Protective Effect of Hydroalcoholic Olive LeafExtract on Experimental Model of Colitis in Rat:Involvement of Nitrergic and Opioidergic Systems
Nahid Fakhraei,1,6 Amir Hossein Abdolghaffari,2,3 Nastaran Rahimi,1 Bahram Delfan,4Ata Abbasi,5 Azadeh Khansari,4 Reza Rahimian1,6 and Ahmad Reza Dehpour1*1ExperimentalMedicineResearchCenter, PharmacologyDepartment, School ofMedicine, TehranUniversity ofMedical Sciences, Tehran, Iran2Pharmacology and Applied Medicine Department of Medicinal Plants Research Center, Institute of Medicinal Plants, ACECR, Karaj, Iran3International Campus, Tehran University of Medical Sciences, ICTUMS, Tehran, IranQ24Razi Herbal Medicine, Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran5Department of Pathology, Imam Khomeini Medical Center, Tehran University of Medical Sciences, Tehran, Iran6Brain and Spinal Injury Research Center, Tehran University of Medical Sciences, Tehran, Iran
Q4 Inflammatory bowel disease (IBD) is characterized byrecurrent inflammation and disruption of gut wallresulting from leukocyte infiltration and excessivegeneration of inflammatory mediators and oxidants.The two major types of IBD are ulcerative colitis andCrohn disease. These inflammatory bowel diseases arenow recognized to be caused by crosstalk between avariety of factors. It is now known that inflammatorycytokines such as interleukin (IL)-1, IL-2, IL-6 andinterferon gamma are upregulated at focal lesionsinduced by dietary antigen and/or intestinal bacteria(Nagura et al., 2001; Ludwiczek et al., 2004). Secretionof tumour necrosis factor-α (TNF-α) by epithelial cellsmay also represent a crucial event in the pathogenesisof IBD (Hagar et al., 2007). It has been suggested thatinflammation of mucosa impairs antioxidant defencemechanisms and exposes tissue to oxidative attackimposed by infiltrating macrophages and neutrophils.Increased oxidative and nitrosative stress and decreased
antioxidant defenses are reported in colonic mucosalbiopsies of patients with IBD (McCafferty, 2000).
Nitric oxide (NO) regulates major epithelial functionsinvolved in host defence such as mucus production andepithelial fluid secretion. Nitric oxide has also beenfound to alter the cytokine profile released by macro-phages so that following a T helper 1 (Th1) response,Th1-associated cytokines are down-regulated and Thelper 2 (Th2) cytokines are favoured (Huang et al.,1998). Nitric oxide has many well-documentedantiinflammatory effects in the gastrointestinal tract(Wallace and Miller, 2000). Endothelial NO synthase Q5
appears to be a homeostatic regulator of numerousessential functions of the gastrointestinal mucosa, suchas maintenance of Q6adequate perfusion (Moncada,1992), and regulation of microvascular and epithelialpermeability (Alican and Kubes, 1996). There is alsoevidence for the involvement of oxidative stress andprofound alterations in the biosynthesis of the freeradical NO from L-arginine in the pathogenesis of colitis(La et al., 2003). Furthermore, it has been identified bothin the studies held on patients with ulcerative colitis andexperimental colitis that inducible NO synthase (iNOS)
Q7is upregulated in the colon and the levels of citrulline,nitrate and nitrite of the end metabolites of NO pathwayare increased in blood, urine and rectal tissues(Macnaughton et al., 1998; Wallace and Miller 2000).
* Correspondence to: Ahmad Reza Dehpour, Experimental MedicineResearch Center, Department of Pharmacology, School of Medicine, TehranUniversity of Medical Sciences, Tehran, Iran.E-mail: [email protected]
Nahid Fakhraei1,3, Amir Hossein Abdolghaffari4,6, Nastaran Rahimi3, Bahram Delfan2, Ata Abbasi5, Azadeh Khansari2, Reza Rahimian1,3, Ahmad Reza Dehpour3* 1 Brain and Spinal Injury Research Center, Tehran University of Medical Sciences, Tehran, Iran 2 Razi Herbal Medicine, Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran 3 Experimental Medicine Research Center, Pharmacology Department, School of Medicine, Tehran University of Medicalc Sciences, Tehran, Iran 4 Pharmacology and Applied Medicine Department of Medicinal Plants Research Center, Institute of Medicinal Plants, ACECR, Karaj, Iran 5 Department of Pathology, Imam Khomeini Medical Center, Tehran University of Medical Sciences, Tehran, Iran 6 International Campus, Tehran University of Medical Sciences , ICTUMS
na.fakhrayi
Comment on Text
endothelial nitric oxide synthase (eNOS)
Intestinal opioid receptors (ORs) have now beenfound to be widely expressed in peripheral tissuesincluding the gastrointestinal tract. Intestinal ORs areinvolved in regulation of motility, intestinal secretionand bowel transit time (Wood and Galligan 2004). Theexpression of μ-ORs is upregulated in ileal and colonicenteric neurons, and the immunocytes and mucosa ofIBD patients, a process driven in part by inflammatorycytokines (Philippe et al., 2006). Evidence supports arole for endogenous opioid peptides (enkephalins andendorphins) in the development and or persistence ofinflammation (Pol and Puig, 2004). Opioids representa major part of their impact on the immune responseby modulating cytokine production. Studies of theeffects of endogenous and exogenous opioids have shownthat the opioids possess the capacity to modify theexpression of a large number of cytokines and cytokinereceptors. Opioids selectively promote proinflammatoryor antiinflammatory effects depending on the involve-ment of μ-ORs. Opioids are central participants in theinflammatory response in the brain and in the periphery(Rogers and Peterson, 2003).Experimental animal studies demonstrated antiathero-
genic, antiinflammatory, hypoglycemic and hypocholeste-rolemic effects of olive tree leaf (Olea europaea L.), all ofthese positive effects were at least partly related to itsantioxidative action (El andKarakaya, 2009). It was shownthat a total olive leaf extract (OLE) had an antioxidantactivity higher than those of vitamins C and E, because ofthe synergy between flavonoids, oleuropeosides andsubstituted phenols (Garcia et al., 2000). Orally appliedOLE had a significant protective effect in hepatic oxidativestress and that OLE inhibited the inflammatory response(Wang et al., 2008). Oleuropein is the main constituent ofolive leaf, which thought to be responsible for its pharma-cological effects. It has remarkable antioxidant activityin vitro (Speroni et al., 1998), as do other constituents ofolive leaf (Briante et al., 2002). In vitro, oleuropein and itsmajor metabolite, hydroxytyrosol, exhibited a rangeof pharmacological properties, antiinflammatory effects(Miles et al., 2005), scavenging of free radicals in additionto inhibition of 5-lipoxygenase and 12-lipoxygenase (Visioliet al., 2002). Oleuropein and hydroxytyrosol enhanced NOproduction by mouse macrophages (Visioli et al., 1998). Inacetic acid-induced writhing in mice, oleuropein-rich andhydroxytyrosol-rich extracts reduced significantly thenumber of writhing, which is associated with the releaseof endogenous substances including serotonin, histamine,prostaglandin and bradykinin (Collier et al., 1968).Assuming the antiinflammatory and antioxidative
properties of OLE and its main constitutes and thatinflammation of mucosa impairs antioxidant defencemechanisms in IBD, we have attempted to show its prob-able protective impact on acetic acid-induced ulcerativecolitis in rats. Moreover, we demonstrate if nitrergic oropioidergic systems take part in this healing power.
METHOD AND MATERIALS
Animals. Male Wistar rats (6–7weeks old; 200–250 g)were used throughout these experiments. The rats werehoused under specific pyrogen-free conditions andmaintained on standard pellet chow and tap water adlibitum. The whole study was conducted in accordance
with Tehran University of Medical Sciences guidelinesfor the care and use of laboratory animals.
Preparation of extract and quantification of some iden-tified phenolic compounds by HPLC. Olive leaves ex-tract, extremely enriched in oleuropein, was providedby Herbal Medicine Institute (Lorestan, Iran) followingan ethanol (80% m/m) extraction procedure. After apatented filtration process (EFLA® Hyperpure), thecrude extract was dried. By using high-performance liquidchromatography (HPLC), the amount of main constitu-ents of the extract was measured in 1 g of the dry extract.For the HPLC separation and quantitation, the chromato-grams were acquired at 240nm (Hashemi et al., 2010).The main phenolic compositions of OLE are oleuropein(356mg/g), tyrosol (3.73mg/g), hydroxytyrosol (4.89mg/g)and caffeic acid (49.41mg/g) of the dry extract, and theirpercentage is given in Table T11.
Experimental groups. Study period for all these groupswas 3 days. Drugs were administered for two successivedays, starting from the colitis induction day (day one).The rats were divided into ten groups of six. Controlgroup received intrarectal (i.r.) acetic acid 1 h afteradministration of saline (i.p.), whereas the sham-treatedgroup underwent the cannulation procedure withoutinstillation of acetic acid. The extract was given orallyto three groups at doses of 250, 500 and 750mg/kg dilutedin 1ml normal saline 1 h after acetic acid administration(i.r.). Finally, the standard treatment group received aceticacid (i.r.) 1 h before administration of dexamethasone(i.p.) (1mg/kg) (Antonioli et al., 2007). To assess theinvolvement of nitrergic and opioidergic systems, twogroups received either L-NG-Nitroarginine MethylEster (L-NAME) (10mg/kg) (i.p.) or naltrexone (5mg/kg)(i.p.), respectively, 30min before administration of theextract (750mg/kg) for two successive days. Finally, twogroups were administered either naltrexone (5mg/kg)or L-NAME (10mg/kg).
Induction of colitis. Acetic acid-induced colitis is an an-imal model that mimics some of the acute inflammatoryresponses seen in ulcerative colitis. Induction of colitisin rats using acetic acid is a classical method used to pro-duce an experimental model of human IBD (Sekizukaet al., 1988). The rats were fasted 24 h prior to anyintracolonic studies but were always allowed access towater. Colitis was then induced according to the methodof Kojima et al. (2001). Briefly, rats were anaesthetized,and a medical-grade polyurethane canal for enteralfeeding (external diameter 2mm) was inserted into theanus, and the tip was advanced 7 cm proximal to theanus verge. After that, 1ml 4% acetic acid (Merck,Darmstadt, Germany) was introduced into the colon.
Table 1. Percentage (%) of the main constituents of olive leafextract (in 1 g). Q8
Forty-eight hours following induction of colitis, animalswere euthanized. In an ice bath, distal colons were cutopen, cleansed gently with normal saline, and macro-scopic scores were determined. Subsequently, colonswere cut into two same pieces, one for histopathologicassessment (kept in 5ml of 10% formalin) and the otherfor analysis of biochemical markers.
Determination of ulcer index
Macroscopic scoring was performed under a magnifyingglass by an independent observer according to thefollowing criteria: 0, intact epithelium with no damage;1, localized hyperemia but no ulcer; 2, linear ulcerwith no significant inflammation; 3, linear ulcer withinflammation at one site; 4, two or more sites of ulcerand inflammation; 5, two or more sites of ulcer and in-flammation extending over 1 cm (Morris et al., 1989).For evaluation based on microscopical (histologic)
characters, the tissue was fixed in phosphate-bufferedformaldehyde, embedded in paraffin and 5-mm sectionswere prepared. The tissue was stained with haematoxylinand eosin and evaluated by light microscopy, being scoredin a blinded manner by an expert pathologist. Avalidatedhistological grading scale was used; each of the individualparameters estimated was graded 0–3 (inflammationseverity, inflammation extent and crypt damage) 0, nochange; 1, mild; 2, moderate; 3, severe (Murthy et al.,1993). The evaluated parameters were erosion, ulceration,mucosal necrosis, haemorrhage of mucosa, lamina propriaand submucosal edema, and inflammatory cell infiltration.The severity of changes was subjectively graded and com-pared with controls. Histological evaluation and scoringwas carried out using a Zeiss® microscope equipped withan Olympus® colour video camera for digital imaging.
Biochemical assays
Determination of inflammatory mediators. Coloniclevels of TNF-α and IL-2 were determined with an enzymelinked dimmunosorbent assay (ELISA kit) (Enzo LifeSciences, Lorrach/Germany). For the measurement ofinflammatory cytokines, the colon was dissected out andhomogenized in 50-mmol/L ice-cold potassium phosphatebuffer (pH 6.0) containing 0.5% of hexadecyltrimethyla-mmonium bromide. Afterwards, homogenates were cen-trifuged at 4000 rpm for 20min at 4 °C, and supernatantswere separated and kept at �80 °C until analysis.Briefly, wells pre-coated with a monoclonal antibodyserving to trap cytokine molecules in homogenatedspecimen. The results were expressed as picogram permilligram of wet tissue.
Data and statistical analysis
All values are expressed as means ±standard error SPSS(version 19.0, Chicago, USA). One-way analysis ofvariance was employed for analysing the data, followedby Tukey’s test for multiple comparisons. Significanceascribed when p< 0.05.
RESULTS
Macroscopic and histopathological scores
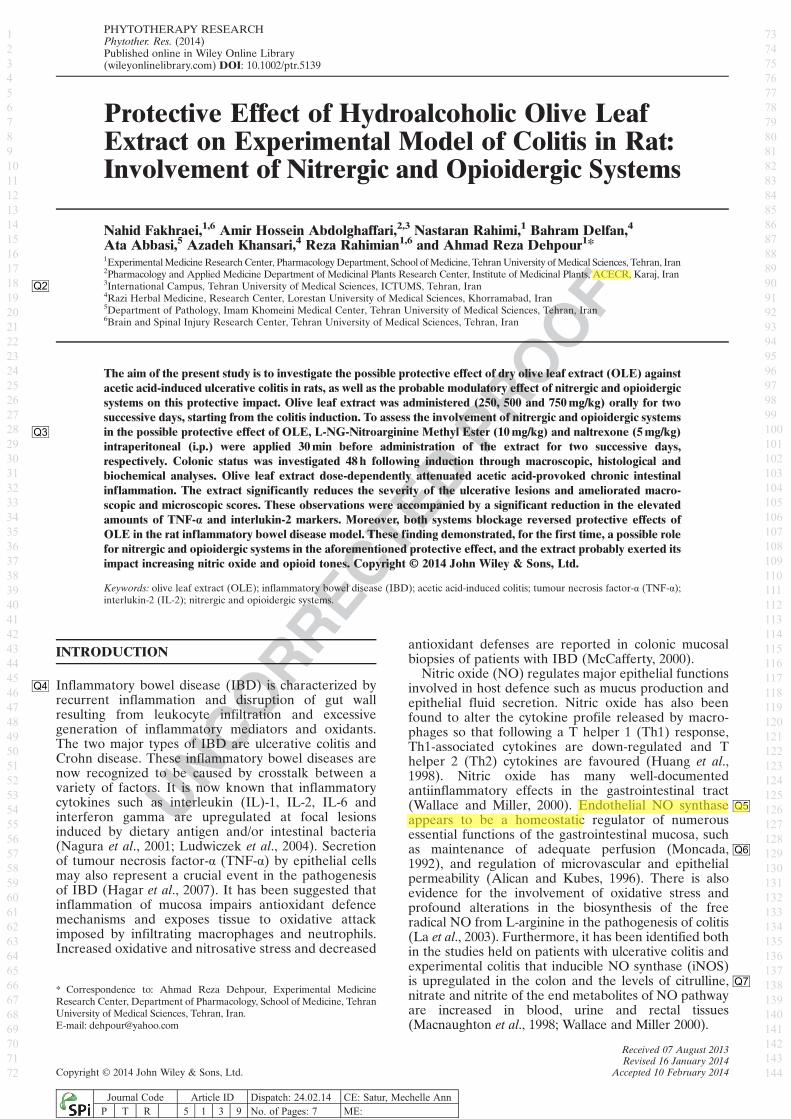
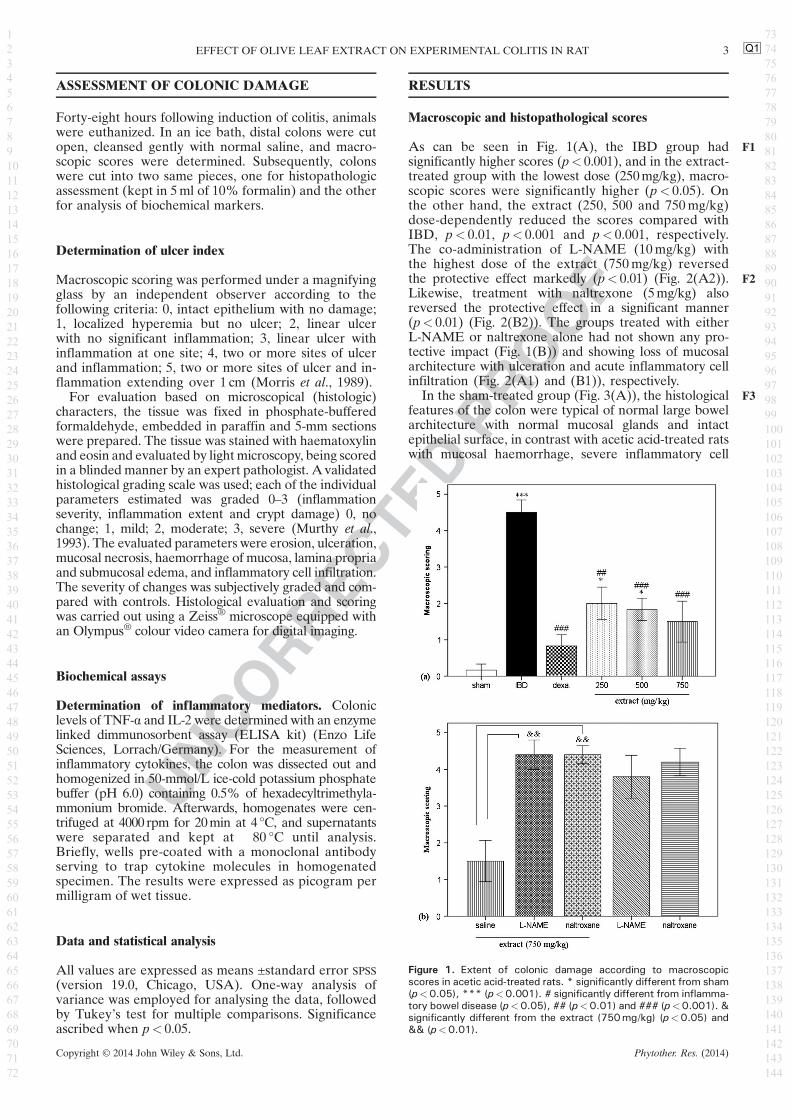
As can be seen in Fig. F11(A), the IBD group hadsignificantly higher scores (p< 0.001), and in the extract-treated group with the lowest dose (250mg/kg), macro-scopic scores were significantly higher (p< 0.05). Onthe other hand, the extract (250, 500 and 750mg/kg)dose-dependently reduced the scores compared withIBD, p< 0.01, p< 0.001 and p< 0.001, respectively.The co-administration of L-NAME (10mg/kg) withthe highest dose of the extract (750mg/kg) reversedthe protective effect markedly (p< 0.01) (Fig. F22(A2)).Likewise, treatment with naltrexone (5mg/kg) alsoreversed the protective effect in a significant manner(p< 0.01) (Fig. 2(B2)). The groups treated with eitherL-NAME or naltrexone alone had not shown any pro-tective impact (Fig. 1(B)) and showing loss of mucosalarchitecture with ulceration and acute inflammatory cellinfiltration (Fig. 2(A1) and (B1)), respectively.
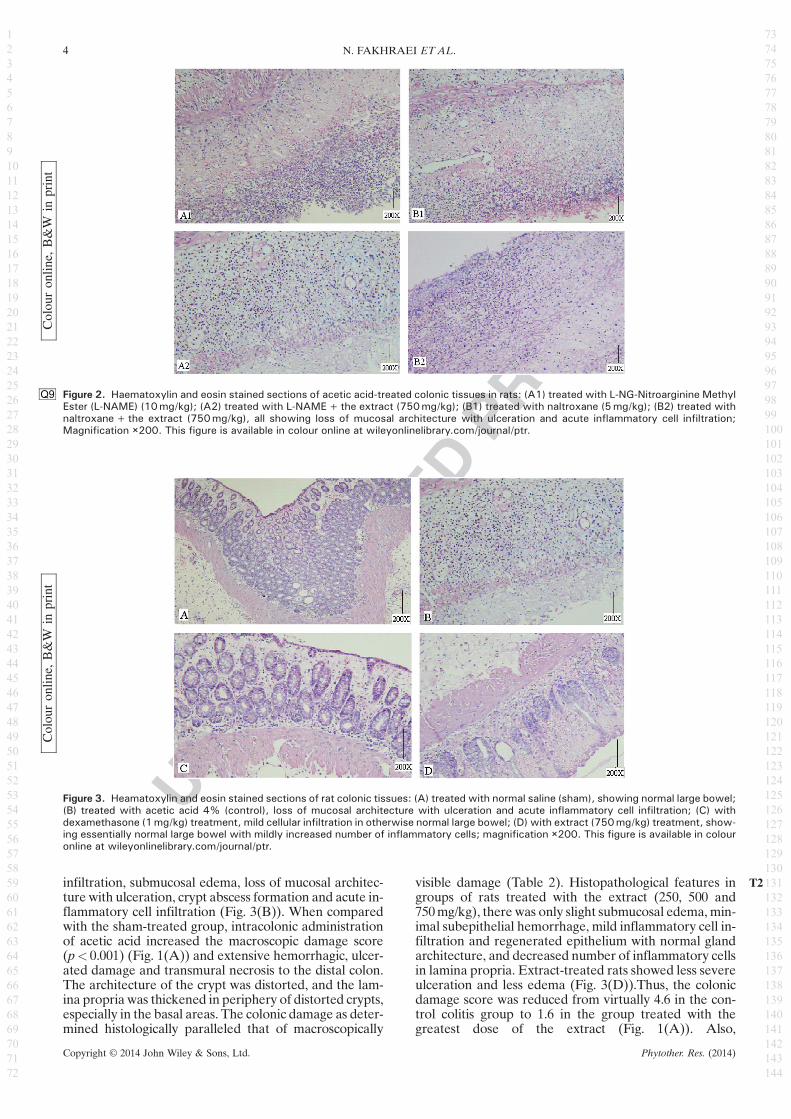
In the sham-treated group (Fig. F33(A)), the histologicalfeatures of the colon were typical of normal large bowelarchitecture with normal mucosal glands and intactepithelial surface, in contrast with acetic acid-treated ratswith mucosal haemorrhage, severe inflammatory cell
Q1
Figure 1. Extent of colonic damage according to macroscopicscores in acetic acid-treated rats. * significantly different from sham(p<0.05), *** (p<0.001). # significantly different from inflamma-tory bowel disease (p<0.05), ## (p<0.01) and ### (p<0.001). &significantly different from the extract (750mg/kg) (p<0.05) and&& (p<0.01).
3EFFECT OF OLIVE LEAF EXTRACT ON EXPERIMENTAL COLITIS IN RAT
infiltration, submucosal edema, loss of mucosal architec-ture with ulceration, crypt abscess formation and acute in-flammatory cell infiltration (Fig. 3(B)). When comparedwith the sham-treated group, intracolonic administrationof acetic acid increased the macroscopic damage score(p< 0.001) (Fig. 1(A)) and extensive hemorrhagic, ulcer-ated damage and transmural necrosis to the distal colon.The architecture of the crypt was distorted, and the lam-ina propria was thickened in periphery of distorted crypts,especially in the basal areas. The colonic damage as deter-mined histologically paralleled that of macroscopically
visible damage (Table T22). Histopathological features ingroups of rats treated with the extract (250, 500 and750mg/kg), there was only slight submucosal edema, min-imal subepithelial hemorrhage, mild inflammatory cell in-filtration and regenerated epithelium with normal glandarchitecture, and decreased number of inflammatory cellsin lamina propria. Extract-treated rats showed less severeulceration and less edema (Fig. 3(D)).Thus, the colonicdamage score was reduced from virtually 4.6 in the con-trol colitis group to 1.6 in the group treated with thegreatest dose of the extract (Fig. 1(A)). Also,
Figure 2.Q9 Haematoxylin and eosin stained sections of acetic acid-treated colonic tissues in rats: (A1) treated with L-NG-Nitroarginine MethylEster (L-NAME) (10mg/kg); (A2) treated with L-NAME+the extract (750mg/kg); (B1) treated with naltroxane (5mg/kg); (B2) treated withnaltroxane+the extract (750mg/kg), all showing loss of mucosal architecture with ulceration and acute inflammatory cell infiltration;Magnification ×200. This figure is available in colour online at wileyonlinelibrary.com/journal/ptr.
Colou
ron
line,
B&W
inprint
Figure 3. Heamatoxylin and eosin stained sections of rat colonic tissues: (A) treated with normal saline (sham), showing normal large bowel;(B) treated with acetic acid 4% (control), loss of mucosal architecture with ulceration and acute inflammatory cell infiltration; (C) withdexamethasone (1mg/kg) treatment, mild cellular infiltration in otherwise normal large bowel; (D) with extract (750mg/kg) treatment, show-ing essentially normal large bowel with mildly increased number of inflammatory cells; magnification ×200. This figure is available in colouronline at wileyonlinelibrary.com/journal/ptr.
ultrastructural studies of colonic tissue provided evidencethat the extract administration resulted in reduced inflam-mation. Treatment of rats with the extract (250, 500 and750mg/kg) resulted in a significant decrease in the extentand severity of injury of the large intestine p< 0.01,p< 0.001 and p< 0.001, respectively, as evidenced bymacroscopic damage score (Fig. 1(A)) as well as histo-pathological assessment (Fig. 3(D), Table 2) and stronglyprevented propagation of colitis. In colitis rats treatedwith the extract (250mg/kg), slight recovery of microvilliin some epithelial cells was observed. The greater inhibi-tory effect was achieved using the doses (500 and750mg/kg), which indicated a reduction of neutrophil infiltra-tion in colonic tissues. It was comparable with dexameth-asone-treated rats (Fig. 3(C)).
Biochemical markers
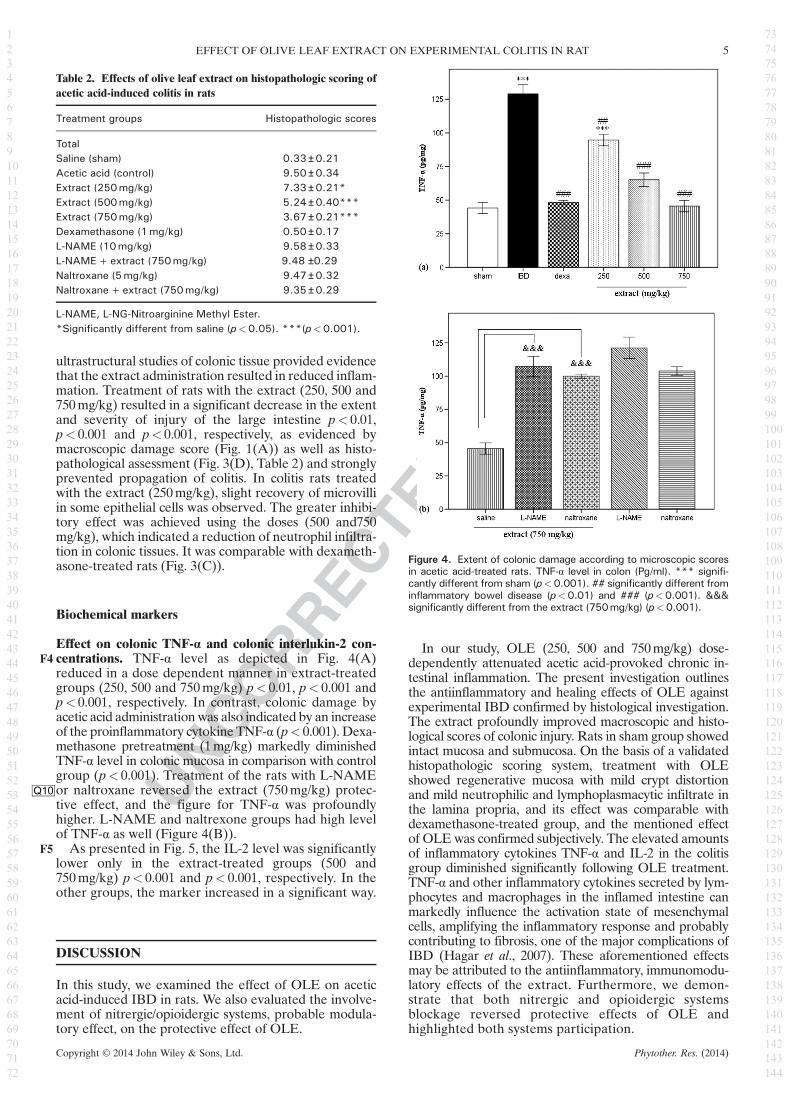
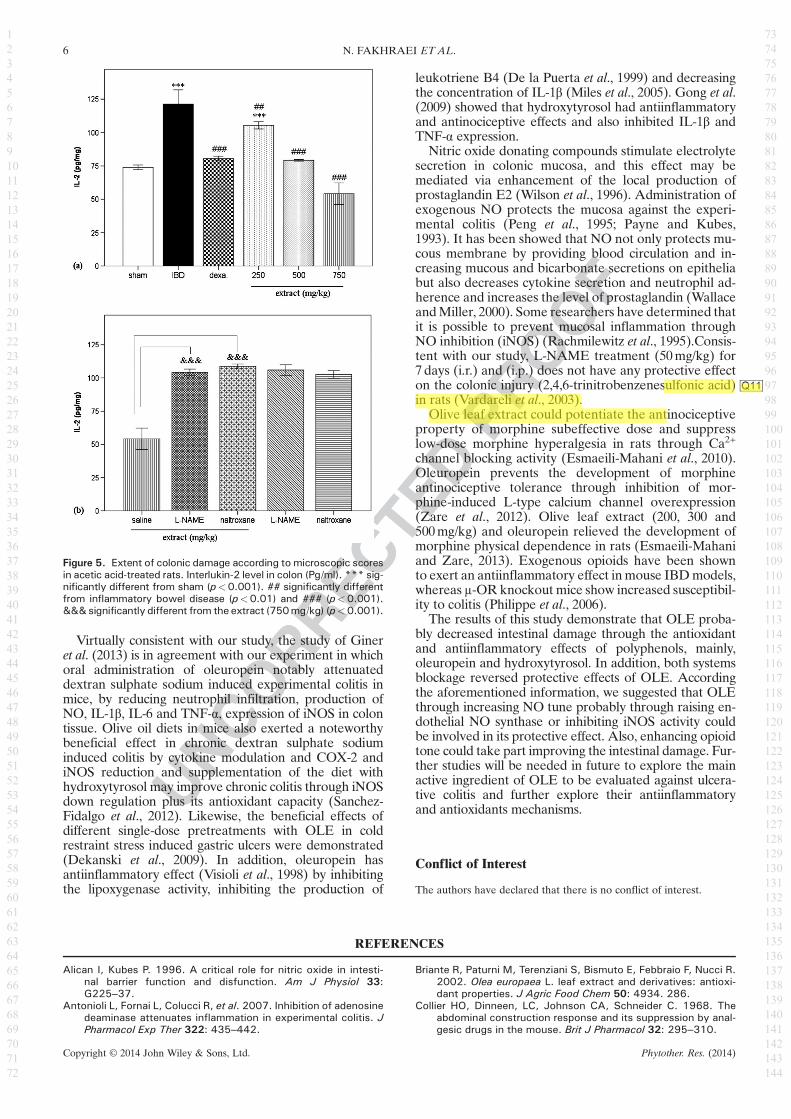
Effect on colonic TNF-α and colonic interlukin-2 con-centrations. TNF-α level as depicted in Fig.F4 4(A)reduced in a dose dependent manner in extract-treatedgroups (250, 500 and 750mg/kg) p< 0.01, p< 0.001 andp< 0.001, respectively. In contrast, colonic damage byacetic acid administrationwas also indicated by an increaseof the proinflammatory cytokine TNF-α (p< 0.001). Dexa-methasone pretreatment (1mg/kg) markedly diminishedTNF-α level in colonic mucosa in comparison with controlgroup (p< 0.001). Treatment of the rats with L-NAMEor naltroxaneQ10 reversed the extract (750mg/kg) protec-tive effect, and the figure for TNF-α was profoundlyhigher. L-NAME and naltrexone groups had high levelof TNF-α as well (Figure 4(B)).As presented in Fig.F5 5, the IL-2 level was significantly
lower only in the extract-treated groups (500 and750mg/kg) p< 0.001 and p< 0.001, respectively. In theother groups, the marker increased in a significant way.
DISCUSSION
In this study, we examined the effect of OLE on aceticacid-induced IBD in rats. We also evaluated the involve-ment of nitrergic/opioidergic systems, probable modula-tory effect, on the protective effect of OLE.
In our study, OLE (250, 500 and 750mg/kg) dose-dependently attenuated acetic acid-provoked chronic in-testinal inflammation. The present investigation outlinesthe antiinflammatory and healing effects of OLE againstexperimental IBD confirmed by histological investigation.The extract profoundly improved macroscopic and histo-logical scores of colonic injury. Rats in sham group showedintact mucosa and submucosa. On the basis of a validatedhistopathologic scoring system, treatment with OLEshowed regenerative mucosa with mild crypt distortionand mild neutrophilic and lymphoplasmacytic infiltrate inthe lamina propria, and its effect was comparable withdexamethasone-treated group, and the mentioned effectof OLE was confirmed subjectively. The elevated amountsof inflammatory cytokines TNF-α and IL-2 in the colitisgroup diminished significantly following OLE treatment.TNF-α and other inflammatory cytokines secreted by lym-phocytes and macrophages in the inflamed intestine canmarkedly influence the activation state of mesenchymalcells, amplifying the inflammatory response and probablycontributing to fibrosis, one of the major complications ofIBD (Hagar et al., 2007). These aforementioned effectsmay be attributed to the antiinflammatory, immunomodu-latory effects of the extract. Furthermore, we demon-strate that both nitrergic and opioidergic systemsblockage reversed protective effects of OLE andhighlighted both systems participation.
Table 2. Effects of olive leaf extract on histopathologic scoring ofacetic acid-induced colitis in rats
L-NAME, L-NG-Nitroarginine Methyl Ester.*Significantly different from saline (p<0.05). ***(p<0.001).
Figure 4. Extent of colonic damage according to microscopic scoresin acetic acid-treated rats. TNF-α level in colon (Pg/ml). *** signifi-cantly different from sham (p<0.001). ## significantly different frominflammatory bowel disease (p<0.01) and ### (p<0.001). &&&significantly different from the extract (750mg/kg) (p<0.001).
5EFFECT OF OLIVE LEAF EXTRACT ON EXPERIMENTAL COLITIS IN RAT
Virtually consistent with our study, the study of Gineret al. (2013) is in agreement with our experiment in whichoral administration of oleuropein notably attenuateddextran sulphate sodium induced experimental colitis inmice, by reducing neutrophil infiltration, production ofNO, IL-1β, IL-6 and TNF-α, expression of iNOS in colontissue. Olive oil diets in mice also exerted a noteworthybeneficial effect in chronic dextran sulphate sodiuminduced colitis by cytokine modulation and COX-2 andiNOS reduction and supplementation of the diet withhydroxytyrosol may improve chronic colitis through iNOSdown regulation plus its antioxidant capacity (Sanchez-Fidalgo et al., 2012). Likewise, the beneficial effects ofdifferent single-dose pretreatments with OLE in coldrestraint stress induced gastric ulcers were demonstrated(Dekanski et al., 2009). In addition, oleuropein hasantiinflammatory effect (Visioli et al., 1998) by inhibitingthe lipoxygenase activity, inhibiting the production of
leukotriene B4 (De la Puerta et al., 1999) and decreasingthe concentration of IL-1β (Miles et al., 2005). Gong et al.(2009) showed that hydroxytyrosol had antiinflammatoryand antinociceptive effects and also inhibited IL-1β andTNF-α expression.
Nitric oxide donating compounds stimulate electrolytesecretion in colonic mucosa, and this effect may bemediated via enhancement of the local production ofprostaglandin E2 (Wilson et al., 1996). Administration ofexogenous NO protects the mucosa against the experi-mental colitis (Peng et al., 1995; Payne and Kubes,1993). It has been showed that NO not only protects mu-cous membrane by providing blood circulation and in-creasing mucous and bicarbonate secretions on epitheliabut also decreases cytokine secretion and neutrophil ad-herence and increases the level of prostaglandin (WallaceandMiller, 2000). Some researchers have determined thatit is possible to prevent mucosal inflammation throughNO inhibition (iNOS) (Rachmilewitz et al., 1995).Consis-tent with our study, L-NAME treatment (50mg/kg) for7 days (i.r.) and (i.p.) does not have any protective effecton the colonic injury (2,4,6-trinitrobenzenesulfonic acid Q11)in rats (Vardareli et al., 2003).
Olive leaf extract could potentiate the antinociceptiveproperty of morphine subeffective dose and suppresslow-dose morphine hyperalgesia in rats through Ca2+
channel blocking activity (Esmaeili-Mahani et al., 2010).Oleuropein prevents the development of morphineantinociceptive tolerance through inhibition of mor-phine-induced L-type calcium channel overexpression(Zare et al., 2012). Olive leaf extract (200, 300 and500mg/kg) and oleuropein relieved the development ofmorphine physical dependence in rats (Esmaeili-Mahaniand Zare, 2013). Exogenous opioids have been shownto exert an antiinflammatory effect inmouse IBDmodels,whereas μ-OR knockout mice show increased susceptibil-ity to colitis (Philippe et al., 2006).
The results of this study demonstrate that OLE proba-bly decreased intestinal damage through the antioxidantand antiinflammatory effects of polyphenols, mainly,oleuropein and hydroxytyrosol. In addition, both systemsblockage reversed protective effects of OLE. Accordingthe aforementioned information, we suggested that OLEthrough increasing NO tune probably through raising en-dothelial NO synthase or inhibiting iNOS activity couldbe involved in its protective effect. Also, enhancing opioidtone could take part improving the intestinal damage. Fur-ther studies will be needed in future to explore the mainactive ingredient of OLE to be evaluated against ulcera-tive colitis and further explore their antiinflammatoryand antioxidants mechanisms.
Conflict of Interest
The authors have declared that there is no conflict of interest.
REFERENCES
Alican I, Kubes P. 1996. A critical role for nitric oxide in intesti-nal barrier function and disfunction. Am J Physiol 33:G225–37.
Antonioli L, Fornai L, Colucci R, et al. 2007. Inhibition of adenosinedeaminase attenuates inflammation in experimental colitis. JPharmacol Exp Ther 322: 435–442.
Briante R, Paturni M, Terenziani S, Bismuto E, Febbraio F, Nucci R.2002. Olea europaea L. leaf extract and derivatives: antioxi-dant properties. J Agric Food Chem 50: 4934. 286.
Collier HO, Dinneen, LC, Johnson CA, Schneider C. 1968. Theabdominal construction response and its suppression by anal-gesic drugs in the mouse. Brit J Pharmacol 32: 295–310.
Figure 5. Extent of colonic damage according to microscopic scoresin acetic acid-treated rats. Interlukin-2 level in colon (Pg/ml). *** sig-nificantly different from sham (p<0.001). ## significantly differentfrom inflammatory bowel disease (p<0.01) and ### (p<0.001).&&&significantly different from the extract (750mg/kg) (p<0.001).
De la Puerta, Ruiz Gutiérrez RV, Hoult JR. 1999. Inhibition of leuko-cyte 5-lipoxygenase by phenolics from virgin olive oil.Biochem Pharmacol 57: 445–449.
Dekanski D, Janićijević-Hudomal S, Ristić S, et al. 2009. Attenua-tion of cold restraint stress-induced gastric lesions by an oliveleaf extract. Gen Physiol Biophys 28: 135–42.
El SN, Karakaya S. 2009. Olive tree (Olea europaea) leaves: poten-tial beneficial effects on human health. Nutr Rev 67: 632.
Esmaeili-Mahani S, Rezaeezadeh-Roukerd M, Esmaeilpour K, et al.2010. Olive (Olea europaea L.) leaf extract elicits antinociceptiveactivity, potentiatesmorphine analgesia and suppressesmorphinehyperalgesia in rats. J Ethnopharmacol 28: 132.
Esmaeili-Mahani S, Zare L. 2013. Olive (Olea europaea L.) leafextract and its main component (oleuropein) mitigate thedevelopment of morphine physical dependence in rats. PhysiolPharmacol 16: 360–370.
Garcia, OB, Castillo J, Lorente J, Ortuno A, Del-Rio JA. 2000. An-tioxidant activity of phenolics extracted from Olea europaea L.leaves. Food Chem 68: 457–462.
GongD,GengC, Jiang L, Cao J, YoshimuraH, Zhong L. 2009. Effectsof hydroxytyrosol-20 on carrageenan induced acute inflamma-tion and hyperalgesia in rats. Phytother Res 23: 646–650.
Hagar HH, El-Medany A, El-Eter Eman, Arafa M. 2007. Ameliora-tive effect of pyrrolidine dithiocarbamate on acetic acid-induced colitis in rats. Eur J Pharmacol 554: 69–77.
Hashemi P, Raeisi F, Ghiasvand AR, Rahimi A. 2010. Reversed-phase dispersive liquid-liquid microextraction with centralcomposite design optimization for pre-concentration andHPLC determination of oleuropein. Talanta 80: 1926–31.
Huang FP, Niedbala W, Wei XQ, et al. 1998. Nitric oxide regulatesTh1 cell development through the inhibition of IL-12 synthesisby macrophages. Eur J Immunol 28: 4062–70.
Kojima R, Hamamoto S, Moriwaki M, Iwadate K, Ohwaki T. 2001.The new experimental ulcerative colitis model in rats inducedby subserosal injection of acetic acid. Folia Pharmacol J118: 123–30.
La JH, Kim TW, Sung TS, Kang JW, Kim HJ, Yang IS. 2003.Visceral hypersensitivity and altered colonic motility aftersubsidence of inflammation in a rat model of colitis. World JGastroenterol 9: 2791–2795.
Ludwiczek O, Vannier E, Borggraefe I, et al. 2004. Imbalancebetween interleukin-1 agonists and antagonists: relationshipto severity of inflammatory bowel disease. Clin Exp Immunol138: 323–9.
MacnaughtonWK, Lowe SS, Cushyng K. 1998. Role of nitric oxidein inflammation-induced suppression of secretion in a mousemodel of acute colitis. Am J Physiol 275: 1353–1360.
McCafferty DM. 2000. Peroxynitrite and inflammatory boweldisease. Gut 46: 436–439.
Miles EA, Zoubouli P, Calder PC. 2005. Differential anti-inflammatoryeffects of phenolic compounds from extra virgin olive oil identi-fied in human whole blood cultures. Nutrition 21: 389–94.
Moncada S. 1992. The 1991 Ulf von Euler Lecture. The L-arginine:nitric oxide pathway. Acta Physiol Scand 145: 201–27.
Morris GP, Beck PL, Herridge MS, Depew WT, Szewezuk MR,Wallace JL. 1989. Hapten-induced model of chronic in-flammation and ulceration in the rat colon.Gastroenterology96: 795–803.
Murthy SN, Cooper HS, Shim H, Shah RS, Ibrahim SA, SedergranDJ. 1993. Treatment of dextran sulfate sodium-induced
murine colitis by intracolonic cyclosporin. Dig Dis Sci38: 1722–1734.
Nagura H, Ohtani H, Sasano H, Matsumoto T. 2001. The immuneinflammatory mechanism for tissue injury in inflammatorybowel disease and Helicobacter pylori-infected chronic activegastritis roles of the mucosal immune system. Digestion63: 12–21.
Payne D, Kubes P. 1993. Nitric oxide donors reduce the rise inreperfusion-induced intestinal mucosal permeability. Am JPhysiol 265: G189–95.
Peng HB, Libby P, Liao JK. 1995. Induction and stabilization of Ikappa B alpha by nitric oxide mediates inhibition of NF-kappaB. J Biol Chem 270: 14214–9.
Philippe D, Chakass D, Thuru X, et al. 2006. Mu opioid receptorexpression is increased in inflammatory bowel diseases:implications for homeostatic intestinal inflammation. Gut55: 815–23.
Pol O, Puig MM. 2004. Expression of opioid receptors duringperipheral inflammation. Curr Top Med Chem 4: 51–61.
Rachmilewitz D, KarmelIi F, Okon E, Bursztyn M. 1995. Experimen-tal colitis is ameliorated by inhibition of nitric oxide synthaseactivity. Gut 37: 247–255.
Sánchez-Fidalgo S, Sánchez de Ibargüen L, Cárdeno A, Alarcón dela Lastra C. 2012. Influence of extra virgin olive oil dietenriched with hydroxytyrosol in a chronic DSS colitis model.Eur J Nutr 51: 497–506.
Rogers TJ, Peterson PK. 2003. Opioid G protein-coupled recep-tors: signals at the crossroads of inflammation. TrendsImmunol 24: 116–121.
Sekizuka E, Grisham MB, Li M, Deitch EA, Granger DN. 1988.Inflammation-induced intestinal hyperemia in the rat: role ofneutrophils. Gastroenterology 95: 1528–34.
Speroni E, Guerra MC, Minghetti A, et al. 1998. Oleuropeinevaluated in vitro and in vivo as an antioxidant. PhytotherRes 12: 98–100.
Vardareli E, Dundar E, Angin K, Saricam T, Inal M. 2003. Effects ofintrarectal and intraperitoneal N (G)-nitro-L-arginine methylester treatment in 2,4,6-trinitrobenzenesulfonic acid inducedcolitis in rats. Exp Toxicol Pathol 55: 271–6.
Visioli F, Bellomo G, Galli C. 1998. Free radical-scavenging proper-ties of olive oil polyphenols. Biochem Biophys Res Commun247: 60–4.
Visioli F, Poli A, Gall C. 2002. Antioxidant and other biologicalactivities of phenols from olives and olive oil. Med Res Rev22: 65–75.
Wallace JL, Miller MJ. 2000. Nitric oxide in mucosal defense: alittle goes a long way. Gastroenterology 119: 512–520.
Wang L, Geng C, Jiang L, et al. 2008. The anti atheroscleroticeffect of olive leaf extract is related to suppressed inflamma-tory response in rabbits with experimental atherosclerosis.Eur J Nutr 47: 235–243.
Wilson kT, Vaandrager A B, De Vente J, Musch MW, De Jonge HR,Chang EB. 1996. Production and localization of cGMP andPGE2 in nitroprusside-stimulated rat colonic ion transport.Am J Physiol 270: C832–840.
Wood JD, Galligan JJ. 2004. Function of opioids in the entericnervous system. Neurogastroenterol Motil 16: 17–28
Zare L, Esmaeili-Mahani S, Abbasnejad M, RasoulianB, Sheibani V,Sahraei H, Kaeidi A. 2012. Oleuropein, chief constituent ofolive leaf extract, prevents the development of morphineanti-nociceptive tolerance through inhibition of morphine-induced L-type calcium channel overexpression. PhytotherRes 11: 1731–1737.
7EFFECT OF OLIVE LEAF EXTRACT ON EXPERIMENTAL COLITIS IN RAT
During the copyediting of your paper, the following queries arose. Please respond to these by annotating your proofs with thenecessary changes/additions.• If you intend to annotate your proof electronically, please refer to the E-annotation guidelines.• If you intend to annotate your proof by means of hard-copy mark-up, please refer to the proof mark-up symbols guidelines. Ifmanually writing corrections on your proof and returning it by fax, do not write too close to the edge of the paper. Pleaseremember that illegible mark-ups may delay publication.
Whether you opt for hard-copy or electronic annotation of your proofs, we recommend that you provide additional clarificationof answers to queries by entering your answers on the query sheet, in addition to the text mark-up.
Query No. Query Remark
Q1 AUTHOR: The running head short title exceeds 60 characters, thus needs to bemodified. Please check if appropriate.
Q2 AUTHOR: Please check that authors and their affiliations are correct.
Q3 AUTHOR: L-NG-Nitroarginine Methyl Ester. Is this the correct definition for L-NAME? Please change if this is incorrect.
Q4 AUTHOR: Please check the levels of section heads if correct.
Q5 AUTHOR: Endothelial nictric oxide synthase. Is this the correct definition for eNOS?Please change if this is incorrect.
Q6 AUTHOR: ’eNOS appears to be a homeostatic......epithelial permeability.’ Thissentence has been modified. Please check if appropriate.
Q7 AUTHOR: Inducible nitric oxide synthase. Is this the correct definition for iNOS?Please change if this is incorrect.
Q8 AUTHOR: Tables 1 and 2 have been renumbered according to citation order. Pleasecheck.
Q9 AUTHOR: Figures 2 and 3 have been renumbered according to citation order. Pleasecheck.
Q10 AUTHOR: All occurrences of ’naltroxan’ have been changed to ’naltroxane’. Pleasecheck if appropriate.
Q11 AUTHOR: 2,4,6-trinitrobenzenesulfonic acid. Is this the correct definition for TNBS?Please change if this is incorrect.
Q12 AUTHOR: Please check volume if capture correctly, if correct please provide pages.
na.fakhrayi
Sticky Note
appropriate
na.fakhrayi
Sticky Note
The order of the affiliations has changed.
na.fakhrayi
Sticky Note
correct
na.fakhrayi
Sticky Note
correct
na.fakhrayi
Sticky Note
correct
na.fakhrayi
Sticky Note
correct
na.fakhrayi
Sticky Note
checked
na.fakhrayi
Sticky Note
checked
na.fakhrayi
Sticky Note
appropriate
na.fakhrayi
Sticky Note
correct
na.fakhrayi
Sticky Note
76 (6): 1113–1120
USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
Required software to e-Annotate PDFs: Adobe Acrobat Professional or Adobe Reader (version 7.0 or above). (Note that this document uses screenshots from Adobe Reader X) The latest version of Acrobat Reader can be downloaded for free at: http://get.adobe.com/uk/reader/
Once you have Acrobat Reader open on your computer, click on the Comment tab at the right of the toolbar:
1. Replace (Ins) Tool – for replacing text.
Strikes a line through text and opens up a text box where replacement text can be entered.
How to use it
Highlight a word or sentence.
Click on the Replace (Ins) icon in the Annotations section.
Type the replacement text into the blue box that appears.
This will open up a panel down the right side of the document. The majority of tools you will use for annotating your proof will be in the Annotations section, pictured opposite. We’ve picked out some of these tools below:
2. Strikethrough (Del) Tool – for deleting text.
Strikes a red line through text that is to be deleted.
How to use it
Highlight a word or sentence.
Click on the Strikethrough (Del) icon in the Annotations section.
3. Add note to text Tool – for highlighting a section to be changed to bold or italic.
Highlights text in yellow and opens up a text box where comments can be entered.
How to use it
Highlight the relevant section of text.
Click on the Add note to text icon in the Annotations section.
Type instruction on what should be changed regarding the text into the yellow box that appears.
4. Add sticky note Tool – for making notes at specific points in the text.
Marks a point in the proof where a comment needs to be highlighted.
How to use it
Click on the Add sticky note icon in the Annotations section.
Click at the point in the proof where the comment should be inserted.
Type the comment into the yellow box that appears.
USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
For further information on how to annotate proofs, click on the Help menu to reveal a list of further options:
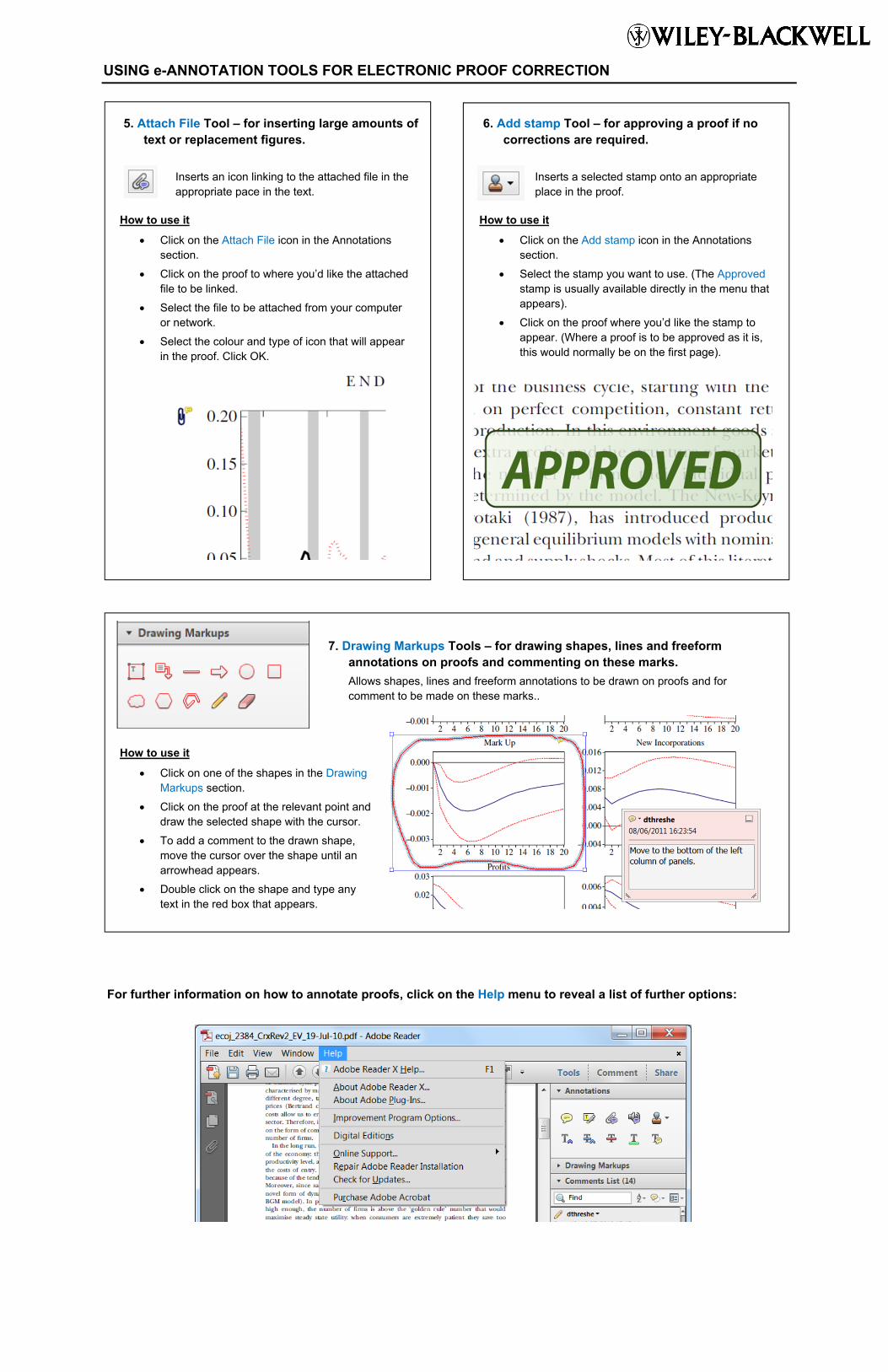
5. Attach File Tool – for inserting large amounts of text or replacement figures.
Inserts an icon linking to the attached file in the appropriate pace in the text.
How to use it
Click on the Attach File icon in the Annotations section.
Click on the proof to where you’d like the attached file to be linked.
Select the file to be attached from your computer or network.
Select the colour and type of icon that will appear in the proof. Click OK.
6. Add stamp Tool – for approving a proof if no corrections are required.
Inserts a selected stamp onto an appropriate place in the proof.
How to use it
Click on the Add stamp icon in the Annotations section.
Select the stamp you want to use. (The Approved stamp is usually available directly in the menu that appears).
Click on the proof where you’d like the stamp to appear. (Where a proof is to be approved as it is, this would normally be on the first page).
7. Drawing Markups Tools – for drawing shapes, lines and freeform annotations on proofs and commenting on these marks.
Allows shapes, lines and freeform annotations to be drawn on proofs and for comment to be made on these marks..
How to use it
Click on one of the shapes in the Drawing Markups section.
Click on the proof at the relevant point and draw the selected shape with the cursor.
To add a comment to the drawn shape, move the cursor over the shape until an arrowhead appears.
Double click on the shape and type any text in the red box that appears.