45
$KXGPVTKEWNCT 'PNCTIGOGPV*[RGTVTQRJ[

Cardiology TODAY
VOLUME XXI No. 2MARCH-APRIL 2017
PAGES 49-92
Rs. 1700/- ISSN 0971-9172 RNI No. 66903/97
www.cimsasia .com
MANAGING DIRECTOR & PUBLISHERDr. Monica Bhatia
EDITOR IN CHIEFOP Yadava
SECTION EDITORSSR Mittal (ECG, CPC), David Colquhou n (Reader’s Choice)
NATIONAL EDITORIAL ADVISORY BOARDArun K Purohit, Arun Malhotra, Ashok Seth, Ashwin B Mehta, CN Manjunath, DS Gambhir, GS Sainani, Harshad R Gandhi, I Sathyamurthy, Jagdish Hiremath, JPS Sawhney, KK Talwar, K Srinath Reddy, KP Misra, ML Bhatia, Mohan Bhargava, MR Girinath, Mukul Misra, Nakul Sinha, PC Manoria, Peeyush Jain, Praveen Jain, Ramesh Arora, Ravi R Kasliwal, S Jalal, S Padmavati, Satyavan Sharma, SS Ramesh, Sunil Kumar Modi, Yatin Mehta, Yogesh Varma, R Aggarwala.
INTERNATIONAL EDITORIAL ADVISORY BOARDAndrew M Tonkin, Bhagwan Koirala, Carlos A Mestres, Chuen N Lee, David M Colquhoun, Davendra Mehta, Enas A Enas, Gerald M Pohost, Glen Van Arsdell, Indranill Basu Ray, James B Peter, James F Benenati, Kanu Chatterjee, Noe A Babilonia, Pascal R Vouhe,Paul A Levine, Paul Simon, P K Shah, Prakash Deedwania, Salim Yusuf, Samin K Sharma, Sanjeev Saxena, Sanjiv Kaul, Yutaka Imoto.
DESK EDITORGandhali
DESIGNER A run Kharkwal
OFFICES UBM Medica India Pvt LtdRegistered OfficeMargosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengaluru -560 003 Karnataka, IndiaTel: +91-80-4346 4500Fax: +91-80-4346 4530
Corporate OfficeBoomerang (Kanakia Spaces), Wing-B1, 403,4th Floor, Chandiwali Farm Road, ChadiwaliPowai, Mumbai - 400 072Tel.: +91-22-6612 2600 Fax : +91-22-6612 2626
Regional Off ice709, 7th Floor, Devika Tower, Nehru Place, New Delhi-110 019, India. Tel: +91-11-4285 4300Fax: +91-11-4285 4310
EDITORIALBudgeting the Doctors- Aren't we one too many? 51OP YADAVA
REVIEW ARTICLEDoor to Balloon Time for STEMI in Indians: Challenges and Solutions 53H.K. CHOPRA
REVIEW ARTICLEDrug Therapy for Treating Chronic Heart Failure 57ABHISHEKH SINGH, UPENDRA KAUL
REVIEW ARTICLEManaging Persistent Hyperglycemia is a Challenge for Patient and Physician 68MOHIT MINAL, SABOO BANSHI, SANJEEV MAHESHWARI, MOHIT VOHRA
Cardiology Today VOL.XXI NO. 2 MARCH-APRIL 2017 49

FOR MARKETING QUERIESAparna Mayekar: +91-9930937020+91-22-6612 [email protected]
FOR EDITORIAL QUERIESDr Gandhali : [email protected]
©2017 UBM Medica India Pvt Ltd Copyright in the material contained in this journal (save for advtg. and save as otherwise indicated) is held by UBM Medica India Pvt Ltd Margosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengal uru-560 003, Karnataka, India. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, photocopying or otherwise, without prior permission of the publisher and copyright owner.
The products and services advertised are those of individual advertisers and are not necessarilty endorsed by or connected with the publisher or with Cardiology Today or UBM Medica India Pvt Ltd. Cardiology Today does not guarantee, directly or indirectly, the quality or efficacy of any product or services described in the advertisements in this issue, which are purely commercial in nature.
The editorial opinions expressed in this publication are those of individual authors and not necessarily those of the publisher. Whilst every effort has been made to ensure the accuracy of the information in this publication, the publisher accepts no responsibility for errors or omissions.
For reprints (minimum order: 500) contact the production Department. Further copies of Cardiology Today are available from UBM Medica India Pvt Ltd, 709, Devika Tower, Nehru Place, New Delhi-110 019, India.
Cardiology Today is Published and Printed by UBM Medica India Pvt Ltd, Margosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengaluru - 560 003, IndiaTel: +91-80-4346 4500 (Board); Fax: +91-80-4346 4530
Printed at Modest Print Pack (P) Ltd., C-52, DDA Sheds Okhla Industrial Area, Phase-I, New Delhi-110 020.
IMAGEEchocardiographic evaluation of complica-tions of infective endocarditis 82SR MITTAL
ECG OF THE MONTHBiventricular Enlargement/ Hypertrophy 85SR MITTAL
PICTORIAL CMEWolff-Parkinson-White Syndrome Mimicking High Lateral Myocardial Infarction 90MONIKA MAHESHWARI
50 Cardiology Today VOL. XXI NO. 2 MARCH-APRIL 2017

Cardiology Today VOL.XXI NO. 2 MARCH-APRIL 2017 51
Budgeting the Doctors - Aren’t we one too many ?
EDITORIAL
Union Budget 2017, as usual gave a short shrift to health, but arguably a shorter shrift. There is a 28% increase in allocation for health. However, it is not the quantitative nature of this budget which excites me, but the qualitative aspects with respect to the formulation and introduction of medical device rules. Just as removal of regulatory bottle necks for manufacturing and importing medical devices, based on risk appropriation, is a welcome step as also the system of third party confi rmatory assessment and certifi cation through notifi ed bodies, these third party bodies should be free of governmental control and interference. It should also be made mandatory that these bodies have on board professional and clinical experts, practicing actively, rather than just degree holders and administrators having no knowledge of ground realities. Self compliance of class A medical devices is laudable but unfortunately, historically has always failed. Infact in an editorial1 recently in the New England Journal of Medicine, Resar and Weisfeldt commented, ‘we have virtually no structured, standardised way in the US – or any where else in the world for that matter – to assess the performance of medical devices after they have been approved. And there is no real incentive for industry to do so, except for device iteration and market competitiveness’. Infact most post-marketing studies conducted by the industry for self compliance are under powered, incomplete and the results manipulated and juggled to suit the industry. Its therefore important that we don’t rely on the industry to provide post-marketing surveillance, but there should be a system evolved, which captures data directly for the users without the interference and intervention of the industry. The proposed third party appraisers must create a database, where the users should be enrolled directly and the industry should be kept blinded till such a late stage, that the data has been collected, collated, analysed and conclusions drawn. It is only at this stage, the fi ndings should be released along with the raw data to the industry, so that they can view it with a fresh perspective and point out if any inadvertent error of interpretation has crept in. However, the database must keep the user un-identifi ed, as a lot of top doctors are not only infl uenced, but also sponsored, by the industry and may fear retribution and harm to their pre-eminence in the respective fi eld of performance. We should also make sure that any end user with fi nancial or other dealings with industry, is either kept away from this surveillance, or else, weightage of the feed back is given according to the neutrality
DR. OP YADAVACEO and Chief Cardiac Surgeon
National Heart Institute,New Delhi

52 Cardiology Today VOL. XXI NO. 2 MARCH-APRIL 2017
EDITORIAL
of the user. Patient is usually a hapless stake holder in this industry-profession nexus, unless this post-marketing surveillance is made a verifi able and authentic mechanism, he shall continue to be so.
Increase of 5,000 post graduate seats amounting to 15% of the existing seats, seems counter intuitive to the focus of developinghealth and welfare centres and promoting health in a holistic way. Post graduate seats will add to the provisioning of tertiary care but what this country needs is primordial and primary care. Leave alone a developing country like ours, chasing disease is not anaffordable option even for developed world. Specialist work force would only do that, so what we need is gross root medical andpara medical workforce working toward promoting health and preventing disease. It would therefore have served the government well, if instead of increasing these post graduate seats, time, energy and funding had been diverted to develop infrastructure in rural and semi-urban areas to draw the inequitably distributed specialist work force in health from cities to these under-served areas.
We don’t need more, we just need equitable distribution of the existing workforce. History and past experiences bear testimony -eventhese extra specialists, once they pass out, will concentrate in urban areas, thus adding to the mess there, rather than contributing to the health of the country, which lies in our rural areas.
India needs ‘health providers’ and not ‘disease mongers’ and ‘treaters’.
REFERENCE1. Resar J and Weisfeldt ML. Linkage of safety information to Regulatory Action. N Engl J Med. 2017;376:578-579.

Cardiology Today VOL.XXI NO. 2, 2017 53
Door to Balloon Time for STEMI in Indians: Challenges and Solutions
REVIEW ARTICLE
H.K. CHOPRAKeywords � PCI � STEMI � Door to balloon time � TNK � LAD � Thrombolysis
Dr. H.K. Chopra is Chief Cardiologist, Moolchand Medcity, New Delhi
A scenario not infrequently encountered in our practice is given below. A 45-year-old normotensive and non-diabetic male shopkeeper had chest and upper abdominal pain beginning early in the morning. The pain initially was intermittent and temporarily subsided. Our patient attributed the discomfort to upper gastrointestinal discomfort and he had some home available remedies for gastric discomfort. Four hours later, after reaching his workplace, the pain returned
in a severe form and was associated with vomiting. He reached out to the local general practitioner, who evaluated him and administered injectable ranitidine and antiemetics. There was temporary improvement and he went back to his offi ce. He applied for leave to take rest. On the way home, he had an episode of fainting and was rushed to the hospital in the nearby town which was 40 kms away. He was admitted and evaluated to have extensive ST Elevation anterior
AbstractThe issue brings out glaring defi ciencies at various levels in STEMI care in India. Individually, we have excellent hospitals, physicians, clinical cardiologists, and cardiac interventionists. Of late we are having good ambulance services, at least in some states. This commentary focuses on the possible systems that may be put in place to improve the acute care of STEMI across India. The scenario brings forth a few major lacunae in STEMI care that include lack of dedicated STEMI care systems, lack of instantaneously available ECG facility at fi rst point of medical contact, lack of patient awareness, lack of physician readiness, lack of equipped ambulance systems network for patient transport. These are the major reasons for the excess mortality and poorer outcomes seen in Indian patients with STEMI. Signifi cant barriers to effective STEMI care include public awareness level, patient level, hospital/physician level and at Government and societal levels. Organized patient education and awareness programs are needed to overcome these problems.

54 Cardiology Today VOL. XXI NO. 2, 2017
wall myocardial infarction (STEMI) with qRBBB. He was thrombolysed with streptokinase with a window period of 14 hours. He seemed to be stable. Later in the night, the patient developed acute pulmonary edema and required intravenous diuretics, nitroglycerine and morphine. Next day morning, the patient was referred to a percutaneous coronary intervention (PCI) capable centre, which was 50 kms away. He underwent an angiogram that showed an occluded proximal left anterior descending artery and an ejection fraction (EF) of 20-25%. He underwent rescue PCI and stenting to proximal left anterior descending coronary artery (LAD) with non-medicated stent. The procedure was complicated by no fl ow and hypotension, for which adjunctive pharmacotherapy along with intra-aortic balloon pump were used. He remained in coronary care unit (CCU) for 7 days and was later discharged with an EF of 20-25%. The patient was discharged on multiple medications. One month after his acute myocardial infarction (MI), the patient continued to have class III dyspnea with exertion and was unable to return to work. A follow-up echocardiogram (ECG) demonstrated impaired left ventricular systolic function (EF 25%) with severe apical hypokinesis. He was advised an implantable cardiac defi brillator, which he could not afford.
The above scenario is fairly frequently seen by Indian cardiologists even in 2017. The case brings out glaring defi ciencies at various levels in STEMI care in India. Individually, we have excellent hospitals, physicians, clinical cardiologists, and cardiac interventionists. Of late, we are having good ambulance services, at least in some states. However, we do not have any system in place for STEMI care across the country. Dedicated STEMI programs are successfully implemented in many Western countries for nearly three decades. This commentary focuses on the possible systems that may be put in place to improve the acute care of STEMI across India. Most of the improvement in outcomes in Indian patients could be achieved by timely implementation of the proven therapies focusing on the time window.
PROBLEMS IN STEMI CARE IN INDIAIndian acute coronary syndrome (ACS) patients, for reasons not exactly clear, seem to present with higher percentage of STEMI. They are less likely to receive timely reperfusion therapy, invasive therapy and evidence based medicines.1-3
The above patient scenario brings forth a few major lacunae in STEMI care that include lack of dedicated STEMI care systems, lack of instantaneously available ECG facility at fi rst point of medical contact, lack of patient awareness, lack of physician readiness, lack of equipped ambulance systems network for patient transport (Emergency Cardiac Services : ECS) and pay from pocket for even Emergency Medical Services (EMS). These are the major reasons for the excess mortality and poorer outcomes seen in Indian patients with STEMI.3
In a registry involving 50 cities, only 58.5% of patients with STEMI were thrombolysed mostly with streptokinase and a minority received PCI. The average delay in presentation was >6 hours. The real situation in most parts of India is likely to be lower as these registries have sampled data from tertiary care centres and some of the better developed states. The reported 30-day outcomes for patients with STEMI in the CREATE registry were death (8.6%), reinfarction (2.3%), and stroke (0.7%).3 Mortality benefi ts of Primary PCI are lost if it is delayed more than 60 minutes as depicted in the Global Registry of Acute Coronary Event.4 Importantly, the poor are marginalized in STEMI care and are less likely to receive thrombolytics, PCI and even lipid-lowering drugs. Consequently, the mortality was also higher for poor patients.5
In the Italian Registry of tenecteplase (TNK) in STEMI of 27,000 patients,6 it has been shown that thrombolysis with TNK is easily, accessible and available everywhere. If door to balloon time in PPCI exceeds 90 minutes, then PPCI does not reduce mortality consistently. Rapid diagnosis and early reperfusion are pillars of success in STEMI Care. TNK is Class 1A recommendation for STEMI (ACCP Guidelines7) and is recommended in Pre-Hospital Thrombolysis Protocol (Vienna
STEMI Registry8, The Mayo Clinic STEMI Protocol9 and The French FAST-MI registry10). The potential of TNK cannot be overemphasized. It is given in a bolus dose with no hypertension, no allergic reactions, longer half life, high fi brin specifi city and simplifi ed weight adjusted dose, with mostly very minor manageable bleeding. It is an agent of fi rst choice for pre-hospital thrombolysis in STEMI. It has been shown in one of the study that only 4% of transferred patients received PPCI within 90 Min.11 Pre-hospital thrombolysis is the strongest independent predictor of in-hospital survival in UK.12
Recently published Indian registry on STEMI consisting of 15,222 patients 722 centres, treated with indigenous TNK has shown clinically successful thrombolysis in 96.5% of patients in less than three hours, 96% in three to six hours and 85.3% in more than six hours of STEMI.13 Pharmaco invasive therapy includes early administration of thrombolysis (TNK) followed by PCI within 3-24 hours after initiation of thrombolytic therapy regardless of success of thrombolysis. However, in case of thrombolytic failure, a rescue PCI should be instantaneously performed. Timely guided protocol for early thrombolysis with TNK (Grade IA) at the level of physician, non-PCI capable centres/nursing homes with intensive care facility and subsequent access to PCI capable centres improves STEMI outcome.14 Such a strategy may be the preferred strategy in India as PPCI is possible only in 10% of STEMI patients.14
STEMI CARE IN INDIA: BARRIERS AND PROSPECTSThere are signifi cant barriers to effective STEMI care. They are at public awareness level, patient level, hospital/physician level and at Government and societal levels. Patients often ignore symptoms, self medicate and even when they decide to seek medical attention, they consult non-physicians in India. To overcome these barriers, organized patient education and awareness programs are urgently needed. Cardiology Society of India (CSI), Association of Physicians of India (API) and the Indian Medical
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 55
Association (IMA) should join hands in these awareness programs. Such programs should not only use the traditional methods like public lectures, print materials, but should also focus on television, internet and social media. The public should be educated that for anyone beyond their teens, an ECG is a must for acute pain or discomfort from jaw to umbilicus including upper limbs. Public should be educated about the signifi cance of time, seeking immediate medical attention and timely reaching the ‘right’ hospital or physician for STEMI care.
Another most important barrier is at the level of hospital systems. For a country like India, wherein only less than 10% of STEMI patients receive PCI, primary PCI cannot and will not be the answer for every patient of STEMI. We should rely on thrombolysis, especially bolus agents like TNK, and promptly shifting the patients to a PCI capable centre. Considering the effi cacy, a strategy of prehospital thrombolysis should be ideally suited for Indian conditions. Considering the diverse Indian conditions, a combination of strategies could be more appropriate. For instance, primary PCI should be the preferred strategy in most of the hospitals, who are already offering 24 x7 emergency PCI services and the patient can reach the available STEMI Care PPCI capable centres in less than 90 min.15 A delay in access to PPCI capable centre may occur due to lack of transfer facility, densely populated cities, traffi c congestions etc. Other cities and small district towns should have certifi ed STEMI care physicians and hospitals. These hospitals should do the initial care, thrombolysis with TNK, management of complications and then should have an organized way of early transfer to nearby cities wherein early angiogram and PCI are possible. For rest of rural India, pre-hospital thrombolysis with TNK could be the ideal strategy. For this to become practical, we need to have “Integrated STEMI Care Systems”. We need to have emergency (108) ambulances, equipped with a facility to do an ECG and transmit to a central station, wherein a cardiologist can ascertain STEMI. Upon confi rmation of STEMI, the patient should receive aspirin
and statin. These ambulances should also have medical and paramedical personnel who can assess sickness, administer a questionnaire to assess the suitability for thrombolysis with TNK. The patient should be taken in the ambulance that has facility to monitor rhythm and defi brillator. Automated algorithms can decide, based on the place, distance to a STEMI hospital or a PCI capable centre, whether to shift for primary PCI or to a hospital for thrombolysis or pre-hospital thrombolysis in the ambulance itself. Accordingly, the hospital should be activated and no time should be wasted at the hospital emergency. If pre-hospital thrombolysis is decided, the patient or relative may talk to a centrally stationed cardiologist and the medical personnel get a consent and administer the agent under cardiac monitoring inside the ambulance, while the patient is being shifted to a nearby hospital.
The above ambitious plan could only work if there is governmental participation and the STEMI care is integrated to the existing emergency care systems in India. The government should make emergency STEMI treatment at subsidized cost to all Indians, may be through medical insurance schemes. The Government should identify STEMI care centres in each city, district and rural areas and certify them. The information on the list of PCI capable and other STEMI care centres should be widely and easily available. Government should also ensure the availability of thrombolytic, especially bolus agents like TNK, at subsidized cost to the poor. Recently published STREAM Trial 2014 with 1 year mortality follow up data has shown that PPCI less than 60 minutes is not practical in most of the STEMI patients, thus, TNK followed by PCI in 24 hours is strongly recommended protocol.16
Therefore, Golden time window of Door to Balloon Time of <2 hours is most powerful predictor of salvaging jeopardized myocardium in STEMI and signifi cantly reduce STEMI infl icted morbidity and mortality. If TNK is given in <60 minutes, it may reduce infarct size from larger to smaller, transmural to subendocardial or may even abort
MI, thus help improving subsequent PCI outcome by reducing thrombus burden and better TIMI fl ow. Time delay >90 minutes reduces the benefi t of PPCI. Thus the objective of Integrated TIMI Care is to minimize time from chest discomfort to ECG <30 minutes ((FMC), ECG to drug intervention <60 minutes, drug intervention to PCI <90-120 minutes and this will defi nitely have STEMI infl icted morbidity and mortality benefi t in our country and create global impact. We must act locally to impact globally.
FUTURE DIRECTIONS FOR STEMI PROGRAMME IN INDIACSI Forum: Consensus Statement: Framework for a National STEMI Program: Consensus document developed by STEMI INDIA, Cardiology Society of India and Association of Physicians of India17: Addressing some of these issues, STEMI India, a not-for-profi t organization, CSI and API have developed a protocol of “systems of care” for effi cient management of STEMI, with integrated networks of facilities. Leveraging newly-developed ambulance and emergency medical services, incorporating recent state insurance schemes for vulnerable populations to broaden access, and combining innovative, “state-of-the-art” information technology platforms with existing hospital infrastructure, are the crucial aspects of this system. A pilot program was successfully employed in the state of Tamilnadu. The purpose of this statement is to describe the framework and methods associated with this programme with an aim to improve delivery of reperfusion therapy for STEMI in India. This programme can serve as model STEMI systems of care for other low-and-middle income countries.17
REFERENCES1. Chopra KL, Chopra HK, Aggarwal KK, et al. Intravenous
streptokinase and oral nifedipine in evolving myocardial infarction--a pilot study. Indian Heart J. 1984;36(6):347–51.
2. Chopra KL, Chopra HK, Aggarwal KK, et al. IV stk in AMI. 6-36 months follow up HK Chopra, Indian Heart J. 1990;42(1):13–25.
3. Xavier D, Pais P, Devereaux PJ, et al. CREATE registry investigators. Treatment and outcomes of acute coronary syndromes in India (CREATE): A prospective analysis of registry data, Lancet. 2008;371(9622):1435–42.

56 Cardiology Today VOL. XXI NO. 2, 2017
4. Nallamothu B, Fox KA, Kennelly BM, et al. GRACE Investigators. Relationship of treatment delays and mortality in patients undergoing fibrinolysis and primary percutaneous coronary intervention.The Global Registry of Acute Coronary Events. Heart. 2007;93:1552–1555.
5. Mehta Sameer, et al. STEMI Interventions-Future Perspectives, Excerpt from: Chapter 19, Cath Lab Digest. Volume 16 - Issue 2- February, 2008.
6. Melandri G et al. Italy Review of tenecteplase (TNKase) in the treatment of acute myocardial infarction Vascular Health and Risk Management. 2009;5:249–256.
7. Hirish J, Guyatt G, Gregory W, et al. Antithrombotic and Thrombolytic Therapy*: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition), Chest. 2008;133(6_suppl):110S–112S.
8. Kalla K1, Christ G, Karnik R, et al. Vienna STEMI Registry Group.Implementation of guidelines improves the standard of care: the Viennese registry on reperfusion strategies in ST-elevation myocardial infarction (Vienna STEMI registry). Circulation. 2006;113(20):2398–405.
9. Ting HH1, Rihal CS, Gersh BJ, et al. Regional systems of
care to optimize timeliness of reperfusion therapy for ST-elevation myocardial infarction: the Mayo Clinic STEMI Protocol. Circulation. 2007;116(7):729–36.
10. Cambou JP1, Simon T, Mulak G, et al. The French registry of Acute ST elevation or non-ST-elevation Myocardial Infarction (FAST-MI): study design and baseline characteristics. Arch Mal Coeur Vaiss. 2007;100(6-7):524–34.
11. Nallamothu BK, Bates ER, Herrin J, et al. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States: National Registry of Myocardial Infarction (NRMI)-3/4 analysis. Circulation. 2005;111:761–767.
12. Gale CP, Manda SOM, Batin PD, et al. Predictors of in-hospital mortality for patients admitted with ST-elevation myocardial infarction: A real-world study using the Myocardial Infarction National Audit Project (MINAP) database. Heart. 2008;94:1407–1412.
13. Iyengar SS, Nair T, Hiremath JS, et al. Pharmacologic reperfusion therapy with indigenous tenecteplase in 15,222 patients with ST elevation myocardial infarction
- the Indian Registry. 2013;65(4):436–441.14. Dalal JJ, Alexander T, Dayasagar V, et al. 2013 Consensus
Statement for Early Reperfusion and Pharmaco-Invasive approach in patients presenting with Chest pain Diagnosed as STEMI (ST Elevation Myocardial Infarction) in an Indian Setting JAPI.2013;62.
15. Sameer M, Oliveros E, Reynbakh O, et al. Thrombolytic Therapy in STEMI Interventions, CSI Cardiology Update 2014.
16. Sinnaeve PR, Armstrong PW, Gershlick AH. For the STREAM investigators ST–Segment-Elevation Myocardial Infarction Patients Randomized to a Pharmaco-Invasive Strategy or Primary Percutaneous Coronary Intervention Strategic Reperfusion Early After Myocardial Infarction (STREAM) 1-Year Mortality Follow-Up Circulation. 2014;130:1139–1145
17. Alexandera T, Mullasari AS, Kaifoszova Z, et al. CSI Forum: Consensus Statement Framework for a National STEMI Program: Consensus document developed by STEMI INDIA, Cardiological Society of India and Association Physicians of India Indian Heart Journal. 2015;67(5):497–502.
REVIEW ARTICLE

Cardiology Today VOL.XXI NO. 2, 2017 57
Drug Therapy for Treating Chronic Heart Failure
REVIEW ARTICLE
ABHISHEKH SINGH, UPENDRA KAULKeywords � heart failure � NYHA classifi cation � effi cacy, adverse events � ACE inhibitors � hyperglycemia � beta blocker
Dr. Abhishekh Singh is Consultant, Upendra Kaul is Dean and Executive director, Fortis Escorts Heart Institute, Okhla Road, New Delhi
DEFINITIONHeart failure (HF) is a clinical syndrome characterized by symptoms (eg breathlessness, fatigue) and signs (eg edema, crepitation) resulting from structural and/or functional abnormalities of cardiac function leading to reduced cardiac output or high fi lling pressures at rest or with stress.
ETIOLOGYHF may arise as a consequence of a myocardial, valvular, pericardial, endocardial or arrhythmic problem (or some combination of these).
CLASSIFICATIONHF can be classifi ed in various ways. This can be on the basis of ejection fraction (reduced versus preserved),
clinical status (stable versus acutely decompensated) and symptom severity (New York Heart Association (NYHA) classifi cation or American College of Cardiology/American Heart Association (ACC/AHA) classifi cation.
NYHA Functional Classifi cation1Class SymptomI No limitation of physical activity.
Ordinary physical activity does not cause symptoms of HF
II Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF.
III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF.
AbstractHeart failure is a chronic disease and need life-long management. However, with treatment, signs and symptoms of heart failure can improve with amelioration of structural and functional abnormalities at times. Treatment may help you live longer and reduce mortality rate. Several classes of drugs have shown to be effective for the treatment of heart failure, each one treats a different symptoms or contributing factor.
58 Cardiology Today VOL. XXI NO. 2, 2017
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
ACCF/AHA Stages of HF2Class SymptomA At high risk for HF but without
structural heart disease or symptoms of HF
B Structural heart disease but without signs or symptoms of HF
C Structural heart disease with prior or current symptoms of HF
D Refractory HF requiring specialised interventions
PHARMACOLOGICAL THERAPIES FOR CHRONIC HEART FAILUREIn contrast to acute heart failure where the aim of treatment is to allay the symptoms and avoid short-term mortality risk due to acute hemodynamic and neurohormonal disarrangement; the therapy for chronic heart failure is directed to prevent chronic progressive myocardial damage with resultant adverse myocardial remodelling. This therapeutic approach is more directed in reducing heart failure related long-term morbidity and mortality along with symptomatic relief. For obvious reasons the therapy in acute heart failure is more via intravenous route compared to predominant oral therapy in chronic heart failure.
VARIOUS CLASSES OF DRUGS USED IN MANAGEMENT OF CHRONIC HEART FAILURE ARE1. Diuretics a) Loop diuretics b) Thiazides c) Mineralocorticoid receptor
antagonists d) Potassium sparing e) Carbonic anhydrase inhibitors f) Vasopressin antagonists2. ACE inhibitors3. ARBs 4. Beta blockers 5. Ivabradine6. Renin inhibitor7. Angiotensin receptor/ Neprilysin
inhibitors 8. Cardiac Glycosides- Digitalis,
Digoxin9. Hydralazine and Isosorbide Di-nitrate
Drugs with Proven Mortality Benefi t in Chronic Heart Failure1. ACE inhibitors and ARBs 2. Beta blockers 3. Spironolactone or eplerenone 4. Isosorbide di-nitrate, hydralazine
combination (in African-American patients)
Drugs which Improve Symptoms in Chronic Heart Failure1. Diuretics 2. Nitrates 3. Ivabradine
Drugs with no Proven Benefi t (to be used cautiously)1. Inotropes and inotropic dilators 2. Anti-arrhythmics, except beta
blockers and amiodarone 3. Calcium channel blockers 4. Digoxin
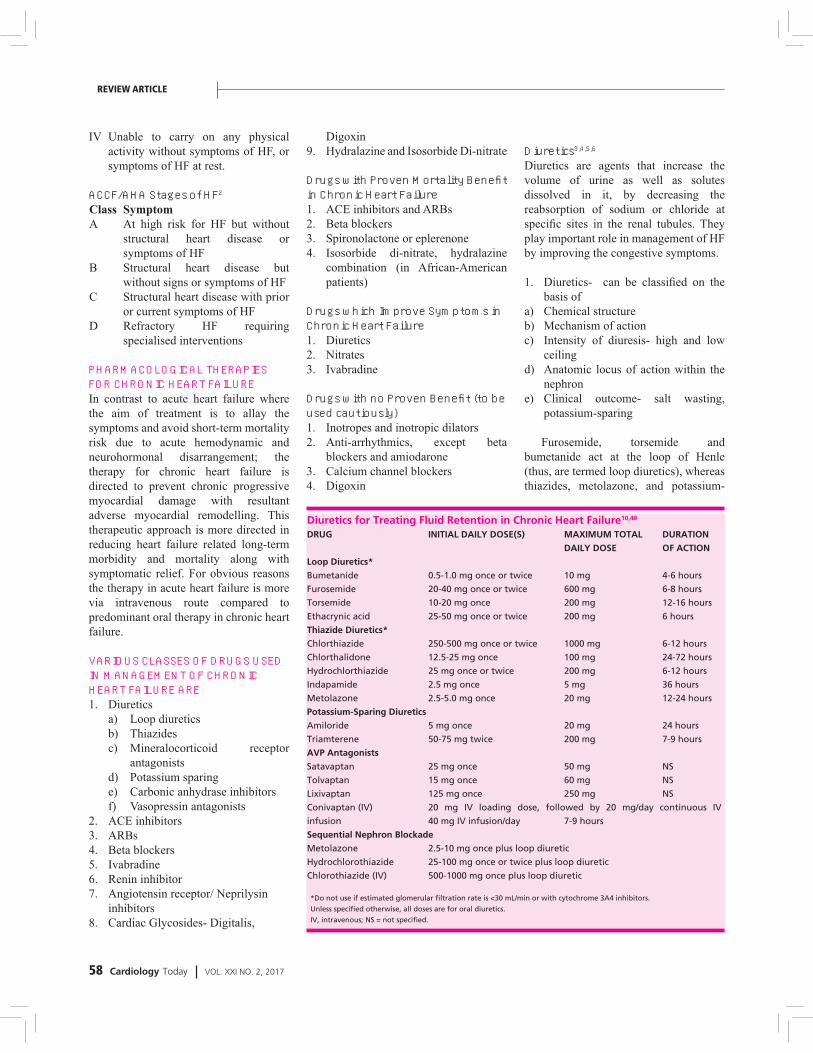
Diuretics3,4,5,6Diuretics are agents that increase the volume of urine as well as solutes dissolved in it, by decreasing the reabsorption of sodium or chloride at specifi c sites in the renal tubules. They play important role in management of HF by improving the congestive symptoms.
1. Diuretics- can be classifi ed on the basis of
a) Chemical structureb) Mechanism of actionc) Intensity of diuresis- high and low
ceilingd) Anatomic locus of action within the
nephrone) Clinical outcome- salt wasting,
potassium-sparing
Furosemide, torsemide and bumetanide act at the loop of Henle (thus, are termed loop diuretics), whereas thiazides, metolazone, and potassium-
Diuretics for Treating Fluid Retention in Chronic Heart Failure10,40
DRUG INITIAL DAILY DOSE(S) MAXIMUM TOTAL DURATION DRUG INITIAL DAILY DOSE(S) MAXIMUM TOTAL DURATION
DAILY DOSE OF ACTION DAILY DOSE OF ACTION
Loop Diuretics*Loop Diuretics*
Bumetanide 0.5-1.0 mg once or twice 10 mg 4-6 hours Bumetanide 0.5-1.0 mg once or twice 10 mg 4-6 hours
Furosemide 20-40 mg once or twice 600 mg 6-8 hours Furosemide 20-40 mg once or twice 600 mg 6-8 hours
Torsemide 10-20 mg once 200 mg 12-16 hours Torsemide 10-20 mg once 200 mg 12-16 hours
Ethacrynic acid 25-50 mg once or twice 200 mg 6 hours Ethacrynic acid 25-50 mg once or twice 200 mg 6 hours
Thiazide Diuretics*Thiazide Diuretics*
Chlorthiazide 250-500 mg once or twice 1000 mg 6-12 hours Chlorthiazide 250-500 mg once or twice 1000 mg 6-12 hours
Chlorthalidone 12.5-25 mg once 100 mg 24-72 hours Chlorthalidone 12.5-25 mg once 100 mg 24-72 hours
Hydrochlorthiazide 25 mg once or twice 200 mg 6-12 hours Hydrochlorthiazide 25 mg once or twice 200 mg 6-12 hours
Indapamide 2.5 mg once 5 mg 36 hours Indapamide 2.5 mg once 5 mg 36 hours
Metolazone 2.5-5.0 mg once 20 mg 12-24 hours Metolazone 2.5-5.0 mg once 20 mg 12-24 hours
Potassium-Sparing Diuretics Potassium-Sparing Diuretics
Amiloride 5 mg once 20 mg 24 hours Amiloride 5 mg once 20 mg 24 hours
Triamterene 50-75 mg twice 200 mg 7-9 hours Triamterene 50-75 mg twice 200 mg 7-9 hours
AVP Antagonists AVP Antagonists
Satavaptan 25 mg once 50 mg NS Satavaptan 25 mg once 50 mg NS
Tolvaptan 15 mg once 60 mg NS Tolvaptan 15 mg once 60 mg NS
Lixivaptan 125 mg once 250 mg NS Lixivaptan 125 mg once 250 mg NS
Conivaptan (IV) 20 mg IV loading dose, followed by 20 mg/day continuous IV Conivaptan (IV) 20 mg IV loading dose, followed by 20 mg/day continuous IV
infusion 40 mg IV infusion/day 7-9 hours infusion 40 mg IV infusion/day 7-9 hours
Sequential Nephron Blockade Sequential Nephron Blockade
Metolazone 2.5-10 mg once plus loop diuretic Metolazone 2.5-10 mg once plus loop diuretic
Hydrochlorothiazide 25-100 mg once or twice plus loop diuretic Hydrochlorothiazide 25-100 mg once or twice plus loop diuretic
Chlorothiazide (IV) 500-1000 mg once plus loop diuretic Chlorothiazide (IV) 500-1000 mg once plus loop diuretic
*Do not use if estimated glomerular filtration rate is <30 mL/min or with cytochrome 3A4 inhibitors. *Do not use if estimated glomerular filtration rate is <30 mL/min or with cytochrome 3A4 inhibitors.
Unless specified otherwise, all doses are for oral diuretics. Unless specified otherwise, all doses are for oral diuretics.
IV, intravenous; NS = not specified.IV, intravenous; NS = not specified.
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 59
sparing agents (e.g., spironolactone) act in the distal portion of the tubule. Because of high intensity diuresis, loop diuretics relieve signs and symptoms of congestion, like dyspnea and edema much rapidly and effectively compared to thiazides thus making it preferred diuretic agents in most patients with HF. Thiazide diuretics may be considered in hypertensive patients with HF and mild fl uid retention because they confer more persistent antihypertensive effects but less intense volume depletion.
Unlike ACE inhibitors, beta blockers, and mineralocorticoid receptor antagonists, the effects of diuretics on mortality and morbidity have not been studied in patients with HF. Thiazides may be less effective in patients with reduced kidney function but in some situations a combination with loop diuretics works by acting at multiple sites.
After initial aggressive therapy to achieve euvolaemia (restoration of dry body weight), the diuretic requires moderation to lowest possible maintenance dose to avoid the risk of dehydration leading to reduced cardiac output, hypotension and renal dysfunction, thus depriving the patient of (or achievement of the target dose of) other important therapies like ACE inhibitors, ARBs, beta blockers and mineralocorticoid receptor antagonists which have proven mortality benefi t.
LOOP DIURETICS39,40,49The loop diuretics, act by reversible inhibition of Na+-K+-2Cl− symporter present on the apical membrane of epithelial cells in the thick ascending limb of loop of Henle. Because of extensive plasma proteins binding, their delivery to the tubule by fi ltration is limited. However, they are secreted effi ciently in the proximal tubule by the organic acid transport system and thus gain access to the Na+-K+-2Cl− symporter in the luminal membrane of the ascending limb. Thus the effi cacy of loop diuretics is dependent on suffi cient renal plasma blood fl ow and proximal tubular secretion to deliver these agents to their site of action. Because of being more bioavailable, bumetanide and torsemide are more effective than furosemide, in advanced HF or right-sided HF. Ethacrynic acid exhibits a slower onset of action, with delayed and only partial reversibility, but can be safely used in sulfa-allergic patients with HF.
Adverse eff ects � Hypovolemia � Hypotension- reduced GFR,
circulatory collapse � Thromboembolic events, � Dyselectrolemia-
• Hyponatraemia• Hypokalemia• Hypocalcaemia• Hypomagnesaemia
� Hypochloremic alkalosis � Hepatic encephalopathy in patients
with liver disease � Tinnitus, vertigo, and a sense of
fullness in the ears � Ototoxicity Sensory neural deafness
(can be irreversible) � Rashes, photosensitivity, paresthesias � Bone marrow depression � GI disturbances.
THIAZIDE AND THIAZIDE-LIKE DIURETICS40,49The thiazide diuretics block the Na+-Cl− transporter in the cortical portion of the ascending limb of loop of Henle and the distal convoluted tubule. Metolazone, a thiazide-like diuretic can be used in combination with furosemide in patients to overcome diuretic resistance. Because thiazides prevent maximal dilution of urine, they decrease the free water clearance, contributing to the development of hyponatremia. Thiazides increase Ca2+ resorption in the distal nephron and may cause small increase in serum Ca2+ levels, but by decreasing Mg2+ resorption may cause hypomagnesaemia on long term use. Direct enhancement of K+ and H+ secretion from collecting duct may lead to clinically important hypokalemia.
Adverse eff ects � Hypokalemia � Hyperurecemia � Glucose intolerance � Weakness � Impotence � Skin rashes � Serious allergic reactions (e.g.
thrombocytopenia) are rare �MINERALOCORTICOID RECEPTOR ANTAGONISTS7,8,9,40,49Mineralocorticoids, such as aldosterone, cause salt and water retention and increase the excretion of K+ and H+ by binding to specifi c mineralocorticoid receptors. Spironolactone and eplerenone are a specifi c pharmacologic antagonist of aldosterone, acting primarily through competitive binding of receptors at the aldosterone-dependent sodium-potassium exchange site in the distal convoluted renal tubule. Spironolactone has
Figure 1. Site of actions of various agents in Renal Tubules
ACEIs, ARBs (RAAS inhibitors)ACEIs, ARBs (RAAS inhibitors)
ProximalProximaltubuletubule
Distal Distal convoluted convoluted tubuletubule
MRAs, BNP, NOMRAs, BNP, NO
AldosteroneAldosterone
VasoperessinVasoperessin
(V2RAs, B1RAs/V2RAs)(V2RAs, B1RAs/V2RAs)
Loop diureticsLoop diuretics
Thick ascending Thick ascending loop of Henleloop of Henle
DopamineDopamine
BNP, dopamineBNP, dopamine
AA11RARA AdenosineAdenosineThiazidesThiazides
VasopressinVasopressin
HH++
NaNa++NHE3NHE3
ATPaseATPaseNaNa++
NKCCNKCCNaNa++KK++
2Cl2Cl––
AQP2AQP2HH22OO
NaNa++
KK++
HH––
ATPaseATPase
NaNa++ClCl––
NCCTNCCT
Collecting ductCollecting duct

60 Cardiology Today VOL. XXI NO. 2, 2017
antiandrogenic and progesterone-like effects, which may cause gynecomastia or impotence in men, and menstrual irregularities in women. Eplerenone has more selectivity for the mineralocorticoid receptor than for steroid receptors, thus having fewer sex hormone side effects and shorter half-life compared to spironolactone. Despite being weak diuretics, both have shown signifi cant morbidity and mortality benefi t in clinical trials in HF patients by virtue of their ability to antagonize the deleterious effects of aldosterone in the cardiovascular system. Hence mineralocorticoid receptor antagonists are used in HF for their ability to antagonize the renin-angiotensin-aldosterone system, rather than for their diuretic properties.
Adverse eff ects � Hyperkalemia can be caused by both. � Spironolactone may cause
• Gynecomastia• Impotence• Decreased libido• Menstrual irregularities• Diarrhea, gastritis, gastric
bleeding, and peptic ulcers• CNS adverse effects include
drowsiness, lethargy, ataxia, confusion, and headache.
� Spironolactone may cause rashes and, rarely, blood dyscrasias.
� Eplerenone causes GI disorders.
POTASSIUM-SPARING DIURETICS10Triamterene and amiloride are referred to as potassium-sparing diuretics. Both drugs cause small increases in NaCl excretion and usually are employed for their antikaliuretic actions to offset the effects of other diuretics that increase K+ excretion. Both drugs are organic bases that are transported into the proximal tubule, where they block Na+ reabsorption in the late distal tubule and collecting duct. However, because Na+ retention occurs in more proximal nephron sites in HF, neither of them is effective in achieving a net negative Na+ balance when given alone in patients with HF.
Adverse eff ect � Hyperkalemia
� Megaloblastic anemia with triam-terene (a weak folic acid antagonist)
� Triamterene also causes glucose tol-erance, photosensitization, interstitial nephritis and renal stones.
CARBONIC ANHYDRASE INHIBITORS11,12,13,14Carbonic anhydrase plays a key role in NaHCO3 reabsorption and acid secretion. Carbonic anhydrase inhibitors potently inhibit both the membrane-bound and cytoplasmic forms of carbonic anhydrase, resulting in nearly complete abolition of NaHCO3 reabsorption in the proximal tubule. Despite being weak diuretics, they are used in HF patients to correct the metabolic alkalosis caused by other diuretics.
Adverse eff ects• Metabolic acidosis and severe
hypokalemia can result from repeated use
• Calculus formation and ureteral colic due to precipitation of calcium phosphate salts in an alkaline urine
• Bone marrow depression• Nephropathy• Allergic reactions• Dermatological abnormalities• Drowsiness• paresthesias.
Contraindications• Hepatic cirrhosis- Urinary
alkalinization because of diversion of ammonia of renal origin from urine into the systemic circulation, may induce or worsen hepatic encephalopathy
• Severe chronic obstructive pulmonary disease-worsened metabolic or respiratory acidosis
• Contraindicated in patients with hyperchloremic acidosis-reduced urinary excretion of weak organic bases.
VASOPRESSIN ANTAGONISTS15-24,40,49Increased circulating levels of the pituitary hormone arginine vasopressin (AVP) contribute to the increased systemic vascular resistance and positive water balance seen in patients with HF. The cellular effects of AVP are mediated
by interactions with three types of receptors: V1a, V1b, and V2. V1a-selective receptor agonists block the vasoconstricting effects of AVP in peripheral vascular smooth muscle cells, whereas V2-selective receptor antagonists inhibit recruitment of aquaporin water channels in the apical membranes of collecting duct epithelial cells, thereby reducing the ability of the collecting duct to resorb water. Combined V1a-V2 antagonists lead to a decrease in systemic vascular resistance and prevent the dilutional hyponatremia that occurs in patients with HF.
The two most studied vasopressin antagonists, Conivaptan and tolvaptan have differing affi nities for the vasopressin receptor. Conivaptan is more potent than tolvaptan as an inhibitor of the V1 receptor, but tolvaptan is more potent inhibitor of the V2 receptor than conivaptan. The relative inhibition of the two receptors (V2:V1 selectivity ratio) is much greater with tolvaptan than with conivaptan. Thus, conivaptan is a nonselective vasopressin inhibitor, whereas tolvaptan is a more selective V2 inhibitor. Both increase urine fl ow and the excretion of electrolyte-free water, without substantial changes in sodium or potassium excretion, leading to their designation as aquaretic agents. They consistently increased plasma sodium levels. Neither drug is effective in patients with advanced chronic kidney disease.
Adverse eff ects• Gastrointestinal- nausea, belching,
cramps, and an urge to defecate or constipation.
• Cardiovascular- coronary spasm, peripheral vasoconstriction and gangrene, arrhythmia and decreased cardiac output.
• Renal- Frequency of urine, polyuria, Dry mouth, increase thirst
• CNS- Excessive correction of hyponatremia increases the risk of the osmotic demyelination syndrome.
• Hepatic- elevations in hepatic enzymes. The FDA recommends limiting the use of tolvaptan to 30 days and specifi cally states that the drug should not be used in patients
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 61
with liver disease.• Others- Mild facial fl ushing and
headache, edema, rhinorrhea, nasal congestion, irritation, pruritus, and ulceration.
Summary of use of diuretics in clinical practice Most heart failure patients with signifi cantly reduced ejection fraction require log term diuretic therapy to maintain euvolaemia. Patients with volume overload are started on higher doses of loop diuretics with close monitoring of vitals (weight, BP and hydration status). Once euvolaemia is achieved the drug is reduced to a minimum possible maintenance dose. Renal function, electrolytes and acid-base balance should be monitored if higher doses or prolonged therapy with diuretics in instituted. Potassium sparing diuretic can be added to loop diuretics in cases of hypokalemia but to be used with caution if being given in patient with renal dysfunction or being used concomitantly with ACE inhibitors or ARBs due to risk of severe hyperkalemia.
General adverse eff ects of Diuretics• Electrolyte and Metabolic
Disturbances• Hypotension and Azotemia• Neurohormonal Activation
Causes of Diuretic Resistance in Heart Failure25,26• Noncompliance with medication or
salt restriction• Aggressive diuretic or vasodilator
therapy leading to excessive intravascular volume depletion and hypotension resulting in decreased renal perfusion and glomerular fi ltration rate.
• Decline in cardiac output due to worsening heart failure, arrhythmias, or other primary cardiac causes
• Selective reduction in glomerular perfusion pressure following initiation (or dose increase) of ACE inhibitor therapy
• Nonsteroidal anti-infl ammatory drugs
• Primary renal pathology
• Reduced or impaired bioavailability of diuretic due to intestinal edema and reduced splanchnic blood fl ow
ACE INHIBITORS (TABLE 1)27-35,40,49Several large randomized controlled trials have shown the benefi ts of angiotensin converting enzyme inhibitors (ACE I) in patients with HF with reduced EF (both symptomatic and asymptomatic) with or without coronary artery disease (CAD). ACE I prevent LV remodeling, reduce morbidity and mortality in heart failure patient with reduced ejection fraction and thus ACE I are ACC/ AHA class I indication in patients with HF with reduced EF and current or prior symptoms, unless contraindicated.
ACE I block the angiotensin converting enzyme (ACE) and thus prevents the conversion of angiotensin I to angiotensin II. However, ACE being a pluripotent enzyme also mediates breakdown of several vasoactive peptides (eg kininase mediated bradykinin breakdown); thus ACE inhibitors may induce the upregulation of bradykinin. Despite blocking ACE, ACE I are not able to stop generation of angiotensin II by non-ACE dependent pathways. These alternate chymase and other tissue based proteases dependent pathways are the dominant mode of angiotensin II generation in both myocardial and vascular tissue. On chronic ACE I treatment a gradual rise in angiotensin II levels result, a phenomenon known as “angiotensin escape” due to up-regulation in the activity of these alternate pathways. Also with fall of angiotensin II levels due to ACE inhibition, the negative feedback on RAAS is lost and leads to increased concentration and activity of renin and angiotensin I. This increased levels and
activity of plasma renin and angiotensin I levels act as a substrate for alternate pathway action and adds to angiotensin escape.
Because the ACE I induced fall of angiotensin II levels is transient (days to weeks), the persistent fall in BP despite angiotensin escape indicates alternate vasodepressor mechanism. ACE I induced increased bradykinin stimulates production of endothelium-derived relaxing factor and prostacyclin (PGI2) causing blood pressure reduction. These drugs also reduce the activity of sympathetic nervous system (both central and peripheral) and inhibit sympathetically mediated vasoconstriction.
ACE I improve endothelial function, viscoelastic properties of blood vessels and facilitate vascular remodeling thus explaining enhanced BP reduction over long term exceeding the initial response.
Mechanism leading to improved outcome in patients with systolic dysfunction on ACE inhibition is the induction of a more favorable hemodynamic state. ACE Inhibition commonly reduces afterload and systolic wall stress, and increase cardiac output, indices of stroke work, stroke volume and arterial compliance. Systemic blood pressure falls, initially, but later return to baseline levels. Renal blood fl ow increases due to fall of renovascular resistance, reduced stimulus to the secretion of aldosterone by angiotensin II, and the diminished direct effects of angiotensin II on the kidney. Natriuresis occurs as a result of the improved renal hemodynamics. The excess volume of body fl uids contracts, which reduces venous return to the right side of the heart. A further reduction results from venodilation and an increased capacity
Table 1. ACE InhibitorsAngiotensin-Converting INITIATING DAILY DOSE MAXIMAL DAILY DOSEAngiotensin-Converting INITIATING DAILY DOSE MAXIMAL DAILY DOSE
Enzyme InhibitorsEnzyme Inhibitors
Captopril 6.25 mg 3× 50 mg 3×Captopril 6.25 mg 3× 50 mg 3×
Enalapril 2.5 mg twice 10 mg twiceEnalapril 2.5 mg twice 10 mg twice
Lisinopril 2.5-5.0 mg once 20 mg onceLisinopril 2.5-5.0 mg once 20 mg once
Ramipril 1.25-2.5 mg once 10 mg onceRamipril 1.25-2.5 mg once 10 mg once
Fosinopril 5-10 mg once 40 mg onceFosinopril 5-10 mg once 40 mg once
Quinapril 5 mg twice 40 mg twiceQuinapril 5 mg twice 40 mg twice
Trandolapril 0.5 mg once 4 mg onceTrandolapril 0.5 mg once 4 mg once

62 Cardiology Today VOL. XXI NO. 2, 2017
of the venous bed. The response to ACE inhibitors also involves reductions of pulmonary arterial pressure, pulmonary capillary wedge pressure, and left atrial and left ventricular fi lling volumes and pressures. Consequently, preload and diastolic wall stress is diminished. The better hemodynamic performance results in increased exercise tolerance and suppression of the sympathetic nervous system. Cerebral and coronary blood fl ow usually is well maintained, even when systemic blood pressure is reduced.
The benefi cial effects of ACE inhibitors in systolic dysfunction also involve improvements in ventricular geometry. In heart failure, ACE inhibitors reduce ventricular dilation and tend to restore the heart to its normal elliptical shape. ACE inhibitors may reverse ventricular remodeling via changes in preload/afterload, by preventing the growth effects of angiotensin II on myocytes, and by attenuating cardiac fi brosis induced by angiotensin II and aldosterone.
Inhibition of ACE in patients with systolic dysfunction prevents or delays the progression of heart failure, decreases the incidence of sudden death and myocardial infarction, decreases hospitalization, and improves the quality of life. The more severe the ventricular dysfunction, the greater is the benefi t from ACE inhibition. The absolute benefi t is greatest in patients with the most severe HF. Indeed, among patients with NYHA class IV HF, the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS I) had a much larger effect size than the SOLVD treatment trial in which patients were in NYHA class II-IV.
ACE I should be started at a low dose especially if the patient is already on diuretic therapy and gradually up titrated every 3-5 days, till either symptom like dizziness indicating hypotension appear or the dose used in clinical trials is achieved. Trial recommended higher doses are more effective than lower doses in lowering morbidity and mortality. Initially the diuretic dose may require lowering to avoid fi rst dose hypotension. Also to be kept in mind is that volume overload can attenuate the effects of ACE
inhibitors, thus explaining the synergistic role of diuretics with ACE I.
Because these patients have high renin levels leading to higher concentration and activity of Angiotensin I they should be treated with beta-adrenergic blocking agents for synergistic response.
Although enalapril is the only ACE inhibitor showing mortality benefi t in controlled trials of chronic HF, multiple ACE inhibitors have proven to be more or less equally effective. ACE inhibitors markedly improved the functional status and survival in patients with signs or symptoms of HF after MI. Thus the effects of ACE inhibitors on the natural history of chronic HF seem to represent “class effects” of these agents.
Because of increased level of renin and Angiotensin I, sudden withdrawal of ACE I can be hazardous. In absence of life-threatening indications, the drug withdrawal should be gradual.
Adverse effect- Serious untoward reactions to ACE inhibitors are rare, and they generally are well tolerated. No major metabolic side effects seen on long-term treatment with ACE inhibitors. There is no change in uric acid or Ca2+; may improve insulin sensitivity in diabetic patients; improve cholesterol and lipoprotein(a) levels in proteinuric nephropathy.
Initial minor derangement in kidney function test (blood urea, BUN and serum creatinine) and fall of blood pressure does not require lowering of dose of ACE I and is generally well tolerated. If symptomatic hypotension or signifi cant renal dysfunction occurs with initiation of ACE I, patient is to be evaluated for hydration, and diuretic needs to be reduced, or withdrawn if patient is salt depleted or dehydrated. In case if this happens with euvolumia it requires dose reduction or withdrawal of ACE I.
Dry cough in (5–20% of patients)- due to increased levels of bradykinin, substance P, and/or prostaglandins. It is not dose-related, more common in women, mostly develops between 1 week and 6 months after initiation of therapy. If intolerable, it may require termination of therapy. The cough usually disappears, within 4 days of drug termination.
Hyperkalemia-Serious hyperkalemia
is rare unless the patient has baseline renal dysfunction or is concomitantly on other hyperkalemia causing drugs (eg- potassium sparing diuretics, potassium supplements, beta blockers or NSAIDs).
Acute Renal Failure- In patients with low renal perfusion pressure due to low cardiac output, renal artery stenosis or hypovolemia, ACE I can induce acute renal insuffi ciency because of fall in GFR due to efferent arteriolar dilatation. Elderly heart failure patients are more susceptible to this side effect. This is reversible with appropriate treatment however.
Teratogenicity- ACE inhibitors are contraindicated in pregnancy. Oligohydramnios, fetal calvarial hypoplasia, fetal growth retardation, pulmonary hypoplasia, fetal death, neonatal anuria, and neonatal death have been documented if a drug used in the second and third trimesters of pregnancy. Once pregnancy is diagnosed, ACE inhibitors should be discontinued as soon as possible within 1st trimester.
Dermatological issues- ACE in-hibitors can cause rash with or without itching. Incidence being higher with captopril.
Proteinuria- As such they reduce proteinuria in diabetic nephropathy but rarely ACE I can cause proteinuria.
Angioedema- It is rare side effect, caused probably due to kinin induced accumulation of bradykinin. Just like cough angioedema, is not dose dependent, and usually occurs within few hours of fi rst dose and airway obstruction and respiratory distress may lead to death. African Americans have a 4.5 times greater risk of ACE inhibitor–induced angioedema than do Caucasians.
Others- Dysgeusia (more frequent with captopril). Neutropenia, renal glycosuria (in the absence of hypergly-cemia), hepatotoxicity (cholestatic type), are rare and reversible side effects of unknown mechanism.
ANGIOTENSIN RECEPTOR BLOCKERS (TABLE 2)36-40,49Angiotensin receptor blockers (ARBs) are another class of RAAS inhibitors. ARBs block angiotensin receptor subtype
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 63
1 (site of action of angiotensin II) that virtually mediates all of the known physiological effects relevant to a angiotensin II on cardiovascular and cardiorenal hemostasis i.e.- vascular smooth muscle contraction, fast and slow pressor responses, vasopressin release, aldosterone secretion, thirst, catecholamines release, increases in sympathetic tone, and cellular hypertrophy and hyperplasia. Incidence of a cough, skin rash, and angioedema are signifi cantly less with ARBs compared to ACE I and therefore can be used in ACE-I intolerant patients with low EF. The same is not true for intolerance due to hyperkalemia or renal insuffi ciency as its incidence is same in both groups. Major differences between ARBs and ACE I are• AT1 activation is suppressed more
effectively by ARB than by ACE inhibitors because ACE inhibitors do not inhibit alternative non-ACE dependent Angiotensin II–generating pathways, whereas ARBs block the actions of Angiotensin II via the AT1 receptor regardless of how Angiotension II is formed.
• Activation of AT2 receptors is more with ARB than with ACE I as blockade of AT1, receptors by ARBs inhibits feedback suppression, thus increasing renin and in turn Angiotensin II levels leading to increased activation of AT2 receptors.
• Angiotensin levels are more with ACE I than do ARBs, since ACE is involved in the clearance of Angiotensin.
• ACE inhibitors increase the levels of several of ACE substrates, including bradykinin.
Whether these pharmacological differences between ARBs and ACE inhibitors result in signifi cant differences
in therapeutic outcomes is not clear. In patients with symptomatic HF who were intolerant of ACE inhibitors, ARBs are as effective as ACE inhibitors in reducing HF-related morbidity and mortality. As per the heart failure guidelines ACE inhibitors remain fi rst-line agents for the treatment, whereas ARBs are recommended for ACE-intolerant patients. Of the available lot three (losartan, valsartan, and candesartan) have ample data accesible in the setting of HF. Similar to ACE I, ARBs should be initiated with the lower doses, and up-titrated every 3 to 5 days. As with ACE inhibitors, blood pressure, renal function, and potassium should be reassessed within 1 to 2 weeks after initiation and after changes in dose.
Complications of Angiotensin Receptor Blocker UseAs expected most of the adverse effects of ARBs are similar to that of ACE I.• Symptomatic hypotension• Azotemia• Hyperkalemia• Teratogenicity• cough and angioedema (less
common)In patients who are intolerant of ACE inhibitors and ARBs, the combined use of hydralazine and isosorbide dinitrate may be considered for treatment.
BETA BLOCKERS (TABLE 3)39-49Heart failure is a state of sympathetic over activity. Initially this hyperactivity supports circulatory function by enhancing inotropy, lusitropy, chronotropy but sustained activation of the sympathetic system leads to myocardial injury and results in the progression of contractile dysfunction with demonstrable adverse consequences such as, maladaptive proliferative signaling in the myocardium, direct cardiomyocyte toxicity, and myocyte apoptosis. Increased sympathetic tone can potentiate the renin angiotensin system leading to increased salt and water retention, increased vascular tone and increased ventricular pre and after load. Also there is a negative impact on myocardial contractility at cellular level
causing myocyte hypertrophy and vascular remodeling. This is associated with decreased exercise tolerance, hemodynamic abnormalities and increased mortality.
Beta blockers protect the heart from deleterious effects of sustained activation of the sympathetic system by antagonizing adrenergic receptors (alpha1, beta1, and beta2). Majority of the deleterious effects of sympathetic activation are mediated by the beta1 adrenergic receptor. Beta blockers improve symptoms, ventricular function and functional capacity, reverse the process of LV remodeling, and reduce need for hospitalization and mortality. Therefore ACC/AHA recommends Beta blockers to be prescribed to all patients with stable heart failure with reduced ejection fraction (EF <40%) unless they have a contraindication to their use or are intolerant of these drugs.
Which beta blocker to choose- The situation here is different from ACE I or ARBs where the benefi t was considered to be a class effect of a drug. Of the beta blockers three have shown mortality benefi ts in patients with chronic HF: They are bisoprolol and sustained-release metoprolol succinate (both selectively block beta1 receptor), and carvedilol (non-selective alpha1, beta1, and beta2 receptor blocker). On the contrary short-acting metoprolol tartrate and Bucindolol were not so effective in HF clinical trials, also Beta-1 selective blocker nebivolol demonstrated a nonsignifi cant reduction in the primary endpoint of all-cause mortality or cardiovascular hospitalization.
One of the three trial proven beta blocker should be started as soon as heart failure with reduced ejection fraction is
Table 2. Angiotensin Receptor Blockers36-40,49
Angiotensin Initiating MaximalAngiotensin Initiating Maximalreceptor daily dose daily dosereceptor daily dose daily doseblockersblockers
Valsartan 40 mg twice 160 mg twiceValsartan 40 mg twice 160 mg twice
Candesartan 4-8 mg once 32 mg onceCandesartan 4-8 mg once 32 mg once
Losartan 12.5-25 mg once 50 mg onceLosartan 12.5-25 mg once 50 mg once
Table 3. Chronic Heart FailureBeta Blockers Initiating MaximalBeta Blockers Initiating Maximal Daily Dose Daily Dose Daily Dose Daily Dose
Carvedilol 3.125 mg twice 25 mg twiceCarvedilol 3.125 mg twice 25 mg twice
(50 mg twice (50 mg twice
in patients in patients
weighing weighing
> 85 kg) > 85 kg)
Carvedilol-CR 10 mg once 80 mg onceCarvedilol-CR 10 mg once 80 mg once
Bisoprolol 1.25 mg once 10 mg onceBisoprolol 1.25 mg once 10 mg once
MetoprololMetoprolol
Succinate CR 12.5-25 mg qd 200 mg onceSuccinate CR 12.5-25 mg qd 200 mg once

64 Cardiology Today VOL. XXI NO. 2, 2017
diagnosed even with mild or no symptoms because of its proven benefi ts on survival and disease progression.
Initiation of beta blocker should be in low doses with gradual uptitration with monitoring of vital parameters like blood pressure and pulse rate and symptoms. The dose escalation should be with a target to achieve doses used in the clinical trials. The up-titration should be careful and very gradual, at not less than 2 weeks interval to avoid volume overload because of abrupt withdrawal of adrenergic support to the heart and the circulation. The rapid institution of the usual doses of beta blockers used for other conditions like hypertension or coronary artery disease may cause decompensation in many patients who would have otherwise tolerated a slower dose titration. In case of worsening of heart failure due to fl uid retention dose of diuretics may be increased to achieve euvolumia.
Beta blockers are well tolerated if added in a patient, at discharge, hospitalized for heart failure if condition at discharge is stable and he did not require intravenous HF therapy during hospital stay.
Beta blocker therapy is well tolerated even by the patients with comorbidities such as diabetes mellitus, chronic obstructive lung disease, and peripheral vascular disease. Withdrawal of beta blocker should not be abrupt except if indicated for life-threatening condition as it can lead to sudden clinical deterioration. Although some trial data suggest that patients with NYHA Class IIIB and IV heart failure may tolerate beta blockers and benefi t from their use, this group of patients should be approached with considerable caution as the real world practice does not provide such ideal and strict monitoring and follow-up as employed in trials. With lack of data in patients with new-onset, recently decompensated heart failure, such patients should not be treated with b blockers until after they have stabilized for several days to weeks.
Adverse Eff ects of Beta Blockers• Fluid retention and worsening
HF- is added in higher doses in
decompensated heart failure patient. • Low cardiac output-leading to
fatigue and hypotension especially in volume depleted patients (patients on aggressive diuresis).
• Conduction blocks-symptomatic bradycardia (dizziness or lighthead-edness) or second- or third-degree heart block warrants reduction in dose or complete withdrawal of the beta blocker.
• Beta blockers should be avoided in patients with, sinoatrial or atrioventricular nodal dysfunction, or in combination with other drugs that inhibit AV conduction.
• Hyperglycemia- Should be used with caution in diabetic patients.
• Dyslipidemia- Beta blockers without intrinsic sympathomimetic activity increase triglycerides and lower high-density lipoprotein. Beta blockers with intrinsic sympathomimetic activity do not have this problem.
• Sudden Withdrawal of beta blockers can exacerbate the symptoms of heart failure, concomitant coronary artery disease and rebound rise of blood pressure because of up-regulation of beta receptors during blockade, leading to increased tissue sensitivity to endogenous catecholamines.
IVABRADINE (TABLE 4)39-41,49-53Ivabradine is a heart rate–lowering drug with unique mechanism of action. It selectively blocks the If (“funny”) current channel in the pacemaker cells that controls the spontaneous diastolic depolarization of the sinoatrial node. Ivabradine can block If channels are open. Ivabradine is most effective at higher heart rates because the magnitude of If inhibition is directly related to the frequency of channel opening. It's only known pharmacological effect is to slow the heart rate in patients in sinus rhythm with no known off-target myocardial, vascular, or other adverse effects (it does
not slow the ventricular rate in AF).CARVIVA-HF, a the small, unblinded
study, suggests that ivabradine alone or in combination with carvedilol is safe and effective for improving exercise capacity and quality of life in heart failure patients on optimized ACE-inhibitor therapy.
Ivabradine has shown to improve outcomes in patients of heart failure with reduced ejection fraction in the “Systolic Heart Failure Treatment with the If Inhibitor Ivabradine Trial” (SHIFT). IT showed that ivabradine (uptitrated to a maximal dosage of 7.5 mg twice daily) reduced the primary composite outcome of cardiovascular death and HF hospitalization. But this positive result was due to reduced hospitalization for worsening of heart failure ant not reduction in cardiovascular mortality.
“BEAUTIFUL trial” was done in patients with coronary heart disease and an EF below 40% which failed to meet its primary endpoint of reducing cardiovascular death, MI, or HF hospitalization, but provided the evidence of drug safety in heart failure patients.
ESC has approved use of ivabradine in the treatment of symptomatic chronic heart failure (NYHA classes II to IV) patients with systolic dysfunction (LVEF ≤35%) who are in sinus rhythm with resting heart rate ≥ 70 bpm, despite treatment with an evidence-based dose of beta blocker (or maximum tolerated dose below that, or intolerant to, or contra indication for beta blockers).
Note- Caution to be taken is to attempt to up titrate the beta blockers to maximally tolerable dose and then to add ivabradine for heart rate lowering only if target is not achieved by beta blockers, and not use ivabradine as a substitute of beta blockers that have shown signifi cant survival benefi t in several trials with mortality risk reductions of 24%-65%, which Ivabradine has failed to show in two large trials ( 10,917 patient in BEAUTIFUL trial and 6558-patient in SHIFT trial).
Side Eff ects• Bradycardia- Uncommon because
heart rate lowering with Ivabradine is rate dependent.
Table 4: IvabradineAgent Initiating MaximalAgent Initiating Maximal Daily Dose Daily Dose Daily Dose Daily Dose
Ivabradine 5 mg twice 7.5 mg Ivabradine 5 mg twice 7.5 mg
daily twice daily daily twice daily
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 65
• Photopsia- Luminous phenomenon due to blocked of If current in retina, the only other place in humans these channels are known to be present.
• Headache and dizziness• Nausea vomiting and constipation• Eosinophilia
RENIN INHIBITORS54-57Aliskiren is fi rst in class nonpeptide low molecular weight orally active, transition state, direct renin inhibitor. It is potent in vitro and highly specifi c inhibitor of human renin preventing the conversion of angiotensinogen to angiotensin I. Degree of Suppression of the RAS is similar to that as by ACE inhibitors and dose dependent. Prolonged treatment with ACE I is not able to suppress the circulating RAS and with time the angiotensin II and aldosterone tend to rise to pretreatment level. This is not so with ARBs and renin inhibitors. The implication of this can be important in because angiotensin II is considered to be responsible for tissue damage; thus renin inhibitors may provide greater effi cacy than ACE inhibition. Also ACE inhibitors and ARBs provoke a compensatory increase in renin and downstream intermediaries of the renin-angiotensin-aldosterone system which is not so with renin inhibitors.
Large trials to compare standard therapy vs aliskiren plus standard therapy in heart failure would improve clinical outcomes. The Aliskiren Trial on Acute Heart Failure Outcomes (ASTRONAUT) included patients with low ejection fraction (<40%) and elevated natriuretic peptide (BNP) or NT-proBNP who were being discharged from the hospital after treatment for acute decompensated heart failure. No signifi cant difference in the primary endpoint of cardiovascular death or HF rehospitalisation at 6 months was observed in the aliskiren treated group compared with patients treated with standard medical therapy. Moreover, the rate of adverse events was higher in aliskiren group. Further trials for the role of aliskiren in heart failure are ongoing.
Adverse eff ects• Fatigue, headache, dizziness,
diarrhea are common• Cough, angioedema are rare• Hyperkalemia• Renal dysfunction
ANGIOTENSIN RECEPTOR/NEPRILYSIN INHIBITORS58Neprilysin, a neutral endopeptidase, degrades several endogenous vasoactive peptides, including natriuretic peptides, bradykinin, and adrenomedullin. Inhibition of neprilysin increases the levels of these substances, countering the neuro-hormonal overactivation that contributes to vasoconstriction, sodium retention, and maladaptive remodeling.PARADIGM-HF was a large trial which compared LCZ696 a combination of sacubitril a neprilysin inhibitor and valsartan to enalapril in patients of heart failure with a reduced ejection fraction. The trial was terminated prematurely because of strongly signifi cant benefi t of the combination compared to enalapril for the primary end point of reducing the risks of death and of hospitalisation for heart failure with a median follows up of 27 months. Combination was also superior to enalapril in reducing the risk of death from any cause and reducing symptoms and physical limitations of heart failure. Fewer patients stopped their study medication overall or because of an adverse event in the LCZ696 group than in the enalapril group, thus discarding any safety concern of combination over enalapril.
Thus patients with heart failure with reduced ejection fraction who have ongoing symptoms of heart failure, NYHA class II-III, LVEF ≤40% despite optimal treatment should be given sacubitril/valsartan instead of their ACE inhibitor or ARB, unless contraindicated. It may be considered in patients with NYHA class IV symptoms.
Adverse eff ect• Angioedema- may be related to
it's inhibition of three enzymes responsible for the degradation of bradykinin. If the patient is already on an ACE inhibitor, the ACE inhibitor should be stopped for 36 hours before initiating sacubitril/valsartan to minimize the risk of angioedema.
• Cough
• Hyperkalemia• May rarely potentiate dementia from
accumulation of amyloid plaques in the brain
CARDIAC GLYCOSIDES (TABLE 5)39-41,49,59-65Digoxin is the only glycoside that has been evaluated in placebo-controlled trials, for the management of patients with chronic HF. Digoxin is a potent and highly selective inhibitors of Na+K+-ATPase leading to inhibition of the active transport of Na+ and K+ across cell membranes by their reversible binding to the subunit. Inhibition of the Na+K+-ATPase pump leads to an increase in intracellular calcium and hence increased cardiac contractility (positive inotropy). Also in patients with heart failure who have increased activation of the sympathetic system, digoxin increases the activity of vagal afferent nerves leading to increased vagal tone that counter balance the adrenergic toxicity. Target therapeutic serum digoxin level should be below 1.0 ng/mL, especially in renal dysfunction, elderly or low body mass patients. Higher doses are not recommended for the management of patients with HF.
Despite being one of the oldest drugs to be used for chronic HF confusion persist regarding the effectiveness. Digoxin is recommended to be reserved for patients with heart failure with atrial fi brillation, or for patients in sinus rhythm who remain symptomatic despite maximal therapy with ACE inhibitors and beta blockers. Despite not being the fi rst line drug for HF digoxin unlike most other inotropic agents does not increase mortality in CHF.
Adverse eff ects of Digoxin Use• Cardiac arrhythmias including
atrial or ventricular extrasystoles, paroxysmal atrial tachycardia with AV block, ventricular tachycardia or fi brillation, and heart block.
Table 5. Cardiac glycosidesAgent Initiating Maximal Agent Initiating Maximal
Daily Dose Daily Dose Daily Dose Daily Dose
Digoxin 0.125 mg qd Digoxin 0.125 mg qd 0.375 mg/day0.375 mg/day

66 Cardiology Today VOL. XXI NO. 2, 2017
• Neurologic complaints such as visual disturbances, xanthopsia (yellow-green halos and problems with color perception) disorientation, and confusion, drowsiness, dizziness, insomnia, nightmares, agitation, and depression.
• Rarely psychosis, delirium, amnesia, convulsions can occur.
• Rarely Gynecomastia due to the estrogen-like steroid moiety of the digoxin molecule.
• Gastrointestinal symptoms such as anorexia, nausea, and vomiting.Most side effects can be minimized
by maintaining trough levels of 0.5 to 1.0 ng/mL. Patient on digoxin therapy should be strictly monitored for serum levels of potassium and magnesium because mostly overt digitalis toxicity tends to emerge at serum levels >2.0 ng/mL but can occur at lower levels, if hypokalemia or hypomagnesemia coexist. This should be noted that digitalis produces hyperkalemia but digitalis toxicity is precipitated by hypokalemia. Special care should be taken in patient on concomitant diuretic, potassium spairing diuretics, ACE I, ARBs, renal failure patients. Patients with advanced heart block should not receive the digitalis unless a pacemaker is in place.
Stoping the drug and electrolyte correction is mostly suffi cient to manage digoxin toxicity but in severe or life-threatening digoxin toxicity antidigoxin immunotherapy using purifi ed Fab fragments may be required. Dialysis has no role in treatment of digoxin toxicity.
Hydralazine and Isosorbide Dinitrate (Table 6)39-41,49,66-70A large trial showed use of hydralazine and isosorbide dinitrate reduced mortality but not hospitalisations in patients with HF treated with digoxin and diuretics but not an ACE inhibitor or beta blocker. However, other trials that compared this
vasodilator combination with an ACE inhibitor showed ACE inhibitor to be more favorable. A meta-analysis of these vasodilator trials showed isosorbide dinitrate and hydralazine combination to be benefi cial in the African-American cohort. In a subsequent trial, in African- Americans, the addition of a fi xed-dose combination of hydralazine and isosorbide dinitrate to standard therapy with an ACE inhibitor or ARB, a beta blocker, and an aldosterone antagonist offered signifi cant benefi t.
Thus combination of hydralazine and isosorbide dinitrate is recommended for African-Americans with HFrEF who remain symptomatic despite concomitant use of ACE inhibitors, beta- blockers, and aldosterone antagonists. This combination should not be used in treatment of HFrEF patients who have not been prior challenged with standard neurohumoral antagonist therapy and should not be substituted in patients who are well tolerating ACE inhibitor or ARBs.
Despite the lack of data this treatment can be used in patients who are intolerant of ACE I or ARBs.
Adverse effects-• Hypotension• Headache, dizziness• Gastrointestinal complaints.• Peripheral neuritis• Systemic Lupus Erythematosus
Some of the side effects can be minimised by slower titration of the drugs.
REFERENCES1. The Criteria Committee of the New York Heart
Association. Nomenclature and criteria for diagnosis of diseases of the heart and great vessels. Boston (Mass): Little, Brown; 1994.
2. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr., Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on practice guidelines. Circulation 2013;128(16):e240-327.
3. Brater DC. Diuretic therapy. N Engl J Med. 1998;339:387–95.
4. Cody RJ, Kubo SH, Pickworth KK. Diuretic treatment for the sodium retention of congestive heart failure. Arch Intern Med. 1994;154:1905–14.
5. Patterson JH, Adams KF Jr, Applefeld MM, et al. Oral torsemide in patients with chronic congestive heart failure: effects on body weight, edema, and electrolyte excretion: Torsemide Investigators Group. Pharmacotherapy. 1994;14:514–21.
6. Sherman LG, Liang CS, Baumgardner S, et al. Piretanide, a potent diuretic with potassium-sparing properties, for the treatment of congestive heart failure. Clin Pharmacol Ther. 1986;40:587–94.
7. Pitt B, Zannad F, Remme WJ, et al; Randomized Aldactone Evaluation Study Investigators. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med. 1999;341:709–17.
8. Zannad F, McMurray JJ, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364:11–21.
9. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348:1309–21.
10. Hunt SA, Abraham WT, Chin MH, et al: ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 112:e154, 2005.
11. Friedberg CK, Taymor R, Minor JB, Halpern M. The use of diamox, a carbonic anhydrase inhibitor, as an oral diuretic in patients with congestive heart failure. N Engl J Med. 1953;248:883–889
12. Karmazyn M. Therapeutic potential of Na-H exchange inhibitors for the treatment of heart failure. Expert Opin Invest Drugs. 2001;10:835–843
13. Li X, Alvarez B, Casey JR, Reithmeier RAF, Fliegel L. Carbonic anhydrase II binds to and enhances activity of the Na+/H+ exchanger. J Biol Chem. 2002;277:36085–36091.
14. Pastorekova S, Parkkila AK, Pastorek J, Supuran C. Carbonic anhydrases: current state of the art, therapeutic applications and future prospects. J Enzyme Inhib Med Chem. 2004;19:199–229.
15. Schrier RW, Abraham WT. Hormones and hemodynamics in heart failure. N Engl J Med. 1999; 341: 577–585.
16. Thibonnier M. Vasopressin receptor antagonists in heart failure. Curr Opin Pharmacol. 2003; 3: 683–687.
17. Lee CR, Watkins ML, Patterson JH, Gattis W, O'connor CM, Gheorghiade M, Adams KF Jr. Vasopressin: a new target for the treatment of heart failure. Am Heart J. 2003; 146: 9–18.
18. Jackson EK. Vasopressin and other agents affecting the renal conservation of water. In: Goodman LS, Gilman A, Brunton LL, Lazo JS, Parker KL, eds. Goodman & Gilman’s the Pharmacological Basis of Therapeutics. 11th ed. New York, NY: McGraw-Hill; 2006: 2021.
19. Kalra PR, Anker SD, Coats AJ. Water and sodium regulation in chronic heart failure: the role of natriuretic peptides and vasopressin. Cardiovasc Res. 2001; 51: 495–509.
20. Tahara A, Saito M, Sugimoto T, et al. Pharmacological characterization of YM087, a potent, nonpeptide human vasopressin V1A and V2 receptor antagonist. Naunyn Schmiedebergs Arch Pharmacol 1998; 357: 63-9.
21. Yamamura Y, Nakamura S, Itoh S, et al. OPC-41061, a highly potent human vasopressin V2-receptor antagonist: pharmacological profile and aquaretic effect by single and multiple oral dosing in rats. J Pharmacol Exp Ther 1998; 287: 860-7.
22. Tomas Berl, M.D. Vasopressin Antagonists. . N Engl J Med. 2015; 372:2207-16.
Table 6. Hydralazine and Isosorbide DinitrateAgent Initiating Daily Dose Maximal Daily DoseAgent Initiating Daily Dose Maximal Daily Dose
Combination of hydralazine– 10-25 mg/10 mg 3× 75 mg/40 mg 3×Combination of hydralazine– 10-25 mg/10 mg 3× 75 mg/40 mg 3×
isosorbide dinitrateisosorbide dinitrate
Fixed dose of hydralazine– 37.5 mg/20 mg (one tablet) 3× 75 mg/40 mg (two tablets) 3×Fixed dose of hydralazine– 37.5 mg/20 mg (one tablet) 3× 75 mg/40 mg (two tablets) 3×
isosorbide dinitrateisosorbide dinitrate
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 67
23. Greenberg A, Verbalis J, Amin A, et al. Hyponatremia: current treatment practice and outcomes report of the hyponatremia registry: an observational multicenter international study. Kidney Int 2015 February11.
24. Food and Drug Administration. FDA safety communication: FDA limits duration and usage of Samsca (tolvaptan) due to possible liver injury leading to organ transplant or death, 2013 (http://www .fda .gov/ Drugs/ DrugSafety/ ucm350062 .htm).
25. Ellison DH. Diuretic resistance: physiology and therapeutics. Semin Nephrol 1999:19:581–97.
26. Loon NR, Wilcox CS, Unwin RJ. Mechanism of impaired natriuretic response to furosemide during prolonged therapy. Kidney Int 1989;36:682–9.
27. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 1991;325:293-302.
28. Pfeffer MA, Lamas GA, Vaughan DE, Parisi AF, Braunwald E. Effect of captopril on progressive ventricular dilatation after anterior myocardial infarction. N Engi J Med. 1988;319:80-86.
29. Konstam MA, Rousseau MF, Kronenberg MW, Udelson JE, Melin J, Stewart D, Dolan N, Edens TR, Ahn S, Kinan D, Howe DM, Kilcoyne L, Metherall J, Benedict C, Yusuf S, Pouleur H, the SOLVD Investigators: Effects of the angiotensin converting enzyme inhibitor, enalapril, on the long-term progression of left ventricular dysfunction in patients with heart failure. Circulation. 1992;86:431-438.
30. Francis GS, Benedict C, Johnstone DE, Kirlin PC, Nicklas J, Liang C, Kubo SH, Rudin-Toretsky E, Yusuf S, SOLVD Investigators. Comparison of neurohormonal activation in patients with left ventricular dysfunction with and without congestive heart failure: a substudy of the Studies of Left Ventricular Dysfunction (SOLVD). Circulation. 1990;82:1724-1729.
31. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian enalapril survival study (CONSENSUS). N Engl J Med 1987; 316: 1429–35.
32. Izzo JL Jr, Weir MR. Angiotensin-converting enzyme inhibitors. J Clin Hypertens (Greenwich) 2011; 13:667.
33. Taylor AA, Siragy H, Nesbitt S. Angiotensin receptor blockers: pharmacology, efficacy, and safety. J Clin Hypertens (Greenwich) 2011; 13:677.
34. ONTARGET Investigators, Yusuf S, Teo KK, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008; 358:1547.
35. Kostis JB, Shelton B, Gosselin G, et al. Adverse effects of enalapril in the Studies of Left Ventricular Dysfunction (SOLVD). SOLVD Investigators. Am Heart J 1996; 131:350.
36. Pitt B, Segal R, Martinez FA, Meurers G, Cowley AJ, Thomas I, Deedwania PC, Ney DE, Snavely DB, Chang PI, on behalf of ELITE Study Investigators. Randomized trial of losartan versus captopril in patients over 65 with heart failure (Evaluation of Losartan in the Elderly Study, ELITE). Lancet. 1997;349:747–752.
37. Dickstein K, Chang P, Willenheimer R, Haunsø S, Remes J, Hall C, Kjekshus J. Comparison of the effects of losartan and enalapril on clinical status and exercise performance in patients with moderate or severe chronic heart failure. J Am Coll Cardiol. 1995;26:438–445.
38. McKelvie RS, Yusuf S, Pericak D, Avezum A, Burns RJ, Probstfield J, Tsuyuki RT, White M, Rouleau J, Latini R, Maggioni A, Young J, Pogue J. Comparison of candesartan, enalapril, and their combination in congestive heart failure: Randomized Evaluation of Strategies for Left Ventricular Dysfunction (RESOLVD) Pilot Study. Circulation. 1999;100:1056–1064.
39. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al, for the American College of Cardiology Foundation and the American Heart Association. 2009 focused update incorporated into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the International Society for Heart and Lung Transplantation. J Am Coll Cardiol2009;53:e1-90
40. Braunwald EBonow R. Braunwald's heart disease. Philadelphia: Saunders; 2012.
41. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J2012;33:1787-847.
42. Poole-Wilson PA, Swedberg K, Cleland JG, Di Lenarda A, Hanrath P, Komajda M, et al, for the Carvedilol Or Metoprolol European Trial Investigators. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomised controlled trial. Lancet2003;362:7-13
43. Beta-Blocker Evaluation of Survival Trial Investigators. A trial of the beta-blocker bucindolol in patients with advanced chronic heart failure. N Engl J Med2001;344:1659-67
44. CIBIS Investigators and Committees. A randomized trial of beta-blockade in heart failure: the Cardiac Insufficiency Bisoprolol Study (CIBIS). Circulation1994;90:1765-73.
45. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet1999;353:9-13.
46. Willenheimer R, van Veldhuisen DJ, Silke B, Erdmann E, Follath F, Krum H, et al, for the CIBIS III Investigators. Effect on survival and hospitalization of initiating treatment for chronic heart failure with bisoprolol followed by enalapril, as compared with the opposite sequence: results of the randomized Cardiac Insufficiency Bisoprolol Study (CIBIS) III. Circulation2005;112:2426-35.
47. Hjalmarson A, Goldstein S, Fagerberg B, Goldstein S, Fagerberg B, Hjalmarson A, et al. Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure: the Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). JAMA2000;283:1295-302.
48. Fonarow GC, Abraham WT, Albert NM, Stough WG, Gheorghiade M, Greenberg BH, et al, for the OPTIMIZE-HF Investigators and Coordinators. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure: findings from the OPTIMIZE-HF program. J Am Coll Cardiol2008;52:190-9.
49. 4. Opie LGersh B. Drugs for the heart. Philadelphia, PA: Elsevier; 2013.
50. Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 2010; 376:875–85.
51. Borer JS, Böhm M, Ford I, et al. Effect of ivabradine on recurrent hospitalization for worsening heart failure in patients with chronic systolic heart failure: the SHIFT study. Eur Heart J 2012;33:2813–20.
52. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomised controlled trial. Lancet 2008;372:817-821.
53. Volterrani M., Cice G., Caminiti G., et al; Effect of carvedilol, ivabradine or their combination on exercise
capacity in patients with heart failure (the CARVIVA HF trial). Int J Cardiol. 2011;151:218-224.
54. Andersen, K., Weinberger, M., Egan, B., Constance, C., Ali, M., Jin, J. et al; Comparative efficacy and safety of aliskiren, an oral direct renin inhibitor, and ramipril in hypertension: a 6-month, randomized, double blind trial. J Hypertens 2008; 26: 589–599
55. Azizi, M., Webb, R., Nussberger, J. and Hollenberg, N. Renin inhibition with aliskiren: where are we now, and where are we going? J Hypertens 2006; 24: 243–256.
56. Blumenstein, M., Romaszko, J., Calderon, A., Andersen, K., Ibram, G., Liu, Z. et al; Antihypertensive efficacy and tolerability of aliskiren/ hydrochlorothiazide (HCT) single-pill combinations in patients who are non-responsive to HCT 25 mg alone. Curr Med Res Opin 2009; 25: 903–910.
57. Gheorghiade, M., Böhm, M., Greene, S., Fonarow, G., Lewis, E., Zannad, F. et al; Effect of aliskiren on postdischarge mortality and heart failure readmissions among patients hospitalized for heart failure: the ASTRONAUT randomized trial. JAMA 2013; 309: 1125–1135.
58. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. PARADIGM-HF; N Engl J Med. 2014;371:993–1004
59. The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J of Med. 1997;336:525–533.
60. Rathore SS, Curtis JP, Wang Y, Bristow MR, Krumholz HM. Association of serum digoxin concentration and outcomes in patients with heart failure. JAMA. 2003;289:871– 878.
61. Rathore SS, Wang Y, Krumholz HM. Sex-based differences in the effect of digoxin for the treatment of heart failure. N Engl J Med. 2002;347: 1403–1411.
62. Adams KF, Patterson JH, Gattis WA, O’Connor CM, Lee CR, Schwartz TA, Gheorghiade M. Relationship of serum digoxin concentration to mortality and morbidity in women in the Digitalis Investigation Group trial: a retrospective analysis. J Am Coll Cardiol. 2005;46:497–504.
63. Packer M, Gheorghiade M, Young JB, Costantini PJ, Adams KF, Cody RJ, Smith LK, Van Voorhees L, Gourley LA, Jolly MK. Withdrawal of digoxin from patients with chronic heart failure treated with angiotensinconverting- enzyme inhibitors. N Engl J Med. 1993;329:1–7.
64. Rahimtoola SH, Tak T. The use of digitalis in heart failure. Curr Probl Cardiol. 1996; 21: 781–756.
65. Captopril-Digoxin Multicenter Research Group. Comparative effects of therapy with captopril and digoxin in patients with mild to moderate heart failure. JAMA. 1988; 259: 539–544.
66. Davies RF, Beanlands DS, Nadeau C, et al. Enalapril versus digoxin in patients with congestive heart failure: a multicenter study. J Am Coll Cardiol. 1991; 18: 1602–1609.
67. Cohn JN. Vasodilator therapy for heart failure: the influence of impedance on left ventricular performance. Circulation. 1973;48:5–8.
68. Franciosa JA, Mikulic E, Cohn JN, Jose E, Fabie A. Hemodynamic effects of orally administered isosorbide dinitrate in patients with congestive heart failure. Circulation. 1974;50:1020–1024.
69. Cohn JN, Johnson G, Ziesche S, Cobb et al; A comparison of enalapril with hydralazine-isosorbide dinitrate in the treatment of chronic congestive heart failure. N Engl J Med. 1991;325:303–310.
70. Taylor AL, Ziesche S, Yancy C et al; Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med. 2004;351:2049

68 Cardiology Today VOL. XXI NO. 2, 2017
Managing PersistentHyperglycemia is a Challenge for Patient and Physician
REVIEW ARTICLE
MOHIT MINAL, SABOO BANSHI, SANJEEV MAHESHWARI, MOHIT VOHRAKeywords � persistent hyperglycemia � HbA1C goal � Diabetes Therapeutic Wheel
Dr. Mohit Minal is Consultant & Head, Dept. of Endocrinology, Manipal Hospital Jaipur; Dr. Saboo Banshi is Diabetologist-Endocrine–Metabolic Physician, Dr. Maheshwari Sanjeev is Professor in Medicine, J.L.N. Medical College, Ajmer; Dr. Vohra Mohit is Consultant & Head, Department of Pediatrics, Manipal Hospital, Jaipur
AbstractThe treatment of patients with type 2 diabetes mellitus includes education, with emphasis on lifestyle changes including diet, exercise, and weight reduction when appropriate. In the absence of contraindications, metformin is usually the initial pharmacologic therapy for most patients with type 2 diabetes. After a successful initial response to oral therapy, the majority of patients fail to maintain target glycated hemoglobin (A1C) levels, than the addition of a second medication is recommended to achieve a treatment goal A1C of <7 percent, though this goal is not appropriate for all patients, especially older adults and those with comorbid conditions. Also, the goal is not practical for all patients, due to patient preferences regarding combination therapy, particularly insulin therapy. This decision is typically made after two to three months of initial therapy; in patients with inadequate glycemic control on metformin and A1C >8.5 percent, adding insulin is suggested. In patients with inadequate glycemic control on metformin (A1C >7.0 percent), with A1C close to target (≤8.5 percent), adding a short acting sulfonylurea, such as glipizide is suggested. The addition of repaglinide is an alternative option, which can be considered in individuals who do not reach glycemic goals with metformin, if there are contraindications to sulfonylureas or patient preference limits the use of insulin. Glucagon like peptide 1 (GLP 1) receptor agonists may be appropriate to use in certain clinical setting, e.g., when weight loss or avoidance of hypoglycemia is a primary consideration and the A1C level is close to target. The addition of pioglitazone (where available) is also an option in individuals without risk factors for heart failure (HF) or fracture, who do not reach glycemic goals with metformin alone, if there are contraindications to sulfonylureas or patient preference limits the use of sulfonylureas or insulin. In individuals with contraindications

Cardiology Today VOL. XXI NO. 2, 2017 69
BACKGROUNDBoth the prevalence and incidence of type 2 diabetes are increasing worldwide, particularly in developing countries, in conjunction with increased obesity rates and westernisation of lifestyle. The attendant economic burden is skyrocketing, owing to the costs associated with treatment and diabetes complications. Type 2 diabetes remains a leading cause of cardiovascular disorders, blindness, end-stage renal failure, amputations, and hospitalisations. It is also associated with increased risk of cancer, serious psychiatric illness, cognitive decline, chronic liver disease, accelerated arthritis, and other disabling or deadly conditions. Effective management strategies are of obvious importance.
RELATIONSHIP OF GLYCEMIC CONTROL TO OUTCOMES It is well established that the risk of microvascular and macrovascular complications is related to glycemia, as measured by HbA1c; this remains a major focus of therapy.1 Type 2 diabetes is a disease that is heterogeneous in both pathogenesis and in clinical manifestation. Antihyperglycemic agents are directed at one or more of the pathophysiological
defects of type 2 diabetes, or modify physiological processes relating to appetite or to nutrient absorption or excretion. So it seems, in the present era, diabetes management should be a cakewalk. Advances in pathophysiology have provided a rational basis for choosing appropriate therapy. Developments in pharmacology have created a wide spectrum of drugs, drug combinations, delivery devices, and formulations to choose from. Improvements in diagnostics have allowed better screening and monitoring of diabetes, as well as early detection of complications and comorbidities. Enhanced understanding of the psychosocial determinants of diabetes has facilitated the support that people
with diabetes require for adequate control. A large number of persons having diabetes, however, still do not achieve optimal control. Many hypothesis try explain this state of affairs. Glycemic management in type 2 diabetes mellitus has become increasingly complex and to some extent, controversial, with a widening array of pharmacological agents now available,2-6 mounting concerns about their potential adverse effects and new uncertainty regarding the benefi ts of intensive glycemic control on macrovascular complications.7-10 Many clinicians are therefore perplexed as to the optimal strategies for their patients. Poor healthcare-seeking behavior and lack of adherence on part of the patient, clinical inertia, and inappropriate choice
to metformin, sulfonylureas are often fi rst line therapy. In patients with inadequate glycemic control on sulfonylureas, with A1C >8.5 percent, we suggest switching to insulin. In patients who are intolerant or cannot take metformin for any reason and who have an A1C that is <8.5 percent but not at target on sulfonylurea alone, there are a number of agents that are available and can be used with a sulfonylurea. The choice of therapy should be individualized based upon patient characteristics, preferences, and costs. Options include thiazolidinedione, dipeptidyl peptidase 4 (DPP 4) inhibitors, GLP 1 agonists, sodium glucose co transporter 2 (SGLT2) inhibitors, alpha -glucosidase inhibitors and insulin. All of these medications have advantages and disadvantages. In individuals with inadequate glycemic control (A1C >7 percent) on two oral agents (usually metformin and sulfonylurea), we suggest switching to insulin (discontinue sulfonylurea and continue metformin). Another option is two oral agents and a GLP 1 receptor agonist. It is reasonable to try a GLP 1 agonist before starting insulin in patients who are close to glycemic goals, who prefer not to start insulin, and in whom weight loss or avoidance of hypoglycemia is a primary consideration. An alternative that is less likely to work and is more expensive is three oral agents. However, three oral agents (e.g., metformin, sulfonylurea, pioglitazone) can be considered in patients with A1C values that are not too far from goal (A1C ≤8.5 percent). A DPP 4 inhibitor or SGLT2 inhibitor may have a role as a third agent in those who cannot or will not take insulin when full doses of metformin and a sulfonylurea have not produced satisfactory metabolic control. However, long-term safety has not been established.
Table 1: Markers of a Refractory PatientHistory History
Early onset of diabetes Early onset of diabetes
Long duration of diabetes Long duration of diabetes
Complications Complications
Microvascular complications at presentation to specialist care Microvascular complications at presentation to specialist care
Drug therapy Drug therapy
Insulin use Insulin use
Complexity of therapy Complexity of therapy
Number of therapeutic agents Number of therapeutic agents
Examination Examination
Higher body mass index (in insulin treated patients) Higher body mass index (in insulin treated patients)
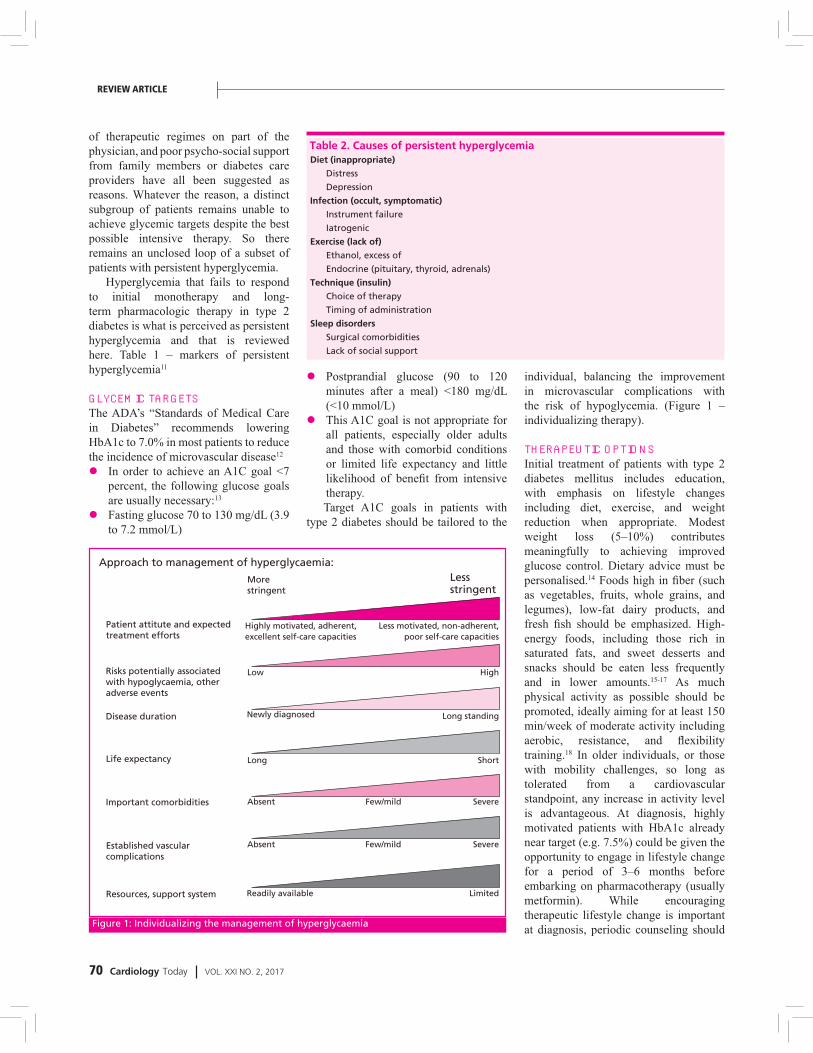
70 Cardiology Today VOL. XXI NO. 2, 2017
of therapeutic regimes on part of the physician, and poor psycho-social support from family members or diabetes care providers have all been suggested as reasons. Whatever the reason, a distinct subgroup of patients remains unable to achieve glycemic targets despite the best possible intensive therapy. So there remains an unclosed loop of a subset of patients with persistent hyperglycemia.
Hyperglycemia that fails to respond to initial monotherapy and long-term pharmacologic therapy in type 2 diabetes is what is perceived as persistent hyperglycemia and that is reviewed here. Table 1 – markers of persistent hyperglycemia11
GLYCEMIC TARGETSThe ADA’s “Standards of Medical Care in Diabetes” recommends lowering HbA1c to 7.0% in most patients to reduce the incidence of microvascular disease12
� In order to achieve an A1C goal <7 percent, the following glucose goals are usually necessary:13
� Fasting glucose 70 to 130 mg/dL (3.9 to 7.2 mmol/L)
� Postprandial glucose (90 to 120 minutes after a meal) <180 mg/dL (<10 mmol/L)
� This A1C goal is not appropriate for all patients, especially older adults and those with comorbid conditions or limited life expectancy and little likelihood of benefi t from intensive therapy.Target A1C goals in patients with
type 2 diabetes should be tailored to the
Table 2. Causes of persistent hyperglycemiaDiet (inappropriate)Diet (inappropriate)
Distress Distress
Depression Depression
Infection (occult, symptomatic)Infection (occult, symptomatic)
Instrument failure Instrument failure
Iatrogenic Iatrogenic
Exercise (lack of)Exercise (lack of)
Ethanol, excess of Ethanol, excess of
Endocrine (pituitary, thyroid, adrenals) Endocrine (pituitary, thyroid, adrenals)
Technique (insulin)Technique (insulin)
Choice of therapy Choice of therapy
Timing of administration Timing of administration
Sleep disordersSleep disorders
Surgical comorbidities Surgical comorbidities
Lack of social support Lack of social support
individual, balancing the improvement in microvascular complications with the risk of hypoglycemia. (Figure 1 – individualizing therapy).
THERAPEUTIC OPTIONSInitial treatment of patients with type 2 diabetes mellitus includes education, with emphasis on lifestyle changes including diet, exercise, and weight reduction when appropriate. Modest weight loss (5–10%) contributes meaningfully to achieving improved glucose control. Dietary advice must be personalised.14 Foods high in fi ber (such as vegetables, fruits, whole grains, and legumes), low-fat dairy products, and fresh fi sh should be emphasized. High-energy foods, including those rich in saturated fats, and sweet desserts and snacks should be eaten less frequently and in lower amounts.15-17 As much physical activity as possible should be promoted, ideally aiming for at least 150 min/week of moderate activity including aerobic, resistance, and fl exibility training.18 In older individuals, or those with mobility challenges, so long as tolerated from a cardiovascular standpoint, any increase in activity level is advantageous. At diagnosis, highly motivated patients with HbA1c already near target (e.g. 7.5%) could be given the opportunity to engage in lifestyle change for a period of 3–6 months before embarking on pharmacotherapy (usually metformin). While encouraging therapeutic lifestyle change is important at diagnosis, periodic counseling should
Approach to management of hyperglycaemia:Approach to management of hyperglycaemia:
More More stringentstringent
Patient attitute and expected Patient attitute and expected treatment effortstreatment efforts
Risks potentially associatedRisks potentially associatedwith hypoglycaemia, otherwith hypoglycaemia, otheradverse eventsadverse events
Disease durationDisease duration
Life expectancyLife expectancy
Important comorbiditiesImportant comorbidities
Established vascular Established vascular complicationscomplications
Resources, support systemResources, support system Readily availableReadily available LimitedLimited
ShortShort
SevereSevere
SevereSevere
Long standingLong standing
HighHigh
Few/mildFew/mild
Few/mildFew/mildAbsentAbsent
AbsentAbsent
LongLong
Newly diagnosedNewly diagnosed
LowLow
Highly motivated, adherent, Highly motivated, adherent, excellent self-care capacitiesexcellent self-care capacities
Less motivated, non-adherent, Less motivated, non-adherent, poor self-care capacitiespoor self-care capacities
Less Less stringentstringent
Figure 1: Individualizing the management of hyperglycaemia
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 71
also be integrated into the treatment program. Those with moderate hyperglycemia or in whom lifestyle changes are anticipated to be unsuccessful should be promptly started on an antihyperglycemic agent (usually metformin) at diagnosis.
MONOTHERAPYMetformin a biguanide, remains the most widely used fi rst-line type 2 diabetes drug; its mechanism of action predominately involves reducing hepatic glucose production.19,20 It is generally considered weight-neutral with chronic use and does not increase the risk of hypoglycemia. Metformin is associated with initial gastrointestinal side effects, and caution is advised to avoid its use in patients at risk of lactic acidosis (e.g., in advanced renal insuffi ciency, alcoholism), a rare complication of therapy. There may be some cardiovascular benefi ts from this drug, but the clinical trial data are not robust.
Insulin may be indicated for initial treatment for some.21 Although several studies have noted remissions of type 2 diabetes mellitus that may last several years, most patients require continuous treatment to maintain normal or near normal glycaemia.
Sulfonylurea, the oldest oral agent class, is an insulin secretagogue. Through the closure of ATP-sensitive potassium channels on b-cells, these drugs stimulate insulin release.22 While effective in controlling glucose levels, their use is associated with modest weight gain and risk of hypoglycemia. Additionally, studies have demonstrated a secondary failure rate that may exceed other drugs, ascribed to an exacerbation of islet dysfunction.23 Shorter-acting secretagogues, the meglitinides (or glinides), stimulate insulin release through similar mechanisms but may be associated with less hypoglycemia.24 They require more frequent dosing.
Regardless of the initial response to therapy, the natural history of most patients with type 2 diabetes is for blood glucose concentrations to rise gradually with time.Indications For A Second Agent
American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) consensus guideline for pharmacotherapy to control hyperglycemia in type 2 diabetes, recommends testing glycated hemoglobin (A1C) levels every three months and the addition of a second medication when the treatment goal of A1C <7 percent with metformin plus lifestyle intervention is not achieved within three months (algorithm 1).21
After a successful initial response to monotherapy, patients fail to maintain target A1C levels (<7 percent) at a rate of 5 to 10 percent per year (fi gure 2).25-
27 An analysis from the United Kingdom Prospective Diabetes Study (UKPDS) found that 50 percent of relatively new-onset patients identifi ed clinically and initially controlled with a single drug required the addition of a second drug after three years; by nine years, 75 percent of patients needed multiple therapies to achieve the target A1C value.28
Among the factors that can contribute to worsening glycemic control are: (Table 2: Causes of persistent hyperglycemia “DIETS”).11
� Decreased compliance with diet,
exercise, or the medical regimen, or weight gain.
� Intercurrent illness or the ingestion of drugs that can increase insulin resistance, interfere with insulin release, or increase hepatic glucose production.29 The latter factor (ingestion of certain drugs) is particularly important in older patients who are taking multiple drugs.
� Progression of the underlying disease process, including worsening insulin resistance and insulin secretion.
� The patient may have type 1 diabetes with gradual destruction of the pancreatic beta cells, sometimes referred to as "latent autoimmune diabetes in adults" (LADA).
� The physician may not have made appropriate changes in therapy often enough or at all ("therapeutic inertia").30-33 A population-based study of over 7200 patients with type 2 diabetes demonstrated that many patients remain with A1C levels higher than ideal for years because changes in therapy to improve glycemic control was not made or were only made slowly.30 Adherence
Figure 2: Glycemic control, estimated from the median hemoglobin A1C value, in patients with type 2 diabetes mellitus in the United Kingdom Prospective Diabetes Study (UKPDS) who were randomly assigned to receive intensive therapy with a sulfonyurea or insulin or to conventional treatment with diet; drugs were added if there were hyperglycemic symtoms or if the fasting blood glucose concentration was greater than 270 mg/dL (15 mmol/L). The A1C values were lower in the intensive therapy group but rose in both groups over time. The circles represent date for all patients, while the lines represent data for patients followed for 10 years. A1C : HbA1C, glycated hemoglobin
1010
99
88
77
66
000 2 4 6 8 100 2 4 6 8 10
ConventionalConventional
IntensiveIntensive
Years of randomizationYears of randomizationUKPDS 33, Lancet, 1998;352:837-853UKPDS 33, Lancet, 1998;352:837-853
%%
UKPDS HbA1C, values over 10 years

72 Cardiology Today VOL. XXI NO. 2, 2017
to algorithms that dictate changes in treatment at designated intervals and computerized decision aids may improve A1C more effi ciently than standard care.32-34
TREATMENT OPTIONS The therapeutic options for patients who fail initial therapy with lifestyle intervention and monotherapy are to add a second oral or injectable agent, including insulin, or to switch to insulin.21,36
Metformin monotherapy failures— for patients who fail initial therapy with metformin, there are a number of agents that are available and can be used with metformin (Table 3).21,36 We favor insulin or sulfonylureas as the preferred second-line agents because of effi cacy, side-effect profi le, long-term safety, and relative cost (algorithm 1).
Insulin is the preferred second-line medication for patients with A1C>8.5 percent or with symptoms of hyperglycemia despite initial therapy with metformin and lifestyle intervention. For those close to A1C target, we prefer to add a shorter-duration sulfonylurea (such as glipizide, to reduce the risk of
hypoglycemia compared with longer-acting sulfonylureas) rather than insulin. Another reasonable alternative is the addition of repaglinide, if there are contraindications to sulfonylureas or patient preference limits the use of insulin. Repaglinide is principally metabolized by the liver, with less than 10 percent renally excreted. Thus, it can be used safely in patients with chronic kidney disease.
GLP-1 receptor agonists may be appropriate to use when weight loss or avoidance of hypoglycemia is a primary consideration, the A1C level is close to target, and cost is not a major barrier. A prior history of myocardial infarction or stroke might also favor choosing liraglutide as the second drug to be added to metformin, based on the results of the liraglutide and cardiovascular outcomes study.
Empaglifl ozin may also be considered in patients with established cardiovascular disease (CVD). Although both liraglutide and empaglifl ozin appear to decrease cardiovascular morbidity and mortality in patients with type 2 diabetes and established CVD, the balance between benefi ts and risks have not been examined
in the long term. In addition, there are few data on benefi ts and risks in patients who have not had a major CVD event.
DPP-4 inhibitors can be considered as add-on drug therapy for patients who are inadequately controlled on metformin. However, the modest glucose-lowering effectiveness, expense, and limited long-term clinical experience may temper enthusiasm for these drugs.
Thiazolidinediones are not considered fi rst-choice agents, due to the risk of congestive heart failure (HF), fractures, and expense. However, in certain clinical settings, such as especially high risk for hypoglycemia or intolerance of or contraindications to sulfonylureas, a thiazolidinedione may be added. As an example, in a patient who would be at particularly high risk if hypoglycemia occurred (e.g., a construction worker) and who has inadequate glycemic control on metformin (A1C >7 but <8.5 percent), pioglitazone (where available) could be used. The use of rosiglitazone is not recommended, because of the greater concern about its atherogenic lipid profi les and a potential increased risk for cardiovascular events.21
Combination tablets of metformin and other oral agents are available in several doses. For patients who are doing well on these particular doses, the combination tablets offer the convenience of taking fewer pills. However, if the patient needs the dose of either drug to be changed independent of the other drug, then a fi xed combination is unhelpful. In addition, the cost of the brand name combinations is substantially greater than taking the generic components individually.
In meta-analyses of placebo-controlled trials evaluating different drugs (sulfonylureas, thiazolidinediones, meglitinides, alpha-glucosidase inhibitors, glucagon-like peptide-1 [GLP-1] agonists, dipeptidyl peptidase-4 [DPP-4] inhibitors) as add-on therapy to metformin, reductions in glycated hemoglobin (A1C) with different classes of drugs ranged from 0.42 to 1.0 percentage points.37,38 In one analysis, the reduction in A1C with sulfonylureas compared with placebo was greater than that of thiazolidinediones compared Algorithm 1: l
Algorithm for the metabolic management of type 2 diabetes; reinforce lifestyle interventions at every visit and check A1C every three Algorithm for the metabolic management of type 2 diabetes; reinforce lifestyle interventions at every visit and check A1C every three months until A1C is <7% and then at least every six months. The interventions should be changed if A1C is >7%.months until A1C is <7% and then at least every six months. The interventions should be changed if A1C is >7%.$CHF: congestive heart failure; A1C: glycated hemoglobin; GLP-1: glucagon-like peptide-1; DPP-4: dipeptidyl peptidase 4; SGLT2: $CHF: congestive heart failure; A1C: glycated hemoglobin; GLP-1: glucagon-like peptide-1; DPP-4: dipeptidyl peptidase 4; SGLT2: sodium-glucose co-transproter 2.sodium-glucose co-transproter 2.*Sulfonylureas other than glybenclamide (glyburide) or chlorpropamide.*Sulfonylureas other than glybenclamide (glyburide) or chlorpropamide.Alternative agents include: GLP-1 agonists, DPP-4 inhibitors, alpha-glycoidase inhibitors, SGLT2 inhibitors.Alternative agents include: GLP-1 agonists, DPP-4 inhibitors, alpha-glycoidase inhibitors, SGLT2 inhibitors.
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 73
with placebo.37 However, these trials did not directly compare different agents in combination with metformin. As expected, the use of thiazolidinediones, sulfonylureas, and meglitinides was associated with weight gain, while GLP-1 agonists, alpha-glucosidase inhibitors, and DPP-4 inhibitors were associated with weight loss or no change.38 Sulfonylureas and glinides were associated with higher rates of hypoglycemia than placebo.
Insulin was not included in the meta-analysis,38 although it is clearly the most effective and one of the least expensive of the antidiabetic medications available. As an example, in a 24-week trial of insulin glargine versus sitagliptin in 515 patients with type 2 diabetes inadequately
controlled with metformin monotherapy, there was a greater reduction in A1C in patients randomly assigned to glargine (-1.72 versus -1.13 percent).39
Sulfonylurea monotherapy failure — In individuals with contraindications to metformin, sulfonylureas are often fi rst-line therapy. In patients who have an A1C that is <8.5 percent but not at target on sulfonylurea alone, there are a number of agents that are available and can be used with a sulfonylurea. The choice of therapy should be individualized based upon patient characteristics, preferences, and costs. Options include thiazolidinediones, DPP-4 inhibitors, GLP-1 agonists, sodium-glucose co-transporter 2 (SGLT2) inhibitors, alpha- glucosidase inhibitors,
and insulin. All of these medications have advantages and disadvantages (table 3). Hypoglycemia remains a risk when any of these medications are used in combination with a sulfonylurea. In patients with inadequate glycemic control on sulfonylureas and with A1C >8.5 percent, we suggest switching to insulin. . In general, sulfonylureas are tapered and stopped if insulin is added and especially if the insulin regimen includes pre-prandial rapid-acting insulin.
The glycemic effi cacy of sulfonylureas in combination with other oral agents is illustrated by the fi ndings of a meta-analysis of trials in which sulfonylureas were added to oral agents (predominantly metformin or thiazolidinedione).40-43 Compared with placebo, the addition of sulfonylureas to oral diabetes treatment lowered A1C by 1.62 percentage points. Thus, the modest glucose-lowering effectiveness, expense, and limited long-term clinical experience with these drugs temper our enthusiasm.
Dual agent failure — if target A1C is not achieved with metformin combined with sulfonylurea or basal insulin, we suggest starting or intensifying insulin therapy. In patients on sulfonylureas and metformin who are starting insulin therapy, sulfonylureas are generally tapered and discontinued, while metformin is continued. Part of the rationale for combination metformin and insulin therapy is that by suppressing hepatic glucose production, the patient can retain the convenience of oral agents while minimizing total insulin requirements and therefore the degree of hyperinsulinemia.44
Another option is two oral agents and a GLP-1 receptor agonist. It is reasonable to try a GLP-1 agonist before starting insulin in patients who are close to glycemic goals, who prefer not to start insulin, and in whom weight loss or avoidance of hypoglycemia is a primary consideration. In randomized trials comparing GLP-1 agonists with insulin in patients with type 2 diabetes inadequately controlled with metformin and sulfonylurea, there were similar reductions in A1C in the two groups.
Another option is to try a third oral
Table 3. Summary of glucose-lowering interventionsIntervention Expected decrease Advantages Disadvantages Intervention Expected decrease Advantages Disadvantages in A1C with mono- in A1C with mono- therapy percent therapy percentTier 1: Well-validated coreTier 1: Well-validated core
Step 1: Initial therapyStep 1: Initial therapy
Lifestyle to 1.0 to 2.0 Broad benefits Insufficient for most within Lifestyle to 1.0 to 2.0 Broad benefits Insufficient for most within decrease weight first year decrease weight first year and increase and increase activity activity Metformin 1.0 to 2.0 Weight neutral GI side effects, contraindicated Metformin 1.0 to 2.0 Weight neutral GI side effects, contraindicated with renal insufficiency with renal insufficiencyStep 2: Additional therapyStep 2: Additional therapy Insulin 1.5 to 3.5 No dose limit, One to four injections daily, Insulin 1.5 to 3.5 No dose limit, One to four injections daily, rapidly eccective, monitoring, weight gain, rapidly eccective, monitoring, weight gain, improved lipid hypoglacemia, analogues are improved lipid hypoglacemia, analogues are profile expensive profile expensive Sulfonylurea 1.0 to 2.0 Rapidly effective Weight gain, hypoglycemia Sulfonylurea 1.0 to 2.0 Rapidly effective Weight gain, hypoglycemia (especially with glibenclamide (especially with glibenclamide or chlorpropamide) or chlorpropamide)Tier 2: Less well validatedTier 2: Less well validated Thiazolidinedione 0.5 to 1.4 Improved lipid profile Fluid retention, HF, weight gain, Thiazolidinedione 0.5 to 1.4 Improved lipid profile Fluid retention, HF, weight gain, (pioglitazone), bone fractures, expensive, (pioglitazone), bone fractures, expensive, potential decrease potentional increase potential decrease potentional increase in MI (pioglitazone) in MI (rosiglitazone) in MI (pioglitazone) in MI (rosiglitazone) GLP-1 agonist 0.4 to 1.0 Weight loss Requires injecting, frequent GI GLP-1 agonist 0.4 to 1.0 Weight loss Requires injecting, frequent GI side effects, long-term safety not side effects, long-term safety not established, expensive established, expensiveOther therapyOther therapy Alpha- 0.5 to 0.8 Weight neutral Frequent GI side effects, three Alpha- 0.5 to 0.8 Weight neutral Frequent GI side effects, three glucosidase times/day dosing, expensive glucosidase times/day dosing, expensive inhibitor inhibitor Glinide 0.5 to 1.5* Rapidly effective Weight gain, three times/day Glinide 0.5 to 1.5* Rapidly effective Weight gain, three times/day dosing, hypoglycemia, expensive dosing, hypoglycemia, expensive Pramlintide 0.5 to 1.0 Weight loss Three injectinos daily, frequent GI Pramlintide 0.5 to 1.0 Weight loss Three injectinos daily, frequent GI side effects, long-term safety not side effects, long-term safety not established, expensive established, expensive DPP-4 inhibitor 0.5 to 0.8 Weight neutral Long-term safety not established, DPP-4 inhibitor 0.5 to 0.8 Weight neutral Long-term safety not established, expensive, possible increased risk expensive, possible increased risk of HF with saxagliptin of HF with saxagliptin SGLT2 inhibitor 0.5 to 0.7 Weight loss, Vulvovaginal candidasis, urinary SGLT2 inhibitor 0.5 to 0.7 Weight loss, Vulvovaginal candidasis, urinary reduction in tract infections, long-term safety reduction in tract infections, long-term safety systolic blood not established systolic blood not established pressure pressure
A1C: Glycated hemoglobin; DPP-4: Dipeptidyl peptidase 4; GLP-1: glycagon-like peptide-1; A1C: Glycated hemoglobin; DPP-4: Dipeptidyl peptidase 4; GLP-1: glycagon-like peptide-1; GI: Gastrointestinal; HF: Heart failure; MI: Myocardial infarction; SGLT2: Sodium-glucose cotransporter 2.GI: Gastrointestinal; HF: Heart failure; MI: Myocardial infarction; SGLT2: Sodium-glucose cotransporter 2.*Repaglinide more effective in lowering A1C than nateglinide.*Repaglinide more effective in lowering A1C than nateglinide.

74 Cardiology Today VOL. XXI NO. 2, 2017
agent (eg, pioglitazone, DPP-4 inhibitor) before starting insulin in patients who are close to glycemic goals and who prefer not to start insulin.45,46 This was illustrated in a study of 217 patients inadequately controlled on dual therapy with sulfonylureas and metformin, who were randomly assigned to receive either insulin glargine or rosiglitazone.45 At study end (24 weeks), improvements in A1C (approximately 1.5 percentage points) were similar in both groups.
However, insulin glargine was superior in reducing A1C values when baseline A1C values were >9.5 percent. Although insulin glargine was associated with more hypoglycemic events, there were fewer overall adverse events, signifi cant improvements in the serum lipid profi le, and it was less expensive. Subjects treated with insulin glargine also reported greater improvements in several health-related quality-of-life measurements.47 These fi ndings, combined with the greater
concern about adverse cardiovascular events with thiazolidinediones, particularly rosiglitazone, favor the addition of insulin glargine over rosiglitazone.
For patients who are not well controlled on two oral agents, switching to insulin is usually less expensive than adding a third oral or injectable agent. This was demonstrated in a study of 188 type 2 diabetic patients with inadequate glycemic control on two oral agents who were randomly assigned to receive a third oral agent or be switched to twice-daily insulin along with metformin.48 Patients on three oral agents (a sulfonylurea, metformin, and a thiazolidinedione) had similar glycemic control but more side effects, a more atherogenic profi le, and substantially higher costs than patients on twice- daily insulin along with metformin.
Insulin initiation and intensifi cation— The American Diabetes Association/European Association for the Study of Diabetes (ADA/EASD) have developed a fl ow diagram for initiating and titrating insulin in the management of type 2 diabetes (algorithm 2).21 The dose of insulin may be adjusted every three to four days until glycemic targets are achieved.
Diet and exercise patterns should be reviewed in patients whose glycemic control is poor despite insulin therapy. Insulin doses should then be adjusted to achieve target glycemic control. This will usually entail additional injections, often including short or rapid-acting insulin based on postprandial glucose readings (algorithm 2). Daily insulin doses typically exceed 65 to 100 units per day, and may sometimes be much higher, for obese type 2 diabetic patients to achieve near- normal glycemia. Patients should measure blood glucose two to four times daily and should only reduce their insulin dose if hypoglycemia develops.
Use of an intensive insulin regimen (similar to that used in type 1 diabetes) results in higher serum insulin concentrations and better glycemic control than that achieved with either an oral drug or conventional insulin therapy (basal insulin only) alone.26 This regimen may require large doses of insulin to
Figure 3: In this study, 96 patients who were inadequately controlled with a sulfonylurea drug alone were randomly assigned to receive bedtime intermediate-acting insulin (BI) plus either glyburide, metformin, glyburide plus metformin, or a second injection of intermediate-acting insulin in the morning. After 12 months, the group receiving bedtime insulin plus metformin alone had significantly less weight gain (upper panel) and lower HbA1c values (lower panel) than the other three treatment groups.
REVIEW ARTICLE
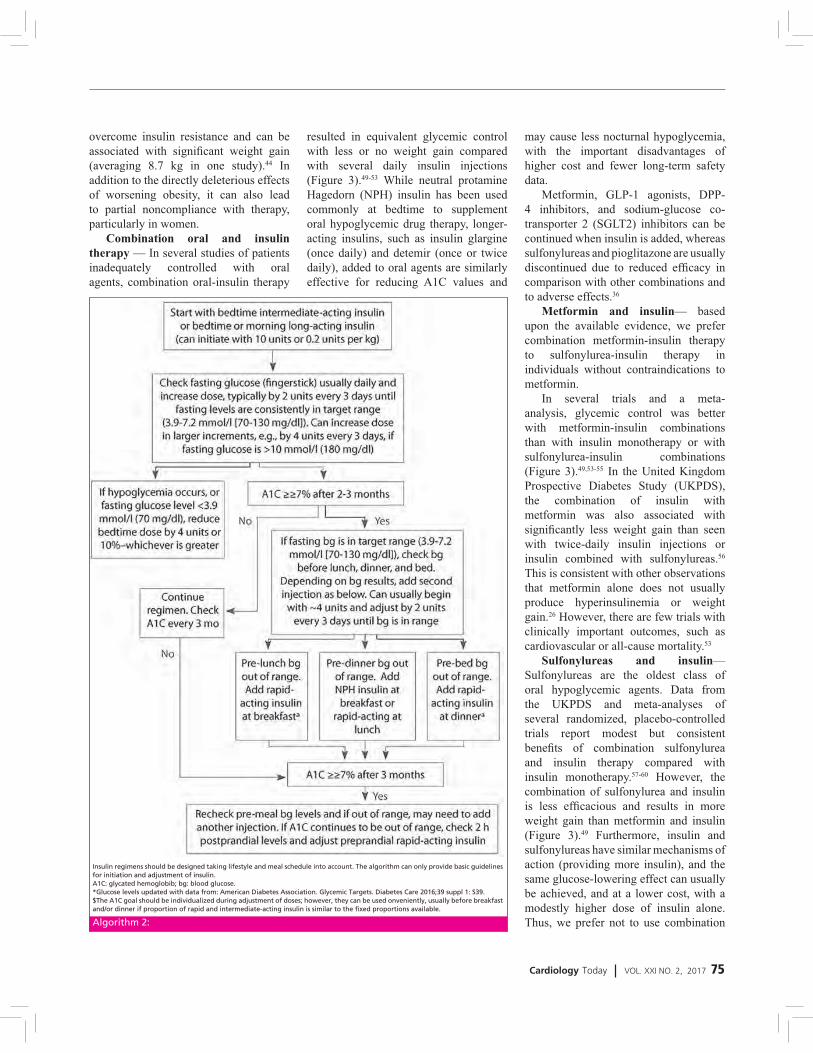
Cardiology Today VOL. XXI NO. 2, 2017 75
overcome insulin resistance and can be associated with signifi cant weight gain (averaging 8.7 kg in one study).44 In addition to the directly deleterious effects of worsening obesity, it can also lead to partial noncompliance with therapy, particularly in women.
Combination oral and insulin therapy — In several studies of patients inadequately controlled with oral agents, combination oral-insulin therapy
resulted in equivalent glycemic control with less or no weight gain compared with several daily insulin injections (Figure 3).49-53 While neutral protamine Hagedorn (NPH) insulin has been used commonly at bedtime to supplement oral hypoglycemic drug therapy, longer-acting insulins, such as insulin glargine (once daily) and detemir (once or twice daily), added to oral agents are similarly effective for reducing A1C values and
may cause less nocturnal hypoglycemia, with the important disadvantages of higher cost and fewer long-term safety data.
Metformin, GLP-1 agonists, DPP-4 inhibitors, and sodium-glucose co-transporter 2 (SGLT2) inhibitors can be continued when insulin is added, whereas sulfonylureas and pioglitazone are usually discontinued due to reduced effi cacy in comparison with other combinations and to adverse effects.36
Metformin and insulin— based upon the available evidence, we prefer combination metformin-insulin therapy to sulfonylurea-insulin therapy in individuals without contraindications to metformin.
In several trials and a meta-analysis, glycemic control was better with metformin-insulin combinations than with insulin monotherapy or with sulfonylurea-insulin combinations (Figure 3).49,53-55 In the United Kingdom Prospective Diabetes Study (UKPDS), the combination of insulin with metformin was also associated with signifi cantly less weight gain than seen with twice-daily insulin injections or insulin combined with sulfonylureas.56 This is consistent with other observations that metformin alone does not usually produce hyperinsulinemia or weight gain.26 However, there are few trials with clinically important outcomes, such as cardiovascular or all-cause mortality.53
Sulfonylureas and insulin— Sulfonylureas are the oldest class of oral hypoglycemic agents. Data from the UKPDS and meta-analyses of several randomized, placebo-controlled trials report modest but consistent benefi ts of combination sulfonylurea and insulin therapy compared with insulin monotherapy.57-60 However, the combination of sulfonylurea and insulin is less effi cacious and results in more weight gain than metformin and insulin (Figure 3).49 Furthermore, insulin and sulfonylureas have similar mechanisms of action (providing more insulin), and the same glucose-lowering effect can usually be achieved, and at a lower cost, with a modestly higher dose of insulin alone. Thus, we prefer not to use combination Algorithm 2:
Insulin regimens should be designed taking lifestyle and meal schedule into account. The algorithm can only provide basic guidelines Insulin regimens should be designed taking lifestyle and meal schedule into account. The algorithm can only provide basic guidelines for initiation and adjustment of insulin.for initiation and adjustment of insulin.A1C: glycated hemoglobib; bg: blood glucose.A1C: glycated hemoglobib; bg: blood glucose.*Glucose levels updated with data from: American Diabetes Association. Glycemic Targets. Diabetes Care 2016;39 suppl 1: S39.*Glucose levels updated with data from: American Diabetes Association. Glycemic Targets. Diabetes Care 2016;39 suppl 1: S39.$The A1C goal should be individualized during adjustment of doses; however, they can be used onveniently, usually before breakfast $The A1C goal should be individualized during adjustment of doses; however, they can be used onveniently, usually before breakfast and/or dinner if proportion of rapid and intermediate-acting insulin is similar to the fixed proportions available.and/or dinner if proportion of rapid and intermediate-acting insulin is similar to the fixed proportions available.

76 Cardiology Today VOL. XXI NO. 2, 2017
sulfonylurea and insulin therapy.Thiazolidinediones and insulin—
The addition of a thiazolidinedione to insulin improves glycemic control compared with insulin monotherapy.61 However, the combination of insulin plus either rosiglitazone or pioglitazone causes an increased incidence of heart failure (HF) and should be avoided in patients with HF.62 In addition, both available thiazolidinediones have been associated with bone loss, and rosiglitazone may be associated with other cardiovascular risks, as described above. Thiazolidinediones are also more expensive than metformin.
GLP-1-based therapy and insulin— Short-term studies using glucagon-like peptide-1 (GLP-1) agonists or DPP-4 inhibitors (vildagliptin, alogliptin) in combination with basal insulin (glargine, detemir) have demonstrated safety and effi cacy.
Cardiovascular And Other Outcomes— the long-term benefi ts and risks of using one combination over another are unknown. There is a paucity of high-quality, head-to-head drug comparison trials and trials with important clinical endpoints, such as effects on microvascular and macrovascular complications and mortality.63 Many of the recently approved diabetes drugs are now being required by the US Food and Drug Administration (FDA) to prove cardiovascular disease (CVD) safety with large trials.
On the basis of these trials and other data, there does not appear to be an increased risk of adverse cardiovascular outcomes with metformin, insulin glargine, or short-term use of dipeptidyl peptidase-4 (DPP-4) inhibitors, used in combination with another oral agent. However, DPP-4 inhibitors may be associated with an increased risk of hospitalisation for heart failure (HF).
Thiazolidinediones are associated with an increased risk of fl uid retention and HF, and the use of rosiglitazone in particular is not recommended, because of the greater concern about its atherogenic lipid profi les and a potential increased risk for cardiovascular events.
OTHER MEDICATIONS
Alpha-glucosidase inhibitors — Acarbose and miglitol can reduce glycated haemoglobin (A1C) values slightly (0.5 to 1.0 percentage points) when taken in conjunction with any another form of therapy.64,65 They act predominantly by lowering glucose concentrations after meals but may be poorly tolerated because of fl atulence and other gastrointestinal (GI) side effects. They are not preferred second-line medications, because of lower effi cacy, poorer tolerance, and increased cost compared with the alternatives above.21,36
Pramlintide — Amylin (also known as islet amyloid polypeptide) is a peptide hormone secreted by pancreatic beta cells in conjunction with insulin in response to nutrient stimuli. Pramlintide is a synthetic analog of human amylin that slows gastric emptying, reduces postprandial rises in blood glucose concentrations, and modestly improves A1C concentrations in patients with type 1 and type 2 diabetes when injected subcutaneously three times per day. Pramlintide is only approved for use in patients also taking insulin. It may be considered for patients with type 2 diabetes inadequately controlled on insulin that are overweight or experience weight gain refractory to lifestyle measures.
Colesevelam— given the modest glucose-lowering effectiveness, expense, and limited clinical experience, we typically do not recommend colesevelam to improve glycemic control in patients with type 2 diabetes. Colesevelam is a bile acid sequestrant that lowers low-density lipoprotein (LDL) cholesterol in patients with primary hypercholesterolemia. Colesevelam's mechanism of action to improve glycemic control is uncertain.66 One possibility is that bile acid sequestrants act in the GI tract to reduce glucose absorption. Side effects can include constipation, nausea, and dyspepsia. In contrast to its effects on LDL cholesterol, colesevelam increases triglyceride concentrations by approximately 20 percent.68,69 The clinical implications of this increase are unknown.
Bromocriptine — Given its modest glucose-lowering effect, very frequent GI
side effects, and the availability of more effective drugs, we do not recommend bromocriptine for the treatment of type 2 diabetes. Bromocriptine is an ergot-derived dopamine agonist that has been used for over two decades for the treatment of hyperprolactinemia and Parkinson disease. A quick release formulation of bromocriptine was approved by the FDA for the treatment of type 2 diabetes mellitus.70 In short-term clinical trials in patients with type 2 diabetes mellitus, bromocriptine (up to 4.8 mg daily) as monotherapy or as adjunctive therapy to sulfonylureas was minimally effective in reducing A1C compared with placebo (mean difference 0.4 to 0.5 percentage points).70,71 Common side effects include nausea, vomiting, dizziness, and headache.72 The mechanism of action in reducing blood sugar is unknown.
Surgical Treatment Of Obesity — Surgical treatment of obese patients with diabetes results in the largest degree of sustained weight loss (20 to 30 percent after one to two years) and, in parallel, the largest improvements in blood glucose control. There are a growing number of unblinded trials comparing bariatric surgery with medical therapy for the treatment of type 2 diabetes.73-80 Remission of diabetes is generally defi ned as a glycated haemoglobin (A1C) level less than 6.5 percent without the use of diabetes medications. Despite these impressive short-term metabolic results, concerns remain about acute postoperative complications including the need for reoperations and rehospitalisations and rare, but potentially severe, adverse events; the long-term success rates in maintaining weight loss;81,83 and the reproducibility of the results in patients with an extensive history of diabetes or with a different surgical team.84 Some weight regain is typical within two to three years of bariatric procedures, and different bariatric procedures result in different levels of weight loss and corresponding reductions in glycemia. Long-term follow-up of clinically relevant endpoints, such as effects on microvascular and macrovascular complications and mortality, are required before laparoscopic banding or other
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 77
bariatric surgery procedures can be routinely recommended for the treatment of persistent hyperglycemia, resistant to multiple medications, in obesity-related type 2 diabetes.
OTHER CONSIDERATIONS Age
Older adults (65–70 years) often have a higher atherosclerotic disease burden, reduced renal function, and more comorbidities.85,86 Many are at risk for adverse events from poly pharmacy and may be both socially and economically disadvantaged. Life expectancy is reduced, especially in the presence of long-term complications. They are also more likely to be compromised by hypoglycemia; for example, unsteadiness may result in falls and fractures87 and a tenuous cardiac status may deteriorate into catastrophic events. It follows that glycemic targets for elderly with long-standing or more complicated disease should be less ambitious than for the younger, healthier individuals.88 If lower targets cannot be achieved with simple interventions, an HbA1c of 7.5–8.0% may be acceptable, transitioning upward as age increases and capacity for self-care, cognitive, psychological and economic status, and support systems decline. While lifestyle modifi cation can be successfully implemented across all age groups, in the aged, the choice of anti-hyperglycemic agent should focus on drug safety, especially protecting against hypoglycemia, heart failure, renal dysfunction, bone fractures, and drug–drug interactions. In contrast, healthier patients with long life expectancy accrue risk for vascular complications over time. Therefore, lower glycemic targets (e.g., an HbA1c, 6.5–7.0%) and tighter control of body weight, blood pressure, and circulating lipids should be achieved to prevent or delay such complications. This usually requires combination therapy, the early institution of which may have the best chance of modifying the disease process and preserving quality-of-life.
WeightThe majority of individuals with type 2 diabetes are overweight or obese
(~80%).89 In these, intensive lifestyles intervention can improve fi tness, glycemic control, and cardiovascular risk factors for relatively small changes in body weight.90 Although insulin resistance is the predominate driver of diabetes in obese patients, they actually have a similar degree of islet dysfunction to leaner patients.91 Perhaps as a result, the obese may be more likely to require combination drug therapy.88,92 While common practice has favoured metformin in obese patients, because of weight loss/weight neutrality, this drug is as effi cacious in lean individuals.93 TZDs, on the other hand, appear to be more effective in those with higher BMIs, although their associated weight gain makes them, paradoxically, a less attractive option here. GLP-1 receptor agonists are associated with weight reduction,94 which in some patients may be substantial. Bariatric surgery is an increasingly popular option in severe obesity. Type 2 diabetes frequently resolves rapidly after these procedures. The majority of patients are able to stop some, or even all, of their anti-hyperglycemic medications, although the durability of this effect is not known.95 In lean patients, consideration should be given to the possibility of latent autoimmune diabetes in adults (LADA), a slowly progressive form of type 1 diabetes. These individuals, while presenting with mild hyperglycemia, often responsive to oral agents, eventually develop more severe hyperglycemia and require intensive insulin regimens.96 Measuring titres of islet-associated autoantibodies (e.g., anti-GAD) may aid their identifi cation, encouraging a more rapid transition to insulin therapy.
Sex/racial/ethnic/genetic diff erences Certain racial/ethnic features increase the risk of diabetes [greater insulin resistance in Latinos,97 more b-cell dysfunction in East Asians.]98 Several forms of MODY, diabetes monogenic variants often confused with type 2 diabetes, respond preferentially to sulfonylureas.100 While there are no prominent sex differences in the response to various anti-hyperglycemic drugs, certain side effects
(e.g., bone loss with TZDs) may be of greater concern in women.
ComorbiditiesCoronary Artery DiseaseType 2 diabetic patients develop atherosclerosis at increased frequency and are thus at high risk for coronary artery disease (CAD), optimal management strategies for them are therefore important. Since hypoglycemia may exacerbate myocardial ischemia and may cause dysrhythmias,101 medications that predispose patients to this adverse effect should be avoided, if possible. Because of possible effects on potassium channels in the heart, certain sulfonylureas have been proposed to aggravate myocardial ischemia through effects on ischemic preconditioning.102 Metformin may have some cardiovascular benefi ts and would appear to be a useful drug in the setting of CAD, barring prevalent contraindications.103 In a single study, pioglitazone was shown to reduce modestly major adverse cardiovascular events in patients with established macrovascular disease. It may therefore also be considered, unless heart failure is present.104 In very preliminary reports, therapy with GLP-1 receptor agonists and DPP-4 inhibitors has been associated with improvement in either cardiovascular risk or risk factors, but there are no long-term data regarding clinical outcomes.105 There are very limited data suggesting that AGIs106 and bromocriptine107 may reduce cardiovascular events.
Heart FailureIncreasing life expectancy and decrease in mortality after myocardial infarction, the diabetic population with progressive heart failure is increasing.108 This population presents unique challenges given their poly pharmacy, frequent hospitalisations, and contraindications to various agents. TZDs should be avoided.109,110 Metformin, previously contraindicated in heart failure, can now be used if the ventricular dysfunction is not severe, if patient’s cardiovascular status is stable, and if renal function is normal.111 As mentioned, cardiovascular effects of incretin-based therapies,

78 Cardiology Today VOL. XXI NO. 2, 2017
including those on ventricular function, are currently under investigation.112
Chronic Kidney DiseaseKidney disease is highly prevalent in type 2 diabetes, and moderate to severe renal functional impairment (eGFR, 60 mL/min) occurs in approximately 20–30% of patients.113,114 The individual with progressive renal dysfunction is at increased risk for hypoglycemia, which is multifactorial. Insulin and, to some degree, the incretin hormones are eliminated more slowly, as are anti-hyperglycemic drugs with renal excretion. Thus, dose reduction may be necessary, contraindications need to be observed, and consequences (hypoglycemia, fl uid retention, etc.) require careful evaluation. Current U.S. prescribing guidelines warn against the use of metformin in patients with a serum creatinine >133 mol/L (>1.5 mg/dL) in men or 124 mol/L (>1.4 mg/dL) in women. Metformin is eliminated renally, and cases of lactic acidosis have been described in patients with renal failure.115 There is an ongoing debate, however, as to whether these thresholds are too restrictive and that those with mild–moderate renal impairment would gain more benefi t than harm from using metformin.116,117 In the U.K., the National Institute for Health and Clinical Excellence (NICE) guidelines are less proscriptive and more evidence based than those in the U.S., generally allowing use down to a GFR of 30 mL/min, with dose reduction advised at 45 mL/min.118
Most insulin secretagogues undergo signifi cant renal clearance (exceptions include repaglinide and nateglinide) and the risk of hypoglycemia is therefore higher in patients with chronic kidney disease (CKD). For most of these agents, extreme caution is imperative at more severe degrees of renal dysfunction. Glyburide (known as glibenclamide in Europe), which has a prolonged duration of action and active metabolites, should be specifi cally avoided in this group. Pioglitazone is not eliminated renally, and therefore there are no restrictions for use in CKD. Fluid retention may be a concern, however. Among the DPP-4 inhibitors, sitagliptin, vildagliptin, and saxagliptin
share prominent renal elimination. In the face of advanced CKD, dose reduction is necessary. One exception is linagliptin, which is predominantly eliminated enterohepatically. For the GLP-1 receptor agonists exenatide is contraindicated in stage 4–5 CKD (GFR, 30 mL/min) as it is renally eliminated; the safety of liraglutide is not established in CKD though pharmacokinetic studies suggest that drug levels are unaffected as it does not require renal function for clearance. More severe renal functional impairment is associated with the slower elimination of all insulins. Thus doses need to be titrated carefully, with some awareness for the potential for more prolonged activity profi les.
Liver DysfunctionIndividuals with type 2 diabetes frequently have hepatosteatosis as well as other types of liver disease.119 There is preliminary evidence that patients with fatty liver may benefi t from treatment with pioglitazone.120-122 It should not be used in an individual with active liver disease or an alanine transaminase level above 2.5 times the upper limit of normal. In those with steatosis but milder liver test abnormalities, this insulin sensitizer may be advantageous. Sulfonylureas
can rarely cause abnormalities in liver tests but are not specifi cally contraindicated; meglitinides can also be used. If hepatic disease is severe, and secretagogues should be avoided because of the increased risk of hypoglycemia. In patients with mild hepatic disease, incretin-based drugs can be prescribed, except if there is a coexisting history of pancreatitis. Insulin has no restrictions for use in patients with liver impairment and is indeed the preferred choice in those with advanced disease.
HypoglycemiaHypoglycemia in type 2 diabetes was long thought to be a trivial issue, as it occurs less commonly than in type 1 diabetes. In the ACCORD trial, the frequency of both minor and major hypoglycemia was high in intensively managed patients - threefold than that associated with conventional therapy.123 Hypoglycemia is more dangerous in the elderly and occurs consistently more often as glycemic targets are lowered. Hypoglycemia may lead to dysrhythmias, but can also lead to accidents and falls (which are more likely to be dangerous in the elderly),124 dizziness (leading to falls), confusion (so other therapies may not be taken or taken incorrectly), or infection
Figure 4. Research Society for the Study of Diabetes in India (RSSDI) Diabetes Therapeutic Wheel
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 79
(such as aspiration during sleep, leading to pneumonia). Hypoglycemia may be systematically under-reported as a cause of death, so the true incidence may not be fully appreciated. Perhaps just as importantly, additional consequences of frequent hypoglycemia include work disability and erosion of the confi dence of the patient (and that of family or caregivers) to live independently. Accordingly, in at-risk individuals, drug selection should favour agents that do not precipitate such events and, in general, blood glucose targets may need to be moderated.
RSSDI 2015 Recommendations‒ ABCD (EFGH) Approach for Diabetes Management
� Choice of any anti-diabetic agent should take into account the patient’s general health status and associated medical disorders
� This patient centric approach may be referred to as the ABCD (EFGH) approach for diabetes management
� For any T2DM patient fi rst line of therapy should be Metformin unless not tolerated or contraindicated (Figure 4)
KEY POINTS � Glycemic targets and glucose-
lowering therapies must be individualised.
� Diet, exercise, and education remain the foundation of any type 2 diabetes treatment program.
� Unless there are prevalent contraindications, metformin is the optimal fi rst-line drug.
� After metformin, there are limited data to guide us. Combination therapy with additional 1–2 oral or injectable agents is reasonable, aiming to minimize side effects where possible.
� Ultimately, many patients will require insulin therapy alone or in combination with other agents to maintain glucose control.
� All treatment decisions, where possible, should be made in conjunction with the patient, focusing on his/her preferences, needs, and values.
� Comprehensive cardiovascular risk reduction must be a major focus of therapy.
REFERENCES1. Stratton IM, Adler AI, Neil HA, et al. Association of
glycaemia with macro- vascular and microvascular complica- tions of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405–412.
2. Bolen S, Feldman L, Vassy J, et al. Sys- tematic review: comparative effective- ness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med 2007;147:386–399
3. Bergenstal RM, Bailey CJ, Kendall DM. Type 2 diabetes: assessing the relative risks and benefits of glucose-lowering medications. Am J Med 2010;123:374. e9–374.e18.
4. Nyenwe EA, Jerkins TW, Umpierrez GE, Kitabchi AE. Management of type 2 di- abetes: evolving strategies for the treat- ment of patients with type 2 diabetes. Metabolism 2011;60:1–23.
5. Nolan JJ. Consensus guidelines, algo- rithms and care of the individual patient with type 2 diabetes. Diabetologia 2010; 53:1247–1249.
6. Blonde L. Current antihyperglycemic treatment guidelines and algorithms for patients with type 2 diabetes mellitus. Am J Med 2010;123(Suppl.):S12–S18.
7. Greenfield S, Billimek J, Pellegrini F, et al. Comorbidity affects the relationship between glycemic control and cardiovas- cular outcomes in diabetes: a cohort study. Ann Intern Med 2009;151:854–860.
8. Matthews DR, Tsapas A. Four decades of uncertainty: landmark trials in glycaemic control and cardiovascular outcome in type 2 diabetes. Diab Vasc Dis Res 2008; 5:216–218 in Canada. Canadian Journal of Diabetes 2008;32:S1–S201.
9. NICE. Type 2 Diabetes: The Management of Type 2 Diabetes: NICE Clinical Guide- line 87. National Institute for Health and Clinical Excellence, 2009.
10. Skyler JS, Bergenstal R, Bonow RO, et al.; American Diabetes Association; American College of Cardiology Foundation; American Heart Association. Intensive glycemic control and the prevention of cardiovascular events: implications of 1050 the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart Association. Diabetes Care 2009; 32:187–192.
11. Yudkin JS, Richter B, Gale EA. Intensified glucose control in type 2 diabetesdwhose agenda? Lancet 2011;377:1220–1222.
12. American Diabetes Association. Stand- ards of medical care in diabetesd2011. Diabetes Care 2011;34(Suppl. 1):S11–S61.
13. Wei N, Zheng H, Nathan DM. Empirically establishing blood glucose targets to achieve HbA1c goals. Diabetes Care 2014;37:1048.
14. Bantle JP, Wylie-Rosett J, Albright AL, et al.; American Diabetes Association. Nutrition recommendations and in- terventions for diabetes: a position statement of the American Diabetes As- sociation. Diabetes Care 2008;31(Suppl. 1):S61–S78.
15. Elmer PJ, Obarzanek E, Vollmer WM, et al.; PREMIER Collaborative Research Group. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control: 18-month results of a randomized trial. Ann Intern Med 2006;144:485–495
16. Gordon NF, Salmon RD, Franklin BA, et al. Effectiveness of therapeutic lifestyle changes in patients with hypertension, hyperlipidemia, and/or hyperglycemia. Am J Cardiol 2004;94:1558–1561.
17. Wing RR, Tate DF, Gorin AA, Raynor HA, Fava JL. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–1571.
18. Boulé NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of exercise on gly- cemic control and body mass in type 2 diabetes mellitus: a meta-analysis of con- trolled clinical trials. JAMA 2001;286: 1218–1227.
19. Bailey CJ, Turner RC. Metformin. N Engl J Med 1996;334:574–579.
20. Lamanna C, Monami M, Marchionni N, Mannucci E. Effect of metformin on cardiovascular events and mortality: a meta- analysis of randomized clinical trials. Diabetes Obes Metab 2011;13:221–22.
21. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009;32:193.
22. Bryan J, Crane A, Vila-Carriles WH, Babenko AP, Aguilar-Bryan L. Insulin secretagogues, sulfonylurea receptors and K(ATP) channels. Curr Pharm Des 2005; 11:2699–2716.
23. Kahn SE, Haffner SM, Heise MA, et al.; ADOPT Study Group. Glycemic dura- bility of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med 2006;355:2427–2443.
24. Gerich J, Raskin P, Jean-Louis L, Purkayastha D, Baron MA. PRESERVE-b: two-year efficacy and safety of initial combination therapy with nateglinide or glyburide plus metformin. Diabetes Care 2005;28:2093–209.
25. Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy. Update regarding the thiazolidinediones. Diabetologia 2008;51:8.
26. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837.
27. United Kingdom Prospective Diabetes Study (UKPDS). 13: Relative efficacy of randomly allocated diet, sulphonylurea, insulin, or metformin in patients with newly diagnosed non-insulin dependent diabetes followed for three years. BMJ 1995;310:83.
28. U.K. prospective diabetes study 16. Overview of 6 years' therapy of type II diabetes: a progressive disease. U.K. Prospective Diabetes Study Group. Diabetes 1995;44:1249.
29. Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA 1999;281:2005.
30. Bressler P, DeFronzo RA. Drugs and diabetes. Diabetes Reviews 1994;2:53.
31. Brown JB, Nichols GA, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care 2004;27:1535.
32. Shah BR, Hux JE, Laupacis A, et al. Clinical inertia in response to inadequate glycemic control: do specialists differ from primary care physicians? Diabetes Care 2005;28:600.
33. Ziemer DC, Doyle JP, Barnes CS, et al. An intervention to overcome clinical inertia and improve diabetes mellitus control in a primary care setting: Improving Primary Care of African Americans with Diabetes (IPCAAD) 8. Arch Intern Med 2006;166:507.
34. 34. Grant RW, Buse JB, Meigs JB, University HealthSystem Consortium (UHC) Diabetes Benchmarking Project Team. Quality of diabetes care in U.S. academic medical centers: low rates of medical regimen change. Diabetes Care 2005;28:337.

80 Cardiology Today VOL. XXI NO. 2, 2017
35. Fanning EL, Selwyn BJ, Larme AC, DeFronzo RA. Improving efficacy of diabetes management using treatment algorithms in a mainly Hispanic population. Diabetes Care 2004;27:1638.
36. Grant RW, Cagliero E, Sullivan CM, et al. A controlled trial of population management: diabetes mellitus: putting evidence into practice (DM-PEP). Diabetes Care 2004;27:2299.
37. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient- centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015;38:140.
38. Monami M, Lamanna C, Marchionni N, Mannucci E. Comparison of different drugs as add-on treatments to metformin in type 2 diabetes: a meta-analysis. Diabetes Res Clin Pract 2008;79:196.
39. Phung OJ, Scholle JM, Talwar M, Coleman CI. Effect of noninsulin antidiabetic drugs added to metformin therapy on glycemic control, weight gain, and hypoglycemia in type 2 diabetes. JAMA 2010;303:1410.
40. Aschner P, Chan J, Owens DR, et al. Insulin glargine versus sitagliptin in insulin-naive patients with type 2 diabetes mellitus uncontrolled on metformin (EASIE): a multicentre, randomised open-label trial. Lancet 2012;379:2262.
41. Kipnes MS, Krosnick A, Rendell MS, et al. Pioglitazone hydrochloride in combination with sulfonylurea therapy improves glycemic control in patients with type 2 diabetes mellitus: a randomized, placebo-controlled study. Am J Med 2001;111:10.
42. Charbonnel B, Schernthaner G, Brunetti P, et al. Long-term efficacy and tolerability of add-on pioglitazone therapy to failing monotherapy compared with addition of gliclazide or metformin in patients with type 2 diabetes. Diabetologia 2005;48:1093.
43. Zhang F, Xiang H, Fan Y, et al. The effects of sulfonylureas plus metformin on lipids, blood pressure, and adverse events in type 2 diabetes: a meta-analysis of randomized controlled trials. Endocrine 2013;44:648.
44. Hirst JA, Farmer AJ, Dyar A, et al. Estimating the effect of sulfonylurea on HbA1c in diabetes: a systematic review and meta-analysis. Diabetologia 2013;56:973.
45. Henry RR, Gumbiner B, Ditzler T, et al. Intensive conventional insulin therapy for type II diabetes. Metabolic effects during a 6-mo outpatient trial. Diabetes Care 1993;16:21.
46. Rosenstock J, Sugimoto D, Strange P, et al. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naive patients. Diabetes Care 2006;29:554.
47. Lingvay I, Legendre JL, Kaloyanova PF, et al. Insulin-based versus triple oral therapy for newly diagnosed type 2 diabetes: which is better? Diabetes Care 2009;32:1789.
48. Vinik AI, Zhang Q. Adding insulin glargine versus rosiglitazone: health-related quality-of-life impact in type 2 diabetes. Diabetes Care 2007;30:795.
49. Schwartz S, Sievers R, Strange P, et al. Insulin 70/30 mix plus metformin versus triple oral therapy in the treatment of type 2 diabetes after failure of two oral drugs: efficacy, safety, and cost analysis. Diabetes Care 2003;26:2238.
50. Yki-Järvinen H, Ryysy L, Nikkilä K, et al. Comparison of bedtime insulin regimens in patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med 1999;130:389.
51. Abraira C, Colwell JA, Nuttall FQ, et al. Veterans Affairs Cooperative Study on glycemic control and complications in type II diabetes (VA CSDM). Results of the feasibility trial. Veterans Affairs Cooperative Study in Type II Diabetes. Diabetes Care 1995;18:1113.
52. Yki-Järvinen H, Kauppila M, Kujansuu E, et al. Comparison of insulin regimens in patients with non-
insulin- dependent diabetes mellitus. N Engl J Med 1992;327:1426.
53. Chow CC, Tsang LW, Sorensen JP, Cockram CS. Comparison of insulin with or without continuation of oral hypoglycemic agents in the treatment of secondary failure in NIDDM patients. Diabetes Care 1995;18:307.
54. Hemmingsen B, Christensen LL, Wetterslev J, et al. Comparison of metformin and insulin versus insulin alone for type 2 diabetes: systematic review of randomised clinical trials with meta-analyses and trial sequential analyses. BMJ 2012;344:e1771.
55. Wulffelé MG, Kooy A, Lehert P, et al. Combination of insulin and metformin in the treatment of type 2 diabetes. Diabetes Care 2002;25:2133.
56. Kooy A, de Jager J, Lehert P, et al. Long-term effects of metformin on metabolism and microvascular and macrovascular disease in patients with type 2 diabetes mellitus. Arch Intern Med 2009;169:616.
57. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854.
58. Johnson JL, Wolf SL, Kabadi UM. Efficacy of insulin and sulfonylurea combination therapy in type II diabetes. A meta-analysis of the randomized placebo-controlled trials. Arch Intern Med 1996;156:259.
59. Wright A, Burden AC, Paisey RB, et al. Sulfonylurea inadequacy: efficacy of addition of insulin over 6 years in patients with type 2 diabetes in the U.K. Prospective Diabetes Study (UKPDS 57). Diabetes Care 2002;25:330.
60. Pugh JA, Wagner ML, Sawyer J, et al. Is combination sulfonylurea and insulin therapy useful in NIDDM patients? A metaanalysis. Diabetes Care 1992;15:953.
61. Landstedt-Hallin L, Adamson U, Arner P, et al. Comparison of bedtime NPH or preprandial regular insulin combined with glibenclamide in secondary sulfonylurea failure. Diabetes Care 1995;18:1183.
62. Raskin P, Rendell M, Riddle MC, et al. A randomized trial of rosiglitazone therapy in patients with inadequately controlled insulin-treated type 2 diabetes. Diabetes Care 200124:1226.
63. US Food and Drug Administration. MedWatch the FDA Safety Information and Adverse Event Reporting Program - Avandia (rosiglitazone), April 2002. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm154468.htm (Accessed on June 13, 2012).
64. Palmer SC, Mavridis D, Nicolucci A, et al. Comparison of Clinical Outcomes and Adverse Events Associated With Glucose-Lowering Drugs in Patients With Type 2 Diabetes: A Meta-analysis. JAMA 2016;316:313.
65. Chiasson JL, Josse RG, Hunt JA, et al. The efficacy of acarbose in the treatment of patients with non-insulin- dependent diabetes mellitus. A multicenter controlled clinical trial. Ann Intern Med 1994;121:928.
66. Johnston PS, Feig PU, Coniff RF, et al. Long-term titrated-dose alpha-glucosidase inhibition in non-insulin-requiring Hispanic NIDDM patients. Diabetes Care 1998;21:409.
67. In Brief: A new indication for colesevelam. Med Lett Drugs Ther 2008;50:33.
68. Ooi CP, Loke SC. Colesevelam for type 2 diabetes mellitus. Cochrane Database Syst Rev 2012;12:CD009361.
69. Fonseca VA, Rosenstock J, Wang AC, et al. Colesevelam HCl improves glycemic control and reduces LDL cholesterol in patients with inadequately controlled type 2 diabetes on sulfonylurea-based therapy. Diabetes Care 2008;31:1479.
70. Goldberg RB, Fonseca VA, Truitt KE, Jones MR. Efficacy and safety of colesevelam in patients with type 2 diabetes mellitus and inadequate glycemic control receiving insulin-based therapy. Arch Intern Med 2008;168:1531.
71. Bromocriptine (Cycloset) for Type 2 Diabetes. Med Lett Drugs Ther 2010;52:97.
72. Cincotta AH, Meier AH, Cincotta Jr M. Bromocriptine improves glycaemic control and serum lipid profile in obese Type 2 diabetic subjects: a new approach in the treatment of diabetes. Expert Opin Investig Drugs 1999;8:1683.
73. Gaziano JM, Cincotta AH, O'Connor CM, et al. Randomized clinical trial of quick-release bromocriptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes. Diabetes Care 2010;33:1503.
74. Dixon JB, O'Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA 2008;299:316.
75. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med 2012;366:1577.
76. Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med 2012;366:1567.
77. Ikramuddin S, Korner J, Lee WJ, et al. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes, hypertension, and hyperlipidemia: the Diabetes Surgery Study randomized clinical trial. JAMA 2013;309:2240.
78. Maggard-Gibbons M, Maglione M, Livhits M, et al. Bariatric surgery for weight loss and glycemic control in nonmorbidly obese adults with diabetes: a systematic review. JAMA 2013;309:2250.
79. Gloy VL, Briel M, Bhatt DL, et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ 2013;347:f5934.
80. Courcoulas AP, Goodpaster BH, Eagleton JK, et al. Surgical vs medical treatments for type 2 diabetes mellitus: a randomized clinical trial. JAMA Surg 2014;149:707.
81. Puzziferri N, Roshek TB 3rd, Mayo HG, et al. Long-term follow-up after bariatric surgery: a systematic review. JAMA 2014;312:934.
82. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet 2015;386:964.
83. Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. N Engl J Med 2014;370:2002.
84. Courcoulas AP, Belle SH, Neiberg RH, et al. Three-Year Outcomes of Bariatric Surgery vs Lifestyle Intervention for Type 2 Diabetes Mellitus Treatment: A Randomized Clinical Trial. JAMA Surg 2015;150:931.
85. Ludwig DS, Ebbeling CB, Livingston EH. Surgical vs lifestyle treatment for type 2 diabetes. JAMA 2012;308:981.
86. Del Prato S, Heine RJ, Keilson L, Guitard C, Shen SG, Emmons RP. Treatment of patients over 64 years of age with type 2 diabetes: experience from nateglinide pooled database retrospective analysis. Diabetes Care 2003;26:2075–2080.
87. Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet 2006;368:29–36.
88. Nelson JM, Dufraux K, Cook PF. The relationship between glycemic control and falls in older adults. J Am Geriatr Soc 2007;55:2041–2044.
89. Ismail-Beigi F, Moghissi E, Tiktin M, Hirsch IB, Inzucchi SE, Genuth S. In- dividualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials. Ann Intern Med 2011;154: 554–559.
90. Sluik D, Boeing H, Montonen J, et al. Associations between general and ab- dominal adiposity and mortality in in- dividuals with diabetes mellitus. Am J Epidemiol 2011;174:22–34.
REVIEW ARTICLE

Cardiology Today VOL. XXI NO. 2, 2017 81
91. Unick JL, Beavers D, Jakicic JM, et al.; Look AHEAD Research Group. Effec- tiveness of lifestyle interventions for in- dividuals with severe obesity and type 2 diabetes: results from the Look AHEAD trial. Diabetes Care 2011;34:2152–2157.
92. Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA. Beta- cell function in subjects spanning the range from normal glucose tolerance to overt diabetes: a new analysis. J Clin Endocrinol Metab 2005;90:493–500.
93. Krentz AJ, Bailey CJ. Oral antidiabetic agents: current role in type 2 diabetes mellitus. Drugs 2005;65:385–411.
94. Hermansen K, Davies M, Derezinski T, Martinez Ravn G, Clauson P, Home P. A 26-week, randomized, parallel, treat- to-target trial comparing insulin dete- mir with NPH insulin as add-on therapy to oral glucose-lowering drugs in in- sulin-naive people with type 2 diabetes. Diabetes Care 2006;29:1269–1274.
95. Nauck MA. Incretin-based therapies for type 2 diabetes mellitus: properties, func- tions, and clinical implications. Am J Med 2011;124(Suppl.):S3–S18.
96. Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta- analysis. Am J Med 2009;122:248–256.e5
97. Davis TM, Wright AD, Mehta ZM, et al. Islet autoantibodies in clinically diagnosed type 2 diabetes: prevalence and relation- ship with metabolic control (UKPDS 70). Diabetologia 2005;48:695–702.
98. Park YW, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield SB. The meta- bolic syndrome: prevalence and associated risk factor findings in the US population from the Third National Health and Nu- trition Examination Survey, 1988-1994. Arch Intern Med 2003;163:427–436.
99. Chen KW, Boyko EJ, Bergstrom RW, et al. Earlier appearance of impaired in- sulin secretion than of visceral adiposity in the pathogenesis of NIDDM. 5-Year follow-up of initially nondiabetic Japanese- American men. Diabetes Care 1995;18: 747–753.
100. Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunc- tion to the pathophysiology of type 2 di- abetes. Diabetologia 2003;46:3–19
101. Malecki MT, Mlynarski W. Monogenic diabetes: implications for therapy of rare types of disease. Diabetes Obes Metab 2008;10:607–616.
102. Nordin C. The case for hypoglycaemia as a proarrhythmic event: basic and clinical evidence. Diabetologia 2010;53: 1552–1561.
103. Riveline JP, Danchin N, Ledru F, Varroud-Vial M, Charpentier G. Sulfo- nylureas and cardiovascular effects: from experimental data to clinical use. Available data in humans and clinical applications. Diabetes Metab 2003;29:207–222.
104. Turner RC, Holman RR, Cull CA, et al.; UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complica- tions in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352: 854–865.
105. Dormandy JA, Charbonnel B, Eckland DJ, et al.; PROactive investigators. Sec- ondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macro- Vascular Events): a randomised con- trolled trial. Lancet 2005;366:1279–1289.
106. Sulistio M, Carothers C, Mangat M, Lujan M, Oliveros R, Chilton R. GLP-1 agonist-based therapies: an emerging new class of antidiabetic drug with potential cardioprotective effects. Curr Atheroscler Rep 2009;11:93–99.
107. Hanefeld M, Schaper F. Acarbose: oral anti-diabetes drug with additional car- diovascular benefits. Expert Rev Cardio- vasc Ther 2008;6:153–163.
108. Gaziano JM, Cincotta AH, O’Connor CM, et al. Randomized clinical trial of quick- release bromocriptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes. Diabetes Care 2010;33:1503–1508.
109. Masoudi FA, Inzucchi SE. Diabetes mellitus and heart failure: epidemiology, mechanisms, and pharmacotherapy. Am J Cardiol 2007;99:113B–132B.
110. Lago RM, Singh PP, Nesto RW. Con- gestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: a meta-analysis of randomised clinical trials. Lancet 2007;370:1129–1136.
111. Chaggar PS, Shaw SM, Williams SG. Review article: Thiazolidinediones and heart failure. Diab Vasc Dis Res 2009;6:146–152.
112. Tahrani AA, Varughese GI, Scarpello JH, Hanna FW. Metformin, heart failure, and lactic acidosis: is metformin absolutely contraindicated? BMJ 2007;335:508–512
113. Inzucchi SE, McGuire DK. New drugs for the treatment of diabetes: part II: Incretin-based therapy and beyond. Circulation 2008;117:574–584.
114. Huang ES, Liu JY, Moffet HH, John PM, Karter AJ. Glycemic control, complications, and death in older diabetic patients: the Diabetes and Aging Study. Diabetes Care 2011;34:1329–1336.
115. Koro CE, Lee BH, Bowlin SJ. Antidiabetic medication use and prevalence of chronic kidney disease among patients with type 2 diabetes mellitus in the United States. Clin Ther 2009;31:2608–2617.
116. Holstein A, Stumvoll M. Contraindications can damage your healthdis metformin a case in point? Diabetologia 2005;48: 2454–2459.
117. Lipska KJ, Bailey CJ, Inzucchi SE. Use of metformin in the setting of mild-to-moderaterenal insufficiency. Diabetes Care 2011; 34:1431–1437.
118. Nye HJ, Herrington WG. Metformin: the safest hypoglycaemic agent in chronic kidney disease? Nephron Clin Pract 2011;118:c380–c383.
119. NICE. Type 2 Diabetes: The Management of Type 2 Diabetes: NICE Clinical Guide- line 87. National Institute for Health and Clinical Excellence, 2009.
120. Ong JP, Younossi ZM. Epidemiology and natural history of NAFLD and NASH. Clin Liver Dis 2007;11:1–16, vii
121. Ahmed MH, Byrne CD. Current treatment of non-alcoholic fatty liver disease. Diabetes Obes Metab 2009;11:188–195.
122. Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med 2011;43:617–649.
123. Tushuizen ME, Bunck MC, Pouwels PJ, van Waesberghe JH, Diamant M, Heine RJ. Incretin mimetics as a novel thera- peutic option for hepatic steatosis. Liver Int 2006;26:1015–1017.
124. Gerstein HC, Miller ME, Genuth S, et al.; ACCORD Study Group. Long-term ef- fects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med 2011;364:818–828.
125. Berlie HD, Garwood CL. Diabetes med- ications related to an increased risk of falls and fall-related morbidity in the el- derly. Ann Pharmacother 2010;44:712–717.
82 Cardiology Today VOL. XXI NO 2, 2017
Echocardiographic evaluation of complications of infective endocarditis
IMAGE
SR MITTAL
Keywords � annular abscess � embolism � fi stula � pseudo aneurysm
Dr. SR Mittal is Head, Department of Cardiology at Mittal Hospital and Research Centre, Ajmer, Rajasthan
ECHOCARDIOGRAPHIC EVALUATION OF COMPLICATIONS OF INFECTIVE ENDOCARDITIS(1) Embolism An embolism can occur even when there is no detectable vegetation.1 Th is is because currently available equipments can detect vegetations only larger than 2 mm.2,3 Further, a vegetation begins as a microscopic focus of infection which only gradually grows into a detectable mass. Vegetations on a pre-existing severe lesion
or a prosthetic valve may also be missed.4 Non-oscillating vegetations, vegetations of atypical location (chordae or chamber wall) and cardiac device-related infective endocarditis can also be missed as “normal”.4 Risk of embolism increases with increasing size and mobility of vegetation.5 Vegetation on mitral valve specially on anterior leafl et is more likely to embolise.6 Risk of embolism is also higher with multivalvular endocarditis and vegetations increasing in size under
AbstractEmbolism can occur even when there are no vegetations detectable on routine echocardiography. Risk of embolism increases with increasing size and mobility of vegetation. Vegetations on anterior mitral leafl et are more likely to embolise. Perivalvular complications are more frequent with aortic valve endocarditis. Mitral aortic intervalvular fi brosa is frequently involved. Transesophageal echocardiography is more sensitive in detecting early abscess which appears as thickening of aortic root. Later it appears as an area of reduced echo density. There is no blood fl ow inside the abscess. Pseudo aneurysm is an echo free space communicating with cardiovascular lumen and having blood fl ow on colour doppler imaging. Rupture of an abscess or pseudo aneurysm can result in connection between two distinct cardiac blood spaces with high-velocity jet across the defect (fi stula). Perivalvular regurgitation can occur as a complication of prosthetic valve endocarditis. In native valve endocarditis acute regurgitation can be due to acute perforation or fl ail leafl et. Acute severe aortic regurgitation results in very short pressure half time of AR jet, restrictive pattern of mitral valve infl ow and premature closure of mitral valve. Acute severe mitral regurgitation results in truncation of continuous wave doppler regurgitation signal.

Cardiology Today VOL. XXI NO 2, 2017 83
Figure 1. Diagrammatic representation of the usual site for early perivalvular abscess formation (arrow) in aortic valve infective endocarditis. AML- Anterior mitral leaflet.
Figure 2. Diagrammatic representation of short axis view of the usual site for perivalvular abscess (arrow) in aortic valve infective endocarditis. LA- Left atrium, L- left coronary cusp, N- Non coronary cusp, R- Right coronary cusp, RA- right atrium, TV- Tricuspid valve, RV- Right ventricle, PV – Pulmonary valve, MPA- Main pulmonary valve.
Figure 3. Diagrammatic representation of extension of aortic root abscess in interventricular septum (arrow). IVS- Interventricular septum, LA- Left atrium, LV- Left ventricle, PW- Left ventricular posterior wall, RVOT- right ventricular outflow tract.
Figure 4. Diagrammatic representation of extension (arrow), of sinus of valsalva aneurysm in right ventricular outflow tract (RVOT). IVS- Interventricular septum, LA- Left atrium, LV- left ventricle, PW- left ventricular posterior wall.
antibiotic therapy.7 Risk of embolism decreases rapidly within the fi rst week of eff ective antibiotic therapy.3 Vegetations frequently persist aft er successful medical treatment.8 Such vegetations are more echogenic and relatively fi xed. Th ese are less likely to embolise. Nearly 50% of systemic emboli are clinically silent3 and may be detected only by CT scan of abdomen and head.4 Right-sided endocarditis produces pulmonary embolism. Echocardiography aft er removal of intracardiac leads may reveal residual fl oating masses in right atrium (ghosts).9 Th ese masses have been related with pulmonary embolism and sudden death. Perivalvular complications Th ese are more frequent with aortic valve endocarditis than with mitral valve en-docarditis.4 Mitral aortic intervalvular fi -brosa (MAIF) is frequently involved. It is the fi brous zone of continuity between the noncoronary cusp of the aortic valve and the insertion of anterior mitral leafl et.10 Being one of the least vascular structures of the heart, MAIF is more susceptible to infection and mycotic false aneurysm for-mation.
(a) AbscessIt commonly involves aortic valve annulus at the junction of the aortic root and anterior mitral leafl et3 (Figure 1, 2). Th en it may extend into adjacent interventricular septum (Figure 3), right ventricular outfl ow tract, interatrial septum or anterior mitral leafl et. In early stage, it
appears as thickening of the aortic root. Th ickening may be better appreciated by transesophageal echocardiography. Aortic root replacement or Bentall’s procedure may themselves also produce echocardiographic thickening of aortic root in absence of infective endocarditis. Later it appears as an area of reduced echo density which is nonhomogeneous. Subsequently it appears as clear echofree space. Th ere is no blood fl ow inside the abscess on colour Doppler imaging. Th ere is diffi culty in echocardiographic diagnosis of a small abscess localised around calcifi ed posterior mitral annulus.11
(b) Pseudoaneurysm (Figure 4,5)It is a perivalvular echofree space communicating with cardiovascular lumen. In aortic position, communication is usually from subvalvular left ventricular outfl ow tract.10 Communication results in color doppler fl ow inside the cavity and pulsation of the aneurysm. Potential complications include fi stulous communication with left atrium or aorta, extension around the aortic root, compression of proximal left coronary artery, systemic embolization or rupture in pericardial sac.
(c) Fistula12 (Figure 6)It is defi ned as connection between two distinct cardiac blood spaces through a nonanatomic channel.13 Th ere is clear
Figure 5. Diagrammatic representation of aneurysm (A) of anterior mitral leaflet. LA- Left atrium, LV- Left ventricle, RA- right atrium, RV- Right ventricle.
defect with high velocity jet across the defect or continuous wave doppler.3 Small defects are likely to be missed. Jet of valvular regurgitation can also mask fl ow through fi stulous tract.
(3) Acute regurgitation It can be due to new perivalvular regurgi-

84 Cardiology Today VOL. XXI NO 2, 2017
tation in case of a prosthetic valve (Figure 7). In native valve endocarditis it can be due to perforation (Figure 8), prolapse or fl ait of the involved cusp or leafl et. Perfo-ration is defi ned as defect in the body of a leafl et with evidence of fl ow across it.3 Multiple views may be needed to diff er-entiate perforation from leafl et regurgita-
tion.3 dimensional echocardiography may help precise location of perforation. Cleft in the valve may also produce regurgita-tion that may resemble perforation. Acute severe aortic regurgitation results in rapid elevation of left ventricular diastolic fi ll-ing pressure. It results in very short pres-sure half time of aortic regurgitation jet (Figure 9a), restrictive pattern of mitral valve infl ow (Figure 9b) and premature closure of mitral valve10 (Figure 9c). Acute severe mitral regurgitation results in trun-cation of the usual parabolic continuous wave Doppler regurgitation signal (Figure 10) due to late systolic equilibration of left ventricular and left atrial pressures.
(4) Pericardial eff usion14It is commonly secondary to renal failure, pulmonary hypertension or heart failure. Purulent pericardial eff usion is uncom-mon these days because of early diagnosis and eff ective management. It can occur due to extension of infection or rupture of an abscess.
(5) Mycotic aneurysm2It is defi ned as echo-lucent outpouching of a vessel wall. It may be fi lled with in-fectious material or contain free fl owing blood. It is produced due to embolism in vasavasorum. It may involve coronary sinuses, aorta, cerebral or peripheral ves-sels.
REFERENCES1. Sanfilippo AJ, Picard MH, Newell JB, et al. Echocardio-
graphic assessment of patients with infective endocardi-tis :Prediction of risk for complications. J Am Coll Cardiol 1991;18:1191-99.
2. Armstrong WF, Ryan T. Infective endocarditis. In Arm-strong WF, Ryan T (eds). Feigenbaum’s Echocardiography. Wolters Kluwer, Philadelphia; 2010:361-84.
3. Samad Z, Wang A. Clinical decision making in patients with infective endocarditis. The role of echocardiography. In Otto CM (ed). The practice of Clinical Echocardiogra-phy. Elsevier, Philadelphia; 2012:408-24.
4. Habib G, Thung F. Endocarditis. In Zamorano JL, Bax JJ, Rademakers FE, Knuuti J (eds). ESC Textbook of Cardio-vascular Imaging. Springer, New York; 2010:206-22.
5. Thung F, Di Salve G, Belliard O, et al. Risk of embolism and death in infective endocarditis: prognostic value of echocardiography: a prospective multicenter study. Cir-culation 2005;112:69-75.
6. Cabell CH, Pond KK, Peterson GE, et al. The risk of stroke and death in patients with aortic and mitral valve endo-carditis. Am Heart J 2001;142:75-80.
7. Habib G. Embolic risk in subacute bacterial endocarditis: Role of transesophageal echocardiography. Curr Cardiol Rep 2003; 5:129-36.
8. Vuille C, Nidarf M, Weyman RE, et al. Natural history of vegetations during successful medical treatment of en-docarditis. Am heart J 1994;128:1200-9.
9. Le Dolley Y, Thung F, Mancini J et al. Diagnosis of cardiac device related infective endocarditis after device removal. JACC Cardiovascular Imaging 2010;3:673-86.
10. Baddour LM, Freeman WK, Suri RM, Wilson WR. Cardio-vascular infections. In Mann DL, Zipes DP, Libby P, Bonow RO (eds). Braunwald’s Heart Disease. Elsevier, Philadel-phia; 2005:1524-47.
11. Hill EE, Herizgers P, Claus P, Vanderschueren S, Peeter-mans WE, Herregade MC. Abscess in infective endocardi-tis: the value of transesophageal echocardiography and outcome: a 5 year study. Am Heart J 2007;154:923-8.
12. Anguera I, Miro JM, Vilacosta I et al. Aorto-cavitary fistu-lous tract formation in infective endocarditis: Clinical and echocardiographic features of 76 cases and risk factors for mortality. Eur Heart J 2005;26:288-97.
13. Halder SM, O’Gara PT. Infective endocarditis. In Fuster V, Walsh RA, Harrington RA(eds) Hurst’s The Heart. Mc Graw Hill, New York; 2011:1940-69.
14. Lopez J, Sevilla T, San Roman JA et al. Echocardiography in infective endocarditis. In Nanda NC (ed). Comprehen-sive Textbook of Echocardiography. Jaypee, New Delhi ; 2014:1042-62.
IMAGE
Figure 7. Diagrammatic representation of dehiscence of prosthetic aortic valve (PAV) with perivalvular aortic regurgitation (AR). LA- Left atrium, LV- Left ventricle, IVS- Interventricular septum, PW- left ventricular posterior wall.
Figure 8. Diagrammatic representation of perforation (arrow) of anterior mitral leaflet resulting in mitral regurgitation (MR).LA- Left atrium, LV- Left ventricle, RA- Right atrium, RV- right ventricle.
Figure 9. Diagrammatic representation showing echocardiographic differences between chronic aortic regurgitation and acute aortic regurgitation. (a) Doppler evaluation of jet of aortic regurgitation (b) Doppler evaluation of mitral inflow (c) M- mode echo of mitral valve (d) Electrocardiogram.
Figure 10. Diagrammatic representation of difference in doppler evaluation of jet of acute and chronic mitral regurgitation.
Figure 6. Diagrammatic representation of sites of rupture of aortic root abscessAO- Aortic root, LA- Left atrium, RA- Right atrium, RV- Right ventricle, MPA- Main pulmonary artery.

Cardiology Today VOL. XXI NO 2, 2017 85
Biventricular Enlargement/ Hypertrophy
ECG OF THE MONTH
SR MITTAL
AbstractElectrocardiographic diagnosis of early biventricular hypertrophy is diffi cult because opposing forces of hypertrophy of two ventricles cancel each other. In presence of voltage criteria of LVH, right axis deviation, clockwise rotation, signs of right atrial overload and R/s ratio greater than 1 in V1 suggest biventricular hypertrophy. Tall R with deep S in leads V2 to V4 with combined amplitude greater than 60 mm (Katz Wachtel sign) also suggests biventricular hypertrophy. This sign is common in children with ventricular septal defect and pulmonary artery hypertension. These signs have high specifi city but low sensitivity.
Keywords � congenital heart disease � left ventricular hypertrophy � right ventricular hypertrophy
INTRODUCTIONECG diagnosis of early biventricular hypertrophy (BVH) is diffi cult because normally greater left ventricular forces require much greater degree of right ven-tricular hypertrophy, before it can mani-fest on ECG.1 Th is is because opposing forces of hypertrophy of two ventricles cancel each other.2 Further, intraven-tricular conduction defects, accompany-ing hypertrophy of either ventricle also aff ect electrocardiographic diagnosis of ventricular hypertrophy. Several criteria are used for diagnosis of biventricular hy-pertrophy.
(1) ETIOLOGYCommon causes include
- Mitral regurgitation with pulmonary artery hypertension. Th is is common with rheumatic etiology.
- RVH from any cause with systemic hypertension/ gross aortic regurgita-tion/ mitral regurgitation.
- Cardiomyopathy.
(2) SPECIFIC CRITERIA(A) In the presence of voltage criteria of
left ventricular hypertrophy (LVH), one or more of the following fi ndings suggest BVH.3,4
• Right axis deviation.• Clockwise rotation- shift in
precordial transition zone to left (Figure 1).
• Deep S in V5V6• Signs of right atrial overload
Dr. SR Mittal is Head, Department of Cardiology at Mittal Hospital and Research Centre, Ajmer, Rajasthan

86 Cardiology Today VOL. XXI NO 2, 2017
(Figure 2,3).• Tall R in right precordial loads• R/S ratio greater than 15 (Figure
1, 2,3).Caution-
• Asthenic individuals may have LVH voltage criteria in absence of
true LVH• Emphysema and obesity may
mask LVH voltage criteria.
(B) Katz Wachtel phenomenon5Tall R with deep S in leads V2 to V4 with combined amplitude greater than 60mm3 (Figure 4, 5, 6). It is more likely to occur in children with ventricular-septal defect or AV- canal defect with pulmonary artery hypertension. In these conditions, left ventricular volume overload is associated with right ventricular pressure overload.Standard criteria have high specifi city but low sensitivity.2
(3) NON-SPECIFIC CRITERIAMost of the patients do not fulfi l standard
criteria because eff ects of enlargement of one ventricle cancel the eff ects of enlarge-ment of another ventricle. Several sub-tle ECG fi ndings may also suggest early BVH.
� Right axis deviation with – qR con-fi guration in V5,V6 (Figure 7) or
- Predominant R in V5V62 but not
fulfi lling LVH voltage criteria or
(a) (b) (b)(a)
ECG OF THE MONTH
Figure 1. Electrocardiogram from a patient of VSD with pulmonary artery hypertension showing right axis deviation, prominent R wave in lead V1, left atrial overload (prominent negative deflection of P wave in lead V1), clockwise rotation and prominent qR in leads V4 and V5.
(b)(b)(b)))(a)(a)(a)(a(a(a(a(aaa
Figure 2. Electrocardiogram showing prominent R wave in lead V1, right atrial overload (tall peaked P waves in leads II, aVF and V1 to V4) with tall R waves in leads V2 to V6.
Figure 3. Electrocardiogram from a patient of Tetralogy of Fallot with aortic regurgitation showing right axis deviation, right atrial overload (tall peaked P wave in leads V1, V2) with tall R waves in leads V2 and V4.
Figure 4. Electrocardiogram from a case of Eisenmenger syndrome showing right axis deviation, prominent R in lead V1, left atrial overload and tall RS (55 mm) in leads V4 and V5 (Katz-Wachtel sign).

Cardiology Today VOL. XXI NO 2, 2017 87
Figure 5. Electrocardiogram from case of Ventricular septal defect (VSD) with pulmonary artery hypertension showing incomplete RBBB with tall RS (>60 mm) in leads V3 to V5 (Katz-Wachtel sign).
Figure 6. Electrocardiogram from a case of A-V canal defect with pulmonary artery hypertension showing SISIISIII, counter clockwise loop (q in I and aVL), prominent R in lead V1 with tall RS in lead V3 (70 mm) and V4 (80 mm) (Katz Wachtel sign).
Figure 7. Electrocardiogram from a case of VSD with right ventricular outflow tract obstruction showing right axis deviation, prominent R in lead V1 and qR in leads V5V6.
Figure 8. Electrocardiogram showing atrial fibrillation, right axis deviation, deep S wave in leads V3 (35 mm) and V4 (35 mm).
Figure 9. Electrocardiogram showing atrial fibrillation, qR in V1 and deep S in leads V3 (45mm) and V4 (35 mm).
- RS in V1 and very deep S in V22,6
(Figure 8, 9) or - Prominent R with ST-depression
in lead V5 V6 suggestive of LVH (Figure 10) or
- Left atrial enlargement2 (Figure 11,12) (Except in mitral stenosis).
Caution-Left inferoposterior hemiblock should not be wrongly interpreted as right axis
deviation. � S1S2S3 with prominent R or qR in V5V6 � Tall equiphasic RS in leads V3 and
V4 not fulfi lling criteria of 60 mm (Figure 13)

88 Cardiology Today VOL. XXI NO 2, 2017
� Tall R in right as well as left precordial leads.4
Th ese criteria are less specifi c but more sensitive.
REFERENCES1. Mirvis DM, Goldberger AL. Electrocardiography. In Mann
DL, Zipes DP, Libby P, Bonow RO (eds). Braunwald’s Heart Disease. Elsevier, Philadelphia; 2015:114-152.
2. De luna AB, Goldwasser D, Fiol M, Bayes- Genis A. Sur-face electrocardiography. In Fuster V, Walsh RA, Har-rington RA(eds). Hurst’s The Heart. Mc Graw Hill, New York; 2011:307-370.
3. Hancock EW, Deal BJ, Mirvis DM, Okin P, Kligfield P. Gettes LS. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardio-gram. Part V Electrocardiogram changes associated with cardiac chamber hypertrophy. J Am Coll Cardiol 2009; 53:992-1002.
4. Mirvis DM, Goldberger AL. Electrocardiography. In Bonow RO, Mann DL, Zipes DP, Libby P(eds). Braunwald’s Heart Disease. Elsevier, St Louis; 2012:126-165.
5. Schamroth C. Right ventricular hypertrophy. In Schamroth C(ed). An introduction to electrocardiography. Blackwell Science, France; 1982:78-85.
6. Wagner GS, Lim TH. Chamber enlargement. In Wagner GS(ed). Marriott’s Practical electrocardiography. Wolters Kluwer, Philadelphia; 2008:71-96.
Figure 10. Electrocardiogram showing P-Pulmonale (tall peaked P waves in V2, V3), qr configuration in lead V1 and V2, and ST depression in leads V4-V6.
Figure 11. Electrocardiogram showing right axis deviation, incomplete RBBB and left atrial overload (prominent negative deflection of P wave in lead V1).
Figure 12. Electrocardiogram showing right axis deviation, biatrial enlargement (tall peaked P wave in leads II, III, aVF, prominent negative P wave in leads V1 to V3 and wide and notched P wave in V5) and qR in V7.
Figure 13. Electrocardiogram showing SISIISIII counter clockwise loop (q in I and aVL), RVH (tall R in V1), tall RS in V3 and qRS in V5V6.
ECG OF THE MONTH

Cardiology Today VOL. XXI NO 2, 2017 89
Q.1. Which ECG fi ndings suggest bi-ventricular enlargement?
(A) LVH +LAD(B) LVH + RAD (C) LVH + Clockwise rotation(D) LVH + Counter clockwise rotation
Q.2. Which ECG fi ndings do not sug-gest biventricular enlargement?
(A) LVH + deep S in V5V6(B) LVH + Tall R in V1(C) LVH + left atrial overload(D) LVH + right atrial overload
Q.3. Katz- Wachtel phenomenon is seen in
(A) Leads V3R to V1(B) Leads V2 to V4(C) Leads V7 to V8 (D) Leads I and aVL
MCQsQ.7. Causes of right axis deviation - (A) RVH (B) Left postero-inferior fascicular
block(C) Left antero-superior fascicular
block (D) RBBB
Q.8. Causes of voltage criteria of LVH(A) Asthenic individuals(B) Emphysema(C) Obesity (D) Pericarditis
Q.4. In Katz-Wachtel phenomenon R + S amplitude should be more than
(A) 30 mm(B) 40 mm(C) 50 mm(D) 60 mm
Q.5. Katz- Wachtel phenomenon is commonly seen in
(A) VSD + PAH (B) AV canal defect with PAH(C) LV to RA shunt(D) TOF + AR
Q.6. Which ECG fi nding are not sug-gestive of biventricular hyper-trophy ?
(A) R in V1 + qR in V5(B) R in V1 + S in V6(C) R in V1 + deep S in V2(D) RAD + left atrial overload
Biventricular enlargement /hypertrophy
Answers:(1) B, C, (2) A,C, (3)B, (4) D, (5) A, B, (6) B, (7) A, B, (8) A.

90 Cardiology Today VOL. XXI NO 2, 2017
PICTORIAL CME
MONIKA MAHESHWARI
Dr. Monika Maheshwari is Associate Professor at Jawahar Lal Nehru Medical College, Ajmer, Rajasthan
Wolff-Parkinson-White Syndrome Mimicking High Lateral Myocardial Infarction
Figure 2. Electrocardiogram showing normal sinus rhythm with normalisation of ST segment in leads I and aVL, normalization of PR segment and disappearance of delta wave –type QRS configuration.
Th e electrocardiogram of a young male with Wolf–Parkinson-White Syndrome, erroneously interpreted as acute high lateral myocardial infarction is described herein. (Figure 1,2,3,4).
Figure 1. Electrocardiogram showing ST elevation in Leads I and aVL, withshort PR segment, delta wave and slurred upstroke of wide QRS complex
Figure 3. CT Coronary Angiography showing normal Left circumflex artery (LCx) and left anterior descending artery (LAD) and its diagonal branches (D1 and D2)
Figure 4. CT Coronary Angiography showing normal obtuse marginal branches (OM1 and OM2) of Left circumflex artery.

MANUSCRIPTManuscripts must be neatly typed in double space typing throughout on one side of the sheet of good quality bond pa-per of the size 28 x 22cm with 3cm margins on both sides. Words should not be hyphenated at the end of a line.Authors are requested to send the article on e-mail ([email protected]) or CD with one orginal copy of the type script should be submitted alongwith to the Publisher, CIMS Medica India Pvt Ltd, 709, Devika Tower, Nehru Place, New Delhi-1100 19.Material received for publication will be acknowledged and the decision regarding publication will be communicated to the “Author for correspondence”. The manuscript of case reports/studies and original articles should be arranged in the following sequence : Title page, Abstract, Key Words, Introduction, Material and Methods, Results, Discussion, Acknowledgments, References, Tables and legends to fi gures.Article title: Title should be concise, easier to read and should include all information in the title that will make electronic re-trieval of the article both sensitive and specifi c.Authors’ names and institutional affi liations: The name of the department(s) and institution(s) to which the work should be attributed.Disclaimers, if any, Source(s) of support in the form of grants, equipment, drugs, or all of these. Declaration of Confl ict of InterestContact information for corresponding authors: The name, mailing address, telephone and fax numbers, and e-mail ad-dress of the author responsible for correspondence about the manuscript (“corresponding author-may or may not be the “guarantor” for the integrity of the study). The name and ad-dress of the author to whom requests for reprints should be addressed or a statement that reprints are not available from the authors.Abstract: Structured abstracts are preferred for all original research, systematic reviews articles and case studies. The abstract should provide the background for the study or the article. In case of original research article abstract should state the study’s purpose, basic procedures, main fi ndings, principal conclusions, and funding sources. Introduction: Provide a context or background for the study (that is, the nature of the problem and its signifi cance). State the specifi c purpose or research objective of, or hypothesis tested by, the study or observation; the research objective is often more sharply focused when stated as a question. Both the main and secondary objectives should be clear, and any prespecifi ed subgroup analyses should be described. Provide only directly pertinent references, and do not include data or conclusions from the work being reported.Methods: The Methods section should include only informa-tion that was available at the time the plan or protocol for the study was being written; all information obtained during the study belongs in the Results section.Selection and Description of Participants: Describe your selection of the observational or experimental participants (patients or laboratory animals, including controls) clearly, including eligibility and exclusion criteria and a description of the source population. Because the relevance of such vari-ables as age and sex to the object of research is not always clear, authors should explain their use when they are included in a study report—for example, authors should explain why only participants of certain ages were included or why women were excluded. The guiding principle should be clarity about how and why a study was done in a particular way. When authors use such variables as race or ethnicity, they should defi ne how they measured these variables and justify their relevance.Technical Information: Identify the methods, apparatus (give the manufacturer’s name and address in parentheses), and procedures in suffi cient detail to allow others to reproduce the results. Give references to established methods, including statistical methods (see below); provide references and brief descriptions for methods that have been published but are not well-known; describe new or substantially modifi ed methods, give the reasons for using them, and evaluate their limita-
CARDIOLOGY TODAYINSTRUCTIONS TO AUTHORS
tions. Identify precisely all drugs and chemicals used, includ-ing generic name(s), dose(s), and route(s) of administration.Authors submitting review manuscripts should include a sec-tion describing the methods used for locating, selecting, ex-tracting, and synthesizing data. These methods should also be summarised in the abstract.Statistics: Describe statistical methods with enough detail to enable a knowledgeable reader with access to the original data to verify the reported results. When possible, quan-tify fi ndings and present them with appropriate indicators of measurement error or uncertainty (such as confi dence intervals). Avoid relying solely on statistical hypothesis test-ing, such as P values, which fail to convey important informa-tion about effect size. References for the design of the study and statistical methods should be to standard works when possible (with pages stated). Defi ne statistical terms, abbre-viations, and most symbols. Specify the computer software used.Results: Present your results in logical sequence in the text, tables, and illustrations, giving the main or most important fi ndings fi rst. Do not repeat all the data in the tables or il-lustrations in the text; emphasise or summarise only the most important observations. Extra or supplementary materials and technical detail can be placed in an appendix where they will be accessible but will not interrupt the fl ow of the text, or they can be published solely in the electronic version of the journal.When data are summarised in the Results section, give nu-meric results not only as derivatives (for example, percent-ages) but also as the absolute numbers from which the de-rivatives were calculated, and specify the statistical methods used to analyse them. Restrict tables and fi gures to those needed to explain the argument of the paper and to assess supporting data. Use graphs as an alternative to tables with many entries; do not duplicate data in graphs and tables. Avoid nontechnical uses of technical terms in statistics, such as “random” (which implies a randomising device), “normal,” “signifi cant,” “correlations,” and “sample.”Where scientifi cally appropriate, analyses of the data by such variables as age and sex should be included.Discussion: Emphasise the new and important aspects of the study and the conclusions that follow from them in the context of the totality of the best available evidence. Do not repeat in detail data or other information given in the Introduction or the Results section. For experimental studies, it is useful to begin the discussion by briefl y summarising the main fi nd-ings, then explore possible mechanisms or explanations for these fi ndings, compare and contrast the results with other relevant studies, state the limitations of the study, and ex-plore the implications of the fi ndings for future research and for clinical practice.Link the conclusions with the goals of the study but avoid unqualifi ed statements and conclusions not adequately sup-ported by the data. In particular, avoid making statements on economic benefi ts and costs unless the manuscript includes the appropriate economic data and analyses. Avoid claiming priority or alluding to work that has not been completed. State new hypotheses when warranted, but label them clearly as such.Examples:1. Malik V, Roy D. Management of locally advanced breast
cancer. Cardiology Today 1997;2(5):45-51.(for Journal)2. Sambasivan M. References to central nervous system in
the ancient texts: In: S. Venkatraman (ed). Progress in Clinical Neurosciences, 11th Ed, Mediworld Publications 1996:116-118. (for Chapter in a Book)
For full details, please refer to International Committee of Medical journals Edition. Uniform requirement for manu-script submitted to biomedical journals. N Engl J Med 1991; 324:424-8. BMJ 1991;302:338-341.Tables: Tables should capture information concisely and dis-play it effi ciently. Number tables consecutively in the order of their fi rst citation in the text and supply a brief title for each. Give each column a short or an abbreviated heading. Authors should place explanatory matter in footnotes, not in the head-ing. Explain all nonstandard abbreviations in footnotes. Iden-
tify statistical measures of variations, such as standard devia-tion and standard error of the mean. Be sure that each table is cited in the text. If you use data from another published or unpublished source, obtain permission and acknowledge that source fully.Illustrations (Figures): Figures should be either professionally drawn and photographed, or submitted as photographic-qual-ity digital prints. In addition fi gures can also be in the format of electronic fi les (for example, JPEG or GIF). Letters, numbers, and symbols on fi gures should therefore be clear and consist-ent throughout, and large enough to remain legible when the fi gure is reduced for publication. Figures should be made as self-explanatory as possible, since many will be used directly in slide presentations. Titles and detailed explanations belong in the legends—not on the illustrations themselves.Photomicrographs should have internal scale markers. Sym-bols, arrows, or letters used in photomicrographs should con-trast with the background.Photographs of potentially identifi able people must be ac-companied by written permission to use the photograph.Figures should be numbered consecutively according to the order in which they have been cited in the text. If a fi gure has been published previously, acknowledge the original source and submit written permission from the copyright holder to reproduce the fi gure. Permission is required irrespective of authorship or publisher except for documents in the public domain.For illustrations in color, ascertain whether the journal re-quires color negatives, positive transparencies, or color prints. Accompanying drawings marked to indicate the region to be reproduced might be useful to the editor. Some journals publish illustrations in color only if the author pays the ad-ditional cost.Authors should consult the journal about requirements for fi gures submitted in electronic formats.Legends for Illustrations (Figures): Type or print out legends for illustrations using double spacing, starting on a separate page, with Arabic numerals corresponding to the illustrations. When symbols, arrows, numbers, or letters are used to iden-tify parts of the illustrations, identify and explain each one clearly in the legend. Explain the internal scale and identify the method of staining in photomicrographs.UNITS OF MEASUREMENTMeasurements of length, height, weight, and volume should be reported in metric units (meter, kilogram, or liter) or their decimal multiples.Temperatures should be in degrees Celsius/ Fahrenheit. Blood pressures should be in millimeters of mercury, unless other units are specifi cally required by the journal.Journals vary in the units they use for reporting hematologic, clinical chemistry, and other measurements. Authors must consult the Information for Authors of the particular journal and should report laboratory information in both local and International System of Units (SI). Editors may request that authors add alternative or non-SI units, since SI units are not universally used. Drug concentrations may be reported in ei-ther SI or mass units, but the alternative should be provided in parentheses where appropriate.ABBREVIATIONS AND SYMBOLSUse only standard abbreviations; use of nonstandard ab-breviations can be confusing to readers. Avoid abbreviations in the title of the manuscript. The spelled-out abbreviation followed by the abbreviation in parenthesis should be used on fi rst mention unless the abbreviation is a standard unit of measurement.
Address submissions to:The Publisher
CARDIOLOGY TODAYCIMS Medica India Pvt Ltd,
709, 7th Floor, Devika Tower, Nehru Place, New Delhi-110 019.
Tel: 011-4285 4300, Fax: 011-4285 4310E-mail: [email protected]


















