9 Psychosocial interventions for the treatment of perinatal depression Cindy-Lee Dennis, PhD, Professor and Canada Research Chair in Perinatal Community Health, Shirley Brown Chair in Women’s Mental Health Research, Women’s College Research Institute * Lawrence S. Bloomberg, Faculty of Nursing, University of Toronto, Canada Keywords: postpartum depression social support support group peer support non-directive counselling home-based interventions randomised-controlled trials systematic review Epidemiological investigations and meta-analyses of predictive studies have consistently demonstrated the importance of psy- chosocial variables as postpartum depression risk factors. To address this, several psychosocial treatment strategies have been evaluated for the treatment of postpartum depression. The pur- pose of this paper is to determine the current state of scientific knowledge related to the treatment of postpartum depression from a psychosocial perspective. Thirteen trials were included in the review that evaluated the following interventions: peer sup- port, partner support, non-directive counselling, home visits by mental health nurses, and collaborative models of care. Owing to methodological limitations of the included trials, the effectiveness of most psychosocial approaches for the treatment of postpartum depression is equivocal. Large, multisite randomised-controlled trials are needed to compare different treatment approaches, examine the effectiveness of individual treatment components, and determine which treatments are most useful for women with different risk factors or clinical presentations of postpartum depression. Ó 2013 Published by Elsevier Ltd. * University of Toronto,155 College Street, Room 280, Toronto, ON, M5T 1P8, Canada. Tel.: þ1 416 946 8608; Fax: þ1 416 978 8222. E-mail address: [email protected]. Contents lists available at ScienceDirect Best Practice & Research Clinical Obstetrics and Gynaecology journal homepage: www.elsevier.com/locate/bpobgyn 1521-6934/$ – see front matter Ó 2013 Published by Elsevier Ltd. http://dx.doi.org/10.1016/j.bpobgyn.2013.08.008 Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111
Transcript
Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111
Contents lists available at ScienceDirect
Best Practice & Research ClinicalObstetrics and Gynaecology
Psychosocial interventions for the treatmentof perinatal depression
Cindy-Lee Dennis, PhD, Professor and Canada Research Chairin Perinatal Community Health, Shirley Brown Chair inWomen’s Mental Health Research, Women’s College ResearchInstitute *
Lawrence S. Bloomberg, Faculty of Nursing, University of Toronto, Canada
1521-6934/$ – see front matter � 2013 Publishedhttp://dx.doi.org/10.1016/j.bpobgyn.2013.08.008
Epidemiological investigations and meta-analyses of predictivestudies have consistently demonstrated the importance of psy-chosocial variables as postpartum depression risk factors. Toaddress this, several psychosocial treatment strategies have beenevaluated for the treatment of postpartum depression. The pur-pose of this paper is to determine the current state of scientificknowledge related to the treatment of postpartum depressionfrom a psychosocial perspective. Thirteen trials were included inthe review that evaluated the following interventions: peer sup-port, partner support, non-directive counselling, home visits bymental health nurses, and collaborative models of care. Owing tomethodological limitations of the included trials, the effectivenessof most psychosocial approaches for the treatment of postpartumdepression is equivocal. Large, multisite randomised-controlledtrials are needed to compare different treatment approaches,examine the effectiveness of individual treatment components,and determine which treatments are most useful for women withdifferent risk factors or clinical presentations of postpartumdepression.
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–11198
Introduction
The cause of postpartum depression is multifactorial [1,2]; however, meta-analytic findingsconsistently highlight the importance of psychosocial variables, such as the lack of social support,marital conflict, and stressful life events. Analyses of social support variables in predictive studiesclearly show a significant increase in the risk of postpartum depression in womenwho (1) do not havesomeone to talk openlywith who has shared and understood a similar problem [3]; (2) lack an intimateconfidant or friend [3–6]; (3) do not receive support without having to ask for it [3]; and (4) feel sociallyisolated [7]. In addition, women who report marital difficulties have been found to be at risk ofdeveloping postpartum depression [2,8]. Depressed mothers are more likely to be dissatisfied with thesupport received from their partners [9], feel communication is poor [4], perceive their partner asuncaring [10], report a decline in the affection and cohesion in their relationship [11], and find adiscrepancy between their expectations and later experiences of closeness to their partner [12–14].Higher levels of postpartum depressive symptomatology have been linked to perceived stress duringpregnancy [15,16], childcare stressors [17–19], and the number of stressful life events since delivery[17,20]. To address this issue, a variety of psychosocial interventions with the aim of enhancing theavailability or perception of support have been developed to treat postpartum depression [21]. Thepurpose of this paper is to determine the current state of scientific knowledge related to the treatmentof postpartum depression from a psychosocial perspective.
Theoretical underpinnings of psychosocial interventions
Social relationships and social support can affect mental health through several pathways. Membersof a social network can exert a salutary influence on mental health by role modelling health-relevantbehaviours [22]. Integration in a social network might also directly produce positive psychologicalstates, including sense of purpose, belonging, and recognition of self-worth [23]. These positive states,in turn, might benefit mental health because of an increased motivation for self-care, as well as themodulation of the neuroendocrine response to stress [23]. Being part of a social network enhances thelikelihood of accessing various forms of social support, which in turn protects against distress [24].Social support may also act on several different points in the pathway between stressful life events andmental health. The perceived availability of social support in the face of a stressful event may lead to amore benign appraisal of the situation, thereby preventing a cascade of ensuing negative emotionaland behavioural responses [25]. Perceived or received support may either reduce the negativeemotional reaction to a stressful event or dampen the physiologic, behavioural response to stress, orboth [26]. These findings are consistent with Thoits’s [27] theoretical model of the mechanismsthrough which social ties affect physical and psychological wellbeing. According to Thoits, sevendifferent psychosocial mechanisms link aspects of social relationships to physical and emotional well-being. The theorised seven mechanisms are as follows: social influence and social comparison; socialcontrol; role-based purpose and meaning (mattering); self-esteem; sense of control; belonging andcompanionship; and perceived support availability.
Thoits [27] suggests that the effectiveness of social support as a stress buffer requires actuallyreceived or enacted support, and is based on specific combinations of source and type of support.Primary group members are individuals who have not had past personal experience with the healthproblem or stressor that the distressed person is currently facing (experientially dissimilar), andsecondary groupmembers are individuals who have experienced or are experiencing a similar stressor(experientially similar). Thoits hypothesises that emotional support (e.g. love, caring, and sympathy)and instrumental support are likely to be the most effective stress buffers when coming from signif-icant others, whereas informational and appraisal support (e.g. validation of feelings, advice, and rolemodelling) are most helpful coming from similar others. The provision of emotional support is likely tobemore effective coming from significant others given such groupmembers’ lives are also disrupted bythe stressor, and their attempts at providing informational support may be ineffective, as they are lesslikely to have direct experience. In comparison, secondary group members or similar others may bebetter sources of informational support, and they may be better able to provide empathy, rolemodelling, and coping assistance given their past or current experience.
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111 99
Psychosocial treatment interventions
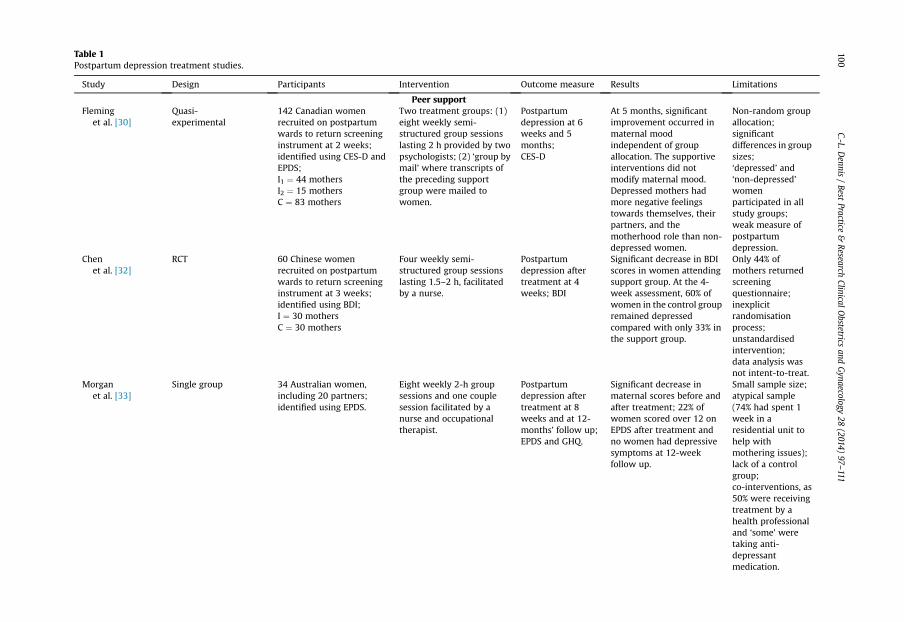
Several psychosocial treatment strategies have been evaluated for the treatment of postpartumdepression based on the importance of psychosocial variables and the theoretical premise that sup-portive relationships during the perinatal period could reduce depressive symptoms and enhance amother’s feeling of wellbeing (Table 1).
Peer support
Several researchers have recommended the provision of peer (mother-to-mother) support in agroup modality for women experiencing postpartum depression [28,29]. The results, however, fromthree investigations are equivocal. In a Canadian study, the effect of a support group was evaluatedthrough the recruitment of mothers on the second postpartum day who were asked to complete andreturn via mail a set of mood scales during the first 2 weeks postpartum [30]. Of the 1081 ques-tionnaires distributed over a 3-year period, 781 (72%) were returned, with 156 mothers scoring abovethe depression threshold of 35 on the Current Experience Scale, and either above 13 on the EdinburghPostnatal Depression Scale (EPDS) or 21 on the Multiple Affect Adjective Checklist. Seventy-sixmothers with depressive symptomatology (48% of all depressed mothers) and 76 non-depressedmothers were recruited into the study. Participants were non-randomly allocated to either a sup-port group (eight weekly 2-h semi-structured group sessions facilitated by two psychologists;n ¼ 44), a ‘Group-by-Mail’ group (to determine whether the support group effects were due to socialinteractions with other women; participants in this group received scripts via mail that were adaptedfrom the support group sessions; n ¼ 15), or a control group (usual postpartum care; n ¼ 83). Par-ticipants completed the Center for Epidemiological Studies Depression Scale at 6 and 20 weekspostpartum, and were categorised as either depressed or non-depressed. The analysis of variance forsocial support compared with the control group at the 6-week assessment showed that ‘depressed’women had significantly more negative feelings about themselves, their partners, and motherhoodthan non-depressed mothers. At 20 weeks, although over 90% of the women in the support groupreported that the intervention was beneficial, depressed mothers showed significantly lessimprovement in self-image than those in the control group, and some underwent deterioration intheir feelings. Although most participants experienced an improvement in mood from 2–20 weekspostpartum regardless of group allocation, the support group interventions did not significantlyalleviate maternal depression and were detrimental to depressed mothers’ self-image. Study limi-tations included poor measure of postpartum depression, non-random group allocation, unequalgroup numbers, and a significant difference between study groups in relation to maternal age. Inaddition, theoretical limitations also existed. Research suggests that depressed individuals prefer tobe with others who are depressed and that they feel worse after speaking with non-depressedpeople, but not after speaking with similar others [31]. As such, the finding that depressed womenfelt worse after the support group meetings is not unexpected.
On the basis of this theoretical principle, a Chinese trial evaluated the effect of weekly supportgroup meetings for women who were all experiencing postpartum depression [32]. Mothers wererecruited in hospital on the second or third day postpartum to complete and return via mail the BeckDepression Inventory (BDI) at 3 weeks postpartum. Eighty-five per cent of the mothers approachedagreed to participate (n ¼ 941), with 414 returning the completed BDI. Sixty mothers with BDI scoresabove 9 were randomised to either a support group (four weekly semi-structured sessions facilitatedby a nurse, each 1.5–2 h in duration; n ¼ 30) or a control group (usual postpartum care; n ¼ 30). At the4-week assessment, mothers who attended the support sessions had significantly decreased BeckDepression Inventory scores thanmothers in the control group. In particular, 60% (n¼ 18) of mothers inthe control group had depressive symptomatology compared with only 33% (n ¼ 9) of mothers in thesupport group. Although this is the first randomised-controlled trial to evaluate the effectiveness ofsupport groups, several limitations existed, including the following: (1) only 44% of mothers returnedthe screening questionnaire; (2) inexplicit randomisation method; (3) of the 115 mothers who met theinclusion criteria, only 60 were randomised, and it is unknown what happened to the other 55 po-tential participants; (4) unstandardised intervention as two support groups met for five sessions
Table 1Postpartum depression treatment studies.
Study Design Participants Intervention Outcome measure Results Limitations
Peer supportFleming
et al. [30]Quasi-experimental
142 Canadian womenrecruited on postpartumwards to return screeninginstrument at 2 weeks;identified using CES-D andEPDS;I1 ¼ 44 mothersI2 ¼ 15 mothersC ¼ 83 mothers
Two treatment groups: (1)eight weekly semi-structured group sessionslasting 2 h provided by twopsychologists; (2) ‘group bymail’ where transcripts ofthe preceding supportgroup were mailed towomen.
Postpartumdepression at 6weeks and 5months;CES-D
At 5 months, significantimprovement occurred inmaternal moodindependent of groupallocation. The supportiveinterventions did notmodify maternal mood.Depressed mothers hadmore negative feelingstowards themselves, theirpartners, and themotherhood role than non-depressed women.
Non-random groupallocation;significantdifferences in groupsizes;‘depressed’ and‘non-depressed’womenparticipated in allstudy groups;weak measure ofpostpartumdepression.
Chenet al. [32]
RCT 60 Chinese womenrecruited on postpartumwards to return screeninginstrument at 3 weeks;identified using BDI;I ¼ 30 mothersC ¼ 30 mothers
Four weekly semi-structured group sessionslasting 1.5–2 h, facilitatedby a nurse.
Postpartumdepression aftertreatment at 4weeks; BDI
Significant decrease in BDIscores in women attendingsupport group. At the 4-week assessment, 60% ofwomen in the control groupremained depressedcompared with only 33% inthe support group.
Only 44% ofmothers returnedscreeningquestionnaire;inexplicitrandomisationprocess;unstandardisedintervention;data analysis wasnot intent-to-treat.
Morganet al. [33]
Single group 34 Australian women,including 20 partners;identified using EPDS.
Eight weekly 2-h groupsessions and one couplesession facilitated by anurse and occupationaltherapist.
Postpartumdepression aftertreatment at 8weeks and at 12-months’ follow up;EPDS and GHQ.
Significant decrease inmaternal scores before andafter treatment; 22% ofwomen scored over 12 onEPDS after treatment andno women had depressivesymptoms at 12-weekfollow up.
Small sample size;atypical sample(74% had spent 1week in aresidential unit tohelp withmothering issues);lack of a controlgroup;co-interventions, as50% were receivingtreatment by ahealth professionaland ‘some’ weretaking anti-depressantmedication.
C.-L.Dennis
/Best
Practice&
ResearchClinical
Obstetrics
andGynaecology
28(2014)
97–111
100
Dennis [34] Pilot RCT; randomallocation using sealedenvelopes; intent-to-treat.
42 Canadian womenscreened by public healthnurses duringimmunisation clinic;identified using EPDS;I ¼ 20 mothersC ¼ 22 mothers
Telephone-based supportfrom a mother recruitedfrom the community whopreviously experiencedpostpartum depression andreceived a 4-h trainingsession.
Postpartumdepression at 4 and8 weeks afterrandomisation;EPDS.
Significant groupdifferences in probablemajor postpartumdepression (EPDS >12) atall time periods. At the 4-week assessment, 40.9% ofwomen in the control groupscored over 12 on the EPDScompared with only 10% inthe peer support group;similar findings at 8 weeks.
Small sample size.
Letourneauet al. [35]
RCT;random allocationusing sealed envelopes.
60 Canadian women withEPDS over 12 and healthyinfant less than 9 months;I ¼ 27 mothersC ¼ 33 mothers
Home visits and telephonecalls for 12 weeks by peerswho were mothers that hadrecovered from postpartumdepression for 2 years ormore.
Postpartumdepression at 6 and12 weeks afterrandomisation;EPDS.
At 12 weeks, a significantdifference was found inEPDS scores favouring thecontrol group (P ¼ 0.04).
met the DSM-IV criteria formajor depressive disorderwith postpartum onset;I ¼ 16 mothersC ¼ 13 mothers
Seven psycho-educationalvisits with a psychiatristduring which the mother’spartner participated in fourof the seven sessions.
Postpartumdepression aftertreatment and 4-week follow up;EPDS
Immediately after theintervention, no significantgroup differences wereobserved in mean EPDSscores (P ¼ 0.20). At the 4-week follow up, significantgroup differences in meanEPDS scores favouring theintervention group(M ¼ 8.6, SD ¼ 5.2 vM ¼ 14.7, SD ¼ 7.2,P ¼ 0.013).
Small sample size;significant groupdifference inbaselinecharacteristicsrelated to theirpartners’ marriageappraisals;inexplicitrandomisationprocess.
Non-directive counsellingHolden
et al. [37]RCT;group allocation basedon random numbers.
50 UK women;community-based EPDSscreening at 6 weeks with asecond screening at 13weeks using psychiatricinterview;I ¼ 26 mothersC ¼ 24 mothers
Eight weekly counsellingvisits at home by healthvisitors trained in non-directive counselling.
Postpartumdepression at 13weeks afterrandomisation;EPDS and clinicalinterview.
Significant groupdifferences. According toRDC criteria, 18 (69%) of the26 depressed women in thecounselled group had fullyrecovered compared withonly nine (38%) of the 24women in the controlgroup.
Small sample size;3 women in eachgroup wereconsidered to havetaken anti-depressantmedication at atherapeutic level.
(continued on next page)
C.-L.Dennis
/Best
Practice&
ResearchClinical
Obstetrics
andGynaecology
28(2014)
97–111
101
Table 1 (continued)
Study Design Participants Intervention Outcome measure Results Limitations
Wickberg andHwang [38]
RCT 31 Swedish women;two-stage population-based screening at 8 and 12weeks using EPDS;I ¼ 15 mothersC ¼ 16 mothers
Six weekly 1-h counsellingvisits at home by nursestrained in non-directivecounselling.
Postpartumdepression at 6weeks afterrandomisation;modified MADRS.
Significant groupdifferences. Twelve (80%) of15 women with majordepression in the studygroup were fully recoveredafter the interventioncompared with four (25%)of 16 in the control group.
Small sample size;inexplicitrandomisationprocess.
Cooper et al. [39] RCT;group allocation basedon drawing colouredballs.
193 UK womenscreened with a mailedEPDS;identified using DSM-III-Rcriteria;I1 ¼ 43 mothersI2 ¼ 50 mothersI3 ¼ 48 mothersC ¼ 52 mothers
Three treatments: (1)cognitive–behaviouraltherapy; (2)psychodynamic therapy; or(3) non-directivecounselling providedweekly at home from 8 to18 weeks postpartum.
Postpartumdepression at 18, 36and 72 weeks and 5years’ follow up;EPDS and clinicalinterview.
Significant improvementsin all three treatmentgroups. Mean EPDS scorefor the counselling group at18 weeks was 9.9 (SD¼ 5.9)compared with 11.3(SD ¼ 4.8) for the controlgroup (P ¼ 0.02); all groupimprovements werecomplete by 36 weeks.
35% of women inthe control groupwere experiencinghigh socialadversity atbaseline.
Morrell et al. [40] Cluster RCT;computerrandomisation;stratified by number ofexpected births peryear; intent-to-treat.
Two treatments: (1)cognitive–behaviouraltherapy; or (2) person-centred therapy (non-directive) provided weeklyat home for 8 weeks bytrained health visitors.
Postpartumdepression at 6, 12,and 18 months;EPDS, SF-12 mentalcomponent.
At 6 months, a significanteffect was found fortreatment on depressionscores, but no significantgroup difference betweenthe two approaches. For thesubgroup of women with 6-week EPDS scores of 12 orhigher, the mean EPDSscore for the interventiongroup at 6 months was 9.2(SD ¼ 5.4) compared with11.3 (SD ¼ 5.8) for thecontrol group; similarfindings were found at 12months.
High attrition at 12and 18 months.
C.-L.Dennis
/Best
Practice&
ResearchClinical
Obstetrics
andGynaecology
28(2014)
97–111
102
Sharp et al. [41] RCT;computerrandomisation;intent-to-treat.
254 UK women who metICD-10 criteria for majordepression in the first 6months postpartum;I1 ¼ 129 mothersI2 ¼ 125 mothers
Two treatments: (1)antidepressants or (2) non-directive counselling(listening visits) by trainedhealth visitors, whichcommenced after 4 weeks.
Postpartumdepression at 4 and18 weeks afterrandomisation;EPDS
At the 4-week assessment,recovery rates based onEPDS scores (<13)significantly favoured theantidepressant group (45%)over the supportive caregroup (20%). At the 18-week follow up, againrecovery favouredantidepressants (62% v51%).
No true controlgroup after 4weeks;change in studyprotocol beforecompletion;high number ofwomen in bothgroups receivedboth interventions.
Home visits by mental health nursesTamaki [42] RCT;
random allocation bycomputer-generatednumbers.
18 Japanese women withdiagnosis of majordepression;two-stage screening at 4and 8 weeks using EPDSand SCID;I ¼ 9 mothersC ¼ 9 mothers
4 weekly home visits over 8weeks by nurse or midwifetrained to provide support
Postpartumdepression at 1 and6 weeks aftertreatment; EPDSand clinicalinterview.
At the 1-week assessment,66.7% of women in thecontrol group remaineddepressed compared withonly 28.6% in theintervention group. Asignificant reduction inEPDS scores over time inthe intervention group butnot the control group.
Small sample size;data analysis wasnot intent-to-treat.
Collaborative models of careGjerdingen
et al. [43]RCT;group allocation viacomputer-generatedblock sizes of 10;stratification by clinic.
39 US women;identified using the SCIDand PHQ-9;I ¼ 19 mothersC ¼ 20 mothers
Stepped collaborative carewhich included (1) referralto primary care provider forinitial treatment; (2)regular telephone follow-up with care manager; (3)decision support forprimary care providers; (4)consultation or referral tomental health specialist forspecial cases; and (5)patient education providedthrough primary physician,care manager, and mailedPPD brochure
Postpartumdepression at 8, 12,24 and 36 weeks;PHQ-9 and SF-36mental health scale
No significant groupdifferences related toPostpartum depression.
Small sample size;training in steppedcare provided to allhealth providers(including thosewho gave usualcare);3 health providersgave care to womenin both groups;lack of intent-to-treat.
(continued on next page)
C.-L.Dennis
/Best
Practice&
ResearchClinical
Obstetrics
andGynaecology
28(2014)
97–111
103
Table 1 (continued)
Study Design Participants Intervention Outcome measure Results Limitations
Yawn et al. [44] Cluster RCT 28 practices wererandomised;I ¼ 14 practicesC ¼ 14 practices;2343 women were enrolledbetween 5 and 12 weekspostpartum.
Practices receivededucation and tools for PPDscreening, diagnosis,initiation of treatment, andfollow up within theirpractices.
Postpartumdepression at 6 and12 months;EPDS and PHQ-9
Among the 654 womenwith elevated postpartumdepression screeningscores, those in theintervention practices weremore likely to receive adiagnosis (P ¼ 0.0006) andtreatment for postpartumdepression (P ¼ 0.002).They also had lowerdepressive symptom levelsat 6 (P ¼ 0.07) and 12months (P ¼ 0.001)postpartum.
BDI, Beck Depression Inventory; C, control group; CES-D, Center for Epidemiological Studies Depression Scale; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders-FourthEdition; EDPS, Edinburgh Postnatal Depression Scale; GHQ, General Health Questionnaire; I, intervention group; ICD-10, International Classification of Diseases 10th revision; MADRS,Montgomery-Asberg Depression Rating Scale; PHQ-9, Patient Health Questionnaire; RCT, randomised-controlled trial; RDC, Research Diagnostic Criteria; SCID, Structured Clinical Interviewfor DSM-IV; SF-36, Short Form (36) Health Survey.
C.-L.Dennis
/Best
Practice&
ResearchClinical
Obstetrics
andGynaecology
28(2014)
97–111
104
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111 105
instead of the scheduled four; and (5) data analysis was not based upon intent-to-treat procedures.Thus, the positive results of this trial are questionable.
Finally, a group programme for postnatally distressed Australian women and their partners wasevaluated [33]. The term ‘distress’ was used to indicate that no diagnostic interview was undertaken todetermine eligibility but rather women had depressive symptomatology based on EPDS scores above 12.The programme consisted of eightweekly 2-h sessions, including one session for the couple, facilitated byan occupational therapist and nursewhere psychotherapeutic and cognitive–behavioural strategies wereused. The results from six separate groups are reported, in which 34 couples participated; only onemother dropped out, and attendance was over 90%. Seventeen mothers were simultaneously receivingtreatment by another health professional, and somewere taking antidepressant medication. Participantscompleted the EPDS and General Health Questionnaire during the first and last session, and were fol-lowed up at 12 months. At programme initiation, 66% of mothers had EPDS scores above 12, whichdecreased to 22% at thefinal session, and no participant had depressive symptomatology at the 12-monthfollow up. These results seem promising, although the lack of a control group, and the fact that over one-half of the mothers were receiving additional treatment for their postpartum depression, including an-tidepressant medication, render the therapeutic effectiveness of these group sessions unknown.
Transcending the typical group modality, a pilot trial evaluating the effect of telephone-based peersupport on postpartum depression symptomatology was conducted [34]. Canadian mothers who scoredabove 9 on the EPDS were identified through region-wide screening at the 8-week immunisation clinicsmanaged by public health nurses. Forty-two eligible and consentingmothers were randomly allocated toeither a control group (standard postpartum care; n¼ 22) or a peer support group (standard postpartumcare plus telephone-based support, initiated within 48–72 h of randomisation, from a mother who hadpreviouslyexperiencedpostpartumdepressionandhadattendeda4-hour trainingsession;n¼20). Followupwas conducted at 4 and 8 weeks after randomisation by blinded research assistants. Significant groupdifferenceswere found inprobablemajor depressive symptomatology (EPDS score above 12) at the 4- and8-week assessments. Specifically, at the 4-week assessment, 40.9% ofmothers in the control group scoredabove12ontheEPDScomparedwithonly10%inthepeer supportgroup. Similarfindingswere foundat the8-week assessment, in which 52.4% of mothers in the control group continued to score above 12 on theEPDS comparedwith15%ofmothers in thepeer-support group. A significantmeandifferencewas foundatthe 4-week assessment between mothers in the control (M¼ 12.1; SD¼ 4.6) and peer support (M¼ 8.5;SD¼ 3.7) (t¼ 2.8, P¼ 0.008) groups. Comparable group differenceswere found at the 8-week assessment(t ¼ 2.9; P ¼ 0.006). These preliminary results suggest that telephone-based peer support may be aneffective intervention and a larger randomised-controlled trial is warranted.
Letourneau et al. [35] built upon Dennis’ individualised peer-support model for postpartumdepression. They conducted a randomised-controlled trial to evaluate the effect of home-based peersupport that includedmaternal–infant interaction teaching for mothers with symptoms of postpartumdepression and their infants. Mothers with postpartum depression based on EPDS scores above 12were randomised to either a control group (standard postpartum care; n¼ 33) or an intervention group(12 weeks of home-based peer support that includedmaternal–infant interaction teaching; peers weremothers who had recovered from postpartum depression andwere trained to provide support; n¼ 27).Data were collected at baseline and at 6 and 12 weeks after randomisation. The primary outcome wasmaternal–infant interactions assessed by the observational nursing child assessment satellite trainingprogramme feeding and teaching scales. Secondary outcomes includedmaternal depressive symptoms(EPDS >12), maternal perceptions of social support, infant development, and infants’ salivary cortisollevels. Contrary to expectations, the results favoured the control group where a significant groupdifference was observed for one of the two measures of maternal–infant interactions. Several othermeasures favoured the control group, including maternal depressive symptoms and social supportscores. No significant treatment effects were observed in infant IQ scores or diurnal salivary cortisollevels. Given the small sample size, the results are questionable and additional research is warranted.
Partner support
In a Canadian trial to determine the effect of partner support in the treatment of mothers sufferingfrom postpartum depression, womenwho met the DSM-IV criteria for major depressive disorder with
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111106
postpartum onset were randomly allocated to either a control group (seven psycho-educational visitswith a psychiatrist; n ¼ 13) or an intervention group (seven psycho-educational visits with a psychi-atrist during which the mother’s partner participated in four of the sessions; n ¼ 16) [36]. All womenwere given a set of questionnaires that included the EPDS, and underwent a clinical assessment usingthe Mini International Neuropsychiatric Instrument during visits one and seven. No significant dif-ferences in mean EPDS scores were observed immediately after the intervention between the inter-vention (M¼ 11.4, SD¼ 6.2) and control (M¼ 14.6, SD¼ 7.2; P¼ 0.20) groups. At the 4-week follow up,significant group differences were found favouring the intervention group (M ¼ 8.6, SD ¼ 5.2 vM ¼ 14.7, SD ¼ 7.2; P ¼ 0.013). Study limitations included a small sample, inexplicit randomisationprocedures, and significant group difference in baseline characteristics; partners of the women in theintervention group had a significantly higher level of dyadic adjustment, suggesting they had a morepositive appraisal of the marriage than did their control-group counterparts. This is a serious limitationconsidering that the intervention is the inclusion of partner support in the psycho-educational visits.Despite these considerable limitations, the initial results from this trial suggest partner support mayhave a measurable effect on women experiencing postpartum depression and warrants furtherinvestigation.
Non-directive counselling
The importance of non-directive counselling, sometimes called ‘listening visits,’ has been evaluatedin several studies. To determine the effectiveness of these ‘listening visits,’ 55 UK women identified asdepressed, through community-based EPDS screening at 6 weeks postpartum and a home psychiatricinterview at 13 weeks, were randomised to either a control group (routine primary care) or a coun-selling group (eight weekly counselling visits by health visitors who received minimal training in non-directive counselling methods) [37]. Fifty of the 55 participants completed the trial, 26 in the coun-selling group and 24 in the control group. After a mean time interval of 13 weeks, mothers were re-administered the standardised psychiatric interview and EPDS at home by a psychiatrist blinded togroup allocation. According to research diagnostic criteria, 18 (69%) women in the counselling grouphad fully recovered compared with only nine (38%) women in the control group. When women in theintervention group were asked if they had received any help for their depression, 23 (88%) womenresponded that talking to their health visitor had been themost important recovery factor; one-third ofthe counselled women did not recover despite the intervention. Of this sub-group, two had a longhistory of depression, another had postpartum depression previously, and a further two had a familyhistory of depression, signifying postpartum depression occurring in the context of a continuum ofpsychiatric disturbances may be less likely to respond to a psychosocial intervention. It is also note-worthy that three women in each groupwere considered to have taken antidepressant medication at atherapeutic level. Even with the limitations of a small sample and the possible antidepressant co-intervention, the trial results suggest that counselling by health visitors may be valuable in man-aging postpartum depression.
Wickberg and Hwang [38] extended the findings of Holden et al. [37] in a population-based trialconducted to evaluate the effect of counselling among Swedish women. Mothers participated in a two-stage screening procedure, completing the EPDS at 8 and 12 weeks postpartum. Women who scoredabove 11 on both screening occasions were interviewed at home by a clinical psychologist, blinded toEPDS scores, at 13 weeks postpartum using the Montgomery-Asberg Depression Rating Scale. Womenwho were identified as depressed according to DSM-III-R criteria were randomly allocated to receiveeither routine primary care (n ¼ 16) or counselling (n ¼ 15), which consisted of six weekly 1-hcounselling sessions provided in the home or clinic by a nurse who received brief training in non-directive counselling methods. Twelve (80%) women who received counselling were fully recoveredafter the intervention comparedwith four (25%)mothers in the control group. The findings of this well-conducted trial are tempered by the small sample size.
In a UK trial to evaluate the effect of three psychological treatments in relation to routine primarycare, 193 women with postpartum depression (DSM-III-R criteria) were randomly assigned to one offour conditions: (1) routine primary care; (2) non-directive counselling; (3) cognitive–behaviouraltherapy; or (4) psychodynamic therapy [39]. Women were assessed with the EPDS and the Structured
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111 107
Clinical Interview for DSM-III-R (SCID) immediately after the treatment phase (at 4.5 months) and at 9,18 and 60months postpartum. Compared with the control group, all three treatments had a significanteffect at 4.5 months on maternal mood. Specifically, 54% of women in the counselling group, 57% ofwomen in the cognitive–behavioural group, and 71% of women in the psychodynamic group had fullyrecovered compared with only 40% in the control group. Only psychodynamic therapy, however,produced a rate of reduction in depression significantly superior to that of the control group. Thebenefit of treatment was no longer apparent by 9 months postpartum. Further, treatment did notreduce subsequent episodes of postpartum depression. Study limitations included a significant groupdifference in baseline characteristics: the control group had more mothers with social adversity (35%),whereas the psychodynamic group had less (10%).
In a larger UK cluster trial to evaluate the effect of two psychologically informed interventions byhealth visitors, 101 general practices were randomised with mothers followed up to 18 monthspostpartum [40]. Overall, 2749 women were allocated to the intervention group and 1335 to thecontrol group. For the intervention, health visitors (n ¼ 89; 63 clusters) were trained to identifydepressive symptoms at 6–8 weeks postpartum using the EPDS and clinical assessment, and toprovide psychologically informed sessions based on cognitive–behavioural or non-directive coun-selling for 1 h a week for 8 weeks. Health visitors in the control group (n ¼ 49; 38 clusters) providedusual care. The primary outcome was depressive symptoms (EPDS > 11) at 6 months postpartum, andsecondary outcomes included global distress, anxiety, general mental health, and parenting stress at6, 12, and 18 months. In total, 4084 eligible women consented and 595 women had a 6-week EPDSscore above 11. Of these, 418 had EPDS scores available at 6 weeks and 6 months. At 6 months,women’s EPDS scores were significantly lower in the intervention group than in the control group(OR ¼ 0.62, 95% CI ¼ 0.40 to 0.97), with 34% of women in the intervention group scoring above 11 onthe EPDS compared with 46% of women in the control group (P ¼ 0.036). Benefit for women in theintervention group with a 6-week EPDS score above 11 was maintained at 12 months postpartum. Nodifferential benefit was found for either psychological approach over the other. Training health vis-itors to assess women, identify symptoms of postpartum depression, and deliver psychologicallyinformed sessions was clinically effective at 6 and 12 months postpartum compared with usual care.Study limitations included (1) high attrition of participants at 12 and 18 months; (2) participants mayhave been aware of the group allocation of their cluster before enrolling in the study; (3) the homevisitor doing the recruitment of participants was aware of her cluster allocation before recruitmentbegan; (4) three clusters were lost during the course of the trial (one from the control group beforethe baseline assessment and two from the intervention group between the 6- and 12-month followups).
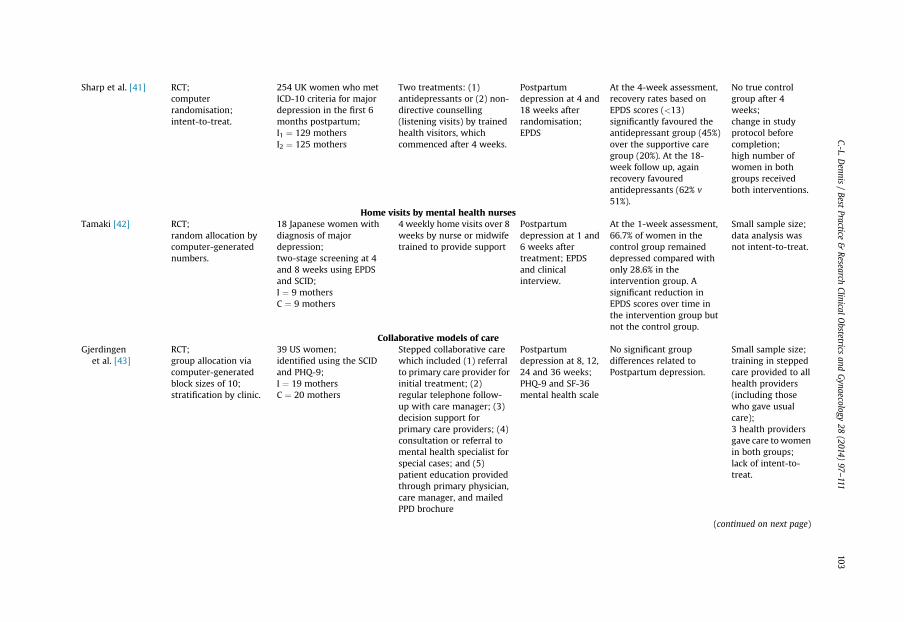
Lastly, in another UK trial, 254 women who fulfilled International Classification of Diseases version10 criteria for major depression in the first 6 months postpartum were recruited from 77 generalpractices and randomised to receive either an antidepressant, usually a selective serotonin reuptakeinhibitor prescribed by their general practitioner, or non-directive counselling (listening visits) from aspecially trained research health visitor [41]. The trial was designed to compare antidepressants withgeneral supportive care for the first 4 weeks, after which women allocated to listening visitscommenced their sessions. The primary outcome was depression assessed using the EPDS at 4 and 18weeks after randomisation. At 4weeks, womenweremore than twice as likely to have improved if theyhad been randomised to antidepressants comparedwith listening visits, which started after 4 weeks ofgeneral supportive care. In particular, more women allocated to the antidepressant group hadimproved as defined by having an EPDS score below 13 (n¼ 48, 45%) at 4 weeks thanwomen allocatedto receive listening visits (n ¼ 22; 20%) (OR ¼ 3.4, 95% CI ¼ 1.8 to 6.5; P < 0.001). At 18 weeks, 60 (62%)women in the antidepressant group had improved compared with 56 (51%) women in the listeningvisits group, although the difference was not statistically significant (OR ¼ 1.5, 95% CI ¼ 0.8 to 2.6;P ¼ 0.19). Overall, a difference was observed between the groups in favour of the antidepressant groupof about 25 percentage points at 4 weeks, which reduced to about 11% at 18 weeks. Qualitative in-terviews with women revealed a preference for listening visits but an acceptance that antidepressantsmight be necessary. Serious trial limitations included the high number of women in both groups thatreceived both treatments by 18 weeks, there was no true control group after 4 weeks, and there was achange in study protocol before trial completion.
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111108
Home visits by mental health nurses
In a Japanese trial to evaluate the effect of home visits by mental health nurses on the treatment ofpostpartum depression, 18 women identified as depressed, through community-based EPDS screeningat 4 weeks postpartum and a home psychiatric interview at 8 weeks, were randomly allocated to anintervention (n ¼ 9) or control (n ¼ 9) group [42]. The intervention group received four weekly homevisits by a mental health nurse, which consisted of active listening, providing support and acceptanceof the woman, psycho-education on depression, and advice about coping strategies. Control groupparticipants received usual care, which consisted of a postpartumvisit at homewith amidwife or nurseand a 4-month postpartum check-up at a community-based centre. Two women in the interventiongroup did not complete the study. At 1 week after the intervention, five (71.4%) women in the inter-vention group had fully recovered according to DSM-IV criteria compared with only three (33.3%)women in the control group. At 6 weeks, seven (100%) women in the intervention group had fullyrecovered compared with six (66.7%) women in the control group. When women in the interventiongroup were asked about their satisfaction with the home visits, the qualitative analysis of commentsrevealed four categories related to ‘setting their mind at ease’, ‘clarifying thoughts’, ‘improving copingabilities’, and ‘removing feelings of withdrawal from others’. Study limitations included a small sampleand data analysis was not intent-to-treat. It is also noteworthy that if it was considered that a womanneeded treatment, a psychiatrist was consulted, the intervention was stopped, and treatment wasstarted. It is unclear how this might have affected the trial results, how the ‘need for treatment’ wasdefined, what treatment was given, and how often this happened in each of the study groups.
Collaborative models of care
Another treatment approach has been improving the quality of care provided to women withpostpartum depression. In a US pilot trial to evaluate the effect of a stepped collaborative care inter-vention for women with postpartum depression and to evaluate health differences between self-diagnosed depressed and non-depressed women, 506 mothers of infants from seven clinicscompleted surveys at 0 to 1, 2, 4, 6, and 9 months postpartum [43]. Women positive for clinicaldepression as measured on the Structured Clinical Interview for DSM-IV were randomised to steppedcollaborative care or usual care. Nine-month treatment, health, and work outcomes were evaluated forstepped care women (n ¼ 19) compared with control depressed women (n ¼ 20), and self-diagnoseddepressed women (n ¼ 122) compared with non-depressed women (n ¼ 344). Forty-five women hadSCID-positive depression, whereas 122 had self-diagnosed depression. For SCID-positive depressedwomen, the stepped care intervention increased mothers’ awareness of their depression diagnosis(100% v 61%; p¼ 0.008) and their receipt of treatment (94% v 56%; P¼ 0.019). Self-diagnosed depressedwomen had more depressive symptoms and acute care visits, worse general and mental health, andgreater impact of health problems on regular activities. The stepped care intervention improvedwomen’s knowledge of their postpartum depression diagnosis and their receipt of treatment. Theformal diagnostic procedures missed many women whose depressed mood interfered with theirhealth and function. Study limitations included (1) a small sample for the stepped care intervention;(2) training in stepped care treatment was provided to all health providers, including those who gaveusual care; (3) three health providers gave care towomen in both groups; and (4) data analysis was notintent-to-treat.
In a large US trial to evaluate the effect of a primary-care-based screening, diagnosis, and man-agement of postpartum depression, 28 primary care practices in the US were randomised to usual care(n ¼ 14) or intervention (n ¼ 14) [44]. The intervention sites received education and tools for post-partum depression screening, diagnosis, initiation of treatment, and follow up within their practices.Usual care sites received a 30-min presentation about postpartum depression. Outcomes were basedon patient-reported measures (level of depressive symptoms) from surveys at 6 and 12 months, plusmedical record review (diagnosis and therapy initiation). Among the 2343 women enrolled between 5and 12 weeks postpartum, 1897 (80.1%) provided outcome information, and were included in theanalysis. Overall, 654 (34.5%) women had elevated screening scores indicative of depression, withcomparable rates in the intervention and usual-care groups. Among the 654 women with elevated
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111 109
postpartumdepression screening scores, those in the intervention practices weremore likely to receivetreatment for postpartum depression (P ¼ 0.002) and they had had lower levels of depressive symp-toms at 6 (P ¼ 0.07) and 12 (P ¼ 0.001) months’ postpartum. The results from this trial suggest thatprimary care-based screening, diagnosis, and management may significantly improve maternaldepression outcomes at 12 months.
Conclusion
Postpartum depression can be treated through several different psychosocial approaches, includingpeer support, partner support, non-directive counselling, home visits by mental health nurses, andcollaborative models of care. Research has clearly shown that a lack of social support is a significantpredictor of postpartum depression. As such, peer support interventions potentially have beneficialeffects in treating women who have mild-to-moderate depression. Three studies have evaluated theeffectiveness of professionally facilitated peer support groups. Unfortunately, theoretical limitations,such as the inclusion of both depressed and non-depressed women, and methodological weaknessesrender the results equivocal. Well-designed trials with large, homogeneous samples are warranted.Future research should also include self-help groups (i.e. groups not facilitated by a health professional)to extend the testing of lay support models with mild to moderately depressed women, and evalua-tions of eligible mothers who decline group interventions should be conducted to identify potentialhelp-seeking barriers. Evaluations of group interventions should also include measures that assessgroup dynamics and social comparisons to determine the salutary components of support groups. Anew intervention that holds promise is telephone-based peer support, and well-designed trials withlarge samples are warranted. Another trial evaluated home-based peer support; however, the primaryfocus was on maternal–infant relationship.
One area that has received little attention is the role the spouse or partner plays in the treatment ofor recovery from postpartum depression. Partners can be a good source of instrumental (e.g. sharing ofchildcare and domestic responsibilities) and emotional support, and can be a mediating link betweenthe mother and family members who may not understand the nature of postpartum depression.Further research evaluating interventions with the partner is needed to determine how the partner canbe most effective in providing social support to mothers with postpartum depression.
Five European trials have evaluated the effectiveness of non-directive counselling with positiveresults, suggesting this treatment modality may be a viable option for women with mild to moderatepostpartum depression. The research has demonstrated the feasibility of population-based screeningand the application of home visiting using trained health professionals. Unfortunately, the immediateproblem is the small sample size in all but one of these trials. Contextual factors also decrease theapplication of the results to a US populationwhere differences in the delivery of postpartum care exist.As such, a large randomised-controlled trial is needed to replicate these auspicious results. One trialevaluated the effect of home visits by mental health nurses and further research is warranted. Finally,collaborative models of care hold promise and, with further research, these interventions may bebeneficial treatment option.
Research implications
This review clearly demonstrates postpartum depression research presents many special meth-odological complexities that need to be considered if scientific knowledge is to progress. First,particular difficulties exist in defining the target group to be studied, as diagnosis is much less concretethan in other areas where an initial assessment can be confirmed by physiological tests. Second, manyof the treatments used are hard to define with clarity as psychosocial interventions often involvesupportive interactions and manipulation of the environment; replicating such treatment with fidelityand understanding underlying beneficial mechanisms is challenging. Third, the nature of the in-terventions used frequently result in co-interventions. Finally, the context of postpartum depressionresearch is crucial, as the cultural and organisational environment in which postpartum depressionservices takes place is highly variable. For example, the same intervention can have differing effectsdepending on context and variations in the control group. It is noteworthy that numerous trials have
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111110
evaluated a psychosocial intervention for the prevention of postpartum depression, and a Cochranesystematic review of psychosocial and psychological interventions to prevent postpartum depressionwas recently completed [45]. Growing evidence shows that psychosocial interventions may also behighly beneficial in preventing postpartum depression.
Research agenda
� The effectiveness of telephone-based peer support.� Partner support.� The effectiveness of non-directive counselling in a US context.
Practice points
� Psychosocial interventions may be effective in treating mothers with mild-to-moderatepostpartum depression.
� It is improbable that a single treatment modality will be effective for all women.
Conflict of interest
None declared.
References
*[1] O’Hara MW, Swain A. Rates and risk of postpartum depression: a meta-analysis. Int Rev Psychiatry 1996;8:37–54.*[2] Beck CT. Predictors of postpartum depression: an update. Nurs Res 2001;50:275–85.[3] Brugha TS, Sharp HM, Cooper SA, et al. The Leicester 500 Project. Social support and the development of postnatal
depressive symptoms, a prospective cohort survey. Psychol Med 1998;28:63–79.[4] Paykel ES, Emms EM, Fletcher J, et al. Life events and social support in puerperal depression. Br J Psychiatry 1980;136:
339–46.[5] O’Hara MW, Rehm LP, Campbell SB. Postpartum depression. A role for social network and life stress variables. J Nerv Ment
Dis 1983;171:336–41.[6] Romito P, Saurel-Cubizolles MJ, Lelong N. What makes new mothers unhappy: psychological distress one year after birth
in Italy and France. Soc Sci Med 1999;49:1651–61.[7] Mills EP, Finchilescu G, Lea SJ. Postnatal depression: an examination of psychosocial factors. S Afr Med J 1995;85:99–105.[8] Mauthner NS. Re-assessing the importance and role of the marital relationship in postnatal depression: methodological
and theoretical implications. J Reprod Infant Psychol 1998;16:157–75.[9] Small R, Astbury J, Brown S, et al. Depression after childbirth. Does social context matter? Med J Aust 1994;161:473–7.
[10] Chan SW, Levy V, Chung TK, et al. A qualitative study of the experiences of a group of Hong Kong Chinese womendiagnosed with postnatal depression. J Adv Nurs 2002;39:571–9.
[11] Graff LA, Dyck DG, Schallow JR. Predicting postpartum depressive symptoms: a structural modelling analysis. Percept MotSkills 1991;73:1137–8.
[12] Logsdon MC, Usui W. Psychosocial predictors of postpartum depression in diverse groups of women. West J Nurs Res2001;23:563–74.
[13] Logsdon MC, McBride AB, Birkimer JC. Social support and postpartum depression. Res Nurs Health 1994;17:449–57.[14] Chen CH, Wu HY, Tseng YF, et al. Psychosocial aspects of Taiwanese postpartum depression phenomenological approach:
a preliminary report. Kaohsiung J Med Sci 1999;15:44–51.[15] O’Hara MW, Rehm LP, Campbell SB. Predicting depressive symptomatology: cognitive-behavioral models and postpartum
depression. J Abnorm Psychol 1982;91:457–61.[16] Gotlib IH, Whiffen VE, Wallace PM, et al. Prospective investigation of postpartum depression: factors involved in onset
and recovery. J Abnorm Psychol 1991;100:122–32.[17] O’Hara MW. Social support, life events, and depression during pregnancy and the puerperium. Arch Gen Psychiatry 1986;
43:569–73.[18] Cutrona CE. Social support and stress in the transition to parenthood. J Abnorm Psychol 1984;93:378–90.[19] Atkinson AK, Rickel AU. Postpartum depression in primiparous parents. J Abnorm Psychol 1984;93:115–9.
C.-L. Dennis / Best Practice & Research Clinical Obstetrics and Gynaecology 28 (2014) 97–111 111
[20] O’Hara MW, Schlechte JA, Lewis DA, et al. Controlled prospective study of postpartum mood disorders: psychological,environmental, and hormonal variables. J Abnorm Psychol 1991;100:63–73.
*[21] Dennis C-L, Hodnett ED. Psychosocial and psychological interventions for treating postpartum depression. CochraneDatabase Syst Rev 2007;4. Art No. CD006116.
*[22] Berkman LF, Glass T. Social integration, social networks, social support, and health. In: Berkman LF, Kawachi I, editors.Social epidemiology. New York: Oxford University Press; 2000. p. 137–73.
*[23] Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull 1985;98:310–57.[24] Lin N, Ye X, Ensel WM. Social support and depressed mood: a structural analysis. J Health Soc Behav 1999;40:344–59.[25] Thoits PA. Social support as coping assistance. J Consult Clin Psychol 1986;54:416–23.[26] Kawachi I, Berkman LF. Social ties and mental health. J Urban Health 2001;78:458–67.*[27] Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav 2011;52:145–61.[28] Eastwood P. Promoting peer group support with postnatally depressed women. Health Visit 1995;68:148–50.[29] Pitts F. Comrades in adversity: the group approach. Health Visit 1995;68:144–5.[30] Fleming AS, Klein E, Corter C. The effects of a social support group on depression, maternal attitudes and behavior in new
mothers. J Child Psychol Psychiatry 1992;33:685–98.[31] Rosenblatt A, Greenberg J. Examining the world of the depressed: do depressed people prefer others who are depressed?
J Pers Soc Psychol 1991;60:620–9.[32] Chen CH, Tseng YF, Chou FH, et al. Effects of support group intervention in postnatally distressed women. A controlled
study in Taiwan. J Psychosom Res 2000 Dec;49:395–9.[33] Morgan M, Matthey S, Barnett B, et al. A group programme for postnatally distressed women and their partners. J Adv
Nurs 1997;26:913–20.*[34] Dennis C-L. The effect of peer support on postpartum depression: a pilot randomized controlled trial. Can J Psychiatry
2003;48:61–70.[35] Letourneau N, Stewart M, Dennis C-L, et al. Effect of home-based peer support on maternal-infant interactions among
women with postpartum depression: a randomized, controlled trial. Int J Ment Health Nurs 2011;20:345–57.[36] Misri S, Kostaras X, Fox D, et al. The impact of partner support in the treatment of postpartum depression. Can J Psy-
chiatry 2000;45:554–8.[37] Holden JM, Sagovsky R, Cox JL. Counselling in a general practice setting: controlled study of health visitor intervention in
treatment of postnatal depression. BMJ 1989;298:223–6.[38] Wickberg B, Hwang CP. Counselling of postnatal depression: a controlled study on a population based Swedish sample. J
Affect Disord 1996;39:209–16.[39] Cooper PJ, Murray L, Wilson A, et al. Controlled trial of the short- and long-term effect of psychological treatment of post-
partum depression. I. Impact on maternal mood. Br J Psychiatry 2003;182:412–9.*[40] Morrell CJ, Slade P, Warner R, et al. Clinical effectiveness of health visitor training in psychologically informed approaches
for depression in postnatal women: pragmatic cluster randomised trial in primary care. BMJ 2009;338:a3045.[41] Sharp DJ, Chew-Graham C, Tylee A, et al. A pragmatic randomised controlled trial to compare antidepressants with a
community-based psychosocial intervention for the treatment of women with postnatal depression: the RESPOND trial.Health Technol Assess 2010;14 iii–iv, ix–xi, 1–153.
[42] Tamaki A. Effectiveness of home visits by mental health nurses for Japanese women with post-partum depression. Int JMent Health Nurs 2008;17:419–27.
[43] Gjerdingen D, Crow S, McGovern P, et al. Stepped care treatment of postpartum depression: impact on treatment, health,and work outcomes. J Am Board Fam Med 2009;22:473–82.
*[44] Yawn BP, Dietrich AJ, Wollan P, et al. TRIPPD: a practice-based network effectiveness study of postpartum depressionscreening and management. Ann Fem Med 2012;10:320–9.
*[45] Dennis C-L, Dowswell T. Psychosocial and psychological interventions for preventing postpartum depression. CochraneDatabase Syst Rev 2013;2:CD001134.