Quality Improvement Guidelines for thePerformance of Cervical Carotid Angioplastyand Stent PlacementDeveloped by a Collaborative Panel of the American Society ofInterventional and Therapeutic Neuroradiology, the AmericanSociety of Neuroradiology, and the Society of InterventionalRadiology
John D. Barr, MD, John J. Connors, III, MD, David Sacks, MD, Joan C. Wojak, MD, Gary J. Becker, MD,John F. Cardella, MD, Bohdan Chopko, MD, PhD, Jacques E. Dion, MD, Allan J. Fox, MD,Randall T. Higashida, MD, Robert W. Hurst, MD, Curtis A. Lewis, MD, MBA, Terence A.S. Matalon, MD,Gary M. Nesbit, MD, J. Arliss Pollock, MD, Eric J. Russell, MD, David J. Seidenwurm, MD, andRobert C. Wallace, MD, for the ASITN, ASNR, and SIR Standards of Practice Committees
J Vasc Interv Radiol 2003; 14:S321–S335
Abbreviations: ACAS � Asymptomatic Carotid Atherosclerosis Study, ACR � American College of Radiology, AHA � American Heart Association,ASITN � American Society of Interventional and Therapeutic Neuroradiology, ASNR � American Society of Neuroradiology, CAS � carotid angioplasty andstent placement, CEA � carotid endarterectomy, CREST � Carotid Revascularization: Endarterectomy vs. Stent Trial, NASCET � North American SymptomaticCarotid Endarterectomy Trial, NIHSS � National Institutes of Health Stroke Scale, SIR � Society of Interventional Radiology
PREAMBLE
THE joint Standards of Practice Com-mittee of the American Society of In-terventional and Therapeutic Neuro-radiology (ASITN), American Societyof Neuroradiology (ASNR), and theSociety of Interventional Radiology
(SIR) is comprised of experts in abroad spectrum of interventional prac-tice from both the private and aca-demic sectors of medicine. Individualmembers of the Standards of PracticeCommittee dedicate the vast majorityof professional time to diagnostic andinterventional practice and the jointcommittee includes representativesfrom radiology, neurosurgery, inter-ventional radiology and interventionalneuroradiology, a diverse constitu-ency expert on the subject matter un-der consideration.
Technical documents specifying theexact consensus and literature reviewmethodologies as well as the institu-tional affiliations and professional cre-dentials of the authors of this docu-ment are available on request fromSIR, 10201 Lee Highway, Suite 500,Fairfax, VA 22030.
METHODOLOGY
ASITN, ASNR, and SIR Standardsof Practice documents are producedusing the following process. Standards
documents of relevance and timelinessare conceptualized by the Standards ofPractice Committee members. A rec-ognized expert is identified to serve asthe principal author for the standard.Additional authors may be assigneddepending on the magnitude of theproject.
An in-depth literature search is per-formed with electronic medical litera-ture data bases. Then a critical reviewand selection of peer-reviewed articlesare performed based on study meth-odology, results, and conclusions.Data compiled from selected articlesmeeting evidence thresholds are usedto develop content and to setstandards.
When the evidence of literature isweak, conflicting, or contradictory,consensus for the parameter is reachedby a minimum of 12 Standards ofPractice Committee members with aModified Delphi Consensus Method(1,2). For purposes of these docu-ments, consensus is defined as 80%Delphi participant agreement on avalue or parameter.
This article also appears in J Vasc Interv Radiol 2003;14:1079–1093.
Received July 3, 2003; accepted July 18. Addresscorrespondence to SIR, 10201 Lee Hwy, Suite 500,Fairfax, VA 22030. E-mail [email protected]
Dr. John F. Cardella is chair of the Society of Inter-ventional Radiology Standards of Practice Commit-tee. Dr. David Sacks is Councilor of the Society ofInterventional Radiology Standards Division. Dr.Barr is Vice President of the ASITN and Dr. Connorsis President of the ASITN; they authored the firstdraft of this document and served as topic leadersduring the subsequent revisions of this draft.
This article will also appear in the October 2003issue of AJNR.
J.D.B., J.J.C., and B.C. have identified a potentialconflict of interest.
AJNR Am J Neuroradiol 24:2020–2034, November/December 2003
Reprinted from J Vasc Interv Radiol 2003; 14:S321–S335with permission by Lippincott Williams & Wilkins.
2020
The draft document is critically re-viewed by the Standards of PracticeCommittee members, either by tele-phone conference calling or face-to-face meeting. The finalized draft fromthe Committee is sent to the ASITN,ASNR, and SIR membership for fur-ther input/criticism during a 30-daycomment period. These comments arediscussed by the Standards of PracticeCommittee, and appropriate revisionsmade to create the finished standardsdocument. Before its publication, thedocument was endorsed by the ASITNExecutive Committee, ASNR Execu-tive Committee, and the SIR ExecutiveCouncil.
I. INTRODUCTION
This Quality Improvement Guide-line for the Performance of CervicalCarotid Angioplasty and Stent Place-ment was developed by a writinggroup consisting of members from in-terventional neuroradiology, neuro-surgery, neuroradiology, and inter-ventional radiology. A thoroughreview of the literature was per-formed. Thresholds for quality assur-ance were difficult to set due to therelative paucity of data and lack ofuniform reporting of clinical outcomesand complications. The ASITN, theASNR, and the SIR recognize that bra-chiocephalic revascularization is un-dergoing rapid change in technologyeven as it is being increasinglyadopted in clinical practice for thetreatment of cerebrovascular patholo-gies (3). There is a critical need to en-courage the development of proce-dures that may improve outcomes forpatients with brachiocephalic and in-tracranial atherosclerotic stenoses.Furthermore, due to the implicationsconcerning stroke prevention, theASITN, ASNR, and SIR wish to en-courage the careful and scientificstudy of the safety and efficacy of bra-chiocephalic revascularization as wellas appropriate utilization of thesetechniques (3).
The published standard of practicefor cervicocerebral angiography de-scribes the minimum acceptable re-quirements for performance of themuch less difficult and lower risk pro-cedure of diagnostic cervicocerebralangiography (4); it is the purpose ofthis standard to describe the minimumprerequisite for the performance of the
far more difficult and higher risk pro-cedure of carotid artery angioplastyand stent placement (CAS). Far moreexperience and training and fewercomplications during diagnostic cere-bral angiography are expected of thosewho perform neurovascular interven-tions, similar to what is expected ofthose who perform coronary interven-tions. At a minimum, performance ofCAS requires extensive prior experi-ence and demonstrated competencewith diagnostic cervicocerebral an-giography, as well as experience withangioplasty and stent placement. Suchrequirements for additional trainingand experience in performing CAShave been recognized by the Accredi-tation Council for Graduate MedicalEducation (ACGME) as part of thespecialty training requirements for en-dovascular surgical neuroradiology(5).
Stroke is the third leading cause ofdeath in the United States, and isch-emic stroke accounts for more than80% of the morbidity and mortalityassociated with stroke. Many ischemicstrokes are related to large- and medi-um-vessel atherosclerotic diseasewithin the cerebrovascular circulation.Therefore, procedures such as angio-plasty and/or stent placement to re-verse critical cerebrovascular stenosesmay have great importance. CAS isbeing performed with rapidly increas-ing frequency in the United States. Weanticipate that more data regardingoutcomes and complications will becollected and published in the nearfuture (the National Institutes ofHealth–supported Carotid Revascu-larization: Endarterectomy vs. StentTrial [CREST] as well as other con-trolled series have begun) (6). There-fore, we recommend that this standardbe reviewed and, if necessary, revisedwithin the next 24 months to remainapplicable to contemporary medicineconcerning this rapidly progressingtechnique.
CAS is an innovative procedure.Until the true risks and appropriateindications for this procedure areclearly known, the ASITN, ASNR, andSIR recommend that for patients whohave average surgical risk, such asthose who would have qualified forenrollment in the North AmericanSymptomatic Carotid EndarterectomyTrial (NASCET) and the Asymptom-atic Carotid Atherosclerosis Study
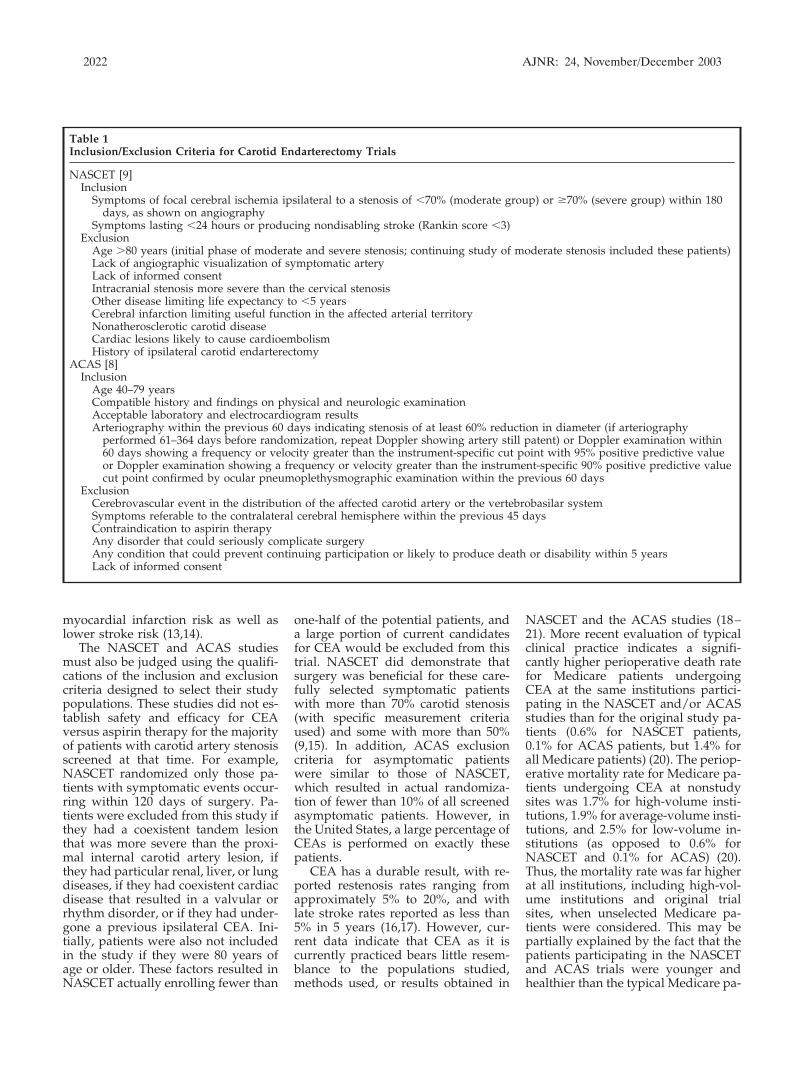
(ACAS), CAS should only be per-formed as part of a randomized clini-cal trial or an institutional reviewboard–approved investigational pro-gram. The inclusion and exclusion cri-teria for the NASCET and ACAS stud-ies are summarized in Table 1. At thistime, CAS has shown promise for thetreatment of patients known to be athigh risk of carotid endarterectomy(Yadav J, presented at the AmericanHeart Association Scientific Sessions,Chicago, November 2002) (5). CASshould only be performed on appro-priate patients by an individual orteam with training and expertise incerebrovascular angiography, patho-physiology, hemodynamics, and neu-rovascular interventions and/or ca-rotid angioplasty/stent placement (7).This recommendation is further ex-tended to encourage multidisciplinaryinput and concurring opinion in clini-cal decision making.
II. OVERVIEW
A. Rationale for Carotid Endarterec-tomy.—Two large randomized stud-ies, NASCET and ACAS, have estab-lished that certain selected patientsbenefit from surgical treatment ofsignificant atherosclerotic stenosis inthe cervical carotid artery (8–10),whereas at least two other random-ized studies of endarterectomy forasymptomatic carotid stenosis indi-cated no benefit from surgery (11,12).NASCET and ACAS showed thatlowered stroke morbidity can beachieved in selected symptomaticand asymptomatic patients undergo-ing carotid endarterectomy (CEA)compared with aspirin therapy ifsurgical endarterectomy can be per-formed with an acceptably low com-plication rate. However, they did notevaluate the risk of endarterectomyversus “best” medical therapy that isnow currently available. No trial hasevaluated the natural history or riskof stroke from cervical carotid ath-erosclerotic stenosis treated withwarfarin, combination warfarin andaspirin, aspirin and dipyridamole,ticlopidine, clopidogrel, or combina-tions of antiplatelet agents. More im-portantly, newer drugs such asstatins and angiotensin-convertingenzyme inhibitors have been provedto stabilize plaque and thus decrease
AJNR: 24, November/December 2003 2021
myocardial infarction risk as well aslower stroke risk (13,14).
The NASCET and ACAS studiesmust also be judged using the qualifi-cations of the inclusion and exclusioncriteria designed to select their studypopulations. These studies did not es-tablish safety and efficacy for CEAversus aspirin therapy for the majorityof patients with carotid artery stenosisscreened at that time. For example,NASCET randomized only those pa-tients with symptomatic events occur-ring within 120 days of surgery. Pa-tients were excluded from this study ifthey had a coexistent tandem lesionthat was more severe than the proxi-mal internal carotid artery lesion, ifthey had particular renal, liver, or lungdiseases, if they had coexistent cardiacdisease that resulted in a valvular orrhythm disorder, or if they had under-gone a previous ipsilateral CEA. Ini-tially, patients were also not includedin the study if they were 80 years ofage or older. These factors resulted inNASCET actually enrolling fewer than
one-half of the potential patients, anda large portion of current candidatesfor CEA would be excluded from thistrial. NASCET did demonstrate thatsurgery was beneficial for these care-fully selected symptomatic patientswith more than 70% carotid stenosis(with specific measurement criteriaused) and some with more than 50%(9,15). In addition, ACAS exclusioncriteria for asymptomatic patientswere similar to those of NASCET,which resulted in actual randomiza-tion of fewer than 10% of all screenedasymptomatic patients. However, inthe United States, a large percentage ofCEAs is performed on exactly thesepatients.
CEA has a durable result, with re-ported restenosis rates ranging fromapproximately 5% to 20%, and withlate stroke rates reported as less than5% in 5 years (16,17). However, cur-rent data indicate that CEA as it iscurrently practiced bears little resem-blance to the populations studied,methods used, or results obtained in
NASCET and the ACAS studies (18–21). More recent evaluation of typicalclinical practice indicates a signifi-cantly higher perioperative death ratefor Medicare patients undergoingCEA at the same institutions partici-pating in the NASCET and/or ACASstudies than for the original study pa-tients (0.6% for NASCET patients,0.1% for ACAS patients, but 1.4% forall Medicare patients) (20). The periop-erative mortality rate for Medicare pa-tients undergoing CEA at nonstudysites was 1.7% for high-volume insti-tutions, 1.9% for average-volume insti-tutions, and 2.5% for low-volume in-stitutions (as opposed to 0.6% forNASCET and 0.1% for ACAS) (20).Thus, the mortality rate was far higherat all institutions, including high-vol-ume institutions and original trialsites, when unselected Medicare pa-tients were considered. This may bepartially explained by the fact that thepatients participating in the NASCETand ACAS trials were younger andhealthier than the typical Medicare pa-
Table 1Inclusion/Exclusion Criteria for Carotid Endarterectomy Trials
NASCET [9]Inclusion
Symptoms of focal cerebral ischemia ipsilateral to a stenosis of �70% (moderate group) or �70% (severe group) within 180days, as shown on angiography
Age �80 years (initial phase of moderate and severe stenosis; continuing study of moderate stenosis included these patients)Lack of angiographic visualization of symptomatic arteryLack of informed consentIntracranial stenosis more severe than the cervical stenosisOther disease limiting life expectancy to �5 yearsCerebral infarction limiting useful function in the affected arterial territoryNonatherosclerotic carotid diseaseCardiac lesions likely to cause cardioembolismHistory of ipsilateral carotid endarterectomy
ACAS [8]Inclusion
Age 40–79 yearsCompatible history and findings on physical and neurologic examinationAcceptable laboratory and electrocardiogram resultsArteriography within the previous 60 days indicating stenosis of at least 60% reduction in diameter (if arteriography
performed 61–364 days before randomization, repeat Doppler showing artery still patent) or Doppler examination within60 days showing a frequency or velocity greater than the instrument-specific cut point with 95% positive predictive valueor Doppler examination showing a frequency or velocity greater than the instrument-specific 90% positive predictive valuecut point confirmed by ocular pneumoplethysmographic examination within the previous 60 days
ExclusionCerebrovascular event in the distribution of the affected carotid artery or the vertebrobasilar systemSymptoms referable to the contralateral cerebral hemisphere within the previous 45 daysContraindication to aspirin therapyAny disorder that could seriously complicate surgeryAny condition that could prevent continuing participation or likely to produce death or disability within 5 yearsLack of informed consent
AJNR: 24, November/December 20032022
tients now undergoing CEA at thesesame or other institutions. Older pa-tients and those with significant co-morbidity have repeatedly beenshown to be at increased risk of peri-operative stroke and death from CEA(20–36). Although recent surgical arti-cles dispute the concept that there is apopulation of patients who have a sig-nificantly higher risk of complicationsafter CEA (37,38), the recently com-pleted Stenting and Angioplasty withProtection in Patients at High Risk forEndarterectomy (SAPPHIRE) Trial(Yadav J, presented at the AmericanHeart Association Scientific Sessions,Chicago, November 2002) indicatesthat these “high surgical risk” patientsare indeed at higher risk of complica-tions from CEA.
The role of endarterectomy inasymptomatic carotid stenosis is con-troversial (39–57). Only one random-ized, controlled trial (ACAS) hasshown surgery to be beneficial,whereas at least two have not(8,11,12). ACAS, however, did not findbenefit for CEA versus medical ther-apy for major stroke, only minorstroke (8). Asymptomatic cervical ca-rotid artery stenosis has been repeat-edly shown to be of relatively lowstroke risk until the remaining lumenapproaches 1 mm in diameter (usuallycorresponding to stenosis of approxi-mately 80%–90% by NASCET criteria)(8,45,49). Even then, the risk is lessthan even a moderate stenosis in asymptomatic patient (8,9,54). Forasymptomatic patients with stenosesof less than 80%, the risk of ipsilateralstroke is approximately 1% per year or5% in 5 years with treatment with onlyaspirin (49,55). Approximately 45% ofstrokes in patients with asymptomaticstenoses are not caused by the stenosisbut rather arise from intracranial orcardiovascular sources, thus furtherreducing the actual risk of the lesionitself (57). Additionally, contrary tothe clinical findings in ACAS, a recentreview of the computed tomographic(CT) scans of ACAS patients revealedthat carotid endarterectomy does notreduce the frequency of CT-identifi-able ipsilateral cerebral infarction inpatients with high-grade asymptom-atic carotid artery stenosis (58). Basedon the ACAS trial, the American HeartAssociation (AHA) considered CEA tobe beneficial for treatment of asymp-tomatic, angiographically proven ca-
rotid stenosis of more than 60% if thecombined perioperative stroke/mor-tality rate is less than 3% (59), whichmight only be achievable in otherwisehealthy individuals. In contrast to theAHA guidelines for endarterectomy,the Canadian Stroke Consortiumreached consensus that there was in-sufficient evidence to endorse CEA forany level of asymptomatic stenosis(60). Reasons cited were lack of proofof reduction of the risk of major dis-abling stroke, the question of repro-ducibility of surgical results in thegeneral population, and the unprovenlong-term benefit of surgical recon-struction. Even a slight reduction inthe intrinsic risk of asymptomatic ca-rotid stenosis achieved by treatmentwith contemporary pharmaceuticalsin addition to (or other than) aspirin,such as statins or angiotensin-convert-ing enzyme inhibitors, might renderCEA nonbeneficial in the majority ofasymptomatic patients (13,14). There-fore, at best, CEA for asymptomaticpatients is only indicated according tothe AHA guidelines, and carotid stentplacement for asymptomatic patientsis rarely indicated outside of clinicaltrials (many of which are underway)until benefit is demonstrated.
B. Rationale for CAS.—CAS is un-dergoing rapid evolution. However,it must be remembered that the con-dition being treated is usually notemergent, and therefore transfer to afacility with the skills, training, andknowledge to perform this procedurewith acceptable quality assurance isalmost always possible. There areseveral preliminary single-center ex-periences that have been publishedas well as an international multi-center compilation (61–79). Four ran-domized, controlled trials for evalua-tion of this technology have beencompleted and reported.
• The Carotid and Vertebral Ar-tery Transluminal AngioplastyStudy (CAVATAS) was a large,prospective, randomized, multi-center trial comparing CEA withcarotid artery angioplasty withselective stent placement in 504patients with symptomatic ste-noses (at least 30% luminal di-ameter reduction) who weresuitable for surgery (80). Thisstudy did not use distal protec-tion, and stent placement wasperformed in only 26% of cases.
There was no significant differ-ence in the risk of stroke ordeath related to the procedurebetween CEA and CAS. Thetechnical success rate for CASwas 89% (successful balloon in-flation or stent placement; thepercentage of residual stenosiswas not reported). The rate ofany stroke lasting longer than 7days or death within 30 days offirst treatment was approxi-mately 10% in both the CEA andCAS groups. The rate of dis-abling stroke or death within 30days of first treatment was 6% inboth groups. Preliminary analy-sis of long-term survival showedno difference in the rate of ipsi-lateral stroke or any disablingstroke in patients up to 3 yearsafter randomization. The rates ofstroke or death within 30 daysin CAVATAS in both groups arehigher than many previous re-ports but not significantly differ-ent from the European CarotidSurgery Trialists (ECST) rate of7% (53). The 1-year restenosisrate was 20% for CAS and 5%for CEA. Cranial nerve injury(9%) and myocardial ischemia(1%) occurred at the time oftreatment in the CEA grouponly. Long-term follow-up is notyet available.
• The Wallstent Trial was an in-dustry supported prospective,randomized trial comparingCEA and CAS for symptomaticstenosis of 60% or more (81,82).This was an early study, per-formed without distal protectionand without the currently ac-cepted antiplatelet therapy. Inthis study, 219 patients withsymptomatic carotid stenosis of60%–90% diameter were ran-domized to CEA or stent place-ment. The technical success ratefor CAS was 97% (successful de-ployment with less than 30%residual stenosis). The risk ofany perioperative stroke ordeath was 4.5% for CEA and12.1% for CAS. At 1 year, therisk of a major stroke was 0.9%for CEA compared with 3.7% forCAS. This trial was stopped pre-maturely due to poor resultsfrom CAS.
• A single-center community hos-
AJNR: 24, November/December 2003 2023
pital study (83) randomized 104symptomatic patients to eitherCEA or CAS without distal pro-tection. Perioperative stroke ordeath rate was 2% for CEA and0% for CAS. Other complicationsfor the CEA group totaled 16%and included hematoma (requir-ing treatment), cranial/cervicalnerve injury, and hypotension(requiring treatment). Othercomplications for the CAS grouptotaled 45% and included tran-sient cerebral ischemia, leg am-putation, retroperitoneal hemor-rhage, bradycardia (requiringtemporary pacing), and hypoten-sion (requiring treatment).
• The SAPPHIRE trial randomized307 patients to CEA or CAS witha distal protection device. Peri-operative (30 days) results werepresented (Yadav J, presented atthe American Heart AssociationScientific Sessions, Chicago, No-vember 2002). The inclusion andexclusion criteria are listed inTable 2. Perioperative strokeand death rates were 7.3% forCEA and 4.4% for CAS. Totalmajor adverse event rate (death,any stroke, or myocardial infarc-tion) for CEA was 12.6% and forCAS was 5.8%. Rates of myocar-dial infarction were 7.3% forCEA and 2.6% for CAS. Of note,
the stroke or stroke/death ratefor asymptomatic patients was6.1% for CEA and 5.8% for CAS,both of which are worse thanmedical therapy alone in ACAS,and higher than the recom-mended AHA guidelines fortreatment, albeit in a differentpatient population.
CAS may have a role in the man-agement of some patients with sig-nificant stenoses of the extracranialcervical carotid artery. In addition,percutaneous endovascular therapyoffers a less invasive method of repairwith apparent reduction of nonneuro-logic morbidity. In the NASCETstudy, for example, reported compli-cation rates were 7.6% for cranialnerve palsies, 5.5% for wound hema-toma, 3.4% for wound infection, 0.9%for myocardial infarction, and 3.0% forother cardiac complications (9). Thesecomplications are virtually all relatedto the operative procedure, are nottrivial, and are rarely associated withCAS.
No large (more than 100 patients)currently reported carotid stent studyhas achieved periprocedural (as longas 30 days after the procedure) mor-bidity and mortality rates as low as thenatural history of medically treateduncomplicated asymptomatic carotidstenosis (80,84–88). In reported caseseries and registries of CAS, for exam-
ple, Roubin et al (84) reported an over-all stroke rate of 5.9% and a mortalityrate of 0.7%; Diethrich et al (86) re-ported a stroke rate of 10.9% and amortality rate of 1.7%; Wholey et al(87,88) reported a stroke rate of 4.4%and a mortality rate of 1.4% in theirinitial report and 4.2% and 0.9%, re-spectively, in their follow-up report.These results compare favorably withthe risk-to-benefit ratio of CEA forsymptomatic cervical carotid stenosisbut fall short of the intrinsically lowrisk of stroke for medically treatedasymptomatic disease. However, Jor-dan et al (89), analyzing the same pa-tients and data as did Roubin et al (84),reported a stroke rate of 12.7% and amortality rate of 1.1% for CAS. Inaddition, the durability of stents,stent restenosis rates, and long-termrates of subsequent stroke have notbeen determined. For these reasons,angioplasty and stent placement forasymptomatic carotid artery stenosisshould only be considered in specialcircumstances.
The National Institutes of Healthhas funded CREST to answer particu-lar questions pertaining to the safetyand efficacy of angioplasty and stentplacement at the cervical carotid bifur-cation and to clarify the specific indi-cations for this procedure. This trialwill compare CEA and CAS in pa-tients with a symptomatic severe ste-nosis (70% or more by ultrasonogra-phy or 50% by NASCET angiographiccriteria). It is important to note thatbecause CREST has inclusion/exclu-sion criteria similar to those ofNASCET, CREST is not designed toassess the safety and efficacy of stentplacement in patients known to be athigher risk of CEA.
C. Cerebral Protection Devices.—CAS is undergoing rapid evolution.An area of intense investigation isthe use of various protection devicesand techniques to prevent what isperceived to be the most commonand severe complication of the proce-dure: embolization of debris to thebrain. This recognition that distal em-bolization is the major complicationassociated with CAS has led to thedevelopment of numerous devicesdesigned to prevent distal emboliza-tion by proximal flow control, distalflow control, or distal particulate fil-tration (90). Several ongoing trials ofCAS have incorporated protection
Table 2Inclusion/Exclusion Criteria for the SAPPHIRE Trial of Carotid Stent Placement
InclusionAsymptomatic stenosis �80% or symptomatic stenosis �50% by angiography or
ultrasonography and at least one of the following conditions that wouldresult in high surgical risk:
Age �80 yearsCongestive heart failure (class III/IV) and/or left ventricular ejection fraction
�30%Open heart surgery needed within 6 weeksRecent myocardial infarction (�24 hours and �4 weeks)Unstable angina (CCS class III/IV)Severe chronic obstructive pulmonary diseaseContralateral carotid occlusionContralateral laryngeal nerve palsySevere tandem lesionsLesions distal or proximal to the usual locationPrevious endarterectomy with restenosisPrevious radiation therapy or radical neck surgery
ExclusionAcute ischemic neurologic event within past 48 hoursTotal occlusion of the target carotid arterySurgical or interventional procedure planned within the next 30 daysCommon carotid ostial lesion
AJNR: 24, November/December 20032024
devices in the study design (91–97),but no one device or type of devicehas been proved to be superior. Ametaanalysis of carotid stent place-ment series suggests that these pro-tective devices do actually reduce theincidence of periprocedure neuro-logic deficit (98), but the extent ofthis reduction remains to be deter-mined in a randomized, controlledtrial. The expectation is that these de-vices will potentially help to furtherdecrease the risk of CAS to the pointthat this procedure would be equalor superior to CEA (99,100). Recentdata also suggest their use is notwithout difficulty or potential com-plication (101,102). A prolonged“learning curve” may exist before re-alization of actual benefit, aboutwhich there is still controversy(101,102).
III. INDICATIONS ANDCONTRAINDICATIONS
Definitions: Severe stenosis is 70% orgreater diameter stenosis by NASCETmeasurement criteria. Preocclusive ste-nosis is 90% or greater diameter steno-sis by NASCET criteria or NASCETdefinition of “near occlusion” (9).
A. Acceptable Indications for CAS1. Symptomatic, severe stenosis
that is surgically difficult to ac-cess (eg, high bifurcation requir-ing mandibular dislocation)(103)
2. Symptomatic, severe stenosis ina patient with significant medi-cal disease that would make thepatient high risk for surgery(20–36,104–109, Table 2).
3. Symptomatic severe stenosisand one of the following condi-tions:a. Significant tandem lesion
that may require endovascu-lar therapy
b. Radiation-induced stenosis(110,111)
c. Restenosis after CEA(112,113)
d. Refusal to undergo CEA af-ter proper informed consent
e. Stenosis secondary to arte-rial dissection
f. Stenosis secondary to fibro-muscular dysplasia
g. Stenosis secondary to Taka-yasu arteritis (1,114)
4. Severe stenosis associated withcontralateral carotid artery oc-clusion requiring treatment be-fore undergoing cardiac surgery
5. Severe underlying carotid ar-tery stenosis revealed after re-canalization of carotid occlusionafter thrombolysis for acutestroke (presumed to be the eti-ology of the treated occlusion)or to enable thrombolysis foracute stroke
B. Relative Contraindications1. Asymptomatic stenosis of any
degree, except in particular cir-cumstances, as described above(A4, A6, A7)
2. Symptomatic stenosis associ-ated with an intracranial vascu-lar malformation
3. Symptomatic stenosis in a pa-tient with a subacute cerebralinfarction
4. Symptomatic stenosis in a pa-tient with a significant contrain-dication to angiography
C. Absolute Contraindications1. Carotid stenosis with angio-
graphically visible intraluminalthrombus
2. A stenosis that cannot be safelyreached or crossed by an endo-vascular approach
IV. QUALIFICATIONS ANDRESPONSIBILITIES OFPERSONNELA. Rationale for Cervicocerebral An-
giographic SkillOfficial standards of training
have existed for over a quarter cen-tury, are the hallmark of medicallicensure, board examinations andresidency programs, and are rec-ognized as vital by the ACGME,the Federation of State MedicalBoards of the United States, Inc.,the American Board of Medi-cal Specialties (ABMS), and theNational Board of Medical Exam-iners� (NBME�) (116–118). Stan-dards of training and for perfor-mance of medical and surgicalprocedures are necessary require-ments for the practice of medicine.The Joint Commission on Accredi-
tation of Healthcare Organizations(JCAHO) is working with twoother accrediting organizations,the National Committee for Qual-ity Assurance and URAC (former-ly known as the Utilization ReviewAccreditation Commission), on co-ordinating and aligning patientsafety standards. Medical societiesand accreditation committees rou-tinely formulate minimum stan-dards for the protection and safetyof patients, including those forboard accreditation, residencytraining and the practice of medi-cine. Examples of such standardsare those written by the AmericanCollege of Cardiology (ACC) forthe performance of coronary inter-vention (which require 300 coro-nary angiograms prior to coronaryintervention) (119–121) as well astraining and performance stan-dards specifically for peripheralvascular intervention (122,123).Standards of performance andtraining specifically for peripheralvascular intervention have alsobeen written by the AHA (124), theSociety of Cardiac Angiographyand Intervention (125), the Soci-ety of Interventional Radiology(126, 127) and the Society for Vas-cular Surgery (128). All trainingand performance standardsabove require substantial diag-nostic angiographic experienceprior to interventional practice inall vascular beds, typically 100angiograms (119 –128). Trainingstandards specifically for neuro-vascular intervention, includingcarotid artery stenting, were writ-ten by a multispecialty group andunanimously endorsed by eachexecutive committee of the Amer-ican Society of Neuroradiology,the American Society of Interven-tional and Therapeutic Neurora-diology, the American Associa-tion of Neurological Surgeons,the Congress of NeurologicalSurgeons (CNS) and the AANS/CNS Section on CerebrovascularSurgery (5). These neurointerven-tional training standards require100 cerebral angiograms as apre-requisite for entry into theACGME-approved residency/fellowship in Endovascular Sur-gical Neuroradiology.
The American College of Radi-
AJNR: 24, November/December 2003 2025
ology’s Standard of Practice forCervicocerebral Angiographywas formulated by a consensuspanel of ACR, ASITN, ASNR, andSIR members (4). Cervicocerebralangiography has a proven set ofindications, contraindications,risks, and benefits due to the factthat cervicocerebral catheteriza-tion is technically challengingand the organ supplied isuniquely vulnerable. The properand safe performance of a cere-bral angiogram is fundamental tothe performance of cervical CAS,just as diagnostic coronary an-giography skills have been reco-gized by the ACC as a pre-requi-site for coronary vascularintervention (119–121).
Stroke is the most feared of allmedical conditions and proceduralcomplications. For this reason, anyprocedure that has “stroke” as aroutine potential risk should beperformed only by medical profes-sionals with appropriate trainingand experience. The rate of strokeas a complication of diagnostic ce-rebral angiography in patientswith asymptomatic carotid steno-sis was approximately 1.2% inACAS; this may be greater than theactual risk of stroke caused by thestenosis itself for many patientswith asymptomatic stenosis (8,49).Importantly, it has been demon-strated that the amount of cervico-cerebral angiographic exerience isinversely related to proceduralcomplication rates, which translateinto temporary and permanentstrokes (129–133). Indeed, the ar-gument has been raised by bothvascular surgeons and neurolo-gists that cervicocerebral angiogra-phy, even performed by neurovas-cular specialists, may be toodangerous to be performed for theindication of asymptomatic carotidartery stenosis (134,135). Operatorrisk factors for stroke/transientischemic attack (TIA) complica-tions from cerebral angiographyare well known and include in-creased procedure and fluoros-copy time, increased number ofcatheters used, and performance ofarch aortography (130,131,136).Many of the above-mentioned fac-tors, including procedural timeand multiple catheter use, are not
independent and are typically re-lated to inexperience and lack ofspecific training. In several studies,neurological complications (strokeand TIA) occurred more frequentlywhen angiography was performedby a trainee or fellow rather thanby an experienced neuroradiolo-gist (130–132,134). A recent reporthas demonstrated that the rate ofstroke during cerebral angiogra-phy when performed by an appro-priately trained and experiencedspecialist is very low (137). How-ever, a separate published reportconfirms that physicians withoutformal training in catheter angiog-raphy did indeed experience alearning curve associated with anunacceptable complication ratethat decreased with angiographicexperience (130). A significantlearning curve has also been dem-onstrated for the carotid stent pro-cedure itself as well as the use ofcerebral embolic protection de-vices, thus necessitating appropri-ate training and experience in bothcomponents of the procedure: cer-vicocerebral angiography as wellas the carotid stent procedure(78,86,99–102).
B. Physician Qualifications For Ca-rotid Angioplasty And Stent Place-ment
1. The surgical team must possessparticular fundamental knowl-edge and skills for the appropri-ate application and safe perfor-mance of CAS; these include
a. A thorough knowledge ofcerebrovascular anatomy,hemodynamics, physiology,and pathophysiology
b. Sufficient knowledge of theclinical and imaging evalua-tion of patients with cerebro-vascular disorders to deter-mine those patients forwhom CAS is indicated; thisincludes thorough knowl-edge of the clinical mani-festations and the naturalhistory of cerebrovascularischemic disease
c. Appreciation of the benefitsand risks of CAS and the al-ternatives to the procedure,such as CEA and/or currentmedical therapy
d. Familiarity with pharma-ceutical agents potentiallyuseful during endovascularprocedures
e. The ability, skills, andknowledge to evaluate thepatient’s clinical status andto identify those patientswho may be at increasedrisk, who may require addi-tional pre- or postprocedurecare, or who have relativecontraindications to the pro-cedure; in particular, thephysicians must be capableof performing a clinical neu-rologic examination and un-derstanding any relevantfindings before, during, andafter the procedure
f. The capability to recognizeprocedure, neurologic, andangiographic complicationsrelated to the CAS pro-cedure; recognition of an-giographic complicationsnecessitates a thoroughknowledge of cerebrovascularanatomy and hemodynamics
g. The capability to provideappropriate endovascularmanagement of vascularcomplications related to theperformance of CAS, includ-ing appropriate treatment ofembolic complications
h. The capability to provide theinitial clinical managementof complications of CAS; ba-sic life support and treat-ment of cardiac arrhythmiasmust be immediately avail-able; in addition, the trainedpersonnel, equipment, andpharmacotherapeutics re-quired to identify and tomanage heart block, cardiacarrhythmias, and majorblood pressure fluctuationsmust also be immediatelyavailable
i. Adequate training in radia-tion physics and safety; thephysician team must be fa-miliar with the principles ofradiation biology, the haz-ards of radiation exposure toboth patients and medicalpersonnel, and radiationmonitoring requirements;such training and knowl-edge are important to maxi-
AJNR: 24, November/December 20032026
mize both patient and physi-cian safety
2. The requirements for meetingthe qualifications listed in(IV.B.1) may be met by obtain-ing the following training andexperience. This training maybe obtained through the appro-priate ACGME-approved resi-dency or fellowship (5,138) orthrough postgraduate experi-ence that should include a, b,and c below. The postgraduateexperiential training must beunder the supervision of a qual-ified physician, defined as aphysician who has already metthe qualifications of section IVwith acceptable indications andoutcomes.
a. Performance (under the su-pervision of a qualified phy-sician and with at least 50%performed as the primaryoperator) of at least 200 diag-nostic cervicocerebral an-giograms with documentedacceptable indications andoutcomes for physicianswith no prior catheter expe-rience (4,139), or at least 100diagnostic cervicocerebralangiograms with docu-mented acceptable indica-tions and outcomes for phy-sicians with experiencesufficient to meet the AHArequirements for peripheralvascular interventions (124).
b. Arterial stent experience aseither:
1. 25 non–carotid stentcomplete procedures,plus attendance at andcompletion of a “hands-on” course in per-formance of CAS, plusperformance and com-pletion of at least foursuccessful and uncom-plicated CAS proceduresas principal operator un-der the supervision of anon-site qualified physi-cian; this must be a com-prehensive course inwhich the attendees earnat least 16 hours of AMAcategory I continuingmedical education credit
OR2. Ten consecutive CAS
procedures as principaloperator under the super-vision of an on-site qual-ified physician on pa-tients treated forappropriate indicationsdocumented by a log ofcases performed andwith acceptable successand complication ratesaccording to the thresh-olds contained in thisguideline and the ACRguideline for cervicoce-rebral angiography(4,78,86)
c. Substantiation in writing bythe director of the depart-ment, the chief of the medi-cal staff, or the chair of thecredentials committee of theinstitution in which thetraining procedures wereperformed and the institu-tion in which privileges willbe granted that the surgicalteam is familiar with all ofthe following:1. Indications and contra-
indications for CAS2. Preprocedural assess-
ment and intraproce-dural physiologic, cere-brovascular, andneurologic monitoring ofthe patient
3. Appropriate use andoperation of fluoro-scopic and radiographicequipment and digitalsubtraction angiogra-phy systems
4. Principles of radiationprotection, hazards ofradiation exposure tothe patient and to theradiologic personnel,and radiation monitor-ing requirements
6. Pharmacology of con-trast agents and cardiacantiarrhythmia drugs andrecognition and treatmentof adverse reactions tothese substances
7. Recognition and treat-ment of cardiac arrhyth-mias associated withCAS
8. Technical aspects of per-forming CAS
9. Recognition of any cere-brovascular abnormalityor complication relatedto the CAS procedure
10. Postprocedural patientmanagement, particu-larly the recognition andinitial management ofprocedure complications
Maintenance of competence re-quires continuing activity including
1. Regular performance of suffi-cient numbers of neurovascularprocedures to maintain successand complication rates as out-lined below
2. Participation in a quality im-provement program that moni-tors these rates
3. Participation in courses thatprovide continuing educationon advances in CAS
4. Continuing education should bein accordance with the ACRStandard for ContinuingEducation
V. SPECIFICATIONS OF THEPROCEDURE
A. Technical RequirementsThere are several technical require-ments that are necessary to ensurethe safe and successful perfor-mance of CAS. These includeadequate clinical facilities, angio-graphic and monitoring equip-ment, and support personnel. Theminimal facility requirements are1. An angiographic suite with suf-
ficient space to allow posi-tioning of patient-monitoringequipment and anesthesiaequipment, while leaving ade-quate room for the circulatingstaff to move without contami-nating the sterile field
2. A high-resolution image inten-sifier and imaging chain withthe ability to acquire and storeimages digitally; imaging andrecording must be consistentwith the as low as reasonablyachievable (ALARA) radiationsafety guidelines
AJNR: 24, November/December 2003 2027
3. Immediate access to computedtomography or magnetic reso-nance imaging to allow eval-uation of any suspected com-plication (eg, intracranialembolization)
4. Adequate physiologic monitor-ing equipment for use duringand after the procedure, includ-ing equipment for cardiopulmo-nary resuscitation and tempo-rary cardiac pacing
B. Emergency SupportThere should be prompt access tomedical, surgical, and interven-tional personnel and resourcesneeded for management of medi-cal or surgical complications.
C. Patient Care1. Preprocedural care
a. The history and indicationsfor the procedure must be re-corded in the patient’s med-ical record; relevant medica-tions, allergies, and bleedingdisorders should be noted
b. The vital signs and physical(general and neurologic)examination must bedocumented
c. Neurologic assessment mustinclude documentation ofthe National Institutes ofHealth Stroke Scale (NIHSS)(140)
2. Procedural carea. Vital signs should be ob-
tained and recorded at regu-lar intervals during thecourse of the procedure
b. Cardiac rhythm should bemonitored continuously
c. Intravenous access must beavailable for administrationof fluids and drugs
d. If the patient is to receiveconscious sedation, pulseoximetry must be used;administration of sedationshould be in accordance withthe ACR Standard for Con-scious Sedation; anesthesiapersonnel, a registerednurse, or other appropriatelytrained personnel should bepresent and have primary re-sponsibility for monitoringthe patient; all medicationdoses and times should berecorded
e. Neurologic deteriorationshould be documented andquantified by the NIHSS
3. Postprocedural care
a. A procedure note must bewritten in the patient’s med-ical record summarizing theprocedure, any immediatecomplications, and the pa-tient’s status at the end of theprocedure; this informationshould be communicated tothe referring physician assoon as possible; the notemay be brief if the formal re-port will be dictated andavailable the same day
b. All patients should be care-fully observed during thepostprocedure period; thepatient’s vital signs and neu-rologic examination, alongwith the status of the punc-ture site and the peripheralpulses should be monitoredat regular intervals by anurse or other qualifiedpersonnel
c. The physician performingthe procedure or a qualifieddesignee (physician ornurse) should evaluate thepatient after the initial post-procedure period; these find-ings should be recorded in aprogress note in the patient’smedical record; the physi-cian and/or designee shouldbe available for continuingcare before and after the pa-tient’s discharge from thehospital
d. Neurologic assessment mustinclude documentation ofthe NIHSS
VI. EQUIPMENT QUALITYCONTROL
The facility must have documentedpolicies and procedures for monitor-ing and evaluating the effective man-agement, safety, and proper perfor-mance of imaging and interventionalequipment. The quality control pro-gram should maximize the quality ofthe diagnostic information. This maybe accomplished as part of a routinepreventive maintenance program.
VII. DOCUMENTATION
A. Informed Consent and ProcedureRisk.—Informed consent must be ob-tained in compliance with institu-tional policy and state law. The phy-sician should be committed to thePrinciples of Medical Ethics and theopinions on clinical investigation, in-formed consent, and prescribing ofdrugs and devices as stated in theCode of Medical Ethics of the Coun-cil on Ethical and Judicial Affairs ofthe American Medical Association(141). Risks cited should include in-fection, bleeding, allergic reaction tocontrast, cardiac arrhythmia, stroke,and death. The potential need foremergency treatment of complica-tions should be discussed. The rela-tive risks and benefits of medicaltherapy and/or CEA should also bediscussed.
B. Documentation.—The results ofall CAS procedures should be moni-tored on a continuous basis. Recordsshould be kept of immediate andlong-term results and complications.The number and types of complica-tions should be documented.
A permanent record of each proce-dure should be maintained (conven-tional film or digital media); labelingshould include facility name, patientname, identification number and/ordate of birth, and examination date.
The physician’s report should in-clude the procedure undertaken,method of anesthesia, specific bal-loons and stents used, and immediatecomplications, if any (including treat-ment and outcome). Reporting shouldbe in accordance with the ACR Stan-dard on Communication.
At least 30 days of clinical fol-low-up is necessary to obtain the nec-essary data for proper quality assur-ance. A permanent record of thepatient’s neurologic status before andafter treatment must be maintained.The long-term outcome and any de-layed complications (including treat-ment and response) must be recorded.Restenosis after CAS may occur as itmay after CEA. Therefore, long-termfollow-up of vessel patency with non-invasive imaging is recommended 6,12, 18, and 24 months after treatment(142).
AJNR: 24, November/December 20032028
VIII. THRESHOLDS, SUCCESSAND COMPLICATION RATES
There is insufficient information todefine technical success scientifically.For extremity and renal angioplasty,technical success requires less than30% diameter residual stenosis byangiography and may require im-provement in transstenotic pressuregradient (143,144). In the coronary lit-erature, technical success for balloonangioplasty and stent placement hadoriginally been defined as 20% relativeimprovement with a decrease in steno-sis to less than 50%, but it has recentlybeen revised to a decrease in stenosisto less than 20% (119,120). However,unlike extremity, renal, or coronarystenoses, carotid stenoses are veryrarely symptomatic due to hemody-namic compromise. Rather, symptomsarise from embolization from a carotidplaque. It is unknown what degree ofcorrection of carotid stenosis is neces-sary to reduce the risk of embolization,but removal of the embolic source isfundamental. It is possible that in theattempt to more completely eliminateresidual stenosis by full balloon dila-tion, additional emboli may be pro-duced during the procedure that couldcause a higher risk of procedure com-plications. Alternatively, leaving ahigher degree of residual stenosis maylead to a higher rate of late restenosis,which at this time is of uncertain clin-ical significance. Some carotid stentplacement trials have defined techni-cal success as residual stenosis of lessthan 30% (Yadav J, presented at theAmerican Heart Association ScientificSessions, Chicago, November 2002).Others have used a definition of resid-ual stenosis of less than 50% (Eles G,The ARCHeR Trial, presented at theSIR Annual Scientific Meeting, SaltLake City, UT, March 2003). In the ab-sence of definitive scientific evidence,technical success in this document is ar-bitrarily defined as stent placement re-sulting in improvement of the stenosisby 20% or more with a final residualstenosis of less than 50% with NASCETmeasurement criteria. Some practicesmay prefer to use a lesser degree of re-sidual stenosis as their desired endpointfor technical success.
As with many endovascular andsurgical techniques, there is a learningcurve associated with CAS. Complica-tions will be more frequent when the
procedure is performed by less expe-rienced practitioners. This phenome-non is also recognized with the perfor-mance of CEA as well as coronaryintervention. To account for the levelof physician experience, an ad hoccommittee of the AHA Stroke Council(145) proposed that a “beginning sur-geon be assigned 100 trouble-freecases as a theoretical statistical basis.”For example, 75 cases would be addedproportionately by indication catego-ries to a beginning surgeon’s 25 casesto form a statistical basis of 100 totalcases. The number of trouble-freecases is decreased by the number ofreal cases performed until the practi-tioner has actually performed 100cases. With this system, a new physi-cian would be considered to have a 5%complication rate, rather than 50%, ifhe or she had complications with fiveof the first 10 cases. This concept ap-pears to be a valid method to accountfor physician inexperience. Becausewe have recommended relatively highthresholds (see Table 3) for the com-plications associated with CAS, thenumber of trouble-free cases assignedto a new physician should be less thanthe 100 cases used for evaluation ofCEA. Otherwise, excessive complica-tions might continue without trigger-ing a review. For the performance ofCAS, 30 trouble-free cases will be as-signed (in both the asymptomatic andsymptomatic patient categories) tonew physicians for initial statisticalanalysis that will be performed as de-scribed in the AHA document.
Previous reports of experience withCAS have described complications,particularly neurologic, in an inconsis-tent and nonstandardized fashion. Werecognize the need for more detailed,clinically relevant, and uniform out-come measures. Both the duration andseverity of neurologic complicationsare important. The necessity for signif-icant postoperative interventions, suchas emergency thrombolytic therapy, isalso thought to be important. How-ever, defining precisely what wouldconstitute a “significant” posttreat-ment intervention would be difficult,as would reporting and analyzing allsuch interventions. Use of the NIHSSfacilitates rapid and uniform assess-ment of neurologic complications. Inaddition, the NIHSS may serve as areasonable surrogate measure for sig-nificant posttreatment interventions.
The rationale for using the NIHSS forthis purpose is that small increases inthe NIHSS are thought to be much lesslikely to result in significant interven-tions, including repeated angiographyand thrombolytic therapy. Therefore,adoption of the NIHSS as a standardoutcome measure will allow uniformassessment of complications and ap-proximate the incidence of significantpostoperative interventions. Differen-tiation between outcomes and compli-cations in patients with asymptomaticversus symptomatic arterial stenosesis critical. The natural history of thetwo groups of patients differs dramat-ically, with much lower risk of strokein asymptomatic patients. As withCEA, the risks associated with CASappear to be lower in asymptomaticpatients and the risk-to-benefit ratiofor CAS appears to be significantly dif-ferent for asymptomatic versus symp-tomatic patients.
Definitions.—Neurologic complica-tion: neurologic deterioration evi-denced by an increase in the NIHSSscore of one or more points
Transient deficit: a neurologic com-plication having complete resolutionwithin 24 hours
Reversible stroke: a neurologic com-plication having a duration of morethan 24 hours and up to 30 days
Permanent stroke: a neurologic com-plication having a duration of morethan 30 days
Minor deficit: neurologic deteriora-tion evidenced by an increase of theNIHSS score of less than four pointswithout the presence of aphasia orhemianopsia
Major deficit: neurologic deteriora-tion evidenced by an increase of theNIHSS score of four or more points orthe presence of aphasia or hemianopsia
Technical success: inflation of angio-plasty balloon/placement of stent inthe carotid stenosis with improvementof the stenosis by 20% or more with afinal residual stenosis of less than 50%using NASCET measurement criteria
While practicing physicians shouldstrive to achieve perfect outcomes (eg,100% success, 0% complications), inpractice, all physicians will fall shortof this ideal to a variable extent. Thus,indicator thresholds may be used toassess the efficacy of ongoing qualityimprovement programs. For the pur-pose of these guidelines, a threshold isa specific level of an indicator that
AJNR: 24, November/December 2003 2029
should prompt a review. When mea-sures such as indications or successrates fall below a (minimum) thresh-old or when complication rates exceeda (maximum) threshold, a reviewshould be performed to determine
causes and to implement changes, ifnecessary. Routine periodic review ofall cases having less than perfect out-comes is strongly encouraged. Intra-cranial embolization and subsequentstroke are the major complications as-
sociated with CAS (60–88). A reviewmay be triggered when the thresholdvalues described in Table 3 are ex-ceeded. The thresholds were derivedfrom critical evaluation of the litera-ture and evaluation of empirical datafrom the committee members’ prac-tices. Consensus on statements in thisdocument was obtained with a modi-fied Delphi technique (1,2).
IX. QUALITY CONTROL ANDIMPROVEMENT, SAFETY,INFECTION CONTROL, ANDPATIENT EDUCATIONCONCERNS
Policies and procedures related toquality, patient education, infectioncontrol, and safety should be devel-oped and implemented in accordancewith the ACR Policy on Quality Con-trol and Improvement, Safety, Infec-tion Control, and Patient EducationConcerns.
These data should be used in con-junction with the thresholds describedin Section VIII to assess angioplastyand stent placement at the cervical ca-rotid bifurcation procedural efficacyand complication rates and, as definedin that section, to trigger institutionalreview when the thresholds defined inthat section are exceeded.
Acknowledgment: Grateful acknowledg-ment is given to Tricia McClenny withoutwhose tireless efforts this document wouldnot have been completed.
References1. Fink A, Kosefcoff J, Chassin M, Brook
RH. Consensus methods: character-istics and guidelines for use. Am JPublic Health 1984; 74:979–983.
2. Leape LL, Hilborne LH, Park RE, et al.The appropriateness of use of coronaryartery bypass graft surgery in NewYork State. JAMA 1993; 269:753–760.
3. Connors JJ 3rd, Seidenwurm D,Wojak JC, et al. Treatment of athero-sclerotic disease at the cervical carotidbifurcation: Current status and re-view of the literature. AJNR Am JNeuroradiol 2000; 21:444–450.
4. American College of Radiology. Stan-dard for the performance of diagnos-tic cervicocerebral angiography inadults. In: American College of Ra-diology Standards 2000–2001. Reston,VA: American College of Radiology,2000;415–426.
5. Higashida RT, Hopkins LN, Beren-stein A, et al. Program requirementsfor Residency Fellowship Education
Table 3Thresholds for Indications, Technical Success, and Complications
IndicationsMeets the indications listed in section III.A 95%
Technical success 90%
Inappropriate comparison of the thresholds in this table to the reported incidencesof complications after CEA might lead to an erroneous conclusion that higherrates of neurologic complications are acceptable for CAS compared with lowerrates for CEA: (a) A “threshold” is not intended to represent a desirable incidenceof complications. A “threshold” implies a complication rate that is significantlyabove the expected rate of complications, such that an audit should be conducted toexamine the cause of the unexpectedly high incidence of complications. (b) Thesethresholds are significantly higher than the complication rates for CEA published inthe randomized ACAS and NASCET trials. Those trials included only low-riskpatients. The thresholds in this document pertain only to high-risk patients. Exceptfor patients treated as part of an approved investigational trial, patients consideredto have normal risk of CEA do not fall within the acceptable indications for carotidartery angioplasty and stent placement as defined in this document. (c) Thethresholds described in this document are comparable with the incidences ofcomplications resulting from CEA performed on similar high-risk patients. (d) Thethresholds described in this document do not apply to low-risk patients treatedunder an approved investigational trial. Lower thresholds, comparable with thewell-established experience with CEA in low-risk patients, would apply for CASperformed under these conditions. (e) The definitions for the neurologiccomplications on which these thresholds are based differ from those used in manyreported series. No accepted, standardized methodology for reporting all neurologiccomplications exists. The neurologic complications defined in this document shouldbe applicable to a broad range of cerebrovascular interventions and surgery. (f) Thethresholds described in this document reflect complications occurring within 30days of CAS, not immediate postoperative results. (g) Thresholds for the reversiblestroke categories are based on the expectation that reversible deficits are likely to beslightly more common than permanent strokes. We recognize that there is not yetadequate scientific literature to confirm this.* At present, there are minimal and insufficient data available to suggest thresholdvalues for transient deficits after CAS. We believe that these data should becollected and reported to further our understanding of CAS and, perhaps, to help todecrease the incidence of permanent neurologic complications. When adequate dataabout transient neurologic complications become available, this document will berevised to include threshold values for such transient complications.† All deaths should be reviewed.
AJNR: 24, November/December 20032030
in Neuroendovascular Surgery/Inter-ventional Neuroradiology: A SpecialReport on Graduate Medical Educa-tion. AJNR 2000; 21:1153–1159.
6. Roubin GS, Hobson RW 2nd, White R,et al. CREST and CARESS to evalu-ate carotid stenting: time to get towork! J Endovasc Therapy 2001;8:107–110.
7. Veith FJ, Amor M, Ohki T, et al.Current status of carotid bifurcationangioplasty and stenting based on aconsensus of opinion leaders. J VascSurg 2001; 33(suppl 2):S111–S116.
8. Executive Committee for the Asymp-tomatic Carotid AtherosclerosisStudy. Endarterectomy for asymp-tomatic carotid artery stenosis. JAMA1995; 273:1421–1428.
9. North American Symptomatic Ca-rotid Endarterectomy Trial Collabora-tors. Beneficial effect of carotid end-arterectomy in symptomatic patientwith high-grade carotid stenosis.N Engl J Med 1991; 325:445–508.
10. Rothwell PM, Eliasziw M, GutnikovSA, et al for the Carotid Endarterec-tomy Trialists’ Collaboration. Anal-ysis of pooled data from the random-ised controlled trials of endarterectomyfor symptomatic carotid stenosis. Lan-cet 2003; 361:107–116.
11. Hobson RW II, Weiss DG, Fields WS,et al. Efficacy of carotid endarterec-tomy for asymptomatic carotid steno-sis. The Veterans Affairs CooperativeStudy Group. N Engl J Med 1993; 328:221–227.
12. Mayo Asymptomatic Carotid Endar-terectomy Study Group. Results of arandomized controlled trial of carotidendarterectomy for asymptomatic ca-rotid stenosis. Mayo Clin Proc 1992;67:513–518.
15. Barnett HJ, Taylor DW, Eliasziw M, etal. Benefit of carotid endarterectomyin patients with symptomatic moder-ate or severe stenosis. N Engl J Med1998; 339:1468–1471.
16. Moore WS, Kempczinski RF, NelsonJJ, Toole JF. Recurrent carotid steno-sis: results of the asymptomatic ca-rotid atherosclerosis study. Stroke1998; 29:2018–2025.
17. Sundt TM Jr, Whisnant JP, HouserOW, Fode NC. Prospective study ofthe effectiveness and durability of ca-rotid endarterectomy. Mayo Clin Proc1990; 65:625–635.
18. Chaturverdi S, Aggarwal R, Muru-gappan A. Results of carotid endar-
terectomy with prospective neurolo-gist follow-up. Neurology 2000; 55:769–772.
19. Barnett HJM, Broderick P. Carotidendarterectomy: another wake-up call.Neurology 2000; 55:746–747.
20. Wennberg DE, Lucas FL, BirkmeyerJD, et al. Variation in carotid endar-terectomy mortality in the Medicarepopulation: trial hospitals, volume,and patient characteristics. JAMA1998; 279:1278–1281.
21. Wong JH, Findlay JM, Suarez-Alma-zoor ME. Regional performance ofcarotid endarterectomy: Appropriate-ness, outcomes, and risk factors forcomplications. Stroke 1997; 28:891–898.
22. Sundt TM Jr, Sandok BA, WhisnantJP. Carotid endarterectomy: compli-cations and preoperative assessmentof risk. Mayo Clin Proc 1975; 50:301–306.
23. Brook RH, Park RE, Chassin MR, et al.Carotid endarterectomy for elderlypatients: predicting complications.Ann Intern Med 1990; 113:747–753.
24. Paciaroni M, Eliasziw M, Kappelle LJ,et al. Medical complications associ-ated with carotid endarterectomy.North American Symptomatic CarotidEndarterectomy Trial (NASCET).Stroke 1999; 30:1759–1763.
25. Jordan WD, Jr, Roye GD, Fisher WS3rd, et al. A cost comparison of bal-loon angioplasty and stenting versusendarterectomy for the treatment ofcarotid artery stenosis. J Vasc Surg1998; 27:16–22.
26. Hill BB, Olcott C, Dalman RL, et al.Reoperation for carotid stenosis is assafe as primary carotid endarterec-tomy. J Vasc Surg 1999; 30:26–35.
28. Rothwell PM, Slattery J, Warlow CP.Clinical and angiographic predictorsof stroke and death from carotid end-arterectomy: systematic review. BMJ1997; 315:1571–1577.
36. Gasecki AP, Eliasziv M, Ferguson GG,et al for the North American Symp-tomatic Carotid Endarterectomy Trial(NASCET) Group. Long term prog-nosis and effect of endarterectomy inpatients with symptomatic severe ca-rotid stenosis or occlusion: resultsfrom NASCET. J Neurosurg 1995; 83:778–782.
37. Brown KR, Kresowik TF, Chin MH, etal. Multistate population-based out-comes of combined carotid endarter-ectomy and coronary artery bypass. JVasc Surg 2003; 37:32–39.
38. Gasparis AP, Ricotta L, Cuadra SA, etal. High-risk carotid endarterecto-my: fact or fiction. J Vasc Surg 2003;37:40–46.
40. Clase CM, Cina CS. Medical man-agement versus investigate-and-oper-ate strategy in asymptomatic carotidstenosis: a decision analysis. J VascSurg 2002; 36:541–548.
41. Aburahma AF, Thiele SP, Wulu JT Jr.Prospective controlled study of thenatural history of asymptomatic 60%to 69% carotid stenosis according toultrasonic plaque morphology. J VascSurg 2002; 36:437–442.
42. Barnett HJ, Meldrum HE, Eliasziw Mfor the North American SymptomaticCarotid Endarterectomy Trial(NASCET) collaborators. The ap-propriate use of carotid endarterec-tomy. CMAJ 2002; 166:1169–1179.
43. Gaudino M, Glieca F, Luciani N, et al.Should severe monolateral asymp-tomatic carotid artery stenosis betreated at the time of coronary arterybypass operation? Eur J CardiothoracSurg 2001; 19:619–626.
44. Barnett HJ, Meldrum HE. Endarter-ectomy for carotid stenosis: new ap-proaches in patient selection. Cere-brovasc Dis 2001; 11(suppl 1):105–111.
AJNR: 24, November/December 2003 2031
45. Longstreth WT, Shemanski L,Lefkowitz D, et al. Asymptomaticcarotid artery stenosis defined by ul-trasound and the risk of subsequentstroke in the elderly. The Cardiovas-cular Health Study. Stroke 1998; 29:2371–2376.
46. Baker WH, Howard VJ, Howard G,Toole JF. Effect of contralateral oc-clusion on long-term efficacy of end-arterectomy in the asymptomatic ca-rotid atherosclerosis study (ACAS).ACAS Investigators. Stroke 2000; 31:2330–2334.
47. Chaturvedi S, Meinke JL, St Pierre E,Bertasio B. Attitudes of Canadianand U.S. neurologists regarding ca-rotid endarterectomy for asymptom-atic stenosis. Can J Neurol Sci 2000;27:116–119.
48. Chambers BR, You RX, Donnan GA.Carotid endarterectomy for asymp-tomatic carotid stenosis. CochraneDatabase Syst Rev 2000; (2):CD001923.
49. Olin JW, Fonseca C, Childs MB, et al.The natural history of asymptomaticmoderate internal carotid artery ste-nosis by duplex ultrasound. VascMed 1998; 3:101–108.
50. Irvine CD, Cole SE, Foley PX, et al.Unilateral asymptomatic carotid dis-ease does not require surgery. Eur JVasc Endovasc Surg 1998; 16:245–253.
51. Chaturvedi S, Halliday A. Is anotherclinical trial warranted regarding end-arterectomy for asymptomatic carotidstenosis? Cerebrovasc Dis 1998;8:210–213.
52. Schneider JR. Which asymptomaticpatients should have carotid endarter-ectomy? Semin Vasc Surg 1998; 11:12–18.
53. European Carotid Surgery TrialistsCollaborative Group. Risk of strokein the distribution of an asymptom-atic carotid artery. Lancet 1995; 345:209–212.
54. Rockman CB, Riles TS, Lamparello PJ,et al. Natural history and manage-ment of the asymptomatic, moder-ately stenotic internal carotid artery. JVasc Surg 1997; 25:423–431.
55. Hennerici M, Hulsbomer HB, HefterH, et al. Natural history of symp-tomatic extracranial arterial disease.Results of a long term prospectivestudy. Brain 1987; 110(pt 3):777–791.
56. Chambers BR, Norris JW. Outcomein patients with asymptomatic neckbruits. N Engl J Med 1986; 315:860–865.
57. Inzitari D, Eliasziw M, Gates P, et al.The causes and risk of stroke in pa-tients with asymptomatic internal-ca-rotid-artery stenosis. North AmericanSymptomatic Carotid Endarterec-
tomy Trial Collaborators. N EnglJ Med 2000; 342:1693–1700.
58. Gebel JM, Brott TG, Howard VJ, et al.Brain injury as detected by computer-ized tomography in CT scan in ACAS(abstr). Stroke 2003; 34:238.
59. Biller J, Feinberg WM, Castaldo JE, etal. Guidelines for carotid endarter-ectomy: a statement for HealthcareProfessionals from a Special WritingGroup of the Stroke Council, Ameri-can Heart Association. Stroke 1998;29:554–562.
60. Perry JR, Szalai JP, Norris JW. Con-sensus against both endarterectomyand routine screening for asymptom-atic carotid artery stenosis. CanadianStroke Consortium. Arch Neurol1996; 54:25–28.
62. Yadav JS, Roubin GS, Iyer S, et al.Elective stenting of the extracranialcarotid arteries. Circulation 1997; 95:376–381.
63. Yadav JS, Roubin GS, King P, et al.Angioplasty and stenting for resteno-sis after carotid endarterectomy.Stroke 1996; 27:2075–2079.
64. Theron J, Raymond J, Casasco A,Courtheoux F. Percutaneous angio-plasty of atherosclerotic and postsur-gical stenosis of carotid arteries.AJNR Am J Neuroradiol 1987; 8:495–500.
65. Tsai FY, Matovich V, Hieshima G, etal. Percutaneous transluminal an-gioplasty of the carotid artery. AJNRAm J Neuroradiol 1986; 7:349–358.
66. Kachel R, Basche ST, Heerkoltz I, et al.Percutaneous transluminal angio-plasty (PTA) of supra-aortic arteriesespecially the internal carotid artery.Neuroradiology 1991; 33:191–194.
67. Bockenheimer AM, Mathias K. Per-cutaneous transluminal angioplastyin arteriosclerotic internal carotid ar-tery stenosis. AJNR Am J Neuroradiol1993; 4:791–792.
69. Courtheoux P, Theron J, Tournade A,et al. Percutaneous endoluminal an-gioplasty of post endarterectomy ca-rotid stenoses. Neuroradiology 1987;29:186–189.
70. Wiggi U, Gratzl O. Transluminal an-gioplasty of stenotic carotid arteries:case reports and protocol. AJNR Am JNeuroradiol 1983; 4:793–795.
71. Shawl FA, Efstratiou A, Hoff S,Dougherty K. Combined percutane-ous carotid stenting and coronary an-
gioplasty during acute ischemic neu-rologic and coronary syndromes.Am J Cardiol 1996; 77:1109–1112.
72. Gil-Peralta A, Mayol A, Marcos JRG,et al. Percutaneous transluminal an-gioplasty of the symptomatic athero-sclerotic carotid arteries. Stroke 1996;27:2271–2273.
73. Marks MP, Dake MD, Steinberg GK,et al. Stent placement for arterialand venous cerebrovascular disease:preliminary experience. Radiology1994; 191:441–446.
74. Al-Mubarak N, Roubin GS, Vitek JJ, etal. Procedural safety and short-termoutcome of ambulatory carotid stent-ing. Stroke 2001; 32:2305–2309.
75. Baudier JF, Licht PB, Roder O,Andersen PE. Endovascular treat-ment of severe symptomatic stenosisof the internal carotid artery: earlyand late outcome. Eur J Vasc Endo-vasc Surg 2001; 22:205–210.
76. Kirsch EC, Khangure MS, van SchieGP, et al. Carotid arterial stentplacement: results and follow-up in53 patients. Radiology 2001; 220:737–744.
77. Dietz A, Berkefeld J, Theron JG, et al.Endovascular treatment of symptom-atic carotid stenosis using stent place-ment: long-term follow-up of patientswith a balanced surgical risk/benefitratio. Stroke 2001; 32:1855–1859.
78. Roubin GS, New G, Iyer SS, et al.Immediate and late clinical outcomesof carotid artery stenting in patientswith symptomatic and asymptomaticcarotid artery stenosis: a 5-year pro-spective analysis. Circulation 2001;103:532–537.
79. Bergeron P, Becquemin JP, JausseranJM, et al. Percutaneous stenting ofthe internal carotid artery: the Euro-pean CAST I Study. Carotid ArteryStent Trial. J Endovasc Surg 1999;6:155–159.
80. Endovascular versus surgical treat-ment in patients with carotid stenosisin the Carotid and Vertebral ArteryTransluminal Angioplasty Study(CAVATAS): a randomised trial. Lan-cet 2001; 357:1729–1737.
81. Alberts MJ, McCann R, Smith TP, etal. A randomized trial of carotidstenting vs. endarterectomy in pa-tients with symptomatic carotid ste-nosis: study design. J Neurovasc Dis1997; 2:228–234.
82. Alberts MJ for the PublicationsCommittee of the Wallstent Trial. Re-sults of a multicenter prospective ran-domized trial of carotid artery stent-ing vs carotid endarterectomy (abstr).Stroke 2001; 32:325.
83. Brooks WH, McClure RR, Jones MR,et al. Carotid angioplasty and stent-ing versus carotid endarterectomy:
AJNR: 24, November/December 20032032
randomized trial in a community hos-pital. J Am Coll Cardiol 2001; 38:1589–1595.
85. Kachel R. Results of balloon angio-plasty in the carotid arteries. J Endo-vasc Surg 1996; 3:22–30.
86. Diethrich EB, Ndiaye M, Reid DB, etal. Stenting in the carotid artery: ini-tial experience in 110 patients. J Endo-vasc Surg 1996; 3:42–62.
87. Wholey MH, Wholey M, Bergeron P,et al. Current global status of carotidartery stent placement. Catheter Car-diovas Diagn 1998; 44:1–6.
88. Wholey MH, Wholey M, Mathias K, etal. Global experience in cervical ca-rotid artery stent placement. CatheterCardiovasc Interv 2000; 50:160–167.
89. Jordan WD Jr, Voellinger DC, FisherWS, et al. A comparison of carotidangioplasty with stenting versus end-arterectomy with regional anesthesia.J Vasc Surg 1998; 28:397–403.
90. Ohki T, Veith FJ. Carotid stentingwith and without protection devices:should protection be used in all pa-tients? Semin Vasc Surg 2000; 13:144–152.
92. Castriota F, Cremonesi A, Manetti R,et al. Impact of cerebral protectiondevices on early outcome of carotidstenting. J Endovasc Ther 2002; 9:786–792.
94. Henry M, Henry I, Klonaris C, et al.Benefits of cerebral protection duringcarotid stenting with the PercuSurgeGuardWire system: Midterm results. JEndovasc Ther 2002; 9:1–13.
95. Al-Mubarak N, Colombo A, GainesPA, et al. Multicenter evaluation ofcarotid artery stenting with a filterprotection system. J Am Coll Cardiol2002; 39:841–846.
96. Parodi JC, La Mura R, Ferreira LM, etal. Initial evaluation of carotid an-gioplasty and stenting with three dif-ferent cerebral protection devices. JVasc Surg 2000; 32:1127–1136.
97. Henry M, Amor M, Henry I, et al.Carotid stenting with cerebral protec-tion: first clinical experience using thePercuSurge GuardWire system. J En-dovasc Surg 1999; 6:321–331.
98. Kastrup A, Groschel K, Krapf H, et al.
Early outcome of carotid angioplastyand stenting with and without cere-bral protection devices: a systematicreview of the literature. Stroke 2003;34:813–819.
99. Angelini A, Reimers B, Della BarberaM, et al. Cerebral protection duringcarotid artery stenting: collection andhistopathologic analysis of embolizeddebris. Stroke 2002; 33:456–461.
100. Al-Mubarak N, Roubin GS, Vitek JJ, etal. Effect of the distal-balloon pro-tection system on microembolizationduring carotid stenting. Circulation2001; 104:1999–2002.
101. Cremonesi A, Manetti R, Setacci F, etal. Protected carotid stenting: Clini-cal advantages and complications ofembolic protection devices in 442 con-secutive patients. Stroke 2003;34:1936–1941.
102. Eckert B, Zeumer H. Editorial com-ment. Carotid artery stenting with orwithout protection devices: Strongopinions, poor evidence? Stroke 2003;34:1941.
103. Dangas G, Laird JR Jr, Mehran R, et al.Carotid artery stenting in patientswith high-risk anatomy for carotidendarterectomy. J Endovasc Therapy2001; 8:39–43.
104. Paniagua D, Howell M, Strickman N,et al. Outcomes following extracra-nial carotid artery stenting in high-risk patients. J Invasive Cardiol 2001;13:375–381.
105. Ouriel K, Hertzer NR, Beven EG, et al.Preprocedural risk stratification: iden-tifying an appropriate population forcarotid stenting. J Vasc Surg 2001; 33:728–732.
106. Malek AM, Higashida RT, PhatourosCC, et al. Stent angioplasty for cer-vical carotid artery stenosis in high-risk symptomatic NASCET-ineligiblepatients. Stroke 2000; 31:3029–3033.
107. Shawl F, Kadro W, Domanski MJ, etal. Safety and efficacy of elective ca-rotid artery stenting in high-risk pa-tients. J Am Coll Cardiol 2000;35:1721–1728.
108. Mericle RA, Kim SH, Lanzino G, et al.Carotid artery angioplasty and use ofstents in high-risk patients with con-tralateral occlusions. J Neurosurg1999; 90:1031–1036.
109. Lopes DK, Mericle RA, Lanzino G, etal. Stent placement for the treatmentof occlusive atherosclerotic carotid ar-tery disease in patients with concom-itant coronary artery disease. J Neuro-surg 2002; 96:490–496.
110. Houdart E, Mounayer C, Chapot R, etal. Carotid stenting for radiation-in-duced stenoses: a report of 7 cases.Stroke 2001; 32:118–121.
111. Al-Mubarak N, Roubin GS, Iyer SS, etal. Carotid stenting for severe radia-
114. Wang Z, Shen L, Yu J, et al. Manage-ment of cerebral ischemia due toTakayasu’s arteritis. Chin Med J 2002;115:342–346.
115. Coldwell DM, Novak Z, Ryu RK, et al.Treatment of posttraumatic internalcarotid arterial pseudoaneurysmswith endovascular stents. J Trauma2000; 48:470–472.
116. Armbruster JS. Accreditation of res-idency training in the US. PostgradMed J 1996; 72:391–394.
117. Redman HC. The route to subspe-cialty accreditation. Radiology 1989;172:893–894.
118. Langsley DG. What is the AmericanBoard of Medical Specialties? Pathol-ogist 1985; 39:30–32.
119. Ryan TJ, Bauman WB, Kennedy JW.Revised guidelines for percutaneoustransluminal coronary angioplasty: Areport of the American College ofCardiology/American Heart Associa-tion Task Force on Assessment of Di-agnostic and Therapeutic Cardiovas-cular Procedures (Subcommittee onPercutaneous Transluminal Angio-plasty). Circulation 1993; 88:2987–3007.
120. Smith SC, Dove JT, Jacobs AK, et al.ACC/AHA guidelines for percutane-ous coronary intervention (revision ofthe 1993 PTCA guidelines): A reportof the American College of Cardiolo-gy/American Heart Association TaskForce on Practice Guidelines (Com-mittee to Revise the 1993 Guidelinesfor Percutaneous Transluminal Coro-nary Angioplasty) endorsed by theSociety for Cardiac Angiography andInterventions. J Am Coll Cardiol 2001:2239i–2239lxvi.
121. Hirshfeld JW Jr., Ellis SG, Faxon DP,et al. Recommendations for the as-sessment and maintenance of profi-ciency in coronary interventional pro-cedures. Statement of the AmericanCollege of Cardiology. J Am Coll Car-diol 1998; 31:722–743.
122. Spittell JA, Nanda NC, Creager MA,et al. Recommendations for trainingin vascular medicine. American Col-lege of Cardiology Peripheral Vascu-lar Disease Committee. J Am CollCardiol 1993; 22:626–628.
AJNR: 24, November/December 2003 2033
123. Spittell JA, Creager MA, Dorros G, etal. Recommendations for peripheraltransluminal angioplasty: Trainingand facilities. J Am Coll Cardiol 1993;21:546–548.
124. Levin DC, Becker GJ, Dorros, et al.Training standards for physiciansperforming peripheral angioplastyand other percutaneous peripheralvascular interventions. A statementfor Health Professionals from the Spe-cial Group of Councils on Cardiovas-cular Radiology, Cardio-Thoracic andVascular Surgery, and Clinical Cardi-ology, the American Heart Associa-tion. Circulation 1992; 86:1348–1350.
125. Babb JD, Collins TJ, Cowley MJ, et al.Revised guidelines for the perfor-mance of peripheral vascular inter-vention. Catheter Cardiovasc Interv1999; 46:21–23.
127. Standards of Practice Committee ofthe Society of Cardiovascular and In-terventional Radiology. Angio-plasty standard of practice. J Vasc In-terv Radiol 1992; 3:269–271.
128. White RA, Hodgson KJ, Ahn SS, et al.Endovascular interventions trainingand credentialing for vascular sur-geons. J Vasc Surg 1999; 29:177–186.
129. Dagirmanjian A, Davis DA, RothfusWE, et al. Detection of clinically si-lent intracranial emboli ipsilateral tointernal carotid artery occlusions dur-ing cerebral angiography. AJR 2000;174:367–369.
130. Davies KN, Humphrey PR. Compli-cations of cerebral angiography in pa-tients with symptomatic carotid terri-
tory ischemia screened by carotidultrasound. J Neurol NeurosurgPsych 1993; 56:9647–9672
131. McIvor J, Steiner TJ, Perkins GD, et al.Neurological morbidity of arch an-giography in cerebrovascular disease.The influence of contrast medium andthe radiologist. Br J Radiol 1987; 60:117–122.
132. Willinsky RA, Taylor SM, TerBruggeK, et al. Neurologic complications ofcerebral angiography: prospectiveanalysis of 2,899 procedures and re-view of the literature. Radiology 2003;227:522–528.
133. Balduf LM, Langsfeld M, Marek JM,et al. Complication rates of diagnos-tic angiography performed by vascu-lar surgeons. Vasc Endovascular Surg2002; 36:439–445.
134. Kuntz KM, Skillman JJ, WhittemoreAD, Kent KC. Carotid endarterec-tomy in asymptomatic patients—Iscontrast angiography necessary? Amorbidity analysis. J Vasc Surg 1995;22:706–716.
135. Moore WS. For severe carotid steno-sis found on ultrasound, further arte-rial evaluation is unnecessary. Stroke2003; 34:1816–1817.
136. Mani RL, Eisenberg RL. Complica-tions of catheter cerebral arteriogra-phy: Analysis of 5000 procedures.AJNR 1978; 131:867–869.
137. Johnston DC, Chapman KM, Gold-stein LB. Low rate of complicationsof cerebral angiography in routineclinical practice. Neurology 2001; 57:2012–2014.
Clenny TE. Position Statement: Doc-umenting physician experience forcredentials for peripheral arterial pro-cedures—what you need to know. JVasc Interv Radiol 2002; 13:453–454.
140. Brott T, Adams HP Jr, Olinger CP, etal. Measurements of acute cerebralinfarction: a clinical examinationscale. Stroke 1989; 20:864–870.
141. Code of Medical Ethics of the Councilon Ethical and Judicial Affairs of theAmerican Medical Association.150th Anniversary Edition. Chicago:The American Medical Association,1997.
142. Hobson II RW, Goldstein JE, Jamil Z,et al. Carotid restenosis: operativeand endovascular management. JVasc Surg 1999; 29:228–238.
143. Sacks D, Marinelli DL, Martin LG,Spies JB, and the members of theTechnology Assessment Committee.Reporting standards for clinical eval-uation of new peripheral arterial re-vascularization devices. J Vasc IntervRadiol 1997; 8:137–149.
144. Martin LG, Rundback JH, Sacks D, etal. Quality improvement guidelinesfor angiography, angioplasty andstenting for the diagnosis and treat-ment of renal artery stenosis in adults.J Vasc Interv Radiol 2002; 13:1069–1083.
145. Beebe HG, Clagett GP, DeWeese JA,et al. Assessing risk associated withcarotid endarterectomy: a statementfor health professionals by an ad hoccommittee on carotid surgery stan-dards of the Stroke Council, AmericanHeart Association. Circulation 1989;79:472–473.
The clinical practice guidelines of the ASITN, the ASNR, and the SIR attempt to define practice principles thatgenerally should assist in producing high-quality medical care. These guidelines are voluntary and are not rules. Aphysician may deviate from these guidelines, as necessitated by the individual patient and available resources.These practice guidelines should not be deemed inclusive of all proper methods of care or exclusive of othermethods of care that are reasonably directed toward the same result. Other sources of information may be used inconjunction with these principles to produce a process leading to high-quality medical care. The ultimate judgmentregarding the conduct of any specific procedure or course of management must be made by the physician, whoshould consider all circumstances relevant to the individual clinical situation. Adherence to the ASITN, ASNR, andSIR Quality Improvement Programs will not ensure a successful outcome in every situation. It is prudent todocument the rationale for any deviation from the suggested practice guidelines in the department policies andprocedure manual or in the patient’s medical record.