Quality Improvement in Reducing Infection: An Example from Edinburgh Claire L Smith Consultant Neonatologist Neonatal Unit, The Simpson Centre for Reproductive Health, Royal Infirmary of Edinburgh [email protected]
Transcript
Quality Improvement in Reducing Infection:
An Example from Edinburgh
Claire L Smith
Consultant NeonatologistNeonatal Unit,The Simpson Centre for Reproductive Health, Royal Infirmary of [email protected]
• Neonatal infection: the significance• Is infection reduction a realistic target? • The importance of data• The Edinburgh experience• Costs• Challenges• An ongoing journey
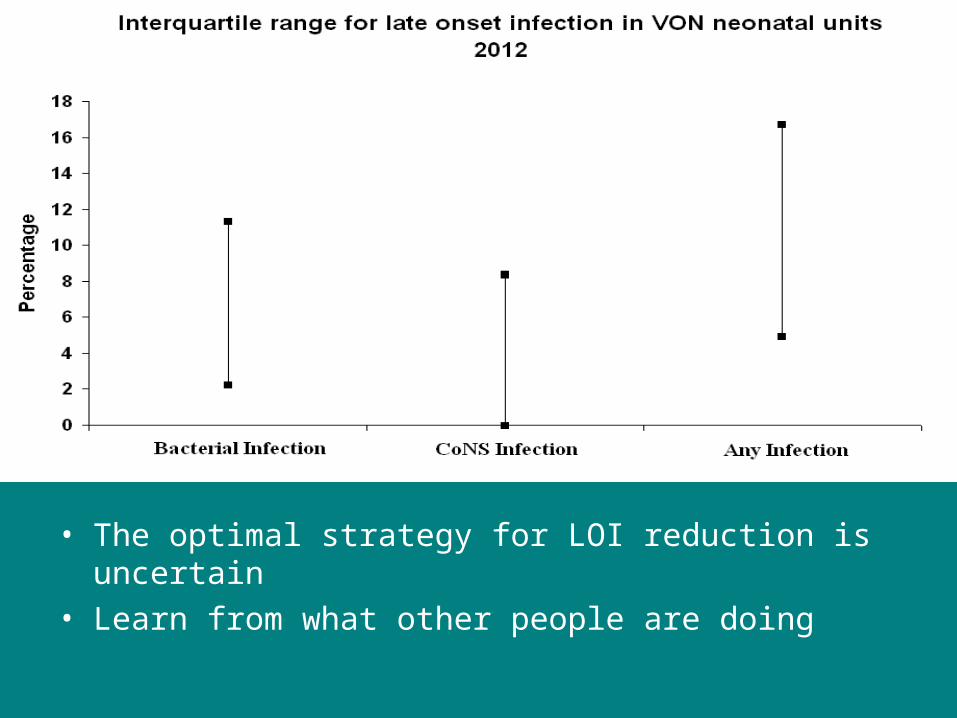
Late Onset Neonatal Infection
Is reducing late onset infection a realistic aim?
• The optimal strategy for LOI reduction is uncertain• Learn from what other people are doing
Good Data Matters
• How can you be sure you are doing something well if you don’t measure it?
• Is anyone doing better- who are they and what are they doing differently?
- Definitions- Benchmarking- Sharing experience
Our experience in Edinburgh
• We thought we were doing OK.
• We paid attention to infection control.
• We measured our infection rates.• Hard to compare with literature: definitions
• The infection rates were fairly static
• Then we joined VON….. and benchmarked
Definitions
• Late onset infection: infection after day 3 of life • Pathogen or Fungal• Coagulase negative staphylococcus: 5 days of
• 40 had at least one episode of sepsis– 31 had 1 episode– 7 had 2 episodes– 2 had 3 episodes
• CLABSI rate 23 per 1000 line days
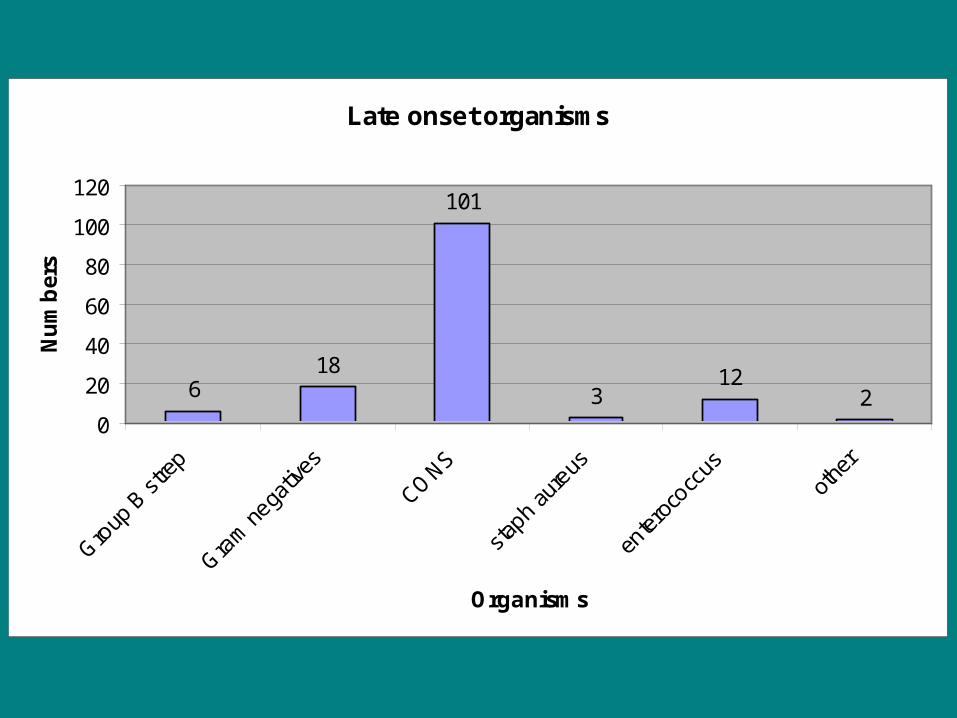
Late onset organisms
618
101
312
20
20
40
60
80
100
120
Group
B st
rep
Gram
nega
tives
CONS
staph
aure
us
enter
ococc
usot
her
Organisms
Nu
mb
ers
Comparison with VON<30 weeks OR < 1500g
VON SCRH
Any late infection
18% 38%
Bacterial pathogen
10% 14%
Coag Neg Staph
10% 26%
Fungal 2% 0%
Infection became our priority for improvement.
Neonatal QIP 2011-13
• Convened MDT • Review of QI literature• Set targets
– CoNS infection rates down to 5% – Zero transmission of MRSA– Zero MSSA bloodstream infections– Zero fungal infection
• Actions• Implementation of practice change• Audit
• Improved hand hygiene• Expand concept of individual patient environment• Reduce environmental reservoirs• Stop movement of babies around unit• Bathing and skin care• Insertion and maintenance of peripheral and central
lines• Promotion of early enteral feeds with human milk• Ventilator (nCPAP) associated pneumonia prevention• Urinary catheter care• Antifungal prophylaxis• Insist on closed system for taking cultures• Improved antibiotic stewardship• Improved staffing levels• Staff feedback
Actions
Hand hygiene and Patient Handling
• Hand washing and alcohol gel• Gloves for every patient contact
in NICU (staff)
• CoNS skin carriage among NICU staff: likely cause for cross transfer of virulent strains
References:V Hira et al. Journal of Clinical Microbiology 2010PC Ng et al. Arch Dis Child Fetal Neonatal Ed 2004Pessoa-Silva et al. Infect Control Hosp Epidemiol 2004
Environment: border control
• Each baby has their own cot space: only enter if really necessary
• Hand gel when entering and leaving cotspace• Dedicated pens/calculators/stethoscopes• No paperwork moved between spaces• Washable keyboards
References:G French et al. Lancet 1998Lu P-L et al. BMC Infectious Diseases 2009
Lines
• Line insertion bundle: aseptic checklist, 2 person technique
• Line maintenance bundle – aseptic and non touch technique
• Cannulae – sterile pack, sterile gloves• Skin preparation• Limit use of central lines
References:D Fisher et al. Pediatrics 2013 132: e1664
Feeding
• Promotion of early enteral feeds• Lactation support• Use of donor EBM
Early enteral feeds > reduced use of lines and PN
Blood culture technique
• Closed technique• Butterfly needle and syringe• Sterile pack and gloves• Skin prep
Antibiotic policies
• Automatic stop orders• Use of CRP• Revised empirical treatment based on local
sensitivities• Reduction of use of drugs requiring venepunture
for monitoring
Staff
• Regular staff feedback
• Monthly run-chart displayed in NNU
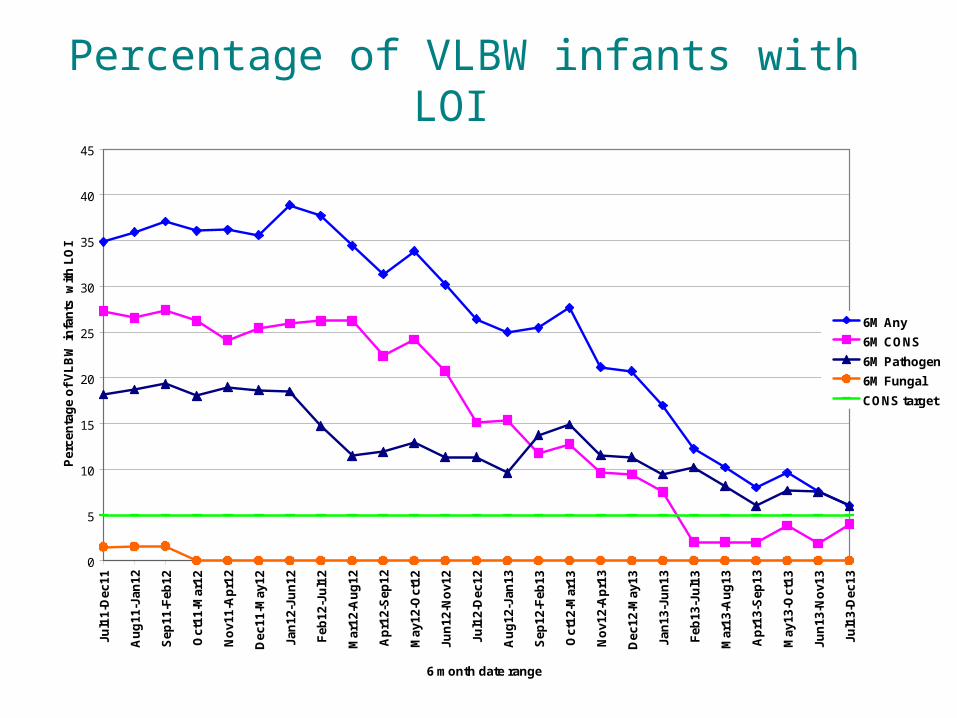
Percentage of VLBW infants with LOI
0
5
10
15
20
25
30
35
40
45
Jul1
1-D
ec11
Au
g11
-Jan
12
Sep
11-F
eb12
Oct
11-M
ar12
No
v11-
Ap
r12
Dec
11-M
ay12
Jan
12-J
un
12
Feb
12-J
ul1
2
Mar
12-A
ug
12
Ap
r12-
Sep
12
May
12-O
ct12
Jun
12-N
ov1
2
Jul1
2-D
ec12
Au
g12
-Jan
13
Sep
12-F
eb13
Oct
12-M
ar13
No
v12-
Ap
r13
Dec
12-M
ay13
Jan
13-J
un
13
Feb
13-J
ul1
3
Mar
13-A
ug
13
Ap
r13-
Sep
13
May
13-O
ct13
Jun
13-N
ov1
3
Jul1
3-D
ec13
6 month date range
Per
cen
tag
e o
f V
LB
W in
fan
ts w
ith
LO
I
6M Any
6M CONS
6M Pathogen
6M Fungal
CONS target
Cost
• Many of measures low/no cost• Staff• Funding in this area important
• Antibiotic bill has reduced significantly• Fewer blood tests for antibiotic levels• Reduced number of suspected infections
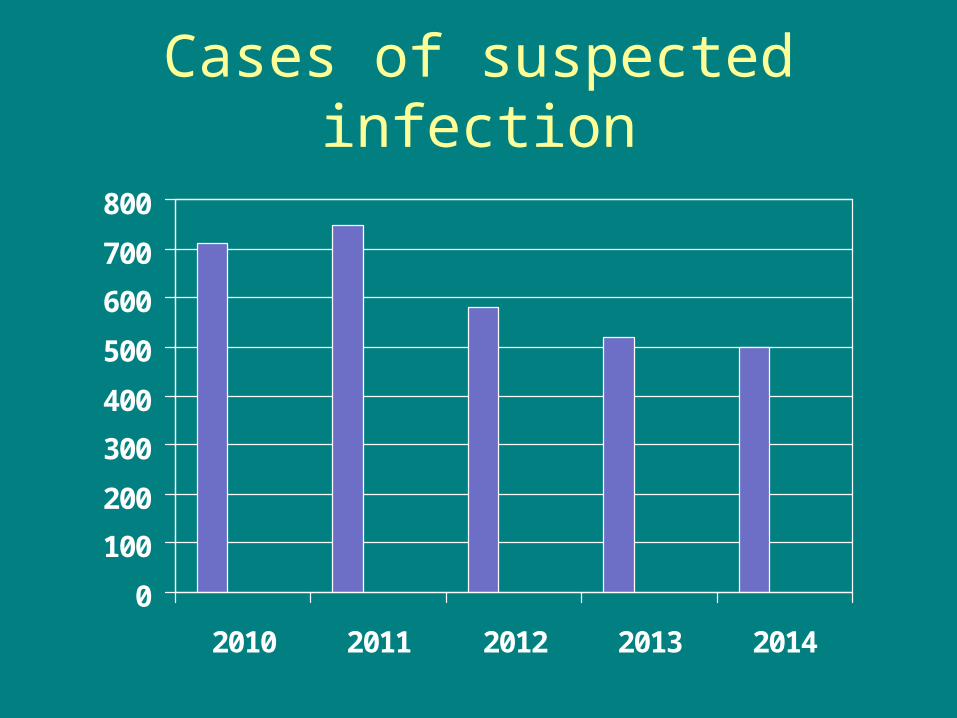
Cases of suspected infection
0
100
200
300
400
500
600
700
800
2010 2011 2012 2013 2014
Going forward
• Continued data monitoring
• Changing the way we present data
• In depth case review of all cases of CLABSI
• Random Safety Audits
• Periodic staff awareness drive – staff feedback is important
Key Challenges
• Measurement is key• Staff awareness and engagement vital• Time • Neonatal team dedicated and go the extra mile
time and again – individual capacity• New ways of working to incorporate patient
safety and quality improvement into everyday practice.
• Share workload and avoid duplication
Conclusions
• QI initiatives can have a large effect size on reducing late onset infection
• Improved outcomes were accompanied by significant cost savings
• Our experience with this QI initiative has been invaluable in taking forward other QI initiatives in our NNU