British Journal of Haematology. 1990, 76, 494-500 Purification and characterization of a pi class glutathione S-transferase from human leukaemic cells ANDREW HALL, SALLY FOSTER, STEPHEN J. PROCTOR AND ALEX R. CATTAN University Departinent of Haernatology, Leukaeniia Research Fund Remission Unit. Medical School, University of Newcastle upon Tyne, Framlington Place. Newcastle upon Tyne Received 22 May 1990; accepted for publication 9 August 1990 Summary. The glutathione S-transferases are a group of enzymes involved in the detoxification of a wide range of xenobiotics. Elevation of the level of activity of glutathione S- transferases within the cytosol has been associated with the development of resistance to a number of cytotoxic drugs, including some commonly used in the treatment of leukae- mia. In this paper we describe the purification and characteri- zation of an anionic (p class) form of the enzyme from the peripheral blood of patients with acute myeloid leukaemia, chronic myeloid leukaemia, and acute lymphocytic leukae- mia and the spleen of a patient with chronic lymphocytic leukaemia. We present evidence that the form of enzyme purified closely resembles pi class glutathione S-transferase purified from human placenta. Immunoblotting performed on cytosol from the leukaemic cells from a range of cases of leukaemia at presentation, or on treatment, demonstrated that this form of glutathione S-transferase was the predomin- ant isoenzyme expressed in all cases studied. However, in the limited number of cases studied there was no correlation between the level of expression and response to chemo- therapy, suggesting that increased expression of pi class GST is not the sole cause of resistance to bifunctional alkylating agent in human leukaemias. Many patients with leukaemia show an initial response to treatment with cytotoxic drugs, followed by a variable period of apparent remission, before relapse occurs with a form of the disease unresponsive to retreatment with agents used in the induction regime. This may be due either to the development of secondary drug resistance, or to the emer- gence of resistant clones of cells present at the onset of treatment. A wide range of reports have suggested that the biochemical mechanisms underlying this process may oper- ate at any one of three levels (Hall et al, 1989b).Firstly, there may be alterations in the cell membrane, with decreased drug uptake or increased efflux, resulting in the lowering of intracellular drug concentrations. Secondly, changes may occur within the cytosol, with decreased drug activation or increased detoxification of a drug, or its metabolites. Lastly, modifications may occur within the nucleus, resulting in, for example, increased DNA repair, which has the effect of mitigating the otherwise lethal effects of cytotoxic agents. One mechanism which has been identified as a possible cause of resistance to a range of cytotoxic drugs, both in isolation, or in conjunction with other biochemical altera- tions, is elevation of the activity of members of a group of Correspondence: Dr A. G. Hall, Leukaemia Research Fund Remission Unit, MMBG, Fourth Floor, Medical School, IJniversity of Newcastle upon Tyne. Framlington Place. Newcastle upon Tyne NE2 4HH. enzymes classified as the glutathione S-transferases (GSTs) (Buller et al. 1987; Robson et nl, 1987). The cytosolicforms of GST are a multigene family ofdimeric proteins with a wide range of substrate activities.They may be divided into three main groups on the basis of their isoelectric points, enzymic properties and immunological reactivity (Boyer. 1989; Mannervik, 1985).Members of the pi class of GSTs have been identified in a variety of normal tissues including placenta (Dao et al, 1984). lymphocytes (Joneset it/, 1988),platelets (Loscalzo&Freedman. 1986) and a range of human tumours (Shea et al. 1988).Alpha class GSTs are the predominant type expressed in hepatocytes (Hayes et 01. 1989). and are also found in some other tissues, including the kidney (Harrison et al, 1989). The mu forms of the enzyme have been detected in liver (Warholm et al. 1983)and normal leucocytes (Hussey et nl, 1987),but appear to be expressed in only about 5 5% of the population (Strange et al. 1984). The normal function of these enzymes is believed to be the detoxification of a wide range of xenobiotics and the intracel- Mar binding of toxic products of metabolism such as bilirubin (Kamisaka et a/, 1975). h vitra studies have suggested that expression of GSTs within tumour cells may lead to enhanced resistance to a range ofcytotoxic drugs. including several used routinely in the treatment of patients with haematological malignancies. These include chlorambucil (Robson et (11, 19871, melphalan (Gupta et al, 1989)and adriamycin (Ratist 494
Transcript
British Journal of Haematology. 1990, 76, 494-500
Purification and characterization of a pi class glutathione S-transferase from human leukaemic cells
ANDREW HALL, SALLY FOSTER, STEPHEN J. PROCTOR AND ALEX R. CATTAN University Departinent of Haernatology, Leukaeniia Research Fund Remission Unit. Medical School, University of Newcastle upon Tyne, Framlington Place. Newcastle upon Tyne
Received 22 May 1990; accepted for publication 9 August 1990
Summary. The glutathione S-transferases are a group of enzymes involved in the detoxification of a wide range of xenobiotics. Elevation of the level of activity of glutathione S- transferases within the cytosol has been associated with the development of resistance to a number of cytotoxic drugs, including some commonly used in the treatment of leukae- mia. In this paper we describe the purification and characteri- zation of an anionic (p class) form of the enzyme from the peripheral blood of patients with acute myeloid leukaemia, chronic myeloid leukaemia, and acute lymphocytic leukae- mia and the spleen of a patient with chronic lymphocytic leukaemia. We present evidence that the form of enzyme
purified closely resembles pi class glutathione S-transferase purified from human placenta. Immunoblotting performed on cytosol from the leukaemic cells from a range of cases of leukaemia at presentation, or on treatment, demonstrated that this form of glutathione S-transferase was the predomin- ant isoenzyme expressed in all cases studied. However, in the limited number of cases studied there was no correlation between the level of expression and response to chemo- therapy, suggesting that increased expression of pi class GST is not the sole cause of resistance to bifunctional alkylating agent in human leukaemias.
Many patients with leukaemia show an initial response to treatment with cytotoxic drugs, followed by a variable period of apparent remission, before relapse occurs with a form of the disease unresponsive to retreatment with agents used in the induction regime. This may be due either to the development of secondary drug resistance, or to the emer- gence of resistant clones of cells present at the onset of treatment. A wide range of reports have suggested that the biochemical mechanisms underlying this process may oper- ate at any one of three levels (Hall et al, 1989b). Firstly, there may be alterations in the cell membrane, with decreased drug uptake or increased efflux, resulting in the lowering of intracellular drug concentrations. Secondly, changes may occur within the cytosol, with decreased drug activation or increased detoxification of a drug, or its metabolites. Lastly, modifications may occur within the nucleus, resulting in, for example, increased DNA repair, which has the effect of mitigating the otherwise lethal effects of cytotoxic agents.
One mechanism which has been identified as a possible cause of resistance to a range of cytotoxic drugs, both in isolation, or in conjunction with other biochemical altera- tions, is elevation of the activity of members of a group of
Correspondence: Dr A. G. Hall, Leukaemia Research Fund Remission Uni t , MMBG, Fourth Floor, Medical School, IJniversity of Newcastle upon Tyne. Framlington Place. Newcastle upon Tyne NE2 4HH.
enzymes classified as the glutathione S-transferases (GSTs) (Buller et al. 1987; Robson et nl, 1987).
The cytosolic forms of GST are a multigene family ofdimeric proteins with a wide range of substrate activities. They may be divided into three main groups on the basis of their isoelectric points, enzymic properties and immunological reactivity (Boyer. 1989; Mannervik, 1985). Members of the pi class of GSTs have been identified in a variety of normal tissues including placenta (Dao et al, 1984). lymphocytes (Joneset it/,
1988), platelets (Loscalzo &Freedman. 1986) and a range of human tumours (Shea et al. 1988). Alpha class GSTs are the predominant type expressed in hepatocytes (Hayes et 01. 1989). and are also found in some other tissues, including the kidney (Harrison et al, 1989). The mu forms of the enzyme have been detected in liver (Warholm et al. 1983) and normal leucocytes (Hussey et nl, 198 7), but appear to be expressed in only about 5 5% of the population (Strange et al. 1984).
The normal function of these enzymes is believed to be the detoxification of a wide range of xenobiotics and the intracel- Mar binding of toxic products of metabolism such as bilirubin (Kamisaka et a/, 1975). h vitra studies have suggested that expression of GSTs within tumour cells may lead to enhanced resistance to a range ofcytotoxic drugs. including several used routinely in the treatment of patients with haematological malignancies. These include chlorambucil (Robson et (11, 19871, melphalan (Gupta et al, 1989) and adriamycin (Ratist
494
Glutathiorie S-Transferuse f rom Leiikaernic Cells 49 5 et ( I / . 1986 ). GSTs may confer resistance by either direct or indirect actions. Direct detoxification may occur by the catalysis of the conjugation of glutathione to the active site(s) of a drug or its metabolites (Dulik et a l , 1986). Alternatively protection may be provided indirectly through the detoxifica- tion of reactive intermediates, for example free radicals, produced by drug interactions within the cell (Batist et al, 1986).
Most studies of drug resistance mechanisms have concen- trated on the use of it1 vitro model systems, using cell lines selected by chronic exposure to cytotoxic agents. Compara- tively little is known of the relevance of these models to the occurrence ofdrug resistance it1 vivo in either solid tumours or haematological malignancies. In this paper we describe the purification and characterization of a form of GST from leukaeinic cells which appears to be identical, or closely related. to the pi class enzyme isolated from human placenta. We also show that this is the predominant form of the enzyme in the leukaemic cell population of a range of patients with acute lymphocytic leukaemia (ALL), acute myeloid leukaemia (AMI,) and chronic myeloid leukaemia (CML) both at presen- tation and on relapse. Similar results were also obtained using cells obtained from patients with chronic lymphocytic leukae- mia (C1,L). either a t presentation or maintained on standard treatment with chlorambucil and prednisolone.
MATERIALS AND METHODS
Materials. Epoxy-activated Sepharose 6B was purchased from Pharmacia (Milton Keynes, U.K.). All other chemicals were obtained from Sigma (Poole, U.K.) unless otherwise stated, and were of the highest grade available.
Cell preparation. For the purification of cytosolic GST. cells were obtained from the peripheral blood of patients with AIJ,. AML and CML. The spleen was used as a source of cells in the case of CLL. Details of the samples used for the purification of GST are given in Table I. At the time of sampling no patient had received any treatment with chemotherapeutic drugs.
Mononuclear cells from peripheral blood were isolated by density gradient centrifugation using Lymphoprep (Nycomed. Birmingham, U.K.). Cells were washed twice in Dulbecco's phosphate-buffered saline, pH 7.4. and stored as a pellet at -20°C prior to purification as described below. Cytospin preparations of the washed cells showed that greater than 90%) of nucleated cells obtained by this pro- cedure belonged to the leukaemic cell population, and that there was minimal red cell contamination.
A similar procedure was used in the preparation of cell pellets from a range of patients with acute and chronic forms
Table 1. Samples used for the purification of GST
Patient Diagnosis Age Sex Sample
1 AML 58 F Peripheral blood
3 CLL 42 M Spleen 4 ALL 75 M Peripheral blood
7 I CML 30 M Peripheral blood
of leukaemia. subsequently used for the immunoblotting of crude lysates. Details of the patients studied are given in Table 11.
The spleen from patient 3 was frozen at - 20°C within 2 h of its surgical removal. Histology revealed that greater than 90% of cells present were of lymphoid origin.
Purification of GST. ( i ) Purification of GSTfroni leukaernic cells arid placenta. All procedures were performed at 4°C. Cell pellets from patients 1, 2 and 4 were homogenized by sonication in 10 mM tris/HCl, pH 7.8, containing 1.4 mM 2- mercaptoethanol and 1 mM EDTA (buffer A). The lysates were centrifuged at 43 000 g for 20 min and the supernatant passed over a 6 .4 ml column of S-hexyl glutathione sephar- ose affinity gel, prepared as previously described (Mannervik & Guthenberg, 1981). The column was washed extensively with buffer A containing 0.2 M NaCl (buffer B). GST was eluted from the affinity matrix using a linear gradient of 0-1 mM S-hexylglutathione in buffer B. Fractions were collected and the enzyme activity against the model substrate 1- chloro-2,4-dinitrobenzene (CDNB) was assessed using a previously described assay (Habig & Jakoby. 1 9 8 1) adapted for use on a multichannel plate reading spectrophotonieter.
Purification of GST from the spleen of patient 3 used essentially the same procedure. Tissue (220 g) was homogen- ized in 800 ml of buffer A containing 0.2 5 M sucrose, using a Waring blender. The homogenate was centrifuged at 2000 g for 20 min followed by centrifugation of the supernatant a t 43 000 g for 20 min. The resulting cytosolic fraction was passed over a 34 ml column of S-hexylglutathione affinity gel. After extensive washing with buffer B. GST was eluted using a 0-1 mM gradient of S-hexylglutathione. Fractions were collected and enzyme activity assessed as described above. GST was purified from full-term human placenta using a similar protocol.
For the production of antisera. GST from the spleen of patient 3 was purified to homogeneity using a Mono Q anion exchange column (Pharmacia, Milton Keynes, U.K.). Active fractions were eluted using a 0-1 M linear gradient of sodium chloride in buffer B.
( i i ) Purification of alpha and ti111 class GSTfroni hunian liver. Alpha and mu class GST, used for the preparation of antisera. were purified from liver obtained at post-mortem. The initial purification steps were essentially as described above for the purification of GST from spleen and placenta, except that the cytosol was centrifuged at 100000 g for 6 0 min to allow removal of lipid by partition. Elution of GST bound to the S- hexylglutathione affinity column using a S-hexylglutathione gradient was found to give partial separation of alpha and mu forms as previously described (Hayes et nl. 1987). Active fractions containing either predominantly alpha or mu enzymes were mixed with a n equal volume of 2 M ammo- nium sulphate and then loaded onto a phenyl superose column (Pharmacia). Alpha class GST was found not to bind at this ionic strength. Mu class GST was eluted using 2 0 mM tris-HC1, pH 7.4, 1 mM EDTA. 1.4 mM 2-mercaptoethanol.
Sodium dodrcul sulphate polgacrylatiiide gel electrophoresis (SDS-PAGE). SDS-PAGE was performed (Laemmli. 1 9 70) using 1 3% polyacrylamide in the running gel. Protein bands were stained using Coomassie blue.
496 Andrew HaIl et a1 Table 11. Details of the patients studied
Patient Diagnosis Age Sex Stage’ Sample2
A
B
C
D
E
F
H I
J K L M N 0
P
v
R
‘r
V
ALL
ALL
ALL
ALL
ALL
ALL
CLL CLL
CLL CLL CLL CLL CML CMML
CML
CMML
AML
AML
AML
18
26
54
19
27
41
56 58
64 65 59 65 28 5 3
3
42
21
62
2 1
M P
M P
F P
M P
M P
M R
F M F R
M M M P M M M M M P M P
F P
M P
M P
M P
M R
__ PB
PB
PB
PB
PB
PB
PB PB
PB PB PB PB PB PB
PB
PB
BM
BM
PB
Response to treatment3 Relative GST4
Responded to standard induction therapy5. Auto BMT at 6 months. Relapse after 24 months. Only temporary response to re-induction. Died 28 months post diagnosis. Responded to standard induction therapy. Auto BMT at 6 months. Remains disease-free 24 months post diagnosis. Responded to standard induction therapy, but CNS relapse at 3 months, unresponsive to further treatment. Responded to standard induction therapy. A110 BMT at 6 months. Remains disease-free at 12 months. Responded to standard induction therapy. Auto BMT at 6 months. Remains disease-free at 20 months. Responded to standard induction therapy. Auto BMT at 6 months. Relapse at 9 months (time of sample). Achieved second remission using vinc, adr. cyto and pred, hut further relapse and death at 11 months. Partial response to chl and pred. No response to chl. pred, cyclo, vinc. hydrox. interferon, oxy, etop. adr. tamoxifen. busulphan. Controlled to 8 yr on chl and pred. Responded to chl and pred: remains controlled after 30 months. Controlled for 3 yr on chl and pred. Controlled for 2 yr on chl and pred. Responded to busulphan. In chronic phase. Presented in transformation to acute leukaemia. Only partial response to chemotherapy. Died after 1 month. Responded to busulphan and pred. In chronic phase 27 months post diagno- sis. Controlled using interferon. bleomycin. VPI 6 and tenoposide. Eventual CNS and marrow relapse 12 months post diagnosis. Only partial response to dnr. cyto, etop. and MAMSA. Died 12 months post diagnosis. Responded to induction chemotherapy using mitoxantrone and cyto. but died 2 months post diagnosis with marrow aplasia. Initial response to dnr, cyto and thioguanine. MAMSA. etop and thioguanine. MAMSA. etop and mitoxantrone. but relapse (this sample) and death after 6 months.
3
1 7
7 I
6
3
11 16
17 16
h
24 14 1 5
4
1 5
3
I2
29
Presentation (P). maintenance (M) or relapse (R). Peripheral blood (PB) or bone marrow (BM). ’ Abbreviations used: pred = prednisolone. vinc = vincristine. adr = adriamycin. cyto = cytosine arabinoside. chl = chloramhuci1, asp = asparagi-
nase, mtx = methotrexate, dnr = daunorubicin, auto BMT = autologous bone marrow transplant, allo BMT = allogeneic hone marrow transplant, CNS = central nervous system, cyclo = cyclophosphamide, hydrox = hydroxyurea, oxy = oxymethalone. etop = etoposide.
Calculated from densitometry of the immuno blots, using purified pi-class GST as a standard. Standard induction therapy=pred, vinc, adr. cyto, 6-mercaptopurine, asp, mtx.
Prepnrntion of antiserum. Polyclonal antisera to purified pi class GST from the spleen of patient 3 , and alpha and mu forms from human liver. were raised in male New Zealand white rabbits. The antigens used were judged to be homo- geneous by both SDS-PAGE and isoelectric focusing prior to immunization. Protein (1 50-200 pg) was injected into the hind quarter intramuscularly on each occasion, initially with Freund’s complete adjuvant. Subsequent monthly injections used Freund’s incomplete adjuvant. Antisera specificity and titre were assessed using an enzyme-linked immunosorbant assay (ELISA) technique.
Isoelectric forming. Flat bed isoelectric focusing was per-
formed in ultra-thin gels using an adaption of the method of Radola (1 980). Protein bands were stained using Coomassie blue.
GST activity against model siibstrntes. GST activity against CDNB and ethacrynic acid was assessed using a standard dual beam spectrophotometer (Habig & Jakoby, 1981 1. Protein concentration was assessed using a dye assay (Bradford, 1976). adapted for use on a multichannel plate reading spectrometer. Bovine serum albumen was used as a control.
Irnrnunoblotting. Cell pellets were homogenized in buffer A , followed by centrifugation at 13 000 rpm for 5 min in a
Glutathione S-Transferase frorri Leukaemic Cells 49 7 give a final dilution of 1 : 1000. Incubation was continued at room temperature for 4 h with gentle agitation. The sheet was then washed three times in TBS/Tween and then incubated for 4 h with 18 5 kBq of 1251-protein A (Amersham, Aylesbury, U.K.). After extensive washing with TBS/Tween, the filter was dried under vacuum before autoradiography at - 80°C for 16 h using intensifying screens. Immunoblots were assessed by densitometry using an image analyser (Joyce Loebl Magiscan). Duplicate cell pellets were processed in some cases to assess the reproducibility of the results obtained.
microfuge to remove insoluble cell debris. Protein concentra- tions in the supernatants were measured using the Bradford technique, and adjusted to give an equal loading of 1 mg/ml in each sample. SDS-PAGE was performed as described above. Proteins were transferred onto nitrocellulose filter paper (Towbin et al, 1979) and the nitrocellulose sheet was washed five times in tris-buffered saline containing 0.5% Tween 20 (TBS/Tween). After 1 h, antisera was added to the buffer to
Fig 1. SDS-PAGE of GST purified from patients 1-4 (lanes 2-51 and placenta (lane 1). Lanes marked St are molecular weight standards. Figures in the margin represent relative molecular weight in kilodaltons.
RESULTS Purification of GST One-step purification of cytosol obtained from the leukaemic
Table 111. Enzyme activity of purified GST
Enxyme activity
Substrate Placenta Liver Spleen'
CDNB 84*7? 2 1 7 f 2 1 551 f 56 Ethacrynic acid 1.32 f0 .07 ' 0 . 0 8 i ~ 0 . 0 2 2.30+04)7
GST purified from the spleen of patient 3. Units/mg +SE. One unit is defined as the amount of enzyme
required to conjugate 1 pnol of substrate per minute. Figures represent the mean of three independent measurements.
Fig 2. Isoelectric focussing (IEF) of purified GST. Lane 1 contains a mixture of mu and alpha class enzymes purified from human liver. Lane 2 contains pi class GST purified from the spleen of patient 3 , using affinity chromatography. Lane 3 contains pi class GST from patient 3 , further purified using anion exchange chromatography. Lane 4 contains pi class GST from human placenta. The figures in the margin represent the pH in the gel calculated from IEF markers.
Fig 3 . Immunoblot of purified GST. Samples were diluted 1 : 5 0 in sample buffer prior to SDS-PACE. Lane 1 is from placenta: lanes 2-5 are from patients 1-4.
498 Andrew Hall et a1
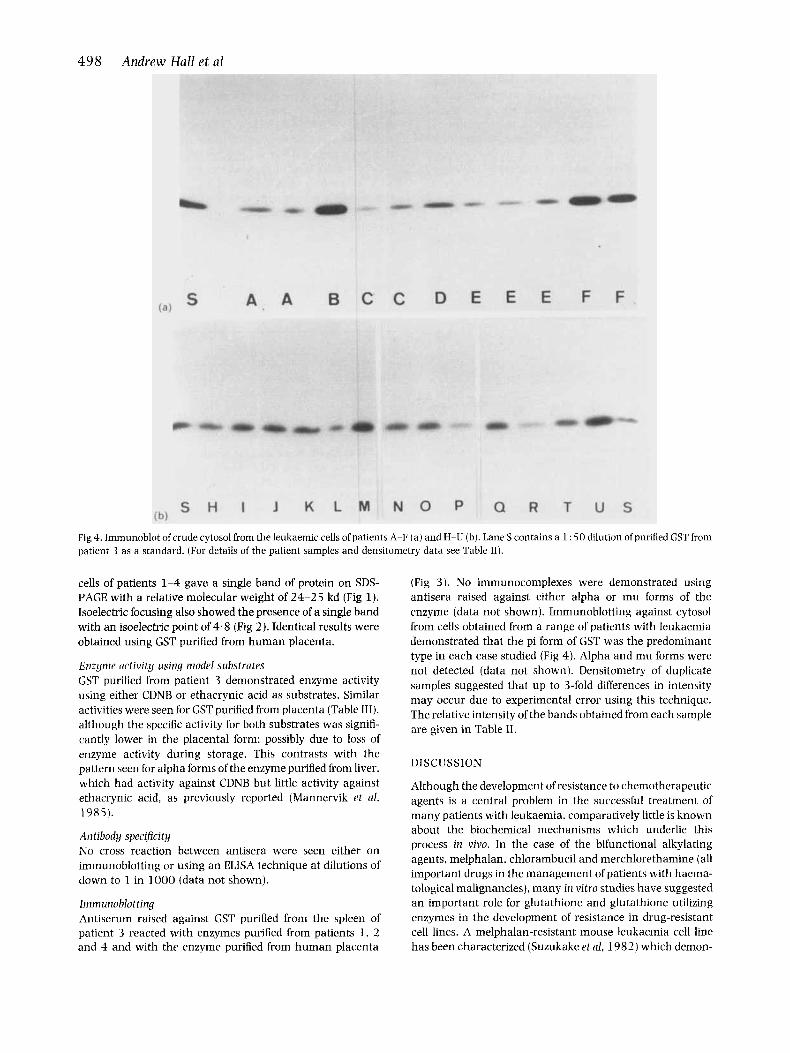
Fig 4. Immunoblot of crude cytosol from the leukaemic cells of patients A-F ( a ) and H-U (b). Lane S contains a 1 : 5 0 dilution of purified GST from patient 3 as a standard. (For details of the patient samples and densitometry data see Table 11).
cells of patients 1-4 gave a single band of protein on SDS- PAGE with a relative molecular weight of 24-25 kd (Fig 1). Isoelectric focusing also showed the presence of a single band with an isoelectric point of 4.8 (Fig 2). Identical results were obtained using GST purified from human placenta.
Enzyine activity using model substrates GST purified from patient 3 demonstrated enzyme activity using either CDNB or ethacrynic acid as substrates. Similar activities were seen for GST purified from placenta (Table III), although the specific activity for both substrates was signifi- cantly lower in the placental form: possibly due to loss of enzyme activity during storage. This contrasts with the pattern seen for alpha forms of the enzyme purified from liver, which had activity against CDNB but little activity against ethacrynic acid, as previously reported (Mannervik et al, 1985).
Antibody specificity No cross reaction between antisera were seen either on immunoblotting or using an ELISA technique at dilutions of down to 1 in 1000 (data not shown).
Imniunoblotting Antiserum raised against GST purified from the spleen of patient 3 reacted with enzymes purified from patients I , 2 and 4 and with the enzyme purified from human placenta
(Fig 3 ) . No immunocomplexes were demonstrated using antisera raised against either alpha or mu forms of the enzyme (data not shown). Immunoblotting against cytosol from cells obtained from a range of patients with leukaemia demonstrated that the pi form of GST was the predominant type in each case studied (Fig 4). Alpha and mu forms were not detected (data not shown). Densitometry of duplicate samples suggested that up to 3-fold differences in intensity may occur due to experimental error using this technique. The relative intensity of the bands obtained from each sample are given in Table 11.
DISCUSSION
Although the development of resistance to chemotherapeutic agents is a central problem in the successful treatment of many patients with leukaemia, comparatively little is known about the biochemical mechanisms which underlie this process in vivo. In the case of the bifunctional alkylating agents, melphalan, chlorambucil and merchlorethamine (all important drugs in the management of patients with haema- tological malignancies). many in vitro studies have suggested an important role for glutathione and glutathione utilizing enzymes in the development of resistance in drug-resistant cell lines. A melphalan-resistant mouse leukaemia cell line has been characterized (Suzukake et al, 1982) which demon-
Glutathione S-Trarzsferase f rom Leukaemic Cells 499 lymphocytic leukaemia has been shown to react with the predominant form of GST identified in a series of samples taken from patients with ALL, AML or CMI, a t presentation or on relapse, and CLL at presentation or on maintenance treatment. Immunoblot analysis indicated that readily de- tectable levels of pi class GST were present in all the cases studied, regardless of the type of leukaemia or the age of the patient from which the samples were obtained. There was no clear relationship between the level of GST expression and the eventual response to chemotherapy. Moreover, there did not appear to be any clear differences between samples obtained at presentation and those obtained on relapse. Samples from patients with CLL were obtained either a t presentation, or whilst maintained on standard chemotherapy. As in the other cases studied, no difference emerged between the two groups, although the amount of data is too limited to make a detailed statistical analysis. In one case samples were obtained from the same patient (IH), both when maintained on standard chemotherapy with prednisolone and chlorani- bucil (sample H), and when highly resistant to this form of treatment (sample 1). Given the variability inherent in this technique, there was no significant difference between the level of enzyme detected on each occasion.
Antisera raised against mu or alpha forms of GST failed to detect expression of either type in any of the cases studied. suggesting that these forms of the enzyme are either expressed only rarely. or at levels below the level of detection using the immunoblotting technique.
The apparent lack of a simple correlation between the level of expression of pi class GST and response to chemotherapy suggest that increased expression of this enzyme is probably not the sole factor involved in the development of resis,ance in human leukaemias. The finding of high levels of the enzyme in cells from patients with CLL who are well controlled by treatment with chlorambucil. provides further evidence for questioning that pi class GST is of central importance in drug resistance in human leukaemias. How- ever, more detailed studies using serial samples obtained from patients during a course of chemotherapy are required to exclude subtle changes in GST levels accounting for enhanced drug resistance. Our study indicates that immuno- blotting is insufficiently accurate for this purpose, as variations in apparent GST expression of up to 3-fold can occur due to experimental error alone. The method may also be insufficiently sensitive to detect low. but biochemically significant. levels of expression of alpha and mu forms of the enzyme. which may be responsible for the development of resistance. In order to overcome these problems, studies are currently underway in our department to improve the sensitivity and accuracy of GST measurement in leukaemic cells using the HPLC assay recently described by La Creta et a! (1 988). Until precise data of this quality is obtained, the exact role of GST expression in resistance to cytotoxic drugs will remain uncertain.
strated a 2-fold increase in cytosolic glutathione as compared to parental cells. Further studies indicated that reversal of this elevation using an inhibitor of glutathione synthesis caused substantial potentiation of melphalan cytotoxicity (Somfai- Relle rt al. 1984). Other reports have indicated that resistance may be associated with elevations in the level of glutathione utilizing enzymes, involving either pi (Gupta et al, 1989) or alpha forms of GST (Buller et al. 1987; Robson el al, 1987). Work in our laboratory using a chlorambucil-resistant Chinese hamster ovary cell line with marked over expression of an alpha class GST has indicated that inhibition of GST activity using indomethacin is associated with a partial reversal of the drug resistant phenotype (Hall et 01, 1989a). A similar study has previously been reported in which ethacry- nic acid was found to potentiate chlorambucil cytotoxicity in a Walker 256 rat breast carcinoma cell line with high levels of alpha class GST (Tew et al, 1988) .
Additional support for the suggestion that GSTs may be directly involved in the development of resistance to alkylat- ing agents comes from studies which have shown that glutathione is capable of forming conjugates with melphalan, both spontaneously, and at a n enhanced rate in the presence of liver cytosol, rich in alpha forms of the enzyme (Dulik rt a/. 1986) . However, detailed reports using highly purified forms of enzyme have not, to our knowledge, been published.
As well as being implicated in the development of resis- tance to alkylating agents, some reports have noted an increase in GST in cells resistant to anthrocyclines. Such a rise may form part of a non-specific ‘stress response’, or directly contribute to the resistance phenotype by the inactivation of free radicals generated by the action of these drugs. It has been suggested that this may be mediated through a contribution to the glutathione peroxidase activity of the cytosol (Sinha et al. 1989). Such activity is normally associated with alpha forms of GST, but has also been identified in a novel pi form purified from an adriamycin- resistant breast carcinoma line (Batist et ul. 1986) .
Further evidence for the potential role of these enzymes in the development of resistance to alkylating agents and anthrocyclines has come from the transfection of cDNA encoding either alpha or pi forms of GST into yeast (Black rt al, 1989). Cos (Puchalski rt al. 1989) or MCF-7 cells (Moscow rt nl, 1989). The resulting enhanced expression of GST has been shown to confer melphalan and anthrocycline resis- tance to the recipient cell line in some, but not all, cases. The most convincing results have been obtained using cDNA for the alpha forms of the enzyme, whereas transfection of the pi form caused no enhancement in the study reported by Moscow r t a1 (1989). and a relatively modest increase in resistance in the study reported by Puchalski et al (1 989).
Although a range of in vitro experiments have suggested a role for GST expression in the development of resistance to alkylating agents and anthrocyclines, comparatively little is known of the pattern and extent of GST expression in leukaemic cells. In this study we have purified GST from examples of each of the four main clinical categories of leukaemia. Our results show that in each case the enzyme has a similar relative molecular weight, isoelectric point and range of substrate activities to the pi form which is predomin- ant in the placenta. In addition, antisera raised against pi class GST purified from the spleen of a patient with chronic
ACKNOWLEDGMENTS
We thank Mrs E. Johnson for technical assistance, Dr J. Lunnec for advice, and Mrs M. Graham for expert help with preparing the manuscript. Placental tissue was kindly col- lected by the staff of Hexham General Hospital.
500 Andrew HaZl et a1 REFERENCES
Batist. G.. Tulpule, A.. Sinha, B.K., Katki. A.G.. Myers, C.E. &Cowan. K.H. (1986) Overexpression of a novel anionic glutathione transferase in multidrug-resistant human breast cancer cells. Journal of Biological Chemistry. 261, 15544-1 5549.
Black, S.. Beggs. J.D.. Miles.].S.. Hayes,].D. & Muramatsu. M. (1989) Expression of human glutathione transferases in S. cerevisiae confers resistance to alkylating agents and chlorambucil, (Abstract). Cancer Research. 30, 51 5.
Boyer. T.D. ( I 989) The glutathione S-transferases: an update. Hcpatology, 9, 486-496.
Bradford. M. (1 976) A rapid and sensitive method for the quanti- tation of microgram quantities of protein using the principle of protein-dye binding. Analytical Biochemistry, 72, 248-2 54.
Dao. D.D.. Partridge, C.A.. Kurosky. Q. & Awasthi. Y.C. (1984) Human glutathione S-transferase-characterization of the anionic forms from lung and placenta. Biochernicnl lourrial, 221, 33-41.
Dulik, D.M.. Fenselau. C. & Hilton. J. (1 986) Characterization of melphalan-glutathione adducts whose formation is catalyzed by glutathione transferases. Biocheniical Pliarmacology. 3 5, 3405- 3409.
Gupta. V.. Singh. S.V.. Ahmad. H.. Medh. R.D. & Awasthi. Y.C. (1989) Glutathione and glutathione S-transferases in a human plasma cell line resistant to melphalan. Biochemical Phnrrnacology.
Habig. W.H. & Jakoby. W.B. (1981) Assays for differentiation of glutathione S-transferases. Methods in Enzymology. 77, 398-405.
Hall, A.. Robson. C.N.. Hickson. I.D.. Harris, A.L., Proctor. S.]. & Cattan. A.R. (1989a) Possible role of inhibition of glutathione S- transferase in the partial reversal of chlorambucil resistance by indomethacin in a Chinese hamster ovary cell line. Caricrr Kesearcli. 49, 6265-6268.
Hall, A.. Cattan, A.K. & Proctor. S.J. (1989b) Mechanisms of drug resistance in acute leukaemia. Leukaeniin Research, 13, 3 51-356.
Harrison, D.J.. Kharbanda, R.. Cunningham, D.S.. McLellan, L.I. & Hayes, 1.D. ( 1 989) Distribution of glutathione S-transferase isoeniymes in human kidney: basis for possible markers of renal injury. Journal of Clinical Pathology. 42, 624-628.
Hayes, J.D., McLellan. L.L. Stockman, P.K.. Howie, A.F.. Hussey. A.J. & Beckett. G.J. (1987) Human glutathione S-transferases; a polymorphic group of detoxification enzymes. Glutathione S- Transferases and Carcinogenesis (ed. by T. J . Mantle, C. B. Pickett and J. D. Hayes), p. 3. Taylor and Francis, London.
Hayes. P.C.. Harrison, D.J.. Bouchier. I.A.D.. McLellan. L.I. &Hayes, J.U. ( 1 989) Cytosolic and microsomal glutathione S-transferase isoenzymes in normal human liver and intestinal epithelium. Gut,
Hussey. A.J.. Hayes, J.D. & Beckett, G.J. (1987) The polymorphic expression of neutral glutathione transferase in human mono- nuclear cells as measured by radioimmunoassay. Biochemical Pharrnarology. 36, 401 3-4014.
Jones. S.M.. Idle, J.R. & Hirom. P.C. ( I 988) Differential expression of glutathione transferases by native and cultured human lympho- cytes. Biochemical Pharmacology. 37, 4586-4590.
Kamisaka. K.. Habig. W.H.. Ketley. J.N., Arias, I.M. & Jakoby, W.B. (1 97 5) Multiple forms of human glutathione S-transferase and their affinity for bilirubin. European Journal of Biochemistry. 60, 153-1 61.
Lacreta. F.P.. Olsxewski. ].I. & Tew. K.D. (1988) Purification of glutathione S-transferases from rat liver and Walker 256 mam- mary carcinoma cells by high-performance liquid chromato-
38. 1993-2000.
30, 854-859.
graphy and a glutathione affinity column. Journal of Chromato- graphy, 434, 83-93.
Laemmli. U.K. ( 1970) Cleavage of structural proteins during the assembly of the head of bacteriophage T-4. Nature. 227.680-685.
Loscalxo. 1. & Freedman. J. (1986) Purification and characterization of human platelet glutathione S-transferase. Blood. 67, 1595- 1599.
Mannervik. B. & Guthenberg, C. (1981) Glutathione transferase (human placenta). Methods in Enzyniology, 77 , 231-235.
Mannervik. B.. A h . P.. Guthenberg. C.. Jensson. H.. Tahir. M.K.. Warholm, M. &]ornvall, H. (1 98 5) Identification of three classes of cytosolic glutathione transferase common to several mammalian species: Correlation between structural data and enzymic proper- ties. Proceedings of the Natiorial Acclderny of Sciences of the United States of Anierira, 82, 7202-7306.
Mannervik. B. (1985) The isoenzymes of glutathione S-transferase. Advances in Enzymology, 57. 357-41 7.
Moscow, J.A., Townsend. A.J. & Cowan. K.H. (1 989) Elevation of pi class glutathione S-transferase activity in human breast cancer cells by transfection of the GST pi gene and its effect on sensitivity to toxins. Molecular Pharniacology, 36, 22-28.
Puchalski, R.B., Manobaran. T.H. & Fahl. W.E. (1989) Transient expression of glutathione S-transferases. pi, Ya and Ybl confer drug resistance in cos cells after continuous flow. GST mediated, cell sorting. (Abstract). Cancer Kcsearch. 30, 516.
Radola. B.J. ( 1 980) Ultrathin-layer isoelectric focusing in 50-100 pm polyacrylamide gels on silanized glass plates or polyester films. Electrophoresis, 1, 43-56.
Robson, C.N.. Lewis, A.D.. Wolf, C.R.. Hayes, J.D., Hall. A.. Proctor, S.J., Harris, A.L. & Hickson. I.D. (1987) Reduced levels of drug- induced DNA cross-linking in nitrogen mustard-resistant Chinese hamster ovary cells expressing elevated glutathione S-transferase activity. Cancer Research. 47, 6022-602 7.
Shea, T.C.. Kelley. S.L. & Henner. W.D. (19x8) Identification of an anionic form of glutathione transferase present in many human tumors and human tumor cell lines. Cancer Research. 48, 527- 533.
Sinha, B.K..Katki.A.G.. Batist. G., Cowan,K.H.&Myers. C.E. (1989) Formation of hydroxyt radicals by Adriamycin in sensitive and resistant NCF-7 human breast tumour cells: implication for the mechanism of action. Proceedings of the American Society for Cancer Research, 27, 955A.
Somfai-Relle. S.. Suzukake, K.. Vistica. B.P. & Vistica. D.T. (1984) Reduction in cellular glutathione by buthionine sulfoximine and sensitization of murine tumor cells resistant to L-phenylalanine mustard. Biochernicol Phnrrnacology. 3 3, 485-490.
Strange, R.C.. Faulder. C.G.. Davis, B.A.. Hume. R.. Brown, J.A.. Cotton. W. & Hopkinson. D.A. (1984) The human glutathione S- transferases: studies on the tissue distribution and genetic varia- tion of the GSTI, GST2 and GST3 isozymes. Annals of Hurnan Genetics, 48, 11-20.
Suzukake. K.. Petro. B.J. & Vistica. D.T. (1982) Reduction in glutathione content of L-PAM resistant L121 cells confers drug sensitivity. Biochernical Pharniacology, 31, 121-1 24.
Tew. K.D., Bomber, A.M. &Hoffman. S.J. (1988)Ethacrynic acid and piriprost as enhancers of cytotoxicity in drug resistant and sensitive cell lines. Cancer Research, 48. 3622-3625.
Towbin, H., Stachelin, T. & Gordon, L. (1979) Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: procedure and some applications. Prowcdirigs oft he National Academy ofSciences oftlie United States ofAmerica. 76.43 50-43 54.
Warholm. M.. Guthenburg. C.. Pero. K.W. & Mannervik. B. 11983) Molecular and catalytic properties of glutathione S-transferase p from human liver: an enzyme efficiently conjugating epoxides. Biochemistry. 22, 3610-361 7.