Perceptual Bias for Affective and Nonaffective Information in AsymmetricParkinson’s Disease
Jared G. Smith and John P. HarrisUniversity of Reading
Saleem KhanRoyal Berkshire Hospital, Reading
Elizabeth A. Atkinson and M. Susan FowlerUniversity of Reading
Ralph P. GregoryRoyal Berkshire Hospital, Reading
Objective: To relate lateralized impairments of visual perception in Parkinson’s disease to asymmetriesin the severity of motor symptoms. Method: Ten patients with worse left-sided motor symptoms(LPD), 15 with worse right-sided (RPD), and 13 healthy age-matched controls (all right-handed) viewedmirror-imaged pairs of emotional chimeric faces, (left side smiling, right neutral, and vice versa), of greyscales (strips whose luminance varied smoothly from black on the left to white on the right, and viceversa) and of gender chimeric faces (left side male, right female, and vice versa). Participants signaledwhich stimulus appeared happier, brighter, or more feminine, respectively, so showing which sidereceived more attention. Results: For emotional chimeras, controls and LPD showed little bias, whereasRPD showed a strong bias to left hemispace ( p .018, r .45). Across all patients, this bias was
associated with severity of right-sided motor impairment ( p .018, r .49). The bias was much weakerand insignicant for greyscales ( p .72, r .14). For gender chimeras, RPD again showed asignicantly greater left hemispace bias than did LPD ( p .037, r .47), although neither patient groupdiffered signicantly from controls. Across all patients, this bias correlated with ratio of right-to-leftsymptom severity ( p .044, r .48). Conclusions: The left hemispace bias in RPD is greater for facialthan for luminance judgments, and is amplied for emotional judgments. Asymmetrical degeneration of the striatum, particularly involving the left side, appears to underlie this decit in visual processing.
Accumulating evidence indicates that Parkinson’s disease (PD)causes difculties in processing emotional facial expressions (for areview, see Assogna, Pontieri, Caltagirone, & Spalletta, 2008).Most studies suggest that disgust is less frequently recognized inPD, although other facial emotions, including anger, fear, surprise,and sadness, are also affected (Clark, Neargarder, & Cronin-Golomb, 2008; Dujardin et al., 2004; Kan, Kawamura, Hasegawa,Mochizuki, & Nakamura, 2002; Lawrence, Goerendt, & Brooks,2007; Sprengelmeyer et al., 2003; Yip, Lee, Ho, Tsang, & Li,2003). Abnormalities in facial emotion recognition in PD areassumed to arise from losses of dopaminergic neurons resulting indysfunction of fronto-subcortical systems and subsequent alter-
ation in areas strategic for the identication of specic facialexpressions, such as insula, amygdala, ventral striatum, inferiororbitofrontal cortex, and anterior cingulate cortex (Assogna et al.,2008; Dujardin et al., 2004; Lawrence et al., 2007; Sprengelmeyeret al., 2003).
In recent years, interest has grown on the clinical correlates of impaired processing of emotional facial expressions. One aspect of the illness that has received attention concerns the relationshipbetween emotion recognition and side of worse motor symptoms.In PD, the motor symptoms typically occur in an asymmetricfashion (Hoehn & Yahr, 1967), reecting asymmetric depletion of dopamine in the substantia nigra, a pattern that appears to persistacross the range of disease severity (Kaasinen et al., 2001). Thesechanges result in asymmetrical dysregulation of the striatum, andso asymmetrical dysfunction of multiple circuits involving thebasal ganglia and cortical regions (Marie et al., 1995; Middleton &Strick, 2000). The asymmetric nature of the disease makes PD a
useful model in which to study the effects of subcortical degener-ation on visuo-cognitive and emotional functions associated witheach hemisphere. Of note, studies of emotional recognition inpatients with asymmetric PD have revealed differential effects of body side of disease onset. For example, Yip et al. (2003) foundworse recognition of all facial emotions, in particular fear andsadness, in a large group of patients with bilateral motor symp-toms, but noted that eight Parkinson’s patients affected only on theright side were particularly impaired in the recognition of sadnessand disgust. More recently, Clark et al. (2008) reported that pa-tients with left symptom onset were less accurate than controls atidentifying angry facial expressions, while patients with right
Jared G. Smith, John P. Harris, Elizabeth A. Atkinson, and M. SusanFowler, School of Psychology and Clinical Language Sciences, Universityof Reading, Reading, United Kingdom; Saleem Khan and Ralph P. Greg-ory, Royal Berkshire Hospital, Reading, United Kingdom.
The work reported in this article was supported by grants from theEngineering and Physical Sciences Research Council (EPSRC) and fromthe Parkinson’s Disease Society of the United Kingdom. We thank Dr.Linda Rueckert for providing electronic versions of the original stimuli forboth the emotional and gender chimeric faces tests. We also thank theParkinson’s Disease Society, Dr. Jeremy Stern, and Dr. Espley for theirassistance in recruiting participants for this study and the reviewers forhelpful comments.
Correspondence concerning this article should be addressed to John P.Harris, School of Psychology and Clinical Language Sciences, Universityof Reading, Whiteknights, Reading RG6 6AL, United Kingdom. E-mail: [email protected]
spatial information (Kim, Levine, & Kertesz, 1990; Rueckert &Naybar, 2008; Rueckert & Pawlak, 2000). Functional brain imag-ing has shown that, in control participants, regions affected by PD,such as the basal ganglia and frontal cortex, are preferentiallyresponsive during facial affect recognition (Kan et al., 2002;Sprengelmeyer et al., 2003). Thus, comparing LPD and RPDpatients’ responses with chimeras could provide insight into howasymmetric dopaminergic transmission in PD affects cerebral lat-eralization of affective facial and nonfacial information. If a par-ticular subgroup has greater difculties in identifying facialexpressions, they are likely to have more difculties in socialinteraction, and so need more targeted information and advicefrom clinicians.
In the present study, we examined whether PD patients would
demonstrate atypical perceptual biases for emotion-based facialand nonfacial chimeras related to the side of worse motor impair-ment. Studies of both facial expression recognition and (lateral-ized) visuospatial function have shown differences in PD related toside of motor symptom onset (Clarke et al., 2008; Davidsdottir etal., 2008; Ebersbach et al., 1996). Based on these ndings, it washypothesized that relative to RPD patients, LPD patients wouldevidence a decreased left spatial bias across tasks, although thiseffect would be heightened in the test of emotional chimeric faces,given the specic disturbance of recognition of facial emotionexpressions in PD patients (Assogna et al., 2009; Clark et al.,2008). In addition to group comparisons of LPD and RPD patients,we investigated whether severity of left- or right-sided symptoms(irrespective of which were worse) was related to perceptualasymmetries. Finally, because impairments in decision-makingand categorization may occur in PD (Filoteo, Maddox, Ing, &Song, 2007), and discrimination or identication of facial expres-sions may be related to cognitive impairment (Dujardin et al.,2004; Yip et al., 2003), a battery of neuropsychological tests wasalso run, to measure any decits in memory and executive func-tions, and so allow assessment of the potential inuence of im-paired cognition.
Method
Participants. Twenty-ve patients with idiopathic PD and 13age-matched healthy controls participated in the experiment. All
were screened for dementia using the Mini-Mental State Exami-nation (MMSE cut-off 24, Folstein, Folstein, & McHugh, 1975)and for depression using the Beck Depression Inventory-II (BDI-IIcut-off 17, Beck, Steer, & Brown, 1996). All were right-handedas assessed by the Edinburgh Handedness Inventory (Oldeld,1971). None had a history of head injury within the preceding 10years, or of alcohol abuse, stroke, or epilepsy, and all had normalor corrected-to-normal vision. The diagnosis of idiopathic PD wasconrmed by a consultant neurologist and all patients met U.K.Parkinson’s disease Brain Bank Criteria for diagnosis of PD (Gibb& Lees, 1988). Ethical approval was given by the Berkshire LocalResearch Ethics Committee, and by the University of Reading
Research Ethics Committee. All participants gave their informedconsent after a verbal and a written description of what theirparticipation would involve.
Clinical assessment. The Unied Parkinson’s disease RatingScale Motor subscale (UPDRSm; Fahn, Elton, & Members of theUPDRS Development Committee, 1987) was used as a measure of current motor severity in patients with PD and to classify patientsinto left- and right-sided PD groups. Patients were evaluated by aconsultant neurologist blind to experimental results 45 to 75 minafter administering their usual PD medication (when the patientwas in an “ON” state), and so in the same state as when theexperimental tasks were performed. One patient was unavailablefor motor function examination, and so was classied as LPD fromthe side of rst symptom onset. For the assessment, right- andleft-sided motor composite scores were created by summing theindividual UPDRS motor subscale items of tremor (items 20 and21), rigidity (item 22) and bradykinesia (items, 23, 24, 25, and 26).Degree of asymmetry of motor dysfunction for each participantwas determined by calculating a motor asymmetry score using theleft and right motor composite scores obtained from patients:
(UPDRSm Right – UPDRSm Left)/(UPDRSm Right UPDRSmLeft). This formula gives a result of zero when left and right motorscores are equal, a negative number when left symptoms areworse, and a positive number when right symptoms are worse.Based on these scores, patients were divided into two groups, thosewith motor symptoms predominantly on the left (LPD, n 10),and those with symptoms predominantly on the right (RPD, n15). LPD asymmetry scores ranged from 0.07 to 0.40 and RPDscores from 0.06 to 1.00.
The demographic and clinical characteristics of the subgroupsare shown in Table 1. There was a high number of men in the RPDgroup (12/15) compared with both the LPD (5/10) and controlgroups (6/13), which tended to have an equal balance of men andwomen. Nevertheless, Fisher’s exact tests revealed nonsignicantdifferences between the PD subgroups ( p .189) and betweenRPD and controls ( p .114). The subgroups were, generallyspeaking, well matched on age and education, and two-tailed t tests(comparing each pair of experimental groups) revealed no signif-icant differences between groups on these variables, although therewas a trend for RPD patients to be more educated than their LPDcounterparts ( p .083). Although BDI-II scores were elevated ineach of the patient subgroups relative to controls, the scores of thePD subgroups were comparable with each other and within thenormal range.
The PD subgroups were also matched on variables related totheir illness, including disease severity and medication regimes. Asassessed by the Hoehn and Yahr (1967) degree of clinical disabil-
ity scale, 2 (LPD) patients were in Stage I, 15 patients (5 LPD, 10RPD) were in Stage II, 7 patients (3 LPD, 4 RPD) were in StageIII, and 1 (RPD) patient was in Stage IV. There were no signicantdifferences between the subgroups with respect to mean stage of illness, disease duration and total UPDRSm. Unsurprisingly, left-sided UPDRSm scores were higher in LPD patients than RPDpatients, while motor symptoms on the right-side of the body weremore severe in RPD than LPD patients. Motor asymmetry scoreswere also signicantly different between the RPD and LPDgroups, reecting RPD participants’ scores that were positive andLPD participants’ scores that were negative. Although the RPDgroup evidenced a numerically larger degree of asymmetry than
445PERCEPTUAL BIAS IN ASYMMETRIC PARKINSON’S DISEASE
the LPD group, a comparison of the absolute values of groupmotor asymmetry scores revealed that this difference was notstatistically signicant, F (1, 23) 2.24, p .149. At the time of testing all 25 patients with PD were receiving anti-parkinsonianmedication and were in an “ON” phase. Specically, three of the(RPD) patients were receiving levodopa (Stalevo, Sinemet and/orMadopar) exclusively, while 7 patients (3 LPD, 4 RPD) weretaking dopamine agonists (Mirapexin, Ropinerole, or Pergolide)exclusively. Eleven of the patients (5 LPD, 6 RPD) were takingboth levodopa and agonist medication, of which 3 (LPD patients)were also receiving Amantadine. In addition to dopamine ago-nists, 1 RPD patient was also taking a MAO-B inhibitor (Rasagi-line) while 1 LPD patient was also receiving anticholinergic med-
ication (Trihexphenidyl). Finally, 1 LPD patient who was receiv-ing levodopa was also taking a MAO-B inhibitor (Selegeline) andAmantadine and 1 RPD patient undergoing levodopa treatmentwas also being administered both a MAO-B inhibitor (Selegeline)and a COMT inhibitor (Entacapone). Fisher’s exact tests indicatedthat the PD subgroups were not signicantly different in theproportion of participants treated with levodopa medication (LPD:6/10, RPD: 10/15, p .999) or dopamine agonists (LPD: 9/10,RPD: 11/15, p .615). One LPD patient was also receiving SSRIantidepressant medication (Fluoxetine).
Aspects of basic visual function were assessed as follows in allbut two of the patients (9/10 LPD; 14/15 RPD). Visual acuity was
measured in each eye with the Times Roman Reading Charts of theMaclureTest (Clement Clarke International Ltd.), on which theability to read a type size of N6 at the normal reading distancecorresponds approximately to a Snellen Acuity of 6/6. Takingacuity in the worst eye when the eyes were not equal, the meanacuity of the LPD group was N5.67 (range N5–N8), while allpatients in RPD group read at N5. Two tests of stereopsis were alsorun. On the Randot test of stereopsis, the scores were: LPD M 119.88s ( SD 194.85, range 20–600); RPD M 84.64s(SD 60.08, range 20–200). On the TNO test of stereopsis, thescores were: LPD M 506.67s ( SD 837.78, range 30–1980);RPD M 299.21s (SD 258.31, range 60–1860). In a groupof healthy elderly individuals, mean scores on the Randot test of
45s and on the TNO test of 275s were found (Fowler, 1996). In agroup of normal participants, whose ages ranged from 4 to 74years, a mean Randot score of 44s and a mean TNO score of 194swere found (Mazow, Prager, & Cathey, 1983). Thus, although theywere somewhat impaired on the Randot test, both patient groupsclearly retained some stereoscopic vision. On clinical examination,all patients except one RPD patient (bilateral restriction of eleva-tion) showed the full range of ocular movements. One patient inthe LPD group and two in the RPD group showed a small hy-pometria of saccades (left right). Pursuit eye-movements weresometimes jerky in four patients in the LPD group and 10 patientsin the RPD group. All patients could converge on a near point
Table 1 Demographic, Clinical, and Neuropsychological Performance Data for Predominantly Left-Sided Parkinson’s Patients (LPD),Predominantly Right-Sided Parkinson’s Patients (RPD), and Control Participants
Note . UPDRSm “ON” Score on motor subscale of Unied Parkinson’s Disease Rating Scale post administration of medication; Motor asymmetryscore (UPDRSm Right UPDRSm Left)/(UPDRSm Right UPDRSm Left); MMSE Mini Mental Status Examination; BDI-II Beck DepressionInventory II; NART National Adult Reading Test (expressed as a Wechsler Adult Intelligence Scale–Revised Full Scale equivalent); COWATControlled Oral Word Association Test; ANT Animal Naming Test; CERAD wordlist memory test from the Consortium to Establish a Registry forAlzheimer’s Disease battery; TMT Trail Making Test.a One patient with LPD did not partake in UPDRS motor assessments. p .05. p .01. p .001. Signicant t values are shown in boldface.
of 20 cm or less except for one LPD patient (30 cm) and 2 RPDpatients (30 cm, 40 cm). Thus, we conclude that the patients werenot suffering from gross disorders of acuity or binocularitywhich would interfere with their perception of chimeric faces orgreyscales.
Neuropsychological assessment. All participants were ad-ministered a small battery of neuropsychological tests, whichincluded the National Adult Reading Test (NART; Nelson &Willeson, 1991) as well as measures of verbal uency, specically,the Controlled Oral Word Association Test (COWAT; Benton &Hamsher, 1976) and the Animal Naming subtest from the BostonDiagnostic Aphasia Examination (ANT; Goodglass & Kaplan,1972). Participants also performed the Stroop task and the TrailMaking Test, while verbal memory was assessed using thewordlist memory test from the CERAD battery (Consortium toEstablish a Registry for Alzheimer’s disease; Rosen, Mohs, &Davis, 1984). A summary of the neuropsychological test results isdisplayed in Table 1. Differences across all experimental groupswere generally small and mostly nonsignicant with the notableexception of CERAD, on which controls outperformed both pa-
tient subgroups, although signicantly so only compared to RPDparticipants. Similarly, t tests comparing the PD subgroups againsteach other showed comparable performance on the MMSE, mea-sures of verbal uency and CERAD recall ( p .10). However,NART performance was marginally better in RPD patients than inLPD patients ( p .082). Although the cost of incongruent color-word condition on the Stroop and task switching on the TrailMaking Test was numerically greater for LPD than RPD patients,suggesting mildly impaired executive abilities in the LPD group,differences were not signicant on either task.
Materials and procedure. Experimental stimuli were theemotional chimeric faces test and the greyscales task, presented ina counterbalanced order within each subject group. Both experi-mental conditions were run on an IBM compatible PC with stimulipresented on a 410 350 mm monitor at XVGA (1600 1200pixel) resolution. Throughout the testing period, participants wereencouraged to align their midlines with the center of the displayand to remain as still as possible. Experimental stimuli wereviewed from a distance of approximately 57 cm. In each task,participants were requested to examine stimuli carefully, and werepermitted to respond without time constraints.
Emotional Chimeric Faces Test. Participants were adminis-tered a computerized version of the Levy et al. (1983) emotionalchimeric faces task in which the 36 stimuli had been scanned andsaved as gif les (for a Web version of this computerized version,see Rueckert, 2005). Each of the stimuli was dened by a thinblack rectangle against a white background and subtended a retinal
angle of about 12.7 degrees (deg) high 9.7 deg wide. Thehorizontal and vertical midlines of the stimulus pairs were alignedwith the center of the display window. Details on construction of the chimeric face stimuli have been provided elsewhere (Levy etal., 1983). Briey, this involved photographing twice each of nineposers, once with a smiling and once with a neutral expression and joining the vertical halves of each together to form a chimeric face(i.e., a left-side smiling face was paired with a right-side neutralface or a right-side smiling face was paired with a left-side neutralface). Each chimera was then paired with its mirror image. Anexample of a pair of chimeras is provided in Figure 1. The verticalposition of each member of a pair was counterbalanced, resulting
in a matched set of four pairs of chimeric stimuli from each poser,yielding a total of 36 stimulus pairs. The counterbalancing of stimuli ensured that any consistent response bias (e.g., alwayschoosing the top face) would result in a mean bias of zero. The 36trials were arranged in a pseudorandom order whereby trials weredivided into four randomly ordered blocks of nine trials. Eachblock consisted of one stimulus pair from each poser (four/ve of these pairs presented the top stimulus with the smiling face on theleft side and the bottom stimulus with the smiling face on the rightand ve/four trials vice versa). Subjects were asked to indicatewhich of the two faces looked happier overall by pressing one of
Figure 1. Example of a chimeric face in the emotional chimeric facestest. The participants’ task is to decide which of the two faces looks,overall, happier. Here the top face is expressing positive emotion in the leftvisual eld and the bottom face is expressing positive emotion in the rightvisual eld. From “Asymmetry of perception in free viewing of chimericfaces,” by J. Levy, W. Heller, M. T. Banich, & L. A. Burton, 1983, Brainand Cognition, 2, p. 406. Reproduced with permission.
447PERCEPTUAL BIAS IN ASYMMETRIC PARKINSON’S DISEASE
two spatially compatible, brightly colored response buttons labeled“upper” and ‘lower.’ The response panel was placed in such a waythat the push-buttons were spatially compatible with the stimuli(i.e., the “upper” button above the “lower” button) and was alignedcentrally with respect to the monitor. To eliminate the potentialeffects of lateralized motor response bias in PD patients (arisingfrom, e.g., hemispatial akinesia), participants indicated their deci-sions in both tasks by using both index ngers to press theappropriate response button. Participants were watched carefullyby an experimenter to ensure responses were made in this manner.In between each response, participants rested their index ngers ona white strip placed horizontally on the response panel between thetwo buttons. After a response, the display was cleared and a newtrial began after an interstimulus period of 1500ms. No feedback was provided. Three practice trials were administered prior toperformance of the chimeric faces test.
Greyscales task. Participants performed the computerizedgreyscales task of Nicholls et al. (1999) and made available by theauthors at http://www.psych.unimelb.edu.au/research/laterality/ greyscales.html. In each of 72 trials, participants made a forced
two-choice discrimination of the relative brightness of two verti-cally aligned gradients presented simultaneously. Each of thestimuli was dened by a thin black rectangle against a graybackground and was 3 deg high. To discourage the use of astandard response, the length of the gradients was varied be-tween 12.2, 15.3, 18.3, 21.4, 24.4, and 27.5 deg (12 trials for eachstimulus length). The horizontal and vertical midlines of the stim-ulus pairs were aligned with the center of the display window. Thegradients changed incrementally from white on one side to black on the other and were arranged so that they were left/right rever-sals of each other (for a detailed description of how changes ingradient brightness were achieved, see Nicholls et al., 1999). Thus,if the upper stimulus was darker on the right, the lower stimuluswas darker on the left (see Figure 2 for an example). Participantswere asked to indicate which of the two gradients comprising eachstimulus appeared darker overall in the same manner as in theemotional chimeric faces test. The greyscales program presentedthe different factorial combinations of length and stimulus orien-tation in a pseudorandom order. As before, the interstimulus in-
terval was 1,500ms and no feedback was provided. Six practicetrials were given before the greyscales task.
Results
Measures of perceptual bias. Responses were categorizedaccording to whether they selected the stimulus with the salientfeature on the left or right side irrespective of whether it was theupper or lower stimulus. For the emotional chimeric faces task, aresponse was dened as left-biased if the participant selected thechimera with the left-side smiling face and right-biased if theyselected the right-side smiling face. Similarly, for the greyscalestask, responses to each stimulus were categorized as left-biased orright-biased according to whether the participant had chosen therectangle with the darker end on the left or right. An asymmetryscore for each test was derived by subtracting the number of leftchoices from the number of right choices, and dividing the resultby the total number of items (36 in emotional chimeric faces, 72 ingreyscales; see Mattingley et al., 1994).
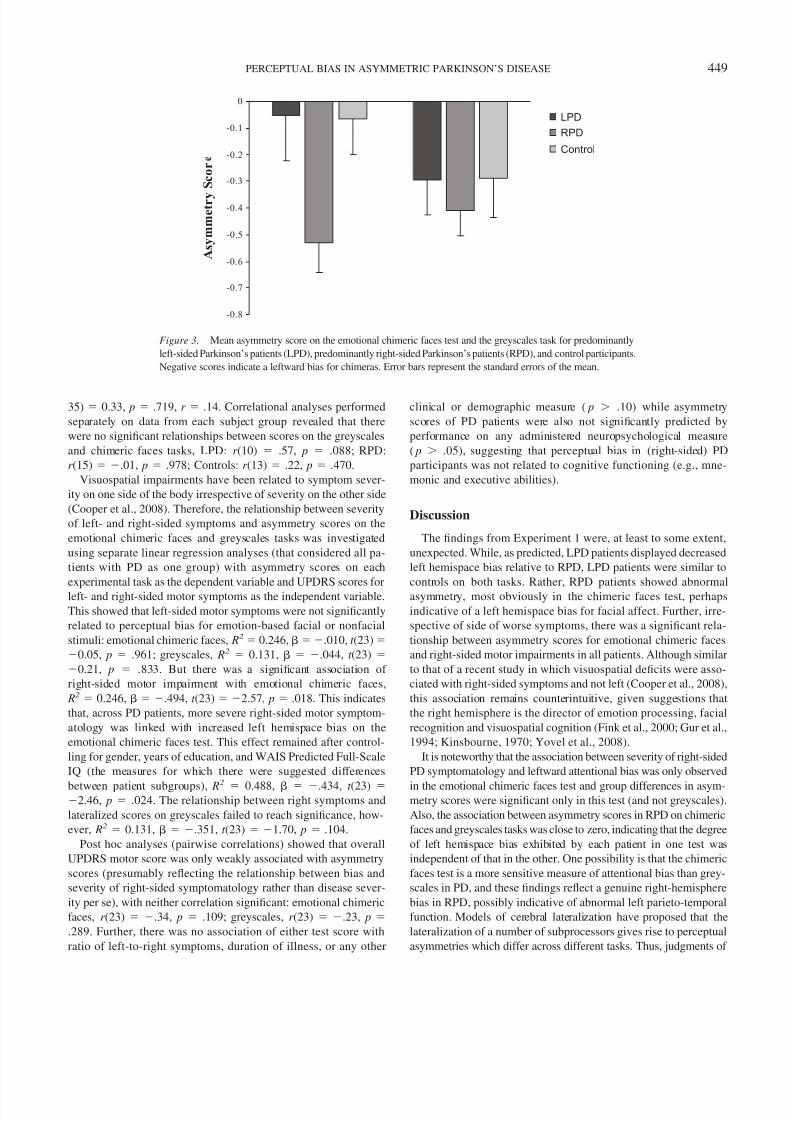
The mean asymmetry scores of each group for emotional chi-
meric faces and greyscales are shown in Figure 3. Although thethree groups showed negative asymmetry scores, suggesting a lefthemispace bias for both tasks, the negative asymmetry scores of RPD patients were larger than those of either the LPD or controlgroups, most obviously on the emotional chimeric faces test. Theseobservations tended to be conrmed in statistical analyses.Whereas the emotional chimeric faces asymmetry scores of bothLPD patients ( M 0.06, SD 0.53) and control subjects ( M
0.07, SD 0.48) were not signicantly different from zero ( p.5), RPD patients exhibited a highly signicant left hemispace biasfor chimeras, ( M 0.53, SD 0.43, t (14) 4.84, p .001,r .79). A one-way analysis of variance (ANOVA) of asymmetryscores for the three groups conrmed a signicant effect of groupon the emotional chimeric faces test, F (2, 35) 4.49, p .018, MSE 0.22, r .45, reecting the greater left hemispace bias inRPD patients compared with the other experimental groups. Thiseffect remained when demographic (gender, years of education)and clinical (BDI-II scores) variables and neuropsychological per-formance (Wechsler Adult Intelligence Scale [WAIS] Full IQ;Consortium to Establish a Registry for Alzheimer’s Disease[CERAD] total and delayed recall), measures for which there weredifferences (or suggested differences) across experimental groups,were factored in as covariates, F (2, 29) 3.52, p .043, MSE 0.23, r .41. Post hoc tests (two-tailed t tests) indicatedthat RPD patients had a greater left hemispace bias when com-pared with either LPD patients ( p .021, r .46) or controls( p .011, r .47), but there was no signicant difference
between LPD patients and controls.In the greyscales task, RPD patients once again showed a strong
left hemispace bias, M 0.41, SD 0.36, t (14) 4.32, p.001, r .76, indicating that they predominantly selected as darkerthe rectangle in which the black end appeared on the left. Incontrast, control subjects showed only a marginally signicant lefthemispace bias, M 0.29, SD 0.53, t (12) 1.95, p .075,r .49, while LPD patients mean asymmetry score just missedsignicance, M 0.29, SD 0.42, t (9) 2.23, p .052, r .60. However, although the RPD group showed a numericallylarger left hemispace bias than did LPD and control participants,there was no signicant effect of group for this task, F (2,
Figure 2. Example of a stimulus from the greyscales task. Participantswere required to indicate which of the two rectangles appeared overall thedarker. The axis of the required response (top/bottom) is orthogonal to theaxis of any attentional bias (left/right), thus avoiding the possible effects of motor response bias. From “Freeviewing perceptual asymmetries for the judgement of brightness, numerosity and size,” by M. E. R. Nicholls, J. L.Bradshaw, & J. B. Mattingley, 1999, Neuropsychologia, 37, p. 308. Re-produced with permission.
35) 0.33, p .719, r .14. Correlational analyses performedseparately on data from each subject group revealed that therewere no signicant relationships between scores on the greyscalesand chimeric faces tasks, LPD: r (10) .57, p .088; RPD:r (15) .01, p .978; Controls: r (13) .22, p .470.
Visuospatial impairments have been related to symptom sever-ity on one side of the body irrespective of severity on the other side(Cooper et al., 2008). Therefore, the relationship between severityof left- and right-sided symptoms and asymmetry scores on theemotional chimeric faces and greyscales tasks was investigatedusing separate linear regression analyses (that considered all pa-tients with PD as one group) with asymmetry scores on eachexperimental task as the dependent variable and UPDRS scores forleft- and right-sided motor symptoms as the independent variable.This showed that left-sided motor symptoms were not signicantlyrelated to perceptual bias for emotion-based facial or nonfacialstimuli: emotional chimeric faces, R2 0.246, .010, t (23)
0.05, p .961; greyscales, R2 0.131, .044, t (23)0.21, p .833. But there was a signicant association of
right-sided motor impairment with emotional chimeric faces, R2 0.246, .494, t (23) 2.57, p .018. This indicatesthat, across PD patients, more severe right-sided motor symptom-atology was linked with increased left hemispace bias on theemotional chimeric faces test. This effect remained after control-ling for gender, years of education, and WAIS Predicted Full-ScaleIQ (the measures for which there were suggested differences
between patient subgroups), R2
0.488, .434, t (23)2.46, p .024. The relationship between right symptoms and
lateralized scores on greyscales failed to reach signicance, how-ever, R2 0.131, .351, t (23) 1.70, p .104.
Post hoc analyses (pairwise correlations) showed that overallUPDRS motor score was only weakly associated with asymmetryscores (presumably reecting the relationship between bias andseverity of right-sided symptomatology rather than disease sever-ity per se), with neither correlation signicant: emotional chimericfaces, r (23) .34, p .109; greyscales, r (23) .23, p.289. Further, there was no association of either test score withratio of left-to-right symptoms, duration of illness, or any other
clinical or demographic measure ( p .10) while asymmetryscores of PD patients were also not signicantly predicted byperformance on any administered neuropsychological measure( p .05), suggesting that perceptual bias in (right-sided) PDparticipants was not related to cognitive functioning (e.g., mne-monic and executive abilities).
Discussion
The ndings from Experiment 1 were, at least to some extent,unexpected. While, as predicted, LPD patients displayed decreasedleft hemispace bias relative to RPD, LPD patients were similar tocontrols on both tasks. Rather, RPD patients showed abnormalasymmetry, most obviously in the chimeric faces test, perhapsindicative of a left hemispace bias for facial affect. Further, irre-spective of side of worse symptoms, there was a signicant rela-tionship between asymmetry scores for emotional chimeric facesand right-sided motor impairments in all patients. Although similarto that of a recent study in which visuospatial decits were asso-ciated with right-sided symptoms and not left (Cooper et al., 2008),this association remains counterintuitive, given suggestions thatthe right hemisphere is the director of emotion processing, facialrecognition and visuospatial cognition (Fink et al., 2000; Gur et al.,1994; Kinsbourne, 1970; Yovel et al., 2008).
It is noteworthy that the association between severity of right-sidedPD symptomatology and leftward attentional bias was only observed
in the emotional chimeric faces test and group differences in asym-metry scores were signicant only in this test (and not greyscales).Also, the association between asymmetry scores in RPD on chimericfaces and greyscales tasks was close to zero, indicating that the degreeof left hemispace bias exhibited by each patient in one test wasindependent of that in the other. One possibility is that the chimericfaces test is a more sensitive measure of attentional bias than grey-scales in PD, and these ndings reect a genuine right-hemispherebias in RPD, possibly indicative of abnormal left parieto-temporalfunction. Models of cerebral lateralization have proposed that thelateralization of a number of subprocessors gives rise to perceptualasymmetries which differ across different tasks. Thus, judgments of
-0.8
-0.7
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
A s y m m e t r y
S c o r
LPD
RPD
Control
Figure 3. Mean asymmetry score on the emotional chimeric faces test and the greyscales task for predominantlyleft-sided Parkinson’s patients (LPD), predominantly right-sided Parkinson’s patients (RPD), and control participants.Negative scores indicate a leftward bias for chimeras. Error bars represent the standard errors of the mean.
449PERCEPTUAL BIAS IN ASYMMETRIC PARKINSON’S DISEASE
emotional content of faces and of brightness would each engage aunique set of subprocessors, leading to differences in patterns of attentional bias and thus the observed perceptual asymmetries (Ni-cholls et al., 1999). In support of this approach, Mattingley andcolleagues (1994) reported that despite a signicant right hemispacebias on both chimeric faces and greyscales in patients with righthemisphere damage after stroke, and a signicant left hemispace biason both tasks in controls, the sizes of directional biases within eachgroup were not related. Thus we may not need to look beyond decitsin attention or visuospatial cognition to explain the small intratask correlations in Experiment 1.
Choosing the chimeric face that looks happier almost certainlyinvolves emotional processes not active in greyscales, and so theexaggerated left hemispace bias in RPD may reect a decit incomprehending emotional facial cues. There is increasing evidencethat it is the left rather than the right hemisphere that mediatespositiveemotions (Fusar-Poli et al., 2009; Gur et al., 1994; Root, Wong, &Kinsbourne, 2006), and recent work has suggested that, after control-ling for depression, RPD patients are more likely than LPD patients toview expressions with an ambiguous valence (e.g., surprise) in a more
negative light (Clark et al., 2008). While the happy chimeras in theLevy et al. (1983) task used here were not intended to be ambiguous,signicant disruption to left hemisphere function in RPD may haveresulted inperception ofemotionsdifferent fromthat in LPD and controlswhich, in turn, could have affected judgments of facial chimeras.
To address this possibility, and to better characterize the later-alized performance of LPD and RPD patients on chimeric stimuli,a second experiment was conducted using a chimeric faces test inwhich the faces have a neutral expression and the task does notinvolve judgment of emotional content. This was the gender chi-meric faces test, a brief test developed in the early 1990s by theLevy group (Luh et al., 1991). This seemed an appropriate measuresince PD does not appear to disrupt the facial perception of gender(Sprengelmeyer et al., 2003).
Experiment 2: Gender Chimeric Faces
Introduction
To check the possible role of emotion in Experiment 1, a chimericfaces test was run which required decisions about the perceivedgender of faces rather than their emotional content. If asymmetricillness disrupts visuospatial processing of facial stimuli, then RPDpatients should exhibit a greater preference for the face on the left.However, if the abnormal perceptual bias in (R)PD patients does notentail processing of affective information, then performance in RPDshould be comparable with that of LPD and control participants.
Materials and Methods
Participants. The same participants took part as in the previ-ous experiment, less 4 RPD patients, 1 LPD patient, and 1 controlparticipant, who were not available. This left 11 RPD patients (1woman, 10 men); 9 LPD patients (4 women, 5 men) and 12 controlparticipants (6 women, 6 men).
Materials and procedure. The experimental apparatus wasidentical to the previous experiment with one exception; the gen-der chimeric faces task was performed using a different IBMcompatible PC. In this instance, stimuli were presented on a
smaller monitor (340 270 mm) although still at XVGA (16001200 pixel) resolution. As before, participants’ responses wererecorded using the same vertically aligned, brightly colored, two-button response panel interfaced with the PC.
Participants were administered a computerized gender chimericfaces task used by Luh et al. (1991) in which the same 12 stimuli hadbeen scanned and saved as gif les. As previously, each of the stimuliwas dened by a thin black rectangle against a white background andwas 12.7 deg high 9.7 deg wide. The horizontal and verticalmidlines of the stimulus pairs were aligned with the center of thedisplay window. Details of the construction of the gender chimericface stimuli have been provided elsewhere (Luh et al., 1991). Briey,this involved photographing four times each of six posers, three malesand three females, and joining thevertical halves of onemale with onefemale to form a chimeric face (i.e., a left-side male face was pairedwith a right-side female face or a right-side male face was paired witha left-side female face). Each chimera was then paired with its mirrorimage (see Figure 4 for an example). The vertical position of each
Figure 4. Example of a chimeric face in the gender chimeric faces test.The participants’ task is to decide which of the two faces looks, overall,more feminine. Here the top face is female in the left visual eld and thebottom face is female in the right visual eld. From “Perceptual asymme-tries for free viewing of several types of chimeric stimuli,” by K. E. Luh,L. M. Rueckert, & J. Levy, 1991, Brain and Cognition, 16, p. 88. Repro-duced with permission.
member of a pair was counterbalanced, resulting in a matched set of four pairs of chimeric stimuli from each male/female pair of posers,yielding a total of 12 stimulus pairs.
Subjects were asked to indicate which of the two faces lookedmore feminine overall. The 12 trials were arranged in a randomorder determined at run time. As in Experiment 1, participantsindicated their decisions by using both index ngers to press theresponse button that spatially corresponded with the selected stim-ulus. After a response, the display was cleared and a new trialbegan after an interstimulus period of 1,500 ms. Again, partici-pants were requested to examine the stimuli carefully, and werepermitted to respond without time constraints. No feedback wasprovided. Three practice trials were administered prior to thegender chimeric faces test.
Results and Discussion
Responses were categorized according to whether the stimuluswith the salient feature on the left or right side was selected,irrespective of whether it was the upper or lower. The asymmetry
score for the gender chimeric faces test was calculated by sub-tracting the number of trials on which the gender decision wasmade on the basis of information available on the left side of theface from the number of trials where the gender decision was madeon the basis of information available on the right side of the face,and dividing the result by the total number of items (12).
The asymmetry scores for each of the experimental groups areshown in Figure 5. One-sample t tests again demonstrated thatwhereas RPD patients demonstrated a signicant left hemispacebias for gender chimeras, M 0.41, SD 0.50, t (10) 2.73, p .021, r .65, both the LPD group, M 0.04, SD 0.36,t (8) 0.31, p .766, and the control participants, M 0.22,
SD 0.47, t (11) 1.65, p .128, did not. Although a one-wayANOVA showed no signicant main effect of group on asymme-try scores in the gender chimeric faces test, F (2, 29) 2.42, p.107, r .38, a pairwise comparison between the patient sub-groups revealed a signicant difference between asymmetryscores, t (18) 2.25, p .037, r .47, suggesting that subgroups
of PD patients, characterized by the side of worse motor symp-toms, can be differentiated by the degree of lateralized attentionalbias exhibited in a perceptual test which does not involve emotion.There were no signicant differences between asymmetry scoresof the control group and each patient subgroup ( p .05).
Of note, correlational analyses performed separately on datafrom each subject group revealed that there were no signicantrelationships between scores on the gender chimeric faces task andthose obtained in the emotional chimeric faces test administered inExperiment 1, (LPD: r (9) .42, p .266; RPD: r (11) .23, p .506; Controls: r (12) .25, p .434), indicating that theasymmetries exhibited for the two versions of the chimeric facestest were independent of each other. There was a highly signicant
association between asymmetry scores on the gender chimericfaces and greyscales in the LPD group, r (9) .82, p .007,suggesting some overlap in the underlying processes for makinglaterality judgments involved in tasks without an emotional com-ponent. However, this relationship was not present in either theRPD group, r (11) .29, p .396, or controls r (12) .19, p.560.
In Experiment 1, right-sided symptoms signicantly predictedperformance on both chimeric faces and greyscales tasks (in con-trast to left-sided symptoms). However, on the gender chimericfaces test, regression analyses including all PD patients in onegroup (with asymmetry score as the dependent variable and right-
-0.7
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
Gender Chimeric Task
A s y m m e t r y
S c o r
LPD
RPD
Control
Figure 5. Mean asymmetry score on the gender chimeric faces tests for predominantly left-sided Parkinson’spatients (LPD), predominantly right-sided Parkinson’s patients (RPD), and control participants. Negative scoresindicate a leftward bias for chimeras. Error bars represent the SEM .
451PERCEPTUAL BIAS IN ASYMMETRIC PARKINSON’S DISEASE
and left-sided motor symptoms as the independent variables) re-vealed that neither right-sided symptoms ( R2 0.333, .245,t (19) 1.08, p .296) or left-sided symptoms ( .259,t (19) 1.14, p .271) were signicantly associated with asym-metry scores. Of note, there was a signicant correlation betweenasymmetry score and the ratio of right-to-left motor symptomseverity, r (17) .48, p .044, indicating the tendency acrosspatients for increased bias toward left hemispace as the severity of right-sided symptoms increased relative to that of left-sided symp-toms . Correlational analyses revealed no signicant associationswith any other clinical or demographic variable, nor with anymeasure of basic visual function or neuropsychological test score( p .05).
In summary, the ndings from Experiment 2 indicate that thedifferences between RPD and LPD patients in laterality judgmentsfor chimeric stimuli are not necessarily the consequence of differ-ential patterns of (impaired) emotional processing in subgroups.Rather, differences in perceptual bias extend to facial chimerainvolving decisions regarding gender. It has been argued thatperceptual biases obtained from chimeric studies employing gen-
der are likely to reect processes that lie closer to true faceprocessing mechanisms than those employing an emotional judg-ment (Butler & Harvey, 2008; Gooding, Luh, & Tallent, 2001). Inline with this, Gooding et al. (2001) have shown that medicatedpatients with schizophrenia display differential patterns of re-sponse to emotion and gender chimeras with decreased left atten-tional bias for the former, concluding that patients with schizo-phrenia may respond differently to emotion chimeras relative tohealthy controls because of an impaired ability to maintain orretrieve affective information. While the accuracy of PD patients’emotional comprehension in Experiment 1 was not specicallymeasured, the results here indicate that the strong left hemispacebias of RPD patients is unlikely to be wholly attributable todifculties in comprehending (positive) emotional facial cues.Rather it appears that lateralized groups of PD patients showdistinct patterns of attentional bias when making laterality judg-ments of facial stimuli, irrespective of their emotional component.
As before, RPD patients were again the only group to evidencea signicant left hemispace bias, suggesting that damage to striatalstructures that is more extensive on the left side compared to theright side (with greater disruption to dopaminergic pathways in theleft hemisphere compared to the right) leads to a left-lateralizedperceptual bias for gender chimeras. Yet, although recent literatureindicates that, in general, perception of facial conguration criti-cally involves the right hemisphere (right fusiform gyrus; Yovel etal., 2008), and, in particular, that there is a right hemisphereadvantage for the recognition of female faces (Parente & Tom-
masi, 2008), severity of left-sided motor symptoms (indicative of degree of dopaminergic dysfunction in the right hemisphere) wasnot associated with PD patients’ lateralized judgments. Unlike onemotional chimeric faces, severity of right-sided motor symptoms(indicative of degree of dopaminergic dysfunction in the lefthemisphere) also failed to predict patients’ asymmetry scores onthe gender chimeric faces task. There was, however, a relationshipbetween patients’ asymmetry scores and the ratio of right- andleft-sided motor symptom severity. This reected the tendency forpatients with a larger disparity between severity levels of motorsymptoms on one side of the body and those on the other side toshow more extreme asymmetry scores in the direction contralateral
to the worse-affected side. This suggests that dopaminergic loss inone hemisphere relative to that in the other is directly related toboth the direction and extent of perceptual bias for gender chime-ras.
General Discussion
This study examined processing of affective and nonaffectiveinformation in dextral Parkinson’s disease patients with predomi-nant motor symptoms on the left or right side using chimericstimuli. In two experiments, patients with PD predominantly af-fecting the right side (RPD) showed a larger left hemispace biasfor perceiving chimeric stimuli than did patients with PD predom-inantly affecting the left side (LPD), although differences wereonly signicant in the case of the tasks involving decision aboutfaces and not on greyscales, for which asymmetry scores con-verged. In Experiment 1 (emotional chimeric faces), differencesbetween patient subgroups arose from this abnormally large lefthemispace bias in the RPD group. Dopaminergic dysfunction inthe left hemisphere appeared to be strongly associated with a left
hemispace bias for emotional chimeras, as asymmetry scores of PD patients (irrespective of the side of worse motor symptoms)correlated signicantly with severity of motor symptoms on theright side of the body. In Experiment 2 (gender chimeric faces), theonly differences to emerge were between a strong left hemispacebias in RPD and a negligible right hemispace bias in LPD. In thisinstance, hemispace bias on the gender task correlated signicantlywith the ratio of left-to-right motor symptoms severity of allpatients, indicating that the extent of hemispatial inattention wasrelated to the degree of hemispheric asymmetry in the dopaminesystem caused by PD, on the assumption that the latter is reectedin the severity of motor impairments. Of note, across all experi-mental tasks, perceptual bias in patients with PD shared littleassociation with performance on any of the cognitive tests, con-sistent with evidence that cognitive task performance in normals isunrelated to perceptual asymmetry on emotional or nonemotionaltasks of cerebral lateralization (Kim et al., 1990).
The use here of both emotion- and non-emotion-based chimerashelped to distinguish whether right-handed patients with PD withasymmetric disease exhibit abnormal perceptual biases only foremotional stimuli. The fact that differences from controls werefound only for emotional chimeras in RPD is broadly consistentwith the assertion that emotional stimuli are processed differentlyfrom nonemotional stimuli in PD. This is further evidence thatpatients with PD have difculties in recognizing facial emotions,and that asymmetric hemispheric dysfunction is important in stud-ies of affective recognition in PD (Clark et al., 2008; Yip et al.,
2003).Recent meta-analyses of studies performed using PET and fMRI
(Fusar-Poli et al., 2009; Wager, Phan, Liberzon, & Taylor, 2003),suggest that, contrary to older ideas (Benton, 1990), each hemi-sphere is specialized for particular types of emotion, the right morewith negative emotions, and the left more with positive emotions(Fusar-Poli et al., 2009; Root et al., 2006; Wager et al., 2003). Inone study of regional cerebral blood ow, participants with greaterleft frontal activation were better at discriminating happy faceswhile participants with greater right than left parietal activationwere better at discriminating sad faces (Gur et al., 1994). Sinceonly happy and neutral expressions were used in the present study,
(Gooding et al., 2001; Luh et al., 1991), our controls exhibited thereverse pattern, that is, the largest left hemispace bias for grey-scales and the smallest for emotional chimeric faces. This mayreect the mediation of left hemispheric structures in the process-ing of happy faces, but might also be due to the increased com-plexity of the emotional chimeric faces, and the participants’ age.There is evidence that bihemispheric structures are recruited inolder adults (so reducing the left hemispace bias to nonsignicantlevels) as visuospatial task difculty increases (Butler & Harvey,2008; Failla, Sheppard, & Bradshaw, 2003). This would not bepossible in our RPD group, because putative dopamine depletionthe left striatum would not allow equal recruitment in both hemi-spheres. In any case, the contrast between patterns of spatial biasacross chimeric tasks of varying complexity in PD and controlparticipants is striking, especially given their comparable age andsimilar cognitive status.
There were several limitations in the present study. First,though widely used in investigations of cerebral asymmetries(e.g., Failla et al., 2003; Levy et al., 1983; Luh et al., 1991;Rueckert, 2005; Rueckert & Naybar, 2008), our facial stimuli
(spliced not blended photographs) do not necessarily engagenormal mechanisms of face perception (Butler & Harvey,2008), though there is presumably substantial overlap. Second,directional eye movements can enhance lateral perceptual bias(Butler et al., 2005; Butler & Harvey, 2008; Chokron, Bartolo-meo, Perenin, Helft, & Imbert, 1998). Fixations and saccadeswere not recorded in the present study, so we cannot directlyevaluate their role in laterality judgments, particularly the largeleft hemispace bias exhibited by RPD patients. Although eyemovements in PD may be restricted in certain directions, mostcommonly for upward gazing (Corin, Elizan, & Bender, 1972),this typically occurs when the task is to gaze on commandrather than when required to gaze at a target (as in the clinicalexamination and, in effect, the experimental tasks used here),which may be why so few of the patients showed any suchrestrictions. In addition, basal ganglia dysfunction can lead tohypometric saccades (Winograd-Gurvich et al., 2003), and threepatients in this study evidenced slight hypometria on clinicalexamination that was more evident toward targets in left hemis-pace. Yet two of these patients, who had RPD, displayed strongleft-lateralized bias in perceptual measures while the otherpatient, who had LPD, exhibited small right-lateralized biasacross tasks, suggesting asymmetrical dysfunction of the basalganglia and related circuitry was more important than oculo-motor decits in determining direction and extent of observedattentional bias.
The male-to-female ratio was somewhat different in the RPD
group (predominantly male) compared to the LPD and controlgroups (approximately equal numbers of males and females), andthere is evidence on visuospatial tasks that males tend to be moreright hemisphere lateralized (Jewell & McCourt, 2000). Yet mostchimeric studies have reported that, irrespective of gender, partic-ipants tend to attend more to the left-side of chimeric faces (Levyet al., 1983; Luh et al., 1991; Rueckert, 2005). Further, a recentstudy reported no signicant differences between males and fe-males using the Levy version of the chimeric faces task (as used inthe present study), with females evidencing a numerically largerleft hemispace bias (Rueckert & Naybar, 2008). Nevertheless,specic gender differences in PD have been reported in both
self-reports of visuospatial problems (Davidsdottir, Cronin-Golomb, & Lee, 2005) and visuospatial tasks (Davisdottir et al.,2008), so that in a line bisection task men in the RPD groupdeviated toward the left, whereas women were close to the mid-point. In contrast, LPD men displayed a small rightward deviationand women a similar left deviation. However, in the present study,the discrepancy in gender ratios between patient subgroups (andcontrols) failed to account for the groups’ contrasting patterns of perceptual asymmetry on chimeric faces tasks, and right-sidedsymptoms predicted patients’ perceptual bias for emotional chi-meras even after controlling for gender.
Tests using chimeric stimuli offer a new approach to investigatedecits in emotional processing and spatial attention in patientswith asymmetric PD, showing that LPD and RPD patients processthe left and right regions of faces differently. The results from bothexperiments strongly suggest that the degree of asymmetry indopaminergic degeneration in each hemisphere is related to later-alization of visuospatial attention in Parkinson’s disease, althoughemotional processing may also be affected. There are likely to beimportant applications for this research. As previously noted, in
studies with healthy participants, left-lateralized performance inemotional chimeric faces has been shown to signicantly correlatewith scores on measures of emotional awareness and empathy,suggesting that as right hemisphere dominance in the perception of facial emotion increases, the ability to perceive complexity duringthe processing of emotional information increases (Lane, Kivley,Du Bois, Shamasundara, & Schwartz, 1995; Rueckert & Naybar,2008; Rueckert & Pawlak, 2000). Further studies are needed toelucidate the functional signicance of an abnormally large leftspatial bias for emotional chimeras, as displayed by patients withpredominantly right-sided symptoms, and how this links withimpaired emotional processing.
Visuospatial asymmetries are also likely to have practical sig-nicance for navigation in PD. Leftward attentional bias in healthypeople causes a subtle rightward neglect, which results in morerightward collisions (Nicholls, Loftus, Mayer, & Mattingley, 2007;Nicholls, Loftus, Orr, & Barre, 2008). Veering in Parkinson’spatients also appears to correspond to the shifting of the perceivedmidline, with LPD patients evidencing a rightward shift in veeringwhereas RPD patients (like healthy controls) veer leftward (Dav-idsdottir et al., 2008). Further, in healthy controls, levadopa im-proves straight-line walking (by reducing veering), indicative of alink between asymmetric organization of dopaminergic functionand the spatial orientation skills involved in navigation (Mohr,Landis, Bracha, Fathi, & Brugger, 2003). In HD, asymmetryindices on greyscales were signicantly related to visual perfor-mance during driving (Tant, Brouwer, Cornelissen, & Kooijman,
2002). Therefore, patterns of attentional bias in PD, illustratedmost clearly in this study by the exaggerated left hemispace bias of RPD patients, have the potential to affect patients’ everyday in-teractions with the environment. Impaired spatial navigation dur-ing gait is well known in Parkinson’s disease (Davidsdottir et al.,2005, 2008; Lee & Harris, 1999), as are problems with driving (Ucet al., 2007). With this in mind, research intended to investigate therelationship between these difculties and attentional bias in PDparticipants, perhaps with a focus on the inuence of dopaminergicmedication, is likely to be benecial in understanding the precisenature of patients’ problems with navigation in everyday settingsand how they may best overcome them.
Amick, M. M., Schendan, H. E., Ganis, G., & Cronin-Golomb. A. (2006).Frontostriatal circuits are necessary for visuomotor transformation:Mental rotation in Parkinson’s disease. Neuropsychologia, 44, 339–349.
Assogna, F., Pontieri, F., Caltagirone, C., & Spalletta, G. (2008). Therecognition of facial emotion expressions in Parkinson’s disease. Euro-
pean Neuropsychopharmacology, 18, 835–848.Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory (2nd ed.). San Antonio, TX: Psychological Corp.
Benton, A. L. (1990). Facial recognition. Cortex, 26, 491–499.Benton, A. L., & Hamsher, K. (1976). Multilingual aphasia examination.
Iowa City: University of Iowa.Bracha, H. S., Shults, C., Glick, S. D., & Kleinman, J. E. (1987). Sponta-
neous asymmetric circling behavior in hemi-parkinsonism; a humanequivalent of the lesioned-circling rodent behavior. Life Sciences, 40,1127–1130.
Butler, S. H., Gilchrist, I. D., Burt, D. M., Perrett, D. I., Jones, E., &Harvey, M. (2005). Are the perceptual biases found in chimeric faceprocessing reected in eye-movement patterns? Neuropsychologia, 43,52–59.
Butler, S. H., & Harvey, M. (2008). Effects of ageing and exposure
duration on perceptual biases in chimeric face processing. Cortex, 44,665–672.Chokron, S., Bartolomeo, P., Perenin, M., Helft, G., & Imbert, M. (1998).
Scanning direction and line bisection: A study of normal subjects andunilateral neglect patients with opposite reading habits. Cognitive Brain Research, 7, 173–178.
Clark, U. S., Neargarder, S., & Cronin-Golomb, A. (2008). Specic im-pairments in the recognition of emotional facial expressions in Parkin-son’s disease. Neuropsychologia, 46, 2300–2309.
Clower, D. M., Dum, R. P., & Strick, P. L. (2005). Basal ganglia andcerebellar inputs to“AIP.” Cerebral Cortex, 15, 913–920.
Cooper, C. A., Mikos, A. E., Wood, M. F., Kirsch-Darrow, L., Jacobson,C. E., Okun, M. S., et al. (2008). Does laterality of motor impairment tellus something about cognition in Parkinson’s disease? Parkinsonism and Related Disorders, 15, 315–317.
Corin, M. S., Elizan, T. S., & Bender, M. B. (1972). Oculomotor functionin patients with Parkinson’s disease. Journal of Neurological Sci-ences, 15, 251–265.
Davidsdottir, S., Cronin-Golomb, A., & Lee, A. (2005). Visual and spatialsymptoms in Parkinson’s disease. Vision Research, 45, 1285–1296.
Davidsdottir, S., Wagenaar, R., Young, D., & Cronin-Golomb, A. (2008).Impact of optic ow perception and egocentric coordinates on veering inParkinson’s disease. Brain, 131, 2882–2893.
Desimone, R., & Duncan, J. (1995). Neural mechanisms of selective visualattention. Annual Review of Neuroscience, 18, 193–222.
Dujardin, K., Blairy, S., Defebvre, L., Duhem, S., Noel, Y., Hess, U., et al.(2004). Decits in decoding emotional facial expressions in Parkinson’sdisease. Neuropsychologia, 42, 239–250.
Ebersbach, G., Trottenberg, T., Hattig, H., Schelosky, L., Schrag, A., &Poewe, W. (1996). Directional bias of initial visual exploration: Asymptom of neglect in Parkinson’s disease. Brain, 119, 79–87.
Fahn, S., Elton, R. L., & Members of the UPDRS Development Committee(1987). United Parkinson’s disease rating scale. In S. Fahn, C. D.Marsden, D. B. Calne, & M. Goldstein (Eds.), Recent developments inParkinson’s disease (Vol. 2, pp. 153–164). Florham Park, NJ: MacmilanHealth Care Information.
Failla, C. V., Sheppard, D. M., & Bradshaw, J. L. (2003). Age andresponding hand related changes in performance of neurologically nor-mal subjects on the line bisection and chimeric faces tasks. Brain and Cognition, 52, 353–363.
Filoteo, J. V., Maddox,W. T., Ing, A. D., & Song, D. D. (2007). Charac-terizing rule-based category learning decits in patients with Parkinson’sdisease. Neuropsychologia, 45, 305–320.
Fimm, B., Zahn, R., Mull, M., Kemeny, S., Buchwald, F., Block, F., et al.(2001). Asymmetries of visual attention after circumscribed subcorticalvascular lesions. Journal of Neurology, Neurosurgery and Psychia-try, 71, 652–657.
Fink, G. R., Marshall, J. C., Shah, N. J., Weiss, P. H., Halligan, P. W.,Grosse-Ruyken, M., et al. (2000). Line bisection judgments implicateright parietal cortex and cerebellum as assessed by fMRI. Neurology, 54,
1324–1331.Finke, K., Bublak, P., Dose, M., Muller, H. J., & Schneider, W. X. (2006).
Parameter-based assessment of spatial and non-spatial attentional de-cits in Huntington’s disease. Brain, 129, 1137–1151.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). “Mini-MentalState”: A practical method for grading the cognitive state of patientsfor the clinician. Journal of Psychiatric Research, 12, 189–198.
Foster, E. R., Black, K. J., Antenor-Dorsey, J. V., Perlmutter, J. S., &Hershey, T. (2008). Motor asymmetry and substantia nigra volume arerelated to spatial delayed response performance in Parkinson disease. Brain and Cognition, 67, 1–10.
Fowler, M. S. (1996). Visual processing in adults with acquired braindamage and children with developmental dyslexia. Unpublished doc-toral dissertation, University of Reading, Reading, United Kingdom.
Fusar-Poli, P., Placentino, A., Carletti, F., Allen, P., Landi, P., Abbamonte,M., et al. (2009). Laterality effect on emotional faces processing: ALEmeta-analysis of evidence. Neuroscience Letters, 452, 262–267.
Gibb, W. R., & Lees, A. J. (1988). The relevance of the Lewy body to thepathogenesis of idiopathic Parkinson’s disease. Journal of Neurology, Neurosurgery and Psychiatry, 51, 745–752.
Goodglass, H., & Kaplan, E. (1972). The assessment of aphasia and related disorders. Philadelphia: Lea & Febiger.
Gooding, D. C., Luh, K. E., & Tallent, K. A. (2001). Evidence of schizo-phrenia patients’ reduced perceptual biases in response to emotionchimera, Schizophrenia Bulletin, 27, 709–716.
Gur, R. C., Skolnick, B. E., & Gur, R. E. (1994). Effects of emotionaldiscrimination tasks on cerebral blood ow: Regional activation and itsrelation to performance. Brain and Cognition, 25, 271–286.
Harris, J. P., Atkinson, E. A., Lee, A. C., Nithi, K., & Fowler, M. S. (2003).Hemispace differences in the visual perception of size in left hemiParkinson’sdisease. Neuropsychologia, 41, 795–807.
Ho, A. K., Nestor, P. J., Williams, G. B., Bradshaw, J. L., Sahakian, B. J.,Robbins, T. W., et al. (2004). Pseudo-neglect in Huntington’s diseasecorrelates with decreased angular gyrus density. Neuroreport, 15, 1061–1064.
Hoehn, M. M., & Yahr, M. D. (1967). Parkinsonism: Onset, progression,and mortality. Neurology, 17, 427–442.
Jewell, G., & McCourt, M. E. (2000). Pseudoneglect: A review andmeta-analysis of performance factors in line bisection tasks. Neuropsy-chologia, 38, 93–110.
Kaasinen, V., Nurmi, E., Bruck, A., Eskola, O., Bergman, J., Solin, O., etal. (2001). Increased frontal [(18)F] uorodopa uptake in early Parkin-son’s disease: Sex differences in the prefrontal cortex. Brain, 124,
1125–1130.Kan, Y., Kawamura, M., Hasegawa, Y., Mochizuki, S., & Nakamura, K.
(2002). Recognition of emotion from facial, prosodic and written verbalstimuli in Parkinson’s disease. Cortex, 38, 623–630.
Karnath, H.-O., Himmelbach, M., & Rorden, C. (2002). The subcorticalanatomy of human spatial neglect: Putamen, caudate nucleus and pulv-inar. Brain, 125, 350–360.
Kim, H., Levine, S. C., & Kertesz, S. (1990). Are variations amongsubjects in lateral asymmetry real individual differences or random errorin measurement? Putting variability in its place. Brain and Cogni-tion, 14, 220–242.
Kinsbourne, M. (1970). The cerebral basis of lateral asymmetries in atten-tion. Acta Psychologica, 33, 193–201.
455PERCEPTUAL BIAS IN ASYMMETRIC PARKINSON’S DISEASE