CASE REPORT Pulmonary Edema Following Pulmonary Valvulotomy Rodney E. Matisonn, M.B. ,. Abdul S. Mitha, M.R.C.P. (Lond.), Mervyn A. Williams, F.R.C.S.E., and Elliot Cheder, M.D. ABSTRACT A previously unreported combination of critical pulmonary valve stenosis and mitral stenosis is described. The initial clinical presentation was one of right ventricular failure that obscured the evidence of pulmonary venous hypertension. Following pulmonary valvulotomy, pulmonary edema ensued because of the increased pulmonary blood flow. The importance of urgent cardiac catheterization postoperatively following an operation that in- creases pulmonary blood flow is discussed. T hose congenital malformations characterized by decreased pulmonary blood flow are rarely associated with an additional anomaly that obstructs pulmonary venous return. When pulmonary blood flow is substantially reduced, however, it may dominate. the clinical picture and obscure the signs of pulmonary venous obstruction. Surgical restoration of normal pul- monary blood flow may alter the hemodynamics, with the emergence of severe pulmonary venous hypertension as a postoperative complication. This paper documents this phenomenon in a patient who had right ventricu- lar failure because of critical pulmonary valve stenosis; following pulmonary valvulotomy, pulmonary edema resulted from unsuspected “tight” mitral stenosis that necessitated an additional valvulotom y. A 10-year-old African girl was admitted to the hospital with an eight-week history of congestive cardiac failure. Her symptoms were fatigue and ankle and abdominal swelling with moderate dyspnea but no orthopnea. There was no history of rheumatic fever. Her blood pressure was 110/70 mm Hg, the pulse was normal and regular From the Cardio-Thoracic Unit, Wentworth Hospital, and the University of Natal, Durban, South Supported by a grant from the Medical Research Council of South Africa. Accepted for publication Mar. 12, 1975. Address reprint requests to Dr. Matisonn, Cardiac Unit, Wentworth Hospital, P. B. Jacobs, Natal Africa. 4026, South Africa. VOL. 20, NO. 5, NOVEMBER, 1975 581
Transcript
CASE REPORT
Pulmonary Edema Following Pulmonary Valvulotomy Rodney E. Matisonn, M.B. ,. Abdul S. Mitha, M.R.C.P. (Lond.), Mervyn A. Williams, F.R.C.S.E., and Elliot Cheder, M.D.
ABSTRACT A previously unreported combination of critical pulmonary valve stenosis and mitral stenosis is described. The initial clinical presentation was one of right ventricular failure that obscured the evidence of pulmonary venous hypertension. Following pulmonary valvulotomy, pulmonary edema ensued because of the increased pulmonary blood flow. The importance of urgent cardiac catheterization postoperatively following an operation that in- creases pulmonary blood flow is discussed.
T hose congenital malformations characterized by decreased pulmonary blood flow are rarely associated with an additional anomaly that obstructs pulmonary venous return. When pulmonary blood flow is
substantially reduced, however, it may dominate. the clinical picture and obscure the signs of pulmonary venous obstruction. Surgical restoration of normal pul- monary blood flow may alter the hemodynamics, with the emergence of severe pulmonary venous hypertension as a postoperative complication.
This paper documents this phenomenon in a patient who had right ventricu- lar failure because of critical pulmonary valve stenosis; following pulmonary valvulotomy, pulmonary edema resulted from unsuspected “tight” mitral stenosis that necessitated an additional valvulotom y.
A 10-year-old African girl was admitted to the hospital with an eight-week history of congestive cardiac failure. Her symptoms were fatigue and ankle and abdominal swelling with moderate dyspnea but no orthopnea. There was no history of rheumatic fever.
Her blood pressure was 110/70 mm Hg, the pulse was normal and regular
From the Cardio-Thoracic Unit, Wentworth Hospital, and the University of Natal, Durban, South
Supported by a grant from the Medical Research Council of South Africa. Accepted for publication Mar. 12, 1975. Address reprint requests to Dr. Matisonn, Cardiac Unit, Wentworth Hospital, P. B. Jacobs, Natal
Africa.
4026, South Africa.
VOL. 20, NO. 5, NOVEMBER, 1975 581
MATISONN ET AL.
with a rate of 100 per minute; the jugular venous pressure was raised to the angle of the jaw with prominent “CV” waves. The abdomen was distended because of ascites, and the liver was palpable 4 cm below the right costal margin. There was a hyperdynamic right ventricular impulse. Auscultation revealed severe pulmonary stenosis and tricuspid insufficiency. A grade 4/6 long ejection systolic murmur in the second left interspace extended beyond the aortic component of the second heart sound; the pulmonary component was inaudible. A pansystolic murmur that increased with inspiration was present at the left sternal border and epigas- trium.
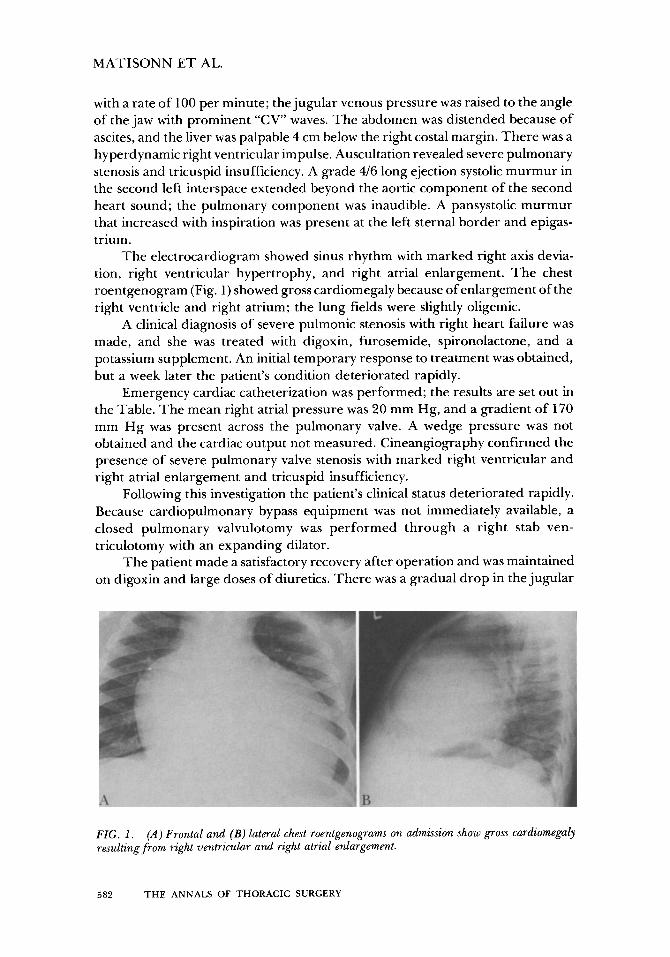
The electrocardiogram showed sinus rhythm with marked right axis devia- tion, right ventricular hypertrophy, and right atrial enlargement. The chest roentgenogram (Fig. 1) showed gross cardiomegaly because of enlargement of the right ventricle and right atrium; the lung fields were slightly oligemic.
A clinical diagnosis of severe pulmonic stenosis with right heart failure was made, and she was treated with digoxin, furosemide, spironolactone, and a potassium supplement. An initial temporary response to treatment was obtained, but a week later the patient’s condition deteriorated rapidly.
Emergency cardiac catheterization was performed; the results are set out in the Table. The mean right atrial pressure was 20 mm Hg, and a gradient of 170 mm Hg was present across the pulmonary valve. A wedge pressure was not obtained and the cardiac output not measured. Cineangiography confirmed the presence of severe pulmonary valve stenosis with marked right ventricular and right atrial enlargement and tricuspid insufficiency.
Following this investigation the patient’s clinical status deteriorated rapidly. Because cardiopulmonary bypass equipment was not immediately available, a closed pulmonary valvulotomy was performed through a right stab ven- triculotomy with an expanding dilator.
The patient made a satisfactory recovery after operation and was maintained on digoxin and large doses of diuretics. There was a gradual drop in the jugular
FIG. I . resulting from right ventricular and right atrial enlargement.
(A) Frontal and (B) lateral chest roentgenograms on admission show gross cardiomegaly
Pulm. art. Brachial art. Pulm. capillary Left ventricle . . . . . . Left ventricle to aorta . . . . . .
. . . . . . 1
a = 23, x = 17 - v = 25, y = 18 (20)
194/6 - 22
112/63 24/12 (rn)
. . .
. . .
. . .
. . . a = 8 , x = 1 - (4) v = 3, y = 2.
110/0-4 40/20 (%) 1 10/60 (22) 106/0-8 106/0-8 to 106/60
venous pressure with recession in liver size, and the murmur of tricuspid insuffi- ciency disappeared. A chest roentgenogram showed a gradual reduction in heart size. Ten days after operation the patient complained of dyspnea and orthopnea, and this was followed by several attacks of subacute pulmonary edema over a period of three weeks. At that time it was noticed that a middiastolic rumbling murmur was present at the apex. The chest roentgenogram showed considerable reduction in heart size, but the left atrium was now prominent and the pulmonary veins appeared cdngested (Fig. 2).
Left atrial enlargement was confirmed electrocardiographically, and cardiac catheterization was repeated. The mean right atrial pressure was 4 mm Hg, and a residual gradient of 70 mm Hg was present across the pulmonary valve. The pulmonary artery pressure was 40/20 mm Hg (mean, 26) and the mean wedge
FIG. 2. (A) Frontal and (B) lateral chest roentgenograms following emergency pulmonary val- vulotomy. The right ventricular and right atrial enlargement has regressed, but left atrial enlargement is evident in the lateral view. Pulmonary congestion is present.
VOL. 20, NO. 5, NOVEMBER, 1975 583
MATISONN ET AL.
pressure was 22 mm Hg; a mean diastolic gradient of 12 mm Hg was found across the mitral valve. The cardiac index was 2.6 liters per minute per square meter of body surface area, and the mitral valve area was calculated by the Gorlin formula to be 0.63 cm2.
Right ventricular cineangiography showed normal ventricular contractility and a thickened pulmonary valve. Follow-through opacification of the left atrium demonstrated slowing of contrast material at the level of the mitral valve. There was no evidence suggestive of cor triatriatum, supravalvular stenosing ring, or anomalous connection of the pulmonary veins.
An elective operation was undertaken using cardiopulmonary bypass. In- spection of the pulmonary valve through the pulmonary artery revealed incom- plete valvulotomy of a congenital bicuspid valve; the valve was fully split by incision of the commissures. The pulmonary arteriotomy was closed and the left atrium then opened. The presence of tight mitral stenosis was confirmed, and a complete valvulotomy was performed using an expanding dilator.
The patient made an uneventful recovery and was discharged from the hospital two weeks later.
Comment The combination of mitral and pulmonary valve stenosis in the absence of
evidence of organic aortic or tricuspid valve involvement has been reported only once before to our knowledge. In the case described by McCredie and Richards [3] the clinical presentation was one of tight mitral stenosis, and a gradient of 46 mm Hg across the pulmonary valve was an unexpected finding at cardiac catheteriza- tion. At operation the pulmonary valve was found to be tricuspid, stenosed to a moderately severe degree, and lightly calcified. Although rheumatic involvement of the pulmonary valve is uncommon, it may have been the cause [6]. In our patient the pulmonary valve was congenitally bicuspid and not calcified, whereas the mitral valve had the typical appearance of rheumatic involvement. It is possible, however, that both lesions were congenital, since pathologically some cases of congenital mitral stenosis are indistinguishable from rheumatic involve- ment [2].
Our patient demonstrates how conditions characterized by decreased pul- monary flow may obscure an additional anomaly that is obstructing pulmonary venous return. Anomalies such as cor triatriatum, supravalvular stenosing ring of the left atrium, mitral atresia, and total infradiaphragmatic venous drainage could be obscured by tetralogy of Fallot or severe pulmonic stenosis. Fortunately, those conditions which obstruct pulmonary blood flow are rarely associated with tetral- ogy of Fallot. Recently, however, Muster and co-workers [51 described 2 small infants with the rare combination of tetralogy of Fallot and total anomalous pulmonary venous drainage. Both patients died when systemic-to-pulmonary artery shunts were performed as palliative procedures; intractable pulmonary edema resulted from a precipitous rise in pulmonary venous pressure. These authors made the point that when pulmonary edema is encountered under such
584 THE ANNALS OF THORACIC SURGERY
CASE REPORT: Pulmonary Edema after Valvulotmy
circumstances, prompt cardiac catheterization is indicated in order to assess the size of the shunt and the degree of pulmonary venous hypertension.
In our patient the reduction in pulmonary blood flow was a consequence of right ventricular failure because of severe pulmonary stenosis. Pulmonary edema was slower to develop because of gradual improvement in right ventricular func- tion and increase in cardiac output. The detection of a middiastolic murmur led to cardiac catheterization, whereupon the correct diagnosis was made. Prior to this, the possibility of left ventricular dysfunction concurrent with and resulting from right ventricular disease had been entertained as a cause of the pulmonary edema. In a recent editorial reviewing this problem, Weisse [71 pointed out that in the absence of systemic hypertension and coronary artery disease, left ventricular dysfunction is most probably a result of coincident cardiomyopathy. This observa- tion is in keeping with our experience: we have documented left ventricular failure with tetralogy of Fallot and mild pulmonary stenosis in the African popula- tion, in whom nutritional or alcoholic cardiomyopathy constitutes the most com- mon form of heart disease [ 1,4]. Differentiation between a lesion that obstructs pulmonary venous return and myopathic left ventricular failure can best be accomplished by cardiac catheterization under these circumstances.
References 1. Cheder, E., Beck, W., and Schrire, V.
81:321, 1971. 2. Edwards, J. E., Carey, L. S., Neufeld, H. W., and Lester, R. G.
Philadelphia and London: Saunders, 1965. 3. McCredie, R. M., and Richards, J. G.
Br Heart J 28: 139, 1966. 4. Mitha, A. S., Matisonn, R. E., and Cheder, E.
myocardial function. S Afr Med J 49:229, 1975. 5. Muster, A. J., Paul, M. H., and Nikaidoh, H.
anomalous pulmonary venous drainage. Chest 64:323, 1973. 6. Schwartz, S. P., and Shelling, D.
ciency. Am Heart J 6:569, 1931. 7. Weisse, A. B.
or right chambers of the heart. Am Heart J 87:654, 1974.
Tetralogy of Fallot and heart failure.Am HeurtJ
CongenitulHeurtDiseclse.
Combined mitral and pulmonary valve stenosis.
Pulmonary stenosis and impaired
Tetralogy of Fallot associated with total
Acquired rheumatic pulmonic stenosis and insuffi-
Contralateral effects of cardiac disease affecting primarily either the left