24
Public-Private Hospital Utilisation: Have the recent PHI policies achieved their objective? By Preety Ramful Centre for Health Economics Monash University September 2006
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| View: | 219 times |
| Download: | 0 times |

Public-Private Hospital Utilisation: Have the recent PHI policies
achieved their objective?
ByPreety Ramful
Centre for Health EconomicsMonash UniversitySeptember 2006

Background• Towards the end of the 1990s, private health
insurance coverage had dropped to about 40%. This raised concern among authorities that health care would drain public revenues.
• To encourage membership, a package of incentives and penalties were introduced towards the end of the nineties. These included– a tax penalty for high-income individuals without
private cover, – a 30% rebate on PHI premiums, and– a lifetime health cover.

Background• However, the role of government subsidies in
easing pressures on the public hospital system has raised a lot of eyebrows (Hall et al., 1999; Duckett and Jackson, 2000; Deeble, 2002; Sundararajan et al., 2004; Fiebig et al., 2006).
• It is argued that despite the increase in PHI membership in recent years, the use of private health services has remained low in Australia.

Background
• Private health insurance covers are said to be taken purely for financial reasons (Fiebig et al. 2006).
• It is argued that the resources could have been better spent if they were used directly to enhancing the capacity of public hospitals to meet the additional demand for health services (see Duckett and Jackson, 2000; Willcox, 2001).

Motivation• The study is motivated by the fact that a
significant proportion of the population who has a private insurance opt for public treatment in hospitals.
• Another motivation arises from the disproportionate use of private health care by households in the upper part of the income distribution. This raises concern whether the tax rebate is regressive.

Previous Studies
• The demand for private health insurance has received a lot of attention in the literature….
• On the other hand, only a small body of research has examined its role in public/private health care utilisation (Propper, 2000; Holly et al., 1998; Harmon and Nolan, 2001; Rodriguez and Stoyanova, 2004; Fiebig et al., 2006).
• Fiebig et al. (2006) examined the relationship between health insurance and hospital admission. Their focus was more on the impact of insurance type - in terms of reasons for purchasing private health insurance - on the probability of hospital admission in Australia.

Previous Studies• Proper (2000) modelled hospital admission status in the
UK. In particular, he found that the demand for private health care was strongly determined by income, political allegiance, attitudes to the role of state in the provision of health care, and more importantly the past use of private care. – Private health insurance data not available. Instead,
he used occupational dummies as instruments for corporate cover.
• A few earlier studies have examined the impact of private health insurance on the admission/non-admission in hospitals making no distinction between whether the patient was admitted as a public or private patient (Cameron et al., 1988; Holly et al., 1998; Harmon and Nolan, 2001).

Objective
• This study examines the impact of PHI on the use of public vs private hospital utilisation using NHS 2004-05 data.

Hospital Admission17%
PHI with hospital cover
46.8%
No PHI53.2%
Private patient at most
recent admission6.9%
Medicare patient at most
recent admission93.1%
Medicare patient at most
recent admission19.6%
Private patient at most
recent admission80.4%
(NHS 2004-05, N=19501)
Public/Private Hospital Utilisation

6%
21%
21%
23%
24%
19%
9%
4%
8%
8%
6%
44%
0.00 0.10 0.20 0.30 0.40 0.50
security or protection or peace of mind
lifetime cover or avoid age surcharge
choice of doctor
allow treatment as private patient in hospital
provides benefits for ancillary services or extras
shorter wait for treament or concerned over publichospital
always had it or parents pay it or condition of job
to gain government benefits or avoid extra medicarelevy
other financial reasons
has condition that requires treatment
elderly or getting older or likely to need treatment
other reason
Incentives for PHI cover

36%
11%
12%
15%
24%
16%
4%
21%
6%
7%
7%
10%
46%
4%
24%
23%
22%
26%
23%
6%
4%
8%
8%
5%
0.00 0.10 0.20 0.30 0.40 0.50
security or protection or peace of mind
lifetime cover or avoid age surcharge
choice of doctor
allow treatment as private patient in hospital
provides benefits for ancillary services orextras
shorter wait for treament or concerned overpublic hospital
always had it or parents pay it or condition ofjob
to gain government benefits or avoid extramedicare levy
other financial reasons
has condition that requires treatment
elderly or getting older or likely to needtreatment
other reason
PHI>5 years
PHI<=5 years
Incentives for PHI cover
pre- and post1999/00 policy
changes
Incentives for PHI cover pre- and post-1999/00 policy changes
• The purchase of PHI in post 1999-00 appears to be driven by financial reasons rather than to access private hospital care.

Econometric ModelBivariate Probit Model with sample selection

Bivariate Probit Results: PP Model
Coefficient S. ErrorConstant -1.385 0.48430-39 0.273 0.12340-49 0.049 0.12350-59 0.249 0.14060-69 0.538 0.18270-79 0.487 0.18180+ 1.014 0.210Male -0.161 0.069Married 0.214 0.066Majorcity -0.059 0.105InnerReg -0.050 0.106WorkFT 0.003 0.125WorkPT 0.006 0.115Workstud 0.161 0.218StudyFT -0.238 0.220Unemp 0.019 0.294Degree 0.292 0.099Trade 0.191 0.089Year12 0.267 0.0884th Decile 0.290 0.1195th Decile 0.303 0.1156th Decile 0.269 0.1227th Decile 0.327 0.1238th Decile 0.282 0.1329th Decile 0.409 0.12910th Decile 0.409 0.132Athritis 0.161 0.077Cancer 0.111 0.164Heart 0.048 0.076Diabetes -0.093 0.121Asthma -0.065 0.094Osteo 0.085 0.116Copay -0.001 0.003Bed -0.098 0.059FTEMP -1.090 0.459PHIhosp 1.760 0.176PHI5M 0.242 0.082RHO(1,2) 0.548 0.159
coefficient SEConstant -0.412 0.10330-39 -0.136 0.04340-49 -0.260 0.04450-59 -0.253 0.04860-69 -0.226 0.05570-79 -0.189 0.06080+ -0.138 0.070Male -0.100 0.027Married 0.032 0.029ProfEng 0.137 0.080Depkid 0.138 0.037Singlepar -0.047 0.057Majorcity -0.011 0.034InnerReg 0.033 0.039Degree 0.048 0.041Trade 0.099 0.034Year12 0.019 0.0334th Decile -0.029 0.0485th Decile 0.091 0.0476th Decile 0.066 0.0507th Decile 0.056 0.0518th Decile 0.032 0.0539th Decile 0.111 0.05310th Decile 0.160 0.054WorkFT -0.369 0.041WorkPT -0.154 0.041Workstud -0.139 0.108StudyFT -0.366 0.082Unemp -0.255 0.087XLhealth -0.743 0.058Vghealth -0.659 0.052Ghealth -0.453 0.048Athritis 0.093 0.030Cancer 0.490 0.065Heart 0.157 0.029Diabetes 0.180 0.050Asthma 0.044 0.037Osteo 0.067 0.054
Public-Private Admission Hospital Utilisation

Selectivity Coefficient
• To test for selection effects, the appropriate approach is to test the hypothesis of no effects which results if
• =0.548 and significant at the 1% level. Implies that sample selection needs to be accounted for.

Income Effect
• Income is a very important determinant of the use of private hospital utilisation
– Those who are under the poverty line (household income <=$249 per week) are less likely to be admitted as private patients in hospitals
– The use of private hospital care (PHC) increases almost progressively with income.
– Those in the middle income group (6th decile) have around 10% higher chances of using PHC than those under the poverty line and those in the highest income group (10th decile) have nearly 14% higher chances of using private hospital services.
• Disproportionate use of private health care by households in the upper part of the income distribution.
4th Decile 0.122 (0.049)** 0.005 (0.009) 0.127 (0.049)**5th Decile 0.127 (0.048)** -0.017 (0.011) 0.110 (0.047)**6th Decile 0.113 (0.052)** -0.012 (0.010) 0.101 (0.051)**7th Decile 0.137 (0.050)** -0.010 (0.010) 0.127 (0.050)**8th Decile 0.118 (0.054)** -0.006 (0.010) 0.112 (0.054)**9th Decile 0.171 (0.052)** -0.020 (0.013) 0.151 (0.052)**10th Decile 0.171 (0.055)** -0.029 (0.015)* 0.142 (0.054)**Standard errors are given in parentheses. * significant at 10% level. ** significant at 5% level.
Direct Effect Indirect Effect Total Effect

• Age effect: There appears to be a more or less progressive use of private hospital care with age. – For instance, individuals ages 30-39 are around 14% more likely
to use PHC than the age group <30 and the age-group 60-79 have about 28% higher chances to be admitted as private patients in hospitals
– The chances of using PHC are even high higher in the 80+ age group. They are more than 50% more likely to use PHC.
Age EffectAge Effect:30-39 0.114 (0.048)** 0.025 (0.012)** 0.139 (0.046)**40-49 0.020 (0.051) 0.047 (0.020)** 0.068 (0.047)50-59 0.104 (0.054)* 0.046 (0.020)** 0.150 (0.049)**60-69 0.226 (0.066)** 0.041 (0.019)** 0.267 (0.062)**70-79 0.204 (0.067)** 0.034 (0.018)* 0.238 (0.064)**80+ 0.425 (0.070)** 0.025 (0.016) 0.450 (0.069)**Standard errors are given in parentheses. * significant at 10% level. ** significant at 5% level.
Direct Effect Indirect Effect Total Effect
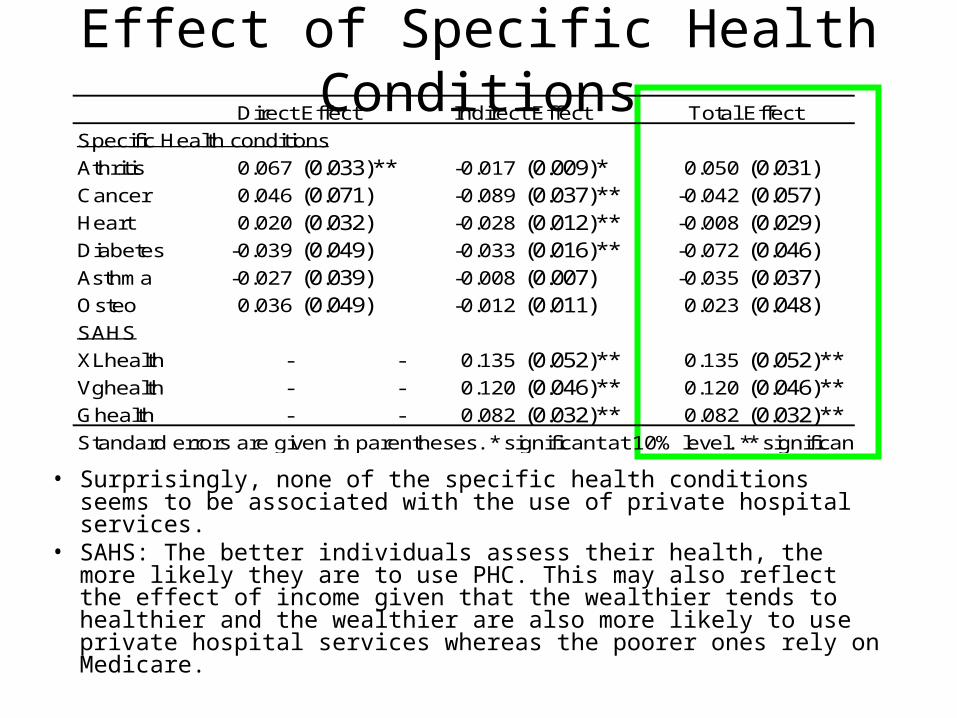
• Surprisingly, none of the specific health conditions seems to be associated with the use of private hospital services.
• SAHS: The better individuals assess their health, the more likely they are to use PHC. This may also reflect the effect of income given that the wealthier tends to healthier and the wealthier are also more likely to use private hospital services whereas the poorer ones rely on Medicare.
Effect of Specific Health ConditionsSpecific Health conditions
Athritis 0.067 (0.033)** -0.017 (0.009)* 0.050 (0.031)Cancer 0.046 (0.071) -0.089 (0.037)** -0.042 (0.057)Heart 0.020 (0.032) -0.028 (0.012)** -0.008 (0.029)Diabetes -0.039 (0.049) -0.033 (0.016)** -0.072 (0.046)Asthma -0.027 (0.039) -0.008 (0.007) -0.035 (0.037)Osteo 0.036 (0.049) -0.012 (0.011) 0.023 (0.048)SAHS
XLhealth - - 0.135 (0.052)** 0.135 (0.052)**Vghealth - - 0.120 (0.046)** 0.120 (0.046)**Ghealth - - 0.082 (0.032)** 0.082 (0.032)**Standard errors are given in parentheses. * significant at 10% level. ** significant at 5% level.
Direct Effect Indirect Effect Total Effect

• Quality of public services: Here, we use some variables to indicate quality of care of in public hospitals, i.e. bed density, density of full-time equivalent medical practitioners (FTEMP), proportion waiting for >1yr for elective procedures. – However, FTEMP and prop waiting for >1yr have very little variation
given that they vary only by states and territories. – There is some more variation in bed density given that there is data by
‘remoteness’.– Here, we find an inverse relationship between use of PHC and quality of
public hospitals. The higher are bed density and FTEMO (i.e. better public hospital services), the lower is the probability of private hospital utilisation.
– The effect of the waiting time is positive but statistically insignificant.
Quality of Public Care and Copayment Effects
Bed -0.041 (0.024)* - - -0.041 (0.024)*FTEMP -0.457 (0.189)** - - -0.457 (0.189)**Copayment -0.001 (0.001) - - -0.001 (0.001)
Direct Effect Indirect Effect Total Effect

Effect of Copayments
• We also examine the effect of copayments on the use of private hospital care. The variable used here represents the ‘average out-of-pocket payments by patients over all hospital services including those services where there was no gap in 2004-05’(source: PHIAC). – Varies at state level- Unfortunately, this variable as
well has very little variation.– The effect of this variable is negative but statistically
insignificant.

State Indicators
• Alternately, we can use state indicators to capture state-level differences (collectively) in copayments and quality of public hospital (such as waiting time for elective procedures, bed availability, doctors availability etc).– we find a significant variation in private hospital utilisation across
states and territories.– The highest use of private hospital services is in QLD and TAS.
For instance in QLD individuals have 15% highest chances of being admitted as a private patient in a hospital than in NSW.
VIC 0.021 (0.042) - - 0.021 (0.042)QLD 0.152 (0.042)** - - 0.152 (0.042)**SA 0.030 (0.043) - - 0.030 (0.043)WA 0.010 (0.045) - - 0.010 (0.045)TAS 0.136 (0.051)** - - 0.136 (0.051)**NTR 0.080 (0.668) - - 0.080 (0.668)ACT 0.049 (0.054) - - 0.049 (0.054)Standard errors are given in parentheses. * significant at 10% level. ** significant at 5% level.
Direct Effect Indirect Effect Total Effect

Effect of PHI
• As expected, those with a private hospital cover have higher chances of using private hospital care than those who do not have a PHI cover.
• The effect of the dummy is also found to be positive and significant.
• This suggest that individuals who have been covered for more than five years are about 83.8% (73.7%+10.1%) more likely to use PHC whereas those who have bought PHI cover in only recent years have 73.7% higher chances to use PHC
• Differential effect between phi>=5 and phi<5.
PHI 0.737 (0.034)** - - 0.737 (0.034)**PHI5M 0.101 (0.034)** - - 0.101 (0.034)**Standard errors are given in parentheses. * significant at 10% level. ** significant at 5% level.
Direct Effect Indirect Effect Total Effect

Conclusions
• There is a disproportionate use of private health care by households in the upper part of the income distribution……this raises concern whether the tax rebate is regressive.
• Those who have bought PHI in recent years have a lower probability of using private health services. Their decision to purchase PHI is mostly driven by financial incentives.
• Given that the recent tax rebates and have failed to increase private hospital utilisation and decrease demand pressures in public hospitals, the expenditure on the rebate could have/can been used more efficiently through supporting public hospitals directly.

Further Work
• Endogenise PHI and estimate as a system of 3 equations

















