Psychosocial and Immune Effects of Self-Hypnosis Training for StressManagement Throughout the First Semester of Medical School
WAYNE G. WHITEHOUSE, PHD, DAVID F. DINGES, PHD, EMILY CAROTA ORNE, BA,STEVEN E. KELLER, PHD, BRAD L. BATES, PHD, NANCY K. BAUER, MSS, ACSW,PAGE MORAHAN, PHD, BARBARA A. HAUPT, RN, MICHELE M. CARLIN, BA,PETER B. BLOOM, MD, LINE ZAUGG, AND MARTIN T. ORNE, MD, PHD
This study was a 19-week prospective conducted to determine the effectiveness of a self-hypnosis/relaxationintervention to relieve symptoms of psychological distress and moderate immune system reactivity toexamination stress in 35 first-year medical students. Twenty-one subjects were randomly selected for trainingin the use of self-hypnosis as a coping skill and were encouraged to practice regularly and to maintain dailydiary records related to mood, sleep, physical symptoms, and frequency of relaxation practice. An additional14 subjects received no explicit training in stress-reduction strategies, but completed similar daily diaries.Self-report psychosocial and symptom measures, as well as blood draws, were obtained at four time points:orientation, late semester, examination period, and postsemester recovery. It was found that significantincreases in stress and fatigue occurred during the examination period, paralleled by increases in counts of Blymphocytes and activated T lymphocytes, PHA-induced and PWM-induced blastogenesis, and natural killercell (NK) cytotoxicity. No immune decreases were observed. Subjects in the self-hypnosis condition reportedsignificantly less distress and anxiety than their nonintervention counterparts, but the two groups did notdiffer with respect to immune function. Nevertheless, within the self-hypnosis group, the quality of theexercises (ie, relaxation ratings) predicted both the number of NK cells and NK activity. It was concluded thatstress associated with academic demands affects immune function, but immune suppression is not inevitable.Practice of self-hypnosis reduces distress, without differential immune effects. However, individual responsesto the self-hypnosis intervention appear to predict immune outcomes.
Key words: examination stress, self-hypnosis, immunity, lymphocyte proliferation, NK cytotoxicity.
INTRODUCTION
Immune system alterations, apparently inducedby exposure to physical or psychological stressors,have been documented in numerous investigationsover the past decade. Academic examination stresshas provided a particularly useful research paradigmbecause it permits the prospective investigation of
From the The Institute of Pennsylvania Hospital and Depart-ment of Psychiatry of the University of Pennsylvania MedicalSchool, Philadelphia, PA (W.G.W., D.F.D., E.C.O., B.L.B., N.K.B.-M., P.B.B., M.T.O.); Department of Psychiatry of the University ofMedicine and Dentistry of New Jersey, Newark, NJ (S.E.K.);Department of Microbiology and Immunology at the MedicalCollege of Pennsylvania, Philadelphia, PA (P.M.); and The Insti-tute of Pennsylvania Hospital, Philadelphia, PA (B.A.H., M.M.C.,L.Z.).
Address reprint requests to: David F. Dinges, PhD, Unit forExperimental Psychiatry, University of Pennsylvania MedicalSchool, 1013 Blockley Hall, 423 Guardian Drive, Philadelphia, PA19104-6021.
Received for publication March 31, 1994; revision receivedOctober 2, 1995.
the impact upon psychological and physiologicalfunctioning of a commonplace, predictable and rel-atively circumscribed stressor. Academic examina-tions clearly increase levels of anxiety and emotionaldistress (1-4), and promote diverse endocrine alter-ations, including catecholamine, thyroid, and glu-cocorticoid effects (3, 5-12). Exam stress also hasdemonstrable immunomodulatory potential. In a se-ries of studies with Ohio State University medicalstudents, Kiecolt-Glaser, Glaser, and colleagues havereported associations between exam stress and anumber of immune parameters, including decreasednatural killer (NK) cell activity (1, 13), decreased NKcell number (14), decreases in percentage of helper/inducer T lymphocytes and in the helper/inducer-suppressor/cytotoxic-cell ratio (9), reduced transfor-mation of B lymphocytes by Epstein-Barr virus(EBV) (15), reductions in levels of certain lympho-kines (eg, interferon gamma (IFN-y) and leukocytemigration inhibition factor (16) as well as increasedplasma levels of interleukin-2 (IL-2) (17), and in-creased antibody titers to latent herpesviruses (16,18). Other investigators have reported a suppression
in the proliferative response of lymphocytes to mi-togens during academic Exam stress (9, 19, 20).
Examining the immunologic effects of interven-tions that are aimed at reducing psychological reac-tivity to stress that is engendered by academic exam-inations allows one to go beyond the correlationalnature of observational studies. In one such investi-gation, Kiecolt-Glaser et al. (13) obtained blood sam-ples from 34 first-year medical students during abaseline period 1 month before major examinations,and again, on the final day of the 3-day examinationperiod. In the interval between the two blood draws,a random half of the subjects participated in ahypnosis/relaxation group, which included homepractice, whereas the remaining subjects received nointervention. The findings suggest that relaxationtraining may have prevented exam-related increasesin self-reported distress symptoms, but there wereno reliable differences between the two treatmentconditions on any of the cellular immune measuresstudied. Interestingly, however, multiple regressionanalyses revealed that frequency of relaxation prac-tice was a significant predictor of increases, relativeto baseline levels, in the percentage of T helper/inducer cells during the exam period.
Relaxation procedures have also been associatedwith immunologic changes in a number of otherinvestigations. After a 1-month intervention period,geriatric patients who received relaxation trainingreported a decrease in distress symptoms coupledwith increased NK cell cytotoxicity and decreasedantibody titers to latent herpes simplex virus(HSV-l) (21). In a study by Peavey and colleagues(22), subjects with high life stress scores on self-report stress and coping scales, coupled with poorphagocytic capacity, were randomly assigned to ei-ther biofeedback-assisted relaxation training or acontrol condition. Following attainment of targetcriteria for reduced frontalis electromyographic ac-tivity and increased hand temperature by the relax-ation group, subjects in both conditions were reas-sessed. Although relaxation training did notsignificantly reduce stress reports, it was associatedwith reductions in tension and anxiety. Further-more, neutrophil activation capacity was reliablyenhanced, suggesting a qualitative improvement inphagocytic ability for subjects who underwent relax-ation training. In another study, a single 20-minutesession, during which subjects were engaged in oneof several forms of relaxation, resulted in a signifi-cant increase in salivary S-IgA concentrations fromprerelaxation to postrelaxation, in contrast to a non-relaxation control group (23). Recently, a study ofthe effects of relaxation on immunity in males at
high risk for HIV-1 infection found significant posi-tive correlations between the frequency of relaxationpractice and numbers of T helper, T inducer cells,the T helper/T suppressor ratio, and the number ofNK cells during the high-stress week of serostatusdetermination (24).
In view of these promising findings on the effectsof relaxation-based interventions on stress-inducedalterations of immune function, the current studysought to evaluate further the utility of self-hypnosispractice as a method of alleviating stress amongfirst-year medical students. The investigation wasdesigned as a major extension of previous researchin several ways:
1. Subjects' ability to experience hypnosis wasindependently assessed in an attempt to distinguisheffects that may be related to hypnotic processesfrom those arising from nonspecific relaxation;
2. Sampling points for the collection of psychoso-cial and immunologic data occurred four times dur-ing the semester—orientation, late semester, duringthe end-of-semester final examinations,* and duringthe recovery period following the semester break—thereby permitting a more extensive evaluation ofthe impact of persistent academic demands on psy-choimmunologic functioning than has been accom-plished in earlier investigations;
3. A comprehensive battery of immune measures(both quantitative and functional) was carried out onall blood samples, representing assays that arewidely used, and which show considerable sensitiv-ity to the influence of stress, bereavement, anddepression in human psychoimmunologic research.
4. The influence of interassay variability, a poten-tially serious confound in longitudinal research, wasstatistically controlled (25).
METHODS
SubjectsProspective participants were introduced to the study by a
letter sent to the incoming freshman class [N = 110; 46% women;72% white; mean age = 24.5) of a local medical school. In this
* The examinations consisted of the individual National Boardsubject examinations in Physiology and Biochemistry, which areused by many medical schools as end-of-course examinations.They also provide an opportunity for students to assess theirreadiness for the complete National Board examination of basicscience subjects, which usually is given at the end of the secondyear of medical school.
250 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
introductory letter, the students were informed that the study wasconcerned with the impact of typical academic stressors on mood,sleep, and immunity, and the extent to which these effects can bebehaviorally mitigated by use of cognitive strategies, such asself-hypnosis and relaxation techniques. It was explained furtherthat a random sample of volunteers would be selected to receivetraining in self-hypnosis for relaxation, while the remainingvolunteers would have an opportunity to receive the same train-ing in the following semester. Thirty-five (14 men, 21 women;71% white; mean age = 24.8) first-year medical student volun-teers participated in the 19-week investigation, including psycho-social assessments and blood draws at each of the four scheduledtime points. A medical screen before each blood draw establishedthat none of the subjects took drugs or medications nor sufferedany chronic illness that might affect the immune system.
discussing their experiences during these group sessions, subjectswere encouraged to engage in self-hypnosis exercises on theirown for at least 15 minutes each day. They also completed dailydiaries (33), which inquired about the extent and quality of sleepobtained, mood, medications, and any problems experienced, inaddition to assessing the frequency of practice and relaxationbenefit of the self-hypnosis exercises.
No-Treatment Control Condition. Those research participantsnot selected for the self-hypnosis condition served as controlsubjects (6 men, 8 women). As such, they received no training inthe use of behavioral coping strategies, but they were offered theopportunity to learn self-hypnosis in the following semester, afterthe current study was completed. Control subjects filled out thesame daily diaries that subjects in the self-hypnosis conditionwere asked to complete; however, references to the self-hypnosisexercise were omitted.
ProcedureSubjects met with the investigators during orientation to the
fall semester, when they completed informed consent materialsand provided a medical history that included questions aboutcurrent usage of medications, drugs, alcohol, caffeine, and to-bacco. After this, subjects completed the Profile of Mood States(POMS) (26), the Brief Symptom Inventory (BSI) (27), and theUCLA Loneliness Scale (28) and had a 30-ml sample of blooddrawn from the nondominant arm by antecubital venipuncture.The same procedures were followed on three subsequent occa-sions: 13 weeks after orientation [late semester), 3 weeks laterwhen the subjects were taking their final examinations in Physi-ology and Biochemistry {exam stress], and 3 weeks after theexamination period, at the end of midyear break [recovery).During the recovery session, subjects also provided retrospectiveratings of perceived stressfulness for each of the target samplingpoints in the investigation.
Self-Hypnosis Training Condition. All volunteers were in-formed at the outset of the study that they might be randomlyselected to receive self-hypnosis training as a means of copingwith stress. Twenty-one subjects (8 men, 13 women) were as-signed to the self-hypnosis condition. Training sessions lastedapproximately 90 minutes and were regularly scheduled aroundthe noon hour, one day per week, throughout the semester.Fourteen such sessions were carried out by two senior psychia-trists with extensive experience in the clinical use of hypnosisand relaxation procedures. The first session included an assess-ment of subjects' hypnotic ability using the Harvard Group Scaleof Hypnotic Susceptibility, Form A (HGSHS:A) (29). During thefollowing week's session, the ability to respond to suggestionsadministered during self-hypnosis was assessed using the Inven-tory of Self-Hypnosis (ISH) (30)+. In addition to practicing and
t The ISH is an adaptation of the widely used HGSHS:A thatretains the item content and self-scoring features of the parentinstrument, but which was conservatively modified to facilitateadministration under conditions of self-hypnosis rather thanheterohypnosis. Two prior studies (31, 32), which comparedbehavioral performances assessed by the two scales, found thatthe overall sample mean scores for the ISH and HGSHS:A werevirtually identical. Nevertheless, Pearson correlations betweenthe total scores on the two measures were only 0.39 in one study(31) and 0.47 in the other (32). Similarly, in the current sample of
Immune MeasuresBlood samples (30 ml) were collected into heparinized syringes
(preservative-free heparin) between 7:00 AM and 8:30 AM oneach of the target days. All assays were performed on freshlydrawn blood by laboratory personnel who were blind to subjects'identities and their assignment to experimental condition.
Lymphocytes were separated from whole blood by Ficoll-Hypaque (Pharmacia Fine Chemicals, Piscataway, NJ) centrifuga-tion. The lymphocytes had greater than 99% viability as assessedby trypan blue exclusion.
Enumeration of T, B, monocyte, granulocyte, NK, T4, T8,helper-inducer, and suppressor-inducer cells was determined bytwo-color flow cytometry. Fifty microliters of heparinized wholeblood was added to 200 /̂ l of the appropriate fluorescein- orphycoerythrin-labeled monoclonal antisera (all from Coulter Im-munology, Hialeah, FL) or control solution, incubated for 30minutes, and processed using the Q-prep system (Coulter), beforequantitation by a flow cytometer.
Mitogen-induced lymphocyte stimulation was performed onisolated lymphocytes according to standard techniques (34). Stim-ulation by ConA (Calbiochem, San Diego, CA), PHA (WellcomeReagents Ltd, Beckenham, England), and PWM (GIBCO, GrandIsland, NY) was performed in triplicate utilizing three concentra-tions of each mitogen as follows: ConA, 0.75.1.50, and 3.00 jig perwell (0.2 ml); PHA, 0.01, 0.05, and 0.40 jig per well; and PWM,0.05, 0.10, and 1.00 jig per well. After an incubation period of 78hours for ConA and PHA and 126 hours for PWM, idoxuridinelabeled with iodine 1Z5I (0.20 /xCi, specific activity, 2000 Ci/mmol;New England Nuclear, Boston, MA) and floxuridine (Sigma, St.Louis, MO), to yield a final concentration of 10~6 mol/liter, wereadded to the cultures. After 18 hours, the cells were harvested andidoxuridine 125I incorporation was measured in a gamma counter.The mean of the triplicate determinations was calculated and thedata were expressed as counts per minute (cpm) in stimulatedcultures minus the cpm in unstimulated cultures (A cpm).
subjects, the mean scores for HGSHS:A and ISH were 7.57 and7.73, respectively, whereas the correlation between the measureswas 0.42. Such modest correlations suggest that self-hypnosis andheterohypnosis involve distinctive processes that may renderstandard heterohypnosis scales, such as the HGSHS:A, poorpredictors of self-hypnotic skill when used on their own.
Psychosomatic Medicine 58:249-263 (1996) 251
W. G. WHITEHOUSE et al.
NK cell activity was assessed using the target cell line K562 ina 4-hour chromium 51 release assay. K562 target cells weremaintained in flask cultures of RPMI 1640 supplemented with10% fetal calf serum (GIBCO), transferred twice weekly andseeded as needed for the assay. Target cells were labeled with 300to 500 piCi of chromium 51 (sodium chromate chromium 51, NewEngland Nuclear) and placed in each well of a microtiter platewith one of three effector-to-target cell concentrations (25:1, 50:1,or 100:1). After incubation for 4 hours at 37°C in a humidified CO2
incubator, the supernatants were collected and counted in agamma counter. Total release was obtained by Triton-X (Mallinck-rodt, Inc, Paris, KY) disruption of aliquots of labeled target cells,and a medium control was included to assess nonspecific releaseof chromium 51 from the target cells. The percentage of specificisotope release, ie, NK activity, was calculated as follows:
Data AnalysisFor the mitogen assays, the delta cpm data were log trans-
formed due to heterogeneity of variance. The mean response ofthe two concentrations that yielded the optimal and suboptimalresponse for each mitogen was utilized as the dependent measurefor analysis (ConA, 1.50 and 3.00 pig; PHA, 0.05 and 0.40 pig;PWM, 0.05 and 0.10 pig). The mean specific release for the twooptimum effector:target ratios was utilized as the unit of measure-ment of NK activity (E:T ratios, 100:1 and 50:1).
Analyses of the immunologic data began with a preliminaryexamination of the effects of the self-hypnosis intervention oversampling time points using repeated-measures multivariate anal-yses of variance (MANOVAs), computed separately for the quan-titative and functional assay measures. These were followed witha hierarchical multiple regression procedure that partitioned thevariance of the criterion variable into between-subjects and with-in-subjects (ie, over repeated sampling points) sources, while aneffects coding scheme (35) was used to represent the repeatedsampling factor. This analytic strategy was adopted in favor ofunivariate repeated-measures analysis of variance (ANOVA) inorder to partial out the influence on immune outcomes of day-to-day variability in assay sensitivity using an analysis of partialvariance (APV), thereby reducing the proportion of unexplainedor error variance and increasing statistical power (25, 35). Toaccomplish this, small groups of comparably aged subjects (N =3-6) in the study environment, but who did not participate in thestudy proper (ie, laboratory technicians and graduate students),provided blood samples that were drawn and analyzed at thesame time as those obtained from the study participants. These"APV control subjects" also received a brief medical screen oneach occasion to ensure the absence of drugs or illnesses thatmight compromise their immune systems. To reduce the likeli-hood of artifact due to uncontrollable, idiosyncratic immunealterations in one or more of these APV subjects, the mean valuefor all APV subjects sampled on a given day was treated as acovariate for the corresponding study participants whose bloodhad been processed contemporaneously. Because each samplingtime point of the study involved the collection of blood samplesover 2 or 3 consecutive days, assays for each day of a givensampling point were associated with separate mean APV controlvalues. APV scores for each immune measure were entered as thefirst predictor variable in the hierarchical regressions in order to
statistically control any effects due to variability in assay qualityover time (25). A second reason for implementing within-subjectsregression analyses was to avoid the loss of cases from theanalyses due to a single missing data point, as would occur withlistwise deletion in repeated-measures ANOVA. Overall, thewithin-subjects hierarchical APV model provides greater statisti-cal power than repeated-measures ANOVA in that it reduces errorvariance related to fluctuations in immune assay sensitivity andutilizes all available data in the analyses, making it ideal for usewith modest sample sizes. The specific hierarchical regressionmodel used for the primary analyses of the investigation consistedof the following order of predictor variables: APV value, gender,sampling point, condition (ie, intervention), gender X condition,gender X sampling point, condition x sampling point, gender xcondition X sampling point. Supplemental analyses examinedthe effects on immunity of loneliness and stress symptomatology(using the positive symptom total index of the BSI), by enteringscores for these measures following the APV control value in theregression model.
Psychosocial data were analyzed by univariate 2 (treatment con-dition) x 4 (sampling point) repeated-measures ANOVAs. Signifi-cant within-subject main effects were examined with planned con-trasts, while interactions were subjected to follow-up multiplecomparisons using the Newman-Keuls procedure (a<.05).
RESULTS
Orientation Baseline Comparisons
No significant intergroup differences were ob-served on any of the immunological measures ob-tained from the orientation baseline sample. Theintervention and control groups were comparable onbaseline measures of loneliness, mood, and virtuallyall of the BSI measures of psychological distressexcept depressive symptomatology, which washigher among the subjects randomized to the controlgroup (M = 56.0 vs. 48.6, i(33) = 2.5, p < .02).
Hypnotic Ability and Frequency of PracticeScores obtained for the two hypnotizability mea-
sures (the heterohypnotic HGSHS:A and the self-hypnotic ISH) were averaged to provide a stableestimate of hypnotic talent. All subjects in the self-hypnosis condition demonstrated adequate ability toderive benefit from the self-hypnosis exercises [M =7.74, SD = 1.28), with 14 subjects scoring in themoderate range (5-8) and 7 subjects scoring in thehigh range (9-12) of the 0 to 12 point assessmentscale.
Frequency of practice of the self-hypnosis exercisewas ascertained by examining daily diary records forthe weeks corresponding to the blood samplingpoints of the investigation. Compliance with therequest that subjects engage in a period of massedpractice of the self-hypnosis exercise during baseline
252 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
resulted in their averaging 1.5 practice sessions(range = 0.6-2.6) per day during the first week aftertraining in self-hypnosis. After this, they continuedto utilize self-hypnosis on roughly a daily basisthroughout both the late semester (M = 5 times/week; SD = 3.23) and acute exam stress (M = 6times/week; SD = 2.87) periods. As expected, self-hypnosis practice occurred less frequently duringthe postexam recovery period (M = 2 times/week;SD = 1.71). Subjects' ratings of the relaxation benefitderived from self-hypnosis were quite stable acrossthe sampling points of the study [F < 1.0), encom-passing weekly mean values between 40 and 50 on a100-mm visual analog rating scale.
Psychosocial Measures
Table 1 presents data for the nine BSI symptomdimensions and three global severity indices at eachsampling point during the investigation. Significantvariation over time was found for four of the indi-vidual symptom scales (ie, obsessive-compulsivesymptoms, depression, anxiety, and hostility) andtwo of the global indices (ie, general severity indexand positive symptom distress index). These maineffects were followed up with specific planned con-trasts in which the score for the exam period wascompared with the average of the scores obtainedfrom the remaining three sampling points. In everycase, the score from the exam period was found to bereliably elevated (p < .05). Additional post hocanalyses found scores for the anxiety scale and thetwo global severity measures to be equally highduring orientation. Thus, the anticipation of begin-ning medical school also engendered significantpsychological distress, which diminished by the latesemester sampling point.
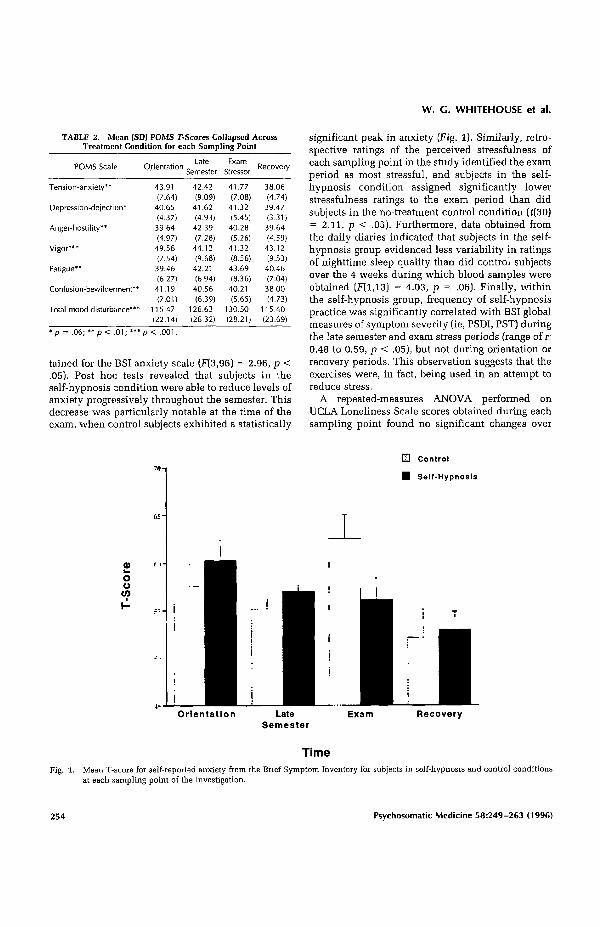
Analysis of the six subscales of the POMS revealedsignificant variation in mood states over time, al-though the individual patterns were different (Table2). Not surprisingly, tension-anxiety was highest atorientation and lowest at recovery (F(3,8l) = 4.06,p < .01), as was confusion-bewilderment (F(3,81) =4.19, p < .01). Depression-dejection tended to behigher throughout all semester sampling points, rel-ative to recovery (F(3,87) = 2.56, p = .06). Anger-hostility scores were elevated only during the latesemester sampling period (F(3,78) = 5.09, p < .01).Vigor scores were highest at orientation and lowestduring the exam (F(3,84) = 9.22, p < .001), whereasfatigue ratings showed a pattern of progressive in-creases at each sampling point through the examphase, after which it declined significantly during
TABLE 1. Mean (SD) BSI T-Scores Collapsed AcrossTreatment Condition for each Sampling Point
the recovery period (F(3,81) = 5.50, p < .01). Thetotal mood disturbance score increased during thelate semester sampling period, peaking at the time ofthe exam, thereafter returning at recovery to thesame lower levels observed during orientation(F(3,84) = 14.33, p < .001).
Daily Diary
Sleep durations, as reported in the daily diaries,were averaged over weekdays for each of the 19weeks of investigation. Similarly, subjective dailystress ratings based on a 100-mm analog scale wereaveraged for the same weeks. The Spearman rank-order correlation between these two summary indi-ces was highly reliable (rho = -0.70, p < .001),demonstrating clearly that there was a reduction insleep during periods when perceived stress washigh.
Intervention EffectsEffects of the self-hypnosis intervention were evi-
dent on several psychological measures. A signifi-cant group x sampling point interaction was ob-
Psychosomatic Medicine 58:249-263 (1996) 253
W. G. WHITEHOUSE et al.
TABLE 2. Mean (SD) POMS T-Scores Collapsed AcrossTreatment Condition for each Sampling Point
POMS Scale OrientationSemester Stressor
Recovery
Tension-anxiety**
Depression-dejection*
Anger-hostility**
Vigor*"*
Fatigue**
Confusion-bewilderment**
Total mood disturbance***
* p = .06; * * p < .01; **•
43.91(7.64)
40.65(4.37)39.64(4.97)
49.56(7.54)
39.46(6.27)
41.19(7.01)
115.47(22.14)
p < .001.
42.42(9.09)
41.62(4.93)42.39(7.28)
44.12(9.68)
42.21(6.94)
40.56(6.39)
126.63(26.32)
41.77(7.08)
41.32(5.45)
40.28(5.26)41.32(8.56)
43.69(8.36)
40.21(5.65)
130.50(28.21)
38.06(4.74)
39.47(3.31)39.64(4.59)
43.12(9.53)
40.46(7.04)38.00(4.73)
115.40(23.69)
tained for the BSI anxiety scale (F(3,96) = 2.96, p <.05). Post hoc tests revealed that subjects in theself-hypnosis condition were able to reduce levels ofanxiety progressively throughout the semester. Thisdecrease was particularly notable at the time of theexam, when control subjects exhibited a statistically
significant peak in anxiety (Fig. 1). Similarly, retro-spective ratings of the perceived stressfulness ofeach sampling point in the study identified the examperiod as most stressful, and subjects in the self-hypnosis condition assigned significantly lowerstressfulness ratings to the exam period than didsubjects in the no-treatment control condition (£(30)= 2.11, p < .05). Furthermore, data obtained fromthe daily diaries indicated that subjects in the self-hypnosis group evidenced less variability in ratingsof nighttime sleep quality than did control subjectsover the 4 weeks during which blood samples wereobtained (F(l,13) = 4.03, p = .06). Finally, withinthe self-hypnosis group, frequency of self-hypnosispractice was significantly correlated with BSI globalmeasures of symptom severity (ie, PSDI, PST) duringthe late semester and exam stress periods (range of r:0.48 to 0.59, p < .05), but not during orientation orrecovery periods. This observation suggests that theexercises were, in fact, being used in an attempt toreduce stress.
A repeated-measures ANOVA performed onUCLA Loneliness Scale scores obtained during eachsampling point found no significant changes over
ED Control
• Self-Hypnosis
Orientation Late ExamSemester
Recovery
TimeFig. 1. Mean T-score for self-reported anxiety from the Brief Symptom Inventory for subjects in self-hypnosis and control conditions
at each sampling point of the investigation.
254 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
TABLE 3. Regression of B Lymphocyte Counts on Gender,Intervention, and Sampling Time Point
TABLE 4. Regression of Activated T Lymphocyte Counts onGender, Intervention, and Sampling Time Point
Factor
Between subjectsGenderTreatmentGender x treatment
Within subjectsAPV controlTime
T l
T2
T3Gender x time
T1T2
T3
Treatment X timeTlT2T3
Gender X TreatmentX time
T l
T2T3
1 R2 uponentry
0.0040.0000.059
0.0790.183
0.004
0.002
0.007
Note: Throughout the course of the icoefficient of variation,subjects, was 49.6%. T1
based on mea
F
0.130.181.96
144.83335.50
7.33
3.67
12.83
-0.060.03
-0.49
0.28
-0.430.220.38
-0.05-0.06-0.03
-0.080.05
-0.03
0.24-0.03-0.22
P <
NSNSNS
.001
.001
.01
.05
.001
nvestigation, the interassayn values for "APVcontrol"
, T2, and T3 represent the "effects coded"
Factor
Between subjectsGenderTreatmentGender X treatment
Within subjectsAPV controlTime
T l
T2T3
Gender x timeT l
T2
T3
Treatment x timeT l
T2T3
Gender X treatmenttime
T1
T2
T3
Note: Throughout thecoefficient of variation,subiects. was 62.7%. Tl
f R2 uponentry
0.0000.0060.001
0.0180.083
0.013
0.026
X 0.008
course of the in1
based on mean
F
0.000.180.03
2.1914.27
2.23
4.47
1.38
0.03-0.08
0.07
0.13
-0.270.130.32
-0.20-0.03
0.09
-0.02-0.28
0.19
0.390.130.07
P <
NSNSNS
NS.001
NS
.01
NS
instigation, the interassayvalues IFor "APV
1, T2, and T3 represent the "effectscontrol"coded"
predictor set for Time (ie, sampling period).
time for either the self-hypnosis group or the no-treatment control group. In addition, the two groupsdid not differ overall in loneliness (self-hypnosisgroup M = 34.1; No-treatment group M = 38.4),despite the opportunity that the self-hypnosis prac-tice sessions may have provided for greater interper-sonal contact.
Immune Measures: Enumeration of CellPhenotypes
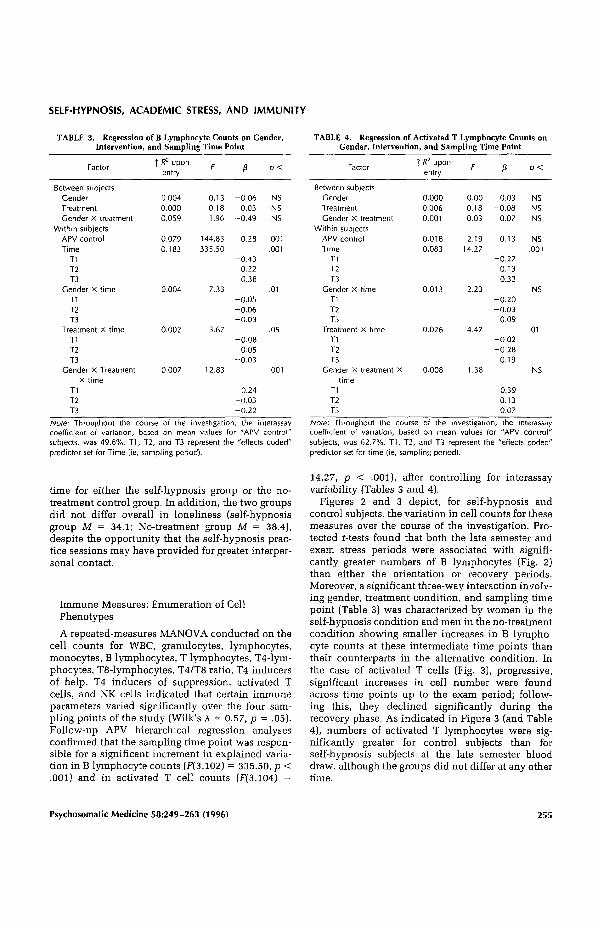
A repeated-measures MANOVA conducted on thecell counts for WBC, granulocytes, lymphocytes,monocytes, B lymphocytes, T lymphocytes, T4-lym-phocytes, T8-lymphocytes, T4/T8 ratio, T4 inducersof help, T4 inducers of suppression, activated Tcells, and NK cells indicated that certain immuneparameters varied significantly over the four sam-pling points of the study (Wilk's A = 0.57, p = .05).Follow-up APV hierarchical regression analysesconfirmed that the sampling time point was respon-sible for a significant increment in explained varia-tion in B lymphocyte counts [F(3,102) = 335.50, p <.001) and in activated T cell counts (F(3,104) =
predictor set for time (ie, sampling period).
14.27, p < .001), after controlling for interassayvariability (Tables 3 and 4).
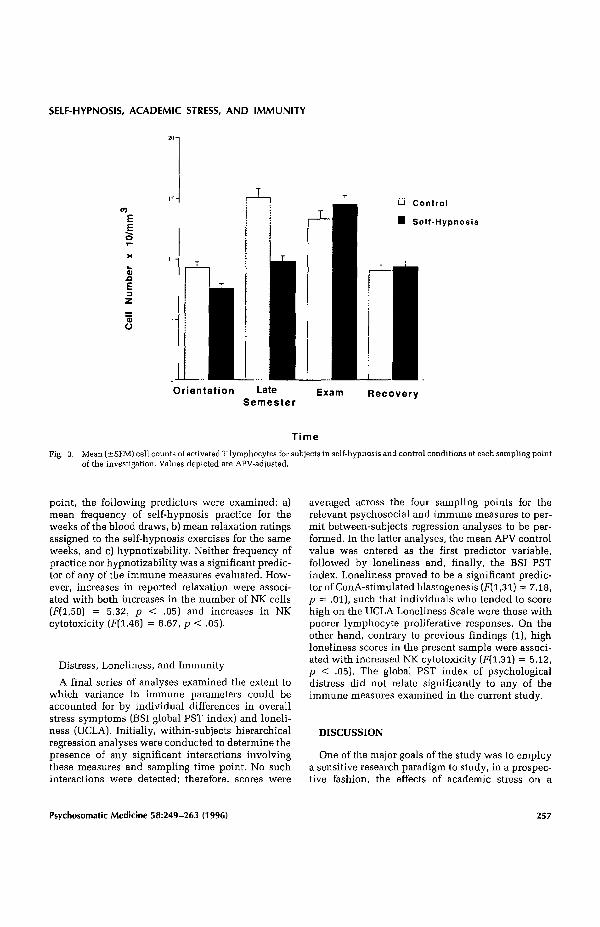
Figures 2 and 3 depict, for self-hypnosis andcontrol subjects, the variation in cell counts for thesemeasures over the course of the investigation. Pro-tected Mests found that both the late semester andexam stress periods were associated with signifi-cantly greater numbers of B lymphocytes (Fig. 2)than either the orientation or recovery periods.Moreover, a significant three-way interaction involv-ing gender, treatment condition, and sampling timepoint (Table 3) was characterized by women in theself-hypnosis condition and men in the no-treatmentcondition showing smaller increases in B lympho-cyte counts at these intermediate time points thantheir counterparts in the alternative condition. Inthe case of activated T cells (Fig. 3), progressive,significant increases in cell number were foundacross time points up to the exam period; follow-ing this, they declined significantly during therecovery phase. As indicated in Figure 3 (and Table4), numbers of activated T lymphocytes were sig-nificantly greater for control subjects than forself-hypnosis subjects at the late semester blooddraw, although the groups did not differ at any othertime.
Psychosomatic Medicine 58:249-263 (1996) 255
W. G. WHITEHOUSE et al.
0).OE3z— 20-
0)
o
GD Control
I Self-Hypnosis
Exam Recovery
TimeFig. 2. Mean (±SEM) cell counts of B lymphocytes for subjects in self-hypnosis and control conditions at each sampling point of the
investigation. Values depicted are APV-adjusted.
Immune Measures: Functional AssaysA repeated-measures MANOVA was computed for
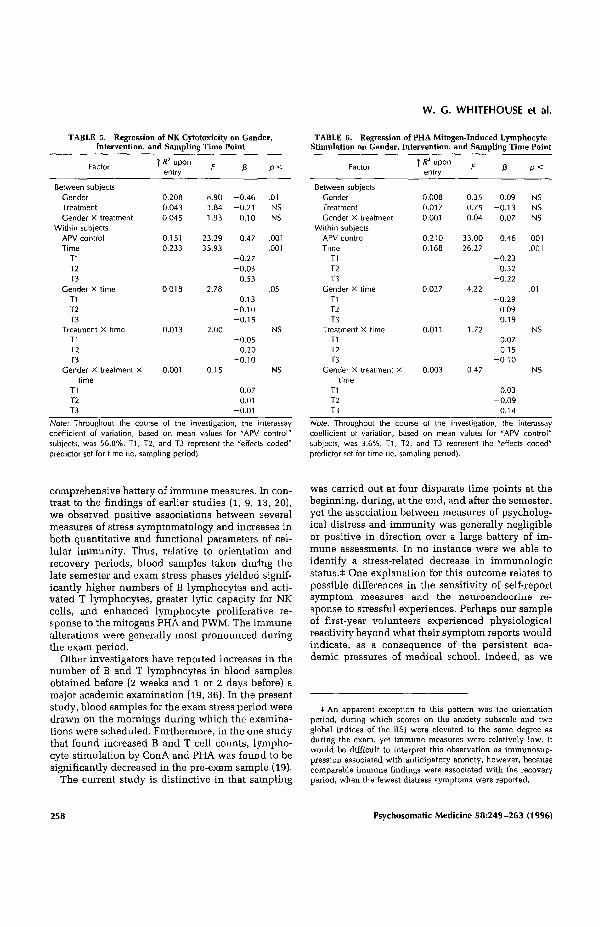
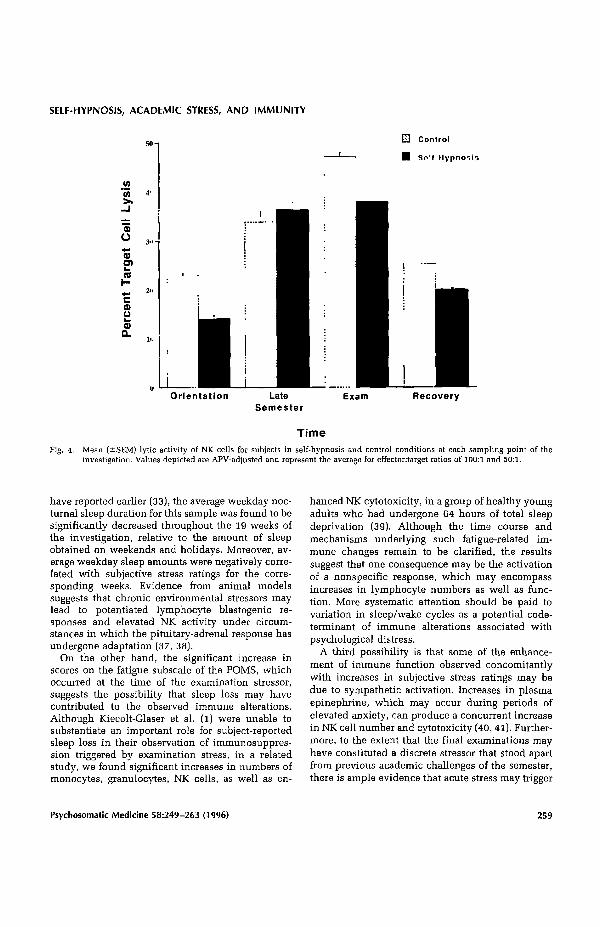
measures of NK cytotoxicity and lymphocyte prolif-eration to the mitogens ConA, PHA, and PWM. Thisanalysis determined that significant changes in lym-phocyte responsivity occurred as a function of thetime during the semester that blood samples wereobtained (Wilk's A = 0.12, p < .001). Thus, asrevealed by APV hierarchical regression analyses(Tables 5 to 8), sampling time point accounted for asignificant amount of the variation in NK activity(F(3,101) = 35.93, p < .001), as well as in theresponse to the mitogens PHA (F(3,103) = 26.27, p <.001) and PWM (F(3,104) = 11.57, p < .001) .Lymphocyte stimulation by ConA did not vary sig-nificantly across sampling periods. Protected i-testsrevealed that NK activity increased significantly ateach time point through the exam stress phase, afterwhich it returned to baseline values (Fig. 4). Overall,NK activity was weaker in women than in men and,in particular, the magnitude of increase in cytotox-icity during the late semester and exam periods wassignificantly lower for women than for men (Table5). The proliferative response of lymphocytes toPHA was significantly elevated during the late se-
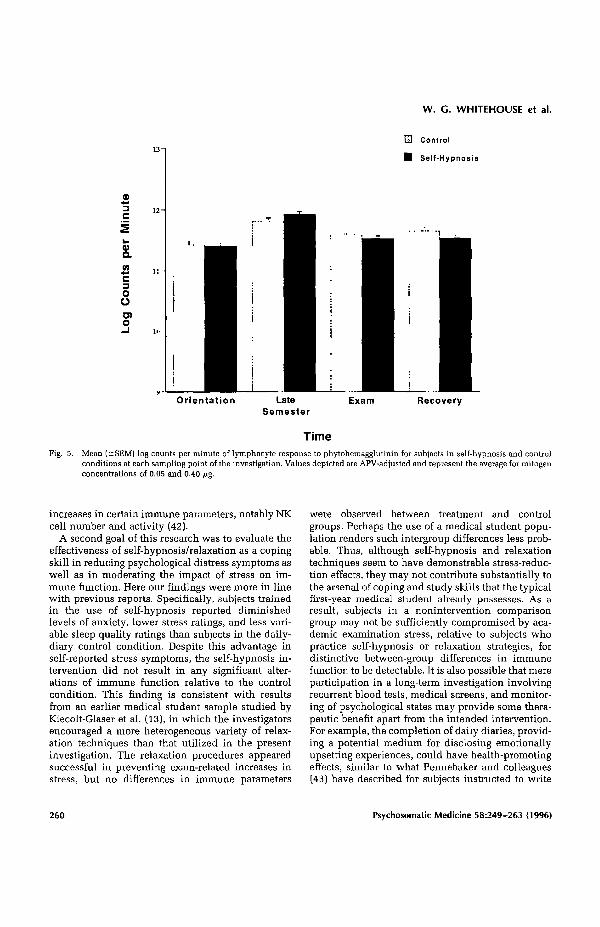
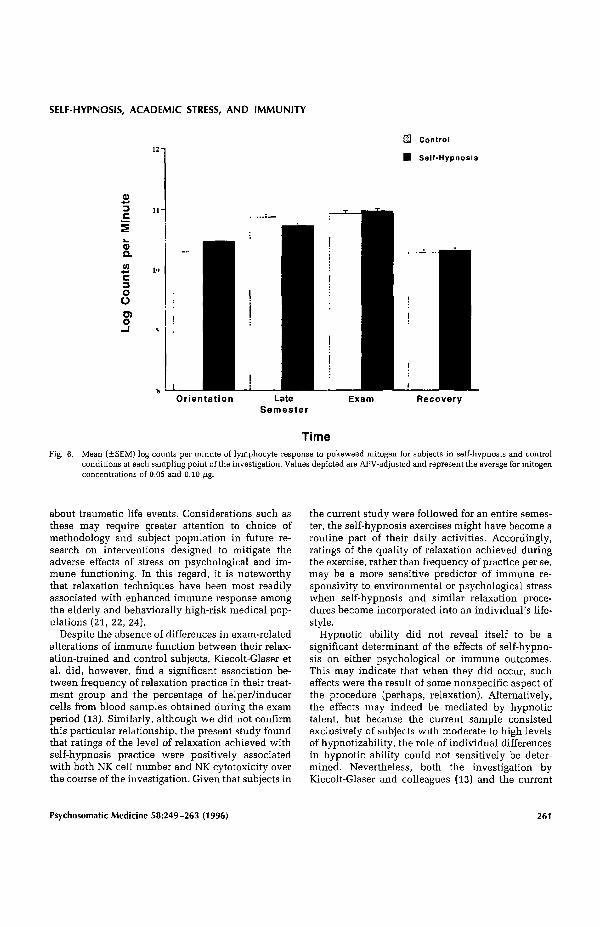
mester phase (Fig. 5), whereas the response to PWMwas significantly augmented both during late semes-ter and exam stress periods (Fig. 6). For both mito-gens, lymphocyte proliferation was greater forwomen than men during the late semester samplingperiod, although no gender-related differences wereevident at other time points (Tables 6 and 7). Therewere no significant differences between subjects inthe self-hypnosis condition and those in the no-treatment condition on any of the functional mea-sures of immunocompetence (Table 8).
Self-Hypnosis Practice, Relaxation,Hypnotizability, and Immunity
Although no group differences emerged as a func-tion of the self-hypnosis intervention, the possibilitywas examined that some aspect(s) of the self-hypno-sis exercises, or individual differences in hypnoticability might be associated with variation in immunesystem parameters. Accordingly, a series of APVhierarchical regression analyses was conducted foreach of the quantitative and functional assays forsubjects in the self-hypnosis condition only. Aftercontrolling for interassay variability and sampling
256 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
COEEo
U Control
• Self-Hypnosis
Orientation Late ExamSemester
Recovery
TimeFig. 3. Mean (±SEM) cell counts of activated T lymphocytes for subjects in self-hypnosis and control conditions at each sampling point
of the investigation. Values depicted are APV-adjusted.
point, the following predictors were examined: a)mean frequency of self-hypnosis practice for theweeks of the blood draws, b) mean relaxation ratingsassigned to the self-hypnosis exercises for the sameweeks, and c) hypnotizability. Neither frequency ofpractice nor hypnotizability was a significant predic-tor of any of the immune measures evaluated. How-ever, increases in reported relaxation were associ-ated with both increases in the number of NK cells(F(l,50) = 5.32, p < .05) and increases in NKcytotoxicity (F(l,46) = 6.67, p < .05).
Distress, Loneliness, and ImmunityA final series of analyses examined the extent to
which variance in immune parameters could beaccounted for by individual differences in overallstress symptoms (BSI global PST index) and loneli-ness (UCLA). Initially, within-subjects hierarchicalregression analyses were conducted to determine thepresence of any significant interactions involvingthese measures and sampling time point. No suchinteractions were detected; therefore, scores were
averaged across the four sampling points for therelevant psychosocial and immune measures to per-mit between-subjects regression analyses to be per-formed. In the latter analyses, the mean APV controlvalue was entered as the first predictor variable,followed by loneliness and, finally, the BSI PSTindex. Loneliness proved to be a significant predic-tor of ConA-stimulatedblastogenesis (F(l,3l) = 7.18,p = .01), such that individuals who tended to scorehigh on the UCLA Loneliness Scale were those withpoorer lymphocyte proliferative responses. On theother hand, contrary to previous findings (1), highloneliness scores in the present sample were associ-ated with increased NK cytotoxicity (F(l,31) = 5.12,p < .05). The global PST index of psychologicaldistress did not relate significantly to any of theimmune measures examined in the current study.
DISCUSSION
One of the major goals of the study was to employa sensitive research paradigm to study, in a prospec-tive fashion, the effects of academic stress on a
Psychosomatic Medicine 58:249-263 (1996) 257
TABLE 5. Regression of NK Cytotoxicity on Gender,Intervention, and Sampling Time Point
W. G. WHITEHOUSE et al.
TABLE 6. Regression of PHA Mitogen-Induced LymphocyteStimulation on Gender, Intervention, and Sampling Time Point
Factor
Between subjectsGenderTreatmentGender x treatment
Within subjectsAPV controlTime
T1T2T3
Gender X timeTlT2T3
Treatment X timeT1T2T3
Gender X treatmenttime
T1T2T3
Note: Throughout thecoefficient of variation,subjects, was 56.8%. Tl
1 R2 uponentry
0.2080.0430.045
0.1510.233
0.018
0.013
X 0.001
F
8.901.841.93
23.2935.93
2.78
2.00
0.15
-0.46-0.21
0.10
0.47
-0.27-0.03
0.53
0.13-0.10-0.15
-0.050.20
-0.10
0.070.01
-0.01
P <
.01NSNS
.001
.001
.05
NS
NS
course of the investigation, the interassaybased on mean values
I, T2, and T3 represent Ipredictor set for time (ie, sampling period).
for "APV control"the "effects coded"
Factor
Between subjectsGenderTreatmentGender x treatment
Within subjectsAPV controlTime
TlT2T3
Gender X timeTlT2T3
Treatment X timeT1T2T3
Gender X treatmenttime
T1T2T3
Note: Throughout thecoefficient of variation,subjects, was 3.6%. Tl
f R2 uponentry
0.0080.0170.001
0.2100.168
0.027
0.011
X 0.003
F
0.350.750.04
33.0026.27
4.22
1.72
0.47
J3
0.09-0.13
0.07
0.46
-0.230.52
-0.22
-0.290 090.19
0.070.15
-0.10
0.03-0.09
0.14
P<
NSNSNS
001.001
.01
NS
NS
course of the investigation, the interassaybased on mean values for "APV
, T2, and T3 represent the "effectspredictor set for time (ie, sampling period!I.
control"coded"
comprehensive battery of immune measures. In con-trast to the findings of earlier studies (1, 9, 13, 20),we observed positive associations between severalmeasures of stress symptomatology and increases inboth quantitative and functional parameters of cel-lular immunity. Thus, relative to orientation andrecovery periods, blood samples taken during thelate semester and exam stress phases yielded signif-icantly higher numbers of B lymphocytes and acti-vated T lymphocytes, greater lytic capacity for NKcells, and enhanced lymphocyte proliferative re-sponse to the mitogens PHA and PWM. The immunealterations were generally most pronounced duringthe exam period.
Other investigators have reported increases in thenumber of B and T lymphocytes in blood samplesobtained before (2 weeks and 1 or 2 days before) amajor academic examination (19, 36). In the presentstudy, blood samples for the exam stress period weredrawn on the mornings during which the examina-tions were scheduled. Furthermore, in the one studythat found increased B and T cell counts, lympho-cyte stimulation by ConA and PHA was found to besignificantly decreased in the pre-exam sample (19).
The current study is distinctive in that sampling
was carried out at four disparate time points at thebeginning, during, at the end, and after the semester,yet the association between measures of psycholog-ical distress and immunity was generally negligibleor positive in direction over a large battery of im-mune assessments. In no instance were we able toidentify a stress-related decrease in immunologicstatus.* One explanation for this outcome relates topossible differences in the sensitivity of self-reportsymptom measures and the neuroendocrine re-sponse to stressful experiences. Perhaps our sampleof first-year volunteers experienced physiologicalreactivity beyond what their symptom reports wouldindicate, as a consequence of the persistent aca-demic pressures of medical school. Indeed, as we
* An apparent exception to this pattern was the orientationperiod, during which scores on the anxiety subscale and twoglobal indices of the BSI were elevated to the same degree asduring the exam, yet immune measures were relatively low. Itwould be difficult to interpret this observation as immunosup-pression associated with anticipatory anxiety, however, becausecomparable immune findings were associated with the recoveryperiod, when the fewest distress symptoms were reported.
258 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
_J
15
O)
u0)Q. .
E3 Control
I Sp'f Hypnosis
Orientation LateSemester
Exam Recovery
TimeFig. 4. Mean (±SEM) lytic activity of NK cells for subjects in self-hypnosis and control conditions at each sampling point of the
investigation. Values depicted are APV-adjusted and represent the average for effector:target ratios of 100:1 and 50:1.
have reported earlier (33), the average weekday noc-turnal sleep duration for this sample was found to besignificantly decreased throughout the 19 weeks ofthe investigation, relative to the amount of sleepobtained on weekends and holidays. Moreover, av-erage weekday sleep amounts were negatively corre-lated with subjective stress ratings for the corre-sponding weeks. Evidence from animal modelssuggests that chronic environmental stressors maylead to potentiated lymphocyte blastogenic re-sponses and elevated NK activity under circum-stances in which the pituitary-adrenal response hasundergone adaptation (37, 38].
On the other hand, the significant increase inscores on the fatigue subscale of the POMS, whichoccurred at the time of the examination stressor,suggests the possibility that sleep loss may havecontributed to the observed immune alterations.Although Kiecolt-Glaser et al. (1) were unable tosubstantiate an important role for subject-reportedsleep loss in their observation of immunosuppres-sion triggered by examination stress, in a relatedstudy, we found significant increases in numbers ofmonocytes, granulocytes, NK cells, as well as en-
hanced NK cytotoxicity, in a group of healthy youngadults who had undergone 64 hours of total sleepdeprivation (39). Although the time course andmechanisms underlying such fatigue-related im-mune changes remain to be clarified, the resultssuggest that one consequence may be the activationof a nonspecific response, which may encompassincreases in lymphocyte numbers as well as func-tion. More systematic attention should be paid tovariation in sleep/wake cycles as a potential code-terminant of immune alterations associated withpsychological distress.
A third possibility is that some of the enhance-ment of immune function observed concomitantlywith increases in subjective stress ratings may bedue to sympathetic activation. Increases in plasmaepinephrine, which may occur during periods ofelevated anxiety, can produce a concurrent increasein NK cell number and cytotoxicity (40, 41). Further-more, to the extent that the final examinations mayhave constituted a discrete stressor that stood apartfrom previous academic challenges of the semester,there is ample evidence that acute stress may trigger
Psychosomatic Medicine 58:249-263 (1996) 259
Q.
(0<-•3oOo
W. G. WHITEHOUSE et al.
E3 Control
I Self-Hypnosis
Orientation LateSemester
Exam Recovery
TimeFig. 5. Mean (iSEM) log counts per minute of lymphocyte response to phytohemagglutinin for subjects in self-hypnosis and control
conditions at each sampling point of the investigation. Values depicted are APV-adjusted and represent the average for mitogenconcentrations of 0.05 and 0.40 /xg.
increases in certain immune parameters, notably NKcell number and activity (42).
A second goal of this research was to evaluate theeffectiveness of self-hypnosis/relaxation as a copingskill in reducing psychological distress symptoms aswell as in moderating the impact of stress on im-mune function. Here our findings were more in linewith previous reports. Specifically, subjects trainedin the use of self-hypnosis reported diminishedlevels of anxiety, lower stress ratings, and less vari-able sleep quality ratings than subjects in the daily-diary control condition. Despite this advantage inself-reported stress symptoms, the self-hypnosis in-tervention did not result in any significant alter-ations of immune function relative to the controlcondition. This finding is consistent with resultsfrom an earlier medical student sample studied byKiecolt-Glaser et al. (13), in which the investigatorsencouraged a more heterogeneous variety of relax-ation techniques than that utilized in the presentinvestigation. The relaxation procedures appearedsuccessful in preventing exam-related increases instress, but no differences in immune parameters
were observed between treatment and controlgroups. Perhaps the use of a medical student popu-lation renders such intergroup differences less prob-able. Thus, although self-hypnosis and relaxationtechniques seem to have demonstrable stress-reduc-tion effects, they may not contribute substantially tothe arsenal of coping and study skills that the typicalfirst-year medical student already possesses. As aresult, subjects in a nonintervention comparisongroup may not be sufficiently compromised by aca-demic examination stress, relative to subjects whopractice self-hypnosis or relaxation strategies, fordistinctive between-group differences in immunefunction to be detectable. It is also possible that mereparticipation in a long-term investigation involvingrecurrent blood tests, medical screens, and monitor-ing of psychological states may provide some thera-peutic benefit apart from the intended intervention.For example, the completion of daily diaries, provid-ing a potential medium for disclosing emotionallyupsetting experiences, could have health-promotingeffects, similar to what Pennebaker and colleagues(43) have described for subjects instructed to write
260 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
E3 Control
B Self-Hypnosis
0)
aW
oOO)
o
Recovery
TimeFig. 6. Mean (±SEM) log counts per minute of lymphocyte response to pokeweed mitogen for subjects in self-hypnosis and control
conditions at each sampling point of the investigation. Values depicted are APV-adjusted and represent the average for mitogenconcentrations of 0.05 and 0.10 /xg.
about traumatic life events. Considerations such asthese may require greater attention to choice ofmethodology and subject population in future re-search on interventions designed to mitigate theadverse effects of stress on psychological and im-mune functioning. In this regard, it is noteworthythat relaxation techniques have been most readilyassociated with enhanced immune response amongthe elderly and behaviorally high-risk medical pop-ulations (21, 22, 24).
Despite the absence of differences in exam-relatedalterations of immune function between their relax-ation-trained and control subjects, Kiecolt-Glaser etal. did, however, find a significant association be-tween frequency of relaxation practice in their treat-ment group and the percentage of helper/inducercells from blood samples obtained during the examperiod (13). Similarly, although we did not confirmthis particular relationship, the present study foundthat ratings of the level of relaxation achieved withself-hypnosis practice were positively associatedwith both NK cell number and NK cytotoxicity overthe course of the investigation. Given that subjects in
the current study were followed for an entire semes-ter, the self-hypnosis exercises might have become aroutine part of their daily activities. Accordingly,ratings of the quality of relaxation achieved duringthe exercise, rather than frequency of practice per se,may be a more sensitive predictor of immune re-sponsivity to environmental or psychological stresswhen self-hypnosis and similar relaxation proce-dures become incorporated into an individual's life-style.
Hypnotic ability did not reveal itself to be asignificant determinant of the effects of self-hypno-sis on either psychological or immune outcomes.This may indicate that when they did occur, sucheffects were the result of some nonspecific aspect ofthe procedure (perhaps, relaxation). Alternatively,the effects may indeed be mediated by hypnotictalent, but because the current sample consistedexclusively of subjects with moderate to high levelsof hypnotizability, the role of individual differencesin hypnotic ability could not sensitively be deter-mined. Nevertheless, both the investigation byKiecolt-Glaser and colleagues (13) and the current
Psychosomatic Medicine 58:249-263 (1996) 261
W. G. WHITEHOUSE et al.
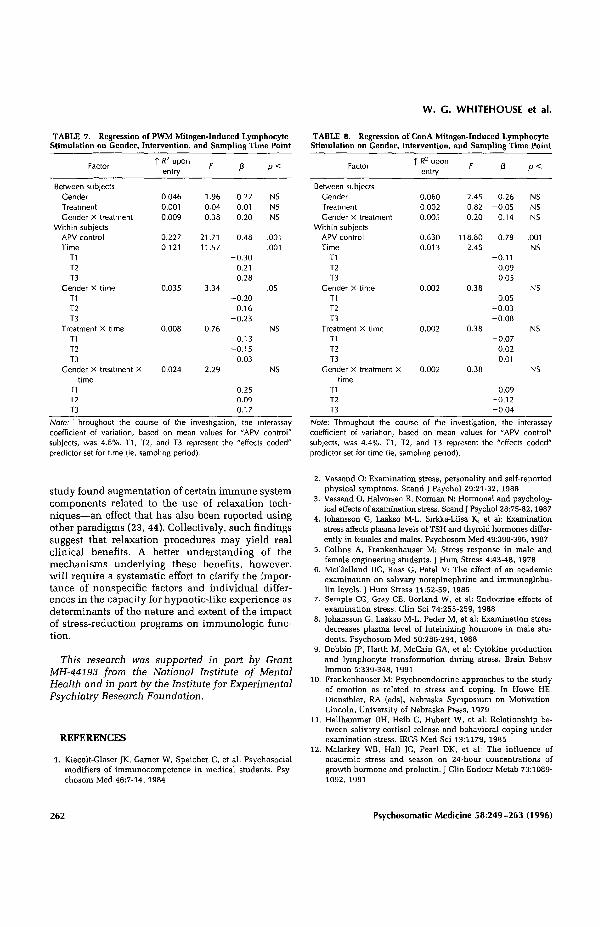
TABLE 7. Regression of PWM Mitogen-Induced LymphocyteStimulation on Gender, Intervention, and Sampling Time Point
TABLE 8. Regression of ConA Mitogen-Induced LymphocyteStimulation on Gender, Intervention, and Sampling Time Point
Factor
Between subjectsGenderTreatmentGender X treatment
Within subjectsAPV controlTime
TIT2T3
Gender X timeTIT2T3
Treatment x timeTIT2T3
Gender X treatment xtime
T1T2T3
t K2 uponentry
0.0460.0010.009
0.2270.121
0.035
0.008
0.024
F
1.960.040.38
21.7111.57
3.34
0.76
2.29
P
0.220.010.20
0.48
-0.300.210.28
-0.200.16
-0.23
0.13-0.15
0.03
0.250.090.17
P <
NSNSNS
.001
.001
.05
NS
NS
Factor
Between subjectsGenderTreatmentGender x treatment
Within subjectsAPV controlTime
TIT2T3
Gender X timeT1T2T3
Treatment X timeT1T2T3
Gender x treatment Xtime
T1T2T3
I R2 uponentry
0.0600.0020.005
0.6300.013
0.002
0.002
0.002
F
2.450.820.20
118.802.45
0.38
0.38
0.38
"CD
0.26-0.05
0.14
0.79
-0.110.090.05
0.05-0.03-0.08
-0.070.020.01
0.09-0.12-0.04
P<
NSNSNS
.001NS
NS
NS
NS
Note: Throughout the course of the investigation, the interassaycoefficient of variation, based on mean values for "APV control"subjects, was 4.8%. T I , T2, and T3 represent the "effects coded"predictor set for time (ie, sampling period).
Note: Throughout the course of the investigation, the interassaycoefficient of variation, based on mean values for "APV control"subjects, was 4.4%. T1, T2, and T3 represent the "effects coded"predictor set for time (ie, sampling period).
study found augmentation of certain immune systemcomponents related to the use of relaxation tech-niques—an effect that has also been reported usingother paradigms (23, 44). Collectively, such findingssuggest that relaxation procedures may yield realclinical benefits. A better understanding of themechanisms underlying these benefits, however,will require a systematic effort to clarify the impor-tance of nonspecific factors and individual differ-ences in the capacity for hypnotic-like experience asdeterminants of the nature and extent of the impactof stress-reduction programs on immunologic func-tion.
This research was supported in part by GrantMH-44193 from the National Institute of MentalHealth and in part by the Institute for ExperimentalPsychiatry Research Foundation.
REFERENCES
1. Kiecolt-Glaser JK, Garner W, Speicher C, et al: Psychosocialmodifiers of immunocompetence in medical students. Psy-chosom Med 46:7-14, 1984
3. Vassend O, Halvorsen R, Norman N: Hormonal and psycholog-ical effects of examination stress. Scand J Psychol 28:75-82,1987
4. Johansson G, Laakso M-L, Sirkka-Liisa K, et al: Examinationstress affects plasma levels of TSH and thyroid hormones differ-ently in females and males. Psychosom Med 49:390-396, 1987
5. Collins A, Frankenhauser M: Stress response in male andfemale engineering students. J Hum Stress 4:43-48, 1978
6. McClelland DC, Ross G, Patel V: The effect of an academicexamination on salivary norepinephrine and immunoglobu-lin levels. J Hum Stress 11:52-59, 1985
8. Johansson G, Laakso M-L, Peder M, et al: Examination stressdecreases plasma level of luteinizing hormone in male stu-dents. Psychosom Med 50:286-294, 1988
9. Dobbin JP, Harth M, McCain GA, et al: Cytokine productionand lymphocyte transformation during stress. Brain BehavImmun 5:339-348, 1991
10. Frankenhauser M: Psychoendocrine approaches to the studyof emotion as related to stress and coping. In Howe HE,Dienstbier, RA (eds), Nebraska Symposium on Motivation.Lincoln, University of Nebraska Press, 1979
11. Hellhammer DH, Heib C, Hubert W, et al: Relationship be-tween salivary cortisol release and behavioral coping underexamination stress. IRCS Med Sci 13:1179, 1985
12. Malarkey WB, Hall JC, Pearl DK, et al: The influence ofacademic stress and season on 24-hour concentrations ofgrowth hormone and prolactin. J Clin Endocr Metab 73:1089-1092, 1991
262 Psychosomatic Medicine 58:249-263 (1996)
SELF-HYPNOSIS, ACADEMIC STRESS, AND IMMUNITY
13. Kiecolt-Glaser JK, Glaser R, Strain EC, et al: Modulation ofcellular immunity in medical students. J Behav Med 9:5-21,1986
14. Glaser R, Rice J, Speicher CE, et al: Stress depresses interferonproduction by leukocytes concomitant with a decrease innatural killer cell activity. Behav Neurosci 100:675-678, 1986
15. Kiecolt-Glaser JK, Speicher CE, Holliday JE, et al: Stress andthe transformation of lymphocytes by Epstein-Barr vims. JBehav Med 7:1-12, 1984
16. Glaser R, Rice J, Sheridan J, et al: Stress-related immunesuppression: Health implications. Brain Behav Immun 1:7-20,1987
17. Glaser R, Kennedy S, Lafuse WP, et al: Psychological stress-induced modulation of interleukin 2 receptor gene expressionand interleukin 2 production in peripheral blood leukocytes.Arch Gen Psychiatry 47:707-712, 1990
18. Glaser R, Kiecolt-Glaser JK, Speicher C, et al: Stress, loneli-ness, and changes in herpesvirus latency. J Behav Med 8:249-260, 1985
19. Dorian B, Garfinkel P, Brown G, et al: Aberrations in lympho-cyte subpopulations and function during psychologicalstress. Clin Exp Immunol 50:132-138, 1982
20. Halvorsen R, Vassend O: Effects of examination stress onsome cellular immunity functions. J Psychosom Res 31:693-701, 1987
21. Kiecolt-Glaser JK, Glaser R, Williger D, et al: Psychosocialenhancement of immunocompetence in a geriatric popula-tion. Health Psychol 4:25-41, 1985
23. Green RG, Green ML: Relaxation increases salivary immuno-globulin A. Psychol Rep 61:623-629, 1987
24. Baggett HL, Antoni MH, August SM, et al: The effects offrequency of relaxation practice on immune markers in anHIV-1 high risk group. Psychosom Med 52:243, 1990
25. Schleifer SJ, Eckholdt HM, Cohen J, et al: Analysis of partialvariance (APV) as a statistical approach to control day to dayvariation in immune assays. Brain Behav Immun 7:243-252,1993
26. McNair DM, Lorr M, Druppleman LF: EITS Manual for theProfile of Mood States. San Diego, Educational and IndustrialTest Services, 1971
27. Derogatis LR, Spencer PM: The Brief Symptom Inventory(BSI): Administration, Scoring, and Procedures Manual—I.Baltimore, MD, Clinical Psychometric Research, 1982
28. Russell D, Peplau LA, Cutrona CE: The revised UCLA Lone-liness Scale: Concurrent and discriminant validity evidence. JPers Soc Psychol 39:472-480, 1980
29. Shor RE, Orne EC: Harvard Group Scale of Hypnotic Suscep-tibility, Form A. Palo Alto, CA, Consulting PsychologistsPress, 1962
30. Shor RE: Inventory of Self-Hypnosis, Form A. Palo Alto, CA,Consulting Psychologists Press, 1978
31. Shor RE, Easton RD: A preliminary report on research com-paring self- and hetero-hypnosis. Am J Clin Hypnosis 16:37-44, 1973
32. Johnson LS: Self-hypnosis: Behavioral and phenomenologicalcomparisons with heterohypnosis. Int J Clin Exp Hypnosis27:240-264, 1979
33. Dinges DF, Orne EC, Keller SE, et al: Inadequate sleep andstress during the first year of medical school. Sleep Res20:133, 1991
34. Keller SE, Schleifer SJ, Sherman J, et al: Comparison of asimplified whole blood and isolated lymphocyte stimulationtechnique. Immunol Commun 10:417-431, 1981
35. Cohen J, Cohen P: Applied Multiple Regression/CorrelationAnalysis for the Behavioral Sciences. Hillsdale, NJ, Erlbaum,1983.
36. Fittschen B, Schulz K-H, Raedler A, et al: Changes of immu-nological parameters in healthy subjects under examinationstress. Int J Neurosci 51:241-242, 1990
37. Irwin MR, Segal DS, Hauger RL, et al: Individual behavioraland neuroendocrine differences in responsiveness to audio-genic stress. Pharmacol Biochem Behav 32:913-917, 1989
39. Dinges DF, Douglas SD, Zaugg L, et al: Leukocytosis andnatural killer cell function parallel neurobehavioral fatigueinduced by 64 hours of sleep deprivation. J Clin Invest93:1930-1939, 1994
40. Tonnesen E, Brinklov MM, Christensen NJ, et al: Naturalkiller cell activity and lymphocyte function during and aftercoronary artery bypass grafting in relation to the endocrinestress response. Anesthesiology 67:526-533, 1987
41. Tonnesen E, Christensen NJ, Brinklov MM: Natural killer cellactivity during cortisol and adrenaline infusion in healthyvolunteers. Eur J Clin Invest 17:497-503, 1987
42. Kemeny ME, Solomon GF, Morley JE, et al: Psychoneuroim-munology. In Nemeroff CB (ed), Neuroendocrinology. BocaRaton, FL, CRC Press, 1992:563-591
43. Pennebaker JW, Kiecolt-Glaser JK, Glaser R: Disclosure oftraumas and immune function: Health implications for psy-chotherapy. J Consult Clin Psychol 56:239-245, 1988
44. Jasnoski ML, Kugler J: Relaxation, imagery, and neuroimmu-nomodulation. Ann NY Acad Sci 496:722-730, 1987














![Hypnosis William Hewitt - Hypnosis for Beginners[2003]](https://static.documents.pub/doc/80x56/552115f3497959734d8b4612/hypnosis-william-hewitt-hypnosis-for-beginners2003.jpg)






