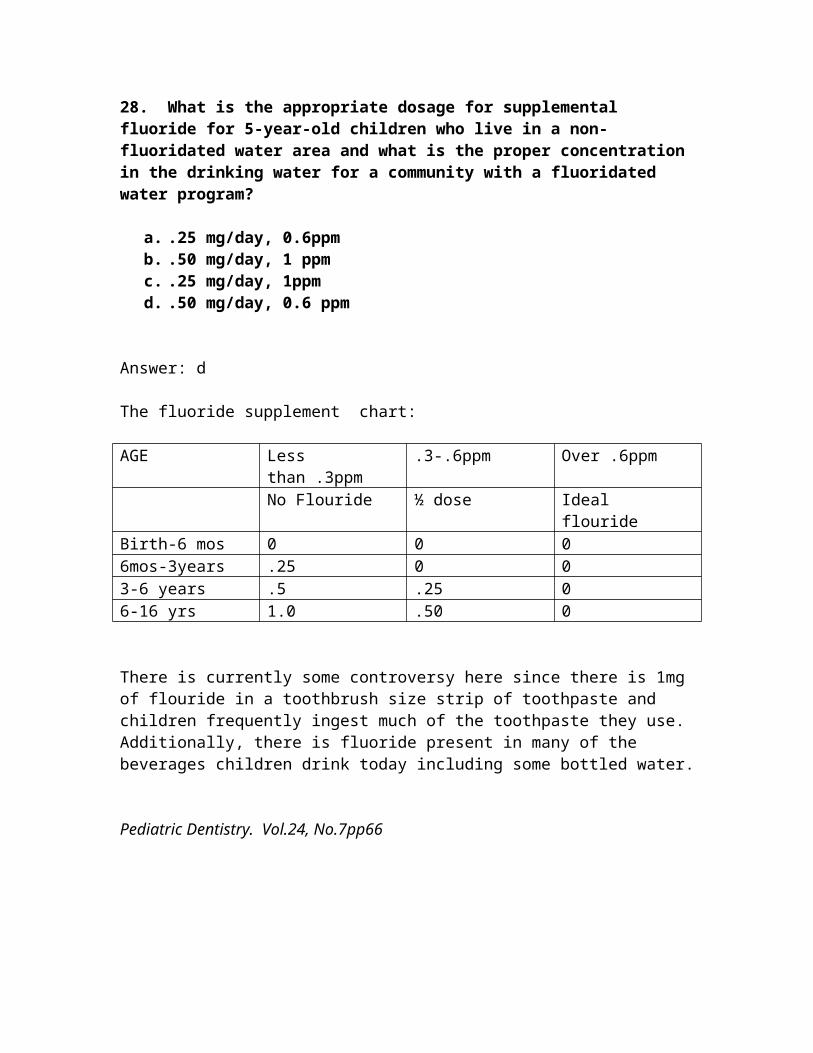
Prosthodontics 1. Arrange the following provisional materials from most desirable to least desirable in terms of temperature increase during setting reaction: a. Trim, Jet, Firmit b. Jet, Firmit, Trim c. Firmit, Jet, Trim d. Firmit, Trim, Jet A: The answer is: d. Firmit, Trim, Jet. In general, the greater the size of the monomer molecule, the less is the exothermic heat of reaction on setting and mechanical properties is accomplished mainly through the filler. An increase in filler content reduces the relative amounts of exothermic heat and contraction while increasing the strength of the set material. For light-activated systems the amount of filler is determined by the manufacturer; for the other systems it is desirable to incorporate as much filler as possible without interfering in the handling or manipulation characteristics of the material. Contemporary Fixed Prosthodontics, 2 nd ed. Rosenstiel et al
Transcript
Prosthodontics
1. Arrange the following provisional materials from most desirable to least desirable in terms of temperature increase during setting reaction:
A: The answer is: d. Firmit, Trim, Jet. In general, the greater the size of the monomer molecule, the less is the exothermic heat of reaction on setting and mechanical properties is accomplished mainly through the filler. An increase in filler content reduces the relative amounts of exothermic heat and contraction while increasing the strength of the set material.
For light-activated systems the amount of filler is determined by the manufacturer; for the other systems it is desirable to incorporate as much filler as possible without interfering in the handling or manipulation characteristics of the material.
Contemporary Fixed Prosthodontics, 2nd ed. Rosenstiel et al
2. You are selecting a shade for a PFM crown to restore tooth #8. The patient is a 49 year old actress with an exacting personality and she said the most important result for her would be to have the new tooth “blend in” so as to be undetectable. Which order should the following parameters be selected in order to best achieve this goal?a. hue, value, chromab. chroma, value, huec. hue, chroma, valued. chroma, hue, value
The answer is C. hue, chroma, value. You would probably also choose supplemental colors and characterization to give the tooth a natural appearance.It is very important to remember what each of these terms describe:Hue = the variety of a color, shade, or tint. The hue of an object can be red, green, yellow, and so on and is determined by the wavelength of light reflected and/or light observed. In the Vita Lumin shade guide, A1, A2, A3, A4 are said to be similar hue as are the B,C, and D shades. The region with the highest chroma (i.e., the cervical region of the canines) should be used for the initial hue selectionChroma = the intensity of a hue. The terms saturation and Chroma are sometimes use interchangeably. Imagine a bucket of water to which 1 pint of latex paint is added. The saturation or Chroma is low. Adding a second pint of paint increases the Chroma, and so on, until the solution is almost all paint and a High chrome results.
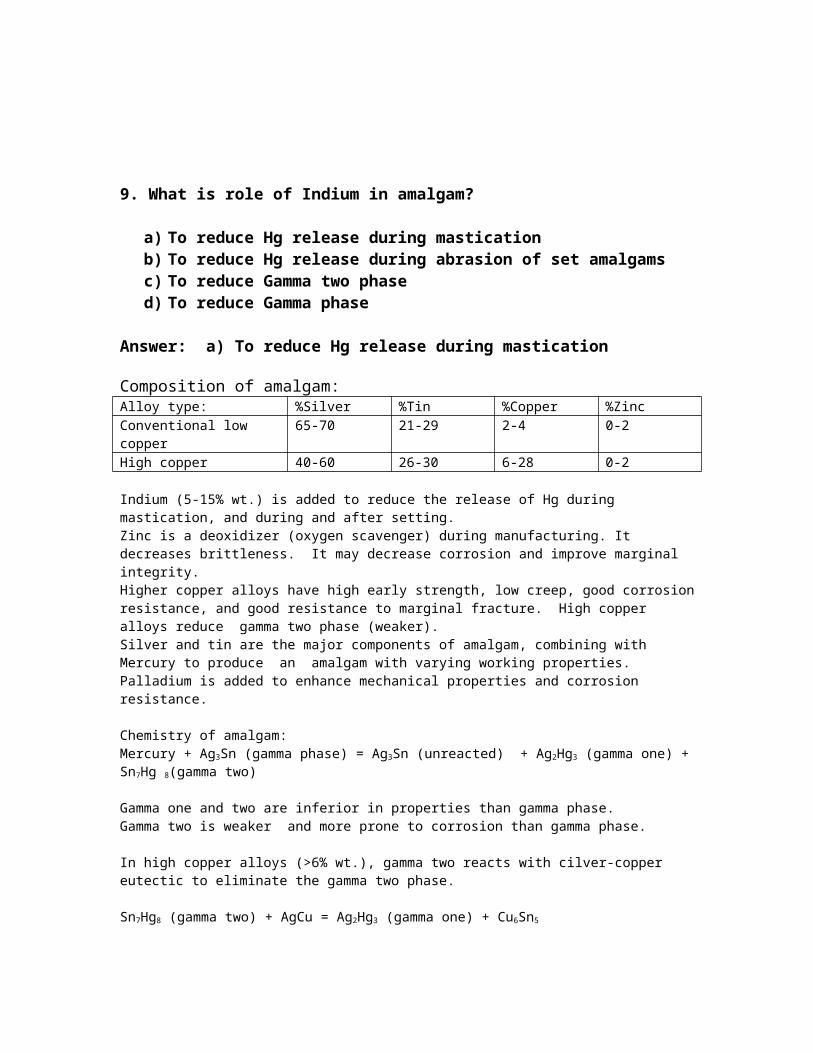
Value = the relative lightness or darkness of a color or the brightness of an object. The brightness of any object is a direct consequence of the amount of light energy that the object reflects or transmits. The value for a given tooth can be determined WITH A SECOND COMMERCIAL SHADE GUIDE whose samples are arranged in order of increasing lightness.Contemporary Fixed Prosthodontics, Rosenstiel, et al. pp 489-494
3. Which of the following statements regarding custom trays is, (are) true?
a. There is a primary sources of error which is eliminated: stresses during removal.
b. Although reducing the bulk of an elastomeric impression material increases its accuracy, the opposite is true for reversible hydrocolloid impression materials.
c. Light-polymerized materials, when used for custom trays offer the advantage of convenience because a storage period of 24 hours is not needed to allow for the completion of poloymerization.
d. Even slight flexing of the custom tray will lead to a distorted impression which is usually undetectable until one attempts to seat the restoration.
e. All of the above
Answer: e. all the above
4. When do you reline a distal extension RPD?1. When the indirect retainer lifts from it’s rest seat upon digital pressure to the
distal Extension
2. When a wash of alginate appears on the buccal shelf area more than .5mm thick.
3. If the natural dentition fails to pierce 2 pieces of 28 gauge soft green wax placed over the denture teeth while the remaining natural teeth in opposition are making firm contact.
4. If rotation and settling of the distal extension base or bases is obvious when alternate finger pressure is applied on either side of the fulcrum line.
a. 1,3 b. 1,4
c. all of the aboved. 1,2,3
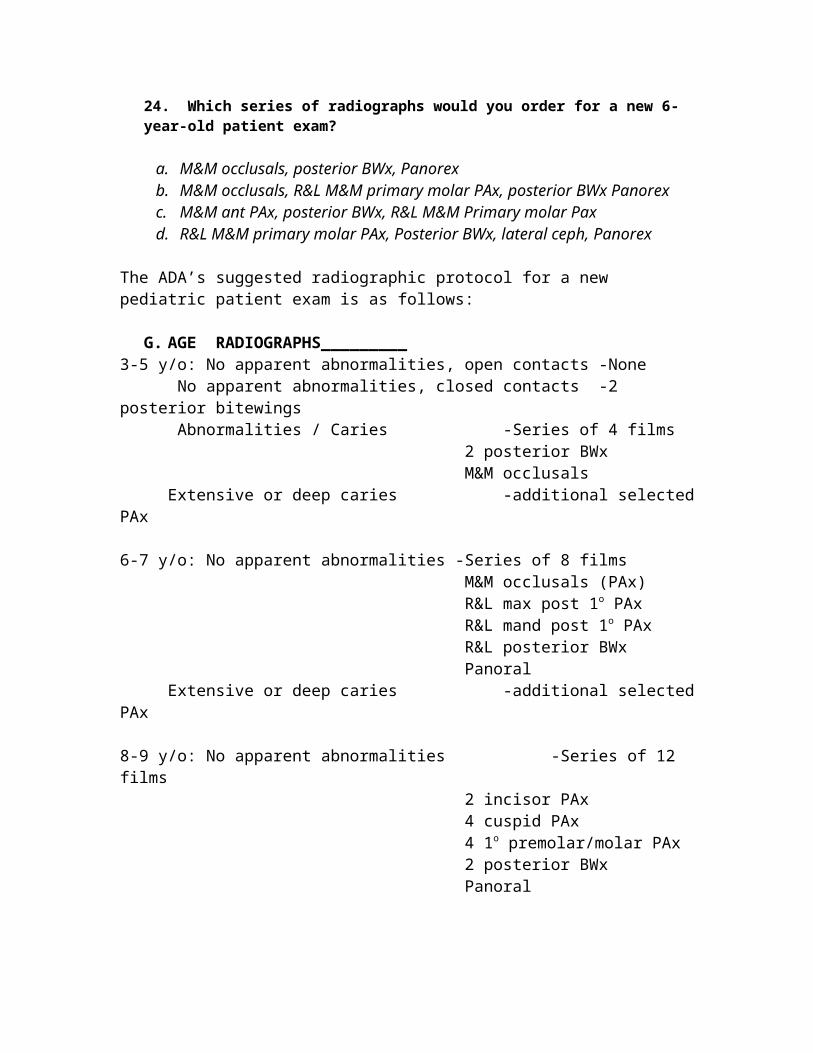
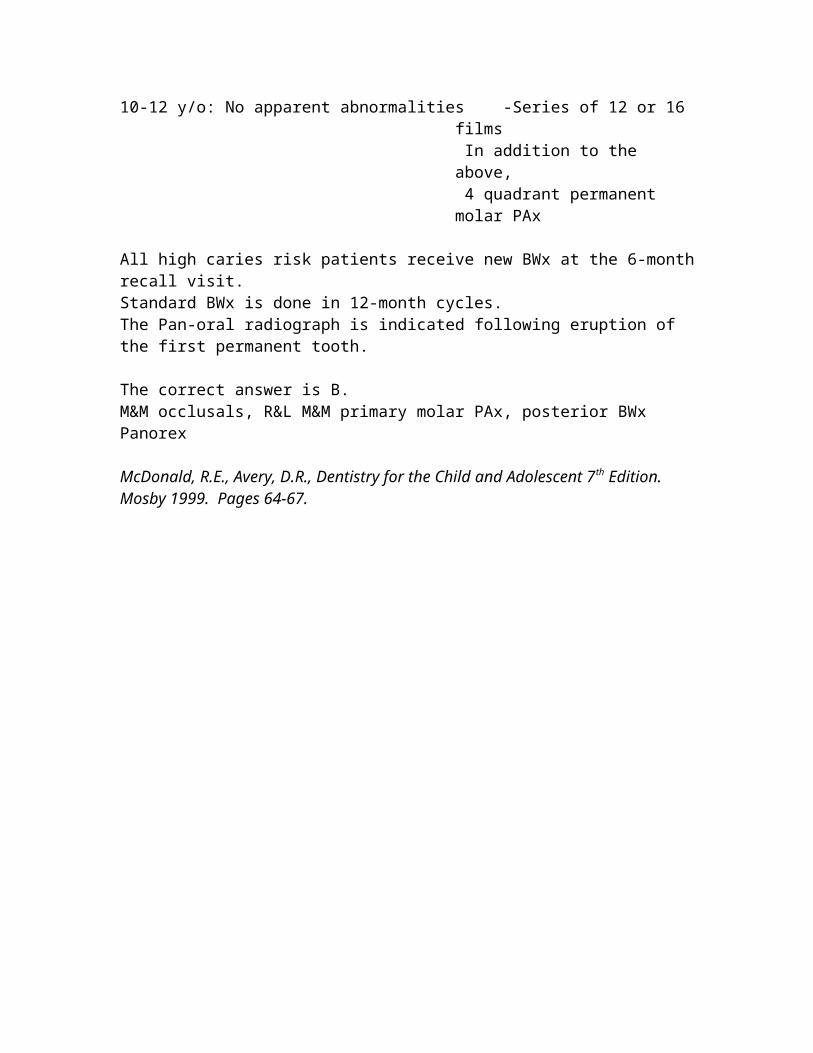
The answer is: CA wash of alginate with 1 scoop of alginate to 2 measures of hot water will provide a mix that is thin enough to not displace soft tissues and yet set quickly. When applying pressure to the most posterior aspect of the denture base, the amount of space under the indirect retainer is an indicator of the amount of space to be found under the denture base. Some clinical judgment is essential here because the length of the distal extension base affects the amount of movement, as does the distance from the indirect retainer to the fulcrum line.
Clinical Removable Partial Prosthodontics, Third ed, Phoenix et al pp 463-464McCracken’s Removable Partial Prosthodontics ninth ed. Pp 449.
5. Which of the following features regarding mutually protected occlusion are true?1. The anterior maxillary teeth and anterior mandibular teeth together guide excursive movements of the mandible.2. No posterior occlusal contacts occur during lateral or protrusive excursions.3. The posterior teeth come into contact only at the end of each chewing stroke acting as stops for vertical closure when the mandible returns to it’s intercuspal position.
a. 1b. 1,2c. 1,3d. all the above
The answer is: DThe study of occlusion can historically be broadly categorized into three categories:-Bilaterally Balanced-Group Function-Mutually ProtectedRecently, the emphasis in teaching fixed prosthodontics and restorative dentistry has been placed on the concept of mutually protected occlusion. More recent investigations that focus on the neuromuscular physiology of the masticatory apparatus are supportive of the advantages associated with a mutually protected occlusal scheme. A subset of this scheme would be canine guidance or cuspid rise.Contemporary Fixed Prosthodontics, 2nd Ed. Rosenstiel et al
6. Which of the following are true concerning casting metals?1. Patients cannot develop a nickel allergy from Jelenko’s “Genesis II”.2. Nickel allergies are more common in males.3. Rexalloy, and Rexillium II, are examples of nickel free alloy.4. Nickel is a noble metal.
a. all the above are trueb. none are truec. 1,2,3 are trued. 3,4,5 are truee. 1 only
The answer is E, only 1 is true. Jelenko’s “Genesis II” is a metal alloy without nickel in it-thus no chance for a nickel allergy. Females are said to have Nickel allergies 9%, and males .9%. (CAPT Beatty lecture). He stated that you can’t give them a nickel allergy, you just may get a reaction to an alloy with nickel in it if they are already sensitive. The Nickel replaces gold in some base metal alloys. It is a base metal. It increases the CTE-Coefficent of thermal expansion, it also has an anti-corrosion characteristic, and may be carcinogenic. (page 117 of Fixed Pros Syllabus). Rexalloy and Rexillium II, are examples of nickel alloys, with Rexalloy being 67% Ni, 14% Chromium, Rexillium=76% Ni, 14% Cr. (page 127 of Fixed Pros Syllabus.
7. Which of the following are true concerning A-P strap facts?1. The A/P palatal strap has limited applications in maxillary partial denture designs.2. The posterior strap should be slightly round and 6 mm. wide.3. The strap should never be placed on moving tissue. And should cross the midline at a right angle not on a diagonal.4. A maxillary torus is a contraindication to the A-P palatal strap design.5. Flexure is almost non-existent in the A-P design.6. It is usually used for Kennedy class II and IV’s. a. all the above are true
b. none are truec. 1,2,3 are trued 2,4,6 are truee. 3,5,6 are true
The answer is FThe A/P palatal strap design can be used in almost any maxillary partial denture design. Thus 1. is false. The posterior strap should be flat and a minimum of 8-12 mm wide. Thus 2 is false. They should be located as far posterior as possible but NEVER on moveable tissues. And they should cross the midline at a right angle; the tongue will not appreciate an asymmetric appliance as readily. So #3 is true. An inoperable maxillary torus may not allow one to use an A-P design but some tori are negotiable. So #4 is false. Flexure is practically nonexistent as each component braces the others against possible torque and flexure. So #5 is true. And finally the A-P strap design is most often used for Class II and IV Kennedy classes. With the single wide palatal strap used for the Kennedy Class III’s.SOURCE: McCRACKEN’S REMOVABLE PARTIAL DENTURES page 52-54.
8. Which of the following is/are a likely cause of sore spots on the ridges from both dentures after delivery?
a. Inaccurate denture baseb. Malocclusionc. Excessive peripheral seald. Overextension of the borderse. Excessive vertical dimension
The answers are a,b,e.A localized sore spot on the ridges can be caused by faulty occlusion, a resin spicule or an inaccurate denture base. If a malocclusion exists then a patient remount will be needed. For excessive vertical dimension, treatment= patient remount to lower VDO, or make new Complete Dentures. For inaccurate denture bases you can reline or rebase or make new dentures. I don’t think you can ever have too much peripheral seal, and an overextension of the borders will give you sore spots in the vestibule not on the ridges. Ref. CAPT Van der Creek Complete Denture Syllabus. p. 113-Troubleshooting.
9. What percentage and type of patient’s have clicking and what percentage have crepitus?
1. Generally about 40-75% of the population have one sign of joint dysfunction. It is possible that joint sounds can be found in 50% of the non-patient population2. Several studies report that progression of intracapsular disorders as determined by joint sounds only occurs in 7-9% of patients.3. de Leeuw study showed that sounds persisted in 54% of patients who had nonsurgical management of intracapsular disorders-yet none had any discomfort or dysfunction.4. Men usually have more symptoms such as headaches, clicking, TMD tenderness and muscle tenderness.5. Signs and symptoms in kids’ increases in frequency with age, joint sounds can be heard 17.5% of the time. The clicking can come and go over a five year period.
A. 1,2,3 are trueB. All are trueC. 1,2,3,5 are trueD. 3,4,5 are true
The answer is C. All are true except 4Women usually have more symptoms such as headaches, clicking, TMD tenderness and muscle tenderness.Crepitus is defined as multiple, rough, gravel-like sound and described as grating and complicated. Joint sounds of a single event of short duration are known as clicks. If the joint sound is loud it is referred to as a pop. Pain in the TMJ is referred to as Arthralgia-the pain originates from the nociceptors located in the soft tissue surrounding the joint. . Joint sounds appear to be much more resistant to therapy and do not always indicate a progressive disorder.REFERENCE: Okeson Orofacial Pain p. 116-118.
10. Which of the following is/are true concerning Kennedy’s/Applegates rules?1. Kennedy class 1 involves bilateral edentulous areas posterior to the natural teeth while a Class II has a unilateral edentulous area posterior to the natural teeth.2. Kennedy Class 3 always has one unilateral edentulous area with teeth posterior to it. A Class 4 has a single edentulous area crossing the midline and anterior to natural teeth.3. You may have up to 2 mods only in a Kennedy Class 4 case. 4. If a second or third molar is missing and is not to be replaced it is not considered in Applegate's rules. If to be replaced it will determine the class.5. Modifications are those areas other than the those that determine the classification and are designated by their number.
A. All the above are trueB. None are trueC. 1,2,3 are trueD. 1,4,5 are trueE. 3,4,5 are trueF. 1,4 are true.
The answer is D.Kennedy class 1 does involve bilateral edentulous areas posterior to the natural teeth while a Class II has a unilateral edentulous area posterior to the natural teeth. So 1 is true.A Kennedy Class 3 has a unilateral edentulous area with teeth Anterior and Posterior to it. A Class 4 does have a single edentulous area crossing the midline and anterior to natural teeth. Thus only the second part is true so the answer is false. You can not have ANY mod spaces in a Kennedy Class 4 case. So #3 is false. If a second or third molar is missing and is not to be replaced it is not considered in Applegate's rules. If to be replaced it will determine the class. Thus #4 is true. Modifications are those areas other than those that determine the classification and are designated by their number. Thus #5 is true. SOURCE: McCracken’s REMOVABLE PARTIAL DENTURES page 20-21.
11. Which of the following are true concerning resin-bonded bridge designs?1. Contraindications would be mutually protected occlusion (with a canine guidance), more than one pontic, and bruxism.2. A cingulum rest or an occlusal rest is needed to provide a vertical stop.3. A single path of insertion, with parallel grooves.4. 120o of encirclement with a centric occlusal contact only.5. Resistance form, a shallow chamfer at a depth of .25 to .5 mm.
a. 1,2,3 are true.b. 3,4,5 are true.c. All are true.d. 2,3,5 are true.e. 1,3,5 are true.
The answer is D.Mutually protected occlusion is not a contraindication, the notes state that it is more desirable than group function, and is only a relative contraindication. A cingulum rest or an occlusal rest is needed to provide a vertical stop, a single path of insertion with parallel grooves is also necessary. 180o of encirclement is needed with a centric occlusal contact only. And finally resistance form is needed with shallow chamfer at a depth of .25 to .5 mm.SOURCE: CAPT Joe Rusz’s lecture 13 FEB 02
12. After surveying your diagnostic casts you determine your RPD design and the necessary alterations. The design is then drawn on the cast and you are now ready to make tooth modifications. In what sequence will you follow?
a. Heights of contour / guiding planes / rest seats / diagnostic impressionb. Guiding planes/ diagnostic impression / heights of contour / rest seats c. Guiding planes / heights of contour / rest seats / diagnostic impressiond. Guiding planes/ heights of contour / diagnostic impression / rest seats
The correct sequence for preparing teeth to serve as RPD abutments is D. Guiding planes/ heights of contour / diagnostic impression / rest seats1.) Proximal surfaces parallel to the path of placement should be prepared to provide guiding planes.2.) Axial tooth contours should be modified lowering the height of contour so that the origin circumferential clasps may be placed below the occlusal surface; and the retentive clasp terminus is located below the junction of the middle and gingival third (better esthetics and mechanical advantage); reciprocal clasps can be placed above HOC at the junction of the middle and occlusal thirds.3.) Diagnostic/verification impression in irreversible hydrocolloid poured in fast set stone to re-survey and confirm adequacy of preparations. If further adjustments need to be made you will not disturb your rest seat preps4.) Occlusal rest seats are always last and should be prepared in a manner that they will direct occlusal forces along the long axes of the abutment tooth
13. The signs of Ellsworth / Kelly Combination Syndrome are:1. Papillary hyperplasia2. Maxillary tuberosity growth3. Ridge resorption of mandibular posterior4. Ridge resorption of anterior maxilla5. Hyper-eruption of mandibular anterior teeth
A. 1, 2, 4, 5 B. 2, 4, 5
C. 2, 3, 4, 5D. All of the above
Correct answer is D. All of the aboveThe Glossary of Prosthodontic Terms1 defines combination syndrome as “the characteristic features that occur when an edentulous maxilla is opposed by natural mandibular anterior teeth, including loss of bone from the anterior portion of the maxillary ridge, overgrowth of the tuberosities, papillary hyperplasia of the hard palatal mucosa, extrusion of mandibular anterior teeth, and loss of alveolar bone and ridge height beneath the mandibular removable partial denture bases, also called anterior hyperfunction syndrome.”
In addition the following have been added as a subset to the classic signs listed above: loss of vertical dimension of occlusion, occlusal plane discrepancy, anterior spatial repositioning of the mandible, poor adaptation of the prostheses, epulis fissuratum, and periodontal changes. However, these changes are not generally associated with combination syndrome.Palmqvist S, Carlsson GE, Owall B. The combination syndrome: a literature review. J Prosthet Dent. 2003 Sep;90(3):270-5.
14. When replacing a missing cuspid with an FPD, occlusion should be shared with the first bicuspid (i.e. Group function). When replacing a missing cuspid with an FPD, occlusion should remain only on the cuspid (i.e. Canine guidance)
a. Both statements are trueb. Both statements are falsec. First statement is true, second statement is falsed. First statement is false, second statement is true
Answer is C. First statement is true, second statement is falseGroup function, also termed unilaterally balanced articulation, is defined as excursive contacts that occur distal to the cuspid (can include or exclude the cuspid) on the working side in laterotrusive movements without contacts on the non-working, mediotrusive side. This can be advantageous if the periodontal support of the cuspid is compromised, or non-existent in this case. Then the load is distributed and shared by directing it over an occlusal surface that has sufficient periodontal support. Canine guidance of laterotrusive movements of the mandible results in complete disclusion of all posterior teeth. This is expanded to the “scheme” of a Mutually Protected Occlusion in which the six maxillary anterior teeth together with the six mandibular anterior teeth guide excursive movements and allow no posterior contacts to occur during lateral or protrusive movements.Rosenstiel, Land, Fujimoto. Contemporary Fixed Prosthodontics 3rd Edition, Mosby 2001, Pages 94-97, 105
15. Post denture insertion pain – everything is sore – Why? 1. Over extended borders2. Acrylic monomer allergy2. Excessive vertical dimension of occlusion3. Insufficient vertical dimension of occlusion4. Occlusal prematurityA. 1, 2, 3, 4B. 1, 3, 4, C. 1, 2, 3, 5D. 1, 3, 5E. 1, 3, 4, 5
Answers: E. 1, 3, 4, 5 Over extended borders, excessive vertical dimension, insufficient vertical dimension, occlusal prematurity. 1- Over extended borders can cause: Soreness in the vestibules, sore spots from a deep posterior palatal seal, trouble swallowing, immediate gagging upon swallowing, and denture instability when out of occlusion.2- Acrylic monomer allergy can cause: Generalized burning sensation.3- Excessive vertical dimension of occlusion can cause: Generalized ridge soreness, immediate gagging, muscle soreness, TMJ symptoms, trouble swallowing, clicking during speech, and excessive display of teeth.4- Insufficient vertical dimension of occlusion can cause: Angular cheilitis, muscle soreness, TMJ Symptoms, and tongue or cheek biting.5- Occlusal prematurity can cause: Sore spots in the vestibule or on the ridges, delayed gagging upon swallowing, muscle soreness, TMJ symptoms, denture instability when in CR occlusion.Naval Post Graduate Dental School, Complete Denture Syllabus, NDS Course #252, Troubleshooting, Pages 113-116
16. When restoring two edentulous spaces on either side of a pier abutment it is beneficial to employ a stress breaker. If you intend to restore a missing #7 and #9 with a 5 unit FPD abutted on #’s 6, 8, and 10, where would you employ the components of the stress breaker
a. Key on distal of #9 pontic, keyway on mesial of #10 abutment b. Key on mesial of #7 pontic, keyway on distal of #8 abutmentc. Key on mesial of #9 pontic, keyway on mesial of #8 abutmentd. Key on distal of #8 abutment, keyway on mesial of #7 pontice. Key on mesial of #8 abutment, keyway on mesial of #9 ponticf. Key on distal of #10 abutment, keyway on mesial of #9 pontic
Answer is B. Key on mesial of #7 pontic, keyway on distal of #8 abutmentA stress breaker, now referred to as a stress director, is a device or system that relieves specific dental structures of part or all of the occlusal forces and redirects those forces to other bearing structures. These can be utilized in fixed partial dentures of long spans, while spanning multiple edentulous spaces when pier abutments are used, for periodontally involved teeth. The director is placed on the mesial of the distal pontic, behind the pier abutment. The key component of the director is always placed on the pontic so that forces of occlusion direct it to seat in the keyway component placed on the pier abutment. If the reverse were done occlusal forces would un-seat the components sliding the keyway out of the key thus making the pontic a lever arm that exerts torque on the abutment to which it is attached.
17.In respects to pontic design, order the following according to decreasing esthetics? a. Modified Ridge-lap, Conical, Ovate, Saddle, Sanitary b. Saddle, Modified Ridge-lap, Conical, Sanitary, Ovate
c. Modified Ridge-lap, Ovate, Conical, Saddle, Sanitary d. Ovate, Modified Ridge-lap, Saddle, Conical, Sanitary e. Ovate, Modified Ridge-lap, Conical, Saddle, Sanitary
The answer is D. Ovate, Modified Ridge-lap, Saddle, Conical, Sanitary Sanitary or Hygienic. Recommended Location: posterior mandible. Advantage: good access for oral hygiene. Disadvantage: poor esthetics (2mm clearance between ridge and pontic). Indications: non-esthetic zones, impaired oral hygiene. Contraindications: esthetic zone, minimal VDO. Saddle-ridge-lap. Recommended Location: none. Advantages: esthetics. Disadvantages: not amenable to oral hygiene. Indications: not recommended. Contraindications: all. Conical. Recommended Location: molars without esthetics requirements. Advantages: good access for oral hygiene. Disadvantages: poor esthetics. Indications: posterior areas where esthetics is of minimal concern. Contraindications: poor oral hygiene. Modified ridge-lap. Recommended Location: High esthetic requirements. Advantages: good esthetics. Disadvantages: moderately easy to clean. Indications: most areas with esthetic concerns. Contraindications: areas with minimal esthetic concern. Ovate. Recommended Location: Maxillary incisor, cuspids, and bicuspids. Advantages: superior esthetics, negligible food entrapment, ease of cleaning. Disadvantages: requires surgical preparation. Indications: desire for optimal esthetics, high smile line. Contraindications: unwillingness for surgery, mandibular posterior. Rosenstiel, Land, Fujimoto. Contemporary Fixed Prosthodontics 3rd Edition, Mosby 2001, Page 520-525
18. What muscles are involved with border molding for a complete denture mandibular final impression?
a. Buccinator, masseter, mylohyoid, palatoglossal, medial pterygoid and the superior constrictor muscleb. Buccinator, masseter, mylohyoid, palatoglossal, and the genioglossus musclec. Buccinator, masseter, mylohyoid, hyoglossus and the superior constrictor muscled. Buccinator and masseter
The answer is AThe borders of the final denture impression are determined by several muscles. The buccal vestibule is influenced by the buccinator muscle. The distobuccal border is determined by the actions of the masseter. The masseter contacts forcing the buccinator muscle in and decreases the space available for the denture. This action can cause it to dislodge. The buccinator, superior constrictor, and the tendon of the temporalis influence the retromolar pad placement of the denture. The posterior lingual border position is controlled by the mylohyoid muscle. During swallowing the muscle contracts and raises the floor of the mouth. The superior constrictor, mylohyoid and palatoglossal, and medial pterygoid muscle can all influence the border molding in the retromylohyoid region. The obicularis oris shapes the labial vestibule. The maxillary denture borders are affected by the obicularis ori, buccinator, levator anguli, and the masseter..Boucher’s Prosthodontic Treatment for Edentulous Patients, Eleventh Edition. Pg 166-172
19. The only universally flexible clasp shape is the round form. Half round will flex away form the tooth.
a. Both statements are trueb. Both statements are falsec. Statement one is true and two is falsed. Statement two is true and one is false
The answer is A.Full round clasps are able to flex in any direction. Half round is flexible in only the direction away from the tooth. The type of material the clasp is made form determines flexibility as well. Cast chromium alloys are less flexible than wrought wire. The bulk or thickness of the clasp is a factor. Gold clasps must be thicker to obtain strength so they are not as flexible as a thinner chromium clasp. A retentive arm that is tapered length wise and width wise is more flexible than one that is not. The longer the retentive arm (I-bar) the more flexible it becomes. The least flexible clasp would be a short, no taper, half round, bulky clasp.
20. Centric relation is defined as:a. The position in which the condyle is in the most superior anterior position in
the articular fossa with the thinnest portion of the disk between the condyle and the fossa.
b. The position in which the condyle is in the most superior retruded position in the articular fossa with the thinnest portion of the disk between the condyle and the fossa.
c. The position in which the condyle is in the most superior retruded position in the articular fossa with the thickest portion of the disk between the condyle and the fossa.
d. The position in which the condyle is in the most inferior retruded position in the articular fossa with the thickest portion of the disk between the condyle and the fossa.
The answer is A.Centric relation is the most physiologic stable and repeatable position of the condyle. This position is helpful in restoring patients that do not have a stable maximum intercuspation or no repeatable jaw relationship. The disk must be situated with the thinnest part between the condyle and the fossa. The Academy of Prosthodontics defines it as the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disk with the complex in the anterior-superior position against the shapes of the articular eminence. This position is independent of tooth contact. The mandible is restricted to purely rotary movement about the transverse axis.Management of Temporomandibular disorders and occlusion, Fifth edition. Pg. 111-113.The Academy of Prosthodontics. Glossary of Prosthodontic Terms, Journal of Prosthetic Dentistry;71:1, 1994.
21. Double abutments can be used as a means of overcoming problems created by unfavorable crown to root ratios. Since there are two abutments acting together it is not necessary for additional abutment to have as much root surface as the first abutment.
a. Both statements are trueb. Both statements are falsec. Statement one is true and two is falsed. Statement two is true and one is false
The answer is C.Antes law indicates that the surface area of roots in bone of the abutment teeth should be equal to or greater than the teeth they are replacing with a FPD. If inadequate root surface area is present it is possible to use double abutments to compensate for this. The secondary abutment must have as much root surface area as the primary abutment tooth. The retainer of the secondary abutment tooth must be as retentive as the primary abutment. There must be sufficient space to allow for soft tissue under the connector between the primary and secondary abutment. Double abutments also help resist the lever arm that can be produced if an FPD spans around the arch; such as a FPD that replaces the four anterior teeth.Shillingburg, Fundamentals of Fixed Prosthodontics, Third Edition, Page 93
22. Electrosurgery units will work without a grounding plate. Grounding plates are only necessary if a metal restoration might be contacted.
a. Both statements are trueb. Both statements are falsec. Statement one is true and two is falsed. Statement two is true and one is false
The answer is C.The grounding plate also known as the indifferent plate, neutral electrode, dispersive electrode r patient return is necessary for using the unit. Electrosurgery units will work without the grounding plate but the patient is at risk of receiving a burn. Proper grounding is the single most important safety issue. It is acceptable to attach the metallic mesh grounding antenna under the upholstery insulated from all metal parts.Fundamentals of Fixed Prosthodontics, Third Edition, 269-271
23. Lingualized occlusion uses anatomic maxillary teeth opposing mandibular monoplane teeth. Lingualized occlusion can be indicated for skeletal Class II and III patients.
a. Both statements are trueb. Both statements are falsec. Statement one is true and two is falsed. Statement two is true and one is false
The answer is A.Lingualized occlusion is useful for patients that are difficult to reproduce an accurate CR position. This scheme gives freedom of movement and reduces interferences to protrusive movements. It is esthetic using maxillary anatomical teeth and is easy to set the teeth and develop a cross arch balanced occlusion.
1. Becker CM, Swoope CC, Guckes AD. Lingualized occlusion for removable prosthodontics. J Prosthet Dent 1977;38(6):601-8.2. Clough HE, Knodle JM, Leeper SH, Pudwill ML, Taylor DT. A comparison of lingualized occlusion and monoplane occlusion in complete dentures. J Prosthet Dent 1983;50(2):176-9.3. Lang BR, Razzoog ME. Lingualized integration: tooth molds and an occlusal scheme for edentulous implant patients. Implant Dent 1992;1(3):204-11.4. Ohguri T, Kawano F, Ichikawa T, Matsumoto N. Influence of occlusal scheme on the pressure distribution under a complete denture. Int J Prosthodont 1999;12(4):353-8.
24. Which are advantages of polyether impression materials?a. Fast setting and good for undercutsb. Fast setting, good shelf life (two years), multiple poursc. Very flexible and good for deep undercutsd. Slow setting with prolonged working time
The answer is B.Polyether is a very stiff material that is not good for undercuts. Undercuts must be blocked out. The material is rigid and dimensional stability is good. Multiple pours can be done. The shelf life for the material is about two years. It sets fast and has a short working time. Finish lines can be easily read. Polyjel, Impregum F, and Permadynes are all examples.Polysulfides have good surface detail, flows into deep subgingival crevices, excellent tear strength, and multiple pours are possible. Disadvantages are it is not good for severe undercuts, hydrophobic, and it has a bad odor and color.Condensation silicones are an older material that has poor dimensional stability, requires immediate pouring, hydrophobic, and produces ethyl alcohol as a by product. Addition silicones are accurate, good for undercuts, and multiple delays pours are possible. The material is costly, and can release hydrogen gas. Palladium is used as a gas scavenger. Powder from the gloves may inhibit set of the putty.Hydrocolloids are accurate and inexpensive, however they have low tear strength and are accurate for only one pour.Zinc oxide eugenol will adhere to compound and acrylic, can build borders with it, hard when set, good working time, accurate, and dimensionally stable. Disadvantages are the bad taste and rigidity is not good in undercuts.Impression compound has little to no taste, minimal mess, hard when set, and has a good working time. It cannot register fine detail and will displace soft tissue.Fundamentals of Fixed Prosthodontics, Second edition. Pages 221-225
25. A patient with complete dentures makes tries to make “T” sounds but he makes a sound like “Th”. What is the most likely cause?
a. Anterior palate too broad.b. Inadequate interocclusal distance.c. Poor retention of dentures.d. Overextended maxillary posterior border.e. Maxillary premolars too far mesially.
Answer: b) Inadequate interocclusal distance (Also caused by maxillary teeth too far lingual)Solution: Remount, increase interocclusal distance by reducing VDO, or make new CD’s. (Or reset teeth)
a) causes sounds like “sh”c) clicking during speechd) causes gagginge) causes whistling
Phonetics and the linguodental and linguopalatal sounds.- Linguodental sounds: “Th”1/3 (3mm) of tip of tongue extends between maxillary and mandibular anterior teeth.If tongue does not protrude past teeth, maxillary anterior teeth are too far labial or there is excessive overlap.If more than 6mm of tip of tongue protrudes, maxillary teeth are set too far lingually. - Linguopalatal sounds: T & DTip of tongue contacts anterior part of palate or lingual side of anterior teeth.Teeth too far lingual, “T” tends to sound like “D”.Teeth too far labial, “D” sounds like “T”.Denture base palate – too thick in rugae area.Phonetics are related to:- Speaking space.- Denture base, “S” sounds, Rugae area, Lingual extension of mandibular denture.- Tooth positioning, “T” and “D” sounds, “F” and “V” sounds, “S”, “J”, and “Ch” sounds. Reference: Complete Denture Syllabus, Prosthodontic Dept, NPDS, NNDC Bethesda.Rahn, A.O., Heartwell, C.M., Textbook of Complete Dentures, 5th Ed. 1993 Lea & Febiger. Page 330.
26. Which functions are simple hinge articulators not capable of doing?1. Two dimensional movements2. Close customization of temporomandibular joint anatomy 3. Reproduction of side shifts4. Accept facebow transfer
a. 1 onlyb. 1,2,3c. 2,3,4d. 1,2,3,4
Answer: c) 2,3,4 The hinge articulator can only perform two dimensional movements.
Fully adjustable articulator (Class IV)Refers to the reproducibility of the patient’s condylar paths.Only instruments that can produce all condylar border movements including protrusive-lateral paths can be called fully adjustable.Accepts facebow transfer.Simple hinge articulators (Class I)Accepts single static record.Barn door hinge. Vertical motion with very limited lateral movement.Smaller arc of closure that does not come close to actual.Simple hinge articulators are limited only to movements a patient cannot make. Dawson also writes that they are a major cause of errors in occlusal contouring and have no value for restorative procedures or occlusal analysis.Ref: Occlusion, Dawson. Page 206.
27. When using a kinematic facebow one should expect at least a 5mm error in recording the true hinge axis. The arbitrary facebow records an approximation of the true hinge axis by means of average measurements.
a. First statement is true, second is false.b. First statement is false, second is true.c. Both statements are true.d. Both statements are false.
Answer: b) First statement is false, second is true. Kinematic facebow can determine the hinge axis to within 1mm. Arbitrary facebow uses average measurements as determined by each manufacturer.Facebow allows for:- Providing a method of transferring the location of the condylar axis in the skull to the articulator and relating the upper cast to the articulator. - To record the spatial position of the maxillary arch relative to the opening and closing axis.Facebow indications:
- Fixed Partial Dentures if posterior vertical stop is included in the FPD.- With Centric Relation record that increases Vertical Dimension of Occlusion.- Full mouth rehabilitation.- When anterior guidance is deficient.- Remount procedures.- When VDO is changed on the articulator.
Two types of facebows:Arbitrary and Kinematic.- Arbitrary facebows are less accurate but are adequate for many routine dental procedures.- Relies on determination by the manufacturer of the average relationship between the true hinge axis and an easily identifiable landmark, usually the external auditory meatus.- Alignment may be achieved through the use of earpieces.- A minimum error of 5mm from the axis can be expected. This error can be worsened by the use of a thick interocclusal record.- The use of an anterior reference point enables the clinician to duplicate measurements made on the articulator at subsequent appointments.- Kinematic facebows are needed when it is critical to reproduce the exact opening and closing movement of the patient on the articulator.- When the relationship between the maxillae and the axis of rotation has been reproduced, the mandibular cast can be accurately positioned through the use of an interocclusal record.- The hinge axis of the mandible can be determined to within 1mm by observing the movement of kinematic facebow styluses positioned immediately lateral to the TMJ in close proximity to the skin.- The kinematic facebow technique is time-consuming, thus limited to extensive prosthodontics. Change in vertical dimension of occlusion may be included in this group. Contemporary Fixed Prosthodontics, 2 nd Ed. Rosenstiel, S.F., Land, M.F., Fujimoto, J. 1995 Mosby
28. What is the main purpose of a cast distal extension posterior metal stop? a. Provides for a more rigid RPD framework.b. Increases overall retention of the RPD to resist displacement.c. Provides a positive apical seat (tissue stop) for the RPD in function.d. Prevents bending of the distal extension framework during acrylic
processing.
Answer: d) Prevents bending of the distal extension framework during acrylic processing.Without a cast stop the minor connector leading to the distal extension framework of an RPD is supported at only one end, the proximal end. The minor connector may bend when force is applied during packing and processing of the RPD framework. To prevent bending of the framework, a small area at the free end of the minor connector (or distal extension) should contact the master cast. This portion of the minor connector is called a cast stop.A cast stop is formed by removing a small square (2x2mm in surface area) from the wax up used to create the refractory cast. It is positioned on the posterior strut of the minor connector as it crosses the center of the ridge.A thickness of at least 1mm is left between the distal extension struts and the master cast to allow for sufficient bulk of acrylic packing during processing. The cast stop helps preserve this thickness during packing. This thickness of acrylic allows for strength of material as well as room for adjustments.It is the acrylic denture base that provides for the apical seating of the distal extension, not the cast metal stop.Stewart’s Clinical Removable Partial Prosthodontics 3 rd Ed., Phoenix, R.D., Cagna, D.R., DeFreest, C.F. 2003 Quintessence Page 42
29. What all-ceramic porcelain system is strongest (in terms of flexural strength)? a. Traditional powder slurry ceramics
Answer: b) Infiltrated ceramics (slip-cast)Approximate flexural strength ranges for different ceramic systems (these vary according to tooth type position):Porcelain fused to metal 300-500+ MPa (for comparison purposes)Traditional slurry 80-140 MPa Infiltrated (slip cast) 450-600 MPa Heat pressed 140-180 MPaCastable 120 MPaMachinable 120-230 MPaTraditional slurry – uses aluminous porcelain formed over platinum foil matrix. Feldspathic porcelain placed over this core. Infiltrated (slip cast) – aluminous porcelain, infiltrated with glass for strength. Not etchable.Heat pressed – 40-50% leucite reinforced ingot heated and physically pressed into lost wax mold. Etchable. Feldspathic porcelain can be placed over this core.Castable – polycrystalline glass ceramic. Processed like lost wax process.Machinable – computer aided design and machining (CAD-CAM). Uses blocks of feldspathic or glass based ceramic and milled to fit the prepared tooth.Adept Report Vol 5 No. 1 Summer 1995 Page 7.Restorative Dental Materials, 11 th Ed. Craig, R.G., Powers, J.M. 2002 Mosby Page 567
30. Which are advantages of screw retained implant prosthesis?
1. Corrections can easily be made for angular discrepancies between implant fixture and restoration.
2. Can be more easily retrieved.3. Easy to obtain path of draw in multiple unit fixed partial dentures.4. Requires less total vertical space for restoration.
a. 1,2b. 1,3c. 2,4d. all of the above
Answer : c) 2,4Cement retainedAdvantages: Simplicity and economy are plus. Angle corrections can be made to compensate for discrepancies between the implant inclination and the facial crown contour. Abutment can include an anti-rotational feature. Best for small tooth replacement. May be more esthetically pleasing and less expensive. Disadvantages:Require more chair time, same propensity to loosen as screw retained. If zinc phosphate, glass ionomer, or composite resin cements are used, retrieval may be very difficult. Requires more vertical space due to two part construction (Estheticone needs 6.7mm vertical space. Multi unit abutment needs 4.3mm).Screw retainedAdvantages:Retrievability. Crown can be more easily removed for repair, soft tissue evaluation, calculus debridement, and modifications to crown. Forces are usually directed down long axis of implant, optimum esthetics more easily achieved. Less vertical space required for restoration.Disadvantages:Primary disadvantage is that screw may loosen in function. Screw is tightened to seat implant crown to a clamping or preload force. Screw will loosen if masticatory force is greater than the clamping force. Proximal contacts need to be checked carefully so abutment is seated properly (cement abutment does not have this problem). Access hole through occlusal table of posterior teeth may affect esthetics. Contemporary Fixed Prosthodontics, 3 rd Ed., Rosenstiel, Land, Fujimoto, 2001 Mosby. Page 344
31. The quality of a preparation that prevents the restoration from being dislodged by the forces parallel to the path of the withdrawal is known as retention. The resistance form of tooth preparation resists the lateral and oblique forces which tend to displace the restoration by causing rotation around the gingival margin.
a. Both statements are true.b. Both statements are false.c. The first statement is true, second statement is false.
d. The first statement is false, second statement is true.
Answer: A Adequate retention and resistance depends on the following:
o Magnitude and direction of the dislodging forceso Type of preparation o Geometry of the tooth preparation
Cylindrical to restrain the movement Near parallel preparation. Increased surface area (axial wall height) Adding grooves or boxes to limit the path of withdrawal and to interfere
with the rotational movemento Surface roughnesso Material being cementedo Type of luting agent
32. A slot is a retention groove whose length is in a horizontal plane and in dentin and a lock is a retention groove whose length is in a vertical plane and in dentin.Gingival slots are placed in 0.5 mm pulpal of the DEJ, and at least 0.5 mm in depth and 1 or more mm in length depending on the distance between vertical walls.
a. Both statements are true.b. Both statements are false.c. The first statement is true, second statement is false.d. The first statement is false, second statement is true.
Answer: A Slot and lock retentions may be used in conjunction with pins or as an alternative
to it. Lock retentions are used more in preparations with vertical walls which allow locks to oppose one another.
Pin retention is used more in preparations with few or no vertical walls. Pins are to retain the amalgam not to increase the strength of the restorative material.
Shorter slots provide as much resistance to horizontal forces do longer slots. Slots in the gingival floor may be used to provide additional retention in an
extensive proximal box that has facial and lingual walls extending beyond the proximal line angles.
Slot dimension will depend on the size of the proximal box.REF: Sturdevant’s Art and Science of Operative dentistry 4th Edition; p-503
33. Deflection of an FPD is proportional to the cube of its length. If the force on one pontic produced certain amount of deflection, the same force on a three pontics will produce eight times the distance of the deflection.
a. Trueb. False
Answer: B According to Law of beams, for 2 Pontics= 8 times the distance, for 3 pontics= 27
times the distance. Edentulous span length will influence the prep design, number of abutments and
the design of FPD connectors. Excessive flexing under occlusal loads may cause failure of a long-span FPD. It
can lead to fracture of porcelain, breakage of a connector, loosening of a retainer, and unfavorable soft tissue response. All FPDs flex slightly under load, the longer the span, the greater the flexing.
When a long-span FPD is fabricated, pontics and connectors should be made as bulky as possible to ensure maximum rigidity without compromise the gingival health. Also, the FPD material should have high strength and rigidity.
34. Stress-bearing areas are recorded with least amount of pressure and selective pressure is applied to the non-stress-bearing areas.The places with less space or relief will transmit more pressure during the impression.
a. Both statements are true.b. Both statements are false.c. The first statement is true, second statement is false.d. The first statement is false, second statement is true.
Answer: D Selective pressure technique combines the principles of both pressure and non-
pressure procedures. Non-stress-bearing areas are recorded with least amount of pressure and selective pressure is applied to the stress-bearing areas that are capable of withstand the forces of occlusion.
The impressions are made in trays that have been selectively relieved, therefore providing more space in some areas while at the same time having areas within the trays that have less space. The places that have less space or relief will transmit more pressure during the impression. This will distribute the greater force during function to a more favorable part of the area.
Clinical evidence seems to favor the selective pressure technique over functional/physiologic or mucostatic technique.
REF: Complete Denture Syllabus, NDS Course#252.
35. What impression material is most stable 24 hours later?a. Polysulfidesb. Polyethersc. Addition siliconesd. Condensation silicones
Answer: C Dimensional change:
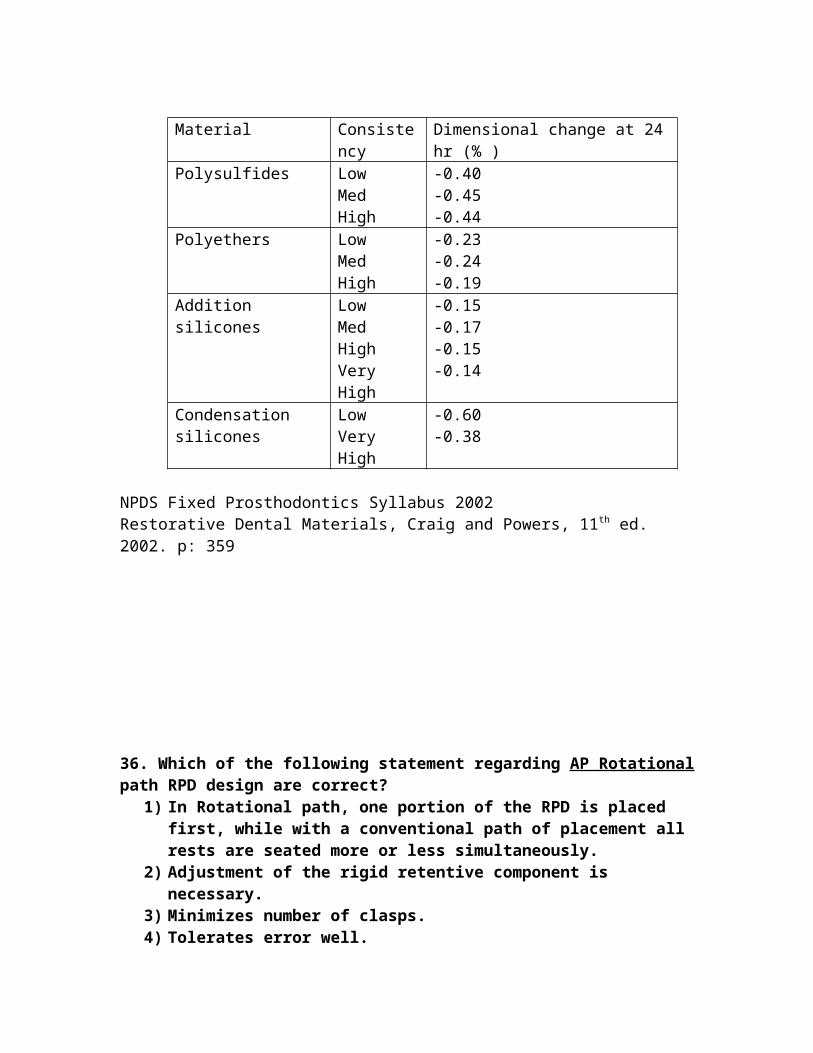
Condensation silicones> Polysulfides>Polyethers> Addition silicones Addition silicones advantages include: accurate, good for undercut, multiple pours
and delay pours. Disadvantages include: costly, some hydrophobic, powder from gloves can inhibit set of putty. Secondary reaction may produce hydrogen gas, and some brands contain Palladium as hydrogen scavenger. Not all addition silicones release hydrogen gas, it is recommended that to wait 30 minutes for the setting reaction to be complete before pouring.
Material Consistency Dimensional change at 24 hr (% )Polysulfides Low
36. Which of the following statement regarding AP Rotational path RPD design are correct?
1) In Rotational path, one portion of the RPD is placed first, while with a conventional path of placement all rests are seated more or less simultaneously.
2) Adjustment of the rigid retentive component is necessary.3) Minimizes number of clasps.4) Tolerates error well.5) May be used as substitute to a long-span anterior FPD.6) Used in absence of lingual or facial undercuts in anterior abutment teeth in
Kennedy class IV anterior abutment teeth.a. 3, 4, 5, 6b. 1, 2, 3, 5c. 2, 3, 5, 6d. 1, 3, 5, 6 e. 1, 2, 3, 6
Answer: D The rotational path concept cannot be reduced simply to a straight path that
deviated marked from the perpendicular. While still fulfilling the requirements of support, stability and retention, proper use of the rotational path permits elimination of clasps. Therefore minimized number of clasp, reduced plaque accumulation and improved aesthetic.
The rigid retentive components are placed or rotated into undercuts and are maintained in intimate tooth contact by their modified rests and other conventional clasp in the design. Adjustment of the rigid retentive component is difficult and little tolerance for error. Distortion of rigid retentive component is unlikely. Rigid retainer may prevent further tipping of abutment teeth contacted.
The retentive undercuts are located in mesial and distal interproximal undercuts (0.20”) therefore often used in absence of lingual or facial undercuts.
37. Researchers have reported that there is little association between the choice of zinc phosphate or glass ionomer cements and increased pulpal sensitivity when manufacturers’ recommendations were followed.
a. Trueb. False
Answer: A If post-cementation sensitivity is a concern, the dentist should evaluate their
technique, especially to avoid desiccation of the prepared dentin surface. Use ZOE with EBA, Zinc polycarboxylate or resin modified glass ionomer, which
have been reported to exhibit less post-cementation sensitivity. Avoid zinc phosphate , which cavity varnish may be necessary to decrease pulp
38. Which of the following are true regarding die spacers?
1. No relief space is necessary when pouring dies with Type IV stone with gypsum hardener due to the percentage of dimensional change caused by hygroscopic expansion.
2. The most common die spacers are epoxy die resin.3. One may substitute proprietary paint-on liquids, such as model paint,
colored nail polish, or thermoplastic polymers dissolved in volatile solvents.
4. Die spacers are placed to within 1.0 mm of the preparation finish line to provide relief for the luting agent.
a. 1, 2, 3b. 2, 3, 4c. 1, 3, 4d. 3, 4
The correct answer is d. (3 and 4)1. Is false. To produce relief space for cement, it is common to use a die spacer with
a stone die.2. Is false. Epoxy die materials are used for fabrication of the die, not as a spacer
material. They are reliable with respect to dimensional change, but are slightly undersized.
3. Is true. One may substitute proprietary pain-on liquids, such as model paint, colored nail polish, or thermoplastic polymers dissolved in volatile solvents.
4. Is true. Die spacers are placed to within 1.0 mm of the preparation finish line to provide relief for the luting agent and to ensure complete searing of an otherwise precisely fitting casting.
39. Which of the following statements regarding the film thickness of dental luting cements includes are true?
1. ADA Specification No. 8 Type I states that film thickness be 100 um (maximum).
2. Zinc phosphate is generally the thickest of the luting agents
3. Polycarboxylate cement has one of the highest compressive strengths, but, does not meet the maximum thickness guidelines.
4. Polycarboxylate cements yields a film thickness of 25 um or less due to the action of spatulation and seating with a vibratory action to reduce the viscosity.
5. Glass ionomer luting cements are a type I cement with a particle size of 15 um or less.
a. 3 onlyb. 1 and 3c. 1 and 2d. 1, 2, 3e. 4 and 5
The correct answer is e. (4 and 5)1. is false. ADA Specification No. 8 Type I states that film thickness be 25 um
(maximum).2. is false. Zinc phosphate is generally the thinnest of the luting agents, with a
thickness of 20 um.3. is false. Polycarboxylate cement has one of the lowest compressive strengths, but,
does meet the maximum thickness guidelines with a thickness rivaling zinc phosphate (21um).
4. is true. Polycarboxylate cements appear to be much more viscous than is a comparable mix of zinc phosphate cement. As the mix is classified as pseudoplastic, it undergoes thinning at an increased shear rate. Clinically, the cement yields a film thickness of 25 um or less due to the action of spatulation and seating with a vibratory action to reduce the viscosity.
5. is true. Don’t’ confuse particle size with film thickness. GIC film thickness is more viscous than Zinc phosphate polycarboxylate cements; it has a minimum thickness of approximately 24 um.
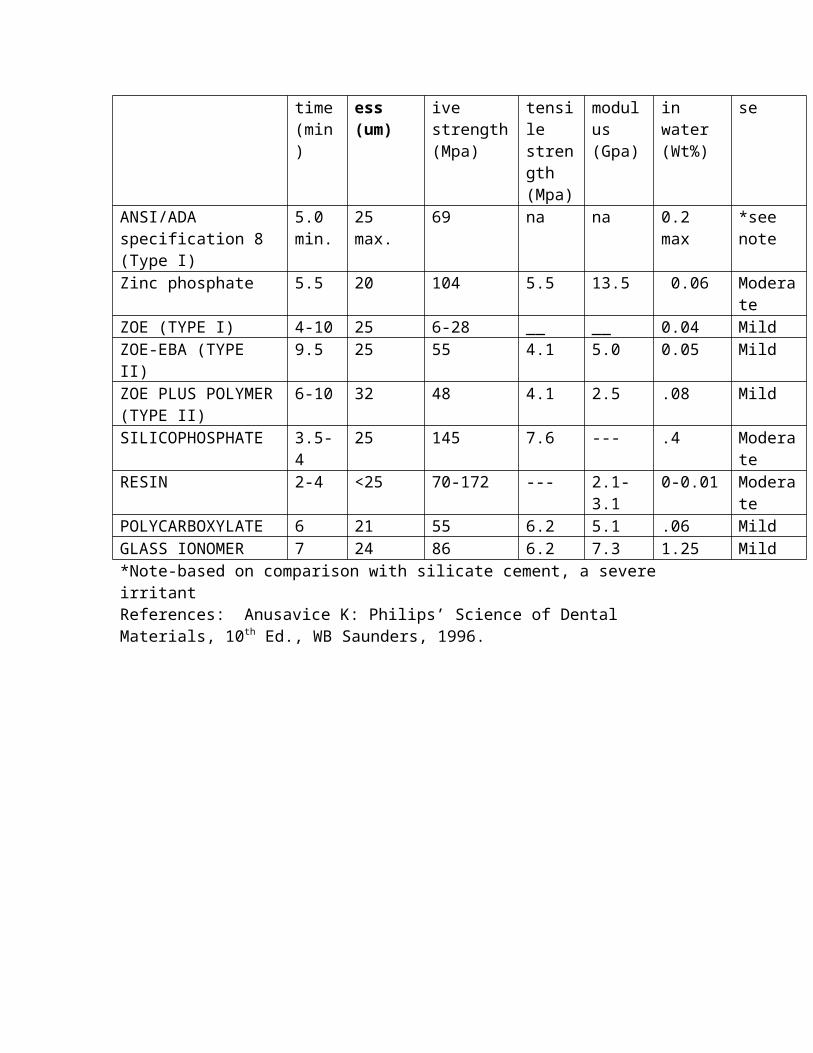
It is important to know the thickness of various cements. Note the following:Cement type Setting
SILICOPHOSPHATE 3.5-4 25 145 7.6 --- .4 ModerateRESIN 2-4 <25 70-172 --- 2.1-3.1 0-0.01 ModeratePOLYCARBOXYLATE 6 21 55 6.2 5.1 .06 MildGLASS IONOMER 7 24 86 6.2 7.3 1.25 Mild*Note-based on comparison with silicate cement, a severe irritantReferences: Anusavice K: Philips’ Science of Dental Materials, 10th Ed., WB Saunders, 1996.
40. Regarding denture impressions, which of the following are true?1. Definite pressure was advocated by many dentists as the best means for obtaining an ideal impression as it logically applied the same pressure as was being applied during chewing.2. The mucostatic technique embodies the idea that the interfacial surface tension was the best way to retain dentures3. The selective pressure concept embodies the principles of both pressure and mucostatic (nonpressure) procedures.4. In selective pressure technique, the non-stress bearing areas are recorded with the least amount of pressure in certain areas of the maxillae and mandible that are capable of withstanding the forces of occlusion.5. Low-fusing Impression waxes are not sufficiently accurate for a final impression.
a. 1 and 3b. 1, 3, 4c. 1, 2, 3, 4d. 2 and 4e. All of the above.
The correct answer is e. All of the above.1. Is true. Definite pressure was advocated by many dentists, as it presumed that the occlusal loading during the impression would be the same as occlusal loading during function. 2. Is true. The mucostatic or nonpressure technique embodies the idea that the interfacial surface tension was the best way to retain dentures. Despite many advocates, it became known that the non-pressure technique could only be obtained by sacrificing the important concepts of maximum ridge coverage and border seal.3. Is true. The selective pressure concept embodies the principles of both pressure and nonpressure procedures.4. Is true. In selective pressure technique, the non-stress bearing areas are recorded with the least amount of pressure, and selective pressure is applied to certain areas of the maxillae and mandible that are capable of withstanding the forces of occlusion. These impression area made in trays that have been selectively relieved, therefore providing more space in some areas while at the same time having areas within the tray that have less space. The places that have less space or relief will transit more pressure during the impression. Ideally, this will then distribute a greater force during function to a more favorable part of the ridge/bone (such as the buccal shelf) and less pressure to unfavorable parts (such as sharp ridge crests or bony spicules). Clinical evidence favors the selective pressure technique. 5. Is true. Low-fusing Impression waxes are not sufficiently accurate for a final impression for complete dentures, but, are satisfactory as a corrective material for a small area and for border refining for a tray. Iowa wax or Type I ZnOE can both be used to correct minor defects.References: Complete Denture Syllabus, NPDS, Bethesda
Rahn AL and Heartwell CM: Textbook of Complete Dentures, 5th Ed., Lea and Febiger, 1993.
41. Which one of the following is true regarding components of a removable partial denture?
a. Major connectors should be flexible so that functional chewing forces are properly transmitted to the teeth and other tissues.
b. A minor connector is the unit of the partial denture that connects the parts of the prosthesis located on one side of the arch with those on the other side.
c. The linguoplate can in itself serve as an indirect retainer. d. Each direct retainer and each occlusal rest are joined to the major connector
by a minor connector.
CORRECT ANSWER: D. is truea. is false. Rigidity of the major connector resists flexing and torque that would be otherwise be transmitted to abutment teeth or other structures as destructive forces.b. is false. A major connector is the unit of the partial denture that connects the parts of the prosthesis located on one side of the arch with those on the other side. It is the unit of the RPD which other all other parts are directly or indirectly attached.c. is false. The linguoplate should be something that is added to, and not something that replaces the conventional lingual bar. The linguoplate and the continuous bar retainer should ideally have a terminal rest at each end regardless of the need for indirect retention. Indications for a linguoplate are:
1. when the lingual frenum is high or the space available for a lingual bar is limited.
2. in class I situations in which the residual ridges have undergone excessive vertical resorption.
3. for stabilizing periodontally weakened teeth.4. when the future replacement of one or more incisor teeth will be facilitated by
the addition of retention loops to an existing linguoplate. There are six types of mandibular major connectors. These include: lingual bar, sublingual bar, lingual bar with cingulum bar (continuous bar) retainer, cingulum bar, Linguoplate and labial bar. There are four basic types of maxillary major connectors. These include: single palatal bar, single palatal strap (U-shaped palatal connector), anterior-posterior palatal bars, combination anterior and posterior palatal strap-type connector.
Components of a typical removable partial denture include major connector, minor connectors, rests, direct retainers, stabilizing or reciprocal components (these serve as parts of a direct retainer assembly), indirect retainers (if the prosthesis has one of more distal extension bases), and one or more bases (each one supports one or more teeth).Minor connectors arise from the major connector, and unites the major connector with other parts of the denture. The minor connector may be continuous with some other part of the denture. An occlusal rest at one end of a linguoplate is actually the terminus of a minor connector, even thought that minor connector is continuous with the linguoplate. Also, the portion of a denture base frame that supports the clasp and the occlusal rest is a minor connector, joining the major connector with the clasp.
The portions of the framework by which the denture bases are attached are minor connectors. The minor connector serves two purposes, which are diametric in function. The first is to transfer functional stress to the abutment teeth.Occlusal forces applied to the artificial teeth are transmitted through the base to the underlying ridge tissues if that base if primarily tissue supported. Occlusal forces applied to the artificial teeth are also applied to the abutment teeth through occlusal rests. This is called prosthesis-to-abutment function of the minor connector. The second is to transfer the effect of the retainers, rests, and stabilizing components to the rest of the denture. This is abutment-to-prosthesis function of the minor connector. References: McGinvney and Castleberry: Mc Cracken’s Removable Partial Prosthodontics, 9th Ed., Mosby 1995.
42. Which of the following factors concerning retention and resistance for single unit crowns are false?
a. Over tapering of the opposing axial walls can be corrected if a band of several millimeters of tooth structure can be prepared circumferentially with a restricted taper of approximately 6 degrees.
b. As taper increases, the free movement of the restoration will do so likewise, and reduce the retention.
c. Molar crowns are more retentive than premolar crowns of similar taper.d. Typical placement for grooves in a single unit are mesial and distal.e. A 7/8 crown with grooves has more retention than a complete crown with no
grooves.
E is the correct answer. It is false statementa. Is a true statement. Over tapering of the opposing axial walls can be corrected if a
band of several millimeters of tooth structure can be prepared circumferentially with a restricted taper of approximately 6 degrees. It is probably unnecessary to further modify the preparation to compensate for the areas of excessive reduction in the occlusal third. If this is not the case, one can used an approach slightly less conservative of tooth structure such as uprighting overtapered axial walls to obtain the mechanical advantage of increased retention or using grooves, boxes, or pinholes as needed.
b. Is a true statement. Theoretically, maximum retention is obtained if a tooth preparation has parallel walls, but, a slight convergence, or taper, is necessary in the completed preparation. As long as this taper is small, the movement of the cemented restoration will be effectively retained by the preparation and will have what is known as a limited path of withdrawal. As taper increases, the free movement of the restoration will do so likewise, and reduce the retention.
c. Is a true statement. Crowns with long axial walls are more retentive than those with short axial walls. Molar crowns are more retentive than premolar crowns of similar taper.Additional information: The factors influencing the resistance of cemented restorations include luting agents of the following in order of decreasing resistance: adhesive resin, glass ionomer, zinc phosphate, polycarboxylate, zinc oxide-eugenol
d. Is a true statement. In a short or excessively tapered complete crown, resistance form is minimal because most of the buccal wall is missing. A mesiodistal groove should be placed to increase resistance form.
A 7/8 crown with grooves has less retention than a complete crown with no grooves. According to a study by Potts RG et al: J Pros Dent 43:303, 1980. The removal force for a complete crown with no grooves was 1080 N versus the 7/8 crown with grooves which required only 507 N of removal force.
References: Rosenthiel, Land and Fujimoto: Contemporary Fixed Prosthodontics, Third Ed., Mosby, 2001.Potts RG et al: J Pros Dent 43:303, 1980.
43. Which of the following are incorrect for gypsum products?1. The smaller the water: powder ratio of the original investment water
mixture, the less the hygroscopic setting expansion.2. As the mixing time is reduced, the hygroscopic expansion is decreased.3. The greatest amount of hygroscopic setting expansion is observed if the
immersion takes place after the initial set. 4. The longer the immersion of the investment in the water bath is delayed
beyond the time of the initial set of the investment; the lower is the hygroscopic expansion.
5. A mixture of silica and gypsum hemihydrate results in setting expansion greater than that of the gypsum product when it is used alone.
a. 1 onlyb. 1 and 2 c. 1 and 3 d. 3 and 4e. 5 only
The correct answer is c. 1 and 3.1. Is false. The smaller the water: powder ratio of the original investment water
mixture, the greater the hygroscopic setting expansion.2. Is true. In general, the less the W:P ratio and the longer the mixing time within
practical limits, the greater is the setting expansion. 3. Is false. The greatest amount of hygroscopic setting expansion is observed if the
immersion takes place before the initial set. 4. Is true. The longer the immersion of the investment in the water bath is delayed
beyond the time of the initial set of the investment, the lower is the hygroscopic expansion.
5. Is true.References: Anusavice K: Philips’ Science of Dental Materials, 10th Ed., WB Saunders, 1996.
PERIO
1). Which of the following statements concerning the classification of periodontal disease and conditions are true:
1. Gingival diseases are classified into either dental plaque induced or non-plaque induced.
2. The plaque-induced diseases can be modified by systemic factors, medications and malnutrition.
3. Periodontic-Endodontic lesions are not in the new classification system.4. Characteristics common to all gingival diseases include non-reversibility
of the disease by removing the etiology and precursor to attachment loss around teeth.
5. Non-plaque induced disease may be affected by specific microorganisms, genetic origin, systemic diseases, and traumatic lesions.
Answer is e. 1, 2 & 5 are correct. Previous classification (1989) did not include a section on gingival diseases. In this classification, gingival diseases are classified into either dental plaque induced or non-plaque induced. Non-plaque induced includes a wide range of disorder that effect the gingiva.3 is false: Periodontic-Endodontic lesions are an additional category in the new classification system.4 is false: Characteristics common to all gingival diseases include reversibility of the disease by removing the etiology and precursor to attachment loss around teeth.
REF: Armitage, G.: Development of a Classification System for Periodontal diseases and Conditions. Ann Periodontal 4: 1-6, 1999
2). What perio procedures are SBE prophylaxis required for?
1. Periodontal procedures including surgery, scaling and root planning, probing and recall maintenance.
2. Dental implant placement.3. Sub gingival placement of antibiotic fibers or strips.4. Prophylactic cleaning of teeth or implants where bleeding is anticipated.
a) 1b) 1, 2c) 1, 2, 3d) 1, 2, 3, 4
Answer: d. All perio procedures require SBE prophylaxis except when bleeding is not anticipated, or suture removal.
REF: Dajani AS, Taubert KA, Wilson W, et al “Preventation of bacterial Endocarditis. Recommendations by the AHA,” JAMA, 1997, 277(22): 1794-801
3). If the color band of the PSR probe completely disappears in the periodontal pocket:
a) Indicates that PD is less than 5.5mm.b) PSR Code for this sextant is 3.c) Comprehensive periodontal examination and charting of the effected sextant
to determine the necessary treatment plan. d) Comprehensive full mouth periodontal examination, charting and treatment
planning are needed.
The color band of the PSR probe is 3.5 to 5.5 mm. If the color band of the PSR probe completely disappears in the periodontal pocket indicates that PD is more than 5.5mm.PSR Code for this sextant is 4.Comprehensive periodontal examination and charting of the effected sextant to determine the necessary treatment plan is indicated for code 3 (color band of the PSR probe is partially submerged).The correct answer is (d): Comprehensive full mouth periodontal examination, charting and treatment planning are needed for code 4 patient and two or more quadrant with code 3 patient.
4). PSR (Periodontal Screening and Recording System) is recorded by which of the following?
1. Code 0 indicates there is no bleeding, no calculus, no defective margins, and the colored band remains completely visible. Gingival tissue is healthy and only preventive care is required.
2. Code 1 indicates the color band is completely visible with minor bleeding detected but no calculus is present and there are no defective margins. Subgingval plaque removal and oral hygiene instructions are indicated.
3. Code 2 the color band is partially submerged with bleeding, supra or sub gingival calculus and/or defective margins are present. Treatment includes the removal of plaque and calculus, defective margins, and oral hygiene instructions.
4. Code 3 The colored band is partially submerged. This indicates that the sextant needs a comprehensive periodontal evaluation. If two or more sextants are code 3 than a complete comprehensive evaluation and charting is necessary.
5. Code 4 The colored band is completely covered indicating a depth greater that 6.5 mm. Full mouth charting and treatment planning are required.
a) All of the above are accurate statements.b) 1, 2, 3, and 4.c) 1, 2, and 4.d) 1 and 5
The correct answer is c.The PSR system uses especially designed probe that has a 0.5 mm ball tip and is colored coded from 3.5 to 5.5 mm. The patient’s mouth is divided into six sextants. At least six areas are examined around each tooth. The deepest finding in each sextant is recorded.Code 2 is incorrect only because the colored band is still fully visible.Code 4 is not correct since the colored band indicates a depth greater than 5.5 mm. Code * : An * after a number indicates that there is one of the following conditions: furcation involvement, tooth mobility, mucogingival problem, or gingival recession extending to the colored band (3.5 mm or greater).
1. Actisite contains tetracycline2. Periostat conatins doxycycline3. Periochip contains minocycline HCl4. Arsestin contains chlorohexidine5. Atridox is a doxycycline gel.
a. 2,3,5b. 3,4c. 2,3,4d. 1,4
Answer: (b). Statement 1 is true. Actisite is a 23cm monofilament of ethylene vinyl acetate impregnated with 12.7mg (0.5mg/cm) of tetracycline. When placed in the pocket for ten days it reaches 100 times the peak levels achieved with systemic oral administration. Indications are sites that fail to respond to conventional therapy.Statement 2 is true. It is a prescription capsule used in conjunction with scaling and root planning. It is a unique form of doxycycline (20 mg caps). It uses the collagenalytic (collagenase inhibitors) properties of tetracycline while limiting bacterial resistance.Statement 3 is not accurate. The Periochip is a 4X5 mm firm gelatin strip impregnated with chlorhexadine. It is inserted into pockets 5mm or greater. It is used as a supplement to scaling and root planning.Statement 4 is not accurate. Arestin contains minocycline HCL (1mg). Microspheres containing the drug are inserted into the pocket. It is used as an adjunct to scaling and root planning. The microspheres are a polymer material that is bioadhesive, bioresorbable. Once inserted it adheres to the periodontal pocket. The drug is slowly released by diffusion form the spheres to the pocket. Arestin maintains therapeutic drug levels for at least 14 days. Statement 5 is correct. It is a gel that solidifies in the pocket and releases tetracycline over a seven day period
Information from a lecture by LT Micheal Cabassa, The Role of Pharmacotherapeutics in Periodontal Therapy, October 2002, Naval Postgraduate Dental School
6). Which of the following statements are correct?
1 Supra gingival plaques contain mainly coccoid and filamentous forms of bacteria.
2 “Corncob” which is filamentous forms of bacteria covered with coccal organisms are present in supragingival plaque.
3 Bacterial cells are densely packed the tooth surface in supragingival plaque4 Subgingival plaque is less organized than supragingival plaque. 5 Numerous spirochetes, gram negative bacteria, and bacteria grouped in
“bottle brush” formations are present in subgingival plaque.
a) 1,2, and 3b) 1,2,3, and 4c) 1 and 3d) All of the above
All of the above are correct. Supragingival plaque is densely packed on the tooth surface about 0.5mm thick or more. Flagellated forms and spirochetes are observed apically and on the outer surface of the supragingival plaque.Subgingival plaque has an outer and inner layer. The inner layer is tightly adherent but is thinner than and not as organized as supraginigal plaque. The outer layer adjacent to the soft tissue is loosely adherent layer. It is composed of the organisms in answer 5.Formation of the dental pellicle is the initial stage of plaque formation. All surfaces of the oral cavity are covered with a glycoprotein. The mechanisms of pellicle formation are electrostatic, Van der Waals forces and hydrophobic forces. Within a few hours bacteria is found on the dental pellicle. The initial bacteria are gram-positive facultative bacteria such as Actinomyces viscosus and Streptococcus sanguis. The initial bacteria adhere to the pellicle by adhesions and fimbriae on the surface of the bacteria. As the plaque matures the bacteria become more gram-negative anaerobic organisms. Secondary colonization of bacteria that do not initially colonize clean tooth surfaces occurs. Coaggreagation is the term to describe different species of bacteria adhering to one another in mature plaque.
The Periodontic Syllabus, Third Edtion. Page 15Clinical Periodontology, 8th Edition Page 86-88
7). Which feature is not found in the implant – soft tissue interface?
a) Sulcular epitheliumb) Hemidesmosomesc) Sharpey’s fibersd) Basal Laminae) Glycoprotein insertion
Answer: (c) No Sharpey’s fibers attachment to implant abutment.
How do fibers form at implant interface?Architecture:- Peri-implant free gingiva corresponds to teeth.- Sulcular epithelium forms peri-implant gingival crevice.- Implant junctional epithelium.- Basal cell layer with hemidesmosomal attachment to the abutment.- Hemidesmosomes have lamina densa (at abutment surface) and lamina lucida.- Surface oxide layer and hemidesmosomal glycoprotein may form a chemical bond attachment.- Not chemically strong, separated with 20-25 grams of pulling force.- Deep within the sulcus, collagen fibers form a tight cuff around the abutment. Some of these fibers run perpendicular to the abutment, others circumferentially. Thus mature collagen “seal” at the bone level may provide contact inhibition to prevent epithelial down growth.
Ref: Bauman G, Rapley J, Hallmon W, Mills M. The Peri-Implant Sulcus. Int J Oral Maxillofacial Implants 1993;8:273-280.
8). What is the order of expected prognosis for treated furcation involved molar teeth from worst to best?
a) Mn 1st, Mn 2nd, Max 1st, Max 2nd
b) Max 2nd, Max 1st, Mn 2nd, Mn 1st
c) Max 1st, Mn 2nd, Max 2nd, Mn 1st
d) None of the above
Answer: (b) Max 2nd, Max 1st, Mn 2nd, Mn 1st
Maxillary molars have worse prognosis than mandibular. Second molars have worse prognosis than first molars.Glickman I – feel fluting, not roofGlickman II – engage roofGlickman III – Probe goes through furcationGlickman IV – Can see through furcation Furcation treatment options:- Non surgical- Regenerative- Resective- ExtractionUnder regenerative option:- Flap curettage- Osseous grafts - Guided tissue regeneration for I and IIMax 2,3rd molars lost most frequently.Maxillary premolars with furcation involvement have a poor to hopeless prognosis.
The diagnosis and treatment of molar furcation invasions. Newell, D.H., Dental Clinics of North America Vol 42 (2) 1998A long-term survey of tooth loss in 600 treated periodontal patients. Hirschfeld, L. and Wasserman, B. J Perio 49: 225, 1978
9.WHAT MAKES A PERSON SUSCEPTIBLE (IMMUNOLOGICALLY) TO RAPIDLY PROGRESSING PERIODONTAL DISEASE?
Rapidly Progressing Periodontal Disease is characterized by which of the following?1. progresses 3-4 times faster than adult periodontitis 2. affects lower incisors and first molars with vertical osseous defects 3. bone loss is inconsistent with the amount of local factors present 4. a gram negative obligate anaerobic cocci is considered a primary etiologic
microorganism a. 1,2,4b. 2,3,4c. 1,2,3d. 1,3,4e. all of the aboveThe correct answer is C- 1,2 3 are true
Definition of RPP: a disease of the periodontium that occurs in an otherwise healthy adolescent, characterized by rapid loss of alveolar bone, lack of severe clinical signs of inflammation, and sparse plaque accumulation. Destruction is not commensurate with local factors.Characteristics of RPP:
Onset around puberty (11-15 years of age)Isolated areas of attachment loss and bone loss
(greater at permanent incisors and 1st molars)Evidence of local, specific bacterial causes
Actinobacillus actinomycetemcomitans, CapnocytophagaRod gram - negative obligate anaerobe, found at the base of pocket
Neutrophil dysfunction is a common featureFamilial distribution of the disease, and there is no identified systemic disease.
PF Fedi et al The Periodontic Syllabus, 4th Ed pp 34-35.
10). Several factors predispose diabetics to periodontitis. Which are correct?1. elevated glucose levels in oral fluids can influence microbial flora2. impaired erythrocyte function, including phagocytosis may reduce resistance
to periodontitis3. altered collagen metabolites and vascular changes including stasis4. impaired chemotactic and phagocytic activity of polymorphonuclear
leukocytes a. 1,2,3 b. 1,3,4 c. 2,3,4 d. 3,4 e. all the above
Answer: (b) The glucose content of gingival fluid and blood was found to be higher in diabetics. Thickening of the basement membrane of capillaries may hamper the transport of nutrients. The increased susceptibility of diabetics to infection has been hypothesized as being due to PMN deficiencies resulting in impaired chemotaxis, defective phagocytosis, or impaired adherence.
Glickman’s Clinical Periodontogy 6th ed. pp. 464-465
11). All of the following have shown some clinical correlation with periodontitis except:
Answer: (c). Ample evidence has shown a relationship of periodontal health as an important component in management of some systemic diseases. A relationship is suggested between acute systemic infections and the occurrence of cardiovascular disease that includes myocardial infarction and stroke. Low birth weight babies- believed to occur because accumulation of gram(-) micro organisms such as those found in periodontitis results in increased release of prostaglandin and cytokines which may act on distant sites such as the placenta. Severe Periodontitis is associated with upper and lower respiratory disease such as hospital acquired pneumonia.
REFERENCE: Fedi Perio Syllabus 4th edition 2000 pg.29 and 90.
12). Concerning grafts which of the following are TRUE.1. Osteoinductive is where the graft acts as a template for bone formation.2. Osteogenesis is where the graft stimulates new bone formation.3. Small particle size of 300 to 500 microns is advantageous.4. Osteoconductive is where the cells of the graft actually produce new bone.5. Cortical bone is the best source of pluripotential osteogenic cells.5. Adequate vascularity is needed (intramarrow penetration with a ½ round bur).6. A mechanically stable wound site-primary flap closure and circumferential seal is necessary.8. Emdogain is enamel matrix proteins obtained from pigs.
a) all are trueb) 1,3,6,7 are truec) 1,2,3,4 are trued) 3,6,7,8 are truee) 4,5,6,8 are true
A. Answer: (d) OSTEOCONDUCTIVE- the graft acts as a template or trellis to assist in bone formation and deposition.OSTEOINDUCTIVE- The graft acts to stimulate or induce new bone formation by undifferentiated cells.OSTEOGENESIS- The cells of the graft actually produce new bone.The smaller size of particles are easier for the body to resorb and more actively induce regeneration in osseous defects. Cancellous bone is the best source of pluripotential osteogenic cells. Adequate vascularity is needed and intramarrow penetration with a ½ round bur can be used to aid in a bleeding bed. A mechanically stable wound site with primary flap closure and circumferential seal is important to keep bacterial contaminants from the wound site and to aid in the bone graft material to not wash out. Emdogain is enamel matrix proteins obtained from pigs- it seems to encourage the formation of acellular cementum that is then followed by associated bone deposition.
REFERENCE: Perio Syllabus 4th edition p. 168-172.
13). The hemiseptal defect is:
a) A one-wall defect with one proximal wallb) A one-wall defect with one linguopalatal wallc) A one wall defect with one buccolabial walld) A two walled defect with two proximal walls
Answer: (a) A one-wall defect presents with either one proximal wall (hemiseptal) or one linguopalatal or buccolabial wall. These defects are generally not amenable to regenerative theraputic approaches. Resective therapy, with the goal of creating a physiologic osseous architecture, will provide a more predictable and stable long-term result.Two-wall defects are bordered by either two proximal walls, a buccal/labial and proximal wall or a buccal/labial and a lingual wall. A two-wall defect consisting of a buccal/labial and a lingual/palatal wall is commonly referred to as an interdental or osseous crater. The adjacent teeth are the other two walls of the defect. According to a study by Manson and Nickolson, the interdental crater constitutes approximately one third of all intrabony defects and as many as two thirds of all mandibular defects.Three-wall intrabony defects are characterized as having three osseous walls; the tooth surface constitutes the fourth wall. These defects may be localized to one proximal or midradicular surface, or may be circumferental, involving two or more root surfaces. The typical clinical encounter is with a combination defect which combines two or more of the above.
Periodontal Therapy, Nevins and Mellonig, pp175,176
14). Which of the following statements are true regarding attachment levels and uprighting molars?
a. Pockets mesial to uprighted molars are shallower than pockets mesial to control teeth that have not been uprighted.
b. Gingival inflammation does not differ from that around control teeth.c. Trauma from occlusion with subsequent bone loss will occur with
uprighted molars if selective equilibration is not performed.d. All of the above
Answer: da. This is due to a reduction in soft tissue height while the bone height remains
Unchanged.b. Same bugs, etiologyc. Vertical loading results from moving the tooth’s occlusal surface toward the
hinge. Selective equilibration and possible coronal restorations should be included in every treatment plan with a molar uprighting component.
15). What is the most significant challenge regarding anterior implants?
a. Difficulty in being able to use a fixture with adequately large enough diameter due to lack of bone.
b. Securing the proper angulation of the fixturec. Getting an esthetically acceptable shade with a single tooth anterior
implant.d. Avoiding the “black triangle” in the papilla area due to lack of bony
support to the gingival contours.
Answer: (d) Although a, b, and c are considerable challenges, the most challenging periodontal aspect is acceptable esthetic gingival contours due to a difference in crestal bone height between the implant and the adjacent natural tooth. GBR and connective tissue grafts are two treatments to correct this.
B.C. CAPT John Mumford, USN, DC
16). Which of the following statements regarding Guided Tissue Regenerations are true?1. Many teeth previously regarded as hopeless are salvageable via GTR using ePTFE2. Class II furcation involvements, large three-walled infrabony defects, and osseous
craters are predictably treatable with Gore Tex GTR3. Routine uses of Gore Tex include two-walled defects and horizontal bone loss that
may have been previously considered not salvageable4. EPTFE titanium is used in wide deep infrabony defects and are best treated with a
prerequisite adequate band of attached gingiva5. Teeth that are amenable to Gore Tex membrane GTR include multirooted teeth
with root proximity of greater than 1 mm6. Gore-Tex regenerative membranes can be placed in transgingival and submerged
configurations a. 4 onlyb. 4 and 5 onlyc. 4, 5, 6d. 2, 3, 4, 5, 6e. 1, 2, 4, 6
Answer: (e) Today, many teeth previously regarded as hopeless are treatable via GTR. This includes the Class II furcations, large three walled infrabony defects and osseous craters. Therefore, 1 and 2 are both true. 3 The first statement is true and the second statement is false. Horizontal bone loss is not amenable to GTR. If the interdental space is wide, the surgical procedure of choice is the modified papilla preservation technique. The interdental papilla is horizontally dissected at its base on the buccal side and elevated with a palatal full-thickness flap. After membranes positioning, the papilla is repositioned though the interdental space to cover the barrier and possibly sutured to the buccal flap to obtain primary closure. If the interdental space is narrow, the simplified papilla preservations technique should be used. The interdental papilla is obliquely dissected to augment the connectible tissue surface for the subsequent primary closure of the lap over the barrier membrane. Anatomic prerequisites for an uneventful procedure include the presence of adequate band of attached gingiva and absence of frena in the area of treatment. 5 is false; the root proximity must be greater than 2 mm to be successful; in shallow defects (<2mm) between the roots of the adjacent teeth, little to no regeneration may be obtained; analysis of the local site must be done to determine if a tooth is treatable; positive findings include:
1. adequate separation (>2mm) for access and to maintain collar.2. an anatomy of the affected dental surface that allows good adaptation of the membrane and closure of the defect,
3. a good quantity of healthy periodontium remaining close to the defect and a thick periodontium and adulated vestibulum to allow for flap stability
6 is true-titanium reinforced Gore-Tex regenerative membranes can be placed in transgingival and submerged configurations allowing extension through the gingiva or where the defect can be completely isolated.
Nobel Biocare Gore Regenerative Materials Product Configuration Information; Critical Decisions in Periodontology by Hall, 4th Ed. Chapters 37, 86, 87, 88, 89; Manual of Clinical Periodontics-Reference manual by Lexi-Comp
17). Page and Schroeder described several phases in the pathogenesis of periodontology; which one the statements is true?
1. The initial lesion is described as a classic chronic exudative vasculitis.2. Within 4 to 10 days, the early lesion develops. It is characterized by a dense
infiltrate of PMNs, pathologic alteration of fibroblasts, and an increase of the connective tissue substance
3. The established lesion develops within 2 to 3 months and is distinguished by a predominance of plasma cells and early horizontal bone loss.
4. In the advanced lesion, plasma cells continue to predominate although loss of the alveolar bone and periodontal ligament, and disruption of the tissue architecture with fibrosis are also important characteristics.
a. 1 is correctb. 2 is correctc. 3 is correctd. 4 is correct
Answer: (d)1. False. The gingival tissues respond within 2 to 4 days to a beginning
accumulation of microbial plaque with a classic acute exudative vasculitis which we have termed the initial lesion.
2. False. Within 4 to 10 days, the early lesion develops. This stage is characterized by a dense infiltrate of lymphocytes and other mononuclear cells, pathologic alteration of fibroblasts, and continuing loss of the connective tissue substance. The structural features of the early lesion are consistent with those expected in some form of cellular hypersensitivity, and a mechanism of this kind may be important in the pathogenesis.
3. False. The early lesion is followed by the established lesion which develops within 2 to 3 weeks and is distinguished by a predominance of plasma cells in the absence of significant bone loss. The established lesion, which is extremely widespread in humans and in animals, may remain stable for years or decades, or it may become converted into a progressive destructive lesion. Factors causing this conversion are not understood.
4. True. In the advanced lesion, plasma cells continue to predominate although loss of the alveolar bone and periodontal ligament, and disruption of the tissue architecture with fibrosis are also important characteristics. The initial, early, and established lesions are sequential stages in gingivitis and they, rather than the advanced lesion which is manifest clinically as periodontitis, make up the major portion of inflammatory gingival and periodontal disease in humans.
Lab Invest. 1976 Mar;34(3):235-49.Pathogenesis of inflammatory periodontal disease. A summary of current work. Page RC, Schroeder HE.
18). Surgical management of implant repair includes all but which of the following?
1. Retreatment of ailing and failing implants depends on an accurate diagnosis and effective nonsurgical intervention to stabilize or arrest progression of an active perimplant lesion
2. If mucogingival defects exist only around the ailing or failing implant, subsequent osseous surgery may not be needed if soft tissue augmentation is successfully performed
3. The goals of perimplant surgical therapies are to reestablish a healthy perimucosal seal and regenerate a soft or hard tissue attachment to the implant.
4. Regenerative procedures, including bone grafting with mandatory GTR, are most appropriate when the adjacent osseous crest is close to the rim of the implant in one-walled defects
5. Detoxification procedures are recommended to treat the infected implant surfaces before regenerative modalities. This may include removal of rough or pitted HA coatings on the surface of the implant fixture.
a. 1 is falseb. 2 is falsec. 3 is falsed. 4 is falsee. 5 is false
Answer: (d)1. is true2. is true; if indicated, osseous repair surgery on keratinized tissues is less
technically demanding.3. is true; this requires a definitive diagnosis, comprehensive therapy, and effective
maintenance.4. false; bone grafting may include GTR for the ailing or failing implant;
regenerative procedures, including bone grafting with or without GTR are most appropriate when the adjacent osseous crest is close to the rim of the implant in narrow two- or three- walled moat, dehiscence or fenestration defects.
5. true; a 30 second to 1 minute application of a supersaturated solution of citric acid (pH1) burnished with a cotton pledget may be beneficial in detoxifying the infected hydroxyapatite-coated implant surface. If the coating is rough or pitted, ultrasonic or air/powder abrasives is necessary to remove the HA. Then a short application of the air/powder abrasive detoxifies the surface of the Ti implant
Critical Decisions in Periodontology by Hall, 4th Ed. Chapters pp260-261
19). Callous formation forms during the fibroplasia stage of extraction site wound healing.
a. Trueb. False
Answer: (b) Four stages of wound healing: inflammation, epithelialization, fibroplasia, and remodeling.Immediately the socket fills with blood, which coagulates and seals bone from air.Inflammatory - week 1: WBCs remove bacteria and break down debrisFibroplasia occurs along with Epithelialization – week 1 to 3: Fibroplasia consists of the ingrowth of fibroblasts and capillaries. Osteoclasts accumulate along the lamina dura. Granulation tissue develops and an osteoid material is laid down starting at the socket wall. Epithelialization consists of the migration of gingival/mucosa from the boarders of the wound into the socket and over the granulation tissue. The duration is dependent on how large the secondary healing site is, but usually complete be week 3 or 4Remodeling starts from week 5 to 6 months. Osteoclasts resorb the cortical bone lining the socket, and together with osteoblasts reorganize the haphazard pattern laid down earlier into regular bone with the reestablishment Haversian canal systems. As bone fills the socket, the epithelial covering is raised to a level that roughly equates to the surrounding tissues.Callous formation only occurs when medulary bone is forced to heal by secondary intention as in a fractured long bone where the ends are not approximated. Fibroblasts and osteoblasts quickly produce so much fibrous matrix, the healing tissue extends circumferentially beyond the free ends of bone. Peterson, Ellis, Hupp, Tucker, Contemporary Oral and Maxillofacial Surgery. Mosby 1998, pages 163-166
Myron Nevins, James Mellonig, Periodontal Therapy: Clinical Approaches and Evidence of Success. Quintessence Books. Page 242
20). Read both parts, choose the best answer for each and make your selection below.
PART A: What is the most common antitarter ingredient in toothpaste?
Part B: In regards to the above, what is the mode of action?
1. Affects polyglycans of bacteria which prevents plaque formation thus reducing tartar 2. Inhibits crystalline matrix formation preventing mineralization 3. Forms a coating on the tooth surface that inhibits calcification build -up4. Prevents minerals from precipitating out of the saliva
a) 1/4b) 2/1c) 3/2d) 4/3
Answers: (b) Anti-Tartar Products: One of the first products to venture beyond fluoride was tartar control toothpaste. The major anti-calculus strategy developed by researchers in the 1970s was to inhibit crystal growth, thus preventing the mineralization of developing plaque and the transition of the plaque into calculus. The most effective agents in vitro were the pyrophosphate s , but in the oral cavity these were rapidly broken down by bacterial and salivary pyrophosphatase enzymes. In the 1980s, formulations were created using high concentrations of pyrophosphates (and other polyphosphate salts) that could be combined with sodium fluoride to both reduce tartar buildup (not preformed tartar) and retain anti-caries potency. The concentration of sodium fluoride was high enough to serve as an anti-enzyme and help inhibit the limiting pyrophosphatase enzymes in the mouth.(Other anti-tartar formulations have not applied for nor received the ADA Seal. One such product, a toothpaste containing Citroxain -- a mixture of the enzyme papain, sodium citrate and alumina -- has some supporting published data and is marketed primarily as a whitening toothpaste.)Mandel ID, Calculus update: Prevalence, pathogenicity and prevention. J Am Dent Assoc 126:573-80, 1995.
Tetrapotassium Pyrophosphate, Inhibits crystalline matrixThe addition of 1 percent of a copolymer of methoxy-ethylene and maleic acid (Gantrez, GAF Corp.) appears to improve the effectiveness of some anti-tartar products.
Schiff TG, Comparative clinical study of two anti-calculus dentifrices. Compend Cont Educ Dent (Suppl 8):S275-7, 1987.
The tartar control products that have received the ADA Seal have been shown in appropriately designed clinical studies to be effective decay preventives as well as to significantly reduce the formation of tartar above the gum line. A caveat is included on the label that such products have not been shown to have a therapeutic effect on periodontal disease. The anti-tartar ingredients are considered by both the ADA and FDA to be primarily cosmetic, not therapeutic. They do not affect the already hardened deposits.
Tartar control dentifrice containing 7.0% sodium hexametaphosphate (5% hexametaphosphate anion) Has been shown to demonstrate anti-tartar properties, but it is new, not approve and only one dentifrice lists it in it’s ingredients
A 0.5 percent zinc citrate combined with 0.2 percent triclosan – is an effective anti-bacterial agent;5 triclosan and the polymer Gantrez;7 and pyrophosphate and triclosan.8 The triclosan/Gantrez combination is part of a multibenefit product that has been approved by the ADA and FDA and is awaiting marketing in the United States.
Total brand toothpaste is essentially a sodium fluoride dentifrice containing the broad-spectrum antibacterial agent triclosan (0.3 percent) and the copolymer PVM/MA (polyvinyl methyl ether malic acid), also marketed under the trade name Gantrez (2 percent). Triclosan has been used in soaps and deodorants for more than 20 years. Its broad spectrum of activity encompasses a large range of oral bacteria, and it is compatible with other ingredients in oral products. The combination of triclosan and PVM/MA inhibits crystal growth and is effective as an antitartar agent, but not the most common.
Fairbrother KJ, Kowolik MJ et al, The comparative clinical efficacy of pyrophosphate/triclosan, copolymer/triclosan and zinc citrate triclosan dentifrices for the reduction of supragingival calculus formation. J Clin Dent 8 (Special Issue):62-6, 1997.
Common Active Ingredients: contains: Sodium Monofluorophosphate (0.14%), Zinc Citrate Trihydrate, Sodium Fluoride 0.243% (Anticavity Toothpaste)
Common Inactive Ingredients: , Tetrasodium Pyrophosphate, Sodium Lauroyl Sarcosinate, Flavor, Sodium Saccharin, Cellulose Gum, Sodium Lauryl Sulfate, Titanium Dioxide, FD&C Blue #1, FD&C Yellow #5 Sorbitol, Water, Hydrated Silica, Sodium Gluconate, Stannous Chloride, Flavor, Sodium Carrageenan, Hydroxyethylcellulose, Sodium Saccharin, Sodium Hydroxide, Glycerin, Sorbitol, Hydrated Silica, Sodium Bicarbonate, Propylene Glycol, Water, Pentasodium Triphosphate, Tetrapotassium Pyrophosphate, Sodium Hydroxide, Calcium Peroxide,FD&C Green #3Pentasodium triphosphate acts as a preservative and an unproven remineralization aid.
PEDO/ORTHO/PUBLIC HEALTH/RAD
1. Which of the following are true regarding tooth eruption pattern?
1. The first permanent premolars replace the primary molars.2. The maxillary succedaneous incisors usually erupt before the mandibular
incisors.3. The most favorable eruption sequence for primary teeth in either arch is
ABDCE (using Palmar notation)4. The eruption sequence for the succedaneous dentition in the mandible
usually includes eruption of the canines before the premolars.5. The eruption sequence for the maxilla usually includes eruption of the
canines before the premolars.
a. 3 and 4 only are correctb. 1, 2, and 3 are correctc. 1, 3, and 4 are correctd. 2, 4, and 5 are correcte. 2, 3, and 4 are correct
PRIMARY DENTITION: ERUPTION TOOTH LETTER ERUPTION
CENTRAL A ~ 6 - 9 MONTHS
LATERAL B ~ 7 - 10 MONTHS
CANINE C ~ 18 MONTHS
1ST MOLAR D ~ 14 MONTHS
2ND MOLAR E ~ 24 MONTHS
Primary Root completion 18 months post eruption. (12-18 mos.)
Teeth erupt when the root is 2/3 complete.most favorable eruption sequence for primary teeth both Max & Man: ABDCE
Primary teeth:germs form at 6-8 wks IUenamel forms 4-6 months roots complete approx 1 yr after eruption
2. Which of the following is false regarding prevention of transmission of M. tuberculosis bacilli?
a. M tuberculosis bacilli (Mtb) transmission cannot occur via fomites.
b. Mtb are major spore forming organisms, making them exceptionally difficult to kill with conventional germicides.
c. Mtb organisms are sensitive to heat and ethylene oxide. All reusable instruments should be sterilized with heat or ethylene oxide.
d. Patients with untreated TB should have their surgery postponed until they can receive treatment for their TB.
e. Mtb organisms are sensitive to irradiation
The only mycobacterial organism of significance to most dentists is Mycobacterium tuberculosis. TB is uncommon in the US and Canada, however, immigration from SE Asia, where tuberculosis is common, brought a new reservoir of M. tuberculosis organisms. Patients who are infected with HIV are another group who may harbor tuberculosis organisms. Some newer strains of TB are resistant to drugs commonly used to treat TB.
Etiology: In the majority of cases of human TB the causative agent is M. tuberculosis, an acid fast, nonmotile, intracellular rod that is an obligate aerobe; hence, it exists best in an atmosphere of high oxygen tension. Humans are the only known reservoir. This explains why it commonly infects the pulmonary system. But, it can infect any organ of the body. Typical mode of transmission is via infected airborne droplets of mucus or saliva that
have been forcefully expelled from the lungs, usually by coughing, speaking, sneezing or singing. It is not spread by fomites (dishes, toys, clothes or linens).It can be spread through unpasturized milk.(M. bovis). Oral lesions can occur via ingestion of sputum and coughing up infected sputum thereby inoculating the oral cavity.
Diagnosis: D. “Tuberculosis infection”
Positive TB skin test, no active disease“LTBI” latent TB infection
E. “TB disease”Presence of clinical signs and symptomsMay result from primary infection or activation of latent TBHighest risk of activation in first two years after exposureDiagnosis
Dental management:Updating the patient’s medical historyRecognizing signs and symptoms of TBFollowing infection control guidelinesNeed to ascertain potential infectivity of patientsActive TB (Infectious)History of TB (Infected)Positive tuberculin test (Infected)Undiagnosed but with suggestive signs and symptoms and risk factorsPatients with clinically active TB:Emergency treatment onlyMinimized aerosolization
Use rubber damMinimize handpiece use
Treatment in hospital setting/isolations rooms-6-12 room-air exchanges per hourDirectional airflow “ negative-pressure vent”Air enters room from hallways and leaves only via outside exhaustAutomated room-pressure monitors with alarms HEPA filtration, UV radiation (germicidal)
Patients with clinically active TBO.K. to treat routinely:
After 2 weeks of anti-TB therapy and confirmed noninfectious by physicianPediatric patient under age 6Considered noninfectious since TB bacilli are rare in sputum and unable to cough up sputum
Confirm stats with pediatrician F. Patient with history of active TB
Initial cautionConsultation with physicianConfirm history of treatment , periodic physical exams, chest radiographsRelapse is rare if treat adequatelyHas patient becalm immunosuppressed since completion of treatment
G. Patients with positive skin testAsk for history of evaluation for active TB, chest RG’s, history of anti-TB drugsRoutine treatment O.K.; no special precautions
H. Patients with suggestive signs and symptomsUnexplained, persistent signs and symptoms
Defer dental treatment until after medical evaluation
Effective chemotherapy of TB is dependent on 1) patients education and compliance, 2) appropriate selection of drugs, 3) multiple drug use, and 4)drug administration continuance for a sufficient time.
Common drug regimens:Non-drug resistant TB3 drugs for 2 months (INH + rifampin + pyrazinamide), followed by 2 drugs for 4 months ( INH + rifampin)6 months total treatment timeDrug resistance4 drugs for 2 months (INH + rifampin + pyrazinamide + either ethambutol or streptomycin)Determination of resistance again: if resistant only to INH: rifampin + pyrazinamide + either ethambutol or streptomycin for 6 months or rifampin + ethambutol continued for 12 monthsImmunosuppressed patients receive treatment for a minimum of 9 monthsConfirmed multiple-drug resistance3-7 drugs (INH + rifampin + pyrazinamide + ethambutol, an aminiglycoside, or capreomycin, ciprofloxacin, or ofloxacin and either cycloserine, ethionamide, or aminosalicyclic acid)-this is continued for 12-24 months or until negative cultures are evident.The correct response is b. (it is false)
References:Petersen, Ellis, Hupp, Tucker: Oral and Maxillofacial Surgery, Mosby, 3rd Ed., 1998.Little and Falace, et. Al.: Dental Management of the medically Compromised Patient, Mosby, 6th Ed., 2002.
3. Which of the following are true regarding disadvantages of Nitrous oxide inhalation use for conscious sedation?
1. Nitrous oxide is considered to be reactive and toxic in doses greater than 60%.
2. It is a weak agent and should be titrated carefully in increments.3. Inconvenience may be a factor when the nasal mask hinders exposure of the
maxillary anterior teeth.4. Potential chronic toxicity has been shown to occur in office personnel. 5. Potentiation may occur when combined with other drugs.
a. 1 onlyb. 1 and 2 c. 2, 3 and 5d. 1, 2, 3 and 4e. 2, 3, 4 and 5
1. is false. Nitrous oxide is inert and nontoxic when administered with adequate oxygen.
2. is true. It is a weak agent with which attempts to push up the concentration can be fraught with failure when attempting to control moderately to severely anxious patients.
3. is true. Inconvenience may be a factor when the nasal mask hinders exposure of the maxillary anterior teeth. This is especially true in very small ch ildren.
4. is true. Potential chronic toxicity has been shown to occur in office personnel. Retrospective studies have shown that office personnel who were exposed to trace levels of nitrous oxide have suggested an increased incidence of spontaneous abortions, congenital malformations, certain cancers, liver disease, kidney disease, and neurological disease.
5. is true. Potentiation may occur when combined with other drugs. Although nitrous oxide is a weak and safe agent when used with oxygen, deep sedation or general anesthesia may be easily produced if it is added to the effects of other sedatives given by parenteral or other route.
4. Which of the following statements are true causes and effects regarding patient positioning in panoramic radiography?
a. Anterior positioning error: Widening and blurring of the anterior teeth images.
b. Patient placed too far posteriorly, outside of focal trough: Causes narrowing of tooth images.
c. Midsagittal plane positioning error: If patient is place asymmetrically in Panorex chin rest, images farthest from the film will be decreased in size
d. Spinal column positioning error: will result in an unexposed area in the middle inferior portion of the film.
e. Occlusal plane positioning error: Downward overangulation: This overangulation results in flattening of the occlusal plane.
Anterior positioning error: Narrowing and blurring of the anterior teeth imagesPatient placed too far posterior outside of focal trough: Causes widening of tooth images.Midsagittal plane positioning error: If patient is place asymmetrically in Panorex chin rest, images farthest from the film will be magnified, whereas images of structures closest to the film will be decreased in size. Spinal column positioning error: Will result in an unexposed area in the middle inferior portion of the film. If the spine is not kept erect, the radiation will be excessively absorbed by the spinal column, resulting in the low density area near the lower center of the film. Also, there may be superimposition of a portion of the spinal column over the neck of the condylar process of the mandible.Occlusal plane positioning error: Downward overangulation: This overangulation (the ala tragus line is greater than the proper 5 degree downward and forward) results in a severe curvature in the occlusal plane and a lack of definition of the incisors on the image.The only correct answer is d.Information about Ghost images: (should know for the Boards)A ghost image is formed what the object is located between the x-ray source and the center of rotation.
1. The ghost image has the same morphology as its real counter part.2. The ghost image appears on the opposite side of the radiograph from its
real counterpart.3. The ghost image appears higher up on the radiograph than its real
counterpart.4. The ghost image is more blurred than its real counterpart.5. The vertical component of a ghost image is more blurred than the
horizontal component.6. The vertical component of a ghost image is always larger than its real
counterpart, whereas the horizontal component of a ghost image may or may not be severely magnified.
Langlais RP, Langland OE, Nortje CJ. Diganostic Imaging of the Jaws. Willams & Wilkins. 1995Langland, Langlais, Morris. Principles and Practice or Panoramic Radiology.Saunders. 1982.
5. Neglect is defined as the inattention to the basic needs of a child, such as food, clothing, shelter, medical care, education, and supervision. Physical abuse tends to be episodic and neglect is chronic.
a. Both statements are trueb. Both statements are falsec. The first statement is true and the second is falsed. The first statement is false and the second statement is true
Dental neglect is a willful failure of parent or guardian to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection. Abuse can occur as physical, sexual or emotional abuse. Physical abuse is the most easily recognizable form of abuse. If the reported history of abuse is not consistent with the injury abuse should be investigated. Facial and head injuries were 50% of physical abuse and oral injuries were 25% of abuse injuries. Neglect was 50-65% of child maltreatment and 25%was physical abuse. The rest was sexual or mental abuse. If children are abused in one method they are more likely to be maltreated in another.
The average age for identification of maltreatment victims is 7.4 years; 49% are male and 68% white, 21% black, and 11% ethnic. Infants to two years are most often neglected. Older children 12-17 years are least likely to be neglected but most often sexually or emotionally abused.
Unexplained or multiple fractures of various stages of healing, spiral fractures, or fractures of very young children should be investigated. Depression, withdrawal, acting out, and clinginess are possible signs of abuse. Delayed treatment or aggression or defensiveness of the parent or caretaker could be signs of abuse.
The answer is A
McDonald RE and Avery DR, Dentistry for the child and adolescent. Seventh edition. Pages 24-28
6. Which of the following are not advantages of digital radiography?a. Reduced need for chemicals to process filmb. Reduced radiation exposure to the patientc. Ability to manipulate and enhance imagesd. Small size of sensor device
There is no need to process films so the need for caustic chemicals is no longer needed. This makes digital radiography more environmental friendly. Less radiation is required to capture an image with the sensor (coupler). Images are viewable in only a matter of seconds. The ability to send images immediately by computer for consult is a benefit for remote clinics. Some programs have functions that let the polarity to be reversed and contrast to be adjusted. This can allow for improved diagnostic skills. The cost for the initial set up can be high. The cost savings in chemicals to develop will offset this eventually. The sensors can be large and bulky and difficult to place in some patients.
The answer is D.
1. Van der Stelt PF. Principles of digital imaging. Dent Clin North Am 2000;44(2):237-48, v.2. Versteeg CH, Sanderink GC, van der Stelt PF. Efficacy of digital intra-oral radiography in clinical dentistry. J Dent 1997;25(3-4):215-24.3. Wenzel A, Grondahl HG. Direct digital radiography in the dental office. Int Dent J 1995;45(1):27-34.
7. HIV can infect most human cells with the most common being those with the CD4 receptors including the T-helper lymphocytes and macrophages. HIV has been found in saliva but transmission has not been documented.
I. Both statements are trueA. Both statements are falseB. The first statement is true and the second is falseC. The first statement is false and the second statement is true
HIV is composed of two subtypes (HIV-1 and HIV-2) with many strains. HIV has been located in blood, saliva, breast milk, cerebrospinal fluid, amniotic fluid, urine, and semen. Antibodies develop in 6-12 weeks after infection. It may take 6 months to seroconvert. Mean incubation for AIDS is 10-12 years. Ninety percent die in three years after diagnosis with AIDS. Most people develop an acute brief viremia within two to six weeks of infection. A temporary fall in CD4 cells occurs. A progressive fall in CD4 cells will occur leading to AIDS. When CD4 cells counts drop below 200 they become more susceptible to opportunistic infections. Candidiasis, herpes zoster, oral hairy leukoplakia, Kaposi’s sarcoma are oral conditions that can occur with low CD4 cell counts. The correct answer is A.
Little JW, Dental Management of the Medically Compromised Patient, Fifth edition
8. The permanent teeth are typically smaller than the primary teeth they replace. The leeway space of the mandibular is approximately 3.4mm to 4.2mm and the maxillary is 1.8mm to 2.4mm.
a. Both statements are trueb. Both statements are falsec. Statement one is true and two is falsed. Statement two is true and one is false
Leeway space is the term to describe the space available when the permanent premolars and canine replace the deciduous primary molars and canine. The mesiodistal width of the permanent teeth is almost always smaller than the primary teeth they replace. This space allows for room in the posterior portion of the arch to accommodate the permanent canine which is usually larger than the primary canine. Sometimes there is a mesial shift of the permanent first molar into the leeway space. The leeway space can be used to solve crowding issues by preventing the permanent first molar from shifting mesial. This can be accomplished with a lingual arch bar.
The answer is a.
J. Braham and Morris, Textbook of Pediatric Dentistry, Pages 42-44
9. What is the oral pediatric dose of Amoxicillin for SBE prophylaxis (for those not allergic to Penicillins)?
a) 100 mg/kg one hour prior to dental procedureb) 75 mg/kg one hour prior to dental procedurec) 20 mg/kg one hour prior to dental procedured) 50 mg/kg one hour prior to dental procedure
Answer: d) 50 mg/kg one hour prior to dental procedure
Suggested Antibiotic Prophylactic Regimens by the American Heart Association:
Children not allergic to penicillin Amoxicillin 50 mg/kg (maximum 2 g) orally 1 h prior to dental procedure
Children not allergic to penicillin and unable to take oral medications
Ampicillin 50 mg/kg (maximum 2 g) IV or IM within 30 min before dental procedure
Children allergic to penicillin Clindamycin 20 mg/kg (maximum 600mg) orally 1 h prior to dental procedure
Children allergic to penicillin and unable to take oral medications
Clindamycin 20 mg/kg (maximum 600mg) IV or IM or Cefazolin 25 mg/kg (maximum 1 g IV or IM within 30 min before dental
procedureUtilization of antibiotic patients at risk does not provide absolute immunity from infection.Post procedural symptoms of acute infection (eg, fever, malaise, weakness, or lethargy) may indicate antibiotic failure and need for further medical evaluation. Indications for antibiotic prophylaxis in general:
Patients with cardiac conditions associated with endocarditis.Patients with compromised immunity.Patients with shunts, indwelling catheters or medical devices.
Pediatric Dentistry Vol 24(7), American Academy of Pediatric Dentistry, Page 107
10. What does not occur with the premature loss of a mandibular primary canine?
a) Shortening of the arch lengthb) Shift of midline to affected sidec) Development of a posterior crossbited) Incisor teeth drift distally and linguallye) Space maintenance is initiated
Answer: c)
Missing primary mandibular canine, what happens….
Primary mandibular canine erupted at 20 months.Permanent mandibular canine erupts at 10.5 years.The permanent canines are positioned to lie nearly in line with the primary canines.
Canine usually comes about as a result of root resorption caused by erupting lateral incisors without enough space.
Early loss of a single primary canine in the mixed dentition requires space maintenance or extraction of the contralateral tooth to eliminate midline changes and the loss of arch symmetry. Arch length shortens as the incisor teeth drift distally and lingually. If the contralateral canine is extracted, a lingual arch space maintainer may still be needed to prevent lingual movement of the incisors.
Space tends to close as the incisors drift lingually and toward the affected side. Asymmetric activation of a lingual lower arch is usually the best approach.
The primary lower canine is usually displaced labially if there is not enough room.
11. What is the optimal age for the child’s first dental visit?
a) After all primary teeth have eruptedb) Within 6 months of first primary tooth eruptionc) After the child’s first birthdayd) After eruption of the permanent first molar
Answer: b) Within 6 months of first primary tooth eruption (and no later than 12 months of age) Infant oral health care begins ideally with prenatal oral health counseling for parents.
At the infant oral evaluation visit, the dentist should:1. Record a thorough medical and dental history.2. Complete a thorough oral examination.3. Perform risk assessments for oral and dental disease and determine a prevention
plan and interval for periodic reevaluation.4. Discuss and provide guidance regarding dental and oral development, fluoride
status, non-nutritive oral habits, injury protection, oral hygiene and effects of diet on the dentition.
Pediatric Dentistry Vol 24(7), American Academy of Pediatric Dentistry, Page 47
12. Which of these statements concerning asepsis is true?1. Moist heat is more efficient than dry heat for sterilization.2. Ethylene Oxide gas is safe to use on human tissue.3. Moist heat does not corrode instruments.4. Antiseptics are chemical agents used topically on skin.5. Sanitization eliminates all viable microorganisms from a surface.
a) 3,5b) 1,4c) 2,5d) All of the abovee) None of the above
Answer: b)Asepsis Definitions1. Sepsis – breakdown of living tissue by action of microorganisms and usually accompanied by inflammation.2. Medical asepsis - is the attempt to keep patients, health care staff, and objects as free as possible of agents that cause infection.
3. Surgical asepsis - is the attempt to prevent microbes from gaining access to surgically created wounds.Levels of AsepsisAntiseptics (for living tissue) or disinfectants (for inanimate objects) – refer to substances that can prevent the multiplication of organisms capable of producing sepsis. Sterility – is the freedom from viable forms of microorganisms. An absolute state, no varying degrees.Sanitization – reduction of the number of viable microorganisms t levels to levels judged safe by public health standards. Decontamination - similar to sanitization except not connected to public health standards. The microbes most resistant to elimination are bacterial endospores. Any sterilization or disinfection method that eliminates endospores should be effective against bacteria, viruses, mycobacteria, fungi, mold, and parasites.Techniques of instrument sterilization:Physical 1. Dry heat – for glassware and items that are susceptible to rust. Range: 250 to 280F (12h to1h respectively)2. Moist heat – steam autoclave, more effective at lower temperatures , takes less time more efficient than dry heat. Dulls and rusts instruments. Range: 240 to 280 (60min to1.5 minutes respectively)3. Mechanical dislodgement 4. Radiation Chemical1. Antiseptics – used to prepare the surgical team’s hands and arms before donning gloves and to disinfect the surgical site. Iodophors, chlorhexidine, hexachlorophene.2. Disinfectants – glutaraldehydes, iodophors, chlorine compounds, formaldehyde. (30 min to 10 hours)3. Ethylene Oxide gas – diffuses through porous materials such as plastic and rubber. At 50C is effective for killing all organisms including spores, in 3 hours. Highly toxic to animal tissue.
13. Which of the following is not a device used to correct crossbite or constricted maxillary arch?
a) W archb) Quad helixc) Split plate hawleyd) Nancee) Hyrax with jackscrew
Answer: d) The Nance appliance is used for space maintenance.
Indications for palatal expansion:
1. Growth modification in the treatment of skeletal problems. Extent growth may be modified. Advantageous to start early.2. Treatment of posterior crossbite or bilateral maxillary constriction. 3. Transverse maxillary deficiency, narrow skeletal width of maxilla = narrow width of the palatal vault. Can be assessed from dental casts.
The most common transverse problem in preadolescent is maxillary constriction and posterior crossbite. Early correction is needed if there is a mandibular shift. If there is no shift, treatment is delayed until eruption of the first molars. Treatment prior to adolescence and midpalatal suture closure is recommended.
Goals of palatal expansion:1. Arch expansion – groups of teeth are moved to expand the arch perimeter.
2. Repositioning of individual teeth.
Fixed appliances are reliable and require little patient cooperation. Removable appliances require greater patient cooperation and risk being lost or not used at all. Removables also mayb become dislodged with the strong forces used in expansion.
Fixed appliances:
W arch (36mil wire or Quad helix 38mil wire, more flexible, more wire). Quad Helix and W arch for treatment of palatal constriction. Gives skeletal and dental movement in the 3-6 year old.
By adolescence, more force may be required to separate the mid palatal suture as it starts to interdigitate. Rapid palatal expansion may be indicated. This consists of a mechanical screw device that is cemented or bonded, opened 0.5mm/day, 2000 to 3000g of force. Active treatment takes 10-14 days. Widens skeletally since PDL is hyalinized. After adolescence, the suture will probably be interlocked, making skeletal expansion impossible.
Slow palatal expansion gives 900-1300 g of force, 1mm/week. Widens skeletally and dentally. Expect 3-5mm of expansion. Lip bumpers or buccal shields work as well. Removable appliances:
Most are Hawley split plate type designs that use clasps to provide retention. Wire springs or jackscrews may be used to provide the expansion force.
14. Concerning the epidemiology of fluoride which of the following questions are true?
1. McKay was the first to note the mottling of enamel in Dental patients in Denver Colorado in 1902.
2. In 1944, in the famous Michigan fluoridation study, the city of Muskegon had 1 ppm of Fluoride added to its water supply and Grand Rapids was the control city.
3. In the Michigan study, caries incidence decreased about 50%.
4. In 1970 it was estimated that 7 million people in 1900 communities in the U.S. have been drinking natural fluoridated water with a concentration of >= to .7 ppm.
5. Adequate ingestion of Fluoride at an early age of enamel development is important in decreasing pit and fissure caries.
6. Fluoride decreases pit and fissure caries more than smooth surface caries.
A. 1,2,3,4 are trueB. 2,3,4,5 are trueC. all are trueD. 1,3,5,6 are trueE. 1,3,4,5 are true
The correct answer is E.Source is Fluoride and Caries Prevention 2nd edition Murray and Ruggs-Gunn p. 10-27.
Statements 1-3 are here for historical purposes. Statement number 4 addresses the safety issue of Fluoride therapy.
2 is false=Grand Rapids was the experimental city, the city officials of Muskegon were so impressed with the results of 50% reduction in caries experience in Grand Rapids that they added Fluoride to their water 6 years later-only negative was the control for the study was then lost after 6 years of results. 6 is false= fluoride ingestion may alter the morphology of pits and fissures decreasing their susceptibility, but Fluoride exerts its effect mostly on decreasing smooth surface caries.Source is Fluoride and Caries Prevention 2nd edition Murray and Ruggs-Gunn p. 10-27.
15. Which of the following are true concerning water lines in dental operatories?
1. The NIDCR has documentation of disease transmission arising from DUWL (Dental Unit Waterline microbial contamination.
2. The goal is to bring microbial content of dental water to no more than 200 CFU/ml.
3. Biofilms are microscopic communities consisting primarily of naturally occurring water bacteria and fungi that form thin layers on surfaces that remain in contact with water.
4. The CDC recommends not using water from dental water lines when performing surgical procedures and that the use of sterile irrigating solution should be used.
5. A prudent guideline is to run the handpiece for 45 seconds to 1 minute before each patient and at the end of the day.
6. These guidelines will reduce the biofilm formation in the waterlines.
7. Four categories of products to improve DWL’s are: independent water systems, chemical treatment protocols, point of use filters and sterile water delivery systems.
8. The EPA’s recommended drinking water standard is 500 CFU/ml of noncoliform bacteria, and Legionella pneumophila, Pseudomonas aeruginosa and non-tubercular mycobacterium have been isolated from DUWL’s.
A. All are trueB. 1,3,5,7,8 are trueC. 2,4,6,8 are trueD. 2,3,4,7,8 are trueE None of the above
The correct answer is D#1 is false- The NIDCR (National Institute of Dental and Craniofacial Research) has NO documentation of disease transmission arising from DUWL (Dental Unit Waterline microbial contamination. There is however irrefutable evidence that water delivered to most patients is of poor microbiological quality.#5 is false the guideline is to run the water for several minutes at the beginning of the day and 20-30 seconds after every patient. #6 is false- These guidelines will NOT reduce the biofilm formation in the waterlines- it only seeks to decrease the number of microorganisms present in the treatment water. To reduce the biofilm you must use a protocol of 5.25 % sodium hypochlorite diluted in a 1:10 ratio. Weekly 10 minute treatments improved the quality of the water and reduced the biofilm. You MUST have multiple treatments and COMPLIANCE is a big issue. Filters help a lot also-more $$.
SOURCE: JADA, Vol. 133 September 2002 p.1199-1206.
16. Which of the following can cause foggy films?
1. l. Light leaks in the darkroom
2. Incorrect bulb, or defective safelite filter or bulb.
3. Developer temperature too high.
4. Improper storage of film.
5. Contamination of the fixer in the developing solution.
6. Processing too fast or fixer solution is depleted.
A. All are trueB. 1,3,5,6 are trueC. 2,3,4,5 are trueD. 4.5.6 are trueE. 1,2,3,4 are true
The answer is E
1-4 are true causes of foggy films. #5 is false contamination of the fixer in the developing solution will cause brown discoloration of the film. #6 is false- processing too fast or fixer solution is depleted-will cause a Greenish-Yellow discoloration of the film.
The source is Principles and Practice of Panoramic Radiology-Langland, Langlais, and Morris, p. 82.
17. Which of the following are true concerning latex allergies?
1. Delayed allergies-Type IV-or irritant dermatitis, are caused by processing chemicals.
2. Immediate allergies are caused by antigens from Hevea brasiliensis trees where latex is harvested from=Immediate –Type 1 reaction. 5-10% of health care workers may have an immediate allergy to NRL.
3. In the 1980’s it was ascertained that natural rubber latex (NRL) allergy is An IgE mediated reaction.
4. Possible symptoms are- pruritis, urticaria, eczema, rhinitis, angioedema, asthma and possibly anaphylaxis.
5. Three common routes of transmission are-cutaneous, percutaneous, and mucous membrane through inhalation of aerosols.
6. Cerebral Palsy patients have a latex allergy incidence of 18-45 %.
7. The SPT is used to determine latex allergy.
A. all are trueB. 1,3,5,7 are trueC. 2,4,6,7 are trueD. 1,2,3,4,5,7 are trueE. 1,2,3,4,5,6 are true
The answer is DAll are true except #6- SPINA BIFIDA patients have an incidence of 18-45 %.SPT is skin prick test, this study quoted data taken from 2166 dental health care workers who volunteered to take the test at the ADA conventions over a two year period.
Source: JADA, Natural Rubber Latex Hypersensitivity: Incidence and prevalence of Type 1 Allergy in the Dental Professional, 1998, p. 43-54.
18. Moyers prediction table is used for mixed dentition space analysis. To utilize Moyers prediction, the mesiodistal width of the lower incisors is measured and this number is used to predict the size of the both lower and upper unerupted canines and premolars.
A) Both statements are true.B) Both statements are false.C) The first statement is true, second statement is false.D) The first statement is false, second statement is true.
Answer: A
Mixed dentition space analysis to estimate the size of the unerupted permanent teeth to calculate the space required. There are 3 basic approaches:
1. Measurement of teeth on Radiograph. A simple proportional relation is set up to estimate the size of the unerupted permanent teeth.
2. Estimation from proportional tables. Most predictions are based on American white school children
Moyers: the mesiodistal width of the lower incisors is measured and this number is used to predict the size of the both lower and upper unerupted canines and premolars from the table.
Tanaka and Johnson: small bias to over estimate. ½ mesiodistal width of 4 lower incisors + 10.5mm= mandibular unerupted
canine and premolars in one quadrant.½ mesiodistal width of 4 lower incisors + 11.0mm= mandibular unerupted canine and premolars in one quadrant.3. Combination of radiograph and prediction table
Stanley and Kerber: Canine width to be estimated directly from the sums of incisors and premolar widths using a graph. Only for mandibular arch.
Tooth size analysis: to determine the disproportion among the sizes of individual teeth (as tooth size discrepancy). If the discrepancy is 1.5mm or greater, it should be included in the problem list.
Bolton Analysis: is determined by measuring the mesiodistal width of each permanent tooth. A standard table is used to compare the total width of maxillary and mandibular anterior teeth and the total width of all upper and lower teeth.
19. SNA angle measures the relative anteroposterior relationship of the maxilla to the anterior cranial base. SNB angle measures the relative anteroposterior relationship of the mandible to the posterior cranial base.
A) Both statements are true.B) Both statements are false.C) The first statement is true, second statement is false.D) The first statement is false, second statement is true.
Answer: C
SNA angle (Steiner) (827) formed by intersection of the planes Sella-Nasion and Nasion-Point A. measures the relative anteroposterior relationship of the maxilla to the anterior cranial base.
SNA angle greater than 82 would indicate a forward or prognathic position of the maxilla relative to the anterior cranial base. Less than 82 would indicate a retrognathic position of the maxilla.
SNB angle (80) measures the relative anteroposterior relationship of the mandible to the anterior cranial base.
20. FMA angle is formed by the intersection of Frankfort horizontal plane and the (Down’s) mandibular planes. As the FMA increases the amount of vertical growth exceeds horizontal growth and the chin is more posterior.
A) Both statements are true.B) Both statements are false.C) The first statement is true, second statement is false.D) The first statement is false, second statement is true.
Answer: A
FMA angle (25) is formed by the intersection of Frankfort horizontal plane and the (Down’s) mandibular planes (tangent to the lower border of the mandible and the lowest point on the symphsis, Menton). It determines mandibular growth pattern and directions.
As the FMA increases the amount of vertical growth exceeds horizontal growth and the chin is more posterior.
High mandibular plane angles are frequently associated with unfavorable vertical growth and anterior open bites.
Low mandibular plane angles are associated with horizontal mandibular growth and deep bites.
21. Which of the following statement is (are) correct?
1) Sterilization strip changes color on exposure to sterilization temperature.2) The indicator strip is placed on top of the packaging.3) The spore of the bacteria Bacillus stearothermophilus is used to test the
reliability of heat sterilization.4) The spore test is used bimonthly to judge the effectiveness of sterilization
technique and equipment.
A) 1, 2B) 2, 4C) 3, 4D) 1, 3
Answer: D
Sterilization strip changed color on exposure to sterilization temperature. It doesn’t indicate duration of sterilization cycle. The indicator strip is placed in the most interior part of the packaging.
The spore of the bacteria Bacillus stearothermophilus is used to test the reliability of heat sterilization. The spore test is used weekly to judge the effectiveness of sterilization technique and equipment.
Dry heat oxidizes the cell proteins where as moist heat causes coagulation of proteins quickly. Dry heat requires higher heat for longer time to achieve sterility.
Autoclaving: pressurized steamTemp Pressure Duration of treatment115C 10 PSI 60 min121C 15 PSI 24 min126C 20 PSI 16 min
Advantages: effectiveness and speed. Disadvantages: Cost of the autoclaves, and dull and rust instrument.
Contemporary Oral and Maxillofacial Surgery, Peterson, Ellis, Hupp and Tucker, 3rd ed, 1998, p 73-77.
22. Which of the following statement is (are) incorrect?
1) It is important to intrude a tooth rapidly to gain periodontal attachment. 2) Excessive force may produce necrosis of the PDL and adjacent alveolar bone.3) The physiologic extrusion or intrusion is when the alveolar bone is brought
along with the tooth.
A) 1B) 2C) 3D) 1,3E) None of the above
Answer: A
To successfully intrude a tooth, it requires careful control of magnitude so that very light forces are applied to the tooth and the force will be concentrated in a small area at the tooth apex. Tooth is expected to tip somewhat as it is being intrude.
If the tooth is intruded, the bone height tend to be lost at the alveolar crest, so that about the same percentage of the root remains embedded in bone as before, even if the intrusion was over a considerable distance.
The bone support around periodontally involved teeth could be improved by intruding the teeth and forcing the roots deeper into the bone; but this doesn’t lead to soft tissue attachment.
Physiologic extrusion or intrusion that brings the alveolar bone along with the tooth, followed by gingival and osseous recontouring is preferable.
23. The use of orthodontic headgear can be utilized to treat Class I, Class II and Class III malocclusions. The most common type of headgear is designed to treat the Class III malocclusion.
A. Both statements are trueB. Both statements are falseC. First statement is true, second statement is falseD. First statement is false, second statement is true
Headgear is used for growth modification, molar correction, vertical control, root torque and dental movement. There are designed to treat Class II malocclusion and Class III malocclusion.
Class II headgear is implemented in the following types: High Pull, Cervical Pull, and Combination Pull. These types change Maxillary Apical Base (ANB) in retarding the advancement of maxillary molar position. The high pull rests on the crown of the skull and is designed to place forces in an upward distal manner. The cervical pull rests on the back of the neck and is designed to place only distal forces. The combination rests in both positions and place more distalising forces than upward.
Class III headgear is implemented in the following types: Chin Cup and Orthopedic Face Mask. These types correct the sagittal-vertical relationship. The chin cup applies a force to against mandibular growth and is for short-term restriction, redirects growth, and is utilized infrequently by orthodontists. The orthopedic face mask (a.k.a. reverse pull) is attached to maxillary molars and rests on the forehead and chin and does the above as well but primarily protracts the maxilla
Answer is B both statements are false.
Moles, J. A. NPDS, NNDC, Orthodontic 240, lecture: Growth Modification dated 18 Nov 02
Anthony D. Viazis. Atlas of Orthodontics: A guide to Clinical Efficiency
24. Which series of radiographs would you order for a new 6-year-old patient exam?
a. M&M occlusals, posterior BWx, Panorex b. M&M occlusals, R&L M&M primary molar PAx, posterior BWx Panorex c. M&M ant PAx, posterior BWx, R&L M&M Primary molar Paxd. R&L M&M primary molar PAx, Posterior BWx, lateral ceph, Panorex
The ADA’s suggested radiographic protocol for a new pediatric patient exam is as follows:
D. AGE RADIOGRAPHS_________3-5 y/o: No apparent abnormalities, open contacts -None
No apparent abnormalities, closed contacts -2 posterior bitewings Abnormalities / Caries -Series of 4 films
2 posterior BWx M&M occlusals
Extensive or deep caries -additional selected PAx
6-7 y/o: No apparent abnormalities -Series of 8 films M&M occlusals (PAx) R&L max post 1o PAx R&L mand post 1o PAx R&L posterior BWx Panoral
Extensive or deep caries -additional selected PAx
8-9 y/o: No apparent abnormalities -Series of 12 films 2 incisor PAx 4 cuspid PAx 4 1o premolar/molar PAx 2 posterior BWx Panoral
10-12 y/o: No apparent abnormalities -Series of 12 or 16 films In addition to the above, 4 quadrant permanent molar PAx
All high caries risk patients receive new BWx at the 6-month recall visit. Standard BWx is done in 12-month cycles. The Pan-oral radiograph is indicated following eruption of the first permanent tooth.
The correct answer is B. M&M occlusals, R&L M&M primary molar PAx, posterior BWx Panorex
McDonald, R.E., Avery, D.R., Dentistry for the Child and Adolescent 7th Edition. Mosby 1999. Pages 64-67.
25. List the LeFort classifications in order of decreasing severity:
a. Class I, Class II, Class III, Class IVb. Class III, Class II, Class Ic. Class IV, Class III, Class II, Class Id. Class I, Class II, Class III
In 1901, the Frenchman Rene LeFort published three consecutive papers on the now famous classification of facial fractures. His work described the great lines of weakness in the face through which most fractures occur by using low velocity impact forces directed against cadaver skulls. These lines, where the facial bones break in trauma, have become known as the LeFort I, II, and III fractures.
The Lefort I fracture, or transverse fracture, extends through the base of the maxillary sinuses above the teeth apices essentially separating the alveolar processes, palate, and pterygoid processes from the facial structures above. This transverse fracture across the entire lower maxilla separates the alveolus as a mobile unit from the rest of the midface. Fracture dislocations of segments of the alveolus may be associated with this fracture. With high-energy injuries, the palate may be split in the midline in addition to the LeFort I fracture.
The LaFort II fracture is synonymous with a pyramidal fracture of the maxilla. This fracture pattern begins laterally, similar to a LeFort I, but medially diverges in a superior direction to include part of the medial orbit as well as the nose. The fracture extending across the nose may be variable, involving only the nasal cartilage or as extensive as to separate the nasofrontal suture. The fracture extends diagonally from the pterygoid plates through the maxilla to the inferior orbital rim and up the medial wall of the orbit to the nose. This separates the maxillary alveolus, medial wall of the orbit and nose as a separate piece.
A LeFort III fracture or craniofacial dysjunction denotes a complete separation of the midface or facial bones from the cranium. This fracture transverses the zygomaticofrontal suture, continues through the floor of the orbit, and finally through the nasofrontal suture. The bones of the orbit are separated through the lateral wall, floor, and medial wall. It is unusual to have this fracture as a single segment of bone; more commonly, it comminutes with varying combinations of zygomatic, nasoethmoid, and orbital fractures. The fractures may not be symmetric on both sides and minimal mobility may be present.
The LeFort IV fracture is a figment of my imagination that tends to run freely at such this late hour during which I am typing this question for all of you. I hope you appreciate it.
The correct answer is B. Class III, Class II, Class I
a. All of the Aboveb. 1, 2, 4 c. 1, 2, 3d. 1, 3, 4
A pulpotomy is the removal of the coronal portion of the pulp of both primary and permanent teeth with carious exposures. Justification for carious exposure is that the coronal pulp tissue contains microorganisms and inflammatory products. Healing can take place in the canals of the normal pulp tissue. Most commonly performed with formocresol to fix the amputated tissue remaining in the orifice, then restoring the tooth with IRM and stainless steel crown
Contraindications are listed as follows: non-restorable teeth, teeth nearing exfoliation, spontaneous or provoked discomfort, periapical or furcal pathosis, internal or external resorption, lack of hemostasis from amputated pulp stumps, fistula, parulis, purulent pulpal discharge, pulpal calcification, pathologic mobility.
For permanent teeth, if the exposure is tramatic and not too large or not a significant amount of time has passed since the injury a Cvek (partial) pulpotomy can be preformed when the coronal pulp inflammation is not wide spread. This preserves as much of the health tissue as possible for maturation of the tooth, root and apex.
The correct answer is C. Asymptomatic carious pulp exposure, inflammation confined to the coronal aspect of the pulp not extending radicularly, healthy periradicular tissues, mildly symptomatic tooth
McDonald, R.E., Avery, D.R., Dentistry for the Child and Adolescent 7th Edition. Mosby 1999. Pages 421-425, 498-500.
27. Which of the following statements regarding fluoride is (are) true?
1. Fluoride absorbs to the crystal surface of enamel attracting phosphate ions, followed by calcium ions leading to new mineral formation.2. Advantages of fluoride varnish are they:
- contain high concentrations of fluoride- are applied locally/topically- are protective- are surface active- do not stain teeth
3. The most popular in-office fluoride is 8% SnF24. The typical over-the-counter dentifrice contains 2000 ppm of fluoride.
a. all of the aboveb. none of the abovec. 1,2,3d. 4 onlye. 2
Answer: b. none of the above
1 – calcium ions are attracted first followed by phosphate ions.2 – fluoride varnish can stain.3 – Sodium fluoride is the most popular.4 – the typical over-the-counter dentifrice is 1000 ppm of fluoride
28. What is the appropriate dosage for supplemental fluoride for 5-year-old children who live in a non-fluoridated water area and what is the proper concentration in the drinking water for a community with a fluoridated water program?
AGE Less than .3ppm .3-.6ppm Over .6ppmNo Flouride ½ dose Ideal flouride
Birth-6 mos 0 0 06mos-3years .25 0 03-6 years .5 .25 06-16 yrs 1.0 .50 0
There is currently some controversy here since there is 1mg of flouride in a toothbrush size strip of toothpaste and children frequently ingest much of the toothpaste they use. Additionally, there is fluoride present in many of the beverages children drink today including some bottled water.
Pediatric Dentistry. Vol.24, No.7pp66
29. Increasing kVp will will increase the contrast of the film image. Decreasing the mA will increase the density of the film image.
a. The first statement is true, the second is falseb. The first statement is false, the second is truec. Both statements are false.d. Both statements are true
Answer: c
High contrast is observed with fewer shades of gray and is better for viewing endodontic files in the canals. Many practitioners use 70 kVp for endo and 90 kVp for caries detection. Low contrast is more desirable for caries diagnosis. Increase of kVp and mA will both increase density. Density is the degree of blackness of a film.
Langland, Langlais Principles of Dental Imaging. Pp53,54
30. Serial extractions are recommended in class I malocclusions, (skeletal and Dental) when the space discrepancy is > 6mm but < 13mm. The first extractions are the primary 1st molars when the underlying premolar has 2/3 root formation completed.
a. The first statement is true and the second is false.b. The first statement is false and the second is true.c. Both statements are trued. Both statements are false.
Answer: a
The first extractions are the primary canines and they are removed as soon as all mandibular permanent incisors are erupted. An evaluation for serial extractions is done at age 8 when there is evidence of crowding. After age 8, there will be continued growth of the arches without an increase in arch length.
Glossary of Dentofacial Orthopedic Terms-Orthodontic Glossary-American Association of Orthodontists
PEDO/ORTHO/PUBLIC HEALTH/RAD
1. Which of the following are true regarding tooth eruption pattern?
6. The first permanent premolars replace the primary molars.7. The maxillary succedaneous incisors usually erupt before the mandibular
incisors.8. The most favorable eruption sequence for primary teeth in either arch is
ABDCE (using Palmar notation)9. The eruption sequence for the succedaneous dentition in the mandible
usually includes eruption of the canines before the premolars.10. The eruption sequence for the maxilla usually includes eruption of the
canines before the premolars.
f. 3 and 4 only are correctg. 1, 2, and 3 are correcth. 1, 3, and 4 are correcti. 2, 4, and 5 are correctj. 2, 3, and 4 are correct
PRIMARY DENTITION: ERUPTION TOOTH LETTER ERUPTION
CENTRAL A ~ 6 - 9 MONTHS
LATERAL B ~ 7 - 10 MONTHS
CANINE C ~ 18 MONTHS
1ST MOLAR D ~ 14 MONTHS
2ND MOLAR E ~ 24 MONTHS
Primary Root completion 18 months post eruption. (12-18 mos.)
Teeth erupt when the root is 2/3 complete.most favorable eruption sequence for primary teeth both Max & Man: ABDCE
Primary teeth:germs form at 6-8 wks IUenamel forms 4-6 months roots complete approx 1 yr after eruption
2. Which of the following is false regarding prevention of transmission of M. tuberculosis bacilli?
a. M tuberculosis bacilli (Mtb) transmission cannot occur via fomites.
b. Mtb are major spore forming organisms, making them exceptionally difficult to kill with conventional germicides.
c. Mtb organisms are sensitive to heat and ethylene oxide. All reusable instruments should be sterilized with heat or ethylene oxide.
d. Patients with untreated TB should have their surgery postponed until they can receive treatment for their TB.
e. Mtb organisms are sensitive to irradiation
The only mycobacterial organism of significance to most dentists is Mycobacterium tuberculosis. TB is uncommon in the US and Canada, however, immigration from SE Asia, where tuberculosis is common, brought a new reservoir of M. tuberculosis organisms. Patients who are infected with HIV are another group who may harbor tuberculosis organisms. Some newer strains of TB are resistant to drugs commonly used to treat TB.
Etiology: In the majority of cases of human TB the causative agent is M. tuberculosis, an acid fast, nonmotile, intracellular rod that is an obligate aerobe; hence, it exists best in an atmosphere of high oxygen tension. Humans are the only known reservoir. This explains why it commonly infects the pulmonary system. But, it can infect any organ of the body. Typical mode of transmission is via infected airborne droplets of mucus or saliva that
have been forcefully expelled from the lungs, usually by coughing, speaking, sneezing or singing. It is not spread by fomites (dishes, toys, clothes or linens).It can be spread through unpasturized milk.(M. bovis). Oral lesions can occur via ingestion of sputum and coughing up infected sputum thereby inoculating the oral cavity.
Diagnosis: K. “Tuberculosis infection”
Positive TB skin test, no active disease“LTBI” latent TB infection
L. “TB disease”Presence of clinical signs and symptomsMay result from primary infection or activation of latent TBHighest risk of activation in first two years after exposureDiagnosis
Dental management:Updating the patient’s medical historyRecognizing signs and symptoms of TBFollowing infection control guidelinesNeed to ascertain potential infectivity of patientsActive TB (Infectious)History of TB (Infected)Positive tuberculin test (Infected)Undiagnosed but with suggestive signs and symptoms and risk factorsPatients with clinically active TB:Emergency treatment onlyMinimized aerosolization
Use rubber damMinimize handpiece use
Treatment in hospital setting/isolations rooms-6-12 room-air exchanges per hourDirectional airflow “ negative-pressure vent”Air enters room from hallways and leaves only via outside exhaustAutomated room-pressure monitors with alarms HEPA filtration, UV radiation (germicidal)
Patients with clinically active TBO.K. to treat routinely:
After 2 weeks of anti-TB therapy and confirmed noninfectious by physicianPediatric patient under age 6Considered noninfectious since TB bacilli are rare in sputum and unable to cough up sputum
Confirm stats with pediatrician M. Patient with history of active TB
Initial cautionConsultation with physicianConfirm history of treatment , periodic physical exams, chest radiographsRelapse is rare if treat adequatelyHas patient becalm immunosuppressed since completion of treatment
N. Patients with positive skin testAsk for history of evaluation for active TB, chest RG’s, history of anti-TB drugsRoutine treatment O.K.; no special precautions
O. Patients with suggestive signs and symptomsUnexplained, persistent signs and symptoms
Defer dental treatment until after medical evaluation
Effective chemotherapy of TB is dependent on 1) patients education and compliance, 2) appropriate selection of drugs, 3) multiple drug use, and 4)drug administration continuance for a sufficient time.
Common drug regimens:Non-drug resistant TB3 drugs for 2 months (INH + rifampin + pyrazinamide), followed by 2 drugs for 4 months ( INH + rifampin)6 months total treatment timeDrug resistance4 drugs for 2 months (INH + rifampin + pyrazinamide + either ethambutol or streptomycin)Determination of resistance again: if resistant only to INH: rifampin + pyrazinamide + either ethambutol or streptomycin for 6 months or rifampin + ethambutol continued for 12 monthsImmunosuppressed patients receive treatment for a minimum of 9 monthsConfirmed multiple-drug resistance3-7 drugs (INH + rifampin + pyrazinamide + ethambutol, an aminiglycoside, or capreomycin, ciprofloxacin, or ofloxacin and either cycloserine, ethionamide, or aminosalicyclic acid)-this is continued for 12-24 months or until negative cultures are evident.The correct response is b. (it is false)
References:Petersen, Ellis, Hupp, Tucker: Oral and Maxillofacial Surgery, Mosby, 3rd Ed., 1998.Little and Falace, et. Al.: Dental Management of the medically Compromised Patient, Mosby, 6th Ed., 2002.
3. Which of the following are true regarding disadvantages of Nitrous oxide inhalation use for conscious sedation?
6. Nitrous oxide is considered to be reactive and toxic in doses greater than 60%.
7. It is a weak agent and should be titrated carefully in increments.8. Inconvenience may be a factor when the nasal mask hinders exposure of the
maxillary anterior teeth.9. Potential chronic toxicity has been shown to occur in office personnel. 10. Potentiation may occur when combined with other drugs.
a. 1 onlyb. 1 and 2 c. 2, 3 and 5d. 1, 2, 3 and 4e. 2, 3, 4 and 5
1. is false. Nitrous oxide is inert and nontoxic when administered with adequate oxygen.
2. is true. It is a weak agent with which attempts to push up the concentration can be fraught with failure when attempting to control moderately to severely anxious patients.
3. is true. Inconvenience may be a factor when the nasal mask hinders exposure of the maxillary anterior teeth. This is especially true in very small ch ildren.
4. is true. Potential chronic toxicity has been shown to occur in office personnel. Retrospective studies have shown that office personnel who were exposed to trace levels of nitrous oxide have suggested an increased incidence of spontaneous abortions, congenital malformations, certain cancers, liver disease, kidney disease, and neurological disease.
5. is true. Potentiation may occur when combined with other drugs. Although nitrous oxide is a weak and safe agent when used with oxygen, deep sedation or general anesthesia may be easily produced if it is added to the effects of other sedatives given by parenteral or other route.
4. Which of the following statements are true causes and effects regarding patient positioning in panoramic radiography?
f. Anterior positioning error: Widening and blurring of the anterior teeth images.
g. Patient placed too far posteriorly, outside of focal trough: Causes narrowing of tooth images.
h. Midsagittal plane positioning error: If patient is place asymmetrically in Panorex chin rest, images farthest from the film will be decreased in size
i. Spinal column positioning error: will result in an unexposed area in the middle inferior portion of the film.
j. Occlusal plane positioning error: Downward overangulation: This overangulation results in flattening of the occlusal plane.
Anterior positioning error: Narrowing and blurring of the anterior teeth imagesPatient placed too far posterior outside of focal trough: Causes widening of tooth images.Midsagittal plane positioning error: If patient is place asymmetrically in Panorex chin rest, images farthest from the film will be magnified, whereas images of structures closest to the film will be decreased in size. Spinal column positioning error: Will result in an unexposed area in the middle inferior portion of the film. If the spine is not kept erect, the radiation will be excessively absorbed by the spinal column, resulting in the low density area near the lower center of the film. Also, there may be superimposition of a portion of the spinal column over the neck of the condylar process of the mandible.Occlusal plane positioning error: Downward overangulation: This overangulation (the ala tragus line is greater than the proper 5 degree downward and forward) results in a severe curvature in the occlusal plane and a lack of definition of the incisors on the image.The only correct answer is d.Information about Ghost images: (should know for the Boards)A ghost image is formed what the object is located between the x-ray source and the center of rotation.
1. The ghost image has the same morphology as its real counter part.2. The ghost image appears on the opposite side of the radiograph from its
real counterpart.3. The ghost image appears higher up on the radiograph than its real
counterpart.4. The ghost image is more blurred than its real counterpart.5. The vertical component of a ghost image is more blurred than the
horizontal component.6. The vertical component of a ghost image is always larger than its real
counterpart, whereas the horizontal component of a ghost image may or may not be severely magnified.
Langlais RP, Langland OE, Nortje CJ. Diganostic Imaging of the Jaws. Willams & Wilkins. 1995Langland, Langlais, Morris. Principles and Practice or Panoramic Radiology.Saunders. 1982.
5. Neglect is defined as the inattention to the basic needs of a child, such as food, clothing, shelter, medical care, education, and supervision. Physical abuse tends to be episodic and neglect is chronic.
e. Both statements are truef. Both statements are falseg. The first statement is true and the second is falseh. The first statement is false and the second statement is true
Dental neglect is a willful failure of parent or guardian to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection. Abuse can occur as physical, sexual or emotional abuse. Physical abuse is the most easily recognizable form of abuse. If the reported history of abuse is not consistent with the injury abuse should be investigated. Facial and head injuries were 50% of physical abuse and oral injuries were 25% of abuse injuries. Neglect was 50-65% of child maltreatment and 25%was physical abuse. The rest was sexual or mental abuse. If children are abused in one method they are more likely to be maltreated in another.
The average age for identification of maltreatment victims is 7.4 years; 49% are male and 68% white, 21% black, and 11% ethnic. Infants to two years are most often neglected. Older children 12-17 years are least likely to be neglected but most often sexually or emotionally abused.
Unexplained or multiple fractures of various stages of healing, spiral fractures, or fractures of very young children should be investigated. Depression, withdrawal, acting out, and clinginess are possible signs of abuse. Delayed treatment or aggression or defensiveness of the parent or caretaker could be signs of abuse.
The answer is A
McDonald RE and Avery DR, Dentistry for the child and adolescent. Seventh edition. Pages 24-28
6. Which of the following are not advantages of digital radiography?e. Reduced need for chemicals to process filmf. Reduced radiation exposure to the patientg. Ability to manipulate and enhance imagesh. Small size of sensor device
There is no need to process films so the need for caustic chemicals is no longer needed. This makes digital radiography more environmental friendly. Less radiation is required to capture an image with the sensor (coupler). Images are viewable in only a matter of seconds. The ability to send images immediately by computer for consult is a benefit for remote clinics. Some programs have functions that let the polarity to be reversed and contrast to be adjusted. This can allow for improved diagnostic skills. The cost for the initial set up can be high. The cost savings in chemicals to develop will offset this eventually. The sensors can be large and bulky and difficult to place in some patients.
The answer is D.
1. Van der Stelt PF. Principles of digital imaging. Dent Clin North Am 2000;44(2):237-48, v.2. Versteeg CH, Sanderink GC, van der Stelt PF. Efficacy of digital intra-oral radiography in clinical dentistry. J Dent 1997;25(3-4):215-24.3. Wenzel A, Grondahl HG. Direct digital radiography in the dental office. Int Dent J 1995;45(1):27-34.
7. HIV can infect most human cells with the most common being those with the CD4 receptors including the T-helper lymphocytes and macrophages. HIV has been found in saliva but transmission has not been documented.
P. Both statements are trueD. Both statements are falseE. The first statement is true and the second is falseF. The first statement is false and the second statement is true
HIV is composed of two subtypes (HIV-1 and HIV-2) with many strains. HIV has been located in blood, saliva, breast milk, cerebrospinal fluid, amniotic fluid, urine, and semen. Antibodies develop in 6-12 weeks after infection. It may take 6 months to seroconvert. Mean incubation for AIDS is 10-12 years. Ninety percent die in three years after diagnosis with AIDS. Most people develop an acute brief viremia within two to six weeks of infection. A temporary fall in CD4 cells occurs. A progressive fall in CD4 cells will occur leading to AIDS. When CD4 cells counts drop below 200 they become more susceptible to opportunistic infections. Candidiasis, herpes zoster, oral hairy leukoplakia, Kaposi’s sarcoma are oral conditions that can occur with low CD4 cell counts. The correct answer is A.
Little JW, Dental Management of the Medically Compromised Patient, Fifth edition
8. The permanent teeth are typically smaller than the primary teeth they replace. The leeway space of the mandibular is approximately 3.4mm to 4.2mm and the maxillary is 1.8mm to 2.4mm.
e. Both statements are truef. Both statements are falseg. Statement one is true and two is falseh. Statement two is true and one is false
Leeway space is the term to describe the space available when the permanent premolars and canine replace the deciduous primary molars and canine. The mesiodistal width of the permanent teeth is almost always smaller than the primary teeth they replace. This space allows for room in the posterior portion of the arch to accommodate the permanent canine which is usually larger than the primary canine. Sometimes there is a mesial shift of the permanent first molar into the leeway space. The leeway space can be used to solve crowding issues by preventing the permanent first molar from shifting mesial. This can be accomplished with a lingual arch bar.
The answer is a.
Q. Braham and Morris, Textbook of Pediatric Dentistry, Pages 42-44
9. What is the oral pediatric dose of Amoxicillin for SBE prophylaxis (for those not allergic to Penicillins)?
e) 100 mg/kg one hour prior to dental proceduref) 75 mg/kg one hour prior to dental procedureg) 20 mg/kg one hour prior to dental procedureh) 50 mg/kg one hour prior to dental procedure
Answer: d) 50 mg/kg one hour prior to dental procedure
Suggested Antibiotic Prophylactic Regimens by the American Heart Association:
Children not allergic to penicillin Amoxicillin 50 mg/kg (maximum 2 g) orally 1 h prior to dental procedure
Children not allergic to penicillin and unable to take oral medications
Ampicillin 50 mg/kg (maximum 2 g) IV or IM within 30 min before dental procedure
Children allergic to penicillin Clindamycin 20 mg/kg (maximum 600mg) orally 1 h prior to dental procedure
Children allergic to penicillin and unable to take oral medications
Clindamycin 20 mg/kg (maximum 600mg) IV or IM or Cefazolin 25 mg/kg (maximum 1 g IV or IM within 30 min before dental
procedureUtilization of antibiotic patients at risk does not provide absolute immunity from infection.Post procedural symptoms of acute infection (eg, fever, malaise, weakness, or lethargy) may indicate antibiotic failure and need for further medical evaluation. Indications for antibiotic prophylaxis in general:
Patients with cardiac conditions associated with endocarditis.Patients with compromised immunity.Patients with shunts, indwelling catheters or medical devices.
Pediatric Dentistry Vol 24(7), American Academy of Pediatric Dentistry, Page 107
10. What does not occur with the premature loss of a mandibular primary canine?
f) Shortening of the arch lengthg) Shift of midline to affected sideh) Development of a posterior crossbitei) Incisor teeth drift distally and linguallyj) Space maintenance is initiated
Answer: c)
Missing primary mandibular canine, what happens….
Primary mandibular canine erupted at 20 months.Permanent mandibular canine erupts at 10.5 years.The permanent canines are positioned to lie nearly in line with the primary canines.
Canine usually comes about as a result of root resorption caused by erupting lateral incisors without enough space.
Early loss of a single primary canine in the mixed dentition requires space maintenance or extraction of the contralateral tooth to eliminate midline changes and the loss of arch symmetry. Arch length shortens as the incisor teeth drift distally and lingually. If the contralateral canine is extracted, a lingual arch space maintainer may still be needed to prevent lingual movement of the incisors.
Space tends to close as the incisors drift lingually and toward the affected side. Asymmetric activation of a lingual lower arch is usually the best approach.
The primary lower canine is usually displaced labially if there is not enough room.
11. What is the optimal age for the child’s first dental visit?
e) After all primary teeth have eruptedf) Within 6 months of first primary tooth eruptiong) After the child’s first birthdayh) After eruption of the permanent first molar
Answer: b) Within 6 months of first primary tooth eruption (and no later than 12 months of age) Infant oral health care begins ideally with prenatal oral health counseling for parents.
At the infant oral evaluation visit, the dentist should:5. Record a thorough medical and dental history.6. Complete a thorough oral examination.7. Perform risk assessments for oral and dental disease and determine a prevention
plan and interval for periodic reevaluation.8. Discuss and provide guidance regarding dental and oral development, fluoride
status, non-nutritive oral habits, injury protection, oral hygiene and effects of diet on the dentition.
Pediatric Dentistry Vol 24(7), American Academy of Pediatric Dentistry, Page 47
12. Which of these statements concerning asepsis is true?6. Moist heat is more efficient than dry heat for sterilization.7. Ethylene Oxide gas is safe to use on human tissue.8. Moist heat does not corrode instruments.9. Antiseptics are chemical agents used topically on skin.10. Sanitization eliminates all viable microorganisms from a surface.
a) 3,5b) 1,4c) 2,5d) All of the abovee) None of the above
Answer: b)Asepsis Definitions1. Sepsis – breakdown of living tissue by action of microorganisms and usually accompanied by inflammation.2. Medical asepsis - is the attempt to keep patients, health care staff, and objects as free as possible of agents that cause infection.
3. Surgical asepsis - is the attempt to prevent microbes from gaining access to surgically created wounds.Levels of AsepsisAntiseptics (for living tissue) or disinfectants (for inanimate objects) – refer to substances that can prevent the multiplication of organisms capable of producing sepsis. Sterility – is the freedom from viable forms of microorganisms. An absolute state, no varying degrees.Sanitization – reduction of the number of viable microorganisms t levels to levels judged safe by public health standards. Decontamination - similar to sanitization except not connected to public health standards. The microbes most resistant to elimination are bacterial endospores. Any sterilization or disinfection method that eliminates endospores should be effective against bacteria, viruses, mycobacteria, fungi, mold, and parasites.Techniques of instrument sterilization:Physical 1. Dry heat – for glassware and items that are susceptible to rust. Range: 250 to 280F (12h to1h respectively)2. Moist heat – steam autoclave, more effective at lower temperatures , takes less time more efficient than dry heat. Dulls and rusts instruments. Range: 240 to 280 (60min to1.5 minutes respectively)3. Mechanical dislodgement 4. Radiation Chemical1. Antiseptics – used to prepare the surgical team’s hands and arms before donning gloves and to disinfect the surgical site. Iodophors, chlorhexidine, hexachlorophene.2. Disinfectants – glutaraldehydes, iodophors, chlorine compounds, formaldehyde. (30 min to 10 hours)3. Ethylene Oxide gas – diffuses through porous materials such as plastic and rubber. At 50C is effective for killing all organisms including spores, in 3 hours. Highly toxic to animal tissue.
13. Which of the following is not a device used to correct crossbite or constricted maxillary arch?
f) W archg) Quad helixh) Split plate hawleyi) Nancej) Hyrax with jackscrew
Answer: d) The Nance appliance is used for space maintenance.
Indications for palatal expansion:
1. Growth modification in the treatment of skeletal problems. Extent growth may be modified. Advantageous to start early.2. Treatment of posterior crossbite or bilateral maxillary constriction. 3. Transverse maxillary deficiency, narrow skeletal width of maxilla = narrow width of the palatal vault. Can be assessed from dental casts.
The most common transverse problem in preadolescent is maxillary constriction and posterior crossbite. Early correction is needed if there is a mandibular shift. If there is no shift, treatment is delayed until eruption of the first molars. Treatment prior to adolescence and midpalatal suture closure is recommended.
Goals of palatal expansion:2. Arch expansion – groups of teeth are moved to expand the arch perimeter.
2. Repositioning of individual teeth.
Fixed appliances are reliable and require little patient cooperation. Removable appliances require greater patient cooperation and risk being lost or not used at all. Removables also mayb become dislodged with the strong forces used in expansion.
Fixed appliances:
W arch (36mil wire or Quad helix 38mil wire, more flexible, more wire). Quad Helix and W arch for treatment of palatal constriction. Gives skeletal and dental movement in the 3-6 year old.
By adolescence, more force may be required to separate the mid palatal suture as it starts to interdigitate. Rapid palatal expansion may be indicated. This consists of a mechanical screw device that is cemented or bonded, opened 0.5mm/day, 2000 to 3000g of force. Active treatment takes 10-14 days. Widens skeletally since PDL is hyalinized. After adolescence, the suture will probably be interlocked, making skeletal expansion impossible.
Slow palatal expansion gives 900-1300 g of force, 1mm/week. Widens skeletally and dentally. Expect 3-5mm of expansion. Lip bumpers or buccal shields work as well. Removable appliances:
Most are Hawley split plate type designs that use clasps to provide retention. Wire springs or jackscrews may be used to provide the expansion force.
14. Concerning the epidemiology of fluoride which of the following questions are true?
7. McKay was the first to note the mottling of enamel in Dental patients in Denver Colorado in 1902.
8. In 1944, in the famous Michigan fluoridation study, the city of Muskegon had 1 ppm of Fluoride added to its water supply and Grand Rapids was the control city.
9. In the Michigan study, caries incidence decreased about 50%.
10. In 1970 it was estimated that 7 million people in 1900 communities in the U.S. have been drinking natural fluoridated water with a concentration of >= to .7 ppm.
11. Adequate ingestion of Fluoride at an early age of enamel development is important in decreasing pit and fissure caries.
12. Fluoride decreases pit and fissure caries more than smooth surface caries.
A. 1,2,3,4 are trueB. 2,3,4,5 are trueC. all are trueD. 1,3,5,6 are trueE. 1,3,4,5 are true
The correct answer is E.Source is Fluoride and Caries Prevention 2nd edition Murray and Ruggs-Gunn p. 10-27.
Statements 1-3 are here for historical purposes. Statement number 4 addresses the safety issue of Fluoride therapy.
2 is false=Grand Rapids was the experimental city, the city officials of Muskegon were so impressed with the results of 50% reduction in caries experience in Grand Rapids that they added Fluoride to their water 6 years later-only negative was the control for the study was then lost after 6 years of results. 6 is false= fluoride ingestion may alter the morphology of pits and fissures decreasing their susceptibility, but Fluoride exerts its effect mostly on decreasing smooth surface caries.Source is Fluoride and Caries Prevention 2nd edition Murray and Ruggs-Gunn p. 10-27.
15. Which of the following are true concerning water lines in dental operatories?
9. The NIDCR has documentation of disease transmission arising from DUWL (Dental Unit Waterline microbial contamination.
10. The goal is to bring microbial content of dental water to no more than 200 CFU/ml.
11. Biofilms are microscopic communities consisting primarily of naturally occurring water bacteria and fungi that form thin layers on surfaces that remain in contact with water.
12. The CDC recommends not using water from dental water lines when performing surgical procedures and that the use of sterile irrigating solution should be used.
13. A prudent guideline is to run the handpiece for 45 seconds to 1 minute before each patient and at the end of the day.
14. These guidelines will reduce the biofilm formation in the waterlines.
15. Four categories of products to improve DWL’s are: independent water systems, chemical treatment protocols, point of use filters and sterile water delivery systems.
16. The EPA’s recommended drinking water standard is 500 CFU/ml of noncoliform bacteria, and Legionella pneumophila, Pseudomonas aeruginosa and non-tubercular mycobacterium have been isolated from DUWL’s.
A. All are trueB. 1,3,5,7,8 are trueC. 2,4,6,8 are trueD. 2,3,4,7,8 are trueE None of the above
The correct answer is D#1 is false- The NIDCR (National Institute of Dental and Craniofacial Research) has NO documentation of disease transmission arising from DUWL (Dental Unit Waterline microbial contamination. There is however irrefutable evidence that water delivered to most patients is of poor microbiological quality.#5 is false the guideline is to run the water for several minutes at the beginning of the day and 20-30 seconds after every patient. #6 is false- These guidelines will NOT reduce the biofilm formation in the waterlines- it only seeks to decrease the number of microorganisms present in the treatment water. To reduce the biofilm you must use a protocol of 5.25 % sodium hypochlorite diluted in a 1:10 ratio. Weekly 10 minute treatments improved the quality of the water and reduced the biofilm. You MUST have multiple treatments and COMPLIANCE is a big issue. Filters help a lot also-more $$.
SOURCE: JADA, Vol. 133 September 2002 p.1199-1206.
16. Which of the following can cause foggy films?
7. l. Light leaks in the darkroom
8. Incorrect bulb, or defective safelite filter or bulb.
9. Developer temperature too high.
10. Improper storage of film.
11. Contamination of the fixer in the developing solution.
12. Processing too fast or fixer solution is depleted.
A. All are trueB. 1,3,5,6 are trueC. 2,3,4,5 are trueD. 4.5.6 are trueE. 1,2,3,4 are true
The answer is E
1-4 are true causes of foggy films. #5 is false contamination of the fixer in the developing solution will cause brown discoloration of the film. #6 is false- processing too fast or fixer solution is depleted-will cause a Greenish-Yellow discoloration of the film.
The source is Principles and Practice of Panoramic Radiology-Langland, Langlais, and Morris, p. 82.
17. Which of the following are true concerning latex allergies?
8. Delayed allergies-Type IV-or irritant dermatitis, are caused by processing chemicals.
9. Immediate allergies are caused by antigens from Hevea brasiliensis trees where latex is harvested from=Immediate –Type 1 reaction. 5-10% of health care workers may have an immediate allergy to NRL.
10. In the 1980’s it was ascertained that natural rubber latex (NRL) allergy is An IgE mediated reaction.
11. Possible symptoms are- pruritis, urticaria, eczema, rhinitis, angioedema, asthma and possibly anaphylaxis.
12. Three common routes of transmission are-cutaneous, percutaneous, and mucous membrane through inhalation of aerosols.
13. Cerebral Palsy patients have a latex allergy incidence of 18-45 %.
14. The SPT is used to determine latex allergy.
A. all are trueB. 1,3,5,7 are trueC. 2,4,6,7 are trueD. 1,2,3,4,5,7 are trueE. 1,2,3,4,5,6 are true
The answer is DAll are true except #6- SPINA BIFIDA patients have an incidence of 18-45 %.SPT is skin prick test, this study quoted data taken from 2166 dental health care workers who volunteered to take the test at the ADA conventions over a two year period.
Source: JADA, Natural Rubber Latex Hypersensitivity: Incidence and prevalence of Type 1 Allergy in the Dental Professional, 1998, p. 43-54.
18. Moyers prediction table is used for mixed dentition space analysis. To utilize Moyers prediction, the mesiodistal width of the lower incisors is measured and this number is used to predict the size of the both lower and upper unerupted canines and premolars.
E) Both statements are true.F) Both statements are false.G) The first statement is true, second statement is false.H) The first statement is false, second statement is true.
Answer: A
Mixed dentition space analysis to estimate the size of the unerupted permanent teeth to calculate the space required. There are 3 basic approaches:
4. Measurement of teeth on Radiograph. A simple proportional relation is set up to estimate the size of the unerupted permanent teeth.
5. Estimation from proportional tables. Most predictions are based on American white school children
Moyers: the mesiodistal width of the lower incisors is measured and this number is used to predict the size of the both lower and upper unerupted canines and premolars from the table.
Tanaka and Johnson: small bias to over estimate. ½ mesiodistal width of 4 lower incisors + 10.5mm= mandibular unerupted
canine and premolars in one quadrant.½ mesiodistal width of 4 lower incisors + 11.0mm= mandibular unerupted canine and premolars in one quadrant.6. Combination of radiograph and prediction table
Stanley and Kerber: Canine width to be estimated directly from the sums of incisors and premolar widths using a graph. Only for mandibular arch.
Tooth size analysis: to determine the disproportion among the sizes of individual teeth (as tooth size discrepancy). If the discrepancy is 1.5mm or greater, it should be included in the problem list.
Bolton Analysis: is determined by measuring the mesiodistal width of each permanent tooth. A standard table is used to compare the total width of maxillary and mandibular anterior teeth and the total width of all upper and lower teeth.
19. SNA angle measures the relative anteroposterior relationship of the maxilla to the anterior cranial base. SNB angle measures the relative anteroposterior relationship of the mandible to the posterior cranial base.
E) Both statements are true.F) Both statements are false.G) The first statement is true, second statement is false.H) The first statement is false, second statement is true.
Answer: C
SNA angle (Steiner) (827) formed by intersection of the planes Sella-Nasion and Nasion-Point A. measures the relative anteroposterior relationship of the maxilla to the anterior cranial base.
SNA angle greater than 82 would indicate a forward or prognathic position of the maxilla relative to the anterior cranial base. Less than 82 would indicate a retrognathic position of the maxilla.
SNB angle (80) measures the relative anteroposterior relationship of the mandible to the anterior cranial base.
20. FMA angle is formed by the intersection of Frankfort horizontal plane and the (Down’s) mandibular planes. As the FMA increases the amount of vertical growth exceeds horizontal growth and the chin is more posterior.
E) Both statements are true.F) Both statements are false.G) The first statement is true, second statement is false.H) The first statement is false, second statement is true.
Answer: A
FMA angle (25) is formed by the intersection of Frankfort horizontal plane and the (Down’s) mandibular planes (tangent to the lower border of the mandible and the lowest point on the symphsis, Menton). It determines mandibular growth pattern and directions.
As the FMA increases the amount of vertical growth exceeds horizontal growth and the chin is more posterior.
High mandibular plane angles are frequently associated with unfavorable vertical growth and anterior open bites.
Low mandibular plane angles are associated with horizontal mandibular growth and deep bites.
21. Which of the following statement is (are) correct?
5) Sterilization strip changes color on exposure to sterilization temperature.6) The indicator strip is placed on top of the packaging.7) The spore of the bacteria Bacillus stearothermophilus is used to test the
reliability of heat sterilization.8) The spore test is used bimonthly to judge the effectiveness of sterilization
technique and equipment.
A) 1, 2B) 2, 4C) 3, 4D) 1, 3
Answer: D
Sterilization strip changed color on exposure to sterilization temperature. It doesn’t indicate duration of sterilization cycle. The indicator strip is placed in the most interior part of the packaging.
The spore of the bacteria Bacillus stearothermophilus is used to test the reliability of heat sterilization. The spore test is used weekly to judge the effectiveness of sterilization technique and equipment.
Dry heat oxidizes the cell proteins where as moist heat causes coagulation of proteins quickly. Dry heat requires higher heat for longer time to achieve sterility.
Autoclaving: pressurized steamTemp Pressure Duration of treatment115C 10 PSI 60 min121C 15 PSI 24 min126C 20 PSI 16 min
Advantages: effectiveness and speed. Disadvantages: Cost of the autoclaves, and dull and rust instrument.
Contemporary Oral and Maxillofacial Surgery, Peterson, Ellis, Hupp and Tucker, 3rd ed, 1998, p 73-77.
22. Which of the following statement is (are) incorrect?
4) It is important to intrude a tooth rapidly to gain periodontal attachment. 5) Excessive force may produce necrosis of the PDL and adjacent alveolar bone.6) The physiologic extrusion or intrusion is when the alveolar bone is brought
along with the tooth.
A) 1B) 2C) 3D) 1,3E) None of the above
Answer: A
To successfully intrude a tooth, it requires careful control of magnitude so that very light forces are applied to the tooth and the force will be concentrated in a small area at the tooth apex. Tooth is expected to tip somewhat as it is being intrude.
If the tooth is intruded, the bone height tend to be lost at the alveolar crest, so that about the same percentage of the root remains embedded in bone as before, even if the intrusion was over a considerable distance.
The bone support around periodontally involved teeth could be improved by intruding the teeth and forcing the roots deeper into the bone; but this doesn’t lead to soft tissue attachment.
Physiologic extrusion or intrusion that brings the alveolar bone along with the tooth, followed by gingival and osseous recontouring is preferable.
23. The use of orthodontic headgear can be utilized to treat Class I, Class II and Class III malocclusions. The most common type of headgear is designed to treat the Class III malocclusion.
A. Both statements are trueE. Both statements are falseF. First statement is true, second statement is falseD. First statement is false, second statement is true
Headgear is used for growth modification, molar correction, vertical control, root torque and dental movement. There are designed to treat Class II malocclusion and Class III malocclusion.
Class II headgear is implemented in the following types: High Pull, Cervical Pull, and Combination Pull. These types change Maxillary Apical Base (ANB) in retarding the advancement of maxillary molar position. The high pull rests on the crown of the skull and is designed to place forces in an upward distal manner. The cervical pull rests on the back of the neck and is designed to place only distal forces. The combination rests in both positions and place more distalising forces than upward.
Class III headgear is implemented in the following types: Chin Cup and Orthopedic Face Mask. These types correct the sagittal-vertical relationship. The chin cup applies a force to against mandibular growth and is for short-term restriction, redirects growth, and is utilized infrequently by orthodontists. The orthopedic face mask (a.k.a. reverse pull) is attached to maxillary molars and rests on the forehead and chin and does the above as well but primarily protracts the maxilla
Answer is B both statements are false.
Moles, J. A. NPDS, NNDC, Orthodontic 240, lecture: Growth Modification dated 18 Nov 02
Anthony D. Viazis. Atlas of Orthodontics: A guide to Clinical Efficiency
24. Which series of radiographs would you order for a new 6-year-old patient exam?
a. M&M occlusals, posterior BWx, Panorex b. M&M occlusals, R&L M&M primary molar PAx, posterior BWx Panorex c. M&M ant PAx, posterior BWx, R&L M&M Primary molar Paxd. R&L M&M primary molar PAx, Posterior BWx, lateral ceph, Panorex
The ADA’s suggested radiographic protocol for a new pediatric patient exam is as follows:
G. AGE RADIOGRAPHS_________3-5 y/o: No apparent abnormalities, open contacts -None
No apparent abnormalities, closed contacts -2 posterior bitewings Abnormalities / Caries -Series of 4 films
2 posterior BWx M&M occlusals
Extensive or deep caries -additional selected PAx
6-7 y/o: No apparent abnormalities -Series of 8 films M&M occlusals (PAx) R&L max post 1o PAx R&L mand post 1o PAx R&L posterior BWx Panoral
Extensive or deep caries -additional selected PAx
8-9 y/o: No apparent abnormalities -Series of 12 films 2 incisor PAx 4 cuspid PAx 4 1o premolar/molar PAx 2 posterior BWx Panoral
10-12 y/o: No apparent abnormalities -Series of 12 or 16 films In addition to the above, 4 quadrant permanent molar PAx
All high caries risk patients receive new BWx at the 6-month recall visit. Standard BWx is done in 12-month cycles. The Pan-oral radiograph is indicated following eruption of the first permanent tooth.
The correct answer is B. M&M occlusals, R&L M&M primary molar PAx, posterior BWx Panorex
McDonald, R.E., Avery, D.R., Dentistry for the Child and Adolescent 7th Edition. Mosby 1999. Pages 64-67.
25. List the LeFort classifications in order of decreasing severity:
e. Class I, Class II, Class III, Class IVf. Class III, Class II, Class Ig. Class IV, Class III, Class II, Class Ih. Class I, Class II, Class III
In 1901, the Frenchman Rene LeFort published three consecutive papers on the now famous classification of facial fractures. His work described the great lines of weakness in the face through which most fractures occur by using low velocity impact forces directed against cadaver skulls. These lines, where the facial bones break in trauma, have become known as the LeFort I, II, and III fractures.
The Lefort I fracture, or transverse fracture, extends through the base of the maxillary sinuses above the teeth apices essentially separating the alveolar processes, palate, and pterygoid processes from the facial structures above. This transverse fracture across the entire lower maxilla separates the alveolus as a mobile unit from the rest of the midface. Fracture dislocations of segments of the alveolus may be associated with this fracture. With high-energy injuries, the palate may be split in the midline in addition to the LeFort I fracture.
The LaFort II fracture is synonymous with a pyramidal fracture of the maxilla. This fracture pattern begins laterally, similar to a LeFort I, but medially diverges in a superior direction to include part of the medial orbit as well as the nose. The fracture extending across the nose may be variable, involving only the nasal cartilage or as extensive as to separate the nasofrontal suture. The fracture extends diagonally from the pterygoid plates through the maxilla to the inferior orbital rim and up the medial wall of the orbit to the nose. This separates the maxillary alveolus, medial wall of the orbit and nose as a separate piece.
A LeFort III fracture or craniofacial dysjunction denotes a complete separation of the midface or facial bones from the cranium. This fracture transverses the zygomaticofrontal suture, continues through the floor of the orbit, and finally through the nasofrontal suture. The bones of the orbit are separated through the lateral wall, floor, and medial wall. It is unusual to have this fracture as a single segment of bone; more commonly, it comminutes with varying combinations of zygomatic, nasoethmoid, and orbital fractures. The fractures may not be symmetric on both sides and minimal mobility may be present.
The LeFort IV fracture is a figment of my imagination that tends to run freely at such this late hour during which I am typing this question for all of you. I hope you appreciate it.
The correct answer is B. Class III, Class II, Class I
e. All of the Abovef. 1, 2, 4 g. 1, 2, 3h. 1, 3, 4
A pulpotomy is the removal of the coronal portion of the pulp of both primary and permanent teeth with carious exposures. Justification for carious exposure is that the coronal pulp tissue contains microorganisms and inflammatory products. Healing can take place in the canals of the normal pulp tissue. Most commonly performed with formocresol to fix the amputated tissue remaining in the orifice, then restoring the tooth with IRM and stainless steel crown
Contraindications are listed as follows: non-restorable teeth, teeth nearing exfoliation, spontaneous or provoked discomfort, periapical or furcal pathosis, internal or external resorption, lack of hemostasis from amputated pulp stumps, fistula, parulis, purulent pulpal discharge, pulpal calcification, pathologic mobility.
For permanent teeth, if the exposure is tramatic and not too large or not a significant amount of time has passed since the injury a Cvek (partial) pulpotomy can be preformed when the coronal pulp inflammation is not wide spread. This preserves as much of the health tissue as possible for maturation of the tooth, root and apex.
The correct answer is C. Asymptomatic carious pulp exposure, inflammation confined to the coronal aspect of the pulp not extending radicularly, healthy periradicular tissues, mildly symptomatic tooth
McDonald, R.E., Avery, D.R., Dentistry for the Child and Adolescent 7th Edition. Mosby 1999. Pages 421-425, 498-500.
27. Which of the following statements regarding fluoride is (are) true?
5. Fluoride absorbs to the crystal surface of enamel attracting phosphate ions, followed by calcium ions leading to new mineral formation.6. Advantages of fluoride varnish are they:
- contain high concentrations of fluoride- are applied locally/topically- are protective- are surface active- do not stain teeth
7. The most popular in-office fluoride is 8% SnF28. The typical over-the-counter dentifrice contains 2000 ppm of fluoride.
a. all of the aboveb. none of the abovec. 1,2,3d. 4 onlye. 2
Answer: b. none of the above
1 – calcium ions are attracted first followed by phosphate ions.2 – fluoride varnish can stain.3 – Sodium fluoride is the most popular.4 – the typical over-the-counter dentifrice is 1000 ppm of fluoride
28. What is the appropriate dosage for supplemental fluoride for 5-year-old children who live in a non-fluoridated water area and what is the proper concentration in the drinking water for a community with a fluoridated water program?
AGE Less than .3ppm .3-.6ppm Over .6ppmNo Flouride ½ dose Ideal flouride
Birth-6 mos 0 0 06mos-3years .25 0 03-6 years .5 .25 06-16 yrs 1.0 .50 0
There is currently some controversy here since there is 1mg of flouride in a toothbrush size strip of toothpaste and children frequently ingest much of the toothpaste they use. Additionally, there is fluoride present in many of the beverages children drink today including some bottled water.
Pediatric Dentistry. Vol.24, No.7pp66
29. Increasing kVp will will increase the contrast of the film image. Decreasing the mA will increase the density of the film image.
e. The first statement is true, the second is falsef. The first statement is false, the second is trueg. Both statements are false.h. Both statements are true
Answer: c
High contrast is observed with fewer shades of gray and is better for viewing endodontic files in the canals. Many practitioners use 70 kVp for endo and 90 kVp for caries detection. Low contrast is more desirable for caries diagnosis. Increase of kVp and mA will both increase density. Density is the degree of blackness of a film.
Langland, Langlais Principles of Dental Imaging. Pp53,54
30. Serial extractions are recommended in class I malocclusions, (skeletal and Dental) when the space discrepancy is > 6mm but < 13mm. The first extractions are the primary 1st molars when the underlying premolar has 2/3 root formation completed.
a. The first statement is true and the second is false.b. The first statement is false and the second is true.c. Both statements are trued. Both statements are false.
Answer: a
The first extractions are the primary canines and they are removed as soon as all mandibular permanent incisors are erupted. An evaluation for serial extractions is done at age 8 when there is evidence of crowding. After age 8, there will be continued growth of the arches without an increase in arch length.
Glossary of Dentofacial Orthopedic Terms-Orthodontic Glossary-American Association of Orthodontists
Operative Dentsitry1. Indirect composite materials have physical characteristics that include which of the following?
1. Some of the polymerization shrinkage occurs outside of the mouth, but the most of the polymerization occurs inside the tooth upon delivery.
2. One potential advantage is a slightly higher degree of polymerization is attained.3. Laboratory processing may employ heat and pressure.4. These resins have greater color stability than light-activated resins.5. Bond failures and induced stresses are reduced
a. 1, 2, 3b. 1, 2, 3, 4c. 2, 3, 4, 5d. 2, 4, 5e. all of the above
The polymerization shrinkage occurs outside of the mouth, not in the tooth, which improves the physical properties and resistance to wear. The polymerization shrinkage does not occur in the tooth. This reduces induced stresses and bond failures. This will theoretically reduce the potential for leakage. These resins are also repairable in the mouth and are not as abrasive to opposing tooth structure as ceramic inlays.
Laboratory processing may employ heat (140 C) and pressure (0.6 MPa for 10 minutes). This polymerization under heat and pressure is used for a homogeneous microfilled resin that is claimed to have a higher filler content, less porosity and greater color stability than light-activated resins. In addition, a slightly higher degree of polymerization (degree of conversion) is attained.
The following are additional physical properties of laboratory composites:Flexural strength is high-90-150 MPaFlexural modulus is variable-4.7-15 GPaCompressive strength is 210-280 MPaHandling characteristics and properties:Advantages-best anatomy and contacts, lower wearDisadvantages-lab cost, special equipment, requires resin cement
1. Is incorrect as noted above. The polymerization occurs completely outside of the mouth.
The correct answer is c. (2, 3, 4, 5.)
Extra notes to recall about all composites (direct) regarding repair: A restoration that has just been cured and polished may have up to 50%of unreacted methacrylate groups to copolymerize with the newly added material. As the restoration ages, fewer and fewer unreacted methacrylate groups resin, and greater cross-linking reduces the ability for fresh monomer to penetrate into the matrix. Then strength of the bond between the original material and the added composite resin decreases in direct proportion to the time that has elapsed between the original polymerization and the addition of new composite. In addition, it should be noted that the polishing step would expose filler particles that are free from silane coating, which will inhibit a chemical bond to the new composite. The strength of the repair composite is less than ½ of the original material.
2. The following statements are problems with bonding agents and solutions in various environments or clinical situations. Choose which of these combinations are correct.
1. Problem: Debonding of a composite core build-up occurred during removal of an impression. Solution: Compatible composite core material should be used. Certain self-cured composite cores are incompatible with certain light cured bonding agents. Choose a dual cured bonding agent or used a light –cured composite core material.
2. Problem: A dentist etched tooth structure prior to using a 6th generation bonding agent.Solution: Sixth generation bonding agents bond effectively to enamel and dentin without prior etching with phosphoric acid. The additional etching could result in over etching of dentin and may lead to nanoleakage.
3. Problem: After etching, a dentist over dried the tooth.Solution: Most modern bonding agents bond best to a moist tooth surface. Dentin should be rehydrated by applying a moist cotton pellet until the dentin surface glistens before applying the primer of the bonding agent.
4. Problem: A ceramic restorative surface has fractured on your patient with a 3-unit anterior FPDPFM, exposing only the fractured porcelain.Solution: The fractured surface should be isolated, prepared and then micro-etched with 50 um aluminum oxide particles; it is then treated with 5-9% hydrofluoric acid for 4 minutes; ; it is then treated with silane to wet the surface and act as a chemical coupling agent; then the bonding system is applied and light cured; and finally, the composite material is applied incrementally and light cured.
5. Problem: A dentist uses a standard unfilled bonding agent to bond a laboratory composite restoration.Solution: Bonding requires agents for both the tooth structure and the undersurfaces of the indirect restoration.
a. 1. is correctb. 1 and 2 are correctc. 1, 2, and 3 are correctd. 1, 2, 3, and 4 are correcte. all of the above
Correct answer is e. all of the above.
Answers for # 1-4 contain self-explanatory responses.Answer for #5 can be best explained as follows:
Resin composite cements are used to fill the space between the laboratory composite and the tooth surface. Bonding to the indirect composite surface is difficult. The goal is to swell the outer surfaces of the resin matrix and allow new monomers from the bonding agent to penetrate spaces among existing polymer chains. At the time of curing, the new polymer chains become micromechanically intertwined with the existing polymer chains, producing relatively strong bonding. Bonding can be enhanced by micro etching with aluminum oxide (50um) etching with hydrofluoric acid, or treating with primers. Sandblasting roughens the surface. Etching removes smear layers and partially dissolves glass filler particles. Primers provide good wetting and potential chemical bonding to exposed glass filler particle surfaces. Commercial primers foe laboratory composites contain silane, unfilled resin monomers, or silane-monomer combinations. Bonding composite cements to laboratory composites can produce bond strengths in the range of 20-35 MPa.
The formation of an optimally bonded interface has the following:1) the surface of the substrate be clean;2) the adhesive wets the substrate well and has a low contact angle;
3) adapts to the substrate to produce intimate approximation of the materials without entrapped air or other intervening materials;
4) the interface include the sufficient physical, chemical and or mechanical strength to resist intraoral forces of debonding; and
5) the adhesive be well cured in the “environment” or conditions for which they are to be used.
3. Regarding environment and biocompatibility (toxicity), which one of the following is not true?
2. The term biocompatible is defined in Dorland’s Illustrated Medical Dictionary as being harmonious with life and not having toxic or injurious effects on biologic function.
3. Biocompatibility is measured on the basis of localized cytotoxicity.4. Naturally occurring mercury can be found in large cold water fish with
concentrations that often exceed FDA limits. 5. Ten percent of the female population is allergic to nickel, compared with only about
1% of the male population. 6. Berylliosis is a disease resulting from contact dermatitis of some RPD alloys.
b. 1.c. 2.d. 3.e. 4.f. 5.
1. Is a true statement.2. Is true. Biocompatibility is measured on the basis of localized cytotoxicity (such as pulp
and mucosal response), systemic responses, allergenicity, and carcinogenicity.3. Is true. Methylated mercury accumulates in the food chain and is derived from areas of
undersea volcanic acidity and hydrothermal waters. Virtually 100% of methyl mercury is absorbed in the gut. Thus, conversion of elemental mercury to methyl mercury would greatly increase absorption via the gastrointestinal route. All of the mercury in seafood is methyl mercury and all is absorbed. The average contribution of one seafood meal per week to blood mercury levels of methyl mercury is many times that of the aberage contribution of elemental mercury from the presence of 8-10 amalgam restorations in the mouth.
4. Is true. Ten percent of the female population if allergic to nickel, compared with only about 1% of the male population. This disparity is attributed to the greater exposure of females to nickel. Almost all gold plated jewelry is made with a nickel undercoat beneath the gold plating Only about 30% of those patients with a known nickel allergy develop a reaction to an intraoral nickel-chromium dental alloy.
5. Is false. Berylliosis is an inflammatory lung disease resulting from the inhalation of beryllium dust or fumes. Beryllium containing alloy should be ground with adequate ventilation.
The correct answer is e. (5 is a false statement).
4. Onlay preparation design for porcelain includes all but which of the following?a. Cuspal onlay preparations should have a 2.5 to 3.0 mm reduction in
vertical height of the cusps and all occluding areas.b. Preparation should have finish lines on any supporting cusps that are
hollow ground chamfers, generally with no bevel.c. Well-rounded angles on the cuspal preparation.d. The typical well-defined internal line and point angles of cast-metal
restorations are rounded for porcelain and the pulpal floor should be indented.
e. Slightly more divergent axial walls than for conventional cast metal inlay.
a. Is the correct answer -It is a false statement: the reduction should incorporate a 1.5- to 2.0 mm reduction in vertical height and all occluding areas. The adhesive nature of the bonded restoration makes the traditional approach of additional preparation to protect unsupported cusps or to develop additional resistance form unnecessary. Removal of additional tooth structure to onlay cusp is contraindicated.
b. Is a true statement The hollow ground chamfer is used to expose and increased number of enamel rods for increased bond strength, increased marginal seal, and a transition for better esthetic color blend. A bevel could lead to fracture of porcelain due to the friability of the thin edge of porcelain. c. Is a true statement: There should be well-rounded angles on the Cuspal preparation, to prevent propagation of porcelain fracture from these sharp stress points.d. Is a true statement: GV Black’s original concepts for restorations demanded
sharp, definitive line angles. These are contraindicated in any form of porcelain restoration. All line and point angles are of necessity rounded. This facilitates the laboratory fabrication and decreases the propagation of fractures within the restoration. The cavity preparation should be indented in the pulpal floor to develop even thickness of porcelain in the restoration in the central fossa region to parallel the cuspal inclines. This allows for a thickness of porcelain in the center that is similar to that on the lateral aspects of the restoration.
e. Is a true statement: The axial walls of the cavity preparation should be slightly more divergent from the pulpal floor toward the enamel surface than would be prepared for a conventional cast-metal inlay, where the 6-10 degree taper is commonly favored to develop retention. Increased taper of the axial walls allows easier placement and removal of the restoration during the true-in phase, but the taper should not be exaggerated so as to unnecessarily remove additional tooth structure.
Reference: Porcelain and Composite Inlays and Onlays. Garber DA and Goldstein RE
5. Glass Ionomer differ from a compomer (polyacid modified resin)in which ways.
1. Compomers contain both composite and glass inomer2. Glass ionomer releases less fluoride than compomers3. Glass inomers use polyacrylic acid4. Compomers have improved physical properties over glass ionomers
Answers: a. 2, 3, and 4b. 2 and 4c. 1 and 2 d. 1, 3, and 4
The answer is D.
Answer 2 is not correct. Conventional glass ionomers release fluoride into the surrounding tooth at a greater amount that compomers. This gives them a higher anticariogenic effect. Glass ionomer have low wear resistance, and relatively low strength compared to composite or amalgam. Compomers have improved strength and wear resistance with the combination of composite and glass ionomer.
Roberson T.M., Heymann H.O., and Swift E.J. Studervant’s Art & Science of Operative Dentistry, Fourth Edition, Mosby Inc. 477-478.
6. Which of the following statement(s) distinguishes a flowable composite from a regular composite.
1. Flowable composite have equal filler content but just smaller particles when compared to regular composites.
2. Flowable composite have lower filler content3. Flowable composites have favorable wettability4. Flowable composite have lower wear resistance and increased strength.
A. 1, 3, and 4B. 1 and 4C. 2 and 3D. 3 and 4
Answer 1. is incorrect since flowable composite achieves its ability to flow by decreasing the amount of filler particles.
Answer 4. is not correct since flowable composite has decreased strength.
Flowable composites have lower filler content which make it have inferior physical properties such as lower wear resistance and decreased strength. It does have increased wettability. Indications are limited to Class 1 restorations, pit and fissure sealants, cavity liners and margin repair materials.
The answer is C.
Roberson T.M., Heymann H.O., and Swift E.J. Studervant’s Art & Science of Operative Dentistry, Fourth Edition, Mosby Inc. 477-478.
7. Which of the statements concerning veneer designs are acceptable veneer designs?
1. A facial veneer that does not include the incisal edge is acceptable.2. An incisal lapping veneer preparation is contraindicated in most situations. 3. The incisal lapping preparation is ideal to lengthen the tooth.4. The margins should always be subgingival
Answers:
A. 1 and 2B. 1C. 1, 3 and 4D. 1 and 3
Veneers can be made of composite; lab processed composite, porcelain or pressed ceramics. The gingival margin should be supraginigival unless the defect, discoloration, or caries extends below the gingival margin. An acceptable design involves the incisal edge that can extend to the lingual surface. This is useful to lengthen the tooth and cover stain or defects on the incisal edge. The incisal lapping preparation is not contraindicated with porcelain and may be used in most situations. There is a potential increase in wear of the opposing dentition with the incisal edge lapping design. A veneer preparation does not have to include the incisal edge.
The answer is D.
Roberson T.M., Heymann H.O., and Swift E.J. Studervant’s Art & Science of Operative Dentistry, Fourth Edition, Mosby Inc. 615-618.
8. Which gives the best results for caries prevention?
a) Low dose/high frequency fluoride
b) High dose/low frequency fluoride
c) High dose/high frequency fluoride
d) Low dose/low frequency fluoride
Answer is a) Low dose/high frequency fluoride
According to Featherstone, primary benefits of are had with a continuous low level of exposure of aqueous fluoride in contact with enamel in the presence of calcium and phosphate ions.
Chronic excessive fluoride intake during tooth development may bring about fluorosis.1ppm fluoride in drinking water is the optimal amount needed for caries prevention before any signs of fluorosis appears.
Remineralization-demineralization balance theory indicates 0.2 to 1.0ppm Fluoride lowers the solubility of enamel.
In vitro experiments have shown that concentrations of Fluoride in range of 100ppm reduce sensitive bacteria population. Sublethal concentrations alter carbohydrate metabolism by reducing acidogenicity, altering the production of extra cellular insoluble polysaccharides, and possibly reducing adhesion.
Fluoride concentration in saliva rarely exceeds a few ppm. Effect of additional Fluoride on plaque metabolism is insignificant except for individuals with reduced saliva flow < 0.5ml/min.
Featherstone, JDB, The science and practice of caries prevention. JADA 2000; 121:887-899Phillips Science of Dental Materials 11th ed., Anusavice, K.J. P447-9
9. What is role of Indium in amalgam?
a) To reduce Hg release during masticationb) To reduce Hg release during abrasion of set amalgamsc) To reduce Gamma two phase d) To reduce Gamma phase
Answer: a) To reduce Hg release during mastication
Composition of amalgam:Alloy type: %Silver %Tin %Copper %ZincConventional low copper 65-70 21-29 2-4 0-2High copper 40-60 26-30 6-28 0-2 Indium (5-15% wt.) is added to reduce the release of Hg during mastication, and during and after setting.Zinc is a deoxidizer (oxygen scavenger) during manufacturing. It decreases brittleness. It may decrease corrosion and improve marginal integrity.Higher copper alloys have high early strength, low creep, good corrosion resistance, and good resistance to marginal fracture. High copper alloys reduce gamma two phase (weaker). Silver and tin are the major components of amalgam, combining with Mercury to produce an amalgam with varying working properties.Palladium is added to enhance mechanical properties and corrosion resistance.
Vaporization of Hg from Hg-in amalgams during setting and after abrasion. Ferracane, Materials in Dentistry, Stannard, J.G. 1986 Denali PublishingDental Materials and Their Selection 2 nd Ed., O’Brien WJ, 1997 page 189 Restorative Dental Materials 10 th Ed., Craig, R.G. 1997 page 210
10. Which is not desired in a Class I amalgam preparation design?
a) Shallow preparation <1.5mmb) Preservation of well supported enamelc) Parallelism of opposing wallsd) Smooth cavosurface outline form
Answer : a) Shallow preparation <1.5mm
Class I Amalgam tooth preparationElimination of caries, preservation of tooth structure, remove enamel that is undermined by caries.Routine extension in non carious fissures and pits is no longer justified.Occlusal cavosurface bevel is contraindicated in these preparations.Outline should include only faulty and defective occlusal pits and fissures.Avoid sharp angles in marginal outline.Need 90-100 degree cavosurface angle.Opposing walls need to be parallel or converge slightly to the occlusal table for retention form.Keep facial and lingual margin extensions as minimal as possible between the central groove and the cusp tips.Sufficient depth (>1.5mm) to give adequate thickness of the restoration.Parallelism or slight occlusal convergence of external walls.Preparations (faciolingually) exceeding the intercuspal distance should have remaining cusps evaluated for restoration.
Conservative Class I Composite tooth (adhesive) preparationLimit removal of tooth structure to amount needed to remove caries and severely thinned enamel.Preparation tends to be shallower than in amalgam preparations.Retention is provided by bonding, no need to penetrate enamel if caries does not.Preserve as much enamel as possible to improve bonding, preparation can be shallower.Preparation should be narrower to limit occlusal wear and reduce polymerization shrinkage.Rounded internal line angles which enhances resin adaptation. No extension for prevention. Occlusal pits only include if there is caries, they can be treated with sealants. An axial and/or pulpal wall of varying depth (not uniform) is allowed.Enamel does not have to be fully supported by dentin.
Ref:Sturdevant, C.M., Sturdevant’s Art and Science of Operative Dentistry 4 th Ed. 2002
11. Bevel margins are indicated in:1. Gold castings2. Dentin margins on composite restorations3. Enamel margins on composite restorations4. Glass Ionomer restorations5. Resin-modified glass Ionomer restorations 6. Porcelain restorations
a) 1, 2, 4, 6b) 1, 3, 5, 6c) 1, 3d) 1, 3, 5e) None of the above
Answer: (c) The bevels for cast metal may slightly improve retention form when they are
opposing bevels. The bevels for cast metal are primarily to afford a better junctional relationship
between the metal and the tooth. Enamel margins of composite restoration have a beveled or flared configuration
to increase both the surface area of etchable enamel. Enamel margin of composite restoration is to maximize the effectiveness of the
bond by etching more enamel rods ends. The porcelain, resin-modified glass ionomer restorations and glass ionomer
restorations require butt-joint (bulk of material at the margin) due to the brittleness and low tensile strength.
Sturdevant’s Art and Science of Operative dentistry 4th Edition. P-298
12. Which of the following is not the indication of miniflaps?
a) Class V lesions with difficult moisture control.b) Restorative margin is significantly deep gingivally.c) Limited access and visibility.d) Gingival margin of the restoration is at the crest of the bone.
Answer: (d) When carious lesion extends gingivally enough that a soft tissue flap is necessary for adequate access and visibility. Proper surgical procedures must be followed including sterile technique, careful soft tissue management and complete debridement of the operating site prior to wound closure. When the gingival margin of the restoration violates the biologic width (Gingival margin of the restoration is less than 3mm from the crest of the bone) osseous crown lengthening may be necessary.
The design of the “mini-flap” is: intersulcular incision around the tooth (or the surface that you need access for restoration), full-thickness flap with small vertical releasing incisions not extending beyond the mucogingival junction. Flap is repositioned at the previous coronal height (note: not apically positioned) and suture may be necessary.
Sturdevant’s Art and Science of Operative dentistry 4th Edition. P- 744
13. Which of the following statement(s) on the mercury hazard is(are) false?
1. Mercury in the environment is bioaccumulative.2. Mercury in the form of dental amalgam is very stable, but when incinerated
mercury may be released to the environment.3. Amalgam sludge is the mixture of liquid and solid material collected within
vacuum pump filters or other amalgam capture devices.4. Mercury can be recovered from amalgam waste through a distillation
process and reuse in new products.5. ADA recommends recycling as a best management practice for dental offices.
a) 1b) 2c) 3d) All of the abovee) None of the above
Answer: (e) Majority (87%) of mercury released to the environment comes from combustion
of fuel and waste. Dentistry contributes less than 1%. Mercury is present in numerous chemical forms. Methylated mercury compounds
and Elemental mercury are toxic. Elemental or inorganic forms can be transformed into organic forms by biological systems.
Some mercury released into the air eventually collects in waterways and then enters the food chain. Amalgam in environment is bioaccumulative, which means that it can build up in fish and cause health problems in any animals that eat fish.
Dental Amalgam is a solid intermetallic compound, quite different from elemental, cationic and organic mercury. Dental amalgam is very stable.
REF: ADA BMP, 2003.
14. How do dentinal tubules change as you approach the pulp?
1. Tomes fibers are absent as you approach the pulp.
2. There are 45,000-60,000/mm2 near the pulp.
3. The lumen diameter decreases to .5 to .9 um near the pulp.
4. The tubules are straighter in the incisal ridges, cusps and root areas.
a. 1 and 2 are trueb. 1,2,3 are truec. 2, 4 are trued. All the above are true
Thus the answer is C.
Each dentinal tubule contains cytoplasmic cell processes (Tomes fibers) of an odontoblast. There is no mention of them being absent as you approach the pulp.There are 15,000-20,000/mm2 at the DEJ and this INCREASES to 45,000-60,000/mm2 at the pulp. The lumen in the coronal dentin is .5 to .9 um then INCREASES to 2-3 um at the pulp. The tubules have a slight S-curve to them in the crown, but are straighter in the incisal ridges, cusps and root areas.
SOURCE: STURDEVANTS ART AND SCIENCE OF OPERATIVE DENTISTRY 4TH EDITION. page 23.
15. What makes a glass ionomer a true glass ionomer?
1. It must have an acid-base reaction (i.e. metal + acid= salt). You must mix materials together to have a true glass ionomer.
2. Calcium ions are gradually replaced by Aluminum ions to produce a more cross linked, more mechanically stronger material.
3. Glass ionomers are materials consisting of ion-cross linked polymer matrices surrounding glass-reinforcing filler particles.
4. Fluoride is an integral part of the matrix formation.
5. Polyacrylic acid may be freeze dried-(anhydrous) and combined with aluminosilicate powder.
6. Water is a key ingredient for the setting reaction.
A. All the above are trueB. none are trueC. 1,2,4 are trueD. 1,2,3,5,6 are trueE. 4,5,6 are true
Answer is DSOURCE: CAPT Cook’s lecture on Glass Ionomers, page 5,6.SOURCE: STURDEVANTS ART AND SCIENCE OF OPERATIVE DENTISTRY 4TH EDITION. Page 207-211.It must have an acid-base reaction (i.e. metal + acid= salt). You must mix materials together to have a true glass ionomer. Calcium initially and the later aluminum replaces the hydrogen ions on the carboxyl groups resulting in the post set hardening stage.Glass ionomers are materials consisting of ion-cross linked polymer matricessurrounding glass-reinforcing filler particles. Fluoride is NOT an integral part of the matrix formation, therefore it is available for release without compromising the structural integrity of the restoration. Polyacrylic acid may be freeze dried and combined with aluminosilicate powder. The freeze dried form is called anhydrous, there also is a semi-hydrous form available. Water is a key ingredient for the setting reaction, it is critical for the reaction to occur. The water hydrates the salts and allows them to crosslink. Too much water results in an opaque weakened restoration, if water is lost during setting crazing will occur.
16. Which of the following advantages for the curing lights are true?
1. Quartz-Tungsten-halogen curing lites- 90% of the light produced is suitable for curing. Output ranges from 400-800 mW/cm2.
2. Plasma arc curing units-PAC- curing times can be as low as 3-10 seconds. This produces a much more rapid polymerization resulting in decreased polymerization stresses and stronger bond strengths.
3. Laser curing lights-curing times can be as low as 3-10 seconds.
4. Light emitting diode (LED) lights-Allows one to generate the appropriate wavelength in a narrow spectrum and curing cycle.
5. Stepped cure lights-may allow the newly formed polymer network to stress-relax and eliminate strains before completion of the curing cycle.
a. 1,2,3 are trueb. 2,3,4 are truec. All the above are trued. All the above are falsee. 3,4,5 are true
The answer is E.The quartz bulbs only produce 0.5% of light suitable for curing. Most is converted into heat. UV and infrared filters eliminate unnecessary light . Output is in the range of 400-800 mW/cm2. Curing times for Lasers and PAC lights are advertised as 3-10 seconds. The fast cure can however cause INCREASED polymerization stress and DECREASED bond strengths. LED’s are advertised as allowing one to generate the appropriate wavelength and curing cycle for the many products on the market. Camphoroquinone is the photoinitiator most used in composites. Stepped cure lights (Elipar 1997) used 100 mW/cm2 for 10 seconds, then 600 mW/cm2 for 30 seconds this shows some promise in decreasing polymerization stresses.SOURCE: STURDEVANTS ART AND SCIENCE OF OPERATIVE DENTISTRY 4TH EDITION. page 198-202.
17. Indicate the optimum restorative material to restore a G.V. Black Class V cavity prep restoring a suspected abfraction lesion on a maxillary anterior.
The common theory accepted for the causative agent of abfraction lesion is of an occlusion orgin. Excessive flexion of the tooth causes compression and relaxation at below the CEJ which forces a fluid exchange to occur. This exchange of fluid also carries with it elements of the tooth structure matrix.
In restoring these types of lesions one must take into account several factors. The majority of the margins will exist on dentin/cementum. Enamel may only be present at the occlusal margin. The material chosen should be able to withstand the flexion forces experienced by the tooth, lesion’s position in the esthetic zone, and patient’s caries risk status.
It is accepted that Glass ionomers have the more favorable, low flexural strength and low modulus of elasticity to withstand these forces. As well, they have a chemical bond to tooth structure, and a coefficient of thermal expansion close to that of natural tooth structure. But their wear resistance is low and esthetics fair. For these reasons this restorative procedure would call for a Sandwich Technique where the prep is restored with a GI on all dentin margins, then a veneer of Resin on the enamel margins to esthetically cover some of the GI leaving the GI/dentin margins exposed.
The correct answer is e. Glass Ionomer / Microfill Composite Resin
-Amalgam would not serve the esthetic needs and has a very high modulus of elasticity.-Hybrid Composite is esthetic but flexural strength is high and no true chemical bond to tooth structure, only micro-mechanical can be made to tooth structure.-Compomers are an option because they are a blend between a GI and Resin. You get a bit of the chemical dentin bond, better wear resistance, some fluoride release, and a bit more flexion.-Glass Ionomer alone has the bond and flex needed and also supplies optimum fluoride release if it is needed, great bond to dentin, flexural strength and thermal expansion similar to tooth structure, but poorer esthetics an low wear restsiance.
18. Which is the correct sequence of reaction stages of Glass Ionomers?
a. Decomposition, gelation, maturation, migration, post-set hardening b. Migration, decomposition, maturation, gelation, post-set hardeningc. Decomposition, migration, gelation, post set hardening, maturationd. Migration, gelation, decomposition, post set hardening, maturation
Glass Ionomers are supplied as powders of various shades and a liquid component. The powder is an ion-leachable calcium fluoro-alumino-silicate glass, and the liquid is a water solution of polymers and co-polymers of acrylic acid. (Although polyacrylic acid is the original, Currently the acid is in the form of a copolymer with Itaconic, Maleic, or Tri-Carboxylic acid. Tartaric acid is also present as it improves the handling characteristics and increases the working time) The material sets through an acid-base reaction in the presence of water. As a result, metallic salt bridges form between the Al++ and Ca++ ions leached from the glass and the acid groups on the polymers. The resulting glass ionomer matrix will bind both the glass particles and water into a cement structure that will contain up to 24% water. Water in a glass ionomer ensures effective 'wetting' of moist tooth surfaces for strong adhesion. Water bound in a mature glass ionomer facilitates continuous fluoride release and uptake, benefiting adjacent tooth surfaces. The reaction goes to completion slowly, with the formation of a cross-linked gel matrix in the initial set and an aluminum ion exchange strengthening the cross-linking in the final set.
A chelation effect takes place with the calcium in the apatite on the exposed tooth surface, creating an ionic adhesive bond. The surface on the new restoration should be protected from saliva during initial set with a varnish or light cured bonding agent.
Types based on their formulation and potential uses:Type I: Luting agentsType II: Restorative materialType III: Liner and bases
The correct answer is c. Decomposition, migration, gelation, post set hardening, maturation
Decomposition - acid reacts with glass, release of metal ionsMigration – ions migrate into aqueous solutionGelation – metal ions gel and initiate cross-links,
Created 1st are Calcium polysalts, 2nd are Aluminum polysaltsPost-Set Hardening – ions become bound, cross-links continueMaturation – increased cross-linking, decreased free water, improved physical properties.
19. Place the following types of G.V. Black cavity preps in order of increasing C-Factor: Class 1, Class 2, Class 4
a. 1, 2, 4b. 2, 4, 1c. 4, 2, 1d. 2, 1, 4
During polymerization the organic matrix of a composite resin can undergo volumetric shrinkage on the order of 2% ~ 7%. This contraction crates stresses at the hybrid layer upwards 18 MPa. These forces can severely strain the bond between composite and tooth structure. This leads to Marginal gap formation, microleakage, stress cracking of composite, or enamel fractures along the margins.
The degree of stress development can be controlled to an extent by the cavity design, expressed in C-Factors, uses of bases, the size, shape, and position of increments, light or chemical curing. Most important and easily controlled in respects to stress relief can be accomplished by maintaining the C-Factor as low as possible.
The calculation of C-Factor is the number of bonded surfaces verses non-bonded surfaces. The higher number of tooth structure walls that will be bonded to yields a higher C-Factor. Conversely the fewer number of tooth structure walls the lower the C- Factor. Thus a standard cavity preps represent the following: Class 1 preps have 5 bonded to 1 non-bonded for a C-Factor of 5. Two surface Class 2 preps have 4 bonded to 2 non-bonded for a C-Factor of 2. Class 3 preps have 4 bonded to 2 non-bonded for a C-Factor of 2. Class 4 preps have 1 to 4, C-Factor 1. Class 5 varies according to depth and can range from 1 to 5. Of course multi-surface Class 2 (MOD, MODB, ETC), 3 (MFL, DFL), and 4 (MIFL, MIDFL) have lower C-Factors than the standard preps in that there are more non-bonded surfaces than bonded.
Answer is c. 4, 2, 1
To compensate for this contraction the following should be factored in to the procedure:All enamel margins, incremental fill, highly filled material (less matrix = less shrinkage, don’t bridge cusps, clear matrix.
Carvalho, R.M. et al. A Review of Polymerization Contraction : The Influence of Stress Development verses Stress Relief. Oper Dent 1996 (21): 17-24 {source of photo}20. What are the predominate microbes are involved in root caries?
a. Fusobacteriumb. Actinomycesc. S. mutansd. Lactobacilluse. Fusobacterium
A: b. The predominate microbes involved in root caries are Actinomyces according to the cited text here. The NIH publication on Diagnosis and Management of Dental Caries Throughout Life claims that convincing data on the source of infection by cariogenic bacteria almost entirely pertain to mutans streptococci. Caries originating on the root is alarming because: (1) it has a comparatively rapid progression, (2) it is often assymptomatic, (3) it is closer to the pulp and (4) it is more difficult to restore
OPERATIVE DENTISTRY, 3rd ed. Sturdevant
21: Primers have excellent ability to wet a surface when they form a high contact angle. A liquid with a relatively low surface tension coefficient will have improved surface wetting properties.
a. The first statement is true, the second is false.b. The first statement is false, the second is truec. Both statements are trued. Both statements are false.
R. A: b
The contact angle is a measurement formed by the balance of energies between the liquid and solid. A higher contact angle means more “bubble-like” and hence poorer wetability.
Surface tension is measured in terms of force (dynes) per centimeter of the surface of liquid. The higher the surface tension, the less the wetability. Some examples at 20 C follow:
1-benzene 29 dynes2-water 72.83-mercury 465
These values are influenced by temperature and purity. Higher temperatures and impurities, especially detergents, decrease surface tension. Just remember:
HIGH SURFACE TENSION OR HIGH CONTACT ANGLE = POOR WETABILITY.
Restorative Dental Materials,11th ed. Craig and Powers
22. Which of the following statements regarding the prep design and characteristics of Glass Ionomer and RMGI are true?
a. A 2mm 45 bevel should be evident at the enamel margins to enhance bonding.
b. All margins should be 90c. Occlusal depths should be at least 3mm deep to allow for thickness of
material for strength.d. Internal line angles should be rounded
A: b,d
A beveled margin would allow for a thin layer of restorative material, more prone to fracture than a 90 cavosurface margin. GI restorative material should not be used in occlusal load areas due to poor wear resistance. Sharp line angles will allow voids under the restorative material since the material lacks adequate flow characteristics. Polyacrylic acid is the agent of choice to remove the smear layer.
1. Question: Clinical presentation of Gardner’s Syndrome may include which of the following?
1. Intestinal polyps.2. Multiple osteomas of the mandible.3. Odontomas and supernumerary teeth.4. Hyper-pigmentation of vermillion border.5. Epidermoid cysts of the skin.6. Multilocular radiolucencies of the mandible.
A. 1,2,3,4B. 3,4,5,6C. 1,2,3,5D. All of the aboveE. None of the above
Answer: C
Gardner’s Syndrome. Rare disorder. May occur at any age. Autosomal dominant.Near 100% penetrance. 1/3 are spontaneous, and represent new gene mutations.Gene found on chromosome 5. Is a part of spectrum of diseases characterized by familial colorectal polyposis. Affects the skin, soft tissues, retina, skeletal system, and teeth.
Occur in 1:8,300 to 1:16,000 of live births.Colonic polyps happen in second decade.They are adematous and transform into adenocarcinomas. Extra colonic polyps possible in small intestine and stomach.
Clinical PresentationUp to 90% of those afflicted have skeletal abnormalities.Osteomas are the most common associated abnormality.Skull, paranasal sinuses and mandible.Mandibular angles, facial deformity.Noted during puberty, and precede the bowel polyps.Osteomas present as radiodensities. Increased incidence of odontomas and supernumerary teeth.One or more epidermoid cysts of the skin.Desmoid tumors (fibrous neoplasms) 10%, 3X more in females.Less common is thyroid carcinoma. Females have it 100X more than males.
S. Treatment and PrognosisHigh rate of malignant transformation to invasive adenocarcinoma.By age 30 , 50% of those with the syndrome will get colorectal carcinoma. Malignant change reaches 100% in older patients.
Prophylactic colectomy recommended. Some osteomas may be removed for function, but the polyps are the main factor.
Other syndromes with intestinal polyposis:Peutz-Jegher’s SyndromeCowden’s SyndromeTurcot’s Syndrome
2. People with well controlled diabetes are no more susceptible to infections than people without. Antibiotic prophylaxis of patients with diabetes is dependent on host factors and invasiveness of the procedure.
A. First statement is true, second statement is falseB. First statement is false, second statement is trueC. Both statements are trueD. Both statements are false
Answer: C
-People with well controlled diabetes are no more susceptible to infections than people without. They do however have more difficulty containing existing infections. This is due in part to altered leukocyte function.-Elective oral surgery in poorly controlled patients should be deferred until control is accomplished. -In the case of an emergency or where a serious oral infection exists, consideration should be given to have the patient admitted to a hospital to manage hyperglycemia and have aggressive management of the infection. Penicillin therapy is initiated. If response is poor, sensitivity testing is used to help choose a more effective antibiotic.
General Surgical Guidelines-Routine antibiotic prophylaxis of patients with controlled diabetes undergoing surgical procedures is controversial. -Surgical procedures must have a high incidence of infection for prophylactic antibiotics to reduce the incidence of infection.-The incidence of infection after tooth extraction, frenectomy, biopsy, minor alveoloplasty, and torus reduction is extremely low, antibiotics would provide no benefit.(These are considered routine in office dental procedures.)
These are factors that may lend themselves to antibiotic coverage.1) Size of bacterial inoculum2) Extent and time of surgery3) Presence of foreign body (including implant placement)4) State of host resistance
Extensive dental procedures in poorly controlled diabetes can also elevate the blood pressure and increase the potential for cardiac or cerebrovascular incidents as well as transient bacteremias and infections.
Contemporary Oral and Maxillofacial Surgery, Petersen, Ellis , Hupp, Tucker, 3rd Ed. 1998 Mosby. Page 16, 410.Ellenberg and Rifkin’s, Diabetes Mellitus, Porte and Sherwin 1997 Appleton and Lange Page 1231Dental Management of the Medically Compromised Patient, Little and Falace, 6th Ed, P266, Mosby 2002
3. TNM cancer staging system stands for Tumor, Nodes and Metastasis.Stage 4 (T3 N1 M1) has better prognosis than stage 2 (T2 N0 M0).
I) Both statements are true.J) Both statements are false.K) The first statement is true, second statement is false.L) The first statement is false, second statement is true.
Answer: C
Clinical staging is of greater importance than histopathologic grading in predicting biologic outcome.
Tumor T1: <2 cm T2: 2.1 to 4.0 cmT3: >4.0 cmT4: >4.0 cm with infiltration of muscles or bone
Nodes N0: No palpableN1: 1 ipsilateral node <3 cmN2a: 1 ipsilateral node 3.1-6.0 cmN2b: Multiple ipsilateral nodes <6 cmN2c: bilateral nodes <6 cm or contralateral nodesN3: node>6 cm
Metastasis M0: no distant metastasisM1: Distant metastasis
Staging:Stage T N M
1 1 0 02 2 0 03 3 0 0
1-3 1 04 4 0 0
1-4 2-3 01-4 1-3 1
Stage 2(T2 N0 M0) has better prognosis than stage 4(T3 N1 M1).
5. Which of the following statement regarding Prothrombin time is false?A) PT measures the effectiveness of the intrinsic coagulation. B) A normal PT indicates normal levels of factor I, II, V, VII and X.C) Normal PT ranges from 10 to 15 seconds, and is usually compared to a daily
control value.D) A prolonged PT can be associated with abnormal postoperative coagulation
and bleeding.
Answer: A
PT measures the effectiveness of the extrinsic coagulation. It is performed by measuring the time it takes to form a clot when calcium and a tissue factor are added to the patient’s plasma. A normal PT indicates normal levels of factor VII and those factors common to both the intrinsic and extrinsic pathways (V, X, Prothrombin(II) and Fibrinogen (I)). Prolongation of less than one and a half times the control value is usually associated with mild bleeding disorders, while further prolongation indicates a more severe bleeding disorder. The PT is used to monitor oral anticoagulant therapy.
International Normalized Ratio (INR): For patients on chronic oral anticoagulants, to report the PT ratio. Using an international sensitivity index (ISI) which is determined for each batch of reagent and is specific to the lab’s particular equipment, the calculation of INR= (patient PT/normal PT) ISI . For most conditions that require ongoing anticoagulation therapy, AHA has recommended INR levels between 2.0 and 3.0.
6. A radiograph is interpreted to have a lesion(s) with a “cotton wool appearance”. What is/are the most likely causes of this?
A. Paget’s disease of boneB. Gardner syndromeC. Cemento-ossesous dysplasiaD. Gigantiform cementomaE. All of the above
Answer: E
All of the following diseases can present with a “cotton wool appearance”. Paget’s is more common in older adults and mainly in the maxilla. Gardner syndrome also has multiple osteomas; epidermoid cysts; gastrointestinal polyps with a high tendency toward malignant transformation and is hereditary. Cemento-osseous dysplasia predominates in middle-aged black women and usually in the mandible. Gigantiform cementoma is hereditary and facial enlargement may be present.
7. Which of these is a painless benign tumor of the salivary glands most often found on the palate?
A. Adenomatoid hyperplasia of the minor salivary glandsB. Pleomorphic adenomaC. Adenoid cystic carcinomaD. Warthin’s tumor
The answer is A.
Pleomorphic adenoma is the most common salivary neoplasm. It makes up most of the parotid tumors. It is also called the benign mixed tumor. It is a painless slow growing mass and is most common in adults between 30 and 50 years old.
Warthin’s tumor is benign and is only in the parotid gland. It is a slow growing nodular mass in the parotid gland and it can occur bilaterally. It is usually in older adults. Surgical removal is the treatment of choice.
Adenoid cystic carcinoma is common salivary malignancy. It can occur in any salivary gland tumor with 50% in the minor salivary glands. It is common in palatal salivary glands. It is rare in ages under 20 more common in middle age adults.
Adenomatoid hyperplasia of the minor salivary glands is rare lesion that mimics a neoplasm. Most often it is a swelling in the hard or soft palate. They are most common in the fourth to six decades of life. They are painless and soft to firm to palpation.
Oral and Maxillofacial Pathology, Neville, 1995. Pages 337-359
8. Nonsteroidal Anti-Inflammatory Agents (NSAID) can cause decreased effectiveness of ACE inhibitors, hydralazine, diuretics and other hypertensive medications. It may also decrease the effectiveness of anticoagulants (warafin and heparin).
G. Both statements are trueH. Both statements are falseI. The first statement is true and the second is falseJ. The first statement is false and the second statement is true
The correct answer is C.
NSAIDs will increase the effectiveness of anticoagulants. NSAIDs may increase warafin’s effect on INR and exacerbate the adverse renal effects of ACE inhibitors. It may increase risk of GI ulceration when used with corticosteroids. Lithium, methotrexate and cyclosporine levels may be increased. CYP2C8 and 2C9 enzyme substrate interactions can occur. Avoid ethanol intake. Pregnancy risk factor is C and D in the third trimester. It may be taken while breast-feeding. Peak serum concentration occurs 1-2 hours after ingestion. Contraindications are hypersensitivity to NSAIDs, aspirin or other NSAIDs.
NSAIDs are broken down in the kidneys.
NSAIDs inhibit prostaglandin formation by decreasing the cyclooxygenase.
CNS disruption, confusion, agitation, or hallucinations are seen with high doses.
Wynn, Miller and Crossley. Drug Information Handbook for Dentistry. Sixth Edition; 2000: 551-552.
9. Which of the following are true concerning traumatic bone cysts?
1. Generally the patient complains of a deep bone pain.2. Radiographically present as a well-demarcated radiopacity.3. Upon aspiration a thin serous fluid will be expressed.4. Easily confused with an apical periodontal cyst.5. Are best treated by surgical enucleation.
A. 1, 2, 3 are trueB. 3,4,5 are trueC. All are trueD. None are trueE. 1,3,5 are true.
The answer is D.
Traumatic bone lesions (hemorrhagic or extravasation cysts) are localized areas of bone necrosis that are purported to result from intramedullary hematomas that do not become organized. The intraosseous hemorrhage is thought to be related to a traumatic incident. The bone lesions are discovered during a routine dental exam (not a pain related visit). They appear as a well-defined radiolucency most frequently near the apices of teeth but are NOT related to periapical inflammation. The teeth in the vicinity will test positive for vitality and thus be differentiated from apical periodontal cysts. Exposure of a traumatic bone cyst will reveal a DRY bony cavity with no cystic lining.
REFERENCE: Robinson’s Color Atlas of Oral Pathology page 126.
10. WHICH OF THE FOLLOWING ARE TRUE CONCERNING HEPATITIS C?
1. Also called non-A, non-B Hepatitis. It is a viral infection.
2. It is the most common chronic blood borne infection in the U.S.
3. Responsible for 30,000 deaths per year or 30% of those infected.
4. The causative agent=double stranded RNA, can modify and mutate within the host.
A. All the above are true.B. 1,2,3 are true.C. 3,4, are trueD 1,2,3,4 are true.
The answer is A.
Also called non-A, non-B Hepatitis. It is a viral infection. It is the most common chronic blood borne infection in the US. Responsible for 30,000 deaths per year or 30% of those infected. The causative agent is a SINGLE stranded RNA, which can modify and mutate within the host.
REFERENCE: The Liver’s Epidemiology Lecture, LCDR Outhouse, Hepatitis C (HCV) lecture by LCDR Carpenter. From Guyton, Textbook of Medical Physiology, 10th ed., Little, Dental Management of the Medically Compromised Patient 6th ed., Glick, Medical Considerations for Dental Care of Patients with Alcohol-Related Liver Disease: JADA Vol 128 Jan 1997.
11. Which of the following are true concerning Addison’s disease?
1. Characterized by weight loss, muscle weakness, fatigue, low blood pressure, nausea, vomiting, diarrhea, and darkening of the skin in exposed and unexposed areas.
2. It occurs because the kidneys do not produce enough cortisol and aldosterone hormones.
3. Most cases-70%, are caused by the body’s own immune system destroying the adrenal cortex. Tuberculosis is a secondary cause.
4. Type 1 occurs in children-hypoglycemia is common, Type 2-also called Schmidt’s syndrome occurs in adults and may include vitiligo-loss of pigmentation on skin.
5. Addison’s Disease can cause irritability and depression and craving of salty food is common.
A. All are true.B. 1,2,3 5 are true.C. 1,3,5 are true.D. 1,3,4,5, are true.
The answer is D
#2 is False- cortisol and aldosterone are of course produced by the Adrenal Glands located just above the kidneys. 1,3,4,5 are TRUE.Addisonian crisis is where a stressful event like an illness or an accident causes the symptoms to suddenly become much worse. It is also called an acute adrenal insufficiency. Symptoms would be 1. sudden penetrating pain in the lower back, abdomen or legs, 2. severe vomiting and diarrhea, followed by dehydration, 3. low blood pressure, 4. loss of consciousness. Treatment involves replacing or substituting cortisol and aldosterone if it is deficient. Crisis therapy would involve IV hydrocortisone, saline, and dextrose.
Resource:National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda MD, November 1998. Corrigan , Eileen K.
12. Which of the following statements is false regarding the disease, erythema multiforme?
A. EM is seen most frequently in middle-aged females and older adults taking multiple medications.
B. EM has an acute onset.C. EM simplex is a self-limiting form of the disease D. Oral lesions commonly appear along with skin lesions in approximately 70%
of EM patientsE. The pathognomonic lesion is the target lesion
The correct response is A. It is false; all other responses are true.
Below are explanations and amplifying information of the acute inflammatory immune mediated disease of the skin and mucous membranes:
EM is seen most frequently in children and young adults and is rare after the age of 50 years.
EM has an acute or explosive onset; generalized symptoms such as fever and malaise appear in severe cases.
EM simplex is a self-limiting form of the disease and is characterized by macules and papules 0.5 to 2 cm in diameter, appearing in a symmetric distribution.
The most common cutaneous areas involved are the hands, feet, and extensor surfaces of the elbows and knees. The face and neck are commonly involved. Only severe cases will affect the trunk. Oral lesions commonly appear along with skin lesions in approximately 70% of EM patients. The oral lesions may occasionally be the predominant form or single site of the disease. The oral lesions are an important part of the clinical picture. These lesions are usually rapidly rupturing vesicles and bullae.
Typical skin lesions of EM are target lesions which are macules or papules with a central area of petechiae. Hence, the pathognomonic lesion is the target or iris lesion. A central bulla or pale clearing area will be surrounded by edema and bands of erythema.
The more severe vesiculobullous forms of the disease, Stevens-Johnson syndrome and TEN have a high mortality rate. EM is classified as Stevens-Johnson syndrome when the generalized vesicles and bullae involve the skin, mouth, eyes, and genitals.
The most severe form of the disease is TEN (toxic epidermal neurolysis), which is typically secondary to a drug reaction and results in sloughing of the skin and mucosa in large sheets. Morbidity occurs in 30-40% of patients and is due to secondary infection, fluid and electrolyte imbalance or involvement of the lung, kidneys or liver. These patients are managed best in burn centers. The necrotic skin is removed under general anesthesia. Xenografts may be used to allow healing of the tissues.
Reference:Greenburg and Glick.: Burkett’s Oral Medicine; BC Decker, Inc.,10th Ed.,2003.
13. Which one of the following is false regarding recurrent aphthous ulcers (RAU’s)?A. The most common oral manifestation of Crohn’s disease is RAU’s.B. Recurrent aphthous ulcerations (RAU’s) are caused by the Coxsackie virus.C. The three disease entities of RAU’s are minor, major and herpetic.D. Diagnosis is based upon clinical and histologic examination.E. Major (recurrent) aphthous ulcerations are larger than 1.0 cm, minor
ulcerations are smaller then 1.0 cm.
Correct answer is B. It is a false statement.
Recurrent aphthous ulcerations (RAU’s) are idiopathic ulcerations. Diagnosis of RAU’s is of exclusion; the clinical impression may be confirmed with histologic examination and by response to treatment.
The three disease entities of RAU’s are minor, major and herpetiform. Minor (recurrent) aphthous ulcerations are smaller than 1.0 cm, well-
circumscribed, round, may have a yellow-gray pseudomembrane, and surrounded by a erythematous halo. Differential diagnosis includes recurrent HSV infection. Treatment is focused to provide symptomatic relief. Analgesic mouth rinses: 2% -4% viscous Lidocaine solution (10 ml swished and expectorated) is the most commonly used. Kenalog in Orabase may also be used.
Major (recurrent) aphthous ulcerations are larger than 1.0 cm. They are well-circumscribed, round, and shallow or deep with indurated margins. A gray pseudo membrane covering the lesion may sometimes be present. They can occur anywhere on the oral mucosa. They are usually single ulcerations. In immunosuppressed individuals, groups of up to 10 lesions can be observed. These ulcers persist for more than 3 weeks and tend to heal with scar formation. In patients with HIV, major (recurrent) aphthous ulcerations have been associated with severe immune suppression, with CD4 counts below 100 cells/mm3, and are markers for HIV disease progression. Treatment for major (recurrent) aphthous ulcerations includes administrations of systemic corticosteroids. Topical formulations include: clobetasol or fluocinolide gel applied directly to the lesion, dexamethasone elixir mouth rinses (0.5 mg/5ml), and systemic administration of 60-80 mg of prednisone per day for 10 days have been used successfully. In steroid resistant patients, alternative therapy of 100-200 mg thalidomide may be used. It has severe side effects, but, has been used with some success to treat both oral and esophageal ulcerations. Refractory cases can be treated with colchicines or levamisole. Antibiotics and antifungal agents may also be used concurrently to prevent bacterial or fungal superinfections.
Herpetiform ulcers are the least common type of aphthous ulcers; they are smaller than 1 mm, with perilesional erythema. They are found in batches of up to 100 on the nonkeratinized mucosa such as the ventral surface of the tongue and soft palate. Treatments are similar to those for minor RAU’s: symptomatic relief, suppression of the local pathologic immune reaction, and treatment of concomitant superinfection.
Reference: Greenburg and Glick: Burkett’s Oral Medicine; BC Decker, Inc.,10th Ed.,2003.
14. The vital sign that varies the least with odontogenic infections is:
A. Respiratory rateB. Blood PressureC. PulseD. Temperature
Answer: B
Only if there is significant pain and anxiety will there be a mild elevation in systolic pressure.
Patients who have systemic involvement of infection will have elevated temperatures. Patients with severe infections will have temperatures elevated to 101 to 102F.
Pulse rates of up to 100 beats per minute are not uncommon in patients with infections. A patient with a pulse rate over 100 may have a severe infection and should be treated more aggressively.
The normal respiratory rate is 14-16 breaths per minute. Patients with mild to moderate infections have elevated respiratory rates of up to 18-20 breaths per minute. As respirations are monitored, the dentist should carefully check to insure that the upper airway is clear and that breathing is without difficulty.
Oral and Maxillofacial Surgery, Peterson et al. pp 397-398
15. The hepatitis B surface antigen (HbsAg) is the first detectable specific marker in the diagnosis of acute HBV infection. HbsAg appears in the blood usually by the fourth week of infection and is followed within a week by the hepatitis B early antigen (HbeAg)
A. The first statement is true, the second is false.B. The first statement is false, the second is trueC. Both statements are trueD. Both statements are false
Failure to produce anti-HbsAg results in a chronic carrier state. Carriers persistently display HbsAg in their serum for over 6 months.
HbeAg in a carrier’s serum indicate an infectious state.T. Essentials of Oral Medicine. Silverman et al pp 155
16. Patients may be encountered that may be identified, upon diagnosis, as harboring the organism Helicobacter pylori. Treatment with antibiotics can oftentimes aid in correcting the ulcerative disease. Which of the following medications is not used for this treatment?
The three P’s are Proton Pump inhibitors and Gastric Acid Secretion Inhibitors.
Drug Information Handbook for Dentistry-Wynn et al. pp1136
17. From the choices below, identify the most common minor salivary gland malignant tumor.
A. Pleomorphic adenomaB. Adenocystic carcinomaC. Midline lethal granuloma
D. Mucoepidermoid carcinoma
The answer is B. Adenocystic carcinoma
The minor salivary glands in the oral cavity can sometimes develop malignant tumors. As a rule, tumors in the minor salivary glands have a greater tendency towards malignancy compared to tumors in the major salivary glands (parotid, submandibular and lingual). They are usually covered by mucosa and mainly found in the hard palate [9]. Adenocystic carcinoma dominates (50 %), followed by mucoepidemoid cancer while pleomorphic adenoma is a benign type of tumor that exists in only 10 per cent of the minor and in 85 per cent of the major salivary glands. Adenocystic carcinoma has a major recurrence tendency. Surgery entails resectioning of part of the soft and hard palate, which communicates directly with the nose or jaw cavities.
Mucocele is the most common lesion in the minor salivary glands with a prevalence of 0.1 per cent [3]. It is localized in the lips, mainly the lower lip and cheeks. It is not a real tumor, but rather mucus retention in one or several of the minor salivary glands in the lip mucosa. In the upper lip adenomas can be found, requiring fine-needle puncture to secure the diagnosis. The lesions are benign but often traumatized, e g when chewing or in connection with bad bite habits, and excision is recommended.
Sialolith or salivary stone represents deposition of calcium salts around a central nidus of cellular debris and mucinous material. Trauma and bacterial or viral infections are among the most common causes.
Approximately 80% of all sialoliths affect major salivary glands and 75% of these are found in the submandibular gland. Minor salivary gland sialolithiasis is mostly found in the upper lip and buccal mucosa. Many sialoliths can be removed by manual manipulation of the stone through the ductal orifice
19. Which of the following is not contraindicated for use in an asthmatic patient?
A. PenicillinB. Nitrous OxideC. AspirinD. Naproxin SoduimE. 2% Lidocaine with 1/100K levonordeferin
The correct answer is B. Nitrous oxide
Drugs that might be implicated in precipitation asthmatic episodes should be avoided, such as Aspirin, NSAIDs, penicillin, and bisulfites. The prevalence of aspirin sensitivity in asthmatics ranges up to 19%. The NSAIDs include indomethacin, femoprofen, naproxin, ibuprofen, mefenamic acid, sulindac, meclofenamate, tolmetin, piroxicam, oxyphenbutazone, and phenylbutazone.Sodium metabisulfate, an antioxidant in certain medications, have been known to cause attacks. Although the volume in dental local anesthetics containing vasopressors is minimal reactions have been noted. LA without vasopressors should be used
Barbiturates sensitize the respiratory reflexes and increase the risk of bronchospasms. Narcotics provoke histamine release and increase the risk of bronchospasm.Both drug groups are contraindicated in the asthmatic patient. Inhalation sedation with nitrous oxide and oxygen, oral sedation with benzodiazepines, and IV or IM routes are not contraindicated in asthmatics.
Malamed, S.F., Medical Emergencies in the Dental Office, Mosby1993, pages 197-19820. Which of the following reversal agents would you administer to a patient who has been overly medicated with a narcotic analgesic?
A. MaziconB. Sodium bicarbonateC. NarcanD. Epinephrine
Answer is C. Narcan
There are four categories of injectable drugs used for the management of emergency situations that arise in response to the administration of drugs used primarily for sedation or general anesthesia. The antidotal drugs are:
The most significant side affect of parenternally administered narcotic agonist is their ability to produce respiratory depression by diminishing the responsiveness of the respiratory centers of the brain to the arterial carbon dioxide level. Duration of action of Nalaxone is 30 minutes. It is common to give a patient IM dose to assist
Although the benzos have been described as the nearly the most ideal agents for anxiety control and sedation, there are still a number of adverse reactions associated with their administration. Flumazenil is recommended to be available whenever diazepam, midazolam, or lorazepam is administered.
Drugs that induce sedation have the ability to produce what is knows as emergence delirium a phenomenon in which the patient appears to lose contact with reality and speech is unintelligible. This has the potential to occur with the use of scopolamine and benzodiazepines. Side affects are hypersalivation, emesis, urination, defecation, bradycardia. (Atropine should be available as an antagonist.) Physostigmine should not be administered to pts with asthma, diabetes, cardiovascular disease, GI or GU obstructs.
Vasodilators are used in the management of vasospasm and compromised circulation following accidental intraarterial injection of medications or extravascular administration of an irritating agent.
U.
Malamed, S.F., Medical Emergencies in the Dental Office, Mosby1993, pages 87-88
ENDODONTICS1. 6% Sodium Hypochlorite provides which of the following:
1. gross removal 2. lubrication3. destruction of microbes4. dissolution of tissues5. **Adding a chelating agent (like EDTA) adds for the removal of
the smear layer.
a. 1,2b. 3c. 2,3
d. 1,2,3,4,5
Dilution of NaOCl reduces the dissolution power. The smear layer consists of organic and inorganic debris present on the surface of dentin after instrumentation. It represents dentinal shavings, tissue debris, odontoblastic processes, and (in previously infected root canals) microbial elements. There is a controversy over whether or not to remove this layer before obturation. The smear layer biologically, has been postulated as the avenue for leakage and a source of substrate for bacterial growth and ingress. Chelating agents remove the smear layer, soften dentin, and facilitate the removal of calcified obstructions. If sealed in the canal, they can soften the dentin throughout the canal system in between visits.
Methods for the removal of the smear layer before obturation have primarily focused on the alternating use of a chelating agent (i.e. disodium ethylene diamine tetra-acetic acid [EDTA]) or weak acid (i.e., 10% citric acid), followed by thorough canal rinsing with 3% to 5% sodium Hypochlorite (NaOCl). The routine use of these techniques, however, has not been universally advocated, and the long-term value of smear layer removal has not been elucidated. Disadvantages:If expressed significant pain is experienced.Foul tastingGreater than size 25 file and you may express it if you use force.Corrosive to plumbing.The answer is d all the above.
Source: Pathways to the Pulp 8th Edition p. 545-546.
2. Patient presents with a sinus tract leading to the base of a periodontal pocket of tooth #3 and there is calculus present on the root surface. The tooth tests non-vital. What is your sequence of treatment?
a. Periodontal therapy, initiate NSRCT at the same visitb. Periodontal therapy, wait 10-12 weeks then NSRCT c. NSRCT and gross scaling; periodontal therapy 10-12 weeksd. Either of the above treatment is appropriate
The correct answer is c. NSRCT and gross scaling; periodontal therapy 10-12 weeks. Classification of Endodontic-Periodontic Lesions1. Primary Endodontic lesions2. Primary Endodontic lesion with secondary periodontal disease3. Primary periodontal lesion4. Primary periodontal lesion with secondary Endodontic involvement5. True combined endo and perio lesions
3. Plaque and calculus results in formation of periodontal pocket.
1. Necrotic pulp2. Loss of
attachment3. Plaque and
calculus4. Not consistent
with periodontal health
5. Angular defect may be present in area of endodontic problem
1. NSRCT2. If calculus is
present, gross scaling
3. Healing not complete in 10-12 weeks – periodontal therapy
Primary perio 1. Periodontal disease
1. Vital pulp2. Periodontal
disease3. Pockets – broader
and more coronal4. Sinus tract traces
to base of pocket
Periodontal therapy
5. Plaque and calculus present at root surface
Primary perio with secondary endo
Periodontal disease causes pulpal necrosis
1. Necrotic/ irreversible pulpitis
2. Periodontal disease
3. Probe: broader and more coronal
4. Sinus tract to base of the pocket
5. Plaque and calculus present on root surface
1. NSRCT2. Gross scaling if
calculus present3. If complete
healing not observed after 10-12 weeks, institute periodontal therapy
True combined endo and perio lesions
1. Independent endo and perio lesion
2. Chronic perio and long standing periradicular pathosis
3. Vertical root fracture
4. Maxillary laterals-palatal grooves.
1. Necrotic pulp2. Periodontal
disease3. Plaque and
calculus present4. Radiographic
“tear drop” or ”J”
1. NSRCT2. Gross scaling if
calculus is present
3. If complete healing is not observed after 10 to 12 weeks, institute periodontal therapy.
4. Vertical root fracture – extraction
Periodontal lesions: usually wide base, swelling usually involves the attached gingiva above the mucogingival junction.Endodontic lesions: usually are vestibular occurring below the mucogingival junction.
Taken from Cohen S, Burns RC, (2002) Pathways of the Pulp 8th Ed. Mosby
3. Which of the following techniques would you employ when treating a C-shaped canal?
a. the use of ultrasonics for debridementb. chemically softened gutta perchac. heat softened gutta perchad. a,be. a,c
The correct answer is e. the use of ultrasonics for debridement and heat softened gutta percha. Chemically softened gutta percha is used for blunderbuss roots with the eucapercha technique.
Ref: Cohen and Burns: Pathways of the Pulp by, 7th EdMelton DC et al: “Anatomical and histological features of C-shaped canals in mandibular second molars.” J Endod 17(8): 384-8
C-shaped canals have a wide variation of canal anastomoses, webbings, and irregular communications. The wide orifices and small surface area of these canals preclude completed debridement using traditional hand instrumentation techniques. Alternative canal cleaning techniques are more effective; these include ultrasonics to increase the removal of debris in inaccessible areas of the root canal system, and an increased volume of irrigants. These canal systems are better obturated using techniques that heat soften the gutta-percha and enhance its movement into the canal irregularities.
Incidence of C-shaped canals:4% of mandibular second molars had one root with a C-shaped canal.
In the study by MELTON, it was found that there was a considerable amount of debris and un-instrumented canal space in the middle and apical 1/3 of the root. Due to this material remaining, root non-instrumentation, thinness of root remaining and possible perforations may explain why some second molar root canal treatments fail.
4. Which statement(s) concerning Periodontal Ligament Injection are correct: 1. A 27-gauge short needle is firmly placed into the periodontal space
between the root of the tooth and the interseptal bone.2. A volume of 0.2 ml of anesthetic is slowly deposited on each root of the
tooth. 3. The most significant contraindication to PDL injection administration
is the presence of infection or inflammation in the areas of needle insertion.
4. Successful PDL injection anesthesia is indicated by the presence of resistance to anesthetic deposition
5. Successful PDL injection anesthesia is indicated by ischemia (whitening) of the soft tissues in the immediate area on injection of the anesthetic.
a. 1, 3, & 4b. 1, 2, & 5c. 1, 2, 3, & 4d. All of the above are correct
A: c. 1,2,3,4 are correct
The PDL injection, or intraligamentary injection (ILI), is frequently used in restorative dentistry when isolated areas of inadequate anesthesia are present. It may also be used alone to achieve pulpal anesthesia in a single tooth. Although the PDL injection may be used on any tooth, its primary importance lies with mandibular molars, when no nerve block technique has proven to be effective. Advantage to the use of the PDL injection in this way include adequate pulpal anesthesia with a minimal volume of anesthetic (0.2 to 0.4 ml) and the absence of lingual and lower lip anesthesia.
A 27-gauge short or 30-gauge ultrashort needle is firmly placed into the periodontal space between the root of the tooth and the interseptal bone. Although bevel orientation is of little significance in the PDL injection, the author recommends the bevel face the root of the tooth. A volume of 0.2 ml of anesthetic is slowly deposited on each root of the tooth. Successful PDL injection anesthesia is indicated by (1) the presence of resistance to anesthetic deposition and (2) ischemia (whitening) of the soft tissues in the immediate area on injection of the anesthetic is not an indication of successful anesthesia.
The most significant contraindication to PDL injection administration is the presence of infection or inflammation in the areas of needle insertion. This might prove a significant impediment in endodontics, where periapical infection exists or where periodontal infection is present. It is also contraindicated with primary teeth, where permanent tooth bud is present. The concern is noted on whether to perform a PDL injection on a vital tooth- Walton and Garnik in JOE 1982 Vol 8 p 22-26, states that it is safe to perform on a vital tooth. There will be an area of repair at the area of injection but no damage is done to the periapical area. To be safe if a tooth has a reversible pulpitis it may be safest to avoid a PDL injection so as not to add further insult to the tooth. The vasoconstrictor has no deleterious effect on the periapical tissue. (Also can refer to Malamed’s handbook of Local Anesthesia section on PDL injections.
Pathways of the pulp by Cohen and Burns, 7th Ed.
5. WHAT ARE INDICATIONS FOR SPLINTING? WHICH OF THE FOLLOWING ARE TRUE??
1. When a tooth suffers a concussion, you must splint it for a minimum of three weeks.
2. For a subluxation injury, hemorrhage may be seen and the tooth is usually mobile.
3. In a lateral luxation injury the tooth is displaced laterally and is mobile in the socket.
4. In an intrusion injury you will have a HIGH metallic sound (as you will in a lateral luxation injury) and the tooth will not be loose.
5. In an extrusion injury the tooth is elongated and needs splinted up to three weeks.
6. Root fractures need splinted for 6-8 weeks. 7. Alveolar fractures need splinting for 3-4 weeks.
ANDRAESON STUDY STATED THAT “RIGID FIXATION PRODUCES A GREATER DEGREE OF REPLACEMENT RESORPTION.” Minimal splinting
that allows physiologic movement results in low incidence of replacement resorption.
Nasjleti study states that “Replanted teeth splinted for seven days recovered uneventfully, whereas replanted teeth splinted for 30 days showed increased root resorption and ankylosis.”
CONCUSSION- Tooth is tender to touch, no mobility no displacement-FLEXIBLE SPLINT 7-10 DAYS. SUBLUXATION-tender to touch and mobile, not displaced, hemorrhage from sulcus possible-FLEXIBLE SPLINT 7-10 DAYS. LATERAL LUXATION - displaced laterally and locked in bone, not tender, not mobile. HIGH metallic sound=ANKYLOTIC SOUND-SPLINT FOR 3 WEEKS. INTRUSION-displaced deeper into the socket, not tender to touch, not mobile, again HIGH ANKYLOTIC sound-extirpate pulp in 1-3 weeks. An intruded adult tooth will not re-erupt, use forceps and gently reposition tooth-you may hear the osseous snap back into place. EXTRUSION- elongated mobile tooth-SPLINT UP TO 3 WEEKS. ROOT FRACTURE- SPLINT 2-3 WEEKS. ALVEOLAR FRACTURE-SPLINT 3-4 WEEKS. A severe blow to the face with a chipped tooth-feel better to see the chip, if no chip, the tooth may have suffered a more direct blow-possible pulpal damage, root fracture/alveolar fracture. 95% of intrusion injuries will need NSRCT.Splint with monofilament.
ANSWER: 1-F , 2- T, 3- F, 4- T, 5-T , 6-F , 7-T .From Guidelines for the Evaluation and Management of Traumatic Dental Injuries, Dental Traumatology, 2001: 17:1-4, 49-52, 97-102, 145-8, 193-6. Class handout.
6. Which of the following statements about the smear layer are true?
1. The smear layer is produced mainly by end cutting files.2. The smear layer is a superficial layer composed of organic and inorganic
debris that forms on the walls of the canal and does not penetrate the dentinal tubules.
3. The smear layer can be removed with 10% citric acid or ethylenediaminetetraacetic acid (EDTA).
4. The failure to remove the smear layer prior to obturation can have significantly more microleakage than an obturated canal with the smear layer removed.
Answers:a. 1,3b. 2,3,4c. 3,4d. 1,4e. 1,3,4
Statement 1 is false it has been shown that all cutting instruments in the canal form a smear layer and not mainly by end cutting files.
Statement 2 is false because the smear layer does penetrate slightly into the tubules. The smear layer contains dentin debris, bacteria, pulpal remnants, endotoxins and sometimes restorative material. It is several microns in thickness and plugs the tubules.
Statement 3 is true. The smear layer can be removed by 10% citric acid and ethylenediaminetetraacetic acid (EDTA). The use of chelating agents, weak acids followed by rinsing with sodium hypochlorite can remove the smear layer. Ultrasonic streaming also may be used in the canal for smear layer removal.
Statement 4 is true. Research has shown that the failure to remove the smear layer prior to obturation does cause increased microleakage. The smear layer may interfere with the penetration of the gutta percha or sealer into the dentin tubules. Removal of the smear layer helps create a tight interface between the gutta percha and the dentin walls. The smear layer is a potential pathway for bacteria to inter the canal. The smear layer might also harbor bacteria that could repopulate the obturated canal.
ANSWER: C
Calt, S. and A. Serper (2002). “Time-dependent effects of EDTA on dentin structures.” J Endodon 28(1): 17-9.
Cohen S. and Burns RC. Pathways of the Pulp. Eight Edition, 2002, Mosby Inc., St. Luois, Misouri. 286-287, 305-306
Gencoglu, N., S. Samani, et al. (1993). “Evaluation of sealing properties of Thermafil and Ultrafil techniques in the absence or presence of smear layer.” J Endod 19(12): 599-603.
Weine FS. Endodontic Therapy. Mosby Inc, St Louis, 1996;5:127-129
7. Which of the following statements are true regarding nickel titanium endodontic files?
6. They have a high elastic modulus, which provides flexibility. 7. Nitinol cannot be strained to the same level as stainless steel without
permanent deformation.8. They are easier to prebend than stainless steel do to nickel titanium’s poor
“memory”.9. When stressed they exhibit transforamation from an austenitic crystalline
phase to a martensitic structure.
Answere. 2,3f. 4g. 2,3,4h. 1,4
Statement 1 is false. Nitinol has a low elastic modulus making it very flexible. The metal expensive and is difficult to instrument and mill. The flexibility aids in instrumentation of curved canals.
Statement 2 is false. Nitinol is able to recover from plastic strain when unloaded.
Statement 3 is false. NiTi is an alloy in a class called “shape memory alloys”. The memory can be hazardous at the apex. The constant tendency to straighten may lead to zipping or transportation or over instrumentation of the apex.
Statement 4 is accurate. Nitinol will change form a austenitic crystalline phase to a martensitic phase. While in the martensitic phase little force is needed to bend the metal. The little force needed to bend makes it helpful in the instrumentation of curved canals. This also causes little filling to be done for the same time period as a stainless steel file. When the stress of the martensitic phase is reached deformation and fracture can occur.
Correct answer b. 4
Cohen S. and Burns RC. Pathways of the Pulp. Mosby Inc., St Louis, 2002;8:526-527,539, 912-914,
Wein, FS. Endodontic Therapy. Mosby Inc., St Louis, 1996;5:352-352
8. Which statement best describes Root ZX apex locators?
1. The apex locator measures the impedance between the file and the mucosa.2. Root ZX measures the resistance of electricity to the PDL.3. The Root ZX uses different frequencies to determine to foramen location.4. The Root ZX must have a dry environment to effectively operate.
Answera. 2,3b. 4c. 2,3,4d. 1,3
Statement 1 and 3 are correct. The Root ZX is the latest generation of apex locators. It operates by measuring the impendence difference between high (8 kHz) and low (400 kHz) frequencies. The difference is greatest at the CDJ. Impedance is based on the theory that the long hollow tube of the canal develops electrical impedance by the transparent dentin that drops sharply at the CDJ. This drop can be measured electrically. They have been shown to be accurate to 0.5mm of the apex. This electrical instrument should not be used on patients with pacemakers.
Statement 2 is false. The first generation of apex locators developed were resistance types.
Statement 4 is false. The canal can be wet with blood or other fluids which is usually necessary to achieve an accurate measurement with impedance - frequency type devices.
Correct answer d. 1,3
Cohen S. and Burns RC. Pathways of the Pulp. Mosby Inc. St Louis, 2002;8: 542Wein, FS. Endodontic Therapy. Mosby Inc., St Louis, 1996;5:408-416
9. Which of the following are true statements concerning tooth reimplantation?
1. The apical diameter (1.5 mm or greater) had an increased pulpal survival rate after reimplantantaion.
2. Inflammatory resorption is usually detected radiographically within two weeks of injury.
3. Replacement resorption (ankylosis) is caused by extensive PDL necrosis with bone formation onto the denuded root surface.
4. Storage and transport should be done in Hank’s balanced salt solution, milk, saline, hydrogen peroxide, saliva, or water.
Answera. 1,2,3b. 3,4a. 2,3,4b. 1,2,3,4
Statement 1 is correct. A large apex opening allows for adequate blood supply to be reestablished for the repair and survivability of the pulpal tissue.
Statement 2 is correct. The types of healing responses are 1. Normal PDL repair 2. 2. Surface resorption (transient)- usually repairs in two three weeks 3. inflammatory response- occurs due to PDL damage, inflammatory response in the PDL with inflammatory resorption of root surface
Statement 3 is correct. ankylosis- often occurs after long extra-alveolar times, if less than 20% is involved reversal may occur, the resorbing cells are osteoclasts. Radiographic moth eaten root and there is no treatment.
Statement 4 is false. All of these are acceptable except hydrogen peroxide. Milk is superior to saliva. The storage medium is more important than the extroral time. Short periods of dry storage results in resorption. Best to maintain viability of PDL cells. Replant as soon as possible. Rinse off debris but do not scrub. Correct answer a. 1,2,3
(Blomlof L, Lindskog S, Hammarstrom L. Periodontal healing of exarticulated monkey teeth stored in milk or saliva. Scan Dent Res 1981;89:251-9. Andreason JO, Hjortting-Hansen E. Replantation of teeth. Part 1. Radiographic and clinical study of 110 teeth replanted after accidental loss. Acta Odontol Scand 1966;24:263-286 Andreason JO Effect of extra-alveolar period and storage media upon periodontal and pulpal healing after replantation of mature permanent incisors in monkeys. Int J Oral Surg 1981, 10:43-7) Anderson FM, Zhijie Y, Thomsen BL. Relationship between pulp dimension and development of pulp necrosis after luxation injuries in the permanent dentition. Endod Detn Traumatol 1986;2:90-8)
10. Which of the following is not an ISO sized instrument?
a. Stainless Steel hand filesb. Hedstroems filesc. NiTi filesd. Greater Taper files
Answer is d. Greater taper files come in a set of four and have increasing tapers of 0.06, 0.08, 0.10, and 0.12 mm that correspond to fine, fine-medium, medium, and medium-large gutta percha. Additionally they have variably pitched flutes that act as reamers and remove more dentin at the shank and function as a file at the tip. (Pathways of the Pulp 8th, p251)
ISO files follow a universal nomenclature according to taper diameter that allows machinists and dentists to specifically fabricate and utilize endodontic files. All of these files have 16mm length of cutting flutes and taper at 0.02mm per 1mm of length giving the overall standard taper of 0.32mm for the cutting surface. (Pathways of the Pulp 8th, p250)
Most all rotary instruments have manufacturer specific tapers, flute pitch, cutting length and depth etc, therefore are not ISO standardized. These include; GG Drills, NiTi Rotary Shaping Instruments, ProFile Rotary Instruments, GT rotary files, Accessory GT files, ProTaper Instruments, and Quantec Files. (Pathways of the Pulp 8th, p251-7)
11. ISO file diameters progressively increase by 0.050 from size No.8 to 90. Regardless of file length ISO 21mm, 25mm, or 31mm, they all have a 16mm fluted cutting surface.
a. Both statements are true
b. First statement is true, second statement is falsec. First statement is false, second statement is trued. Both statements are false
Answer is c. The file number represents the size at D0 which is the tip of the file. The number 10 file is 0.10mm in diameter at D0, and tapers at 0.020mm for 16mm and terminates at a diameter of 0.42mm at D16 which it the end of the flutes at the shank. ISO file sizes 10 through 60 have diameters at D0 that increase by 0.05mm. From No. 60 onward to 140 D0 increases by 0.10mm. How about the No. 6 and 8 file you ask, well just think of them as in hundredths of a millimeter in that a No. 6 file is 0.06mm and No. 8 file is 0.08mm at D0. (Pathways of the Pulp 8th, p250)
12. Files are used in endodontic preparation to:
1. Clean the canal system2. Shape the canal system3. Improve access to canal system4. Facilitate obturation
a. All of the aboveb. 1, 2, 3c. 1, 2, 4d. 2, 3, 4
Answer is c. Goal #1 of shaping is to facilitate cleaning by removing restrictive dentin that allows and effective volume of irrigant to work deeper and circulate in all aspects of the root canal system. Additionally it serves to eliminate the pulp, bacteria and their toxins. Goal #2 of shaping is to facilitate obturation compactly in three dimensions. It removes canal contents and creates a smooth tapered opening to the terminus which allows the unimpeded insertion of an obturating material, by the removal of restrictive dentin and allowing instruments to work deeply in the canal preparation.
Cleaning of the canal is done by irrigants that either dissolve, dissolute, lubricate and rinse debris from the canal while the canal is being shaped. It is the files that produce shape and the irrigants that clean the canal system.
The final shape is specific for the anatomy of each root. (Pathways of the Pulp 8th, p235)
13. For which of the following scenarios is thermoplastic gutta percha technique potentially beneficial over standard lateral compaction?
a. When the canals are curved.b. When there are irregularities in the canal system.
c. When there is an open apex.d. When the canal system is perfectly prepared .
Answer is b. Irregularities such as internal resorption or “C” shaped canals are best filled using thermally manipulated obturating material due to the nature that walls may not be completely instrumented and compaction pressure may not be applied directly.
There are several types of warm techniques. Some are done with standard gutta percha master cones utilizing Enhanced Heated Systems for softening of intracanal gutta percha as is the case with System B. The Core Carries Technique where a firm plastic core coated with gutta percha is place in an oven, heated then inserted into a sealer-lined canal. Most noted of this type is ThermaFil. And finally the Injectable Technique in which a continuously tapered funnel canal prep allows the flow of heat softened (in the neighborhood of 365o to 392oF) gutta percha material from the 20 gauge applicator of an injection gun. A definite apical matrix is essential for these techniques to prevent over extrusion of the material.
(Pathways of the Pulp 8th, p342-53)
14. A patient arrives at your office in severe pain on mandibular right with cellulitis of the buccal mucosa and trismus limited to an opening of 5mm. Intraorally you visualize swelling buccal to #30, which when tested is extremely percussion and palpation sensitive with an EPT of no response at 80/80. With much skill you negotiate radiographic file into position and identify a large periradicular radiolucency associated with #30. What is your anesthetic technique of choice?
a. Inferior alveolar nerve blockb. Auricular-temporal extra oral injection technique c. Akinosi techniqued. Gow-Gates techniquee. Rx of felxaril to relax muscular complex then attempt anesthesia
Answer is c. The Akinosi-san technique is often referred to as the “closed-mouth” technique, but you won’t here be calling it that. I met the guy and he deserves his name on something if not this perhaps a puff pastry, he likes sweets. Indicated in time of limited openings owing to infection, trauma and trismus, the following steps are followed in order to administer this injection. A 27-gauge long needle is held in the maxillary buccal fold at the height of the mucogingival junction of the most posterior tooth. The needle is inserted into soft tissue to the lingual surface of the ramus immediately adjacent to the maxillary tuberosity and advanced to a depth of 25mm at which point 1.8ml of anesthetic is deposited. Thus gaining anesthesia of the inferior alveolar nerve with an 80 to 85% success rate. The disadvantage of this technique is the absence of bony contact
(Pathways of the Pulp 8th, p736)
The Gow-Gates technique is a mandibular nerve V3 block injection that is targeted higher and deeper than the IANB. The aim is at the neck of the condyle below the insertion of the lateral pterygoid. Success rates are reported as high as 97.25%
(PotP 8th, p735)The barrel of an aspirating syringe is larger in diameter than 5mm.The auricular-temporal injection will not get near the mandibular nerve branch.Rx of flexaril could work, but this patient is swelling and needs to be treated pronto.
15. The incidence of external root resorption is increased when heat is applied to the Superoxyl while in the chamber. The incidence of external resorption is increased when Superoxyl placed apical to the level of the CEJ.
a. Both statements are trueb. First statement is true, second statement is falsec. First statement is false, second statement is trued. Both statements are false
Answer a: A 30% solution of Superoxyl and sodium perborate are common materials used in the non-vital chair-side and walking bleach techniques. Heating the bleaching solution in the chamber can double the incidence of resorption.
(Pathways of the Pulp 8th, p755)
The majority of cases of external root resorption appear in patients under the age of 25. It is speculated that this is due to larger pulp canal systems the greater number of patient tubules. Evidence usually does not manifest for 6 months therefore recall are essential. Their repair can sometimes be initialized by calcium hydroxide to arrest the lesion, then flap for access surgery, orthodontic extrusion, or crown lengthening surgery. Therefore it is recommended that after removal of the gutta percha from the chamber and pulp horns, a barrier of a GI or RMGI be placed 2mm thick at a level 1mm incisal to the CEJ. (Pathways of the Pulp 8th, p756)
16. Which of the following are true regarding host defense response to the threat of microbial invasion from the root canal?
11. The plasma cells are the front line fighting force against bacteria.12. The T-lymphocytes, B-lymphocytes and natural killer cells are primary cells
of importance in chronic inflammation and immunity13. Plasma cells are the only cells that can manufacture and secrete antibodies14. PMNs have a life of 8-10 days and die in great numbers at acute
inflammatory sites15. The accumulation and local death of neutrophils is a major cause for tissue
breakdown in chronic phases of apical periodontitis
k. 1 only is correct
l. 2 only is correctm. 3 only is correctn. 2, 4, and 5 are correcto. All of the above are correct
The cells present during inflammation (such as apical periodontitis) are as follows: Neutrophils, macrophages, lymphocytes, plasma cells and epithelial cells.In general, the acute phase reveals high concentrations of neutrophils and some macrophages and chronic phase reveals accumulation of lymphocytes, macrophages, and plasma cells.PMNs-polymorphonuclear leukocytes or neutrophils are the front line fighting force against microbes and are the hallmark of acute inflammation.They locate and destroy microbes as nonspecific phagocytes and are well equipped to attack enemies with weapons already stored within them, classified into primary, secondary, and tertiary groups. Primary contain lysosomes, myeloperoxidase, cationic proteins, and neutral proteases. Secondary granules are marked by lactoferrin and vitamin B12 binding protein. Tertiary granules are released in response to specific stimuli.Lymphocytes-three major classes: T-lymph’s, B-lymph’s and natural killer (NK) cells.Plasma cells-the only cells that can manufacture antibodies.Macrophages-the primary cells of chronic inflammation and immunity; a large mononuclear phagocyte.Epithelial cells-about 30-52% all apical periodontitis lesions contain proliferating epithelium; during periapical inflammation the cells rests of Malassez are stimulated by cytokines and growth factors to undergo division and proliferation called inflammatory hyperplasia.
1. is wrong-PMNs are the font line fighting force against microbes.2. is wrong-macrophages are the “prima donna” of chronic inflammation and
immunity.3. is correct4. is wrong-PMNs are short lived (2-3 days)5. this describes acute phases of apical periodontitis
Answer is c. 3 only
Reference: Pathways of the Pulp, 8th Ed. Cohen and Burns 2002
17. Which of the following are true regarding microorganisms associated with endodontic disease?
1. The vast majority of endodontic infections contain anaerobic bacteria 2. Kobayashi found similar bacteria from caries infections as were found in
products determine which bacteria will predominate
4. Teeth requiring endodontic retreatment have shown a prevalence of Streptococcus faecalis.
5. Facultative bacteria are predominant in the initial infections of root canals.
a. 1 and 3 onlyb. 1, 3, and 5c. 1, 2 and 4d. 2 and 4e. 1, 3 and 4
1. is correct. Many repeated studies continue to show that there are primary anaerobic bacteria cultivated from root canals spaces2. is wrong. The study showed a similarity in bacteria isolated from root canals to those isolated from the sulcus of a periodontal pocket. It is believed from this study that the sulcus is the source of bacteria in root canals infections3. is correct4. is correct
6. is wrong. Strict anaerobes are predominant in the initial infections of root canals.
Chart 1 Demonstrates bacteria from theRoot Canals of teeth with apical lesions: Chart 2 Demonstrates taxonomic changes for previous Bacteroides species:
Chart 1. Chart 2.
The correct answer is e.
18. Which of the following are true of the crown-down technique?
1. To enlarge the coronal 1/3 of the canal preparation.2. To enlarge the apical 1/3 of the canal to properly fit the master cone of gutta percha.3.To use a sequential series of instruments, starting with the smaller sizes and progressing toward the larger sizes, irrespective of the instruments series used.4. To use a series of instruments whereby one begins with larger sizes and progresses towards the smaller sizes.5. NiTi rotary-shaping files are best.6. ISO hand files and GGs are best.
Answers:a. 1, 3, 5b. 1, 3, 6c. 2 and 5d. 3 and 6e. 4 and 5
The Crown-down manner is one technique of coronal two-thirds preenlargement of a canal, involving the serial use of instruments, starting with the larger sizes and progressing toward the smaller sizes. The other type is called Step-back. Step back involves sequentially using instruments, starting with the smaller sizes and progressing toward the larger sizes, regardless of the instrument series.
1 and 2 are both wrong because the technique involves two-thirds preenlargement of the coronal canal preparation3. is wrong because this describes the Step-back technique4. is one of the correct responses as noted in the above5. is correct; this is the virtual consensus on the preferred instrument type for crown-down6. is incorrect; ISO hand files and GGs are best used in a step-back technique
Taken from: Cohen S, Burns RC. Pathways of the Pulp. 8th Ed. (2002). CV Mosby, St. Louis, MO. Pp 265-266.
Correct Answer is e. 4 and 5
19. Which are of the following are true of the balanced-force technique?
1. Balanced force uses three distinct phases that comprise the instrument cycle.2. Phase I involves the use of ultrasonic pre-debridement of the coronal 1/3.3. Phase III involves flute loading.4. The file is withdrawn after two to three dozen rapid rotations of the file.5. The balanced force involves file cutting at the apical extent of the file and not
along its lengtha. 1 onlyb. 1, 2, 3c. 1, 3, 4, 5d. 2, 3, 4, 5e. 1, 3, 5
The balanced force technique uses instruments in a step-back manner to initiate preenlargement of the canal and gain access to the apical third rapidly. This involves three distinct phases as follows:Phase I-file insertion. As advocated by Roane, the balanced force utilizes the newer K-file design called the Flex-R-File (Rhomboid). Recently, NiTi files have been recommended for use as well. The file is inserted and reciprocated by the handle in a back and forth motion until it feels snug. The handle of the file is then turned 45-90 degrees, CW rotation is used to draw the instrument down, which moves the cutting blades deeper into the canal, and engage dentin.Phase II-file cutting. Two forces are applied simultaneously on the file handle. The file is rotated CCW while pushing apically. When rotated CCW, the tendency of the file backing out of the canal is “balanced” by the force of the file being pushed into the canal. One will often hear a clicking sound as the dentin is cut or sheared off of the canal walls. After the first cutting cycle, the file is extended slightly deeper into the canal as in Phase I. Phases I and II can be repeated up to 2-4 times.Phase III-flute loading. The dentin cut in the Phase II lies in the interblade spaces of the file and also in the canal spaces apical to the file. The debris is removed by rotating the file CW and pulling coronally. Flute loading never causes the file tip to advance apically because of the balanced force of the file being lifted out of the canal. Two or three rotations are all that are required to fill the apical flutes with dentin mud. Hence, the file should be withdrawn.Three advantages of balanced force using NiTi are as follows:
1. File cutting occurs at the apical extent of the file and not along it’s length. This increases the control of the file.
2. The safe-ended file tip stays centered in the root when activated in the Phase II file cutting.
3. It is not necessary to pre-curve the files to simulate canal anatomy, but, rather used straight as they were manufactured. The metallurgy and method of use cause the file to stay centered in the canal and guides the files into most curvatures.
The correct answer is e. 1, 3, 5 as can be determined from reading of the above phases I-III of the balanced force technique.Cohen S, Burns RC. Pathways of the Pulp. 8th Ed. (2002). CV Mosby, St. Louis, MO. p. 268.
20. 23 year-old healthy male patient’s maxillary central incisor was avulsed less than one hour ago. The avulsed tooth was stored in milk since the incident. The radiograph and clinical exam showed no sign of fracture of alveolar socket. Treatment of choice is Doxicycline 100mg BID for 7 days, Chlorhexidine mouthrinse (0.1%) BID for 1 week and:
a. Reimplant after rinsing with saline, flexible splint for 7 days, followed by RCT in 7-10 days with Ca(OH)2 as an intra-canal medicament.
b. Soak the avulsed tooth in pH5.5, 2.4% Sodium Fluoride for minimum of 5 minutes, flexible splint for 7 days, followed by NSRCT in 7-10 days with Ca(OH)2 as an intra-canal medicament.
c. Complete NSRCT extra-orally, reimplant and stabilize for 3 weeks.d. Reimplantation is not indicated.
Answer: a Is the recommended treatment for avulsed permanent tooth with closed apex, extra-oral dry time is less than 60 minutes, according to IADT guidelines (Dental Traumatology, 2001: 17: 193-196) .
B is not correct for this situation. This treatment is the recommended treatment for extra-oral dry time is grater than 60 minutes.
C is not correct. If extra-oral dry time is grater than 3 hours, the endodontic treatment may be completed extra-orally since time is of no consequence. Tooth may be stabilized for 3 weeks when the tooth was luxated or extruded.
D is not correct. When the tooth has open apex and extra-oral dry time is greater than 60 minutes, reimplantation is not indicated.
21. Followings are the indications for SBE Prophylaxis on high and moderate-risk patients (prosthetic valves, previous bacterial endocarditic, congenital cardiac malformations, hypertrophic cardiomyopathy, rheumatic heart disease, and MVP with regurgitation) EXCEPT:
- Dental extractions- Periodontal procedures including scaling and root planning, probing
and recall maintenance
- Dental implant placement and reimplantation of avulsed teeth - Endo treatment or surgery only beyond the apex- Local anesthetic injections (nonintraligamentary)
Answer: e
On high and moderate-risk patients, invasive dental procedures where bleeding is likely are recommended to have antibiotic coverage.
REF: Dajani AS, Taubert KA, Wilson W, et al “Preventation of bacterial Endocarditis. Recommendations by the AHA,” JAMA, 1997, 277(22): 1794-801
22. When the patient is taking Amoxicillin for some other reason, prophylaxis is not necessary.
- True.- False.
Answer: bIf a patient is already taking antibiotics for another condition, prophylaxis is accomplished with a drug from another class. If the patient is taking Amoxicillin, Azithromycin or Clarithromycin (500mg PO 1 hr before procedure) is the drug of choice for antibiotic prophylaxis.
REF: Dajani AS, Taubert KA, Wilson W, et al “Preventation of bacterial Endocarditis. Recommendations by the AHA,” JAMA, 1997, 277(22): 1794-801
23. EDTA is a chelating agent that:a. Lubricatesb. Emulsifiesc. Holds debris in suspensiond. Removes smear layere. All of the above
Answer: e
REF: Pathways of the Pulp, Eighth Edition p. 259
24. Danger zone is defined by Abou-Rass, Frank and Glick as the thin area in the root canal wall that is vulnerable to stripping by injudicious filling. Danger zone is located at mandibular first molar mesial root, 1.5mm below the furcation about 1.3mm thick on the distal surface.
a. Both statements are true.b. Both statements are false.c. The first statement is true, second statement is false.d. The first statement is false, second statement is true.
Answer: a
REF: Abou-Rass, Frank and Glick, Anticurvature filing method to prepare the curved root canal, JADA, 101 Nov 1980.
25. What is the goal of root end surgery?
a. Provide an apical sealb. Prevent leakage of potential irritants from the root canal into the
periradicular tissuesc. Remove the necrotic apical 3mm of tooth structure.d. Curettage of the periapical osseous necrotic tissue
A: a&b
When the pathway between the canal and the periradicular tissues has been effectively sealed, resolution of inflammation is rapid.
26. Which of the following statements regarding flap reflection is correct?
a. The horizontal incision for the mucogingival flap is made perpendicular to the cortical bone.
b. The rectangular flap design is most appropriate in the posterior areas.
c. The mucogingival flap with an anterior-releasing incision is preferred in posterior areas.
d. The type of vertical-releasing incision distinguishes the mucogingival flab from the Luebke-Oschsenbein flap.
e. The semilunar flap has the advantage of providing an esthetic result without scar formation.
A: c&d
a. 45º is better to allow the widest cut surface permitting better adaptation once the flap is repositioned.
b. The rectangular flap may be better for anterior teeth because it provides better access to the root
apex, especially when the root is long. Triangular design is better for posterior teeth due to suturing problems from limited spacec. Yes, because distal vertical releasing incisions make for difficult access during
suturing.d. Yes : Mucogingival = vertical releasing incisions or PARALELL
L-O = wider at the base.e. Rarely used, limited access, prone to scarring
Pathways of the Pulp
27. Which of the following statements are true regarding access preparation?
1. The objective of entry is to give direct access to the pulp chamber, not merely the canal orifices.2. Access cavity preparations are similar to operative occlusal preparations3. The likely interior anatomy of a tooth under treatment need not be determined before entry since unroofing will reveal canal orifice locations.4. The rubber dam should always be placed before initial access preparation.
a. All of the aboveb. None of the abovec. 1 and 4d. 1 and 3
A: None of the above
The objective of entry is to gain direct access to the apical foramina, not merely to the canal orifices. Remember straight-line access.
Access cavity preparations are different from typical operative occlusal preparations since operative preparations are based on the topography of occlusal grooves, pits and fissures, and the avoidance of the underlying pulp.
The likely interior anatomy of a tooth under treatment must be determined. Each tooth has a typical length, number, and configuration of canals. Radiographs taken from two different angles must be studied. The information gained before initiation of penetration will greatly facilitate the entry as well as subsequent treatment.
When canals are difficult to find, the rubber dam should not be placed until correct location has been confirmed. Determination of the angle of malposed or extensively restored teeth can sometimes be easier with the dam off.
28. What is the success rate of endodontic treatment?
a. 50%b. 40%c. 53-94%d. 40-95%
A: C. 53-90%
There are a great number of articles reporting the success rate of endodontic treatment, ranging between 53 and 94%. However, even if 90% of all endodontic treatment is successful over time, the reciprocal failure rate is still 10%. In the United States alone where the number of teeth treated per year now exceeds 50 million, a 10% failure rate would represent 5 million treatment failures per year. Extrapolating these numbers over the past 3 to 4 decades reveals that the number of failing endodontically treated teeth is massive and could approach tens of millions!
Bonus question: The major reason for failure, requiring retreatment, is which of the following?
a. Persistent painb. Draining sinus tractc. Restorative indicationsd. Microleakage
A: d. Microleakage
Endodontic failures can be attributable to inadequacies in cleaning, shaping, and obturation, iatrogenic events, or reinfection of the root canal system when the coronal seal is lost after completion of root canal treatment. Regardless of the initial cause, the sum of all causes is microleakage.
References 1. Ruddle, C. Pathways of the Pulp, 8th edition, Mosby, 2002P
29. The posterior tooth with the highest endodontic failure rate is the:
a .Mandibular 1st molar b .Mandibular 2nd molar c. Maxillary 2nd molar d. Maxillary 1st molar
A: D (maxillary 1st molar)
The largest tooth in volume and the most complex in root and canal anatomy, the “six year molar” is possibly the most treated and least understood posterior tooth. Studies vary in the number of canals present however, the clinician should always assume there are two canals in the mesiobuccal root until it is proven that there is only one. In addition, the palatal often curves toward the buccal at the apical 1/3 that may not be obvious on a radiograph.
In contrast, according to a study by Skidmore and Bjorndal, 1/3 of mandibular first molars had four root canals.
References
1. Cohen S et al. Pathways of the Pulp, 8th edition, Mosby, 2002.
30. Which of the following statements regarding the use of intra-osseous anesthesia are accurate:
a. Epinephrine concentration of anesthetic agent should not exceed 1:200,000 b. Mandibular injections should be preceded by conventional block anesthesia c. X-tip injections at the angle of the mandible area should be avoided d. Total volume of anesthetic should not exceed 1 carpule
A: a,c,d
a. The highly vascular cancellous bone can deliver dramatic vasopressor response when concentrations higher than 1:100,00 of vasoconstrictor are used. b. All intraosseous injections should be preceeded by delivery of anesthetic agent in the mucco-buccal fold to prevent discomfort during penetration of the cortical plate. Block anesthesia is not required. (this is the point) c. The bone at the angle of the mandible is thick and penetration can be difficult, therefore it should be avoided d. One carpule of anesthetic agent maximum is adequate for profound anesthesia.
31. Incision and Drainage is indicated under the following conditions:
a. When facial swelling is present b. When cellulitis is present c. involvement of facial spaces d. when a traceable fistula is present
A: a,b,c
Any facial swelling due to infection is a potential life-threatening condition, which can spread to other areas via fascial planes and terminate with airway compromise. The infection is no longer limited to the periradicular region and conventional nsrct will not suffice. In addition, if the practiotioner does not have adequate support staff, facilities and skill to perform the procedure, referral is recommended. A traceable fistula can usually be treated successfully with nsrct.
32. Which would not be a hallmark of a Phoenix Abscess?
a. Pain with slight to large swelling.b. Radiographic lucency.c. Negative EPT.d. Exquisitely percussion sensitive.e. Intact lamina dura.
Hallmarks of Recrudescence of Chronic Periradicular Periodontitis - Phoenix Abscess
1) Chief Complaint: pain with slight to large swelling2) History: coronal microleakage?3) Radiograph: radiolucency4) EPT: -5) Thermal Tests: -6) Percussion: exquisitely sensitive7) Palpation: sensitive8) Mobility: + / -9) Other: necrotic pulp or pulpless tooth
Answer e. Intact lamina dura
Pathways of the Pulp 2002, Page 29
33. Which percentage most correct for the amount of gutta percha in dental gutta percha?
a. 19-22%b. 56-75%c. 2-17%d. 1-4%
Dental gutta percha consists of the following ranges of materials:Gutta Percha 19-22%, Zinc Oxide 56-75%, Heavy metal sulfates 2-17%, Waxes and Resins 1-4%.Dental gutta percha comes in two forms, alpha phase, which is brittle, and beta phase, which is pliant. Alpha phase GP can be rejuvenated back to beta by heating under hot tap water at >55 degrees C, then immediately tempering vertically with cold (<20' C) water. Answer a.Pathways of the Pulp 2002, Page 299
34. Which antibiotic is indicated for management of Penicillin allergic patients with a serious anaerobic bacterial infection?
a) Augmentinb) Erythromycinc) Clindamycin with Flagyld) Keflex
1929 Pen G (IV), V, narrow spectrum, mainly for G+ aerobic and facultatives. And a few anaerobes. (Streptococci, Pneumococci, Bacillus, Clostridium, Neisseria). Antibiotic of choice for endodontic infections due to efficacy and low toxicity.
Extended spectrum PCN's, Ampicillin (IM/IV), Amoxicillin.Amoxicillin - (combined with Clavulinic Acid, a beta-lactamase inhibitor, to form Augmentin). Enhanced activity vs. G- species. Broader spectrum and faster absorption than Pen VK
CephalosporinsBind to enzymes involved in cross linking of peptidoglycan strands of bacterial cell wall (Like PCN's). Expensive.1. First gen. Cephlexin (Keflex), vs. G+ Cocci, G- bacilli (E.Coli, Klebsiella)2. 2nd gen. Vs. Providencia, Proteus Cefaclor.3. 3rd gen. Most effective vs. G- species, H.Influenzae, enterococci, Neisseria, Serratia, Pseudomonas, and anaerobes like B. fragilis.
Erythromycin 1952, macrolide, inhibits bacterial protein synthesis Narrow spectrum like Pen G. Less effective vs. anaerobic species found in endodontic infections.
Clindamycin 1970- spectrum like e-mycin, more effective vs. most G+ and G- anaerobes.Not effective vs. most G- aerobes. Concentrates in bone. Pseudomembranous colitis risk only present in doses greater than that needed for endodontic infections.
Metronidazole- 1959 drug of choice for protozoal infections. Works vs. strict aerobic bacterial infection. ANUG application. Given with PCN to cover G+ and G- bacteria.
Quinolones - 1962, Ciprofloxacin, Broad spectrum, Highly active vs. G- enteric bacteria. Expensive.
Answer c. Clindamycin with Flagyl(Metronidazole)
Pathways of the Pulp, 8th Ed, Cohen and Burns 2002Endodontic Therapy 5th Ed, Weine 1996
35. A patient presents with a radiolucency on a non-angulated periapical film of tooth #5 that appears to be superimposed over both roots. A second film is taken but horizontally angulated more from the distal of #5. One of the roots appears to have moved mesially, while the radiolucency and one root stayed in place. Which root is most likely affected?
a) Buccalb) Lingual
c) Both B and Ld) Neither
SLOB Rule.Same Lingual, Opposite Buccal. Also known as BOR, Buccal Object Rule, or Clark's Rule.
Helps clinician radiographically determine B-L position of fractures, perforations, foreign bodies, and anatomic landmarks in relation to root apices or other bony landmarks.
*Object closest to the buccal surface appears to move in the direction opposite the movement the movement of the cone or tube head when compared with a second film.
This also applies to vertical tube head angulations.
Answer b) lingual
Pathways of the Pulp, 8th Ed, Cohen and Burns 2002, 120-123
36. Ultrasonic instruments allow better access during apical root preparations.Use of burs in the apical root end surgery yields more conservative preparations.
a) The first statement is TRUE, the second statement is FALSE.b) The first statement is FALSE, the second statement is TRUE.c) Both statements are TRUE.d) Both statements are FALSE.
Ultrasonic instruments are Piezo electrical units that create an oscillating sinusoidal wave in a file or accessory tip.. They operate at a frequency of 25-30 kHz.(Sonic devices operate at 2-3 kHz)
Applications for ultrasonics are:
1. Root apical preparation.Advantages over bur preparations are:a) Better access in difficult to reach areas with small tips.b) More thorough debridement of tissue and debris.c) More conservative preparations, follows the canal.d) Precise isthmus preparations with parallel walls allow better retention of filling materials.2. Endodontic paste (resin based) removal.3. Indirect silver point removal.
During silver point removal, direct contact with the point is avoided since the ultrasonic action will erode the silver. The objective is to create a trough around the point to facilitate mechanical instrumentation or use of removal pliers. The ultrasonic unit is used indirectly by contacting the pliers grasping the point.4. Post removal.Direct contact with the post loosens the cement that holds it in place.5. Enhance irrigant effect.Acoustic streaming and cavitation allows for better clearing of debris.Used with 17% EDTA, can help eliminate smear layer.6. Identifying constricted canal orifi.7. During retreatment, can aid in softening gutta percha.
Prolonged use of ultrasonic files may result in file breakage. Files must be changed out frequently.In many cases, the ultrasonic is used as an adjunct and not the primary instrument. Answer aPathways of the Pulp, 8th Ed, Cohen and Burns 2002