16
QEEG Report Australian Neurofeedback Institute

QEEG Report Australian Neurofeedback Institute

ANFI
Australian Neurofeedback Institute
CONTACT
EMAIL:
WEBSITE:
www.anfi.org.au
PHONE:
02 9646 6700
QEEG REPORT
Name:
Date of recording:
Date of Birth:
Gender:
Source of referral:
EEG Technician:
Recording Procedures
The electroencephalograph (EEG) was digitally recorded utilizing 19
electrodes with the International 10/20 System of electrode placement
on a Mitsar amplifier. Electrode impedances were reduced to below
5Kohms. The EEG was recorded continuously in the awake state with
eyes closed and eyes open. The EEG has been visually inspected and
artifact rejected using Independent Component Analysis.
Analysis Procedures
Independent component analysis was conducted and eye movement
artefact extracted from the raw EEG. Threshold artefact removal was
conducted and where required additional sections of jaw clenching
muscle and eye movement artefact were manually cut from the
recording. The absolute spectral analysis was computed for each task.
The output is displayed in topographical maps. Output of magnitude,
power, ratio and coherence have been included.
Signature:
Electroencephalogram Analyst
PRESENTING SYMPTOMS: The client was recently diagnosed with ADHD. He has been prescribed
Dexamphetamine, which he reports makes him hyperactive and more
lucid/aware during sleep. In addition he has been prescribed Zoloft. The
client is experiencing frequent headaches, low mood and sleeping
difficulties.
BEHAVIOUR DURING RECORDING: The client presented appropriately, speaking rapidly and reported a mild
headache, which he attributed to not having consumed his regular
morning coffee. In the previous 24 hours before the recording, the client
consumed the antidepressant Zoloft at 9am and the stimulant
Dexamphetamine at 2pm. No medications were consumed the morning
of the assessment and an appropriate breakfast was consumed at
8:15am. The night before the assessment he slept for 7 hours, waking
frequently. This is typical of his regular sleeping pattern.
EEG PATTERN CLASSIFICATION: Fronto-central beta spindles, temporal lobe instability
DESCRIPTION OF THE EEG
ARTIFACTS AND QUALITY
OF RECORDING: During the eyes open condition, high muscle tension was seen tonically in
the frontalis (Fp1, Fp2, F3, F4), masseter (F7, F8), and temporalis (T3, T4),
muscles, with brief epochs where gross muscle tension occluded the
entire record. There was limited muscle tension with eyes closed, with
occasional spikes of muscle activity in the temporalis (T3, T4),
sternocleidomastoids (T5, T6), and occipitalis (O1, O2), muscles. Vertical
and lateral eye movements were present for the duration of the recording,
predominantly corresponding to the eyes open and closed conditions.
Occasional myogenic spikes from the lateral, medial, superior and inferior
ocular rectus muscles associated with eye movements were observed at
(Fp1, Fp2, F7, F8, F3 & F4). Minor electrode issues were observed at Pz and
Fp2. No sweat, pulse, notch or salt-bridge artifacts were observed.
Excellent impedances were obtained and the overall quality of the EEG
was good.
EYES OPEN: The record was characterised by fast alpha, beta spindles and temporal
instabilities with a sharp and slow morphology. The alpha peak (11.23Hz),
and range (8.79Hz – 15.14Hz), was fast, with a slight fast skew. The alpha
distribution was predominately posterior, with a right hemisphere
asymmetry. However, some frontal alpha was observed, due to brief
epochs of widespread alpha observed in the later portions of the
condition. The right hemisphere alpha (10.74Hz), was slower than the
background activity. In both temporal lobes, instabilities with a sharp and
slow (5.37Hz), morphology were observed. These instabilities were often
concurrent, with the left hemisphere morphology often including a poly-
spike, with minor slowing, while the right hemisphere tended to have a
solitary spike with a well-defined slow wave evolution. At fronto-central
locations rhythmic slow (5.37Hz), and beta spindling (18.55Hz, 25.88Hz,
28.32Hz), was intermixed and the theta-beta ratio was 2.5 to 1. Brief
epochs of mu activity (12.21Hz), were seen in the right hemisphere (C4).
Overall coherences were moderate, with the greatest coherence (r
= .404), in alpha (11.23Hz), was observed at Fp1. There was a right frontal
asymmetry. Elevated absolute and relative Z-scores were seen in the beta
and high beta ranges. Absolute theta power was 16uV2 in comparison to
14uV2 in beta consistent with the theta-beta ratio. Elevated absolute and
relative power in alpha frequencies was seen temporally. Phase lag was
low in theta at left parieto-temporal regions. Beta Z-score coherences
were low. These results are consistent with the raw EEG.
EYES CLOSED: Alpha augmented and anteriorised following eye closure, with a rapid
alpha dropout and descent to deeper sleep stages. B2-stages were
observed within 300s of eye closure and k-complexes were observed
before 400s. Intermittent beta spindles at fronto-central locations
preceded re-alerting to brief A3-states, before deeper states reappeared.
During sleep state transitions and stages alpha transients in the temporal
lobes were observed, with sharp and slow morphological features
identified. These were most apparent in the right hemisphere. The
background alpha was initially fast, slowing as the record progressed.
The alpha peak (11.23Hz), and range (8.30Hz – 13.67Hz), was fast, with a
slight skew towards slower frequencies. The distribution of alpha was
widespread with a focal intensity in the right temporal lobe (T6), where
there was greater power in the slow tail (9.28Hz). Slow content (4.88Hz),
was also slightly elevated in the temporal lobes, relating to the sharp and
slow instabilities. At fronto-central locations, intermixed theta (5.37Hz), and
beta activity (17.09Hz, 23.37, 27.83Hz), was observed. Minor bursts of mu
activity (12.21Hz), were observed bi-centrally (C3, C4).
Hypercoherence (r = .585), in alpha (11.23Hz), observed at Fp1 and overall
coherences were high, with the exception of T4-C4. There was no clear
frontal asymmetry. Elevated absolute and relative Z-score delta, theta
and high beta activity was indicated at fronto-central and occipito-
temporal locations. Spectral mapping indicated delta and theta activity
extending posteriorly from the vertex to occipito-temporal locations. Low
phase lag was predominating in the delta and high beta ranges. These
findings are consistent with the raw EEG.

EEG FINDINGS
& PRESENTING PROBLEMS: The fast background alpha and fronto-central beta activity suggests the
client is over-aroused (1–5). Over-arousal in conjunction with the left
frontal alpha hypercoherence (6–9), and rapid descent to deeper sleep
states (10,11), suggest arousal regulation issues. Over-arousal can relate to
difficulties in salience processing (12), attentional/ impulse control (13),
sleep maintenance (4), and relate to anxiety and depression symptoms
(14–17). These findings may relate to the client’s reported diagnosis of
ADHD, potentially suggesting an impulsive/hyperactive profile (5). This is
consistent with a theta-beta ratio under 3 to 1, which is more typical of the
inattentive subtype (18,19). However, some research doesn’t agree with
this conclusion and the theta-beta ratio have become less diagnostic of
ADHD (20,21).
However, significant consideration should be provided to the temporal
lobe instabilities, which are frequently observed in ADHD (14,22). In
conjunction with the fast activity, these instabilities suggest an easily
kindled cortex (5), which can interfere with surround inhibition (22), and
thus information processing (23,24), presenting similarly to attentional
issues (20). Additionally, temporal instabilities are routinely associated with
mood and cognitive issues, such as depressed mood and memory issues
(25–31), and headaches (32–34), which may be of relevance for the client.
RECOMMENDATIONS: Heart rate variability biofeedback is recommended to enhance self-
regulation capacity (35). If neurofeedback is considered, based on the
EEG analysis, the following protocols might be beneficial, if congruent with
the results of clinical assessment and established treatment goals:
T3-T4, Reward 12.0Hz – 15.0Hz, inhibiting from 2Hz – 9.5Hz and 17Hz – 36Hz,
Cz-T4/T6, Reward 12.0Hz – 15.0Hz, inhibiting from 2Hz – 9.5Hz and 17Hz –
36Hz, C4-Pz, Reward 8Hz -10Hz, inhibiting from 2Hz – 9Hz and 17Hz – 36Hz.
(adjust reward frequencies depending on the client’s response).
If change in medication is considered, the anticonvulsant
Carbamazepine might be useful in addressing temporal lobe instability
(14, 37). Discontinuation of stimulant medication might be considered for
individuals with ADHD where beta spindles are observed(36)*.
* The purpose of the QEEG assessments performed at ANFI are to identify
patterns in brain activity that may help to understand clients’
psychological, cognitive and emotional symptoms. The QEEG reports
associated with these assessments are informative only and never intend
to replace clinical EEGs and their interpretations by a medical specialist. If
a presence of abnormal brain activity is observed, a further investigation
by a medical specialist is recommended. The appropriateness of
medication cannot be determined by a QEEG alone. Formal medical
assessment by a medical professional is required to determine the
appropriateness of any medication.

EEG RECORDED - EO CONDITION: Raw EEG (scale 1cm = 100mv, Speed 30mm/s, Low cut 0.53Hz, High Cut 50Hz)
Note: Average montage. T5-P3-O1 sharp instability (see epoch 285-6). Fronto-
central beta activity (see epoch 287-8).
Raw EEG (scale 1cm = 100mv, Speed 30mm/s, Low cut 0.53Hz, High Cut 50Hz)
Note: Average montage. Right lateral sharp and slow instability (see epoch 501-2 &
504-5). Fronto-central theta activity (see epoch 502). Mu at C4 and to a lesser
extent C3 (see epoch 508-10).
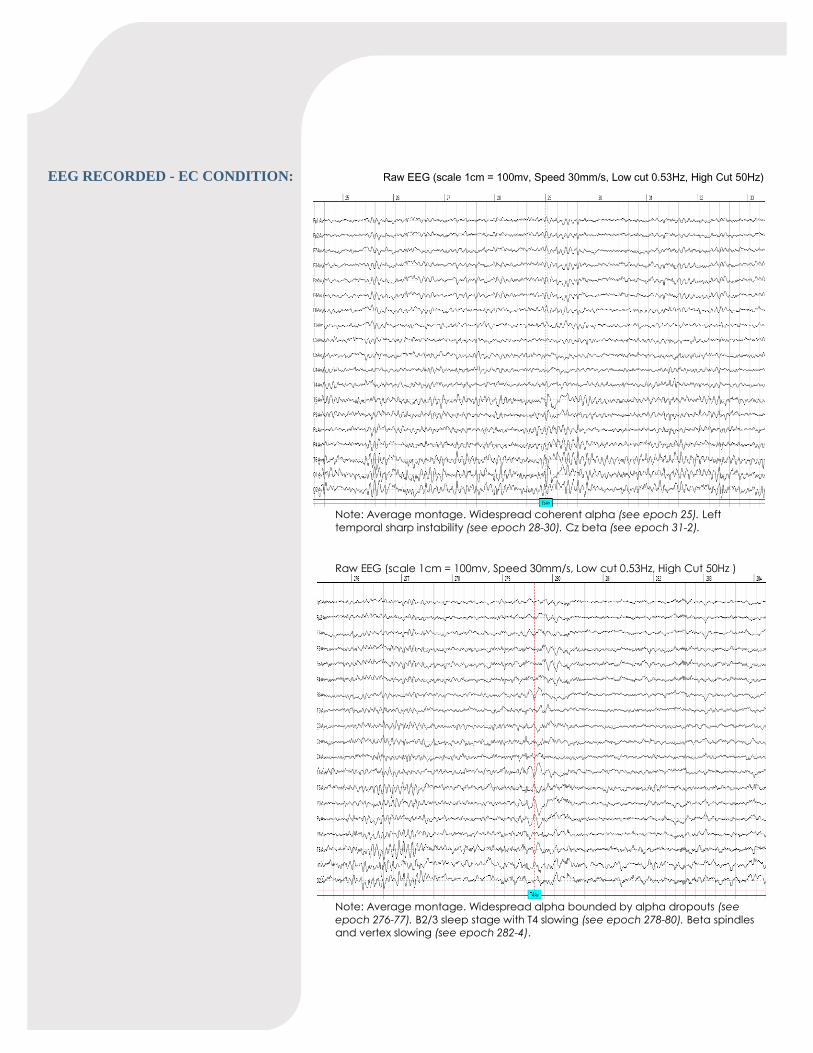
EEG RECORDED - EC CONDITION: Raw EEG (scale 1cm = 100mv, Speed 30mm/s, Low cut 0.53Hz, High Cut 50Hz)
Note: Average montage. Widespread coherent alpha (see epoch 25). Left
temporal sharp instability (see epoch 28-30). Cz beta (see epoch 31-2).
Raw EEG (scale 1cm = 100mv, Speed 30mm/s, Low cut 0.53Hz, High Cut 50Hz )
Note: Average montage. Widespread alpha bounded by alpha dropouts (see
epoch 276-77). B2/3 sleep stage with T4 slowing (see epoch 278-80). Beta spindles
and vertex slowing (see epoch 282-4).
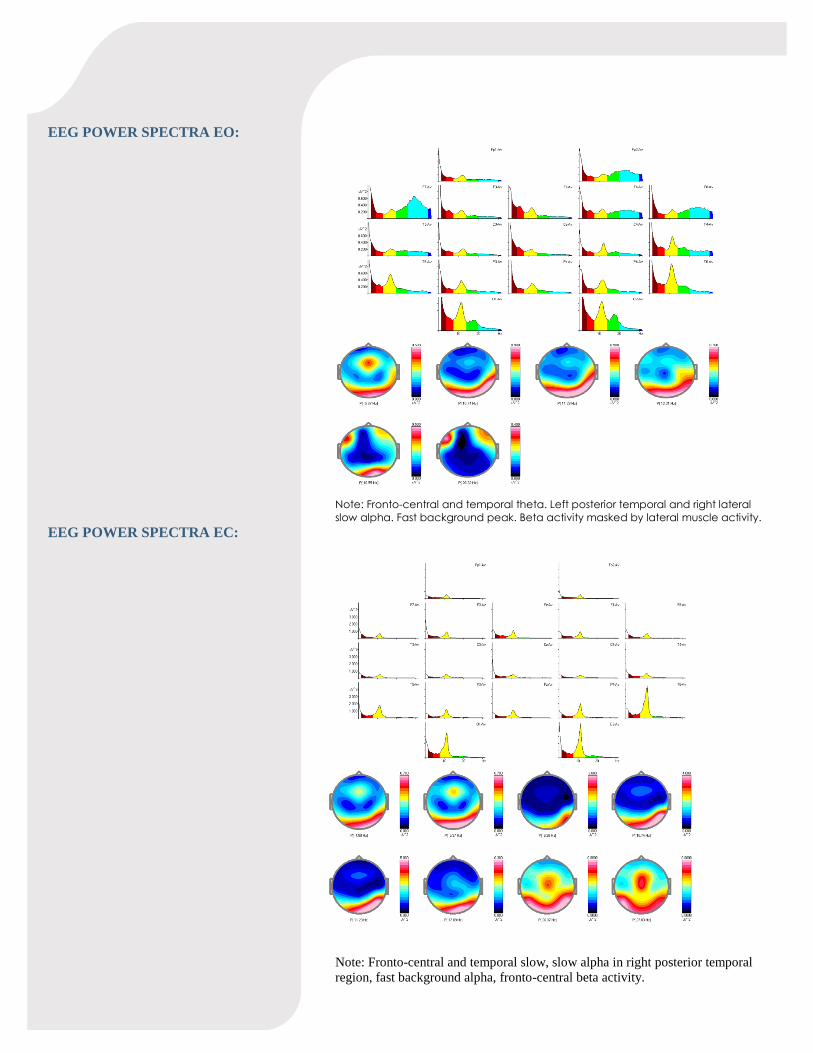
EEG POWER SPECTRA EO:
Note: Fronto-central and temporal theta. Left posterior temporal and right lateral
slow alpha. Fast background peak. Beta activity masked by lateral muscle activity.
EEG POWER SPECTRA EC:
Note: Fronto-central and temporal slow, slow alpha in right posterior temporal
region, fast background alpha, fronto-central beta activity.
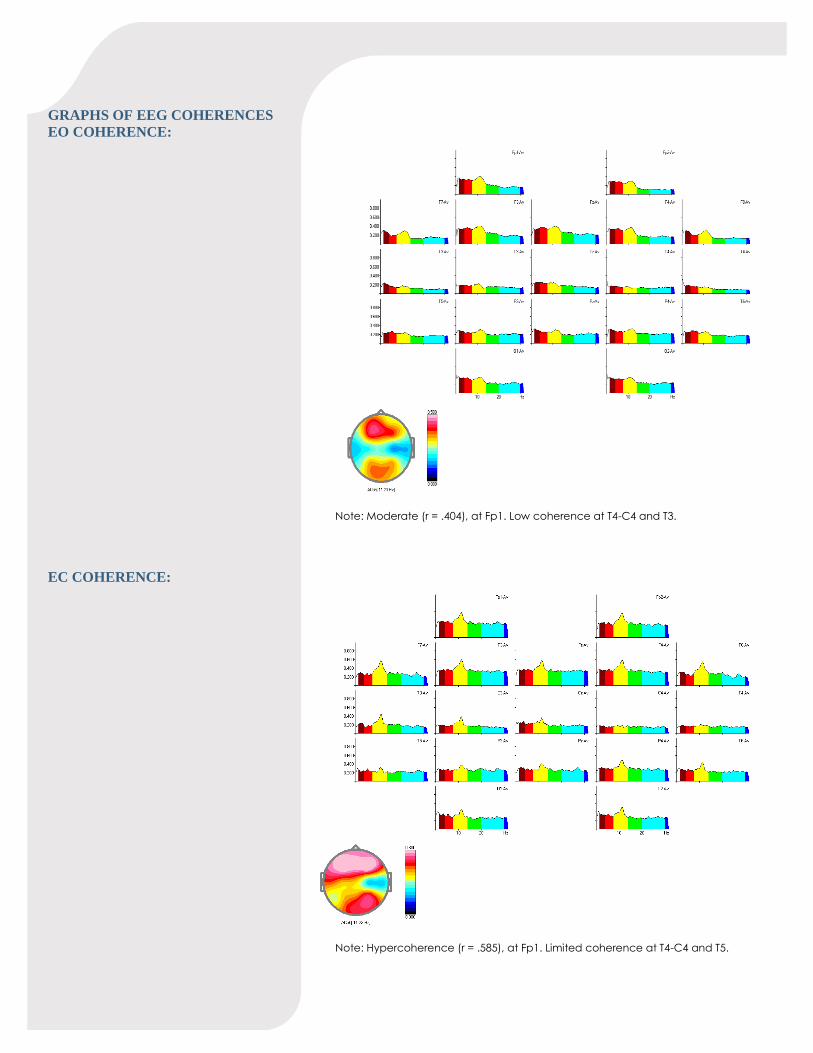
GRAPHS OF EEG COHERENCES
EO COHERENCE:
Note: Moderate (r = .404), at Fp1. Low coherence at T4-C4 and T3.
EC COHERENCE:
Note: Hypercoherence (r = .585), at Fp1. Limited coherence at T4-C4 and T5.

EO SPIKE AVERAGING:
Note: Left field includes T5-P3-O1, right field includes T6-T4 and minor O2
activity.
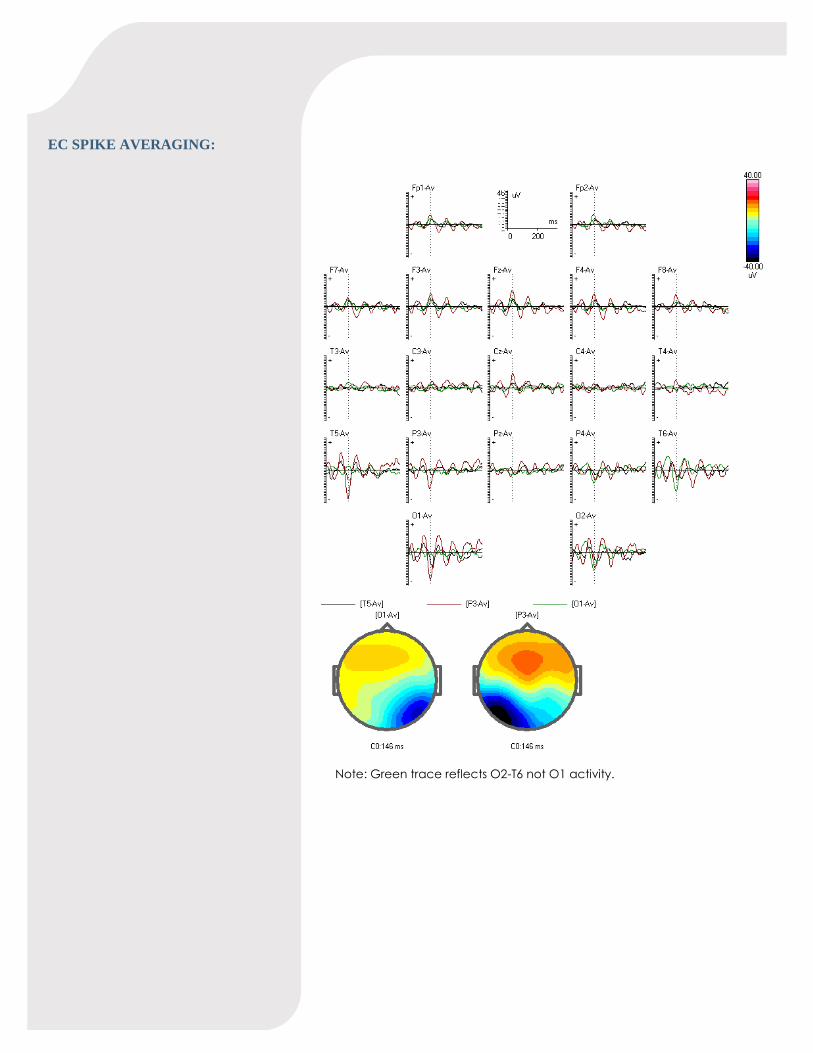
EC SPIKE AVERAGING:
Note: Green trace reflects O2-T6 not O1 activity.
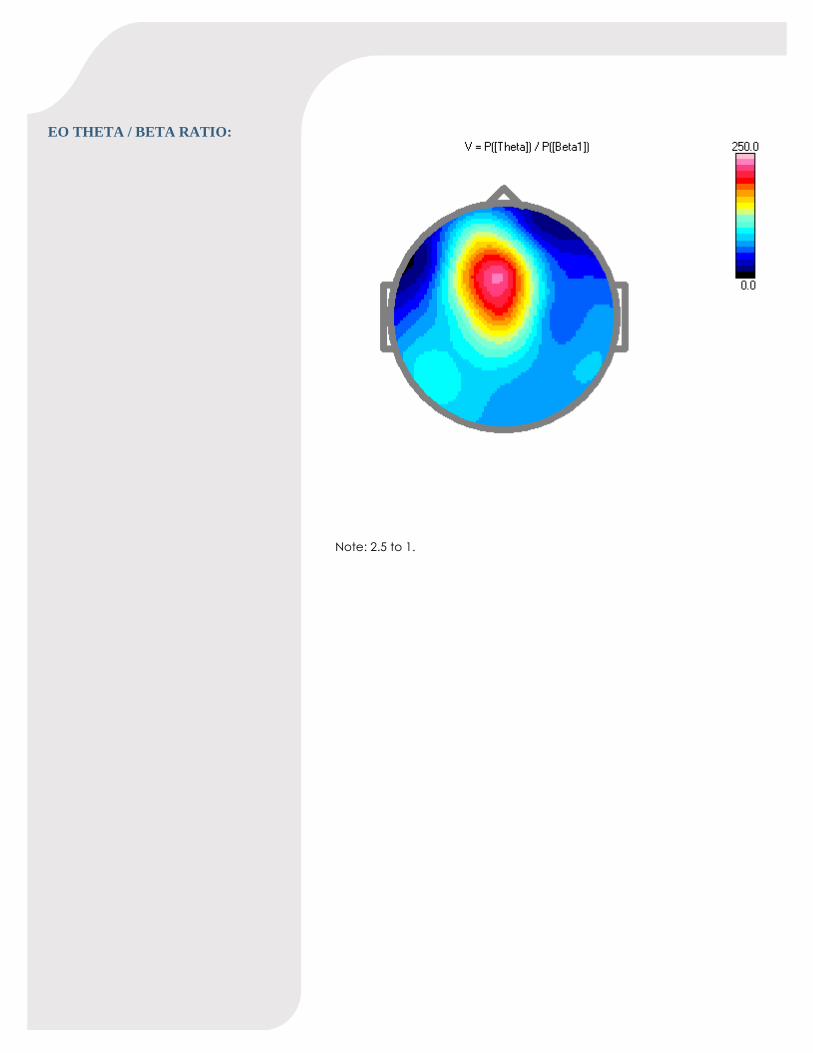
EO THETA / BETA RATIO:
Note: 2.5 to 1.

FRONTAL ASYMMETRY
EYES OPEN:
Note: Slight right frontal (caution due to muscle).
EYES CLOSED:
Note: No clear frontal asymmetry.

REFERENCES
1. Thorpe SG, Cannon EN, Fox NA, Thorpe, s. Cannon, Fox N. Spectral and
source structural development of mu and alpha rhythms from infancy
through adulthood. Clin Neurophysiol [Internet]. 2016;127(1):254–69.
Available from: http://dx.doi.org/10.1016/j.clinph.2015.03.004
2. Bazanova OM, Vernon D. Interpreting EEG alpha activity. Neurosci
Biobehav Rev [Internet]. 2014;44:94–110. Available from:
http://dx.doi.org/10.1016/j.neubiorev.2013.05.007
3. Jin MJ, Kim JS, S K, Hyun MH, Lee S. An Integrated Model of Emotional
Problems , Beta Power of Electroencephalography , and Low Frequency
of Heart Rate Variability after Childhood Trauma in a Non- Clinical
Sample : A Path Analysis Study. Front Psychiatry. 2018;8(314):1–9.
4. Arns M, Swatzyna RJ, Gunkelman J, Olbrich S. Sleep maintenance,
spindling excessive beta and impulse control: an RDoC arousal and
regulatory systems approach? Neuropsychiatr Electrophysiol [Internet].
2015;1(1):5. Available from:
http://npepjournal.biomedcentral.com/articles/10.1186/s40810-015-0005-
9
5. Johnstone J, Gunkelman J, Lunt J. Clinical database development:
Characterization of EEG phenotypes. Clin EEG Neurosci. 2005;36(2):99–
107.
6. Fingelkurts AA, Fingelkurts AA. Altered structure of dynamic
electroencephalogram oscillatory pattern in major depression. Biol
Psychiatry [Internet]. 2015;77(12):1050–60. Available from:
http://dx.doi.org/10.1016/j.biopsych.2014.12.011
7. Lee S-H, Yoon S, Kim J-I, Jin S-H, Chung CK. Functional connectivity of
resting state EEG and symptom severity in patients with post-traumatic
stress disorder. Prog Neuro-Psychopharmacology Biol Psychiatry
[Internet]. 2014;51:51–7. Available from:
http://linkinghub.elsevier.com/retrieve/pii/S0278584614000098
8. Imperatori C, Farina B, Quintiliani MI, Onofri A, Castelli Gattinara P, Lepore
M, et al. Aberrant EEG functional connectivity and EEG power spectra in
resting state post-traumatic stress disorder: A sLORETA study. Biol Psychol
[Internet]. 2014;102(1):10–7. Available from:
http://dx.doi.org/10.1016/j.biopsycho.2014.07.011
9. Olbrich S, Tränkner A, Chittka T, Hegerl U, Schönknecht P. Functional
connectivity in major depression: Increased phase synchronization
between frontal cortical EEG-source estimates. Psychiatry Res -
Neuroimaging [Internet]. 2014;222(1–2):91–9. Available from:
http://dx.doi.org/10.1016/j.pscychresns.2014.02.010
10. Hegerl U, Himmerich H, Engmann B, Hensch T. Mania and attention-
deficit/hyperactivity disorder: Common symptomatology, common
pathophysiology and common treatment? Curr Opin Psychiatry.
2010;23(1):1–7.
11. Gau SSF, Kessler RC, Tseng WL, Wu YY, Chiu YN, Yeh C Bin, et al.
Association between sleep problems and symptoms of attention-deficit/
hyperactivity disorder in young adults. Sleep [Internet]. 2007;30(2):195–
201. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc5&N
EWS=N&AN=2007-13625-006
12. Menon V. Large-scale brain networks and psychopathology: A unifying
triple network model. Trends Cogn Sci [Internet]. 2011;15(10):483–506.
Available from: http://dx.doi.org/10.1016/j.tics.2011.08.003
13. Munakata Y, Herd S, Chatham C, Depue BE, Banich MT, O’Reilly RC. A
unified framework for inhibitory control. Trends Cogn Sci [Internet].
2011;15(10):453–9. Available from:
http://www.sciencedirect.com/science/article/pii/S1364661311001562
14. Olbrich S, Van Dinteren R, Arns M. Personalized Medicine: Review and
Perspectives of Promising Baseline EEG Biomarkers in Major Depressive
Disorder and Attention Deficit Hyperactivity Disorder.
Neuropsychobiology. 2016;72(3–4):229–40.
15. Enoch MA, Shen PH, Ducci F, Yuan Q, Liu J, White K V., et al. Common
genetic origins for EEG, alcoholism and anxiety: The role of CRH-BP. PLoS
One. 2008;3(10):0–10.
16. Hardt J, Kamiya J. Anxiety Change Through Electroencephalographic
Alpha Feedback Seen Only in High Anxiety Subjects. Science (80- ).
1978;201(4350):79–81.
17. Aftanas LI, Pavlov S V. Trait anxiety impact on posterior activation
asymmetries at rest and during evoked negative emotions: EEG
investigation. Int J Psychophysiol. 2005;55(1):85–94.
18. Breteler M, Coenen A, de Ridder S, Arns M, Strehl U. Efficacy of
Neurofeedback Treatment in ADHD: The Effects on Inattention, Impulsivity
and Hyperactivity: A Meta-Analysis. Clin EEG Neurosci. 2012;40(3):180–9.
19. Arns M, de Ridder S, Strehl U, Breteler M, Coenen A, de Ridder S, et al.
Efficacy of Neurofeedback Treatment in ADHD: The Effects on
Inattention, Impulsivity and Hyperactivity: A Meta-Analysis. Clin EEG
Neurosci [Internet]. 2009;40(3):180–9. Available from:
http://journals.sagepub.com/doi/10.1177/155005940904000311
20. Knyazev GG. Motivation, emotion, and their inhibitory control mirrored in
brain oscillations. Neurosci Biobehav Rev. 2007;31(3):377–95.
21. Arns M, Conners CK, Kraemer HC, Arns M, Conners C KH. A Decade of
EEG Theta/Beta Ratio Research in ADHD: A Meta-Analysis. J Atten Disord
[Internet]. 2013;17(5):374–83. Available from:
http://journals.sagepub.com/doi/10.1177/1087054712460087
22. Shelley BP, Trimble MR. “All that Spikes is Not Fits,” Mistaking the Woods for
the Trees: The Interictal Spikes—An “EEG Chameleon” in the Interface
Disorders of Brain and Mind: A Critical Review. Clin EEG Neurosci
[Internet]. 2009;40(4):245–61. Available from:
http://journals.sagepub.com/doi/10.1177/155005940904000407
23. Klimesch W. Alpha-band oscillations, attention, and controlled access to
stored information. Trends Cogn Sci [Internet]. 2012;16(12):606–17.
Available from: http://dx.doi.org/10.1016/j.tics.2012.10.007
24. Klimesch W, Sauseng P, Hanslmayr S. EEG alpha oscillations: The inhibition-
timing hypothesis. Brain Res Rev. 2007;53(1):63–88.
25. Motomura E, Inui K, Shiroyama T, Nakagawa M, Nakase S, Okazaki Y. Is
temporal slow wave on EEG a useful diagnostic tool in vascular
depression? [5]. Psychiatry Clin Neurosci. 2003;57(6):610–1.
26. Emilia M, Andraus C, Alves-leon SV. Non-epileptiform EEG abnormalities
An overview. Arch Neurolpsychiatry. 2011;69(5):829–35.
27. Chen DK, LaFrance WCJ. Diagnosis and Treatment of Nonepileptic
Seizures. Contin (Minneap Minn). 2016;22(1):116–31.
28. Pacia S V., Ebersole JS. Intracranial EEG substrates of scalp ictal patterns
from temporal lobe foci. Epilepsia. 1997;38(6):642–54.
29. Gorji A, Speckmann E-J. Epileptiform EEG spikes and their functional
significance. Clin EEG Neurosci [Internet]. 2009;40(4):230–3. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/19780343
30. Hills MD. The psychological and social impact of epilepsy. Neurol Asia.
2007;12(Supplement 1):10–2.
31. Nicolai J, Kasteleijn-Nolst Trenite D. Interictal discharges and cognition.
Epilepsy Behav [Internet]. 2011;22(1):134–6. Available from:
http://dx.doi.org/10.1016/j.yebeh.2011.06.010

32. Headache Classification Committee of the International Headache
Society (IHS). The International Classification of Headache Disorders, 3rd
edition. Cephalagia [Internet]. 2013;33(9):629–808. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/18808500%5Cnhttp://www.ncbi.nl
m.nih.gov/pubmed/24409431%5Cnhttp://www.ncbi.nlm.nih.gov/pubme
d/22325197%5Cnhttp://www.ncbi.nlm.nih.gov/pubmed/16805756%5Cnht
tp://www.ncbi.nlm.nih.gov/pubmed/24238370%5Cnhttp://www.ncbi.nlm
33. Bolay H, Moskowitz MA. The emerging importance of cortical spreading
depression in migraine headache. Rev Neurol (Paris) [Internet].
2005;161(6–7):655–7. Available from:
http://www.sciencedirect.com/science/article/pii/S0035378705851082
34. Sugahara H. Brain blood perfusion hypothesis for migraine, anger, and
epileptic attacks. Med Hypotheses. 2004;62(5):766–9.
35. Robe A, Dobrean A, Cristea IA, Păsărelu C, Predescu E. Attention-
Deficit/Hyperactivity Disorder and task-related heart rate variability: a
systematic review and meta-analysis. Neurosci Biobehav Rev [Internet].
2019;18:30800–5. Available from:
https://doi.org/10.1016/j.neubiorev.2019.01.022
36. Arns M, Olbrich S. Personalized medicine in ADHD and depression: Use of
pharmaco-EEG. Curr Top Behav Neurosci. 2014;21:345–70.
37. Gunkelman J. Medication Prediction with Electroencephalography
Phenotypes and Biomarkers. Biofeedback [Internet]. 2014;42(2):68–73.
Available from: http://www.aapb-
biofeedback.com/doi/abs/10.5298/1081-5937-42.2.03

















