REVIEW ARTICLE Psychosocial well-being and supportive care needs of cancer patients and survivors living in rural or regional areas: a systematic review from 2010 to 2021 Shannen R. van der Kruk 1,2,3 & Phyllis Butow 4 & Ilse Mesters 1 & Terry Boyle 3 & Ian Olver 5 & Kate White 6 & Sabe Sabesan 7 & Rob Zielinski 8,9 & Bryan A. Chan 10 & Kristiaan Spronk 2,11 & Peter Grimison 12 & Craig Underhill 13 & Laura Kirsten 14 & Kate M. Gunn 2,11 & on behalf of the Clinical Oncological Society of Australia Received: 3 March 2021 /Accepted: 13 July 2021 # The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature 2021 Abstract Purpose To summarise what is currently known about the psychosocial morbidity, experiences, and needs of people with cancer and their informal caregivers, who live in rural or regional areas of developed countries. Methods Eligible studies dating from August 2010 until May 2021 were identified through several online databases, including MEDLINE, EMBASE, PsychINFO, and RURAL (Rural and Remote Health Database). Results were reported according to the PRISMA guidelines and the protocol was registered on PROSPERO (CRD42020171764). Results Sixty-five studies were included in this review, including 20 qualitative studies, 41 quantitative studies, and 4 mixed methods studies. Qualitative research demonstrated that many unique psychosocial needs of rural people remain unmet, partic- ularly relating to finances, travel, and accessing care. However, most (9/19) quantitative studies that compared rural and urban groups reported no significant differences in psychosocial needs, morbidity, or quality of life (QOL). Five quantitative studies reported poorer psychosocial outcomes (social and emotional functioning) in urban cancer survivors, while three highlighted poorer outcomes (physical functioning, role functioning, and self-reported mental health outcomes) in the rural group. Conclusion Recent research shows that rural people affected by cancer have unique unmet psychosocial needs relating to rurality. However, there was little evidence that rural cancer survivors report greater unmet needs than their urban counterparts. This contrasts to the findings from a 2011 systematic review that found rural survivors consistently reported worse psychosocial outcomes. More population-based research is needed to establish whether uniquely rural unmet needs are due to general or cancer-specific factors. Keywords Cancer . Rural . Psychosocial . Healthcare needs . Informal caregivers . Oncology * Kate M. Gunn [email protected]Shannen R. van der Kruk [email protected]Phyllis Butow [email protected]Ilse Mesters [email protected]Terry Boyle [email protected]Ian Olver [email protected]Kate White [email protected]Sabe Sabesan [email protected]Rob Zielinski [email protected]Bryan A. Chan [email protected]Kristiaan Spronk [email protected]Peter Grimison [email protected]Craig Underhill [email protected]Laura Kirsten [email protected]Extended author information available on the last page of the article https://doi.org/10.1007/s00520-021-06440-1 / Published online: 14 August 2021 Supportive Care in Cancer (2022) 30:1021–1064
Transcript
REVIEW ARTICLE
Psychosocial well-being and supportive care needs of cancer patientsand survivors living in rural or regional areas: a systematic reviewfrom 2010 to 2021
Shannen R. van der Kruk1,2,3 & Phyllis Butow4& Ilse Mesters1 & Terry Boyle3
& Ian Olver5 & Kate White6&
Sabe Sabesan7& Rob Zielinski8,9 & Bryan A. Chan10
& Kristiaan Spronk2,11 & Peter Grimison12&
Craig Underhill13 & Laura Kirsten14& Kate M. Gunn2,11
& on behalf of the Clinical Oncological Society of Australia
Received: 3 March 2021 /Accepted: 13 July 2021# The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature 2021
AbstractPurpose To summarise what is currently known about the psychosocial morbidity, experiences, and needs of people with cancerand their informal caregivers, who live in rural or regional areas of developed countries.Methods Eligible studies dating from August 2010 until May 2021 were identified through several online databases, includingMEDLINE, EMBASE, PsychINFO, and RURAL (Rural and Remote Health Database). Results were reported according to thePRISMA guidelines and the protocol was registered on PROSPERO (CRD42020171764).Results Sixty-five studies were included in this review, including 20 qualitative studies, 41 quantitative studies, and 4 mixedmethods studies. Qualitative research demonstrated that many unique psychosocial needs of rural people remain unmet, partic-ularly relating to finances, travel, and accessing care. However, most (9/19) quantitative studies that compared rural and urbangroups reported no significant differences in psychosocial needs, morbidity, or quality of life (QOL). Five quantitative studiesreported poorer psychosocial outcomes (social and emotional functioning) in urban cancer survivors, while three highlightedpoorer outcomes (physical functioning, role functioning, and self-reported mental health outcomes) in the rural group.Conclusion Recent research shows that rural people affected by cancer have unique unmet psychosocial needs relating to rurality.However, there was little evidence that rural cancer survivors report greater unmet needs than their urban counterparts. This contraststo the findings from a 2011 systematic review that found rural survivors consistently reported worse psychosocial outcomes. Morepopulation-based research is needed to establish whether uniquely rural unmet needs are due to general or cancer-specific factors.
Understanding the psychosocial well-being and supportivecare needs of people with cancer has become an importantpublic health concern [1]. As the number of people diagnosedwith cancer and survival rates improve [2], more people livingwith cancer will require ongoing cancer treatment, surveil-lance, and supportive care to address their psychosocial needs[3, 4]. Supportive care can be defined as care that helps aperson with cancer and their family cope with cancer and itstreatment, from pre-diagnosis through the process of diagnosisand treatment to cure, continuing illness or death and intobereavement [5]. Unfortunately, given the increasing preva-lence of cancer survivors and limited health workforce, cur-rent survivorship care leaves survivors with significant unmetneeds [6–8]. Previous research indicates survivors living inrural or regional areas are likely to have more unmet needsthan those residing in urban areas [9, 10]. Fortunately, targetedresearch is being undertaken to understand the specific, cul-turally complex indigenous cancer issues [11], as outcomesare even worse for these members of the rural population.However, it is also important to develop understanding aboutthe supportive care needs of the significant number of non-indigenous rural people affected by cancer and caregivers, toimprove service delivery models, and to inform newapproaches.
Research suggests that rurality negatively impacts survival.A survival analysis in Australian cancer patients showed thatcancer patients living in remote areas are 35% more likely todie within 5 years of a cancer diagnosis than those living inurban areas [12, 13]. Similar patterns have been found in var-ious geographical regions around the world and usingmultipledefinitions of rurality [14]. Contributing factors may includemore labour-intensive work schedules, delayed diagnosis,geographic isolation, and lower levels of income, education,and socioeconomic status (SES) [12, 15, 16]. As there arefewer cancer services in rural or regional areas, rural peoplewith cancer may also experience a lack of local support andservices, and often have to travel significant distances or relo-cate to access cancer care [17–20]. This may affect their treat-ment decisions and follow-up care post-treatment, and pro-foundly impact their psychosocial well-being, resulting inpoorer health status [20–22].
In 2011, a systematic review on psychosocial well-beingand the supportive care needs of people living in urban andrural/regional areas, diagnosed with cancer, was publishedonline [23]. Bringing together the literature on psychosocialmorbidity in rural areas (excluding studies on medical out-comes, survival, interventions etc.), this influential 2011 re-view included 37 studies and found that the majority of con-trolled studies reported worse psychosocial outcomes for ruralcancer patients, who had higher needs, particularly in the do-mains of daily living and physical functioning, compared to
urban cancer patients. Furthermore, many rural patients andfamilies reported rural-specific challenges including travel,financial, emotional, and relationship challenges. The reviewconcluded that more research was needed that included peoplewith heterogenous cancers from rural and urban settings toconfirm these disparities. Since then, increasing research in-terest in this field has been driven, at least in part, by thefinding that although cancer survival is improving overall,disparities between rural and urban populations are continuingto grow [24]. Addressing rural cancer disparities has become akey priority area for the National Cancer Institute in theUnited States (US), which has led to an increase in the amountof research funding being directed towards this field [25].However, the impact of rurality on psychosocial morbidityremains less clear than the impact that it has on physicalmor-bidity and survival. Therefore, the purpose of this study was tosystematically review studies on levels of psychosocial mor-bidity and the experiences and needs of people with cancerand their informal caregivers, living in rural or regional areas,that have been published in the last 10 years, since the 2011review.Where studies included data on both psychosocial andphysical morbidity, we report only the former.
Methods
This systematic literature reviewwas conducted in accordancewith the Preferred Reporting Items for Systematic Reviewsand Meta-Analyses (PRISMA) [26]. The study protocol wasregistered in the online database of PROSPERO(CRD42020171764).
Eligibility criteria
Papers eligible for inclusion were published in English afterJuly 2010 (i.e., the end date of the previous systematic review)and reported on studies comparing rural versus urban-dwelling cancer survivors in terms of their psychosocial mor-bidity or supportive care needs, or alternatively reported onthese issues specifically for rural cancer survivors and/or theirinformal caregivers. Eligible studies included study partici-pants who were adults (18 years or older) within a settingdescribed as a regional or rural area(s) of Australia (i.e., theAccessibility/Remoteness Index of Australia (ARIA) as de-fined by the Australian Bureau of Statistics [27]), or as a ruralarea for countries of the developed world, as defined by theHuman Development Index (HDI) of 0.8 or higher (i.e., highhuman development) [28]. The ARIA classifies locations intofive categories: very remote, remote, moderately accessible,accessible, and highly accessible [27]. Both qualitative andquantitative (non-experimental) studies were included in thereview. As per the previous review [23], studies were exclud-ed if they did not report on the prevalence of psychosocial
1022 Support Care Cancer (2022) 30:1021–1064
morbidity or supportive care needs, i.e., they were interven-tion studies, focussed on medical outcomes or survival rates,reported differences in the uptake of cancer screening or fo-cussed on health attitudes or treatment decision making, anddiscussed service delivery or discussed the effectiveness ofsupport groups or support via videoconferencing. In addition,studies were excluded if they explored psychosocial outcomesin indigenous populations (as the issues facing these popula-tions are unique).
Information sources
Searches were identified via searching four electronic biblio-graphic databases, including RURAL: Rural and RemoteHealth Database (which specifically covers a range of subjectsrelated to rural and remote area health issues and care),PsychINFO, Embase, and Medline. Additionally, backwardand forward citation searching of all included articles wasperformed to identify any additional studies.
Search strategy
The searches were conducted in the final week of April 2020and updated in the third week of May 2021. Search strategieswere amended to the requirements of each database. In gen-eral, the searches included the following combinations ofterms and were combined as (#1 OR #6) AND (#2 OR #7)AND (#3 OR #8) AND (#4 OR #9) NOT (#5 OR #10;Table 1). The search was limited to August 2010 untilMay 2021.
Search selection
Initial search results from all databases were screened for du-plicates and eliminated through a systematic review manage-ment software (Covidence). Screening of articles was com-pleted in two stages: of information provided in the title and
abstract, and subsequently, full text. One reviewer (SK)screened all papers individually and the other reviewersscreened a percentage in duplicate, 20% in the first stage(KG) and 100% in the second stage. Any disagreement wasresolved by discussion and where consensus could not beeasily reached, a third independent reviewer (KS) made thefinal decision.
Data collection and items
Data extraction was conducted by one reviewer (SK). A sec-ond reviewer (KS) checked the data extracted from 20% of thearticles to assess the quality of data collection. Additional datawas extracted for one paper. As per the previous review [23],the included articles were summarised according to reference,study design, response rate, sample size, setting, measures,type of cancer, results, and study quality. In addition, dataon study population was collected to allow for clearer docu-mentation of whether study participants were adult cancersurvivors undergoing treatment (i.e., people who were receiv-ing cancer treatment at time of study — not including hor-monal therapy), adult cancer survivors post-treatment (i.e.,people who had finished cancer treatment at time of study),cancer patients in palliative care, and/or family or friends car-ing for a person with cancer.
Risk of bias
The quality of individual studies was assessed independentlyby two reviewers (SK and KS). Studies were critically ap-praised using the appropriate appraisal tool for the study de-sign (both quantitative and qualitative), available from theJoanna Briggs Institute [29]. Included articles werecategorised as having poor, good, or very good methodolog-ical reporting by calculating the percentages of items onwhichstudies were rated as including essential quality characteristics(i.e., less than 40% were classified as poor, 40–70% as good,
1 Neoplasms 6 cancer OR neoplasm OR carcinoma OR oncology
2 Rural population 7 regional OR remote OR travel
3 ‘Quality of life’ 8 well-being OR ‘quality of life’ OR QOL OR psycho* OR social OR emoti* ORmorbidity OR adjust* OR depress* OR anx* OR distress OR ‘unmet needs’OR need*
4 Adult 9 adult OR adults OR men OR women OR man OR woman OR elderly OR ‘theaged’ OR ‘middle aged’ OR senior* OR geriatric*
5 Oceanic ancestrygroup
10 aborigi* OR indigenous*
*Combined as (#1 OR #6) AND (#2 OR #7) AND (#3 OR #8) AND (#4 OR #9) NOT (#5 OR #10)
1023Support Care Cancer (2022) 30:1021–1064
and higher than 70% as very good). Studies that combinedqualitative and quantitative methods (i.e., mixed methods)were assessed by the Mixed Methods Appraisal Tool(MMAT) [30]. Any initial differences (17%) were resolvedthrough discussion and consensus. Studies of all levels ofquality were included in the data synthesis.
Summary measures
Levels of psychosocial morbidity and quality of life (QOL)were measured in proportions. The unmet needs and experi-ences of people with cancer were documented thematically.
Results
Study selection
The search of electronic databases identified 4589 unique pa-pers published online since August 2010 (Figure 1). Afterremoval of duplicates, 4332 studies remained and were eval-uated on title and abstract. A total of 259 potentially relevantpapers were assessed on full text, of which 61 papers were
included. Four additional papers were identified through back-ward and forward citation searching, resulting in 65 studiesbeing included in this systematic review (August 2010–May 2021).
Study characteristics
Characteristics of studies identified through the systematicreview are presented in Tables 2, 3, 4, 5, 6. Of the 20 qualita-tive studies included, data collection methods included one-on-one interviews (n = 14), focus groups (n = 2), and com-bined interviews and focus groups (n = 4). Of these 20 studies,ten were conducted in Australia, five in the US, four inCanada, and one in Europe.Most studies focussed on a varietyof cancer types (n = 10), three each on breast and haemato-logical cancers, two on gynaecological cancer, and one eachon prostate and myeloma cancer.
Among quantitative studies, 35 utilised a cross-sectionalstudy design while six studies employed a longitudinal studymethodology. Of these 41 studies, 18 were conducted inAustralia, 16 in the US, six in Europe, and one in Canada.Most studies (n = 18) included participants with heterogenouscancers, eight with breast cancer, five with haematological
Records identified
through Embase
database search
(n = 441)
gnineercSdedulcnI
ytilibigilEnoitacifitnedI
Records after duplicates removed
(n = 4332)
Records screened
(n = 4332)
Records excluded
(n = 4073)
Full-text articles assessed for
eligibility
(n = 259)
Full-text articles excluded,
with reasons
(n = 198):
Not a primary study (n =
11)
Design was not
descriptive/ non-
experimental
(n = 8)
Not described as a rural
cancer population (n =
86)
Not focused on
psychosocial morbidity
or needs (n = 86)
Not a developed country
(n = 4)
Other reasons (n = 3)
Eligible studies for inclusion
(n = 61)
Studies included in
qualitative synthesis
(n = 65)
Records identified
through Medline
database search
(n = 3745)
Records identified
through PsycInfo
database search
(n = 231)
Records identified
through RURAL
database search
(n = 172)
Additional records
identified through
citations
(n = 4)
Figure 1 PRISMA studyselection flowchart
1024 Support Care Cancer (2022) 30:1021–1064
Table2
Qualitativestudiesincludingboth
ruraland
urbansurvivors
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
Studieson
unmetneedsof
cancer
survivors
Jones,
2011
(United
States)
[31]
Cancer
survi-
vors
Qualitativedescriptive
study(hermeneutic
phenom
enological
approach
usingfocus
groups;
semi-structured
interview)
N/A
12urbanand
11urban
African
American
prostatecancer
survivorswererecruitedfrom
community
-based
centres(churches,
barbershops,diners,and
prim
arycare
clinics)in
centralV
irginiaand
Maryland
N/A
Prostatecancer
Twocommon
them
esem
erged:
(1)
family
andphysiciansupportare
important;and(2)insuranceisa
necessity
forappropriatehealthcare;
onemajor
difference
betweenrural
andurbanAfrican
American
prostate
cancer
survivorsem
erged:
rural
participantstalked
moreaboutu
sing
spiritu
ality
throughout
their
diagnosisandtreatm
entthanthose
who
lived
inurbanareas
Very go-
od
Miedema,
2013
(Canad-
a)[32]
Cancer
survi-
vors
Qualitativestudy
(open-ended
interviewsusingthe
Constructivist
GroundedTheory
approach)
N/A
15from
New
Brunswick
and15
from
theGreater
Toronto
Area
Twodistinctareasof
Canada:New
Brunswick,aruralE
astern
Canadian
province,and
Toronto,C
anada’s
largestm
etropolitan
centre
N/A
Various
(1to
5years
post--
diagnosis)
Three
them
esem
ergedfrom
the
analysisof
thedata:(1)
delayed
diagnosis(dismissedcomplaints,
wrong
diagnosis,unusualage
for
diagnosis);(2)
costrelatedto
cancer
treatm
ent(medicationcosts,
part-tim
ework,lack
ofsick
leaveand
limitedhealth
insurancecoverage,
andrelianceupon
parental
assistance);and(3)community
support(benefitevents,mealsand
supportfrom
friends,cancer
organisatio
nsupport);additional
them
ewas
satisfactionwith
care
(lackof
inform
ationandsupport,
regionalissues,top
classcancer
facility,andintensefollo
w-up
screening)
Very go-
od
Wenzel,
2012
(United
States)
[33]
Cancer
survi-
vors
Qualitativestudy
(sem
i-structured
focusgroups)
N/A
28urbanand
20rural
(snowball
sampling)
African
Americansresiding
inaruralarea
inVirginiaor
anurbanarea
inMarylandrecruitedfrom
community
-based
centres
N/A
Various
Four
mainissues
emergedfrom
the
analysisof
thedata:(1)
theneed
for
morehealth-related
and
cancer-specificeducation;
(2)the
importance
offaith
andspiritu
ality
;(3)the
availabilityof
support;and(4)
participants’difficulty
identifying
andarticulatingfinancialn
eeds
Good
Studieson
needsandpsychologicalm
orbidity
Galica,
2020
(Canad-
a)[34]
Cancer
survi-
vors
Qualitativedescriptive
study
(sem
i-structured
N/A
6sm
allu
rban
and9rural
Participantscompleted
treatm
entatthe
CancerCentreof
South-eastern
Ontario
inKingston,Ontario,C
anada
N/A
Ovarian
cancer
(average
time
since
Fivethem
esforcoping
wereexpressed
byallw
omen:(1)
healthcare
provider
support;(2)know
ing,
trustin
g,andprioritisingself;(3)
Very go-
od
1025Support Care Cancer (2022) 30:1021–1064
Tab
le2
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
focusgroups
ortelephoneinterviews)
(conve-
nience
sample)
diagnosiswas
2.7years)
findingwhatw
orks;(4)
uniqueness
andbelonging;
and(5)redirecting
thoughtsandactio
ns.O
neadditio
nal
them
ewas
expressedby
most
wom
en:(6)
preparingforthefuture
Studieson
financialissuesandtravelissues
McG
rath,
2015
(Austra-
lia)[35]
Cancer
patients
Qualitativedescriptive
study(open-ended,
in-depth
interviews)
N/A
5metro,16
regional,14
rural,9
remote,1
interstate
(purposive
sample)
The
studywas
funded
bytheLeukaem
iaFo
undatio
nof
Queensland(LFQ
)Australiaandparticipantswerechosen
from
theLFQ
patient
contactd
atabase
for2012;g
eographicallocation
definedby
distance
toprim
ary
specialistcentres
N/A
Haematological
cancer
Twoim
portantstrategies:(1)visitsby
metropolitan
haem
atologistto
regionalareas(benefits
included
not
having
toexperience
thestress
ofseparatio
nfrom
family
,reductio
nin
theneed
forlengthytravel,regional
hospitalisfamiliar,reductio
nin
the
financialcosto
ftreatm
ent,local
treatm
entw
ithregard
totaking
time
off);and
(2)opportunities
for
haem
atologypatientstoundergopart
orallo
ftheirtreatm
entatregional
hospitals(allo
wspatientsto
stay
with
inthecomfortof
theirow
nhome,physically
less
demanding,
very
convenient
andtim
esaving
for
thosewho
livelocally
,more
convenient,bonds
oftrustand
friendship
with
regionalhealth
professionals,regionalhospitalcan
beaccessed
bycar);lessens
the
emotionalimpactof
diagnosisand
treatm
ent,andpatientsarebetteroff
financially
beingtreatedregionally
Good
McG
rath,
2015
(Austra-
lia)[36]
Cancer
patients
Qualitativedescriptive
study(open-ended,
in-depth
interviews)
N/A
5metro,16
regional,14
rural,9
remote,1
interstate
(purposive
sample)
The
studywas
funded
bytheLeukaem
iaFo
undatio
nof
Queensland(LFQ
)Australiaandparticipantswerechosen
from
theLFQ
patient
contactd
atabase
for2012;g
eographicallocation
definedby
distance
toprim
ary
specialistcentres
N/A
Haematological
cancer
Atthe
pointo
fdiagnosisandalongthe
continuum
oftreatm
ent,the
experience
ofrelocatio
nwas
associated
with
psychosocialstress;
major
issues
werethesenseof
disorientatio
nandbeing
overwhelm
edby
thespeedand
complexity
ofthecity;n
eeds
resulting
from
family
separatio
nare
notalwaysaddressedandwas
describedas
the‘biggest’issue
creatin
gdistress;the
distress
was
not
only
associated
with
lack
ofsupport
Good
1026 Support Care Cancer (2022) 30:1021–1064
Tab
le2
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
andlonelin
essforpatientsbutw
asalso
relatedto
concerns
aboutthe
impactof
separatio
non
family
mem
bersremaining
athome;strong
them
eforthosewho
hadto
relocate
forspecialisttreatmentw
asthesense
ofbeingstuckin
thecity;stoicism
isassociated
with
ruralliving,which
couldtranslateinto
individualsnot
talkingabouttheirlongingto
gohome;manywould
prefer
theoptio
nof
accessingtreatm
entlocally
McG
rath,
2015
(Austra-
lia)[37]
Cancer
survi-
vors
Qualitativedescriptive
study(open-ended,
in-depth
interviews)
N/A
5metro,16
regional,14
rural,9
remote,1
interstate
(purposive
sample)
The
studywas
funded
bytheLeukaem
iaFo
undatio
nof
Queensland(LFQ
)Australiaandparticipantswerechosen
from
theLFQ
patient
contactd
atabase
for2012;g
eographicallocation
definedbasedon
thegovernment
schemeforassistingpatientswith
travelandaccommodation(The
Patient
TransitSu
bsidySchem
e=PTSS)
N/A
Haematological
cancer
Eightthem
esem
ergedfrom
theanalysis
ofthedata:(1)
thechallengeof
accessingtreatm
entfrom
adistance;
(2)strategies
forovercomingthe
distance
barrier,includingwhat
works
nowandideasforthefuture;
(3)theim
portance
ofworkissues
for
both
thepatient
andtheirfamily
;(4)
theadditio
nalcostsof
relocatio
nand
treatm
ent;(5)the
factorscontributin
gtofinancialdistressandhardship;(6)
thefinancialb
uffers;(7)
the
possibility
ofaspiralto
poverty;
and
(8)thecontributio
nof
Leukaem
iaFo
undatio
nof
Queensland’s
supportiv
ecare
servicedeliv
eryto
amelioratin
gtheim
pactof
relocatio
n
Good
1027Support Care Cancer (2022) 30:1021–1064
Table3
Qualitativestudiesincludingonly
ruralsurvivors
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
Studieson
theuseof
form
alandinform
almentalh
ealth
resources
Gunn,
2013
(Austra-
lia)[38]
Cancer
survi-
vors
Qualitativestudy
(sem
i-structured,
face-to-face,hour-long
interviews)
N/A
17Participantswererecruitedthrough
CancerCouncilSo
uthAustralia’s
supportedaccommodation
facilities,theruralm
ediaand
personalcontacts;rurality
was
definedby
the
Accessibility/Rem
otenessIndex
ofAustralia(A
RIA
)
N/A
Various
The
them
esidentifiedcouldbe
split
into
twobroadcategories:(A)
Issues
intheprovisionof
psychosocialcare:(1)
psychosocialsupportishighly
valued
bythosewho
have
accessed
it;(2)having
access
toboth
layandprofessional
psychosocialsupportisvitally
important;(3)accessing
psychosocialservices
ismade
difficultbyseveralbarrierssuch
aslack
ofinform
ationaboutservices,
initialbeliefsthey
are
unnecessary,feeling
overwhelm
ed,and
concerns
about
stigmaanddualrelatio
nships;(4)
medicalstafflocatedin
metropolitan
treatm
entcentres
are
notsufficiently
awareof
the
unique
needsof
ruralp
atients;(5)
patientsrequirebetteraccess
topsychosocialservices
post-treatment;(B)How
the
provisionof
psychosocialcare
couldbe
improved:(1)
providing
morerural-specificinform
ationon
psychosocialcare;(2)
improving
communicationbetween
healthcare
providersandreferral
topsychosocialservices;(3)
makingpsychosocialservices
astandard
partof
care
Very go-
od
Pascal,
2014
(Austra-
lia)[39]
Cancer
survi-
vors
Qualitativedescriptivestudy
(in-depthinterviews)
N/A
19(purposive
sampling)
The
samplewas
draw
nfrom
the
geographicsetting
with
inthe
Loddon-Malleeregion
ofCentral
Victoria,Australia;rurality
was
definedby
theAustralianInstitu
teof
Health
andWelfare
definitio
n
N/A
Various
(2years
post--
treatm
ent)
Psychosocialcare
provisionunmet
needsincluded
feelingletd
own
byform
alserviceprovision,sense
ofisolation,lack
ofaccess
topsychosocialcare,lackof
inform
ationandreferrals,lack
offollo
w-upcare,inaccessibilityof
services
dueto
distance
costor
waittim
es,and
lack
ofappropriate
Good
1028 Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
carebasedon
age,stage,ortype
ofcancer;u
nmetneedsbasedon
professionalpsychosocialsupport
werebasedon
luck
ofgetting
support,or
having
family
mem
bers/friends,w
hohad
professionalor
medical
know
ledge;thereisamajor
gapin
psychosocialcare
provision
Studieson
unmetneedsof
cancer
survivorsandpatientsin
palliativecare
Adams,
2017
(United
States)
[40]
Cancer
survi-
vors
Qualitativestudy(focus
groups
andin-depth
interviews,using
semi-structured)
N/A
15Participantswho
lived
inoneof
three
ruralB
lack
Beltcountiesin
Alabamarecruitedthroughthe
Com
munity
Health
Advisorsas
ResearchPartner
(CHARP)
network;
ruralitynotd
efined
N/A
Wom
enwith
breastcancer
(average
5yearsin
survivorship)
Four
overarchingthem
esem
erged
during
theanalysisof
thedata:(1)
cancer
isasecret;(2)
perish
with
lack
ofknow
ledge;(3)startw
itha
good
prayer
life;and(4)lim
ited
survivorship
supportand
education;
thesefour
them
escan
furtherbe
dividedinto
thirteen
subthemes,asfollo
ws:(1)fatalism
atdiagnosis,delayin
treatm
ent,
fear
ofdisclosure;(2)
whatis
lymphedem
a,whatare
theside
effectsof
horm
onaltherapy,
sexuality
andbody
image,fatig
ue,
fearof
weightloss,depression;(3)
relig
ionandspiritu
ality
;and
(4)
family
/friendsupport,education
andsupport,cancer
surveillance,
awarenessof
breastcancer
advocacy
Good
Allen,
2014
(United
States)
[41]
Cancer
survi-
vors
Qualitativestudy
(face-to-faceor
telephone
interviews,
semi-structured
open-ended
interviews
grounded
inasocial
constructio
nisttheoretical
fram
ework)
N/A
20RuralAppalachiarecruitedfrom
cancer
centres:Southwestand
WestV
irginia
N/A
Gynaecological
cancer
The
studyprovides
threenew
perspectives:(A)participants
follo
wed
four
differentroutesin
learning
they
hadcancer:(1)
receivingadiagnosisim
mediately
upon
suspectin
gsymptom
s;(2)
enduring
aseries
oftestsand
waitin
gup
toayear
for
confirmation;
(3)liv
ingwith
the
suspicionthatsomething
was
wrong
butd
elayed
medical
confirmationuntil
aftermeetin
gfamily
responsibilities;(4)having
Very go-
od
1029Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
theircancer
discovered
during
routinegynaecologicalexam
;(B)
There
was
greatv
ariatio
nam
ong
thewom
enin
theirbeliefsabout
cancer
andfour
differentp
atterns
ofcancer
survivorship
were
revealed:(1)
positiv
eattitude;(2)
cautious;(3)
distanced;
(4)
resigned;and
(C)Alth
ough
not
everywom
enresonatedwith
beingacancer
survivor,every
wom
endidperceive
herselfto
bestrong
andfeltsupportedby
strong
family
tiesandstrong
connectio
nsto
higher
power
Coyne,
2019
(Austra-
lia)[42]
Cancer
survi-
vors
Qualitativestudy(in-depth
telephoneinterviews)
200 invited;
16 complet-
ed consent;
14 complet-
ed inter-
view
s
8survivorsand
6family
mem
bers
The
participantsforthisstudy
residedin
ruralQ
ueenslandand
hadstayed
inCancerCouncil
Queensland[CCQ]
accommodationduring
treatm
ent;
ruralisdefinedas
livingup
toand
over
180km
away
from
amajor
city
N/A
Various
Three
them
esem
ergedfrom
the
analysisof
thedata:(1)
confrontingdiagnosis,i.e.,the
initialshock,senseof
disbelief,
working
throughtheshock,and
theim
portance
ofsupportatthis
time,was
imperativ
e;(2)
challenges,i.e.,getting
through
thetreatm
ent,travellin
gto
and
from
treatm
ent;and(3)
negotiatin
gsupport,i.e.,person
with
cancer
feltconcernedabout
beingaburden
totheirfamily
and
inform
ationwas
achallengeas
itwas
notalwaysattheirlevelo
funderstanding(included
community
,spiritual,and
instrumentalsupport)
Very go-
od
Devik,
2013
(Norwa-
y)[43]
Cancer
patients
in pallia-
tive
care
Qualitativestudy
(interview
s;combined
phenom
enological
philo
sophywith
herm
eneutic
interpretatio
n)
N/A
5Contactwas
mediatedthroughan
oncologicpoliclin
icin
alocal
hospitalinNorway;the
participantsresidedin
communities
(bothmountainand
coastal)with
lowpopulatio
ndensity
;rangedfrom
920to
7775
N/A
Various
(incurable
cancer,
receiving
life--
prolonging
chem
othera-
py)
Four
them
esem
ergedfrom
the
analysisof
thedata:(1)
enduring
bykeepinghope
alive(subthem
es:
having
confidence
intheexpertise
atthepoliclin
ic,copingwith
conflictin
gfeelings,dream
ingand
makingplans);(2)
becoming
awarethatyouareyour
own
(subthem
e:navigatin
galone);(3)
livingup
toexpectations
ofbeing
Very go-
od
1030 Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
agood
patient
(subthem
e:having
limitedcontrol,becominga
burden);and(4)beingatrisk
oflosing
identityandvalue
(subthem
e:beingin
decline,
losing
dignity
,losingcontinuity)
Duggleby,
2011
(Canad-
a)[44]
Cancer
patients
in pallia-
tive
care
Qualitativestudy
(open-endedinterviews
andfocusgroups
defined
ingrounded
theory)
N/A
6patients,10
family
caregivers,
and12
rural
healthcare
professionals
(purposive
sampling)
The
palliativecarecoordinatorsfrom
the3ruralh
ealth
regionsin
western
Canadacontacted
participants,self-reported
toliv
ein
aruralarea
N/A
Various
Four
them
esem
ergedfrom
the
analysisof
thedata:(1)
community
connectedness/isolation
(participantsdescribedfeeling
connectedto
theircommunity
aspartof
thesocialcontextb
utalso
isolated,ruralhealthcareproviders
connectedthroughliv
ingand
working
with
peoplethey
knew
both
personally
and
professionally);(2)lack
ofaccessibilitytocare(lackofaccess
topalliativecareservices
andlack
ofcontinuity
ofcare);(3)
communicationandinform
ation
issues
(poorcommunicationwith
healthcare
providersresultedin
palliativepatientsandtheirfamily
mem
bersperceiving
thatthey
werelackingim
portant
inform
ationregardingtheircare);
and(4)independence/dependence
(sharedsensethatpalliative
patients,together
with
their
inform
alandform
alcaregivers,
felttheneed
forretainingthe
patient’ssenseof
independence
asthey
becamemoredependento
nothers)
Very go-
od
Garrard,
2017
(Austra-
lia)[45]
Cancer
patients
and
their
family
Qualitativestudy
(sem
i-structured
interviewsbasedupon
the
Resilience
Modelof
Fam
ilyAdjustm
entand
Adaption)
N/A
10families,34
patientstotal
Participantswererecruitedviaa
mediareleaseandby
rurally
based
doctors;postcode
as‘outer
regional’accordingto
the
Accessibility/Rem
otenessIndex
ofAustralia(A
RIA
)
N/A
Not
reported
Three
keychallenges
were
identified:
(1)frequent
travel;(2)
increasedwork/financial
demands;and
(3)family
separatio
n;protectiv
einternal
factorswerean
adaptiv
ecommunicationapproach,
Very go-
od
1031Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
strength
offamily
relatio
nships
andits
value,andfamily
’sability
toproblem-solve
toprom
ote
norm
ality
;protectiveexternal
factorswereavailabilityand
engagemento
fcommunity
support,andtheability
toaccess
professionalsupportservices
Grimison.
2013
(Austra-
lia)[46]
Cancer
patients
Qualitative(focus
groups
andstructured
interviews
viatelephoneor
face-to-face)
N/A
36patients,14
carers,and
32health
professionals
New
South
Wales,A
ustraliaatfour
ruraland
regionalhospitalsand
threemetropolitan
locatio
ns;rural
area
definedby
Accessibility/remotenessindexof
Australia(A
RIA
)
N/A
Various
(diagnosed
inthelast2
years)
Sixthem
esem
ergedfrom
the
analysisof
thedata:(1)
access
tohealthcare
professionals;(2)
accesstoservices
forinvestig
ation
andtreatm
ent;(3)traveland
accommodation;
(4)quality
oftreatm
ent;(5)inform
ationand
supportn
eeds;and
(6)experience
ofhealthcare
professionals
Good
Loughery,
2019
(Canad-
a)[47]
Cancer
survi-
vors
Qualitativeinterpretiv
estudy
(open-ended,
semi-structured
interviews,face-to-face)
N/A
20(purposive
sampling)
Ruralor
northareasof
Manito
ba,
Canada
N/A
Wom
enwith
breastcancer
Findings
accordingtothedomains
ofthesupportiv
ecarefram
ework:(1)
physical:travelling
andaccess
toexperiencedandqualifiedhealth
professionalsresultedin
additio
nalb
urdens
onfamily
and
friends;however,the
positiv
erolesof
theruralcancerprogram
helped
manytransitio
nthrough
thephysicaldemands
thatwere
encountered;
(2)inform
ation:
numberof
factorsim
pacted
the
ability
toprocesstheinform
ation
such
asescalatin
gfears,long
traveldays,and
lack
ofasupport
person
availableto
attend
the
appointm
ent;(3)social:living
alonewas
positiv
eandnegativ
e,nurses
areim
portantinrural
setting,strongsenseof
community
butlackof
anonym
ityandinvasion
ofprivacy;
(4)
practical:b
urdenof
extensive
travel,relocation,em
ployment
challenges,and
financiallosses;
(5)em
otional:shock,disbelief,
Good
1032 Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
denial,fear,uncertainty,anger,
guilt,feelin
gsof
anxiety,and
travelburden;(6)
psychological:
loss
ofcontrolo
vertheillness
experience,alteredbody
image
relatedto
hairloss,ordecreased
self-esteem;(7)
spiritu
al:as
difficultasthejourneywas,itw
asoftendescribedas
atim
efor
discovery
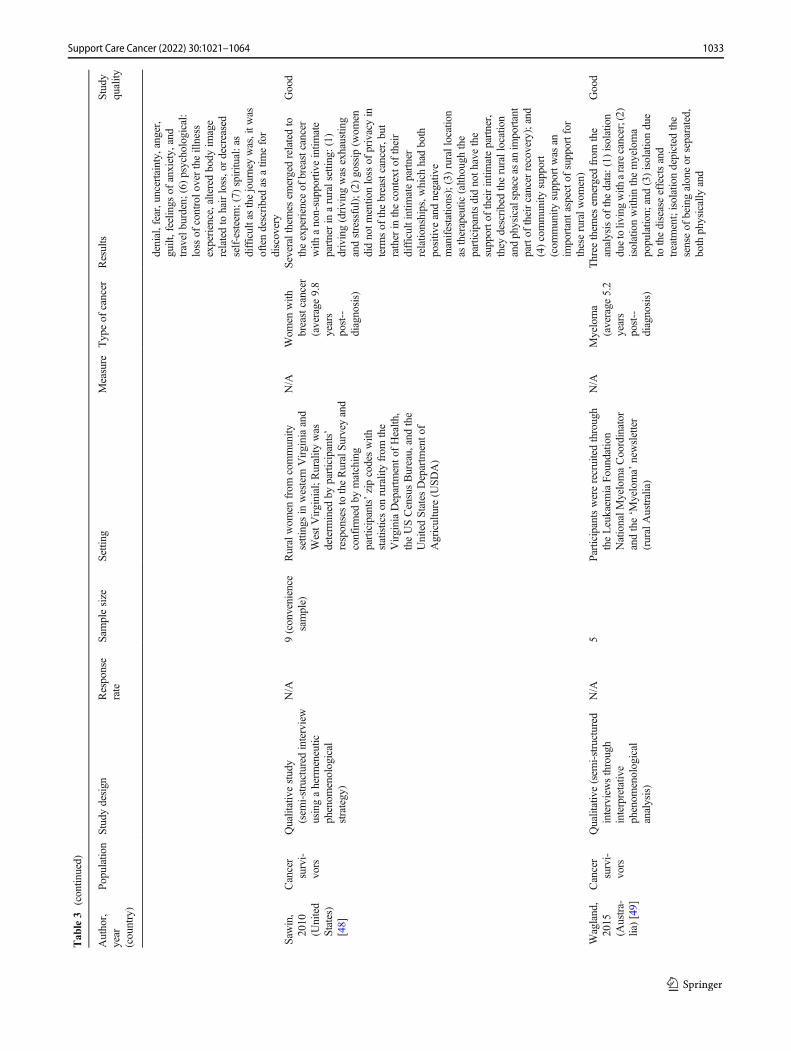
Saw
in,
2010
(United
States)
[48]
Cancer
survi-
vors
Qualitativestudy
(sem
i-structured
interview
usingaherm
eneutic
phenom
enological
strategy)
N/A
9(convenience
sample)
Ruralwom
enfrom
community
settingsin
western
Virginiaand
WestV
irginial;R
urality
was
determ
ined
byparticipants’
responsestotheRuralSu
rvey
and
confirmed
bymatching
participants’zipcodeswith
statisticson
ruralityfrom
the
VirginiaDepartm
ento
fHealth
,theUSCensusBureau,andthe
UnitedStates
Departm
ento
fAgriculture
(USD
A)
N/A
Wom
enwith
breastcancer
(average
9.8
years
post--
diagnosis)
Severalthemes
emergedrelatedto
theexperience
ofbreastcancer
with
anon-supportiv
eintim
ate
partnerin
aruralsettin
g:(1)
driving(driving
was
exhaustin
gandstressful);(2)
gossip
(wom
endidnotm
entio
nloss
ofprivacyin
term
sof
thebreastcancer,but
rather
inthecontexto
ftheir
difficultintim
atepartner
relatio
nships,w
hich
hadboth
positiv
eandnegativ
emanifestatio
ns);(3)rurallocation
astherapeutic
(alth
ough
the
participantsdidnoth
avethe
supporto
ftheirintim
atepartner,
they
describedtherurallocation
andphysicalspaceas
anim
portant
partof
theircancer
recovery);and
(4)community
support
(com
munity
supportw
asan
importantaspecto
fsupportfor
theseruralw
omen)
Good
Wagland,
2015
(Austra-
lia)[49]
Cancer
survi-
vors
Qualitative(sem
i-structured
interviewsthrough
interpretativ
ephenom
enological
analysis)
N/A
5Participantswererecruitedthrough
theLeukaem
iaFo
undatio
nNationalM
yelomaCoordinator
andthe‘M
yeloma’
newsletter
(ruralAustralia)
N/A
Myeloma
(average
5.2
years
post--
diagnosis)
Three
them
esem
ergedfrom
the
analysisof
thedata:(1)
isolation
duetoliv
ingwith
ararecancer;(2)
isolationwith
inthemyeloma
populatio
n;and(3)isolationdue
tothediseaseeffectsand
treatm
ent;isolationdepicted
the
senseof
beingaloneor
separated,
both
physically
and
Good
1033Support Care Cancer (2022) 30:1021–1064
Tab
le3
(contin
ued)
Author,
year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
psychologically
,from
potential
sourcesof
support
Studieson
needsandquality
oflife
Gunn,
2021
(Austra-
lia)[50]
Cancer
survi-
vors
and
their
carers
Qualitative(sem
i-structured,
face-to-face
interviews
throughthem
aticanalysis)
N/A
22Participantsexpressedinterestin
participatingin
response
tomedia
articles,posters,andnotices;rural
area
definedby
Accessibility/remotenessindexof
Australia(A
RIA
)
N/A
Various
(1–5
years
post--
treatm
ent)
Studyconsistedof
twoparts;partA
investigated
theim
pactof
post-treatmentchallenges
onquality
oflifeandfoundfour
overarchingthem
es:(1)
quality
oflifeisnotrestoredaftertreatm
ent
completion,e.g.,fearof
recurrence
andfeelingdepressed
orfatig
ued;
(2)lack
ofconfidence
inruralh
ealth
services’ability
tohelp
addresspost-treatment
quality
oflife;(3)challenges
with
returningto
metropolitan
centres,
such
astim
eaw
ayandfinancial
costs;and(4)mostsupport
provided
byfamily
,friend,nurses,
andsupportg
roups.PartB
investigated
howquality
oflife-relatedneedscouldbe
better
addressedandfoundsix
overarchingthem
es:(1)
engage
with
telephoneor
face-to-face
services;(2)
serviced
need
toreachout;(3)barrierstoaccessing
supportv
iainternet-based
programsstill
exist;(4)continuity
ofcare
highly
valued;(5)
nurses
areappropriateto
deliv
erpost-treatment,quality
oflife-focussed
support;and(6)
telehealth
ispopularalternativeto
face-to-face
appointm
ents
Very go-
od
1034 Support Care Cancer (2022) 30:1021–1064
Table4
Quantitativ
estudieswith
ruraland
urbancomparisongroups
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
Studieson
theuseof
form
alandinform
almentalh
ealth
resources
Andykow
ski,
2010
(United
States)[51]
Cancer
survivors
Cross-sectio
nal
34%
51ruraland
62 nonrural
Cancersurvivorswererecruited
from
thestate-wide,
population-basedKentucky
SEERCancerR
egistry(K
CR);
therural-nonruraldistinction
was
definedby
objective,
geographic,and
population-basedcriteria:2003
UnitedStates
Departm
ento
fAgriculture
(USD
A)
Rural-U
rban
Continuum
(RUC)Codes
The
MentalH
ealth
Resource
Questionnaire(M
HRQ)
Femalebreast
cancer,
colorectalor
haem
atological
cancer;1
to5
years
post-diagnosis
Ruralsurvivorswerelesslik
elyto
reportapsychologist(χ
2=
8.40,p
<0.01)or
support
group(χ
2=9.20,p
<0.01)
with
in30
milesof
home;rural
survivorswereless
likelyto
reportthey
couldaccess
asupportgroup
ifthey
wantedto
(χ2=4.56,p
<0.05);rural
cancer
survivorsreported
less
favourablepersonalattitudes
regardingtalkingto
friends/family
aboutemotional
difficulties(t(111)
=2.31;p
<0.05);ruralsurvivorsreported
less
favourablesocialnorm
sregardingaddressing
emotionald
ifficulties
bytalkingto
friends/family
(t(111)
=2.04;p
<0.05)or
participatinginasupportgroup
(t(111)
=2.17;p
<0.05);rural
survivorsreported
less
favourableattitudes
(t(111)
=2.05;p
<0.05)andsocial
norm
s(t(111)
=2.20;p
<0.05)
regardingMHresource
usage
Very goo-
d
Beraldi,2015
(Germany)
[52]
Cancer
patients
Cross-sectio
nal
89%
251ruraland
283urban
Datawas
obtained
from
the
MunichCancerRegistry;
ruralitywas
categorisedin
asimilarw
ayas
theRural-U
rban
Contin
uum
(RUC)Code,
consideringtheregional
conditionsof
Southern
Germany
Distresswas
evaluatedusingthe
DistressTherm
ometer(D
T)
andtheStress
inCancer
Patients(Q
SC-R10);
depression
andanxietywere
evaluatedby
thePatientHealth
Questionnaire(PHQ-4)
Colorectalcancer;
3monthsafter
surgery
Urban
patientstalked
less
with
theirdoctor
abouttheir
emotionalstate(65%
,p<0.01)
andshow
edpoorerknow
ledge
ofcancer-specificmental
health
resources(60%
,p<
0.002);a
good
doctor-patient
relatio
nshipwas
associated
with
abettermentalh
ealth
outcom
e;asignificant
predictorforacceptance
was
distress;9
4%of
patients
with
outa
nearby
support
facilitylived
inruralareas
(p<
0.001);there
wereno
group
differencesconcerning
distress,m
entalh
ealth
outcom
es,oracceptance
of
Very goo-
d
1035Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
cancer-specificmentalh
ealth
resources
Corboy,
2014
(Australia)
[53]
Cancer
survivors
Cross-sectio
nal
31%
286major
cities,104
inner
regional,
46outer
regional,
8remote,
3very
remote
Registeredwith
Australia
Medicare;geographic
remotenesswas
measuredas
acontinuous
variable,using
the
Accessibility/Rem
oteness
Indexof
Australia(A
RIA
+)
The
Liverpool
Stoicism
Scale
(LSS
);theNeedforControl
andSelf-reliancesubscaleof
theBarriersto
HelpSeeking
Scale
Australianmen
who
had
undergonea
radical
prostatectom
yas
treatm
entfor
prostatecancer;
9.11
months
post-diagnosis
Anincrease
ingeographic
remotenesswas
associated
with
adecrease
inintentions
touseatelephone-basedsupport
service;geographic
remotenessdidnotp
redict
perceivedbehaviouralcontrol;
relatio
nshipbetween
geographicremotenessand
intentionto
usea
telephone-basedsupport
servicewas
partially
mediated
bystoicism
andsubjectiv
enorm
s(r=−0
.04,p<0.001);a
significantd
irectp
ath
indicatedthatstoicism
significantly
increasedwith
distance
from
metropolitan
areas
Very goo-
d
Studieson
unmetneedsof
cancer
survivorsandsupportp
ersons
Ahern,2015
(Australia)
[54]
Cancer
survivors
Cross-sectio
nal
(10-year
replication
study)
81%
224major
cities,62
inner
regional,
39outer
regional,
remote,or
very
remote
Participantsweresourcesfrom
twoAustraliandatabases:
Register4
andtheBCNA
ReviewandSu
rvey
Group;
ruralitywas
definedby
the
AustralianBureauof
Statistics
(ABS)
Rem
otenessArea(RA)
code
Studyused
apreviouslyvalidated
survey;six
questions
were
added
Australianwom
enwith
breast
cancer
who
had
been
diagnosed
between6and
30months
before
thestart
ofthestudy
Therewereno
statistically
significantdifferences
foundin
inform
ationissues
received
andsatisfactionwith
sourcesof
supportb
ased
ongeographic
locatio
n;percentagesof
wom
enusingthenewspaperas
aninform
ationsource
was
statistically
significantlow
er(χ
2=8.033,p=0.018)inouter
regional,rem
ote,andvery
remoteareas(n
=8,21%)
comparedto
major
cities(n
=91,41%
)andinnerregional
areas(n
=30,48%
);a
statistically
significant
difference
was
foundwith
the
breastcancer
nurseas
asource
ofsupport(χ2=6.253,p=
0.044)atahigherpercentage
intheouterregional,rem
ote,and
very
remoteareas(16/39,
41%)comparedto
major
cities
Good
1036 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
(50/224,22%)andinner
regionalareas(17/62,27%
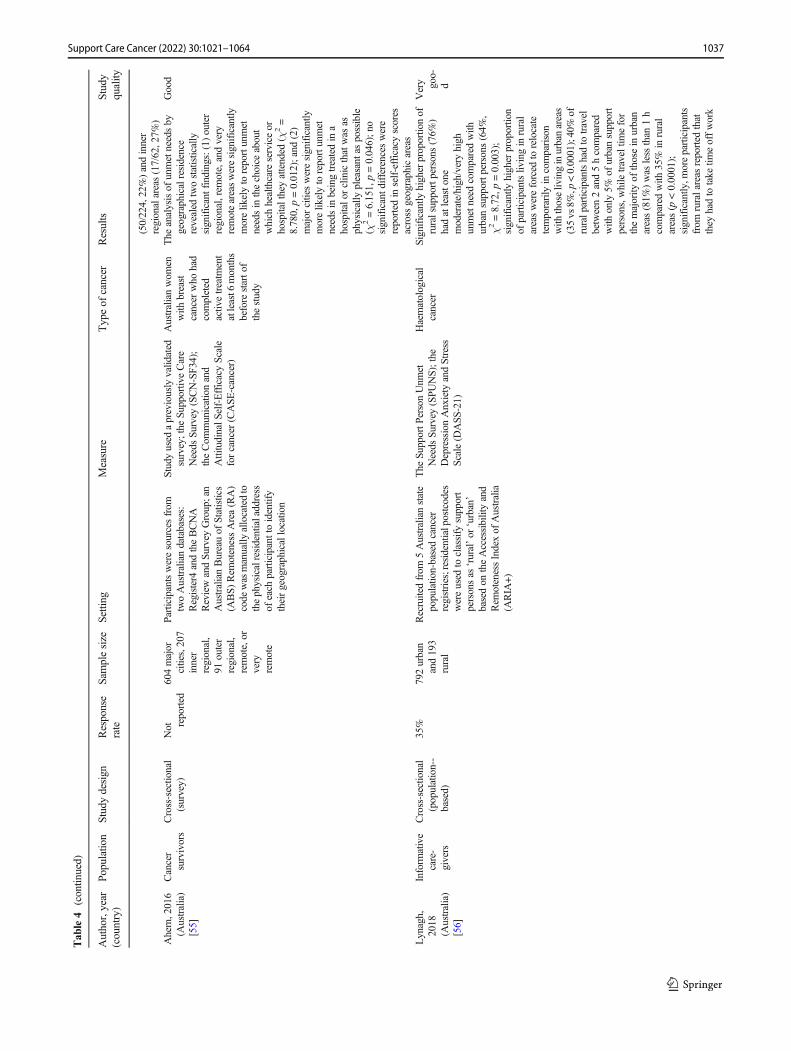
)Ahern,2016
(Australia)
[55]
Cancer
survivors
Cross-sectio
nal
(survey)
Not re
ported
604major
cities,207
inner
regional,
91outer
regional,
remote,or
very
remote
Participantsweresourcesfrom
twoAustraliandatabases:
Register4
andtheBCNA
ReviewandSu
rvey
Group;an
AustralianBureauof
Statistics
(ABS)
Rem
otenessArea(RA)
code
wasmanually
allocatedto
thephysicalresidentialaddress
ofeach
participanttoidentify
theirgeographicallocatio
n
Studyused
apreviouslyvalidated
survey;the
Supportiv
eCare
Needs
Survey
(SCN-SF3
4);
theCom
municationand
AttitudinalS
elf-EfficacyScale
forcancer
(CASE
-cancer)
Australianwom
enwith
breast
cancer
who
had
completed
activ
etreatm
ent
atleast6
months
before
starto
fthestudy
The
analysisof
unmetneedsby
geographicalresidence
revealed
twostatistically
significantfindings:(1)outer
regional,rem
ote,andvery
remoteareasweresignificantly
morelik
elyto
reportunmet
needsin
thechoice
about
which
healthcare
serviceor
hospitaltheyattended
(χ2=
8.780,p=0.012);and
(2)
major
citiesweresignificantly
morelik
elyto
reportunmet
needsin
beingtreatedin
ahospitalo
rclinicthatwas
asphysically
pleasant
aspossible
(χ2=6.151,p=0.046);n
osignificantd
ifferences
were
reported
inself-efficacyscores
across
geographicareas
Good
Lynagh,
2018
(Australia)
[56]
Inform
ative
care-
givers
Cross-sectio
nal
(population--
based)
35%
792urban
and193
rural
Recruitedfrom
5Australianstate
population-basedcancer
registries;residentialpostcodes
wereused
toclassify
support
personsas
‘rural’or
‘urban’
basedon
theAccessibilityand
Rem
otenessIndexof
Australia
(ARIA
+)
The
SupportP
ersonUnm
etNeeds
Survey
(SPU
NS);the
DepressionAnxiety
andStress
Scale(D
ASS
-21)
Haematological
cancer
Significantly
higherproportio
nof
ruralsupportpersons(76%
)hadatleasto
nemoderate/high/veryhigh
unmetneed
comparedwith
urbansupportp
ersons
(64%
,χ2=8.72,p
=0.003);
significantly
higher
proportio
nof
participantsliv
ingin
rural
areaswereforced
torelocate
temporarily
incomparison
with
thoseliv
inginurbanareas
(35vs
8%,p
<0.0001);40%
ofruralp
articipantshadto
travel
between2and5hcompared
with
only
5%of
urbansupport
persons,whiletraveltim
efor
themajority
ofthosein
urban
areas(81%
)was
less
than
1h
comparedwith
35%
inrural
areas(p
<0.0001);
significantly
,moreparticipants
from
ruralareas
reported
that
they
hadto
take
timeoffwork
Very goo-
d
1037Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
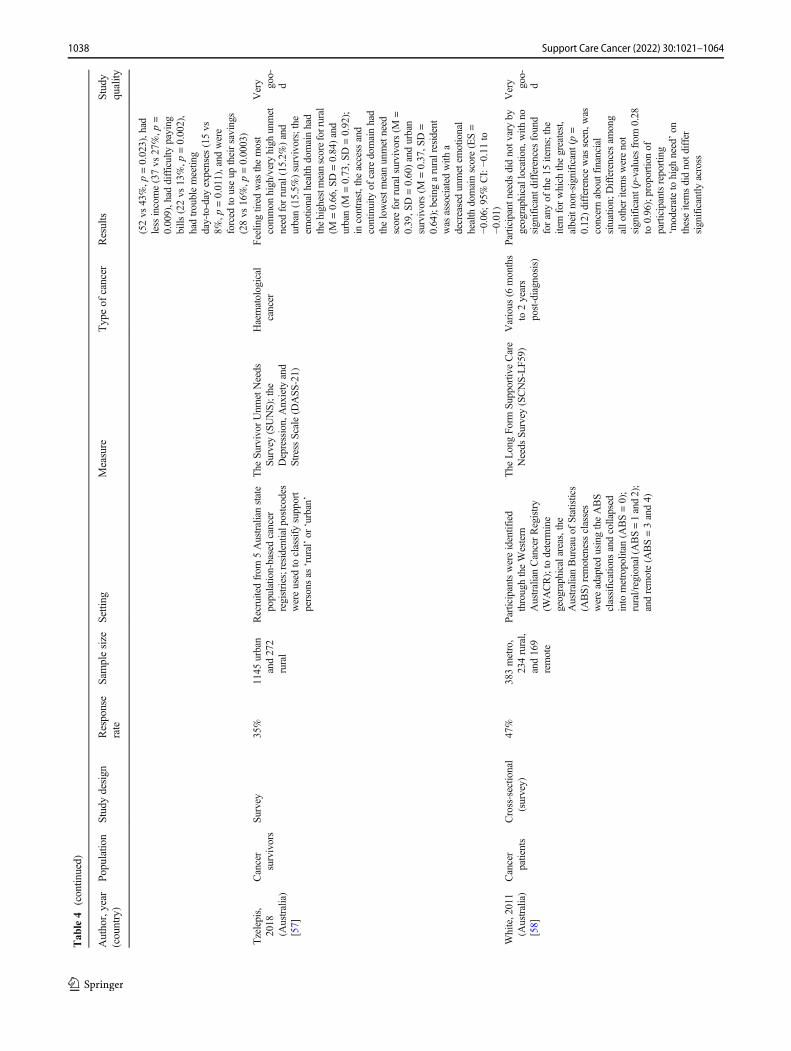
(52vs
43%,p
=0.023),had
less
income(37vs
27%,p
=0.009),had
difficulty
paying
bills
(22vs
13%,p
=0.002),
hadtroublemeeting
day-to-day
expenses
(15vs
8%,p
=0.011),and
were
forced
touseup
theirsavings
(28vs
16%,p
=0.0003)
Tzelepis,
2018
(Australia)
[57]
Cancer
survivors
Survey
35%
1145
urban
and272
rural
Recruitedfrom
5Australianstate
population-basedcancer
registries;residentialpostcodes
wereused
toclassify
support
personsas
‘rural’or
‘urban’
The
Survivor
Unm
etNeeds
Survey
(SUNS);the
Depression,Anxiety
and
Stress
Scale(D
ASS
-21)
Haematological
cancer
Feelin
gtired
was
themost
common
high/veryhigh
unmet
need
forrural(15.2%)and
urban(15.5%
)survivors;the
emotionalh
ealth
domainhad
thehighestm
eanscoreforrural
(M=0.66,S
D=0.84)and
urban(M
=0.73,S
D=0.92);
incontrast,the
access
and
continuity
ofcare
domainhad
thelowestm
eanunmetneed
scoreforruralsurvivors(M
=0.39,S
D=0.60)andurban
survivors(M
=0.37,S
D=
0.64);beingaruralresident
was
associated
with
adecreasedunmetem
otional
health
domainscore(ES=
−0.06;
95%
CI:−0
.11to
−0.01)
Very goo-
d
White,2011
(Australia)
[58]
Cancer
patients
Cross-sectio
nal
(survey)
47%
383metro,
234rural,
and169
remote
Participantswereidentified
throughtheWestern
AustralianCancerRegistry
(WACR);to
determ
ine
geographicalareas,the
AustralianBureauof
Statistics
(ABS)
remotenessclasses
wereadaptedusingtheABS
classifications
andcollapsed
into
metropolitan
(ABS=0);
rural/regional(ABS=1and2);
andremote(A
BS=3and4)
The
LongFo
rmSu
pportiveCare
Needs
Survey
(SCNS-LF5
9)Various
(6months
to2years
post-diagnosis)
Participantn
eeds
didnotv
aryby
geographicallocation,with
nosignificantd
ifferences
found
foranyof
the15
items;the
item
forwhich
thegreatest,
albeitnon-significant(p=
0.12)difference
was
seen,w
asconcernaboutfinancial
situation;
Differences
among
allo
ther
itemswerenot
significant(p-values
from
0.28
to0.96);proportio
nof
participantsreporting
‘moderateto
high
need’on
theseitemsdidnotd
iffer
significantly
across
Very goo-
d
1038 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
geographicalpopulatio
ns(p-valuesfrom
0.13
to0.91)
Studieson
needsandquality
oflife
Cahir,2017
(Ireland)
[59]
Cancer
survivors
Cross-sectio
nal
66%
698ruraland
870urban
Wom
enwith
breastcancer
were
identifiedinAugust2015from
theNationalC
ancerRegistry
Ireland(N
CRI)database;a
compositemeasure
ofurban–ruralclassificationwas
createdusingthreeindicators;
settlem
entsize,populatio
ndensity
,and
proxim
ityto
treatm
enth
ospital
The
Functio
nalA
ssessm
ento
fCancerT
herapy
(FACT-G
);an
endocrinesubscale(ES)
Wom
enwith
breastcancer
1–5years
post-diagnosis
The
associationbetween
urban–ruralresidence/status
andQOLandendocrine
symptom
swas
assessed
using
linearregression
with
adjustmentfor
sociodem
ographicandclinical
covariates;inmultiv
ariable
analysis,ruralsurvivorshada
statistically
significanth
igher
overallQ
OL(β
=3.81,
standard
error(SE1.30,p
<0.01),em
otionalQ
OL(β
=0.70,S
E0.21,p
<0.01),and
experiencedalower
symptom
burden
(β=1.76,S
E0.65,p
<0.01)than
urbansurvivors
Very goo-
d
Pateman,
2018
(Australia)
[60]
Cancer
patients
Prospectivestudy
with
baselin
e(prior
totreatm
ent),1
month,and
6months
post-treatment
86% ba
selin
eand
56.8%
lostto
follo
w--
up
48major
city,25
inner
regional.
18outer
regional,
3remote,
1very
remote
Tertiary
hospitalinBrisbane,
Australia;rurality
was
classified
accordingto
the
AustralianStandard
Geographic
Classification-Rem
oteness
Area(A
SCG-RA)system
The
University
ofWashington
Qualityof
LifeSu
rvey
(UW-Q
OL)
New
lydiagnosed
patientswho
werereferred
for
thediagnosis,
and/or
treatm
ent
ofhead
and
neck
cancer
Atb
aseline,theregional/rem
ote
groupscored
significantly
worse
inthepain
domain
comparedwith
the
metropolitan
group(p
=0.031);P
osth
ocχ2testsdid
notreveala
significant
difference
betweenurbanand
regional/rem
otegroups
for
tumour-relatedvariables,such
asstaging;
therewas
atrend
towards
lower
scores
inthe
globalQOLam
ongthe
regional/rem
otegroupatall
threetim
epoints;h
owever,
thisassociationdidnotreach
statisticalsignificance
Very goo-
d
Pedro,2014
(United
States)[61]
Cancer
survivors
Cross-sectio
nal
(survey)
35%
for
RUCC
7,31%
for
RUCC
8,and
41%
for
RUCC
9
49RUCC7,
28RUCC
8,14
RUCC9
Participantswererecruitedfrom
theColoradoCentralCancer
Registry(CCCR);ruralitywas
basedon
the2003
Rural-U
rban
Contin
uum
Codes
(RUCCs):
RUCC7(urban
populationof
2,500–19,999,not
adjacent
toametro
area),RUCC8
(com
pleteruralityor
less
than
The
RosenbergSelf-EsteemScale
(RSE
S);the
PersonalResource
Questionnaire
(PRQ)2000,a
measure
ofsocialsupport;and
theEuropeanOrganisationfor
theResearchandTreatmento
fCancerQ
ualityof
LifeCore30
(EORTCQLQ-C30)
Various
Asignificantd
ifferencewas
notedbetweenRUCC7and
RUCC9in
socialfunctio
ning
(β=−0
.25,p<0.05),
symptom
-related
QOL(β
=0.26;p
<0.05),andfinancial
difficulties(β
=0.31,p
<0.05);
thoseresiding
inRUCC7
reported
poorer
social
Very goo-
d
1039Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
2,500urbanpopulation,
adjacent
toametro
area),and
RUCC9(com
pleteruralityor
less
than
2,500urban
populatio
n,notadjacenttoa
metro
area)
functio
ning
scores,w
orse
symptom
score,andgreater
financiald
ifficulties
than
those
residing
inRUCC9;
differencesbetweenRUCC8
andRUCC9follo
wed
asimilarpattern,but
RUCC8
reportingmoresymptom
s(β
=0.31,p
<0.05);self-esteem
andsocialsupportstrongly
correlated
with
HRQOL
Thomas,
2014
(Ireland)
[62]
Cancer
survivors
Cross-sectio
nal
(population
survey)
59%
361urban
and214
rural
The
NationalC
ancerRegistry
Irelandwas
used;3
composite
measuresfordefining
rurality
wereused:self-reported
area,
distance
from
theparticipant’s
currentresidence
tothe
hospitalfrom
theregistry,and
populationdensity
The
Functio
nalA
ssessm
ento
fCancerTherapy
(FACT-G
)—
specificto
head
andneck
cancer
survivors(FACT-H
N)
Headandneck
cancer(atleast8
months
post-diagnosis)
Controllin
gfordemographicand
clinicalvariables,rural
survivorsreported
higher
physical(coefficient
1.27,
bias-corrected
andaccelerated
95%
CI0.54–2.43),emotional
(coef.0.99,95%
CI
0.21–2.02),and
HNC-specific
(coef.1.55,95%
CI0
.32–3.54)
QOLthan
theirurban
counterparts;socialand
functio
nalQ
OLdidnotd
iffer
significantly
Very goo-
d
Thomas,
2015
(Ireland)
[63]
Cancer
survivors
Cross-sectio
nal
(survey)
39%
166remote
and330
not
remote
The
NationalC
ancerRegistry
Irelandwas
used;d
istance
from
residenceto
hospitalw
asused
todefine
rurality‘urban’
basedon
theAccessibilityand
Rem
otenessIndexof
Australia
(ARIA
+)
The
EuropeanOrganisationfor
theResearchandTreatmento
fCancerQ
ualityof
LifeCore30
(EORTCQLQ-C30)
Colorectalcancer
(atleast6
months
post-diagnosis)
Livingremotefrom
thetreating
hospitalw
asassociated
with
lower
physicalfunctio
ning
(coefficient
−4.38[95%
CI
−8.13,−0
.91])androle
functio
ning
(coef.−7
.78
[−12.64,−2
.66])am
ongall
colorectalcancer
survivors;in
separategender
models,
remotenesswas
significantly
associated
with
lower
physical
(coef.−7
.00[−13.47,−1
.49])
androlefunctioning
(coef.
−11.50
[−19.66,−2
.65])for
wom
en,but
notfor
men;
remotenesshadasignificant
negativ
erelatio
nshipto
global
health
status
(coef.−4
.31
[−8.46,−
0.27])formen
lowest
meanunmetneed
scorefor
rural(M
=0.39,S
D=0.60)
Very goo-
d
1040 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
andurban(M
=0.37,S
D=
0.64)
Studieson
needsandpsychologicalm
orbidity
Andykow
ski,
2014
(United
States)[64]
Cancer
survivors
Cross-sectio
nal
26% cancer
group;
23%
health
control
group
193cancer
group;
152health
control
match
Cancersurvivorswererecruited
from
thepopulation-based
SEERKentuckyCancer
Registry(K
CR);ruralnessof
residencewas
categorised
basedon
county
ofresidence
using2003
UnitedStates
Departm
ento
fAgriculture
Rural–U
rban
Continuum
(RUC)Codes
The
Medicaloutcom
esstudy
36-item
short-form
health
Survey
(SF-36);theHospital
Anxiety
andDepressionScale
(HADS);the
Distress
Therm
ometer(D
T);Perceived
Stress
Scale(PSS
)
Non-smallcell
lung
cancer
10–15months
post-diagnosis
43%
ofruralreportedclinically
importantd
istress
(HADS-Total≥15)compared
with
24%
ofurbansurvivors
(χ2=8.44,p
<0.01);60%
ofruralsurvivorsmetcriteriafor
moderate/severedistresson
the
DT(D
Tratin
g≥4)
compared
with
43%
foru
rban
(χ2=4.82;
p<0.05);ruralcancer
survivorsreported
poorer
mentalh
ealth
relativeto
urban
cancer
survivorswith
amean
effectsize
of0.43
SDin
unadjusted
analyses
and0.29
SDadjusted
foreducationand
physicalcomorbidity
onthree
mentalh
ealth
indices;therural
cancer
groupreported
poorer
mentalh
ealth
than
therural
controlg
roup
onallm
ental
health
indiceswith
ameanES
of0.51
SD;the
mentalh
ealth
ofurbancancer
andhealth
controlg
roupsdidnotd
iffer
(meanES=0.00
SD)
Very goo-
d
Andykow
ski,
2017
(United
States)[65]
Cancer
survivors
Cross-sectio
nal
26%
117ruraland
76urban
Cancersurvivorswererecruited
from
thestate-wide,
population-based,Su
rveillance
Epidemiology
andEnd
Results
(SEER)KentuckyCancer
Registry(K
CR);ruralnessof
residencewas
categorised
basedon
county
ofresidence
usingthe2003
UnitedStates
Departm
ento
fAgriculture
The
PosttraumaticGrowth
Inventory(PTGI);the
Benefit-FindingQuestionnaire
(BFQ
);theHospitalA
nxiety
andDepressionScale(H
ADS);
theMedicaloutcom
esstudy
36-item
short-form
(SF-36)
Non-smallcell
lung
cancer
10–15months
post-diagnosis
Nosignificantd
ifferencewas
foundbetweenruraland
urban
forBFQ
totalscores;ruraland
urbandiffer
with
regard
toPT
GItotalscores(p
=0.042;
ES=0.30
SD);ruralcancer
survivorsreported
greater
grow
thon
allfivePT
GI
subscales(binom
ialtest,p=
0.062,two-tailed);significant
difference
betweenruraland
urbanwas
evidentfor
the
Spiritu
alChangesubscale(p
=0.03,E
S=0.32
SD);
difference
betweentherural
andurbancancer
survivor
groups
with
regard
toPT
GI
Very goo-
d
1041Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
totalscores(p
=0.045,ES=
0.32
SD);ruralcancer
survivorscontinuedto
report
greatergrowthon
allfivePT
GI
subscales(binom
ialtest,p=
0.062,two-tailed);a
significant
difference
betweenruraland
urbangroups
was
evidentfor
theAppreciationforLife
subscale(p
=0.043,ES=0.31
SD)
Carey,2017
(Australia)
[66]
Inform
ative
care-
givers
Cross-sectio
nal
35% returned
com-
plete
survey;
66%
ofsurvi-
vors
hada
support
person
187ruraland
783urban
Recruitedfrom
5population-basedcancer
registries
inAustralia;the
AccessibilityandRem
oteness
Indexof
Australia(A
RIA
+)
classificationwas
used
todefine
rurality
The
Depression,Anxiety,and
Stress
Scale(D
ASS
-21);the
SupportPerson
Unm
etNeeds
Survey
(SPU
NS)
Haematological
cancer
Nosignificantd
ifferences
inproportionof
urbanversus
ruralsupportpersonsin
elevated
levelsof
depression
(21%
vs23%),anxiety(16%
vs17%),or
stress
(16%
vs20%);odds
ofhaving
atleast1
DASS
outcom
eincreased
between12
and18%
foreach
additio
nalh
igh/very
high
unmetneed
(p<0.0001);odds
ofreportingatleast1
indicator
ofpsychologicalm
orbidity
increasedby
10to17%
andby
2%forthosewho
had
relocatedto
receivetreatm
ent
andwas
decreasedby
5to54%
forthosesupportp
ersons
who
reported
thatthey
hadno
chronichealth
conditions;
supportp
ersons
who
hadto
relocatehad2.06
higher
odds
ofhaving
DASS
≥1(95%
CI:
1.15
to3.70,p
=0.015)
Very goo-
d
Corboy,
2019
(Australia)
[67]
Cancer
survivors
Cross-sectio
nal
Not re
ported
286urban
and161
rural
Registeredwith
Australia
Medicare;geographic
remotenesswas
definedby
the
Accessibility/Rem
oteness
Indexof
Australia(A
RIA
+)
The
Brief
Symptom
Inventory
(BSI);theFu
nctio
nal
Assessm
ento
fCancer
Therapy–P
rostateCancer
Subscale(FACT-PC);the
NeedforControl
and
Self-RelianceSu
bscaleof
the
BarrierstoHelpSeekingScale;
theLiverpool
Stoicism
Scale
(LSS)
Australianmen
who
had
undergonea
radical
prostatectom
yas
treatm
entfor
prostatecancer
Average
psychologicald
istress
scoremeasuredby
BSIwas
49.25(SD=12.54);sim
ilar
percentage
ofmen
intheurban
cohort(n
=61;2
1.3%
)and
men
intheregional/rem
ote
cohort(n
=33;20.4%
)metthe
criteriaforcaseness;p
lace
ofresidencedidnotp
redict
psychologicald
istress;
Stoicism
×Placeof
Residence
Very goo-
d
1042 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
was
asignificantp
redictor
ofpsychologicald
istress(urban:
b=0.18,t(443)=2.20,p
=0.02);regional/rem
otecohort,
theassociationbetween
stoicism
andpsychological
distress
was
notsignificant
Grov,2011
(Norway)
[68]
Cancer
survivors
Cross-sectio
nal
53%
223urban
and256
rural;
1437
control
The
Nord-Trøndelag
Countyof
Norway
consistsof
four
cities,
which
weredefinedurban;
othermunicipalities
were
definedarural
The
HospitalA
nxiety
and
DepressionScale(H
ADS);
Rosenberg
Self-Esteem
instrument
Elderly
cancer
survivors
(ECSs)with
variouscancer;
short-term
ECSs
1–5years
post-diagnosis,
long-term
beyond
5years
Ruralversus
urbanareasof
living
explained6.3%
variance
inbeingaruralinhabitant;
self-reportedhealth
was
significanto
nthemodeland
explained3%
ofthevariance
betweenruraland
urban(O
R=
2.03,95%
CI1.28–3.21,p=
0.003)
Good
Gunn,2020
(Australia)
[69]
Cancer
survivors
Cross-sectio
nal
(survey)
11.8%
3379
urban,
776rural,
140
remote
Datacollected
betweenJanuary
2010
andJune
2015
were
obtained
from
theSo
uth
AustralianMonitoring
and
SurveillanceSy
stem
(SAMSS
)
Self-reportedhealth,
psychologicald
istress(K
essler
PsychologicalD
istressScale–
K10),suicidalideatio
n(four
questions
from
theGeneral
Health
Questionnaire)
Various
Nodifference
intheproportio
nof
cancer
survivorswho
reported
high/veryhigh
levelsof
distress
(urban
9.6%
vsrural
7.0%
,p=0.04);ruralcancer
survivors’lower
odds
ofreportinghigh/veryhigh
distress
was
evidentinthe
partially
adjusted
(OR=0.59,
95%
CI0.41–0.84,p=0.004)
andfully
adjusted
model(O
R=0.47,95%
CI0.32–0.69,p<
0.001);h
igherproportio
nof
ruralcancersurvivorswho
indicatedthey
believedpeople
theirneighbourhoodtrusted
oneanother(89%
vs80%,p
<0.001)
Very goo-
d
Hall,2016
(Australia)
[70]
Cancer
patients
and
survivors
Cross-sectio
nal
(survey)
35%
1144
urban
and270
rural
Survivorswererecruitedfrom
5Australianstate
population-basedcancer
registries(registriesA,B
,C,D
,andE);residentialp
ostcodeat
diagnosisclassified
bythe
AustralianBureauof
Statistics
AccessibilityandRem
oteness
Indexof
Australia(A
RIA
+)
definedrurality
The
DepressionAnxiety
and
Stress
Scale21-item
version
(DASS
-21)
Haematological
cancer
Ofurbansurvivors,25%
(n=
274),24%
(n=268),and
17%
(n=194)
reported
above
norm
allevelsof
anxiety,
depression,and
stress,
respectiv
ely;
27%
(n=70),
28%
(n=74),and15%
(n=
38)of
ruralsurvivorsreported
abovenorm
allevelsofanxiety,
depression,and
stress;anxiety,
depression,and
stresswerenot
significantfor
locatio
n;
Very goo-
d
1043Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
however,O
Rforruralv
ersus
urbanwas
anxietyOR=1.14,
depression
OR=1.38,stress
OR=0.87
Schootman,
2013
(United
States)[71]
Cancer
survivors
Cross-sectio
nal
57.4%
in2009
and
59.5%
2010
471ruraland
3088
control;
701urban
and5270
control
The
2009-2010Missouri
BehaviouralRiskFactor
SurveillanceSy
stem
was
used;
thecounty
ofresidencewas
codedaccordingto
itslocation
inametropolitan
statistical
area
(MSA
)as
definedby
the
USOfficeof
Managem
entand
Budget
Self-reportedby
interview;the
Patient
Health
Questionnaire
(PHQ-8)
Various
Prevalence
offair/poorhealth
was
38.5%
amongruralcom
pared
with
27.4%
amongurban
survivorsandless
than
20%
amongboth
controlg
roups;
aftercontrolling
for
sociodem
ographicfactors,
prevalence
offair/poorhealth
was
similarforruraland
urban
survivorsbuth
igheram
ong
controls;ruralsurvivors
(48.8%
)hadahigher
prevalence
offatig
uethan
rural
controls(27.9%
)andurban
survivors(36.1%
)reported
morefatig
uethan
urban
controls(26.5%
);no
differencesam
ongthe4
groups
whencontrolling
for
sociodem
ographic
characteristics,access
tomedicalcare,orchronic
conditions;percentage
who
reported
getting
socialand
emotionalsupportdidnotvary
significantly
across
the4
groups;ruralsurvivors
(61.7%
)wereless
likelyto
receivefollow-upcare
instructions
than
urban
(78.2%
)survivors(p
=0.2)
Very goo-
d
Watts,2016
(Australia)
[72]
Cancer
patients
Cross-sectio
nal
Not re
ported
67major
city,162
inner
regional,
189outer
regional,
21 remote,
and2very
remote
Distressscreeningdatawere
routinelycollected
follo
wing
implem
entatio
nof
screening
acrosssevenWesternAustralia
health
regions;theAustralian
Standard
Geographical
Classification(A
SGC)
Rem
otenessAreas
was
used
DistressTherm
ometerand
Problem
List(DT-PL)
Various
Nosignificantd
ifferences
indistress
levelsacross
the
remotenesscategories
(χ2=
3.91,p
=0.27);Kruskal-W
allis
testrevealed
asignificant
difference
innumberof
problemsacross
thefour
remotenesscategories
(χ2=
10.58,p=0.01);patientsinthe
remotecategory
reported
alower
mediannumberof
Very goo-
d
1044 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
problems(M
d=7.0)
than
patientsin
theotherthree
categories
combined(M
d=
10.0;U
=3482,z
=−2
.23,p=
0.03,r
=0.11);significant
associationbetween
remotenessand
insurance/financialp
roblem
s(χ
2=8.19,p
=0.04,C
ramer’s
V=0.14),andremotenessand
transportatio
ndifficulties(χ
2=
13.07,p=0.004,Cramer’sV=
0.17);in
theem
otional
domain,remotenesswas
significantly
associated
with
fears(χ
2=16.03,p=0.001,
Cramer’sV=0.19),sadness
(χ2=14.33,p=0.002,
Cramer’sV=0.18),andworry
(χ2=18.56,p<0.001,
Cramer’sV=0.21)
Studieson
financialissuesandtravelissues
Paul,2013
(Australia)
[73]
Cancer
patients
Registry-based
study
37%
149urban
and119
rural
Astate-based(W
estern
Australia)
cancer
registry
inAustralia;
ruralitydefinedby
the
AccessibilityandRem
oteness
Indexof
Australia(A
RIA
+)
The
DepressionAnxiety
and
Stress
Scale(D
ASS
-21)
Haematological
cancer
who
had
been
diagnosed
intheprevious
3years
53%
inouterregional/rem
ote
locatio
nshadto
relocatefor
treatm
entcom
paredto
20%
from
innerregionaland3.4%
from
metropolitan
locatio
ns(χ
2=74.32,p<0.001);5
5%liv
ingin
anonm
etropolitan
area
travelled≥1hcompared
to13%
from
major
city
(χ2=
49.1,p
<0.001);logistic
regression
analysisindicated
thatparticipantsliv
ingin
nonm
etropolitan
areashad17×
theodds
ofreportinga
locatio
nal/financialbarrieron
access
tocare
comparedto
thosein
metropolitan
areas;
survivorslivingin
major
city
reported
significantly
more
financialimpact(χ
2=6.06,p
=0.014)
Very goo-
d
Vanderpool,
2020
Cancer
survivors
Survey
ASK
was
22%
and
179ASK
and504
HIN
TS
Appalachian
Kentucky;
Geographicstratawerebased
onthe2013
U.S.D
epartm
ent
The
Health
Status
ofKentucky
(ASK
)survey;H
ealth
Various
77%
oftheAppalachian
survivors
residedin
countiesdesignated
asstrata3–4;geographicstrata
Very goo-
d
1045Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
(United
States)[74]
HIN
TS
was
34%
ofAgriculture’sRural-U
rban
Contin
uum
Codes
(RUCC):
strataIincluded
countieswith
RUCCcodes1–3,which
are
considered
metro
counties,
whilestrataII(RUCC4–5),
strata3(RUCC6–7),and
strata4(RUCC8–9)
included
countieswith
populatio
nsizes
of20,000
ormore,
2,500–19,999,and
less
than
2,500,respectively
Inform
ationNationalT
rends
Survey
(HIN
TS)
was
significantly
correlated
with
cancer-related
financial
distress
amongAppalachian
Kentuckysurvivorswith
higher
percentagesof
distress
reported
amongresidentsof
strata3and4(p
=0.0013);
majority
ofHIN
TS
respondents(85%
)residedin
strata1counties;am
ong
HIN
TSrespondents,
geographicstratawas
not
significantly
associated
with
cancer-related
financial
distress;A
SKcancersurvivors
weresignificantly
morelik
ely
toreportfinanciald
istress
(64%
)comparedto
HIN
TS
cancer
survivors(37%
,p<
0.0001);geographicstratadid
notretainsignificance
inthe
finalm
odel(p
=0.355)
for
ASK
;intheHIN
TS
multiv
ariateanalysis,
geographicstratawas
not
associated
with
financial
distress
(p=0.983)
Zahnd,2019
(United
States)[75]
Cancer
survivors
Cross-sectio
nal
(population--
basedsurvey)
Between
32and
40.0%
1136
urban
and223
rural
Nationalsurveyby
theNational
CancerInstitu
te;rural-urban
status
was
determ
ined
using
the2003
USDepartm
ento
fAgriculture
Rural-U
rban
Contin
uum
Codes
(RUCC)
The
NationalC
ancerInstitute’s
(NCI)Health
Inform
ation
NationalT
rendsSu
rvey
(HIN
TS):2
012,2014,and
2017
Various
Overallprevalence
offinancial
burden
was
20%
higheram
ong
survivors;50.4%
oftotalrural
cancer
survivorsindicated
financialp
roblem
sfollowing
theirdiagnosisandtreatm
ent
comparedto
38.8%
ofurban
survivors(difference=11.6%,
p=0.02);however,after
adjustmentfor
covariates,
49.3%
ofruralcancer
survivorsreported
financial
problemsfollo
wingdiagnosis
andtreatm
entcom
paredto
38.7%
ofurbansurvivors,but
notstatisticallysignificant(p=
0.06)
Very goo-
d
Cancer
patients
Populatio
n-based
longitudinal
44%
890major
cities,373
Participantswereselected
from
NSW
andVictorian
Cancer
Datawereobtained
byself-report
survey
andfrom
theCancer
Duringthefirst1
2monthsafter
diagnosis,outer
1046 Support Care Cancer (2022) 30:1021–1064
Tab
le4
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Samplesize
Setting
Measure
Typeof
cancer
Results
Study
quality
Zucca,2011
(Australia)
[76]
cohort(at6
and
12months)
inner
regional,
136outer
regional,
and11
remote
Registries;cut-pointfor
travel
burden
as≥2honeway
Registries;singleitem
from
The
EuropeanOrganisationfor
ResearchandTreatmento
fCancerQualityof
Life
Questionnaire
(EORTC
QLQ-C30
v3);singleitem
from
theSu
pportiv
eCare
Needs
Survey
Accessto
Services
Module
Various
(duringthe
first1
2months
afterdiagnosis)
regional/rem
oteresidentshad
thegreatesttravelburden;61%
travelledatleast2
honeway
toreceivetreatm
entand
49%
lived
away
from
hometo
receivetreatm
ent;strongest
associates
oftravelburden
wereliv
ingin
regional/rem
ote
areas(O
R=18.9–135.7),
having
received
surgery(O
R=
6.7)
orradiotherapy
(OR=
3.6);between6and12
months
afterdiagnosis,2%
ofpatients
declined
cancer
treatm
ent
becauseof
thetim
eitwould
take
togettotreatm
ent;
patientswho
travelledmore
than
2hor
lived
away
for
treatm
entreported
significantly
greaterfinancial
difficulties(38%
;40%
)than
thosewho
didnot(12%;14%
),even
afteradjustingfor
covariates
Very goo-
d
Studieson
satisfactionwith
life
Cipora,2018
(Polan-
d)[77]
Cancer
patients
Cross-sectio
nal
Not re
ported
48ruraland
73urban
Wom
enwho
hadundergone
surgicaltreatm
entinthe
Sub-CarpathianOncology
Centrein
Brzozów
,Poland
The
Satisfactionwith
LifeScale
(SLS)
Wom
enwith
illbreastcancer
Levelof
satisfactionwith
life
varied
accordingto
placeof
residence:urbanwas
22.04
(6.15sten
score)vs
18.56(4.85
sten
score)
forruralw
omen
(p<0.001);ineach
category
ofthescale,ruralw
omen
(low
satisfaction)
hadsignificantly
lower
scores
than
urban
wom
en(m
ediocre
satisfaction),the
p-valuefor
individualstatem
entsremained
p=0.001andp=0.000
Good
1047Support Care Cancer (2022) 30:1021–1064
Table5
Quantitativ
estudiesincludingonly
ruralsurvivors
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
Studieson
theuseof
form
alandinform
almentalh
ealth
resources
Corboy,
2011
(Australi-
a)[78]
Cancer
patients
and
survivors
Cross-sectional
Not re
port-
ed
40inner
region-
al,31
outer,
and5
remote
The
men
wereliv
ingin
ruraland
regionalareaswithin
the
Grampiansregion
inthestateof
Victoria,Australia;ruraland
regionalareasweredefinedusing
theARIA
+index(M
oderately
Accessible,Accessible,and
Rem
ote)
Listo
fPh
ysicalCom
plaints;Brief
Symptom
Inventory(BSI);S
ocial
SupportS
ubscaleof
theCoping
Resources
Inventory
Men
with
various
cancers
27participantsmetthedefinitionof
caseness
(i.e.,BSIT-score
of63),
indicatingprobableclinically
significantp
sychologicaldistress;
regression
analysisdemonstrated
thatlevelo
fphysicaldistress
was
significantfor
psychological
distress;8
2%wereaw
areof
atleasto
neform
alserviceoffering
emotionalsupportand49%
had
used
such
aservice;telephone-and
Internet-based
services
weremost
used
type
ofsupport;lower
age
was
apredictorofparticipationina
form
alservice(average
8years
younger;M
=65.00(SD=7.68)
(SD=11.2)versus
M=73.05(SD
=7.68))
Poor
McD
owell,
2011
(Australi-
a)[79]
Cancer
survivors
Longitudinal
study
(baselineand
6months)
61%
396
Regionalcancertreatm
entcentrein
Queensland,Australia;rurality
not
defined
The
ENRICHDSo
cialSu
pport
Instrument;theIm
pactof
Events
Scale(IES)
Various
14%
ofcancerpatientsreported
using
psychosocialsupport;females
(OR
=2.73;9
5%CI1.26–5.94)
and
patientswith
morepositive
attitudes
(OR=1.69;9
5%CI
1.03–2.79)
towards
help
seeking
weremorelik
elyto
have
utiliseda
supportservice;the
relationship
betweenpositiv
eattitudes
toseekinghelp
andpsychosocial
supportservice
usewas
mediated
bybehaviouralintentio
ns(O
R=
1.91,95%
CI1.26–2.90);p
atients
reported
high
levelsof
social
support(M
=20.81,SD
=4.78),
andlowsocialconstraints(M
=1.68,S
D=0.69)
Very goo-
d
Studieson
unmetneedsof
cancer
patientsandsurvivors
Bazzell,
2015
(United
States)
[80]
Cancer
patients
Cross-sectional
(survey)
Not re
port-
ed
52Participantw
ererecruitedatthe
American
CancerSo
ciety
sponsoredevents;the
Health
Resources
andServices
Ad m
inistrationof
theUS
Departm
ento
fHealth
andHum
anServices
definitio
nof
ruralw
asused
The
Survivors’Unm
etNeeds
Survey
(SUNS)
Failedto
collectdata
onthis;
meanyears
since
diagnosis
was
9.65
25%
oftheruralsurvivorsreported
high/veryhigh
emotionalhealth
oraccess
andcontinuity
ofcare
unmetneeds;ANOVAresults
provideevidence
thatthereisa
difference
betweensurvivor
years
sincediagnosisandaccess
and
continuity
ofcare
unmetneeds(F
=4.891,p=.002);ANOVA
results
founddifferencesbetween
Very goo-
d
1048 Support Care Cancer (2022) 30:1021–1064
Tab
le5
(contin
ued)
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
survivor
ageandem
otionalu
nmet
needs;access
tointerventio
nsand
survivorship
resourceswerefound
tobe
limitedin
ruralareas
Glasser,
2013
(United
States)
[81]
Cancer
survivors
andtheir
signifi-
cant
other
Cross-sectional
(survey)
Not re
port-
ed
29survi-
vors
and15
part-
ners
Survivorsof
cancer
wererecruited
from
tworuralcom
munity
cancer
programsin
Illinois;ruralitynot
defined
The
DistressTherm
ometer(D
T);the
Durham
GeriatricResearch,
Educatio
nandClin
icalCentre
(GRECC)DepressionScale;the
PROMIS
SF-G
lobalH
ealth
inventory;
theCancerSu
rvivors’
Unm
etNeeds
(CaSUN)
Not
reported
38%
ofsurvivorsreported
fatigue
and
28%
depression;m
orethan
50%
ofsurvivorsandpartnergroups
were
atrisk
fordepression,and
34%
ofthesurvivorswereatrisk
forsome
type
ofpsychosocialproblem
that
currently
required
assistance;
survivorsexpressing
unmetneeds
tended
toscoreworse
than
those
expressing
noneedsfor
depression,distress,chronic
conditions,quality
oflife,and
generalh
ealth
Good
Riley-Clark,
2014
(United
States)
[82]
Cancer
patients
Cross-sectional
(survey)
Not re
port-
ed
47Adirondackregion
ofnorthern
New
York;
ruralitynotd
efined
Self-designedquestio
nnaire
Various
Supportg
roupswerefoundhelpful,
whileothersindicatednot
attendingcauseof
lack
ofknow
ledgeaboutcurrent
groups
andtim
es,and
lack
ofevening
meetings
andtransportationissues;
high
degree
ofinterestin
acounsellor,yoga
orrelaxation
classes,howevernotp
resent
inruralareas
Poor
Studieson
needsandquality
oflife
Coker,2018
(United
States)
[83]
Cancer
survivors
Cross-sectional
40%
inKentuc-
kyand
41%
inNorth
Carolin-
a
3320
The
KentuckyCancerRegistry
(KCR)andtheNorth
Carolina
CentralCancerRegistry(N
CCR)
wereused;B
ealecode
was
used
todefine
rurality
The
Functio
nalA
ssessm
entofC
ancer
Therapy-G
eneral(FACT-G
);Fu
nctio
nalA
ssessm
ento
fChronic
IllnessTherapy-Spiritual
Well-being(FACIT-SP);the
PerceivedStress
Scale;theBrief
Symptom
Inventory(BSI)
Wom
enwith
various
cancers
(diagnosed
intheprior
12months)
UnadjustedFA
CT-G
scores
were
poorer
amongAppalachian
versus
non-Appalachian
residentsfor
totalscores(61.24
vs63.39)
and
physical(13.03
vs13.91),
emotional(13.67vs
14.09),and
work/lifefunctio
nality(16.66
vs17.31)
domains;h
igherstress
scores
(3.49vs
3.22)w
erereported
byparticipantsliv
ingin
Appalachian;additional
adjustmentfor
depression
and
stress
atdiagnosis,FA
CT-G
total,
physical,w
ork/lifefunctio
nality
domains,and
comorbidconditions
remainedassociated
with
Appalachian
residence;differences
byAppalachian
residence
remainedonly
forFA
CT-G
Very goo-
d
1049Support Care Cancer (2022) 30:1021–1064
Tab
le5
(contin
ued)
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
physicalandnumberof
comorbid
physicalconditions,afteradjustin
gforsocioeconomicfactors
Costrini,
2011
(United
States)
[84]
Cancer
survivors
Cross-sectional
Not re
port-
ed
39Patientsweredraw
nfrom
the
2001–2010recordsof
Georgia
GastroenterologyGroup
andfrom
publicsolicitations
inruralp
ress
outlets;ruralzipcodes(asdefined
bythe2000
Census)in
therural
zoneswestofS
avannahandeastof
Macon
wereused
todefine
rurality
The
Medicaloutcom
esstudy36-item
short-form
health
survey
(SF-36);
theFu
nctio
nalA
ssessm
ento
fCancerTherapy-G
eneral
(FACT-G
)with
the
FACT-Colorectal
Colorectal
cancer
Ofthe71%
ofpatientswho
hadto
travelmorethan
100milesround,
8%judged
distance
asan
impedimenttocare;financial
impactwas
significantand
limited
in18%
ofpatients;ruralG
eorgia
self-reportw
orse
generalh
ealth
,psychicalfunctioning,physical
rolelim
itatio
ns,bodily
pain,and
vitalityscores
comparedtogeneral
populatio
n(p
<0.05);using
FACT-C
tool,ruralpatients
reported
bettersocial/fam
ilywell-beingcomparedto
general
populationwith
effectsize
of0.42
(p=0.002);longertim
esince
diagnosiswas
associated
with
betterfunctio
nalw
ell-beingand
colorectalcancer-related
scores
Poor
Steenland,
2011
(United
States)
[85]
Cancer
patients
Follow-up
study
(baseline,6
and12
months)
58%
260
Southw
estG
eorgia;rurality
not
defined
The
MedicalOutcomes
Study
Short-Fo
rm12-itemHealth
Survey
(SF-12);theUniversity
ofCalifornia,Los
Angles,Prostate
CancerIndex
Prostatecancer
(new
lydiagnosed)
Self-reportedphysical(p
<0.0001)
andem
otional(p<0.0001)QOL
declined
significantly
after
treatm
entfor
alltreatmentg
roups
(declin
edafter6monthsand
remainedaboutthe
sameat12
months);the
declinein
physical/emotionalQ
OLdidnot
differ
byage,race,educatio
n,or
Gleason
score;patientstreated
with
horm
ones
show
edtheworst
deteriorationin
physicaland
emotionalQ
OL
Very goo-
d
Studieson
needsandpsychologicalm
orbidity
Befort,2011
(United
States)
[86]
Cancer
survivors
Cross-sectional
(survey)
77%
770
Three
cancer
centreslocatedin
rural
Kansas;rurald
esignatio
nwas
definedby
theZIP
code
approxim
ationof
theRural-U
rban
Com
mutingArea(RUCA)codes
Studydevelopedsurvey
modelled
aftertheBreastC
ancerPreventio
nTrialSy
mptom
Checklist(BCPT
)
Wom
enwith
breast
cancer
(3monthsto
6years
post--
treatm
ent)
Prem
enopausalw
omen
weremore
likelyto
experience
depression
(39%
vs23%)atthetim
eof
treatm
ent;across
thetotalsam
ple,
themostcom
mon
concerns
were
fear
ofrecurrence
(52%
),diminishedphysicalstrength
(39%
),change
inbody
image
(31%
),andfinancialstress(19%
);wom
enprem
enopausalat
diagnosisweresignificantly
more
Very goo-
d
1050 Support Care Cancer (2022) 30:1021–1064
Tab
le5
(contin
ued)
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
likelythan
postmenopausal
wom
ento
reportpsychosocial
factors,includingfear
ofrecurrence
(68%
vs47%),fear
ofdeath(16%
vs5%
),change
inbody
image(43%
vs27%),change
inrelationships
(21%
vs5%
),and
financialstress(32%
vs15%;allp
≤0.001);w
omen
prem
enopausal
atdiagnosisreported
significantly
lower
satisfactionlevels(3.4–1.5)
comparedto
wom
enpostmenopausalatd
iagnosis
(3.8–1.5)(p
=0.001),alsoafter
adjusting
Duggleby,
2014
(Canada)
[87]
Inform
ative
care-
givers
Cross-sectional
(prospectiv
ecorrelational
design)
16%
122
Western
Canadianprovincialcancer
registries
(Albertaand
Saskatchewan);homeaddresshad
tobe
ruralp
ostcode:postalcodes
inAlbertaincludeanyone
who
does
notlivein
thetwotertiary
orfive
regionalcentres
The
Herth
HopeIndex(H
HI);the
GeneralSelf-EfficacyScale
(GSE
S);the
Non-D
eath
Version
Revised
Grief
Experience
Inventory(N
DRGEI);the
Short
Form
Health
Survey
(SF-12v2)
Various
Mentalh
ealth
/well-beingwas
found
tobe
apredictorof
hope
forrural
wom
encaregivers(p
=0.002);the
mentaland
physicalhealth
ofthe
participantsof
thisstudy,when
comparedtoUSpopulatio
nnorm
s,wereator
belowthe25th
percentile,thisfindingsuggests
thatthehealth
oftheruralw
omen
participantswas
poor;g
eneral
self-efficacywas
asignificant
factor
predictinghope
inthe
participants(p
≤0.05);guilt
(p=
0.002)
was
asignificantp
redictor
ofhope
(one
component
ofgrief)
Very goo-
d
Lashbrook,
2018
(Australi-
a)[88]
Cancer
survivors
Cross-sectional
88%
85region-
aland
49 rural
Studywas
conductedattheRiverina
CancerCareCentre(RCCC)and
itstwooutreach
clinicslocatedin
outly
ingruralareas
oftheRiverina
region
ofsouthern
NSW,
Australia;
Accessibility/Rem
otenessIndexof
Australia(A
RIA
)was
used
forthe
classificatio
nof
remoteness
DT;P
atient-ReportedOutcome
MeasurementInformationSy
stem
(PROMIS)
Survivorswith
breast,
prostate,
colorectal,
orlung
who
had
completed
treatm
ent
Cancersurvivorswithouta
partner
(OR=2.60,95%
CI1.06–6.39)
andwith
advanced
cancer
atdiagnosis(O
R=2.70,95%
CI
1.20–6.08)
hadhigher
odds
for
anxiety;
thosewith
colorectal
cancer
(OR=5.80,95%
CI
1.33–24.91),who
lived
with
outa
partner(O
R=3.90,95%
CI
1.46–10.35)andhadahigher
educationallevel(O
R=4.14,95%
CI1
.60–10.91)
hadincreasedodds
ofdepression;participantslivingin
ruralareas
(OR=5.0,95%
CI
1.75–14.29)hadhigh
odds
ofhaving
sleepdisturbance
comparedto
regional;those
who
Very goo-
d
1051Support Care Cancer (2022) 30:1021–1064
Tab
le5
(contin
ued)
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
hadsurgeryhadhigh
odds
(OR=
7.64,95%
CI2.40–24.20)for
sleepdisturbance,whilethoseof
disadvantagedsocioeconomic
status
(OR=0.30,95%
CI
0.12–0.78)
haddecreasedodds
ofhaving
abnorm
alscores
forsleep
disturbance;cancer
survivorswith
ahigher
educationhadincreased
odds
ofhaving
abnorm
alscoresfor
fatigue
(OR=2.3,95%
CI
1.06–5.10);those
with
advanced
stageatdiagnosishadincreased
odds
ofhaving
abnorm
alscoresfor
paininterference
(OR=2.71,95%
CI1.22–6.02)
Schlegel,
2012
(United
States)
[89]
Cancer
patients
Longitudinal
study(4
surveysover
13months)
92% second
survey,
91%
third,
and
90%
fourth
224
9radiationclinicsin
Missouri;
ruralitywas
quantifiedwith
acontinuous
variableanddefinedby
2indicesof
rurality(countycode
andcity
populatio
n)
The
CentreforEpidemiologic
Studies-DepressionScale
Wom
enwith
breast
cancer
Wom
enwho
werenotm
arried
(p=
0.00)or
hadchild
renliv
ingat
home(p
=0.01)reported
higher
levelsof
depressive
symptom
s;wom
enwith
lower
incomes
reported
increaseddepressive
symptom
safterthecompletionof
treatm
ent(p=0.02);younger
wom
enreported
elevated
depressive
symptom
sduring
initial
treatm
ent(p=0.01)butd
issipated
afterthe
completionoftreatm
ent(p
=0.12)
Very goo-
d
Studieson
financialissues
Mandaliya,
2016
(Australi-
a)[90]
Cancer
patients
Cross-sectional
78%
45Ruraloncology
clinicin
theNew
England
region,N
SW,A
ustralia;
ruralitynotd
efined
The
Qualityof
Lifein
AdultCancer
(QLACS)
SurvivorsScale;the
PersonalandHousehold
Finances
Questionnaire
(HILDA)
Various
(3–5
years
post--
treatm
ent)
There
was
noevidence
ofassociations
betweenany
demographicvariableandeither
financialstressor
cancer-specific
quality
oflifedomains;financial
stress
was
howeversignificantly
associated
with
thecancer-specific
quality
oflifedomains
ofappearance-related
concerns
(estim
ate0.37,p
=0.0152),
family-related
distress
(estim
ate
0.30,p
=0.0132),anddistress
relatedto
recurrence
(estim
ate
0.52,p
=0.0012)
Very goo-
d
Pisu,2017
(United
Cancer
survivors
Longitudinal
study(data
from
atrialat
16% attrition
432
Datawereused
from
theRuralBreast
CancerSurvivorInterventio
ntrial;
ruraleligibility
was
established
The
WorkandFinances
Inventory
(WFI);theBreastC
ancerSu
rvivor
Socio-demographicandTreatment
Wom
enwith
breast
cancer
Meanout-of-pocket(OOP)
burden
was
9%atbaselineandbetween7
and8%
atthenext
assessments;
Very goo-
d
1052 Support Care Cancer (2022) 30:1021–1064
cancer, three each with colorectal and prostate cancer, and twoeach with lung and head and neck cancer. Of these 41 quan-titative studies, 27 included both urban and rural cancersurvivors.
There were four mixed methods studies, of which threewere conducted in the US and one in Scotland. Two of thesestudies were conducted in people with breast cancer and twoin a heterogenous cancer population. None of these four stud-ies integrated the quantitative and qualitative data.
Risk of bias within the studies
Of the 20 qualitative studies, none were considered of poormethodological quality. Ten studies were considered to be ofvery good methodological quality and 10 considered good(Tables 2 and 3). Of the 41 quantitative studies, 33 studieswere considered to be of very good methodological quality,five of good quality, and three poor (Tables 4 and 5). Mostmixed methods studies were of good methodological quality,except for one study that was very good (Table 6).
Results of studies
Results of qualitative studies including both rural and urbansurvivors are presented below, followed by qualitative studiesincluding only rural survivors, quantitative studies with ruraland urban comparison groups, quantitative studies includingonly rural survivors, and mixed methods studies.
Qualitative studies including both rural and urban survivors
Seven qualitative studies with both rural and urban cancergroups [31–37], exploring respectively general needs and psy-chological morbidity, and financial issues and travel issues,were identified (Table 2). Compared with urban cancer survi-vors, more rural cancer survivors discussed having experi-enced a delay in their cancer diagnosis [32]. However, ruralparticipants were more satisfied with their cancer care, eventhough they were aware that not all cancer care services wereavailable where they lived. Rural African American cancerparticipants also talked more about using spirituality through-out their diagnosis and treatment than those who lived in ur-ban areas [31, 33].
An Australian study on travel issues that included bothrural and urban survivors [36] found that the experience ofrelocation was associated with psychosocial stress, due to alack of support and loneliness but also because of concernsabout the impact of separation on family members remainingat home. Another Australian study [37] found that lengthytravel, distance, lack of opportunity to take leave from work,and the additional costs of relocation and treatment all addedto the stress of relocation. A third Australian study [35] foundthat visits by metropolitan haematologists to regional areasT
able5
(contin
ued)
Author,
year
(country)
Populatio
nStudydesign
Response
rate
Sam
ple
size
Settin
gMeasure
Typeof
cancer
Results
Study
quality
States)
[91]
baseline,6,
9,and12
months)
basedon
residencein
oneof
33Floridaruralcountiesor
inarural
pocketof
oneof
34Floridaurban
counties
Survey;
theCentersfor
EpidemiologicStudiesDepression
Scale(CES-D)
thepredictedmeanOOPburden
was
higher
atbaselin
ethan
inthe
otherassessments(p
=0.007);
factorssuggestiveof
contributin
gto
higher
OOPcostsandOOP
burden
wereyoungerage,lower
income,tim
ein
survivorship
from
diagnosis,anduseof
supportiv
eservices;the
lowestpredicted
OOP
burden
was
forwom
enon
disability(5.1%),andthehighest
was
forparticipantswith
incomes
below$20,000(13.0%
)
1053Support Care Cancer (2022) 30:1021–1064
Table6
Mixed
methods
studies
Author,year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
Mixed
methods
studiescomparing
urbanandruralp
articipants
McN
ulty,2015
(UnitedStates)
[92]
Cancer
survi-
vors
Mixed
methods
Not re
port-
ed
42urbanAlaska
and34
urban
Oregon;
26ruralA
laska
and30
rural
Oregon;
19interviews
(convenience
sample)
Cancersurvivorsliv
ingin
AlaskaandOregon;
Alaskaruralw
asdefined
by>1-htraveltim
eto
amajor
regionalhospital;
Oregonruralw
asdefined
asageographicarea
that
isatleast30milesby
road
from
anurbancommunity
The
Impactof
Cancer
version2(IOCv2);the
Mem
orialS
ymptom
Assessm
entS
cale-Short
Form
(MSA
S-SF
)
Various
(average
6.7
years
post--
treatm
ent)
Overallcomparisons
betweenlocatio
n(rural/urban)andregion
(Alaska/Oregon)
show
edno
statistically
significant
ormeaningfuld
ifferences
betweengroups;
follo
w-uptests
comparisons
between4
places
show
edsignificant
results
for:worry,
negativ
eim
pact,and
employmentconcerns;
rural-urbandifferences
from
interviewdata
included
access
tohealthcare
access,care
coordinatio
n,connectin
gandcommunity
,thinking
aboutd
eath
anddying,
public/privatejourney,
andadvocatin
gforself
andhealthcare
services
Very go-
od
Mixed
methods
studieson
ruralp
articipants
Hubbard,2015
(Scotland)[93]
Cancer
patients
and
survi-
vors
Mixed
methods
(surveyand
semi-structured
telephone
interviews)
25%
44;1
0interviews
(purpose
sample)
Samplewas
obtained
from
BreastC
ancerCare’s
electronicdatabase
inruralS
cotland;rurality
was
definedby
residential
postcode
The
short-form
Supportive
CareNeeds
Survey
(SCNS-SF3
4)
Wom
enwith
breast
cancer(55%
were
receiving
treatm
ent)
57%
ofparticipantsreported
atleasto
nemoderateto
high
unmetneed
and11%
reported
lowneeds;the
mostp
revalent
moderate
tohigh
need
was
being
inform
edaboutcancerin
remission,fearsaboutthe
cancer
spreading,being
adequately
inform
edaboutthe
benefitsand
side
effectsof
treatm
ent
andconcerns
aboutthe
worries
ofthosecloseto
you;
wom
en≤5years
reported
greaterunmet
need
than
those>5years
from
diagnosis,and
statistically
significantly
Good
1054 Support Care Cancer (2022) 30:1021–1064
Tab
le6
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
higher
needswere
observed
forthehealth
system
sandinform
ation
domain(67%
vs22%;
Pearson’sχ2=9.03,p
=0.003);interview
shighlig
hted
thefollo
wing
unmetneeds:inform
ation
abouttreatmentand
side
effects,overview
ofcare,
fear
ofrecurrence,impact
onfamily
,and
distance
from
support
Martin
ez-D
onate,
2013
(United
States)[94]
Cancer
patients
Mixed
methods
based
ontheChronic
CareModel
(sem
i-structured,
interviews,and
health
literacy
assessments;focus
groups
andsurveys
with
clinicalstaff)
Not re
port-
ed
53interviews;
30completed
STOFHLA;
51completed
follo
w-up;41
clinicalstaff
(purposive
sample)
Fiveclinicsin
rural
Wisconsin
The
ShortTesto
fFu
nctio
nalH
ealth
Literacy
inAdults
(STOFHLA);follo
w-up
basedon
theConsumer
Assessm
ento
fHealth
careProvidersand
System
sandthe
Assessm
ento
fCancer
CareandSatisfaction
surveys
Various
(receiving
cancer
care)
Resultsalignedwith
4/5
dimensionsof
the
ChronicCareModel:(1)
limitedavailabilityof
form
alsupportservices
andcultu
ralv
aluesof
stoicism
,pragm
atism,
independence,privacy,
andself-reliancewere
oftenin
conflictw
ithpatients’needsresulting
inpatientssufferingin
silence;(2)allw
hocompleted
STOFHLA
reported
adequatehealth
literacy,butstaffreported
thatpatientsstrugglewith
understandingmedical
inform
ation;
(3)need
for
greaterlevelsof
care
coordinatio
n,burden
ofassessingnon-medical
needs,andshorterclinical
form
s;and(4)shared
decision
making,patient
empowerment,andverbal
communicationstrategies
Good
Torres,2015
(UnitedStates)
[95]
Cancer
survi-
vors
Mixed
methods
(surveyand
in-depth,
open-ended
Not re
port-
ed
31(snowball
sampling)
Three
ruralcountiesin
easternNorth
Carolina;
ruralitynotd
efined
Survey
Wom
enwith
breast
cancer
The
mainthem
eswere:(1)
breastcancer
diagnosis
(mostcom
mon
wayswere
self-discovery,via
Good
1055Support Care Cancer (2022) 30:1021–1064
reduce stress associated with separation from family, the needfor lengthy travel, and the financial cost of treatment.Furthermore, this study found that the opportunity to undergopart or all of treatment at regional hospitals is physically lessdemanding, more convenient and time saving, establishesbonds of trust and friendship with regional health profes-sionals, lessens the emotional impact of diagnosis and treat-ment, and has financial benefits for patients.
Qualitative studies including only rural survivors
Thirteen qualitative studies including only rural cancer survi-vors were identified (Table 3) [38–50]. Two Australian stud-ies [38, 39] found several issues in the provision of psychoso-cial care including access to appropriate psychosocial services(e.g., lack of information about services and concerns aboutstigma and dual relationships with service providers as friend/physician) and lack of knowledge of the unique needs of ruralcancer survivors bymedical staff located inmetropolitan treat-ment centres. However, those rural survivors who hadaccessed psychosocial support highly valued that support asit helped reduce uncertainty, fear and loneliness, and normal-ised patients’ experiences [38]. Unmet needs included feelinglet down by formal service provision, a sense of isolation, lackof referrals and follow-up care, inaccessibility of services dueto distance, cost or wait times, and lack of appropriate carebased on age, stage, or type of cancer [39]. Rural cancer pa-tients suggested this could be improved by providing rural-specific information on psychosocial care, improving commu-nication between healthcare providers, and making psychoso-cial services a standard part of care [38]. Another Australianstudy [50] investigated rural cancer survivors’ experiencepost-treatment in relation to QOL. This study found that arange of issues impacted the post-treatment QOL of rural can-cer survivors, including fatigue and fear of cancer recurrence,and that these rural survivors lack information on how to ac-cess support to manage these issues. Participants highlightedseveral acceptable strategies to improve their QOL post-treat-ment, including nurse-led, telephone-based, or face-to-faceinterventions that include support with managing emotionalchallenges [50].
One Canadian study [44] looked at rural people with cancerin the palliative care setting. Four themes emerged: (1) com-munity connectedness/isolation; (2) lack of accessibility tocare; (3) communication and information issues; and (4) inde-pendence/dependence. Some of these findings resonated witha Norwegian study [43] that examined the lived experience ofolder rural persons receiving palliative treatment. This studyfound their participants struggled with having limited control,avoided becoming a burden, tried to live up to the expecta-tions of being a ‘good patient’, and kept hope alive by dream-ing and making plans. Several studies [40–42, 45–49]highlighted rural difficulties with support and isolation, andT
able6
(contin
ued)
Author,year
(country)
Populatio
nStudy
design
Response
rate
Sam
plesize
Settin
gMeasure
Typeof
cancer
Results
Study
quality
questio
nsfocus
groupinterviews)
age-recommended
screening,and/or
their
gynaecologists);(2)
psychosocialwell-being
(fear,coping
mechanism
s,andQOL
concerns);and(3)quality
ofcare
factors
(doctor-patient
relatio
nship,side
effects
oftreatm
ent,adherenceto
follo
w-upcare,and
financialresources)
1056 Support Care Cancer (2022) 30:1021–1064
psychological issues such as a loss of control over the illness,anxiety, and a lack of knowledge. Some rural cancer patientsstated that the information given was complex and in combi-nation with condensed appointment schedules (to minimisetravel) made the processing of information difficult.However, the support of family and home care services helpedmany transition through the physical and psychological de-mands that were encountered.
Quantitative studies with rural and urban comparison groups
Quantitative studies with an urban control group (n = 27) arepresented in Table 4 [51–77]. Three addressed the use of for-mal and informal mental health resources, five examined fi-nancial and travel issues, one measured satisfaction with life,and the remainder explored the general needs, psychologicalmorbidity, and QOL of cancer survivors and informal care-givers. Only two studies were longitudinal [60, 76].
Of the 19 studies exploring needs, psychological morbidi-ty, and QOL, three (one US and two European) reportedpoorer outcomes for rural cancer survivors [63, 64, 68] andone (Australian) reported poorer outcomes for rural informalcaregivers [56]. Five (one Australian, two US, and twoEuropean) reported poorer outcomes for urban cancer survi-vors [57, 59, 61, 62, 65], one (Australian) found needs dif-fered between groups [55], while nine (eight Australian andone US) concluded there were no meaningful differences be-tween groups [54, 58, 60, 66, 67, 69–72]. Physical function-ing, role functioning, and reported mental health outcomeswere more likely to be worse in rural samples, whereas urbancancer survivors reported poorer social functioning and emo-tional QOL.
One US study of 113 heterogenous cancer survivors [51]found that rural cancer survivors reported significantly lessfavourable attitudes (t(111) = 2.05, p < 0.05) and social norms(t(111) = 2.20, p < 0.05) towards mental health resources thanurban cancer survivors. Conversely, a German study of 534colorectal cancer patients [52] showed that urban cancer pa-tients were significantly less likely to talk with their doctorabout their emotional state (65%, p < 0.01) and showed poorerknowledge (60%, p < 0.002) of cancer-specific mental healthresources than rural cancer patients. There were no differencesconcerning distress, mental health outcomes, or acceptance ofcancer-specific mental health resources between rural and ur-ban cancer survivors (undergoing treatment and post-treatment) in the German sample [52].
A study conducted in Appalachian Kentucky (US) foundthat geographic location was significantly correlated withcancer-related financial distress among rural cancer survivors(p = 0.0013) [74]. Survivors who lived in regional or remotelocations were 17 times more likely to report locational orfinancial barriers to accessing care compared to survivors liv-ing in metropolitan locations [73]. Another US study [75]
found that the overall prevalence of financial burden was20% higher among rural cancer survivors than urban cancersurvivors. However, after adjusting for covariates, this findingbecame not statistically significant (p = 0.06). Another study[76] (Australian) found that regional or remote cancer patients(first year after diagnosis) were more likely to report travelburden compared to cancer patients living in major cities(OR = 18.9, p < 0.001; OR = 135.7, p < 0.001, respectively).Similar findings were found for financial difficulties (p <0.05) [61], for which patients who travelled more than 2 h(OR = 2.65, p = 0.0178) or lived away for treatment (OR =2.79, p = 0.0152) reported significantly greater financial dif-ficulties than those who did not 6 months post-diagnosis [76].
One US study of 193 lung cancer survivors [65] examineddifferences between rural and urban cancer survivors in re-ports of positive outcomes, namely posttraumatic growthand benefit-finding of one’s cancer experience. Although nosignificant differences were found for benefit-finding betweenthe two groups, rural cancer survivors reported significantgreater posttraumatic growth (effect size (ES) = 0.30 SD; p= 0.042). Another study examined the satisfaction with lifeamong women with breast cancer and found that rural womenwith breast cancer reported lower satisfaction with life thantheir urban counterparts (p < 0.001) [77].
Quantitative studies including only rural survivors
There were 14 quantitative studies including only rural cancersurvivors [78–91], two on the use of formal and informalmental health resources, four on psychological needs and psy-chological morbidity, two on financial issues, and six on gen-eral needs and QOL. In total, four studies [79, 85, 89, 91] werelongitudinal and only one study [87] was on informal care-givers (Table 5).
The single study on rural informal caregivers [87], with asample of 122 participants, found that participants with higherhope had higher mental health scores (β = 0.266; p = 0.002),lower perceptions of loss and grief (β = −0.356; p = 0.001),and were more confident in their ability to deal with difficultsituations (β = 0.511; p = 0.000). Other studies on psycholog-ical morbidity [86, 88, 89] found that rural cancer survivorswho lived without a partner (OR = 3.90, 95% CI 1.46–10.35)or had a higher educational level (OR = 4.14, 95% CI 1.60–10.91) had increased odds of mild to severe levels of depres-sion (i.e., score of ≥ 55) [88]. One US study in rural womenwith breast cancer found that premenopausal women weremore likely to experience depression at the time of treatmentcompared to postmenopausal women (39% versus 23%, re-spectively; p < 0.001) [86]. This study also found that the mostcommon concerns among all rural women with breast cancer(i.e., percentage of women who reported experiencing psy-chosocial factors) were fear of recurrence (52%), diminished
1057Support Care Cancer (2022) 30:1021–1064
physical strength (39%), change in body image (31%), andfinancial stress (19%) [86].
Four longitudinal studies [79, 85, 89, 91] reported find-ings on several topics. One Australian study [79] found thatrural cancer patients with a more positive attitude towardshelp seeking were more likely to have utilised a supportservice 6 months following study commencement (OR =1.69, p < 0.05). One US study [91] found that the out-of-pocket (OOP) burden (i.e., OOP costs as a percentage ofincome) significantly declined over time for rural cancersurvivors (p = 0.007); the predicted mean OOP burdenwas 9.8% at baseline, and between 7 and 8% at follow-up.Factors suggestive of contributing to higher OOP burden forrural cancer survivors included younger age, lower income,time in survivorship from diagnosis, and use of supportiveservices [91]. Another rural US study [89] found a decreasein depressive symptoms in the first 3 months after the startof treatment but an increase 5 months thereafter. This trendwas observed due to the decrease in psychological distressimmediately after completion of active treatment but in-crease thereafter due to the fear of recurrence. Lastly, onelongitudinal study [85], on the needs and QOL of men withprostate cancer in rural Georgia, found that self-reportedphysical QOL (coefficient = −5.8, p < 0.0001) and emotion-al QOL (coefficient = −5.7, p < 0.0001) declined signifi-cantly after treatment.
A rural-focussed Australian study on financial issues foundthat financial stress was significantly associated with thecancer-specific QOL domains of appearance-related concerns(ES = 0.37, p = 0.015), family-related distress (ES = 0.30, p =0.013), and distress-related to recurrence (ES = 0.52, p =0.001) [90]. One Australian study on service use [78] foundthat despite most (82%) of the rural men being aware of aformal service offering psychosocial support, only 49% ofthe rural men used such a service. This is contrary to anotherrural-focussed Australian study [79] that found only 14% ofparticipants reported having used a psychosocial supportservice.
The remainder of studies [80–85] were on the generalneeds and QOL of rural people affected by cancer, for whichsome also reported data on psychological morbidity and com-pared rural cancer patients with the general population, how-ever excluded urban cancer groups. These studies found that25% of the rural cancer survivors reported high/very highemotional health needs, 38% reported fatigue, and 28% re-ported depression. QOL scores seemed to be lower in ruralcancer survivors compared to the general population.However, rural cancer patients reported better social/familywell-being compared to the general population. Finally, ruralcancer patients reported that support groups were very helpful,though some participants reported that they did not attendbecause of a lack of knowledge about current support groupsand times.
Mixed methods studies
There were four studies that used a mixed methods approach(Table 6) [92–95]. One study, comparing rural and urban can-cer survivors, found no statistically meaningful differencesbetween groups in the quantitative analysis [92]. However,the qualitative analysis revealed that rural cancer survivorshad more challenges than urban cancer survivors includingaccess to healthcare, care coordination, and the very publicjourney of their survivorship due to the close-knit nature oftheir communities. The other three studies among rural cancersurvivors showed that health systems and information, psy-chological needs, and quality of care were the most frequentlyreported domains of unmet needs [93–95]. The interviewsfrom one study [93] also highlighted the following unmet ruralneeds: information about treatment and side effects, overviewof care, fear of recurrence, impact on family, and distancefrom support.
Discussion
Summary of evidence
Main findings
This systematic review examined the research conducted overthe last 10 years on the psychosocial well-being and support-ive care needs of cancer patients and survivors living in urbanand rural/regional areas. The 65 studies included in this re-view, of which most studies were conducted in Australia (28/65; 43%) followed by the US (24/65; 37%), demonstrated thatamong the studies that found a difference, rural cancer survi-vors were more likely to report worse outcomes in physicalfunctioning, role functioning, and reported mental health,whereas urban cancer survivors were more likely to reportpoorer outcomes in social functioning and emotional QOL.However, most studies that compared rural and urban cancersurvivors found no differences between the two populationswith regard to psychosocial well-being and QOL. This reviewalso found that rural cancer survivors were more likely toreport unmet needs relating to financial and travel issues andexperience more difficulties with accessing care compared tourban cancer survivors. This highlights that rural and urbancancer survivors have different psychological needs and con-cerns, and rural cancer survivors have some additional unmetneeds related to rurality that require careful assessment andmanagement
Context within the 2011 systematic review
Over the last 10 years, research on the psychosocial well-being and supportive care needs of rural and urban cancer
1058 Support Care Cancer (2022) 30:1021–1064
survivors has increased. The previous systematic review onthe same topic identified 37 studies that were published beforeAugust 2010. Our review included 65 studies published be-tween August 2010 and May 2021. Compared to the 2011review, more studies included in this review were conductedin people with heterogenous cancers (30 versus 11), and in-cluded a control group of urban cancer survivors (27 versus11) or used a general population control group (3 versus 1).Moreover, the quality of studies seems to have improved overthe last 10 years as the studies included in this review hadbetter reporting of design (68% versus 54%), and more oftendefined rurality or used a validated measurement tool, com-pared to the 2011 systematic review.
This review identified three studies [64, 68, 71] that includ-ed rural and urban general population control groups, anddirectly compared rural and urban cancer populations. Thesestudies found that significant differences existed in health out-comes between rural and urban cancer survivors and healthycontrols (one study was matched on age [68], and one studywas matched on age, gender, and country of residence [64]).More specifically, cancer survivors in general reported poorerself-rated health compared to healthy controls, for which ruralcancer survivors reported slightly poorer outcomes than urbancancer surv ivors . However , a f t e r ad jus t ing forsociodemographic factors, rural and urban cancer survivorsreported similar outcomes, nonetheless poorer than healthycontrols. Conversely, the 2011 review that included onlyone population-based control study found that the age-adjusted QOL was similar among all groups. However, whileour review identified three population-based control studiesthat included a heterogenous or lung cancer population, the2011 review identified a single population-based control studythat included only breast cancer survivors, who in generalreport better QOL outcomes compared to lung cancer survi-vors for example, and have better overall survival rates [96].
While 9 quantitative studies with an urban control group inthis review showed no evidence of meaningful differencesbetween rural and urban cancer survivors [54, 58, 60, 66,67, 69–72], five studies concluded that urban cancer survivorsreported poorer psychosocial outcomes than rural cancer sur-vivors [57, 59, 61, 62, 65] and three studies found that ruralcancer survivors reported poorer psychosocial outcomes thantheir urban counterparts [63, 64, 68]. These findings differfrom the 2011 review on this topic, which found that ruralcancer survivors generally reported worse outcomes than ur-ban cancer survivors. Recent research suggests that rural can-cer survivors may have greater protective factors againstpoorer emotional health, including active coping styles, posi-tive reinterpretation [16], and the belief that a person’s healthis decided by powerful others [97], that urban cancer survivorsmay be lacking. Studies have also shown that people living inrural areas not only tend to be more stoic about their health,which could result in under-reporting of distress, but also
differ in their expectations of health services than people liv-ing in urban areas [98, 99]. In addition, rural cancer survivorsreport higher levels of community trust, which may buffer theimpact of a lack of professional psychosocial support servicesin rural areas [69]. This may explain rural cancer survivorsreporting fewer unmet emotional needs than urban cancer sur-vivors. Further, it is also possible that the introduction of nu-merous regional cancer centres in the last 10 years inAustralia, where many of these studies were conducted, hashelped reduce the psychosocial toll of a cancer diagnosis forrural Australians. Moreover, the increase use in technology(e.g., telehealth) and digital healthcare may also have helpedto overcome the tyranny of distance and led to improvements.
The majority of studies focussed on a heterogenous groupof cancer survivors (30/65; 46%), followed by breast cancersurvivors (13/65; 20%) and haematological cancer patients(8/65; 12%).
In the qualitative studies with urban comparison groups,findings were similar to the 2011 review regarding unmetneeds and travel issues. In both reviews, rural cancer survivorsreported more frequent episodes of delayed diagnosis com-pared to urban cancer survivors [32]. Other challenges thatwere similar to the 2011 review included difficulties withaccess to healthcare and care coordination/navigation, forwhich rural cancer survivors reported more challenges thanurban cancer survivors [92]. Furthermore, in both systematicreviews, the qualitative studies confirmed the findings on trav-el issues in quantitative studies [35–37]. Both reviews foundthat travelling caused additional stress, can put pressure onfamily relationships, and in general posed difficulties to pa-tients. This was also found in qualitative studies without anurban control group in both reviews, highlighting that ruralcancer survivors and families report difficulties with supportand isolation, psychological issues such as a loss of controlover the illness, anxiety, and a lack of knowledge, and accessto mental health services. The current review also highlightedan additional finding that a lack of opportunity to take leavefrom work may mean that some rural cancer survivors cannotundergo treatment [37]. This may be related to the greaterproportion of people who are self-employed in rural versusurban areas [100]. However, although these challenges arestill apparent in rural cancer survivors, more research is need-ed that investigates whether these challenges have improvedwith the increased use and quality of telehealth and digitalhealthcare over time.
In total, six longitudinal studies (four without a controlgroup) were identified in this study. The longitudinal studieswith a control group [60, 76] found that rural cancer survivorsreported lower QOL (6 months post-treatment) and greatertravel burden (12 months post-diagnosis) compared with ur-ban cancer survivors over time. The studies without a controlgroup [79, 85, 89, 91] found that the out-of-pocket burden andQOL declined over time (1–3 years post-diagnosis). However,
1059Support Care Cancer (2022) 30:1021–1064
levels of depression increased 12 months post-diagnosis afteran initial decline 3 months after the start of treatment. The2011 review also found that the health system and informationneeds of rural cancer patients decreased over time. These find-ings suggest that needs may change along the cancer survivor-ship continuum. For instance, post-diagnosis needs might re-volve around providing information and support, whereaspost-treatment needs focus more around the practical issuesof being able to perform activities of daily living.
Limitations
While this systematic review provides updated information onwhat is known about levels of psychosocial morbidity and theneeds of rural people with cancer and their informal care-givers, the results should be interpreted with the followinglimitations in mind. First, this review has brought togetherstudies that were conducted in multiple developed countriesthat used different definitions for rurality, such as the ARIA(Australia) and the Rural-Urban Continuum (RUC; US).Additionally, studies included in this review used differentmethodological approaches and different data sources.Conducting a separate qualitative and quantitative reviewmay have had merit, but we wanted to follow the successfulapproach employed in the previous review. As these studieswere very heterogeneous, no meta-analysis was conducted,and the findings of this review are conceptual rather thanstatistical. As most studies included in this review used across-sectional design, it was impossible to explore causality.Further, all data reported on in the studies contained in thisreviewwere collected prior to the COVID-19 epidemic, whichmay have led to improvements in remote access to supportservices, with particular benefits for rural populations.Second, the search strategy was restricted to English-language publications, which made it impossible to commenton the experiences of rural cancer survivors living in non-English-speaking countries. Lastly, as the scope of this reviewwas psychosocial in nature, physical morbidity and medicaloutcomes or survival rates were excluded. As these outcomesare closely related to a cancer survivor’s psychosocial well-being and needs, there may have been merit in broadening thescope of the review to include them. However, this wouldhave limited our ability tomake comparisons with the findingsfrom the previous review.
Conclusions
Over the last 10 years, the number of studies on the topic ofpsychosocial morbidity and unmet needs in rural cancer sur-vivors has almost doubled.While 37 studies were identified inthe 2011 review, this study identified 65 new studies pub-lished after July 2010. Many (9/19) quantitative studies with
an urban control group did not report any meaningful differ-ences between rural and urban cancer survivors with regard topsychosocial morbidity or general unmet needs. There wereslightly more quantitative studies with control groups that re-ported worse outcomes in urban cancer survivors (5/19) thanrural cancer survivors (3/19), for which urban cancer survivorsreported worse social and emotional functioning and ruralcancer survivors reported worse physical functioning, rolefunctioning, and reported mental health outcomes comparedto their counterparts. Nonetheless, many needs were still un-met in both populations, and people with cancer living in ruralareas were found to face different, additional financial andtravel issues, and experience difficulties accessing care.These uniquely rural psychosocial challenges need carefulassessment and management by health professionals, if equal-ity in treatment outcomes between rural and urban populationsis to be achieved. Further longitudinal research is also war-ranted that includes both rural and urban cancer groups andincludes population-based control groups, to establish wheth-er differences in psychosocial outcomes between rural andurban survivors are due to general geographic or cancer-specific factors. This will help inform the development offuture intervention trials that seek to test new strategies toaddress key issues, in the populations who need them most.
Availability of data and material We have control of all data and agree toallow the journal to review our data if required.
Author contribution Shannen R. van der Kruk: conceptualisation, datacuration, formal analysis, methodology, project administration, writing— original draft
Phyllis Butow: conceptualisation,methodology, supervision, writing— review and editing
Ilse Mesters: methodology, formal analysis, supervision, writing —review and editing
Terry Boyle: methodology, supervision, writing— review and editingIan Olver: methodology, formal analysis, writing — review and
editingKate White: formal analysis, writing— review and editingSabe Sabesan: formal analysis, writing — review and editingRob Zielinski: formal analysis, writing — review and editingBryan A. Chan: formal analysis, writing— review and editingKristiaan Spronk: data curation, formal analysis, writing — review
and editingPeter Grimison: writing — review and editingCraig Underhill: writing — review and editingLaura Kirsten: writing — review and editingKateM.Gunn: conceptualisation, formal analysis,methodology, pro-
ject administration, resources, supervision, writing— review and editing
Declarations
Ethics approval Not applicable.
Consent to participate Not applicable.
Consent for publication Not applicable.
1060 Support Care Cancer (2022) 30:1021–1064
Conflict of interest The authors declare no competing interests.
References
1. Hewitt M, Greenfield S, Stovall E (2005) From cancer patient tocancer survivor: lost in transition. National Academies Press,
2. Australian Institute of Health and Welfare (2020) Cancer data inAustralia. AIHW. https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia. Accessed 13 October 2020
3. Alfano CM, Jefford M, Maher J, Birken SA, Mayer DK (2019)Building personalized cancer follow-up care pathways in theUnited States: lessons learned from implementation in England,Northern Ireland, and Australia. Am Soc Clin Oncol Educl Book39:625–639
4. Wait S, Han D, Muthu V, Oliver K, Chrostowski S, Florindi F, deLorenzo F, Gandouet B, Spurrier G, Ryll B (2017) Towards sus-tainable cancer care: reducing inefficiencies, improvingoutcomes—a policy report from the All Can initiative. J CancerPolicy 13:47–64
5. Gysels M, Higginson I, Rajasekaran M, Davies E, Harding R(2004) Improving supportive and palliative care for adults withcancer: research evidence. Natl Instit Health Clin Excell. https://www.nice.org.uk/guidance/csg4. Accessed 2 June 2020
6. Boyes AW, Girgis A, D’Este C, Zucca AC (2012) Prevalence andcorrelates of cancer survivors’ supportive care needs 6 monthsafter diagnosis: a population-based cross-sectional study. BMCCancer 12(1):150
7. Recklitis CJ, Syrjala KL (2017) Provision of integrated psychoso-cial services for cancer survivors post-treatment. Lancet Oncol18(1):e39–e50
8. Blinman PL, Grimison P, Barton MB, Crossing S, Walpole ET,Wong N, Francis K, Koczwara B (2012) The shortage of medicaloncologists: the Australian Medical Oncologist Workforce Study.Med J Aust 196(1):58–61
9. Beesley V, Eakin E, Steginga S, Aitken J, Dunn J, Battistutta D(2008) Unmet needs of gynaecological cancer survivors: implica-tions for developing community support services. Psycho-Oncol :J Psychol Soc Behav Dimens Cancer 17(4):392–400
10. Harrison JD, Young JM, Price MA, Butow PN, Solomon MJ(2009) What are the unmet supportive care needs of people withcancer? A systematic review. Support Care Cancer 17(8):1117–1128
11. Diaz A, Whop LJ, Valery PC, Moore SP, Cunningham J, GarveyG, Condon JR (2015) Cancer outcomes for Aboriginal and TorresStrait Islander Australians in rural and remote areas. Aust J RuralHealth 23(1):4–18. https://doi.org/10.1111/ajr.12169
12. Jong KE, Smith DP, Yu XQ, O’Connell DL, Goldstein D,Armstrong BK (2004) Remoteness of residence and survival fromcancer in New South Wales. Med J Aust 180(12):618–622
13. Baade PD, Dasgupta P, Aitken JF, Turrell G (2011) Distance tothe closest radiotherapy facility and survival after a diagnosis ofrectal cancer in Queensland. Med J Aust 195(6):350–354
14. Carriere R, Adam R, Fielding S, Barlas R, Ong Y, Murchie P(2018) Rural dwellers are less likely to survive cancer—an inter-national review and meta-analysis. Health Place 53:219–227
15. Angell KL, Kreshka MA, Mc Coy R, Donnelly P, Turner-CobbJM, Graddy K, Kraemer HC, Koopman C (2003) Psychosocialintervention for rural women with breast cancer: the SierraStanford partnership. J Gen Intern Med 18(7):499–507
16. Wilson SE, Andersen MR, Meischke H (2000) Meeting the needsof rural breast cancer survivors: what still needs to be done? JWomens Health Gend Based Med 9(6):667–677
17. Zucca A, Boyes A, Girgis A, Hall A (2009) Travel all over thecountryside: travelling for cancer treatment in NSW and Victoria.Asia-Pac J Clin Oncol 5
18. Shugarman LR, Sorbero ME, Tian H, Jain AK, Ashwood JS(2008) An exploration of urban and rural differences in lung can-cer survival among Medicare beneficiaries. Am J Public Health98(7):1280–1287
19. Probst JC, Laditka SB, Wang J-Y, Johnson AO (2007) Effects ofresidence and race on burden of travel for care: cross sectionalanalysis of the 2001 US National Household Travel Survey.BMC Health Serv Res 7(1):40
20. Charlton M, Schlichting J, Chioreso C, Ward M, Vikas P (2015)Challenges of rural cancer care in the United States. Oncology29(9):633–640
21. Australian Institute of Health Welfare (2019) Rural & RemoteHealth. AIHW. https://www.aihw.gov.au/reports/rural-remote-australians/rural-remote-health. Accessed 16 March 2020
22. Meilleur A, Subramanian S, Plascak JJ, Fisher JL, Paskett ED,Lamont EB (2013) Rural residence and cancer outcomes in theUnited States: issues and challenges. Cancer Epidemiol PrevBiomarkers 22(10):1657–1667
23. Butow PN, Phillips F, Schweder J, White K, Underhill C,Goldstein D (2012) Psychosocial well-being and supportive careneeds of cancer patients living in urban and rural/regional areas: asystematic review. Support Care Cancer 20(1):1–22
24. Yu XQ, Luo Q, Kahn C, O’Connell DL, Houssami N (2015)Temporal trends show improved breast cancer survival inAustralia but widening urban-rural differences. Breast 24(4):524–527. https://doi.org/10.1016/j.breast.2015.03.006
25. Kennedy AE, Vanderpool RC, Croyle RT, Srinivasan S (2018)An overview of the National Cancer Institute’s initiatives to accel-erate rural cancer control research. Cancer Epidemiol PrevBiomarkers 27(11):1240–1244
26. Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferredreporting items for systematic reviews and meta-analyses: thePRISMA statement. Int J Surg 8(5):336–341
27. Australian Government (2001) Measuring remoteness:accessibility/remoteness index of Australia (ARIA). Departmentof Health and Aged Care. https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-historicpubs-hfsocc-ocpanew14a.htm. Accessed 2 March 2020
28. United Nations Development Programme (2019) Human devel-opment report 2019: beyond income, beyond averages, beyondtoday: inequalities in human development in the 21st century.https://www.un-ilibrary.org/content/publication/838f78fd-en.Accessed 8 April 2020
29. Peters MD, Godfrey CM, McInerney P, Soares CB, Khalil H,Parker D (2015) The Joanna Briggs Institute reviewers’ manual2015: methodology for JBI scoping reviews.
30. Pluye P, Robert E, Cargo M, Bartlett G, O’cathain A, Griffiths F,Boardman F, GagnonM-P, RousseauM (2011) Proposal: a mixedmethods appraisal tool for systematic mixed studies reviews.Montréal: McGill University 2:1–8
31. Jones RA,Wenzel J, Hinton I, CaryM, Jones NR, Krumm S, FordJG (2011) Exploring cancer support needs for older African-American men with prostate cancer. Support Care Cancer 19(9):1411–1419
32. Miedema B, Easley JK, Robinson LM (2013) Comparing urbanand rural young adult cancer survivors’ experiences: a qualitativestudy. Rural Remote Health 13(2):2324
33. Wenzel J, Jones RA, Klimmek R, Krumm S, Darrell LP, Song D,Stearns V, Ford JG (2012) Cancer support and resource needsamong African American older adults. Clin J Oncol Nurs 16(4):372–377
34. Galica J, Giroux J, Francis JA, Maheu C (2020) Coping with fearof cancer recurrence among ovarian cancer survivors living in
small urban and rural settings: a qualitative descriptive study. Eur JOncol Nurs 44:101705
35. McGrath P (2015) Overcoming the distance barrier in relation totreatment for haematology patients: Queensland findings. AustHealth Rev 39(3):344–350
36. McGrath P (2015) Findings on family issues during relocation forhematology care. Oncol Nurs Forum 42(3):E250–E256
37. McGrath P (2015) ‘You never leave work when you live on acattle property’: special problems for rural property owners whohave to relocate for specialist treatment. Aust J Rural Health 23(5):286–290
38. Gunn K, Turnbull D, McWha JL, Davies M, Olver I (2013)Psychosocial service use: a qualitative exploration from the per-spective of rural Australian cancer patients. Support Care Cancer21(9):2547–2555
39. Pascal J, Johnson N, Dickson-Swift V, Kenny A (2015) Returninghome: psychosocial care during the re-entry phase of cancer sur-vivorship in rural Australia. Eur J Cancer Care (Engl) 24(1):39–49
40. Adams N, Gisiger-Camata S, Hardy CM, Thomas TF, Jukkala A,Meneses K (2017) Evaluating survivorship experiences and needsamong rural African American breast cancer survivors. J CancerEduc 32(2):264–271
41. Allen KR, Roberto KA (2014) Older women in Appalachia: ex-periences with gynecological cancer. The Gerontologist 54(6):1024–1034
42. Coyne E, Frommolt V, Salehi A (2019) The experience and chal-lenges of rural persons with cancer and their families. Collegian26(6):609–614
43. Devik SA, Enmarker I, Wiik GB, Hellzen O (2013) Meanings ofbeing old, living on one’s own and suffering from incurable cancerin rural Norway. Eur J Oncol Nurs 17(6):781–787
44. Duggleby W, Penz K, Leipert B, Wilson D, Goodridge D,Williams A (2011) ‘I am part of the community but...’The chang-ing context of rural living for persons with advanced cancer andtheir families. Rural Remote Health 11(3):1733
45. Garrard ED, Fennell KM, Wilson C (2017) ‘We’re completelyback to normal, but I’d say it’s a new normal’: a qualitative ex-ploration of adaptive functioning in rural families following aparental cancer diagnosis. Support Care Cancer 25(11):3561–3568
46. Grimison P, Phillips F, Butow P, White K, Yip D, Sardelic F,Underhill C, Tse R, Simes R, Turley K, Raymond C, GoldsteinD (2013) Are visiting oncologists enough? A qualitative study ofthe needs of Australian rural and regional cancer patients, carersand health professionals. Asia Pac J Clin Oncol 9(3):226–238
47. Loughery J, Woodgate RL (2019) Supportive care experiences ofrural women living with breast cancer: an interpretive descriptivequalitative study. Can Oncol Nurs J 29(3):170–176
48. Sawin EM (2010) ‘My husband would not help me, so I wasdriving over there’: older rural women experiencing breast cancerwith a nonsupportive intimate partner. Rural Remote Health10(4):1–13
49. Wagland K, Levesque JV, Connors J (2015) Disease isolation: thechallenges faced bymothers living with multiple myeloma in ruraland regional Australia. Eur J Oncol Nurs 19(2):148–153
50. Gunn KM, Olver I, Skrabal Ross X, Harrison N, Livingston PM,Wilson C (2021) Improving survivors’ quality of life post-treat-ment: the perspectives of rural australian cancer survivors andtheir carers. Cancers 13(7):1600
51. Andrykowski MA, Burris JL (2010) Use of formal and informalmental health resources by cancer survivors: differences betweenrural and nonrural survivors and a preliminary test of the theory ofplanned behavior. Psycho-Oncology 19(11):1148–1155
52. Beraldi A, Kukk E, Nest A, Schubert-Fritschle G, Engel J,Heusner P, Herschbach P (2015) Use of cancer-specific mental
health resources—is there an urban-rural divide? Support CareCancer 23(5):1285–1294
53. Corboy D, McLaren S, Jenkins M, McDonald J (2014) The rela-tionship between geographic remoteness and intentions to use atelephone support service amongAustralianmen following radicalprostatectomy. Psychooncology 23(11):1259–1266
54. Ahern T, Gardner A, Courtney M (2015) Geographical compari-sons of information and support needs of Australian women fol-lowing the primary treatment of breast cancer: a 10-year replica-tion study. Health Expect 18(6):2678–2692
55. Ahern T, Gardner A, Courtney M (2016) Exploring patient sup-port by breast care nurses and geographical residence as modera-tors of the unmet needs and self-efficacy of Australian womenwith breast cancer: results from a cross-sectional, nationwide sur-vey. Eur J Oncol Nurs 23:72–80
56. Lynagh MC, Williamson A, Bradstock K, Campbell S, Carey M,Paul C, Tzelepis F, Sanson-Fisher R (2018)A national study of theunmet needs of support persons of haematological cancer survi-vors in rural and urban areas of Australia. Support Care Cancer26(6):1967–1977
57. Tzelepis F, Paul CL, Sanson-Fisher RW, Campbell HS, BradstockK, Carey ML, Williamson A (2018) Unmet supportive care needsof haematological cancer survivors: rural versus urban residents.Ann Hematol 97(7):1283–1292
58. White KJ, Roydhouse JK, D’Abrew NK, Katris P, O’Connor M,Emery L (2011) Unmet psychological and practical needs of pa-tients with cancer in rural and remote areas of Western Australia.Rural Remote Health 11(3):1784
59. Cahir C, Thomas AA, Dombrowski SU, Bennett K, Sharp L(2017) Urban-rural variations in quality-of-life in breast cancersurvivors prescribed endocrine therapy. Int J Environ Res PublicHealth 14(4):07
60. Pateman KA, Cockburn NL, Batstone MD, Ford PJ (2018)Quality of life of head and neck cancer patients in urban andregional areas: an Australian perspective. Aust J Rural Health26(3):157–164
61. Pedro LW, Schmiege SJ (2014) Rural living as context: a study ofdisparities in long-term cancer survivors. Oncol Nurs Forum41(3):E211–E219
62. Thomas AA, Timmons A, Molcho M, Pearce A, Gallagher P,Butow P, O’Sullivan E, Gooberman-Hill R, O’Neill C, Sharp L(2014) Quality of life in urban and rural settings: a study of headand neck cancer survivors. Oral Oncol 50(7):676–682
63. Thomas AA, Gallagher P, O’Ceilleachair A, Pearce A, Sharp L,Molcho M (2015) Distance from treating hospital and colorectalcancer survivors’ quality of life: a gendered analysis. Support CareCancer 23(3):741–751
64. Andrykowski MA, Steffens RF, Bush HM, Tucker TC (2014)Disparities in mental health outcomes among lung cancer survi-vors associated with ruralness of residence. Psycho-Oncology23(4):428–436
65. Andrykowski MA, Steffens RF, Bush HM, Tucker TC (2017)Posttraumatic growth and benefit-finding in lung cancer survivors:the benefit of rural residence? J Health Psychol 22(7):896–905
66. Carey M, Sanson-Fisher R, Paul C, Bradstock K, Williamson A,Campbell HS (2017) Psychological morbidity among Australianrural and urban support persons of haematological cancer survi-vors: results of a national study. Psychooncology 26(11):1952–1958
67. Corboy D, Meier J, McLaren S (2019) Self-reliance and stoicismas predictors of distress following radical prostatectomy in thecontext of place of residence. Psychol Men Masculinities 20(4):637–646
68. Grov EK, Fossa SD, Dahl AA (2011) Short-term and long-termelderly cancer survivors: a population-based comparative and
1062 Support Care Cancer (2022) 30:1021–1064
controlled study of morbidity, psychosocial situation, and life-style. Eur J Oncol Nurs 15(3):213–220
69. Gunn KM, Berry NM,MengX,Wilson CJ, Dollman J,WoodmanRJ, Clark RA, Koczwara B (2020) Differences in the health, men-tal health and health-promoting behaviours of rural versus urbancancer survivors in Australia. Support Care Cancer 28(2):633–643
70. Hall AE, Sanson-Fisher RW, Carey ML, Paul C, Williamson A,Bradstock K, Campbell HS (2016) Prevalence and associates ofpsychological distress in haematological cancer survivors.Support Care Cancer 24(10):4413–4422
71. Schootman M, Homan S, Weaver KE, Jeffe DB, Yun S (2013)The health and welfare of rural and urban cancer survivors inMissouri. Prev Chronic Dis 10:E152
72. Watts KJ, Good LH, McKiernan S, Miller L, O’Connor M, KaneR, Kruger DJ, Adams BR, Musiello T (2016) “Undressing” dis-tress among cancer patients living in urban, regional, and remotelocations in Western Australia. Support Care Cancer 24(5):1963–1973
73. Paul CL, Hall AE, Carey ML, Cameron EC, Clinton-McHarg T(2013) Access to care and impacts of cancer on daily life: do theydiffer for metropolitan versus regional hematological cancer sur-vivors? J Rural Health 29(Suppl 1):s43–s50
74. Vanderpool RC, Chen Q, Johnson MF, Lei F, Stradtman LR,Huang B (2020) Financial distress among cancer survivors inAppalachian Kentucky. Cancer Rep 3(2):e1221
75. Zahnd WE, Davis MM, Rotter JS, Vanderpool RC, Perry CK,Shannon J, Ko LK, Wheeler SB, Odahowski CL, Farris PE,Eberth JM (2019) Rural-urban differences in financial burdenamong cancer survivors: an analysis of a nationally representativesurvey. Support Care Cancer 27(12):4779–4786
76. Zucca A, BoyesA, NewlingG,Hall A, Girgis A (2011) Travellingall over the countryside: travel-related burden and financial diffi-culties reported by cancer patients in New South Wales andVictoria. Aust J Rural Health 19(6):298–305
77. Cipora E, Konieczny M, Karwat ID, Roczniak W, Babuska-Roczniak M (2018) Satisfaction with life among women withbreast cancer-selected demographic and social factors. AnnAgric Environ Med 25(2):314–319
78. Corboy D, McLaren S, McDonald J (2011) Predictors of supportservice use by rural and regional men with cancer. Aust J RuralHealth 19(4):185–190
79. McDowell ME, Occhipinti S, Ferguson M, Chambers SK (2011)Prospective predictors of psychosocial support service use aftercancer. Psycho-Oncology 20(7):788–791
80. Bazzell JL, Spurlock A, McBride M (2015) Matching the unmetneeds of cancer survivors to resources using a shared care model. JCancer Educ 30(2):312–318
81. Glasser M, Nielsen K, Smith SN, Gray C (2013) Psychosocialneeds of rural survivors of cancer and their partners. J PsychosocOncol 31(3):319–333
82. Riley-Clark A, Pieper BB (2014) Psychosocial needs of cancerpatients living in the Adirondacks: a needs assessment. J N YState Nurses Assoc 44(1):22–29
83. Coker AL, Luu HT, Bush HM (2018) Disparities in women’scancer-related quality of life by Southern Appalachian residence.Qual Life Res 27(5):1347–1356
84. Costrini NV (2011) Quality of life of rural Georgia colorectalcancer survivors. J Med Assoc Ga 100(4):26–29
85. Steenland K, Goodman M, Liff J, Diiorio C, Butler S, Roberts P(2011) Quality of life among men with prostate cancer in ruralGeorgia. Urology 77(4):927–933
86. Befort CA, Klemp J (2011) Sequelae of breast cancer and theinfluence of menopausal status at diagnosis among rural breastcancer survivors. J Women's Health (Larchmt) 20(9):1307–1313
87. DugglebyWD,Williams A, Holstlander L, Thomas R, Cooper D,HallstromLK, Ghosh S, O-RourkeH (2014) Hope of rural womencaregivers of persons with advanced cancer: guilt, self-efficacyand mental health. Rural Remote Health 14:2561
88. Lashbrook M, Bernardes CM, KirshbaumMN, Valery PC (2018)Physical functioning and psychological morbidity among regionaland rural cancer survivors: a report from a regional cancer centre.Aust J Rural Health 26(3):211–219
89. Schlegel RJ, Manning MA, Molix LA, Talley AE, Bettencourt B(2012) Predictors of depressive symptoms among breast cancerpatients during the first year post diagnosis. Psychol Health27(3):277–293
90. Mandaliya H, Ansari Z, Evans T, Oldmeadow C, George M(2016) Psychosocial analysis of cancer survivors in ruralAustralia: focus on demographics, quality of life and financialdomains. Asian Pac J Cancer Prev 17(5):2459–2464
91. Pisu M, Azuero A, Benz R,McNees P, Meneses K (2017) Out-of-pocket costs and burden among rural breast cancer survivors.Cancer Med 6(3):572–581
92. McNulty JA, Nail L (2015) Cancer survivorship in rural and urbanadults: a descriptive and mixed methods study. J Rural Health31(3):282–291
93. Hubbard G, Venning C, Walker A, Scanlon K, Kyle RG (2015)Supportive care needs of women with breast cancer in ruralScotland. Support Care Cancer 23(6):1523–1532
94. Martinez-Donate AP, Halverson J, Simon NJ, Strickland JS,Trentham-Dietz A, Smith PD, Linskens R, Wang X (2013)Identifying health literacy and health system navigation needsamong rural cancer patients: findings from the Rural OncologyLiteracy Enhancement Study (ROLES). J Cancer Educ 28(3):573–581
95. Torres E, Dixon C, Richman AR (2016) Understanding the breastcancer experience of survivors: a qualitative study of AfricanAmerican women in rural eastern North Carolina. J Cancer Educ31(1):198–206
96. Australian Institute of Health and Welfare (2019) Cancer inAustralia 2019. AIHW. https://www.aihw.gov.au/reports/cancer/cancer-in-australia-2019. Accessed 2 March 2020
97. Bettencourt BA, Talley AE, Molix L, Schlegel R, Westgate SJ(2008) Rural and urban breast cancer patients: health locus ofcontrol and psychological adjustment. Psycho-Oncol : Journal ofthe Psychological, Social and Behavioral Dimensions of Cancer17(9):932–939
98. Bain NS, Campbell NC (2000) Treating patients with colorectalcancer in rural and urban areas: a qualitative study of the patients’perspective. Fam Pract 17(6):475–479. https://doi.org/10.1093/fampra/17.6.475
99. Kroneman M, Verheij R, Tacken M, van der Zee J (2010) Urban-rural health differences: primary care data and self reported datarender different results. Health Place 16(5):893–902. https://doi.org/10.1016/j.healthplace.2010.04.015
100. Australian Government (2019) Australian jobs 2019. Departmentof Jobs and Small Business. https://australianjobs.employment.gov.au/. Accessed 21 September 2020
Publisher’s note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.