College of Education School of Continuing and Distance Education 2014/2015 – 2016/2017 PSYC 221 Introduction to General Psychology Session 7 – Human development across the life span Lecturer: Dr. Joana Salifu Yendork, Psychology Department Contact Information: [email protected]
Transcript
College of Education
School of Continuing and Distance Education 2014/2015 – 2016/2017
PSYC 221
Introduction to General
Psychology
Session 7 – Human development across the life span
Lecturer: Dr. Joana Salifu Yendork, Psychology Department Contact Information: [email protected]
Session Overview
• As we go about our daily lives, we develop continuously and we will continue to develop until we die. Development is concerned with the physical, cognitive and socio-emotional changes that occur in humans from conception until death. This session will focus on development across humans’ lifespan.
Slide 2
Session Outline
The key topics to be covered in the session are as follows:
• General overview of human development
• Prenatal development
• Infancy & Childhood
• Adolescence
• Adulthood
Slide 3
Reading List
• Chapter 9 of Essentials of Feldman (2007), Essential of understanding Psychology
• Chapter 3 of Myers (2008), Exploring psychology
Slide 4
GENERAL OVERVIEW OF HUMAN DEVELOPMENT
Topic One
Slide 5
Overview of human development
• Developmental psychology examines how people are continually developing, physically, cognitively, and socially, through out the lifespan (Myers, 2008)
• Developmental psychology research focuses on three major issues:
• Nature vs. nurture: How genetic inheritance (our nature) and experience (the nurture we receive) influence human development
• Continuity vs. change: Is development a gradual, continuous process, or does it proceed through a sequence of separate stages?
• Stability/change: Do our early personality traits persist through life, or do we become different persons as we age?
Slide 6
Overview of human development
• There are three domains of human development:
– Physical
– Cognitive
– Socio-emotional/psychosocial
• Stages of development range from conception to old age
• Conception occurs when a matured egg (released from the ovary) fuses with a sperm
Slide 7
Overview of human development
Slide 8
PRENATAL DEVELOPMENT Topic Two
Slide 9
Prenatal development
• There are three stage of prenatal development
• The zygote stage: first 10-14 days
• After the nuclei of the egg and sperm fuse, cell division begins
• The cell devises into 2, 4, 8, 16, 100…
• At this stage, cells begin to differentiate into specialized locations and structures
• The Embryonic stage: 2 to 8 weeks
This stage begins with the multicellular cluster that implants in the uterine wall.
At this stage, differentiated cells develop into organs and bones
Slide 10
Slide 11
Prenatal development
• The fetal period: 9 weeks to birth
• 9th week of pregnancy until the baby is born.
• Period of rapid growth and refinement of all organ systems
• All the major organ systems begin to function, and the developing organism grows rapidly
• At each prenatal stage, genetic and environmental factors affect our development
• Teratogens: any disease, drug, or other environmental agent that can harm a developing embryo or fetus by causing physical deformities, severely retarded growth, blindness, brain damage, or even death
Slide 12
Prenatal development
• Teratogens include:
• Maternal diseases: rubella/German measles, Syphilis, Genital herpes, AIDS
• Infants are born with skills that aids them to survive outside the womb
• Reflexes are responses that are inborn and do not have to be learned.
• The rooting reflex--when something touches a newborn’s cheek, the infant turns toward that side with an open mouth.
• The sucking reflex can be triggered by a fingertip.
• Crying when hungry is the newborn talent of using just the right sounds to motivate parents to end the noise and feed the baby.
Slide 15
Physical development in infancy and childhood
• Infancy is a period from birth to 2 years
• Brain development
• In the womb, the number of neurons grows by about 750,000 new cells per minute in the middle trimester.
• Beginning at birth, the connections among neurons multiply with formation of more branches and neural networks.
• In infancy, the growth in neural connections takes place initially in the less complex parts of the brain (the brainstem and limbic system), as well as the motor and sensory strips.
– This enables body functions and basic survival skills.
• In early childhood, neural connections multiply in the association areas.
– This enables advancements in controlling attention and behavior (frontal lobes) and also in thinking, memory, and language.
Slide 16
Motor development
Slide 17
• As the body and brain mature, the child’s motor development progresses along the sequence below
• Physical training generally cannot change the timing
• But there are individual differences in the timing
Cognitive development
•Cognition refers to the mental activities associated with thinking, knowing, remembering and communication •These mainly include:
–problem-solving. –figuring out how the world works. –developing models and concepts. –storing and retrieving knowledge. –understanding and using language. –using self-talk and inner thoughts.
Slide 18
Cognitive development: Jean Piaget (1896-1980)
• Piaget’s work revealed that: • The child’s mind is not a miniature model of an adult’s • A child’s mind develops through a series of five stages, in an upward
march from the newborn’s simple reflexes to the adult’s abstract reasoning power
• The driving force behind the intellectual progression is struggle to make sense of our experiences
• Children are active thinkers, constantly trying to construct more advanced understandings of the world
• The maturing brain builds schemas, concepts or mental molds into which we pour our experiences
• We assimilate new experiences—we interpret them in terms of our current understandings (schemas)
• We also adjust, or accommodate, our schemas to fit the particulars of new experiences
Slide 19
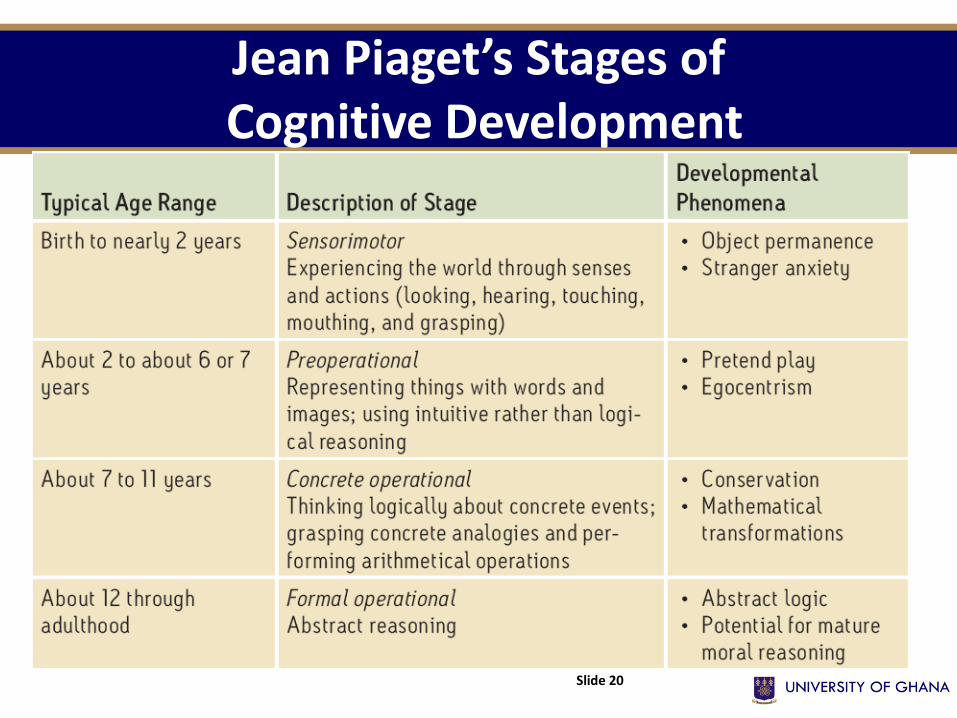
Jean Piaget’s Stages of Cognitive Development
Slide 20
Contributions & criticisms of Piaget’s theory
Contributions:
• Piaget’s early theorizing and research legitimized the study of children’s thinking, and his early work linking moral development to cognitive development contributed immensely to a growing area of developmental research—social cognition.
• Piaget’s theory has also had a strong impact on education. Eg., popular discovery-based educational programs are based on the premise that children do not think like adults and that they learn best by having ―hands-on‖ educational experiences with their environment.
Slide 21
Contributions & criticisms of Piaget’s theory
Criticisms:
1. development is a continuous process.
2. children show some mental abilities and operations at an earlier age than Piaget thought.
3. formal logic is a smaller part of cognition, even for adults, than Piaget believed
Slide 22
Social development
•Children in all cultures develop intense emotional bond with their caregivers right from birth •At about 8 months, they develop separation anxiety: fear of separation from caregiver •By 12 months, they cling tightly to caregivers when frightened or expect separation and when reunited, they meet the caregiver with smiles and hugs •Attachment refers to an emotional tie to another person. In children, attachment can appear as a desire for physical closeness to a caregiver.
• In the past, it was thought that attachment resulted from the need for nourishment
• Studies by Harlow and Harlow in the 1950’s revealed otherwise
Slide 23
Social development
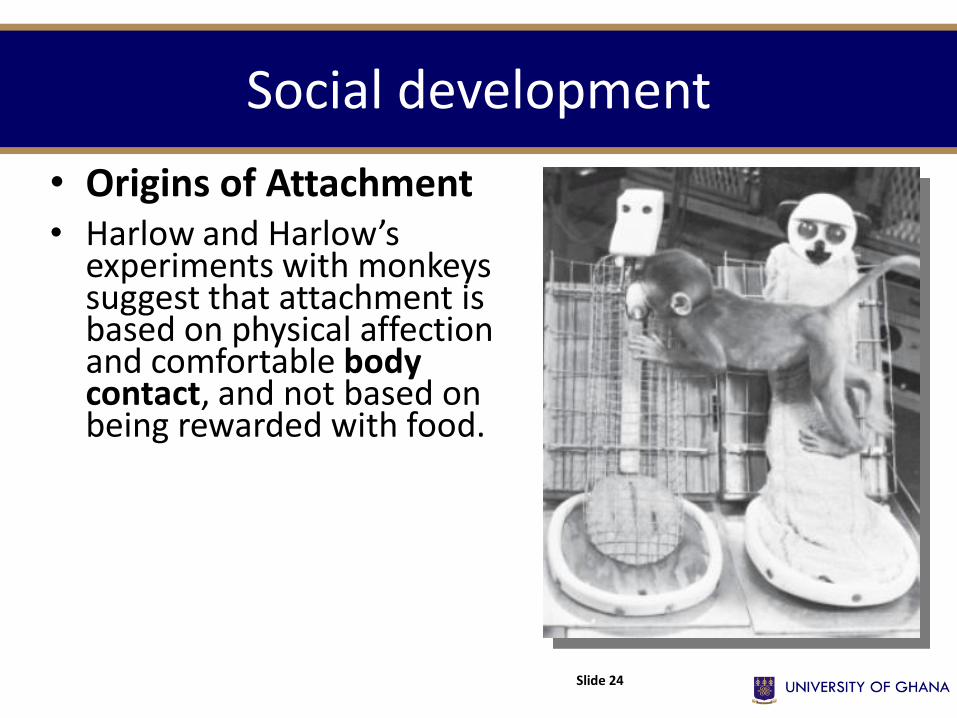
• Origins of Attachment • Harlow and Harlow’s
experiments with monkeys suggest that attachment is based on physical affection and comfortable body contact, and not based on being rewarded with food.
Slide 24
Attachment Variations
The degree and style of parent-child attachment has been tested by Mary Ainsworth in the “strange situations” test. In this test, a child is observed as:
1.a mother and infant child are alone in an unfamiliar (“strange”) room; the child explores the room as the mother just sits.
2.a stranger enters the room, talks to the mother, and approaches the child; the mother leaves the room.
3.After a few moments, the mother returns.
Reactions to Separation and
Reunion •Secure attachment: most children (60 percent) feel distress when mother leaves, and seek contact with her when she returns •Insecure attachment (anxious style): clinging to mother, less likely to explore environment, and may get loudly upset with mother’s departure and remain upset when she returns •Insecure attachment (avoidant style): seeming indifferent to mother’s departure and return •Insecure attachment (disorganized): not forming a coherent or consistent style.
25
Determinants of attachment styles
• It has been found that both temperament and parenting style interact to determine children’s attachment styles
• Temperament refers to a person’s characteristic style and intensity of emotional reactivity. – Some infants have an “easy” temperament; they are happy, relaxed, and
calm, with predictable rhythms of needing to eat and sleep.
– Some infants seem to be “difficult”; they are irritable, with unpredictable needs and behavior, and intense reactions.
• Mary Ainsworth believed that sensitive, responsive, calm parenting is correlated with the secure attachment style.
• Monkeys with unresponsive artificial mothers showed anxious insecure attachment.
• Training in sensitive responding for parents of temperamentally-difficult children led to doubled rates of secure attachment.
Slide 26
Impact of deprivation of attachment
• Genetics and biology still play a role in determining the outcome of prolonged deprivation.
• Some people’s stress hormone systems seem to be more easily damaged by chronic stress, and some people’s serotonin pathways more easily become inefficient.
• If children live without safe, nurturing, affectionate caretaking, they may still be resilient, that is bounce back, attach, and succeed.
• However, if the child experiences severe, prolonged deprivation or abuse, he or she may: – have difficulty forming attachments. – have increased anxiety and depression. – have lowered intelligence. – show increased aggression.
Slide 27
Self-concept
A major task of infancy may be to form healthy attachments.
A major task of childhood may be to form a healthy self-concept: a stable and positive understanding of identity.
By age 8-10, a child moves from “that’s me in the mirror” to “I have skills, preferences, and goals”; this prepares the child for confident success.
Slide 28
ADOLESCENCE Topic Four
Slide 29
Adolescence
• This is the period spent transitioning from child to adult—starts with the physical beginnings of sexual maturity and ends with the social achievement of independent adult status.
• G. Stanley Hall (1904), describe adolescence the tension between biological maturity and social dependence created a period of “storm and stress.”
• Adolescence can also be a time of vitality without the cares of adulthood, a time of rewarding friendships, of heightened idealism and a growing sense of life’s exciting possibilities.
Slide 30
Sexual maturation
• Adolescence begins with puberty: the time of sexual maturation (becoming physically able to reproduce).
•During puberty, increased sex hormones lead to:
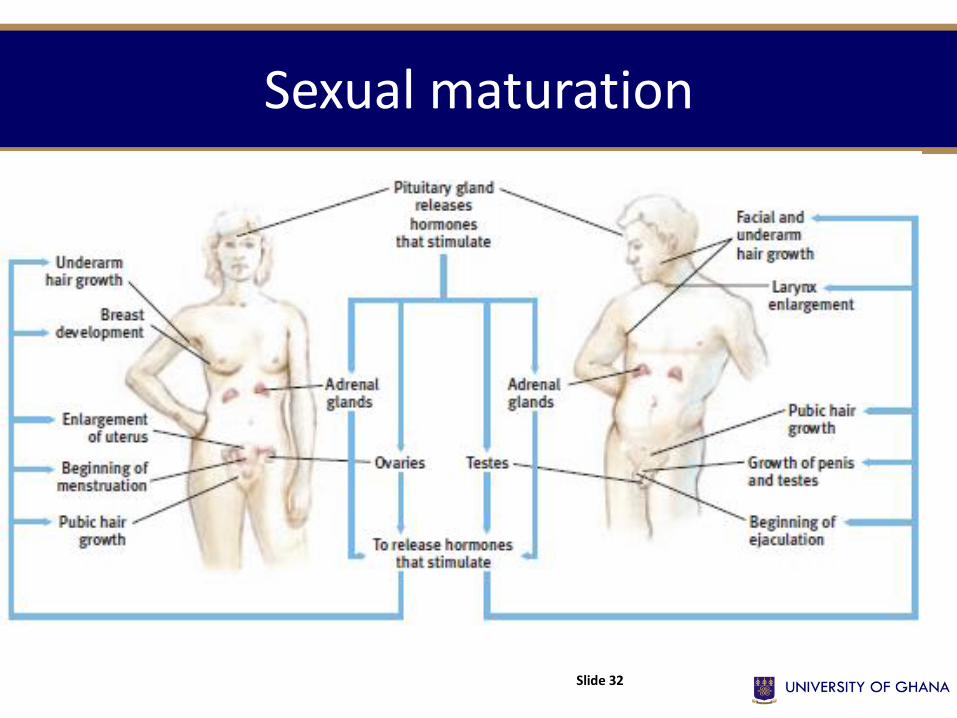
–primary (e.g. reproductive organs and external genitalia) and secondary sex characteristics (breast and hip, facial hair and deepened voice in boys, pubic and underarm hair in both sexes)
–some changes in mood and behavior.
–Beginning of menarche in girls and spermache in boys
•Height changes •Because girls begin puberty sooner than boys, girls briefly overtake boys in height.
Slide 31
Sexual maturation
Slide 32
Brain development • During puberty, the brain stops automatically adding new
connections, and becomes more efficient by “rewiring.” – “pruning” away the connections not being used – coating the well-used connections in myelin, in order to speed up
nerve conduction • This makes early adolescence a crucial time to learn as much as you
can!
• As with the formation of the brain in early childhood, the brain’s rewiring process (pruning and mylenization) starts with the survival functions and gets to the frontal lobes last (they don’t finish maturing until age 25!).
• As a result, although intellectually able to judge consequences of an action, adolescents assign much more weight to benefits
• More likely when around peers. Slide 33
Cognitive development
•According to Jean Piaget, adolescents are in the formal operational stage. They use this reasoning to:
–think about how reality compares to ideals.
–think hypothetically about different choices and their consequences.
–plan how to pursue goals.
–think about the minds of others, including “what do they think of me?”
•Although adolescents are able to make plans to meet goals, they may still tend to make choices based on shorter-term, immediate benefits rather than long-term goals.
•Adolescents can picture the minds of others, but they retain some childhood egocentrism. They mainly wonder what others think about them, and assume no one else can understand their experience
Slide 34
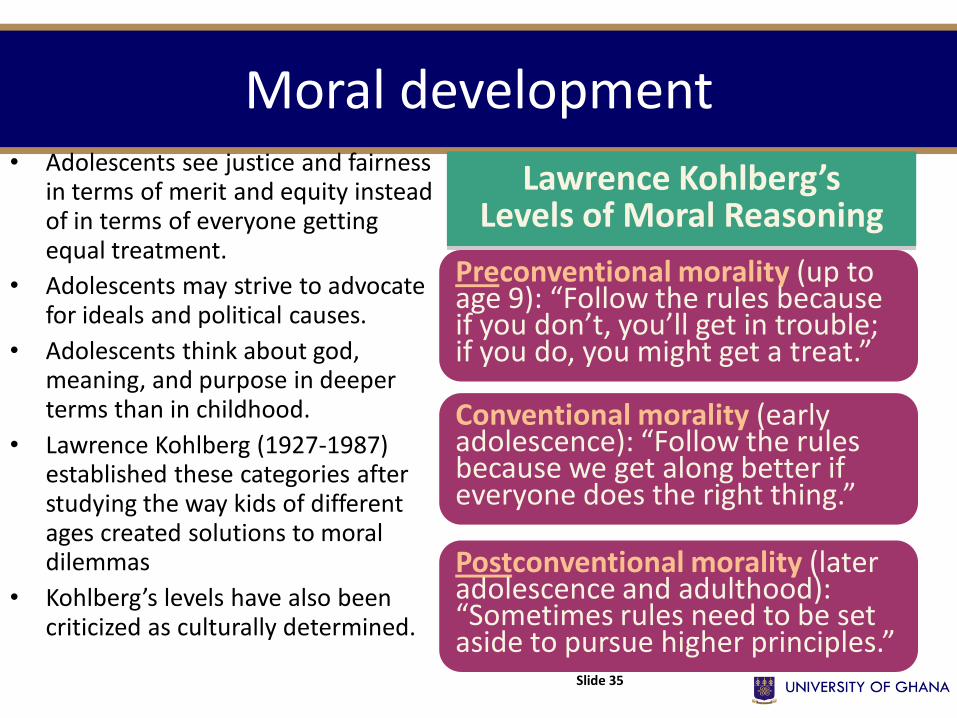
Moral development • Adolescents see justice and fairness
in terms of merit and equity instead of in terms of everyone getting equal treatment.
• Adolescents may strive to advocate for ideals and political causes.
• Adolescents think about god, meaning, and purpose in deeper terms than in childhood.
• Lawrence Kohlberg (1927-1987) established these categories after studying the way kids of different ages created solutions to moral dilemmas
• Kohlberg’s levels have also been criticized as culturally determined.
Slide 35
Preconventional morality (up to age 9): “Follow the rules because if you don’t, you’ll get in trouble; if you do, you might get a treat.”
Conventional morality (early adolescence): “Follow the rules because we get along better if everyone does the right thing.”
Postconventional morality (later adolescence and adulthood): “Sometimes rules need to be set aside to pursue higher principles.”
Lawrence Kohlberg’s Levels of Moral Reasoning
Social development: identity formation
• Erik Erikson’s model of lifelong psychosocial development sees adolescence as a struggle to form an identity, a sense of self, out of the social roles adolescents are asked to play.
• Adolescents may try out different “selves” with peers, with parents, and with teachers.
• For Erikson, the challenge in adolescence was to test and integrate the roles in order to prevent role confusion (which of those selves, or what combination, is really me?).
• Some teens solve this problem simply by adopting one role, defined by parents or peers.
• In some countries, added years of education and later marriage has delayed full adult independence beyond traditional adolescence. This seems to have created a new phase which can be called emerging adulthood, ages 18-25.
• During adolescence, the parent-adolescent relationship is mostly strained and there is increased rate of conflict Slide 36
ADULTHOOD Topic Five
Slide 37
Physical development
Slide 38
• In the mid-20’s, humans reach a peak in the natural physical abilities which come with biological maturation: – muscular strength – cardiac output – reaction time – sensory sensitivity
• To what extent can training overcome the decline that follows?
• With strength and endurance training, one can improve compared to someone not training, but it does not change the decline compared to a younger person doing the same training
Physical development
• Between ages 40 and 60, physical vitality (such as endurance and strength) may still be more of a function of lifestyle than of biological decline.
• Some changes are still driven by genetic maturation, especially the end of our reproductive years.
• Generally, there is a gradual decline in sexual activity in adulthood, although sexuality can continue throughout life.
• This stage is also the time when the reproductive years end for women
• Around age 50, women enter menopause (the end of being able to get pregnant).
Slide 39
Physical development
• Men experience no equivalent to menopause—no cessation of fertility, no sharp drop in sex hormones.
• They do experience a more gradual decline in sperm count, testosterone level, and speed of erection and ejaculation.
• But most age without such problems. After middle age, most men and women remain capable of satisfying sexual activity.
Slide 40
Physical Changes with Age
•The following abilities decline as we age:
–visual acuity, both sharpness and brightness –hearing, especially sensing higher pitch –reaction time and general motor abilities –neural processing speed, especially for complex and novel tasks
41
Health/Immunity Changes with Age
The bad
news
The good news
The immune system declines with age, and can have difficulty fighting off major illnesses.
The immune system has a lifetime’s accumulation of antibodies, and does well fighting off minor illnesses.
42
Changes in the Brain with Age
• Myelin-enhanced neural processing speed peaks in the teen years, and declines thereafter.
• Regions of the brain related to memory begin to shrink with age, making it harder to form new memories.
• The frontal lobes atrophy, leading eventually to decreased inhibition and self-control.
• By age 80, a healthy brain is 5 percent lighter than a brain in middle adulthood. 43
Alzheimer’s Disease and Other Dementias
•Dementia, including the Alzheimer’s type, is NOT a “normal” part of aging but common with aging.
Dementia Symptoms:
•decreased ability to recall recent events and the names of familiar objects and people
•emotional unpredictability; flat, then uninhibited, then angry
•confusion, disorientation, and eventual inability to think or communicate
•Brain Changes of Alzheimer’s Disease •loss of brain cells and neural network connections •deterioration of neurons that produce acetylcholine, the memory neurotransmitter •shriveled and broken protein filaments forming plaques at the tips of neurons •dramatic shrinking of the brain
44
Why don’t we live forever? • Possible biological answers include: • Nurture/Environment: An accumulation of stress,
damage, and disease wears us down until one of these factors kills us.
• Genes: Some people have genes that protect against some kinds of damage.
• Even with great genes and environment, telomeres (the tips at the end of chromosomes) wear down with every generation of cell duplication and we stop healing well.
45
Cognitive development
• Even without the brain changes of dementia, there are some changes in our ability to
learn, process, and recall information.
• The ability to recognize information, and to use previous knowledge as expertise, does
not decline with age.
• Rote memorization ability declines more than ability to learn meaningful information.
• Prospective memory, planning to recall, (“I must remember to do…) also declines.
• The ability to learn new skills declines less than the ability to learn new information.
• Crystallized intelligence—one’s accumulated knowledge as reflected in vocabulary and
analogies tests—increases up to old age. Fluid intelligence—one’s ability to reason
speedily and abstractly, as when solving novel logic problems—decreases slowly up to
age 75 or so, then more rapidly, especially after age 85
Slide 46
Social development
• As people enter their forties, they undergo a transition to middle adulthood, a time when they realize that life will soon be mostly behind them instead of ahead of them.
• For many the midlife transition is a crisis, a time of great struggle, regret, or even feeling struck down by life
• The “midlife crisis”--re-evaluating one’s life plan and success--does not seem to peak at any age.
• For the 25 percent of adults who do have this emotional crisis, the trigger seems to be the challenge of major illness, divorce, job loss, or parenting.
• Although the “midlife crisis” may not be a function of age, people do feel pressured by a “social clock (the definition of “the right time” to leave home, get a job, marry, have children, and retire) of achievement expectation.
Slide 47
Social development
Slide 48
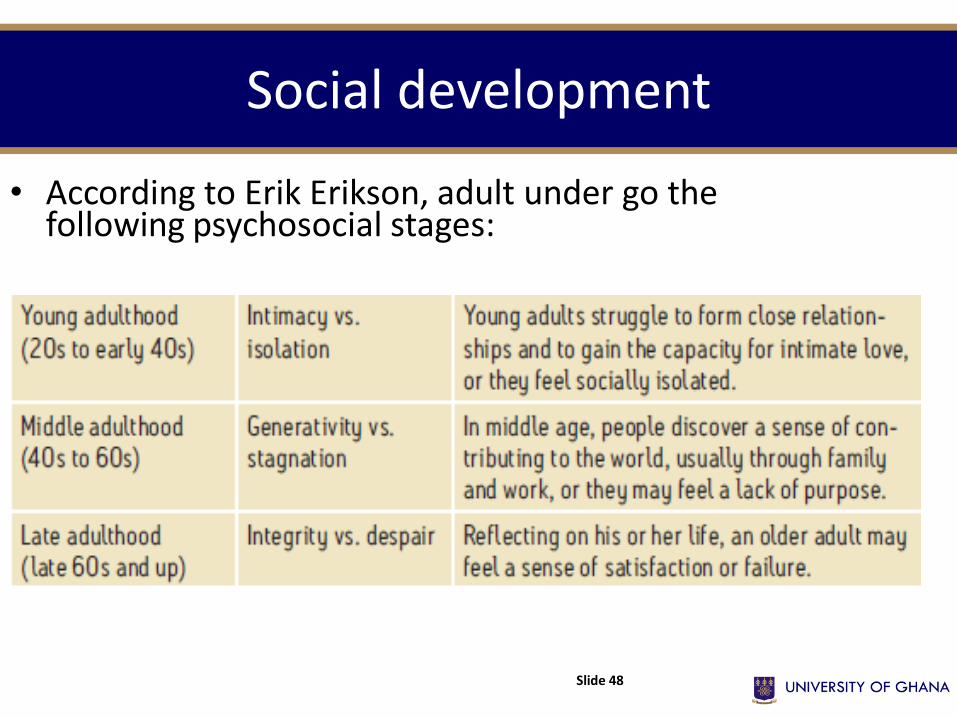
• According to Erik Erikson, adult under go the following psychosocial stages:
Commitment to Love
• The desire to commit to a loving relationship may have evolved to help vulnerable human children survive long enough to reproduce.
• Couples who go through marriage/union ceremonies tend to stay together more than couples who simply live together.
• Marriage, compared to being single, is associated with ‘happiness’ and with fewer social problems such as crime and child delinquency.
• Work roles can largely define adult identity, especially in individualistic capitalist societies.
• Tough economic times make it difficult to find work, much less follow a career path.
• Work satisfaction seems to be a function of having the work fit a person’s interests and providing a sense of competence and accomplishment.
• Work satisfaction is also caused by other factors such as financial reward and control over work tasks and schedules
Commitment to Work
49
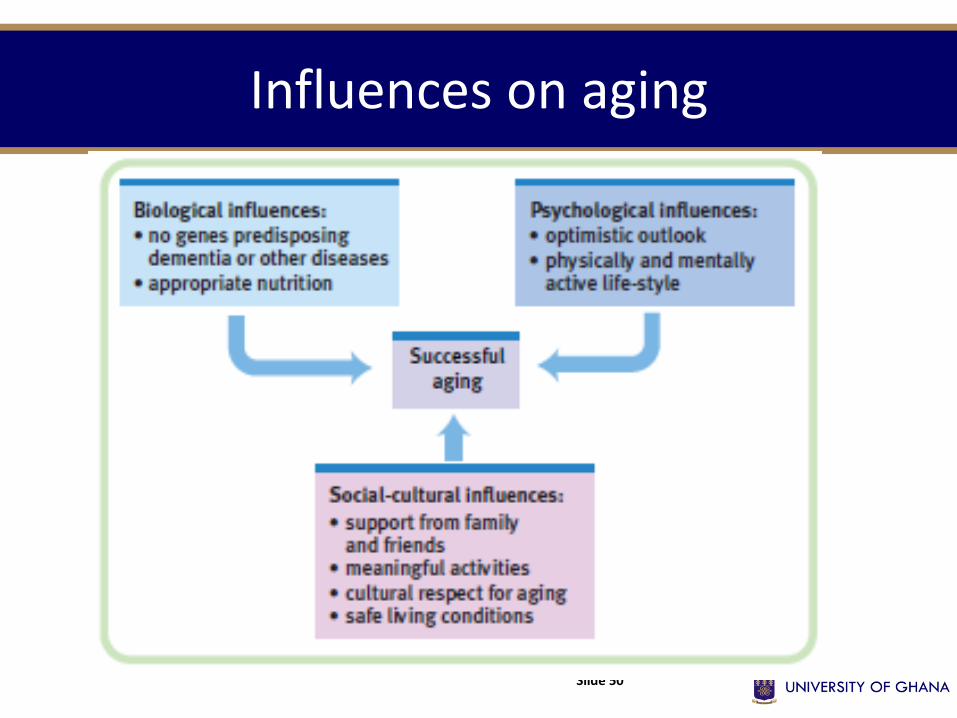
Influences on aging
Slide 50
Coping with death and dying
• Death is inevitable and how individuals respond to death may vary.
•Grief is more intense when death occurs unexpectedly (especially if also too early on the social clock).
•There is NO standard pattern or length of the grieving process.
•It seems to help to have the support of friends or groups, and to face the reality of death and grief while affirming the value of life.
Slide 51
Sample Question
• What major physical changes occur during adolescence?
• How did Piaget and Kohlberg describe cognitive and moral development during adolescence?