33


PSYCHOTIC MAJOR DEPRESSION Alan F. Schatzberg, MD Kenneth T. Norris, Jr. Professor Department of Psychiatry and Behavioral Sciences Stanford University School of Medicine Stanford, CA
PSYCHOTIC MAJOR DEPRESSION Martin B. Keller, MD Professor Department of Psychiatry & Human Behavior Alpert Medical School Brown University Providence, RI

ALAN F. SCHATZBERG, MD
● Research/Grants: None ● Speakers Bureau: None ● Consultant: BrainCells Inc.; CeNeRx BioPharma; Jazz
Pharmaceuticals, Inc.; Neuronetics Inc.; NovaDel Pharma; PharmaNeuroBoost; Sanofi-aventis; Sunovion Pharmaceuticals Inc.; Takeda Pharmaceuticals North America, Inc.
● Stockholder: Amnestix, Inc.; BrainCells Inc.; CeNeRx BioPharma; Corcept Therapeutics; Forest Laboratories, Inc.; Merck & Co., Inc.; Neurocrine Biosciences, Inc.; NovaDel Pharma; Pfizer Inc.; PharmaNeuroBoost; Somaxon; Synosis
● Other Financial Interest: Named inventor on pharmacogenetic and antiglucocorticoid use patents on prediction of antidepressant response; Associate Editor, American Journal of Geriatric Psychiatry
● Advisory Board: None
Disclosures

MARTIN B. KELLER, MD
● Research/Grants: None ● Speakers Bureau: None ● Consultant: CeNeRx BioPharma;
Medtronic, Inc. ● Stockholder: None ● Other Financial Interest: None ● Advisory Board: CeNeRx BioPharma
Disclosures
LEARNING OBJECTIVE Devise a strategy to improve the management and outcomes in patients with psychotic depression.

MM-031-062311-90
Calendar
Menu
Tests
Chart Review: James F.BACKGROUND
Personal: 57-year-old Caucasian male, worked for the Federal Government in the Washington, DC area
Neuropsychiatric History: Unremarkable. No psychiatric history.Intelligent, organized, and described as a hard-working, dedicated man.
Medical History: Unremarkable.
Family History: • Born in Beacon, New York, son of Irish immigrants• Married, wife had a history of problems with alcohol and a
psychiatric history
Work History: • Worked as a news reporter as a teen• Went to Princeton University for 3 years, did not graduate• Worked at a bond company working his way to become president of
the company• Began working for the Federal Government at age 48 to work for the
Treasury Department and then the Defense Department
TODAY’S VISIT
Chief Complaint and Psychiatric Interview Findings: • developed a number of symptoms suggestive of depression • feeling exhausted• having difficulty concentrating• indecisiveness• weight loss with a • haggard appearance and sunken eyes • precipitants included significant political stress at work • made a suicide attempt that did not result in hospitalization
Physical Findings: Weight loss, appears quite run down
Questionnaire and Lab Findings: No abnormal findings

MM-031-062311-90
Calendar
Menu
Tests
Chart Review: James F.Assessment and Plan: What are your initial diagnostic impressions? What further symptoms would you inquire about? How would you assess suicide risk?
Treatment: Patient was started on an SNRI and took off from work. He went to his vacation home on the beach. He was visited by one of his aides at the beach house two weeks later. He said to his aide—“Bob, they are after me.” As they walked on the beach, he thought the metal sockets in the sand for beach umbrellas had been wired to monitor his conversations. He thought the “Kremlin had him marked for liquidation.”
What is your diagnosis? What are your concerns for safety of the patient? What treatment recommendations do you make or institute?
Patient was hospitalized at Bethesda Naval Hospital. There he told a Navy psychiatrist he had failed at his job. At that time he was diagnosed as suffering from a “severe reactive depression…caused by intense pressure.”
He committed suicide in the hospital by a combination of hanging and falling from the 16th floor.
This is the case of James Forrestall, Secretary of Defense, who died in 1949 and as described in Steve Vogel: The Pentagon, New York, Random House, 2007.

MM-031-062311-90
Calendar
Menu
Tests
Chart Review: John R.BACKGROUND
Personal: 50-year-old Caucasian male, accountant, married, father of 3
Neuropsychiatric History: Negative psychiatric history (confirmed by spouse)
Medical History: History of mild hypertension
Family History: • Parents deceased• Married with 3 children• Wife works part-time
Social History: Has friends, enjoys sports
TODAY’S VISIT
Chief Complaint and Psychiatric Interview Findings: • 50-year-old married father of 3 • became depressed for the first time after he started working for a
new boss, the boss was seen as critical of his work • became increasingly agitated at home • difficulty sleeping • developed poor concentration• anhedonic • denied suicidal ideation • denies any past history of depression or hypomania or mania
Physical Findings: Unremarkable
Questionnaire and Lab Findings: Unremarkable

MM-031-062311-90
Calendar
Menu
Tests
Chart Review: John R.ASSESSMENT AND PLAN
What is your diagnostic impression? What treatments would you consider?• You start him on escitalopram and after 3 weeks at 20 mg per day
there is little change. He is still depressed and is finding it more difficult to work. His wife joins him in the session and notes he stands by the window a great deal and peeks out fearing there are men parked in cars who are watching him.
What is your response? What do you ask about?
What treatment recommendations do you make?• The patient his started on olanzapine 5 mg per day and it is increased
to 15 mg per day. A month later he is no better and at this point he has taken a leave of absence from his job. He remains delusional and now fears being poisoned and is refusing to eat.
What do you do next? What treatment changes do you consider?• Patient is hospitalized and ECT is begun. Patient responds nicely to 6
bilateral treatments.
What do you do next in terms of maintenance?

MAJOR DEPRESSION
● Mood-congruent psychotic features ● Delusions of guilt ● Delusions of deserved punishment ● Nihilistic delusions ● Somatic delusions ● Delusions of poverty ● Hallucinations, typically auditory and transient
● Represents 15% of major depressive episodes
Severe with Psychotic Features
American Psychiatric Association [DSM-IV-TR], 2000.

PSYCHOTIC DEPRESSION IN GENERAL POPULATION
● 18,980 subjects in five European countries ● Patients evaluated using Sleep-EVAL
system ● Current prevalence of non-psychotic major
depression: 2.0% ● Current prevalence of psychotic major
depression: 0.4% ● 18.5% of major depression subjects had
psychotic features Ohayon MM, et al. Am J Psychiatry. 2002;159(11):1855-1861.
Cell Membrane
Activated Receptor Complex
Nucleus
Receptor
Regulation of Gene Transcription
Translation and Protein Synthesis
mRNA
Hypothalamus
Adrenal
CRF
(+)
Pituitary (+) (-)
(-)
Glucocorticoid ACTH
Brain “Glucocorticoids influence about 20% of the expressed human genome and their effects spare
almost no organs or tissues.”
Chrousos & Kino. Science STKE 2005(304): pe48.
INTRACELLULAR GLUCOCORTICOID SIGNALING
Chrousos GP, et al. Sci. STKE, 4 October 2005 Vol. 2005, Issue 304, p. pe48

DST NONSUPPRESSION IN 14 COMPARISON STUDIES
64%
41%
0%
10%
20%
30%
40%
50%
60%
70%
PMD (N = 276) NPMD (N = 708)
% N
onsu
ppre
ssio
n
Mantel-Haenszel x2 = 47.43, p < .001 Homogeneity of Effect Size x2 = 11.39, p = NS Nelson JC, et al. Am J Psychiatry. 1997;154:1497-1503.

MAJOR NEUROPSYCHOLOGICAL DEFICITS IN PMD ● Attention
(Kim et al. Prog Neuropsychopharmacol. 1999; Gomez et al. Biol Psych. 2006)
● Executive function (Schatzberg et al. Am J Psychiatry. 2000; Jeste et al. Am J Psychiatry. 1996; Nelson et al. Am J Psychiatry. 1998; Hill et al. Am J Psychiatry. 2004; Mifepristone et al. 2001; Gomez et al. Biol Psych. 2006)
● Response inhibition (Schatzberg et al. Am J Psychiatry. 2000)
See supplemental bibliography for full references.

MAJOR NEUROPSYCHOLOGICAL DEFICITS IN PMD ● Story learning
(Jeste et al. Am J Psychiatry. 1996)
● Verbal declarative memory (Schatzberg et al. Am J Psychiatry. 2000; Belanoff et al. 2001; Gomez et al. Biol Psych. 2006)
● Visual memory & visual-spatial perception (Hill et al. 2004)
See supplemental bibliography for full references.

PMD: TREATMENT RESPONSE
● Low placebo response ● Poor response to tricyclics alone ● Responds well to amoxapine,
antidepressants + antipsychotics, or ECT ● Possible response to atypical
antipsychotics or SSRIs alone
DeBattista C, et al. Treatment of Psychotic Depression. In Halbreich U, Montgomery SA, Eds. Pharmacotherapy for mood, anxiety, and cognitive disorders. American Psychiatric Press, Washington, DC 2000. pp 305-314.

ECT IN PMD
● Psychosis was a predictor of relapse, as was comorbid Axis I and II disorders, site, and number of ECT treatments in the acute phase* ● Relapsed patients had a higher rate of
psychotic depression (31.1% vs. 22.2%)
* When controlling for site, # ECT treatments no longer significant
Prudic J, et al. Biol Psychiatry. 2004;55(3):301-312.

ATYPICAL AP PLUS SSRI IN PMD OLZ + FLU (OFC)
* Olanzapine therapy initiated at 10 mg/day; 249 patients enrolled in this protocol, 2:2:1 ratio of randomization Rothschild AJ, et al. J Clin Psychopharmacol. 2004;24(4):365-373.
Study Period I Screening Study Period II
Double-Blind Therapy Olanzapine 5-20 mg/day
Study Period III Open-Label Therapy
Olanzapine 0-2.5 mg/day Fluoxetine 20-80 mg/day Olanzapine 5-20 mg/day*
Fluoxetine 0-60 mg/day 3-9 days
Weekly Bi-Weekly visits
Placebo
Visit 1 Visit 2 Randomization Visit 6 Visit 8 Visit 301 Visit 304 Visit 307 Visit 311
or final visit Bi-monthly visits Monthly visits Weekly visits 1 Week

MEAN MODAL DOSE SUMMARY
Rothschild AJ, et al. J Clin Psychopharmacol. 2004;24(4):365-373.
Study OFC
(OLZ mg/FLU mg) OLZ (mg)
1 12.4/23.5 11.6
2 13.5/21.7 13.6
Combined 12.9/22.6 12.6

RESPONSE RATE
63.3%
34.9% 28.0%
0%
10%
20%
30%
40%
50%
60%
70%
OFC OLZ PBO
% R
espo
nder
s (H
AM
-D)
Rothschild AJ, et al. J Clin Psychopharmacol. 2004;24(4):365-373.
p = .027
p = .004
(n = 22) (n = 43) (n = 50)

WEIGHT (KG) MEAN CHANGES — COMBINED
* p < .05 vs. OFC Rothschild AJ, et al. J Clin Psychopharmacol. 2004;24(4):365-373.
Subgroup OFC
Change (N) OLZ
Change (N) PBO
Change (N)
Overall 2.74 (45) 3.79 (89) 0.39 (90)*
Male 2.24 (16) 4.69 (45)* 1.11 (47)
Female 3.02 (29) 2.88 (44) -0.39 (43)*

Hamilton Depression Scale (HAM-D) scores in subjects randomized to receive olanzapine plus placebo vs. olanzapine plus sertraline
HAM-D SCORES OLANZAPINE + PLACEBO VS. OLANZAPINE + SERTRALINE
Meyers BS, et al. Arch Gen Psychiatry. 2009;66(8):838-847.

INTRACELLULAR CORTICOSTEROID RECEPTOR TYPES IN THE BRAIN
● Mineralocorticoid (MR) ● High affinity for cs
(kd = 0.5 nM) ● In limbic structures ● Agonist: aldosterone ● Antagonist: RU
26752, spironolactone
● Glucocorticoid (GC) ● Lower affinity for
cs (kd = 5.0 nM) ● Ubiquitous ● Agonist:
dexamethasone ● Antagonist: RU
38486
DeKloet ER, et al. Endocr Rev. 1998;19(3):269-301.

MIFEPRISTONE (AKA, C-1073, RU-486)
● Formulated 1981 by Roussell-Uclaf ● Approved in Europe and Asia – 1988 ● Approved in United States –
September 28, 2000 ● Progesterone receptor antagonist ● GRII antagonist (no GRI antagonist) ● Virtually no affinity for any other receptor
MIFEPRISTONE
● 440 patients
● 300, 600, and 1200 mg mifepristone for 7 days vs. placebo
● Multicenter
● BPRS PSS response at both day 7 and 56
Multiple Fixed-Dose Study
Blasey C, et al. J Clin Psychopharmacol, in press.

MIFEPRISTONE
44%
34%
0%
10%
20%
30%
40%
50%
Mifepristone Placebo
Res
pons
e R
ate
(%)
BPRS PSS at Days 7 and 56
Multiple Fixed-Dose Study
p = .144
Blasey C, et al. J Clin Psychopharmacol, in press.
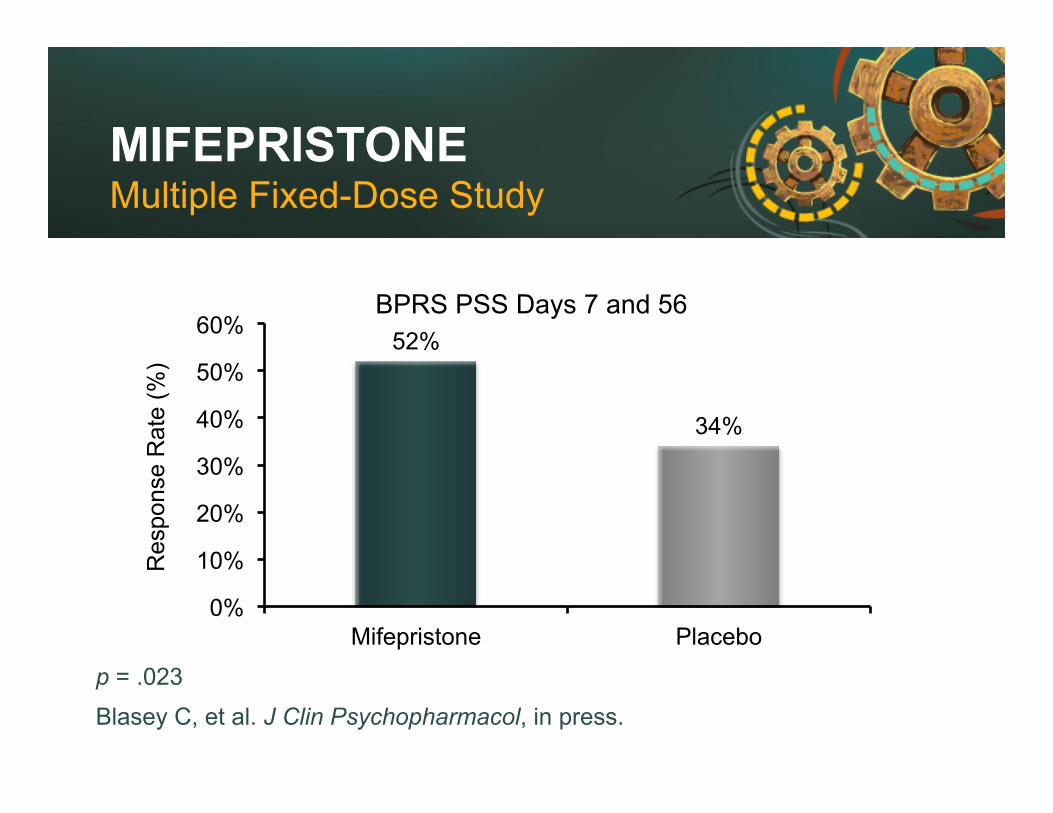
MIFEPRISTONE Multiple Fixed-Dose Study
p = .023
Blasey C, et al. J Clin Psychopharmacol, in press.
52%
34%
0%
10%
20%
30%
40%
50%
60%
Mifepristone Placebo
Res
pons
e R
ate
(%)
BPRS PSS Days 7 and 56
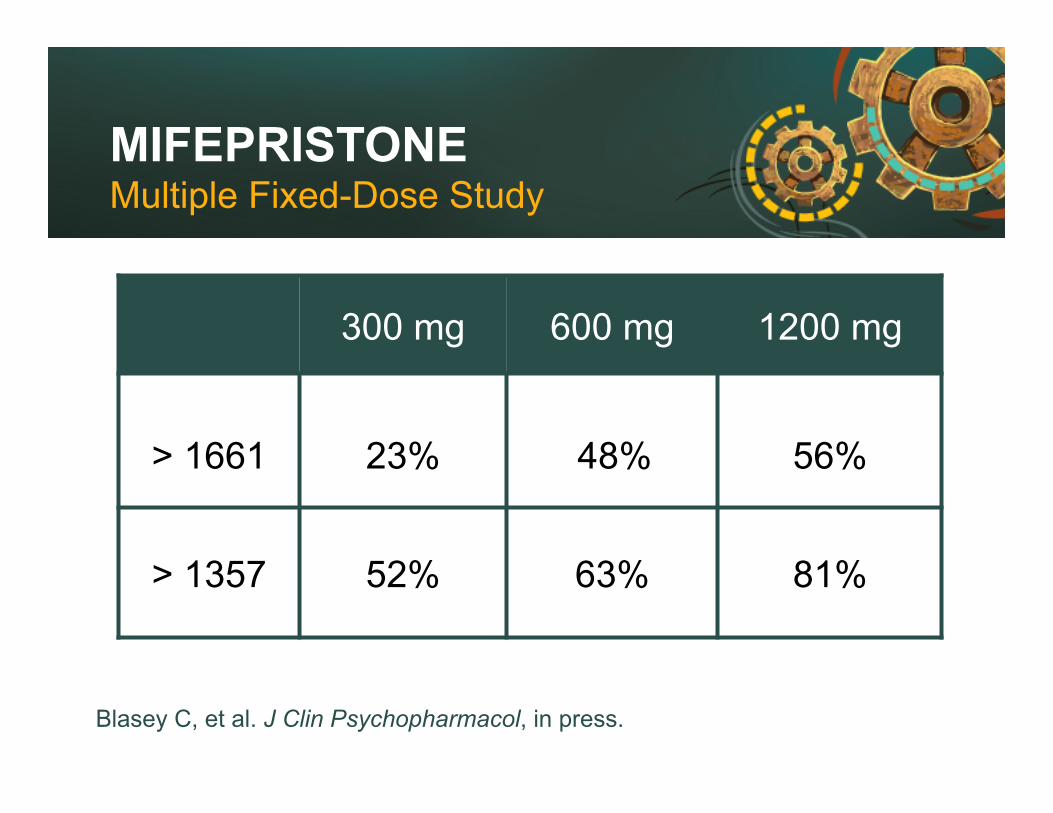
MIFEPRISTONE
300 mg 600 mg 1200 mg
> 1661
23%
48%
56%
> 1357 52% 63% 81%
Multiple Fixed-Dose Study
Blasey C, et al. J Clin Psychopharmacol, in press.

SUMMARY & CLINICAL CONNECTIONS
● PMD is a severe and relatively common subtype ● PMD associated with elevated HPA axis
activity and neurocognitive impairment ● Currently effective therapies are primarily
AP/AD combination and ECT ● Mifepristone appears to reduce psychotic
symptoms in PMD

SUMMARY & CLINICAL CONNECTIONS
● Mifepristone accentuates cortisol and ACTh rhythm ● Changes in HPA measures appear to be
associated with durability of response

QUESTIONS AND ANSWERS


















