54
Grand Rounds Presentation 3/27/2015

Grand Rounds Presentation 3/27/2015
SHORTNESS OF BREATH
Medical History Atrial fibrillation COPD HTN Mitral insufficiency Obesity
HPI
SOB for 2 weeks Orthopnea PND Weakness Lower extremity edema Weight gain
Surgical History Left rotator cuff repair Right total knee
arthroplasty
Family History Father-CVA, CAD Mother-CAD, Cancer
Social History Lives with husband Quit smoking-1ppd 50yrs Denies alcohol/drug use
77 YR F
Allergies NKDS
CASE #1

T98.3 P146 R24 BP 133/86 Pulse Ox 82% on room air
12.19
11.1
189
34.8
141
3.8
105
31
13
0.7147
BNP 1056 POC trop <0.02
Total bili 1.10 AST 10 ALT 26 Alk Phos 83 Albumin 2.7
Physical Examination General Appearance: pale, alert, awake,
conversant, oriented HEENT: AtNc, PERRLA, EOMI, JVD + Cardiovascular: Irregularly irregular,
pedal edema, 3+ pitting tibial edema Respiratory: Crackles, Oxygen-on 4L
NC GI: soft, nontender Extremitites: moves all; pitting edema Neuo: alert, oriented, normal speech

ADMITTING DX HOME MEDICATIONS
Home meds: Metoprolol Tratrate 23mg
PO BID Aspirine 81mg Daily Citalopram 20mg PO daily Tramadol 50mg Q6 prn Rivaroxaban 20 mg c Din Atrovastatin 10mg PO
daily Dronedarone 400mg BID Promethazine 25md PO
Q4 prn
New onset CHF Atrial fibrillation RVR
ED course ▪ Cardizem 60mfg PO▪ ASA 325mg▪ Lasix 20mg IV

ECHO
LVEF 65%, No RWMA Left atrium moderate-
severe dilation Mitral Valve prolapse
with moderate – severe regurgitation
R/LHC
Pulmonary artery pressure 55
Mean PCWP 27 EF 48%, 4+ mitral
regurgitation into enlarged left atrium

45 YR OLD MAN
Medical History Asthma
Surgical History Denies
Social History Broker Denies alcohol, drug use Quit smoking 5 yrs ago▪ 20 pack yr history
PROGRESSIVE DYSPNEA 8 months Attributed to asthma Not responding to
inhalers or oral steroids
Family History Sisters died of breast cancer Brother died of pulmonary
hypertension
CASE #2
Allergies NKDA
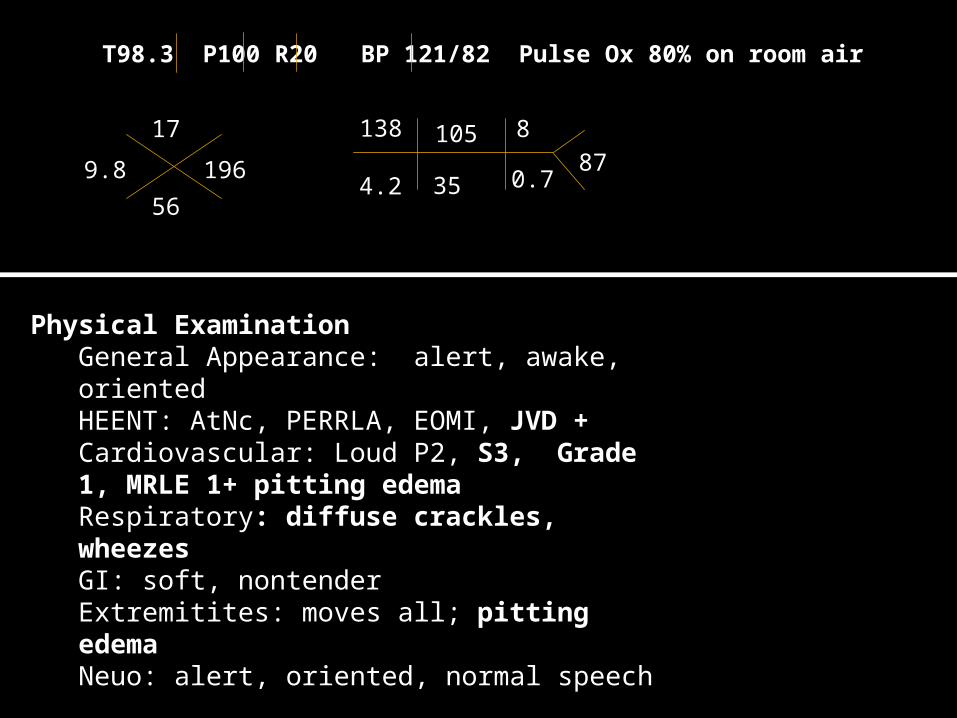
T98.3 P100 R20 BP 121/82 Pulse Ox 80% on room air
9.8
17
196
56
138
4.2
105
35
8
0.787
Physical ExaminationGeneral Appearance: alert, awake, orientedHEENT: AtNc, PERRLA, EOMI, JVD +Cardiovascular: Loud P2, S3, Grade 1, MRLE 1+ pitting edemaRespiratory: diffuse crackles, wheezesGI: soft, nontenderExtremitites: moves all; pitting edemaNeuo: alert, oriented, normal speech

Admitting DX Home Medications Home meds:
Albuterol Symbicort
Duonebs
New onset CHF Acute Asthma
Exacerbation ED course ▪ Bronchodilators▪ Oxygen▪ Lasix 40mg X1
ECHO
Tricuspid regurgitation
PAP of 75mmHg
RHC
PCWP 8
VQ scan pending to rule out embolism
Pulmonary Hypertension
Definition ClassificationPhysiology & PathophysiologySings and Symptoms Diagnostic Approach TreatmentPrognosis Follow up

Definition
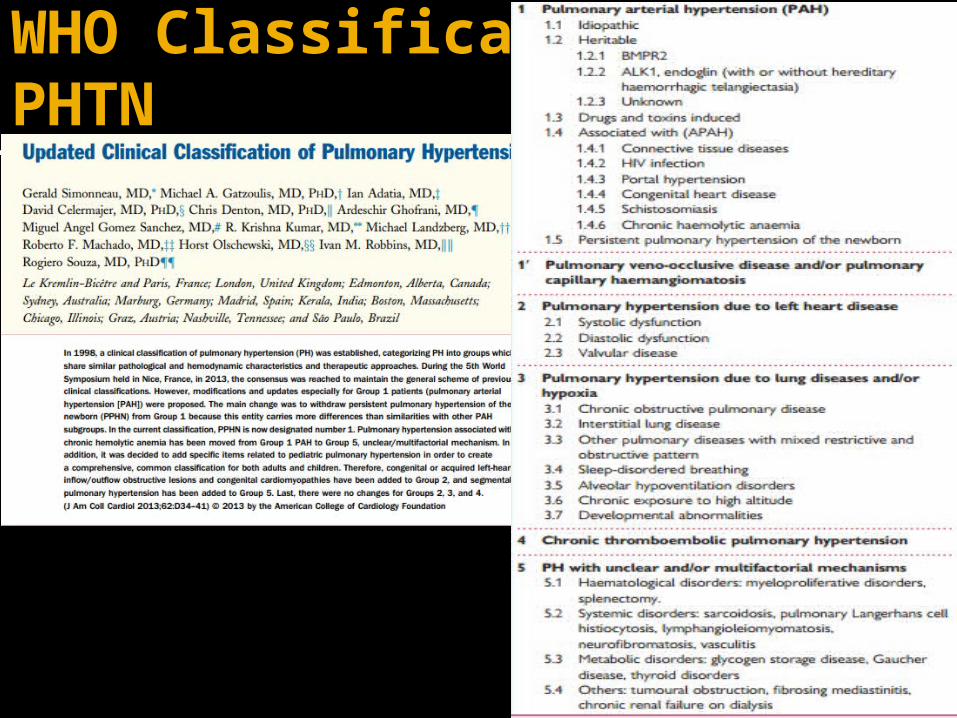
WHO Classification of PHTN


Factors of Late Diagnosis
Symptoms Pulmonary arteries can withstand
changes in hemodynamic 10x the normal Delay in symptoms and signs
manifestation▪ With progressive decline cardiac output

Physiology – Regulation of pulmonary vascular tone
Endothelin Prostacylcin Nitric Oxide
Endothelin
Expressed on endothelial and smooth muscle cells Endothelial cell express Endothelin-B▪ vasodilation
Smooth muscle cells express Endothelin-A and B▪ A-vasoconstriction and cellular proliferation▪ B-vasoconstriction
PAH endothelin levels are elevated Down-regulation of ETB on endothelial cells and
up-regulation on smooth muscle cells Decrease in vasodilation, increased in vasoconstriction Leads to constriction, proliferation and hypertrophy
Nitric Oxide
Continuously produced in the endothelium Vasodilation inhibition of platelet aggregation inhibition of cellular proliferation thrombus formation inflammation
In PAH- levels are decreased, vasoconstriction and cellular proliferation

Prostacylcin
Produced in the endothelial cells Potent vasodilator
In PAH - Reduced Decreased vasodilation and anti-
proliferative effect

Group 1- Pathophysiology and Pathology
Vasoconstriction theory- imbalance between locally produced vasodilators
such as nitric oxide and prostacyclin and vasoconstrictors such as endothelin and thromboxane
New data reflects the role of vascular wall remodeling proliferating endothelial and smooth muscle cells abnormalities in the extracellular matrix ▪ predisposing factors are the mutations in the BMPR2 gene
that result in FPAH and some cases of sporadic IPAH▪ connective tissue disease, the possibility of an
autoimmune injury leading to casulopahty

Group 1- Pathophysiology and Pathology
Destructive vascular changes Inflammation vasoconstriction Cell proliferation/hypertrophy ▪ Tunica intima proliferation▪ Fibrotic changes of tunica intima- concentric and
eccentric▪ Tunica media hypertrophy ▪ Tunica adventitial thickening
Thrombotic lesions Plexiform lesions



Group 2- Pathophysiology and Pathology
Group 2: Left heart disease Enlarged and thickened pulmonary veins Pulmonary capillary dilation Interstitial edema Alveolar hemorrhage Distal pulmonary arteries may be
affected by medical hypertrophy and intimal fibrosis

Group 3- Pathophysiology and Pathology
Group 3 : Lung disease/Hypoxia Medial hypertrophy and intimal
obstructive proliferation of the distal pulmonary arteries
Various degree of destruction of the vascular bed in emphysematous or fibrotic areas

Group 4 &5- Pathophysiology and Pathology
Group 4: Chronic thromboembolic pulmonary hypertension Organized thrombi attached to pulmonary
arterial medial layer in the elastic pulmonary arteries replacing the normal intima
Complete occlusion of the lumen , or form different grade of stenosis , webs or bands
Group 5 Unclear/multifactorial Heterogeneous conditions with different
pathological pictures
Presentation
SYMPTOMS
Non-specific Early symptom s▪ Dyspnea▪ Fatigue▪ Weakness
Late Symptoms ▪ Angina▪ LE edema ▪ Abdominal fullness/pain▪ Syncope▪ Dyspnea at rest
SIGNS
Accentuated P2 Pansystolic murmur of
TR Diastolic murmur of
PR RV third heart sound Jugular vein distention Hepatomegaly Peripheral edema Ascites Cool extremities

Diagnostic Approach
Unexplained dyspnea Comorbidity/ high risk patients
Family history of PAH Connective tissue disease HIV Congenital heart disease Chronic liver disease

Diagnostic Approach
Identifying the presence of PHT Identifying the cause on the bases of
clinical classification Screening/diagnostic tools
Chest radiography Transthoracic Doppler echocardiography Ventilation and perfusion lung scan Chest high resolution computed
tomography Pulmonary angiography


Diagnostic Tools
CHEST RADIOGRAPHY
Central pulmonary arterial dilation with attenuation of peripheral pulmonary vasculature
Cardiomegaly , right ventricular enlargement
Help identify underlying pulmonary parenchymal disease –ILD, COPD, pulmonary vascular congestion due to left hear disease, pleural effusion

Diagnostic Tools
Low specificity & sensitivity Provides supportive evidence RVH, strain, right atrial dilation, left
atrial dilation
Electrocardiogram

Diagnostic Tools
TEE
Initial non-invasive test help screen/suggest diagnosis of PH
Identify valvular abnormalities , left atrial enlargement, myocardial abnormalities, pericardial effusion, ventricular enlargement, pressure
Congenital heart disease
Diagnostic Tools
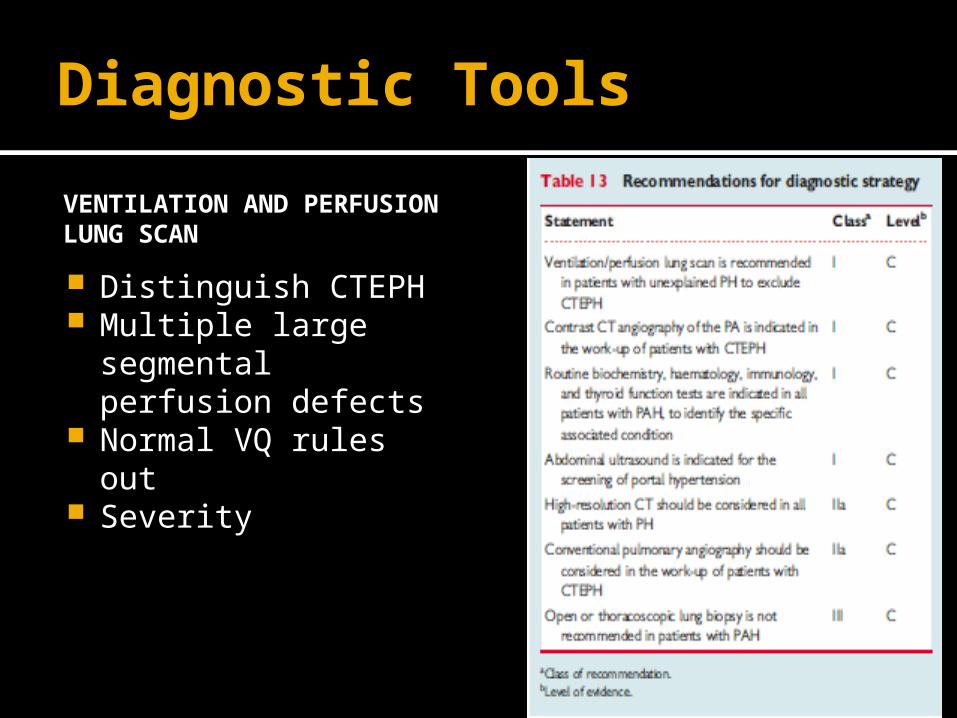
VENTILATION AND PERFUSION LUNG SCAN
Distinguish CTEPH Multiple large
segmental perfusion defects
Normal VQ rules out Severity
Diagnostic Tools
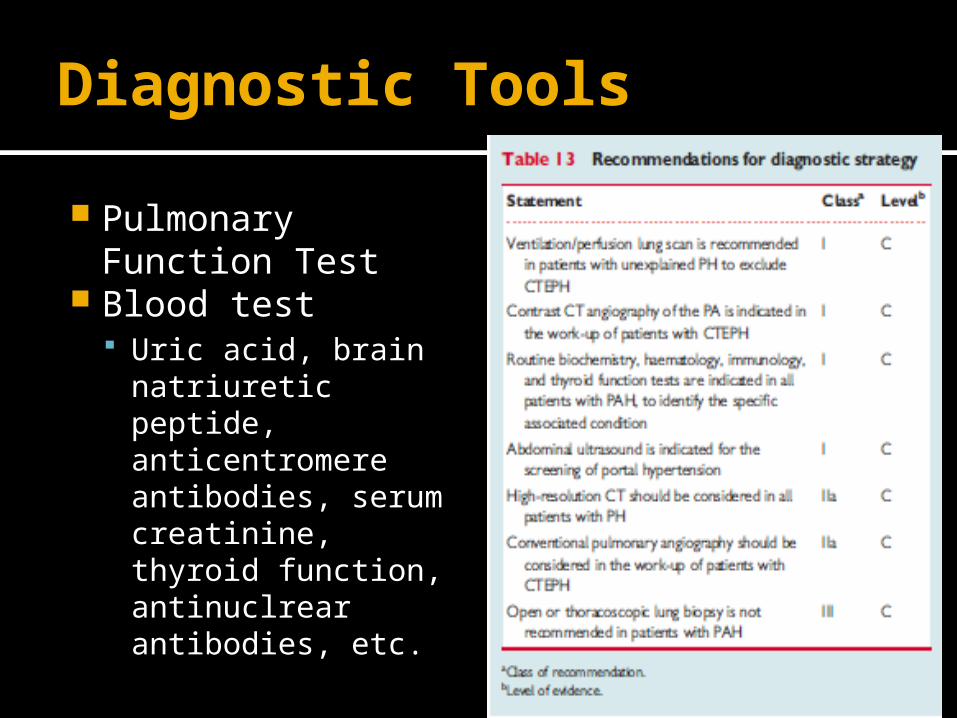
Pulmonary Function Test
Blood test Uric acid, brain
natriuretic peptide, anticentromere antibodies, serum creatinine, thyroid function, antinuclrear antibodies, etc.

AccurateDiagnosis
Determines treatment course
Group 2-5 Treat underlying
disorder Group 1 PAH
Lung disease
Chronic PE
Heart failure

Vasoreactivity with RHC
RHC Required to confirm diagnosis Assess the severity of the
hemodynamic impairment Assess vasoreactivity of the
pulmonary circulation Short acting drugs
Inhaled NO, IV epoprostenol, IV adenosine
Benefit from long-term therapy with CCB
Positive acute response is mPAP >10mmHG to reach an absolute value of MPAP <40mmHg with concurrent increased or unchanged CO
Can be treated safely with high dose CCBs Only positive reactive 95% five-year survival

Treatment in PAH
Based on vasoreactivity and functional class New York Heart Association Functional
Class▪ Class I: No symptoms with ADL▪ Class II: some symptoms with ADL, slight
limitation ▪ Class III: symptoms with less than normal
ADL, increased limitation of physical activity ▪ Class IV: symptoms with any activity, even at
rest

No Treatment
Untreated = 6months Median survival rate is 2.8 yrs
WHO FC IV 6 months WHO FC III 2.5 yrs WHO FC I and II 6 yrs▪ Scleroderma ~1yr

Prognostic Factors

Prognosis

Therapeutic Approaches
No cure Goal
Symptomatic relief Quality of improvement Survival prolongation
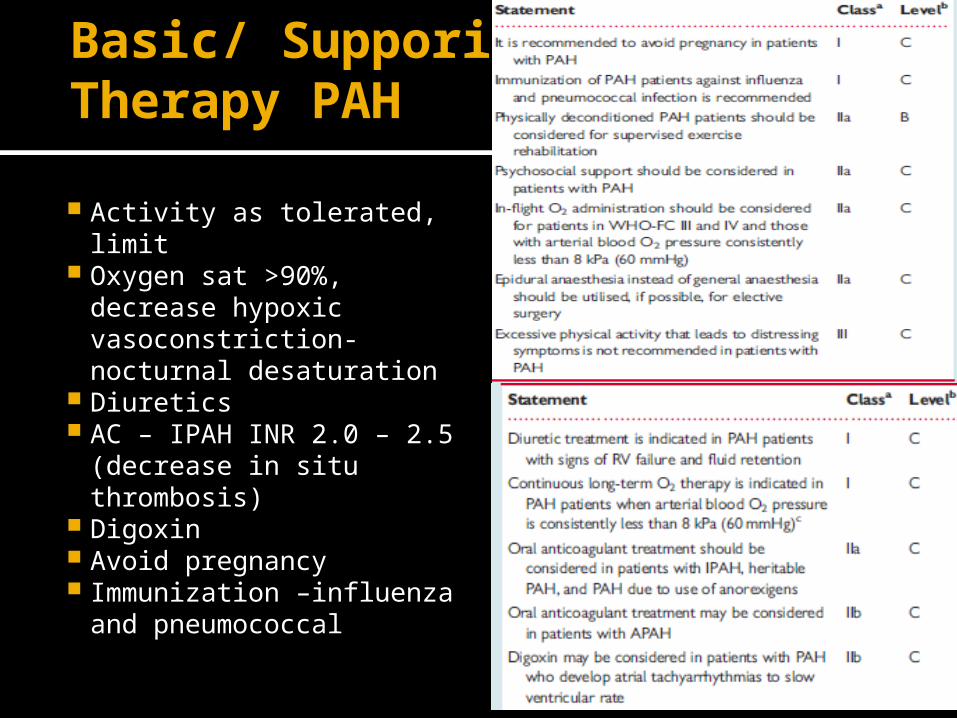
Basic/ Supporitve Therapy PAH
Activity as tolerated, limit
Oxygen sat >90%, decrease hypoxic vasoconstriction-nocturnal desaturation
Diuretics AC – IPAH INR 2.0 – 2.5
(decrease in situ thrombosis)
Digoxin Avoid pregnancy Immunization –influenza
and pneumococcal
PAH specific therapy
Medical Surgical therapy
Atrial septostomy –decrease right sided pressure, improve left sided filling pressure
Transplant
Calcium channel blockers Endothelial Receptor
Antagonists Bodentan, Sitaxsentan,
Ambirisentan Phosphodiestaerases
Inhibitors Sildeneafil, Tadalafil,
Varadenafil Prostaglandins
Epoprostenol, Treprostinil, lloprost
Guanylate cyclase stimulant -Riociguat
Treatment of PAH
CCB Pt who show response to acute vasodilator
testing at the time of RHC Nifedipine, diltiazem, amlodipine ▪ Choice depends on pt’s baseline hear rate ▪ Relative bradycardic –nifedipine and amlodipine▪ Tachycardia – diltiazem
120-240mg nifedipine 240-720mg diltiazem 20mg amlodipine
Limiting factors hypotension, LE edmea Follow up – 3-4 month RHC, change in functional class Negative vasoreactivity should not be started on CCB-severe
side effects –hypotension, syncope, RV failure

Prostanoids
Prostacyclin Developed by endothelial cells Induce potent vasodilation of all vascular beds▪ Inhibitor of platelet aggregation, antiproliferative
▪ Synthesis of stable form
▪ Epoprostenol- an infusion pump and permanent tunnelled catheter
▪ Lloprost- IV, oral and aerosol administration ▪ Treprostinil- IV, SC
Epoprostenol Synthetic prostacyclin Half life of 3-5minutes, stable at room temperature for
~8hrs Administrated an infusion pump and permanent
tunnelled catheter Start at a dose 2-4ng/kg/min and increase at a rate
limited by side effects –flushing, headache, diarrhea, leg pain
Efficacy on three unblinded RCTS in patients with IPAH and in those with PAH associated with scleroderam ▪ Have shows that it improves symptoms, exercise capacity, and
hemodynamics ▪ Only treatment shown to improve survival in IPAH

Endothelin Receptor Antagonists
Endothelin-1 has vasoconstrictive and mitogenic effects pulmonary vascular smooth muscles-endothelin-A and B receptors
Bosertan- Oral Sitaxentan Ambrisentan
Bosertan Oral Dual endothelin-A and B receptor antagonist Started at dose of 62.5 mg BID and uptitrated to 125mg BID
after 4 weeks Five RCTs –Pilot, BREATHE-1, 2, 5 and EARLY Showed improvement in exercise capacity, functional class,
hemodynamics, echocardiographic Two RCT enrolled exclusively patients with WHO-FC II or patients
with Eisenmenger’s syndrome▪ Regulatory authority approval for its use in AHO- FC II and congenital
systemic –to-pulmonary shunts and Eisenmenger’s syndrome Side effects – increase in hepatic aminotransferases 10% , dose
dependent Liver function test monthly
Phosphodiestrease Inhibitors
Vasodilation and antiproliferative effects Sildenafil- Oral Tadalafil Vardenafil

Sildenafil Oral Selective inhibitor RCT – SUPER-1▪ 278 PAH patients treated with sildenafil 20,
40, 80mg tid▪ Favorable results on exercise capacity,
symptoms ▪ Side effects – headache, flushing, epistaxis

Combination Therapy
Fail monotherapy
Some Hemodynamics, exercise capacity and functional class improved

Follow up
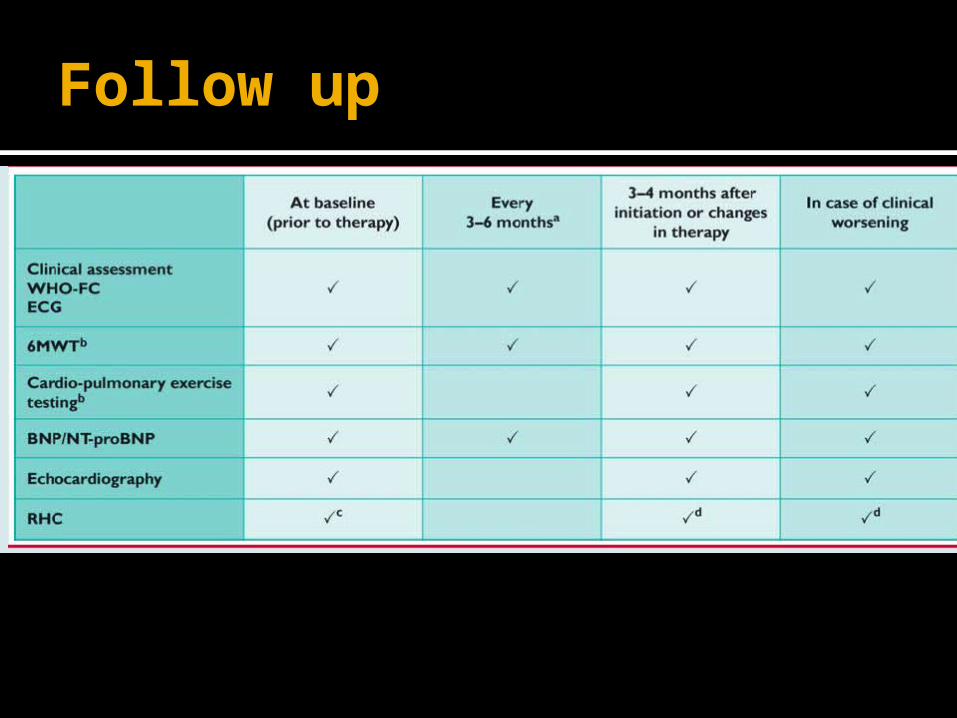
Follow up

















