0 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: November 2018 - data compiled by Chris Panayi Quality Performance Dashboard January 2019 Panayi Chris Angela Cook Head of Nursing & Quality Adults Jo Gregory Head of Nursing & Quality Children & Families
Transcript
0 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: November 2018 - data compiled by Chris Panayi
Quality Performance Dashboard
January 2019
Panayi Chris
Angela Cook Head of Nursing & Quality Adults
Jo Gregory Head of Nursing & Quality Children & Families
1 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
SUMMARY REPORT
Meeting Date: 24th January 2019
Agenda Item:
Enclosure Number:
Meeting: Quality and Safety Committee
Title: Quality and performance Report
Author: Angela Cook, Head of Nursing and Quality Adults Jo Gregory, Head of Nursing and Quality Children & Families Chris Panayi, Quality and Improvement Officer
Accountable Director: Steve Gregory, Executive Director of Nursing and Operations
Other meetings presented to or previously agreed at:
Committee Date Reviewed Key Points/Recommendation from that Committee
None NA NA
Purpose of the report
The purpose of this report is to inform the Committee of current levels of performance as at the end of January 2019. Compliance with NHS targets and a range of local indicators provides an overview of performance and quality within the Trust, to provide assurance and escalate any actual or potential underperformance. In addition to escalate any risk to quality and Safety and mitigations in place to address these. The report, which is structured around the Care Quality Commission domains of: Safe, Effective, Caring, Responsive and Well-Led, has been developed to reflect performance at Trust and Service Delivery Group (SDG) level. Performance compliance underpins clinical quality and safety supporting the delivery of excellent care to our patients, children, young people and carers. All data contained in this report is also monitored, reviewed and discussed at Service Delivery Group level through the monthly Quality and Performance meeting. The Committee is asked to note that the Quality team have reviewed and revised the current quality KPI’s including National, local and Trust performance targets. A summary of the KPIs can be seen in the appendix 1. The review has been approved by the Director of Nursing and Operations.
Consider for Action
Approval
Assurance
Information
2 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Strategic goals this report relates to:
To deliver high quality care
To support people to live independently at home
To deliver integrated care
To develop sustainable community services
Summary of key points in report
SAFE
In December, there were no falls that resulted in a patient experiencing significant harm. There has been an increase in the overall number of falls (33) from previous month’s total of 17.
This month there were 18 reported pressure ulcers . There were 4 Grade 3 Pressure Ulcers wound bed not visible (ungradable) and 14 Grade 2 pressure Ulcers reported in Datix (Page 11)
3 of the 4 Grade 3 pressure ulcers were reported as a Serious Incident ( page 10)
The Venous Thromboembolism (VTE) Risk Assessments overall position improved this month to 92.8% compliance in December but remain below the 95% target ( page 7) .
Safety Thermometer (single day data) – harm free care rate is at 91.8% which is below the 95% target and below the national average for Community Trusts of 94.3% ( page 8).
CARING
A further decrease in compliance rate for new birth visits which is 87.4% against a target of 95%. Gaps in compliance are largely due to parental choice and failed notification (page 18)
The Adult & TEMS SDG wide FFT Score continues to be consistently above the national average rate . 98.6% based on 602 respondents in November 2018 and above the rate of 94% reported by NHS England during November for NHS Trusts (page 19)
RESPONSIVE
100% RTT response time were achieved in December surpassing the 95% target ( Page 25)
The number of written complaints remained unchanged at 5 in December of which 4 related to Adult services and 1 to Children and Families. The main reasons for the complaints were Clinical Treatment/Planning and Appointments Referrals (page 23)
21.5% of children are waiting 12 weeks or less for a community paediatric appointment. A recovery plan is in place to improve the waits and this is an improved position on last month (page 26)
WELL LED
Appraisal rates have remained static overall this month at 86.4% and failed to meet the Trust’s performance target of 95% (page 35)
The Trust vacancy factor fell to 6.04% in December. Funded establishment was 1353 WTE with 82 WTE as vacancies (6.04%). Attracting and retaining substantive staff remains a challenge for the Trust. Leavers outnumbered new starters in December after net gains in each of September, October and November. Workforce areas where we have the highest vacancy rates are as follows: Band 5 and 6 Physiotherapists equating to 9 WTE (20%) vacancies, Bridgnorth Band 5 RNs (4.67 wte, 21%) and Bishops Castle Band 5 RNs (5.43 wte, 42%) and Shropshire 0-19 Service HCAs (5.82 wte, 29%). In the Adult SDG there are 52 WTE vacancies (7.2%), in Children’s 16 WTE vacancies (4.4%) and TEMs 4.1 WTE (3.8%)
3 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Key Recommendations
The Quality and Safety Committee is asked to review and comment the contents of this report. We would specifically like you to discuss:
The areas of further work to identify if we have appropriate actions in place to achieve
Does the content of the report provide assurance on the quality & safety of our clinical services?
Is this report relevant to compliance with any key standards? YES OR NO State specific standard or BAF risk
Board Assurance Framework Yes Entry relating to quality and safety of services
Reporting format
The report is divided into the following sections:
Headlines and positive stories for Adults, TeMs and Children & Families Service Delivery Groups
12 monthly trend charts for each of the KPI agreed within this report. Where possible overall Trust performance has been reported alongside
both SDG performance in the same line graph. However, this hasn’t always been possible due to technical restrictions at this time
Above each graph you will be made aware of the standard/outcome and performance. Commentary enables the reporting of areas requiring
improvement as well as notable improved performance
The risk registers are included for our SDG’s concluding with the InPhase dashboard summarising all KPI’s
The dashboard includes the revised quality KPI’s including National, local and Trust performance targets.
4 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Shropshire Community Health NHS Trust Adults SDG – Headlines/Positive Stories
Most Improved Areas for further work
DTOC levels remain consistently below the 3.5% target
TeMS SDG showed has improved its basic life support (BLS) mandatory training compliance this month to 91.3%
TeMS has achieved an overall mandatory training compliance of 94% this month
Adult SDG services continue to show a sustained improving position at
87% this month with BLS training compliance
Overall adult safeguarding level 2 training continues to show an improving position
Pressure Ulcer Prevention and Management VTE Nurse Led risk assessments and training Discharge Planning and patient involvement in this process MRSA screening compliance Complaint responses Implementation of the NEWS2 programme to incorporate Sepsis Appraisals compliance Mandatory Training compliance in IPC, Safeguarding Adults and Children
compliance at level 2 Staff Flu vaccination uptake is reported at 70.49% compared to a position of
70.51% at the same point in 2017. Due to the number of clinical staff declining the flu vaccination the stretch target of 100% will not be achieved
Celebrating Success Shared Learning
Sustained MIU 4 hour performance -100% within 4 hours in December
Sustained District Nurse 24 and 48 hour response times
Since the Trust presented on the use of Datix to incorporate the new national pressure ulcer safeguarding tool in November , 2 London Hospitals have adopted our approach to their pressure ulcer risk management systems.
Telford Neighbourhood’s Rapid Response team have recently finished
a very successful collaborative pilot with the West midlands ambulance
service whereby nursing staff worked along paramedics and reported
that is approach was very beneficial for patient care and the wider
health system
All our community staff reported they felt incredibly proud when
showcasing their work and services during our recent CQC visit.
Pressure Ulcer Rapid Improvement continues to be embedded and
learning from its implementation being shared across IDT teams leaders
A patient complaint was shared with the Ludlow ward team and a learning event held to improve ward discharges
Staff Away Days held with focused learning sessions and networking have been held
6 Mini CQC away days were held in November and December where different teams were able to share their getting to good and beyond plans and approaches to quality improvement
5 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Shropshire Community Health NHS Trust Children & Families SDG – Headlines/Positive Stories
Most Improved Areas for further work
Shropshire 0-19 Public Health Nursing Service received positive feedback from Public Health Commissioners at Quarter 3 contract review meeting. The hard work of all staff was acknowledged especially in relation to the recent Joint Ofsted/CQC inspection
FNP – excellent outcomes demonstrated, team invited to be part of a national unit quality pilot and congratulations to Jo Bettison who has had an article published by the national unit.
Dentistry - Recruited locum dentist for two days a week. Three successful shortlisted candidates for out of hour’s service. Helpful response from NHS England, Public Health England, HEE and from the wider clinical director workforce in the West/North Midlands. STP and workforce planning workshop planned at end of March to look at rural dentist service. Recruited to dental nurse vacancy.
Appraisals compliance rate for the SDG is 90%. Teams sustaining 100% compliance are Children’s Physio, OT, Psychology, Wheelchair Services and Community Equipment Stores, 0-19 Shropshire South and Telford Paediatric team. Areas needing rapid improvement are 0-19 Shropshire North Team and CCN team. Reassurance given that outstanding staff have dates booked in before end of Jan. Monitoring weekly and offering support.
Level 2 and 3 children’s safeguarding training compliance has improved from 88.5% to 91.5%. Service leads have reported ESR glitches that are impacting on compliance. This is been actioned on an individual basis with OD. Julie Harris is working with OD to seek a solution to ensure training compliance is reflective.
HV, SN & FNP team leads are working well together to develop response to Telford 0-19 Public Health Nursing Service tender. Key messages shared with team on a weekly basis to keep them updated.
New Birth Visit compliance – failed notifications from maternity is increasing. Escalated at CCG CQRM and with LA Commissioners and report shared.
Celebrating Success Shared Learning
We continue to sustain the high number of service users who feedback their experience of care delivered by our services.
Immunisation team have successfully delivered the nasal flu programme. There was an increased year group of 32,000 children, of which the team delivered circa 27,000. Great team work demonstrated with zero sickness absence.
Children and Families Service Delivery Group have significantly contributed to the Trust achieving their apprentice target.
Four members of the targeted admin team have passed their maths exam for their NVQ. Nicola Greaves reported that they are really enjoying the course/development opportunity.
New consultant, Dr Gregory Menah, appointed as Designate Doctor/Medical Advisor for LAC, starts on 1
st April 2019.
Safeguarding Children from Domestic Abuse: Margot McCrone, Specialist Pubic Health Nurse based in Compass in Shropshire presented a staff story at January Quality and Performance meeting. Margot is working in the multi-agency hub at Compass with Children’s services and also the Police HARM Assessment Service. Stimulated lots of discussion around the role of children’s services in supporting C&YP who have experienced domestic abuse.
Hilary Griggs gave a verbal update on the Paediatric Diabetes Specialist Nurse Audit and the complexities for C&YP who live with diabetes
Service and team leads presented their own progress against key quality indicators at January Quality & Performance SDG meeting. Good learning discussion around what individual teams are doing to improve their compliance.
6 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Falls – Number of Falls
Standard and outcomes:
Any fall that occurs in an inpatient setting. The severity of the fall is defined in accordance with NRLS categories. All falls resulting in fracture,
including those categorised as severe harm or death are reported and managed as serious incidents. The trust target is set at 0 for serious
incident falls. The trust has a target of no more than 384 falls in a year. Performance: 33 Commentary: Falls prevention presents a challenge as the Trust’s inpatient activity increases. The purpose of the indicator is to encourage active risk
management in falls prevention and reducing harm from falls. This will in turn contribute to the Trust goal of delivering "harm free care". In December this has proved challenging with a rise in the number of falls reported in our community hospitals. Of the 33 reported falls, 22 occurred within Whitchurch and Ludlow hospital wards. Although no patient’s experienced significant harm. During December Ludlow had an increase in occupied bed days from 601 in November to 895 in December with an increase in patient admissions (51) compared to the previous month (39). Whitchurch’s position was 895 occupied bed days compared to 871 in November with additional escalation beds open during December. Other possible reasons for this month’s rise includes an increase in the frailty and complexity of patients in our care at this time. During December Ludlow has 2 patients who fell more than once, Bridgnorth and Bishops Castle has 2 patients who fell more than once and Whitchurch had 1 patient who fell more than once. This accounts for 13 of the falls recorded. In addition there was increase in the number of inter- hospital transfers at night potentially exacerbating the risk of disorientation for our cognitive impaired patients. To mitigate work continues to strengthen our inter hospitals transfer handover to enable a more robust falls risk identification and support earlier patient transfers. In addition a Falls Task & Finish group is progressing further initiatives to improve our falls prevention work in our hospitals
7 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
VTE (Venous Thromboembolism Risk Assessment)
Standard and outcomes:
All inpatients should undergo a risk assessment for VTE to reduce their risk of venous thromboembolism (VTE or blood clots) and deep vein thrombosis (DVT) in people. The risk assessment aims to help healthcare professionals identify people most at risk and describes interventions that can be used to reduce the risk of VTE. 95% of patients admitted to our community hospitals should have a Venous Thromboembolism Risk (VTE) Assessment
Performance: 92.8%
Commentary:
Performance increased from 87.5% reported in November to the current position of 92.8% compliance in December. This has meant that we have met out recovery target of 90% in December, with a further plan to achieve 95% by January 2019.
Ludlow missed 5 VTE risk assessments = 89.08% compliance 10 of the 12 patients had their VTE risk assessments had it completed within 2 – 7 days. The remaining 2 patient assessments were missed
during an out of hours admission and A&E transfer ( no details of VTE) . No further information was available on one of these and the other
the patient was transferred back to the acute Hospital the following day before the risk assessment was repeated.
All the 12 missed VTEs assessments related to out of hours patients and therefore it is imperative that the nurse led assessment training
programme continues as planned. The trajectory for this is for 75% of staff to have completed face-to-face training by mid-January.
Staff have been reminded to Datix reports any VTE risk assessment that have not been completed as per policy
8 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Safety Thermometer – harm free care
Standard and outcomes:
The Classic Safety Thermometer is a measurement tool for improvement that focuses on the four most commonly occurring harms in healthcare: pressure ulcers, falls, UTI (in patients with a catheter) and VTEs. Data is a snapshot on the day collected on a single day each month and the aim is to have a snapshot picture of the 4 most commonly occurring themes in healthcare due to assisting and measuring improvement over time. The reporting system also enables trusts to benchmark nationally.
Performance:
91.8%
Commentary:
The Safety Thermometer Patient Safety Programme is a quality priority and maintaining 95% Harm free care is a key deliverable. This represents patients
experiencing harm from either a pressure ulcer, fall, catheter associated urinary tract infection or a blood clot on one specific day each month. Please note
the data is 2 months behind the month of reporting.15/517 patient’s experienced new harms during November. These are harms that occurred in our care
and are categorised as follows: 7 New Pressure Ulcers (Bishops Castle Hospital (1 x Grade 2), Broseley & Much Wenlock DN (1 x Grade 3), Market
Drayton DN (1 x Grade 2), Shrewsbury South DN (1 x Grade 3), TELWEL DN (3 – 1 x Grade 4, 2 x Grade 2).6 falls (Bridgnorth DN – 2 Falls, TELWEL –1
Fall, and Ludlow Hospital – 2 Falls. 1 VTE - Bridgnorth, Catheter Bridgnorth 1 Catheter & 1 UTI
91.8% of caseloads were harm free in November compared 93.4% of the caseload in October 2018. This represents a 1.6% decrease in our overall
performance. This data includes patients that have come onto our caseload with one or more of the identified harms already. The target of 95% has not
been achieved. The sample of patients in November was 517 in compared to 621 in October 2018. Further breakdown reveals that our inpatient harm free
prevalence has decreased this month to 86.1% from October’s position 90.9%.Out of 72 patients in our ward areas 5 were recorded with a new harm.
Patients living and being supported by our teams in the community represent the largest cohort of patients sampled and the prevalence of harm free care
for November for this group was 91.8% harm free.399 patients were harm free from the total of 431 patients surveyed. This represents 10 of the 15 total of
new harms.
9 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Serious Incidents (all)
Standard and outcomes:
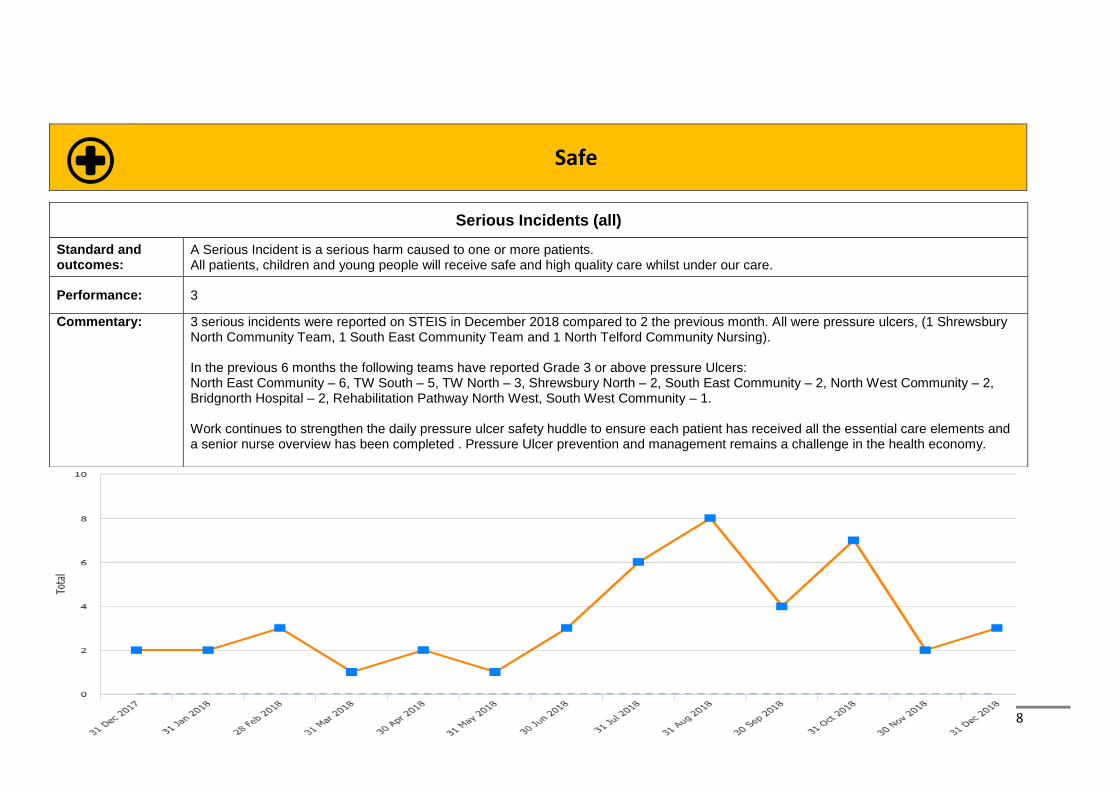
A Serious Incident is a serious harm caused to one or more patients. All patients, children and young people will receive safe and high quality care whilst under our care.
Performance: 3
Commentary: 3 serious incidents were reported on STEIS in December 2018 compared to 2 the previous month. All were pressure ulcers, (1 Shrewsbury North Community Team, 1 South East Community Team and 1 North Telford Community Nursing). In the previous 6 months the following teams have reported Grade 3 or above pressure Ulcers: North East Community – 6, TW South – 5, TW North – 3, Shrewsbury North – 2, South East Community – 2, North West Community – 2, Bridgnorth Hospital – 2, Rehabilitation Pathway North West, South West Community – 1. Work continues to strengthen the daily pressure ulcer safety huddle to ensure each patient has received all the essential care elements and a senior nurse overview has been completed . Pressure Ulcer prevention and management remains a challenge in the health economy.
10 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Proportion of admissions screened for MRSA
Standard and outcomes:
Achievement of this target demonstrates our standard of practice in relation to Control of Infection, links to quality of patient care and to managing our reputation as a healthcare provider and our registration with the Care Quality Commission. In October the Trust did not experience any outbreaks of Methicillin-resistant staphylococcus aureus (MRSA). Proportion of admissions screened for MRSA (97%) target
Performance: 95.2%
Commentary: Performance for December is below the 97% target due to missed screenings at all 4 hospital sites. Ludlow Community Hospital - 3 screenings missed, Whitchurch Community Hospital - 3 screenings missed, Bridgnorth Community Hospital – 1 screening missed and Bishops Castle Hospital - 1 screening missed. Since April 2018 the below teams missed the following amount of screenings: Ludlow Hospital – 23, Whitchurch Hospital 13, Bridgnorth Hospital 10, and Bishops Castle – 8. The IPC team have also notified ward managers and supplied details of each missed screening for review. Bishops Castle & Ludlow hospitals have not achieved the 97% target now for 3 consecutive months. During this period these areas have had a higher use of temporary staffing solutions which may have contributed to the missed screenings. These results will also be discussed at the SDG Quality & Safety meeting and Ward Manager Meetings to improve support improved compliance. Our IPC team are strengthening the link nurse role to support MRSA screening and reporting
11 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Pressure Ulcers
Standard and outcomes:
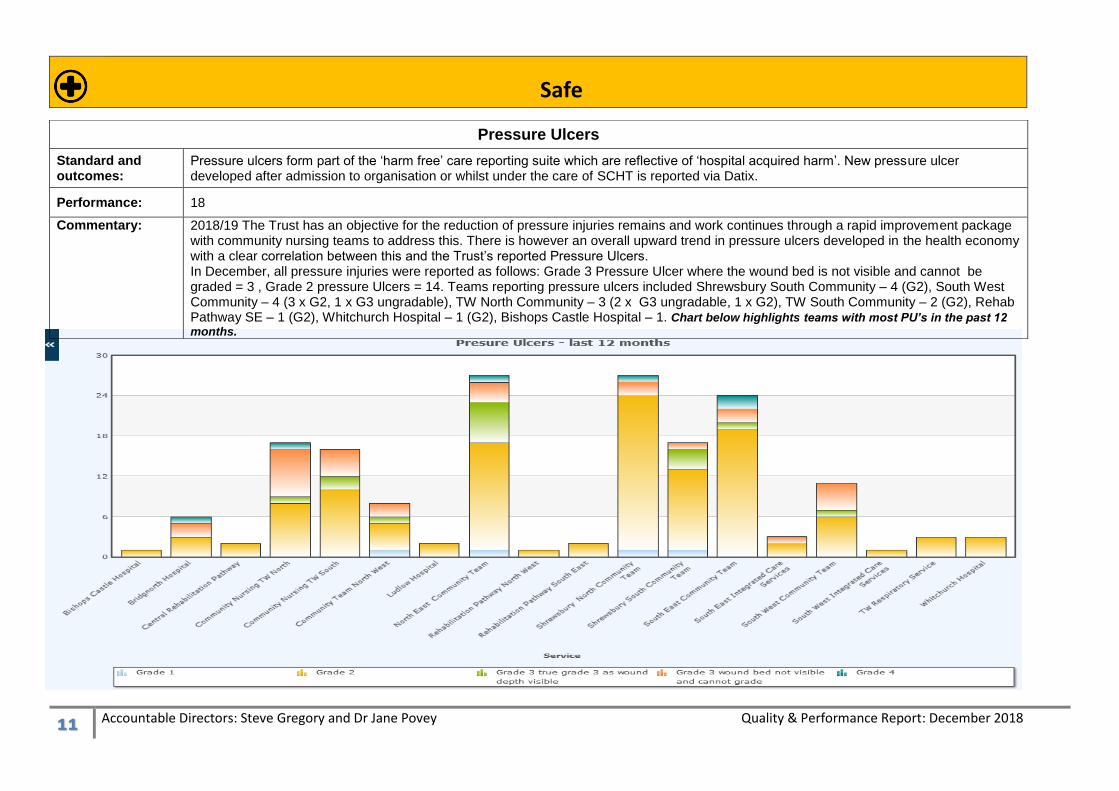
Pressure ulcers form part of the ‘harm free’ care reporting suite which are reflective of ‘hospital acquired harm’. New pressure ulcer developed after admission to organisation or whilst under the care of SCHT is reported via Datix.
Performance: 18
Commentary: 2018/19 The Trust has an objective for the reduction of pressure injuries remains and work continues through a rapid improvement package with community nursing teams to address this. There is however an overall upward trend in pressure ulcers developed in the health economy with a clear correlation between this and the Trust’s reported Pressure Ulcers. In December, all pressure injuries were reported as follows: Grade 3 Pressure Ulcer where the wound bed is not visible and cannot be graded = 3 , Grade 2 pressure Ulcers = 14. Teams reporting pressure ulcers included Shrewsbury South Community – 4 (G2), South West Community – 4 (3 x G2, 1 x G3 ungradable), TW North Community – 3 (2 x G3 ungradable, 1 x G2), TW South Community – 2 (G2), Rehab Pathway SE – 1 (G2), Whitchurch Hospital – 1 (G2), Bishops Castle Hospital – 1. Chart below highlights teams with most PU’s in the past 12
months.
12 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Medication Incidents that affect patients safety
Standards: The number of medication errors resulting in harm is reported. All patients, children and young people requiring medication will remain free from harm
Performance: 15
Commentary: 60 medication incidents were reported in total during December 2018 compared to 40 in November. This was a significant increase compared to the previous month. Of these, 19 were external errors or incidents that did not directly affect a patient and have been removed from reporting. There were no reported errors causing serious harm. There were 15 incidents reported which involved a high risk drug but caused no or minor harm. Internal incidents which had potential to cause harm to a patient equated to 41 in total once the external errors had
been removed from the total. Of these 41 incidents, 14 related to administration (as omitted, delayed or wrong dose given), 26 related to prescription related incidents and 1 related to the storage of medications where the ambient temperature was above the recommended level. There were no incidents involving children’s services
13 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Day Night Total
Registered Nurses 97.5% 92.8% 96.7%
Care Staff 97.9% 95.9% 97.7%
Registered Allied Health Professionals 99.5% 99.5%
Non-registered Allied Health Professionals 108.0% 108.0%
Total 99.4% 94.1% 98.9%
Safer Staffing
The National Quality Board (NQB) document “How to ensure the right people, with the right skills, are in the right place at the right time” (November 2013) set out expectations for providers of NHS services. The Trust reviews how staffing is reported to enable it to capture areas where additional staffing above the reed establishment has been required to ensure wards are safe, e.g. due to acuity of patients. Staffing Fill Rate is the total hours worked divided by total hours planned. A figure over 100% indicates more hours worked than planned The graphs provide the 'fill rate' for those teams reporting less than 100% by staff group and time of day, and also 'fill rate' as recorded on UNIFY. The table provides a summary of Trust overall performance.
Overall for the month of December 2018, the Trust had 97.5% cover for registered nurses (RN) on days and 92.8% registered nurse cover for nights. The unregistered nursing level was 97.9 % for days and 95.9% for nights reflects the activity seen in December 2018. This was due primarily to nursing assistant’s specialist assignments to safely care for confused or mentally unwell adult patients. There were 5 shifts within the inpatient ward setting where there was only 1 RN on duty rather than the recommended 2 RN’s on duty. 4 of these occasions were at Bishops Castle Hospital and 1 at Ludlow Hospital. For Bishops Castle where only 1 RN was on duty on 3 of these shifts there were 3 HCA’s on duty. On the other occasion there where 2 HCA’s present. On 2 of these occasions there were only 10 patients, 1 shift - 9 patients, and the other shifts had a total of 15 patients. For Ludlow Hospital where there was only 1 RN present on a night shift, there were 3 HCA’s present and 21 patients. During December Bishops Castle inpatient numbers varied between 10-14 patients at any one time. Although no significant harms were recorded during the periods where only 1 RN was on duty, Bishops Castle Hospital did have did report 1 patient fall incident which was not witnessed.
14 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
15 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
16 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safer Staffing Summary
The UNIFY return provides information on how actual staffing levels compare to the planned levels (CQC KLOE S4). The December return indicates that
staffing numbers overall were at a 97.9% fill rate. The lowest RN fill rate was at 93.6% on day shifts at Bishops Castle Hospital which is 3% lower than on
the previous month.
The Allied Health Professional (AHP) fill rate at Whitchurch Hospital was suboptimal due to 2 physiotherapy positions being vacant. Temporary staffing
cover remains in place until the newly recruited staff commence in post.
The unregistered fill rate ranged from 95% at Bridgnorth Hospital to 114.5% at Whitchurch Hospital on day shifts. Those areas with a high fill rate were due
to the level of additional patient supervision and to a lesser degree covering RN shifts not filled to ensure minimum numbers
17 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Safe
Staff Vacancy rates
Standard and outcomes:
Vacancy levels are measured as the difference between the Full Time Equivalent (FTE) budgeted establishment and the Full Time Equivalent substantively employed, represented as a percentage.
Performance: In December, funded establishment was 1353 WTE with 82 WTE as vacancies (6.0%)
Commentary: The Trust vacancy factor fell to 6.04% in December. Funded establishment was 1353 WTE with 82 WTE as vacancies (6.04%). Attracting and retaining substantive staff remains a challenge for the Trust. Leavers outnumbered new starters in December after net gains in each of September, October and November. Workforce areas where we have the highest vacancy rates are as follows: Band 5 and 6 Physiotherapists equating to 9 WTE (20%) vacancies, Bridgnorth Band 5 RNs (4.67 wte, 21%) and Bishops Castle Band 5 RNs (5.43 wte, 42%) and Shropshire 0-19 Service HCAs (5.82 wte, 29%). In the Adult SDG there are 52 WTE vacancies (7.2%), in Children’s 16 WTE vacancies (4.4%) and TEMs 4.1 WTE (3.8%)
18 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
95% of new birth visits to be completed within 14 days of birth
Performance: 87.4%
Commentary:
Slight decrease in target this month has been shared with leads. Weekly validation of data continues and a lot of the reasons regarding primary out of time frame is parental choice/situational. E.g. staying with family out of county, or child in neonatal unit at the time visit should be done. In these cases a mutually agreed visit as near to the contracted date would be arranged. It has been noted this month that Datix are
increasing for failed notifications from maternity services. This has been escalated at the CCG Clinical Quality Review Meeting and with
Local Authority Commissioners. A report has been shared detailing the incidents.
19 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Caring
Friends and Family Test – Adult and TeMS SDG Positive Response
Standard and outcomes:
The NHS Friends and Family Test (FFT) is a feedback tool which offers patients of NHS-funded services the opportunity to provide feedback about the care and treatment they have received. The question asks how likely, on a scale ranging from extremely unlikely to extremely likely, they are to recommend the service to their family and friends.
Performance: 98.6%
Commentary:
The Adult SDG wide FFT Score has remained consistent at over 95% based on 602 respondents in November 2018 For November, 98.6% respondents recommended our services overall. TeMS had 213 responses with 97.1% recommending the services. The Trust’s scores on the Friends and Family Test were above the target level in November and above the rate of 94% reported by NHS England during November.
20 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Caring
Friends and Family Test – Children and Families Positive Response
Standard and outcomes:
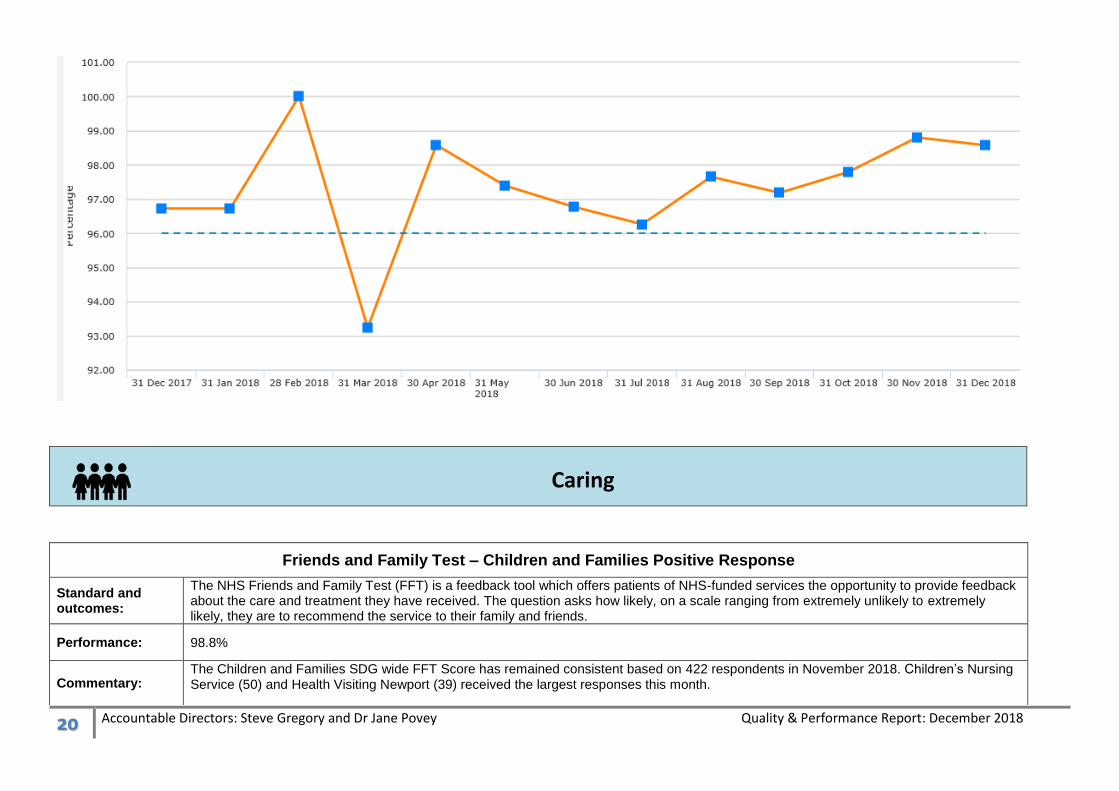
The NHS Friends and Family Test (FFT) is a feedback tool which offers patients of NHS-funded services the opportunity to provide feedback about the care and treatment they have received. The question asks how likely, on a scale ranging from extremely unlikely to extremely likely, they are to recommend the service to their family and friends.
Performance: 98.8%
Commentary: The Children and Families SDG wide FFT Score has remained consistent based on 422 respondents in November 2018. Children’s Nursing Service (50) and Health Visiting Newport (39) received the largest responses this month.
21 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
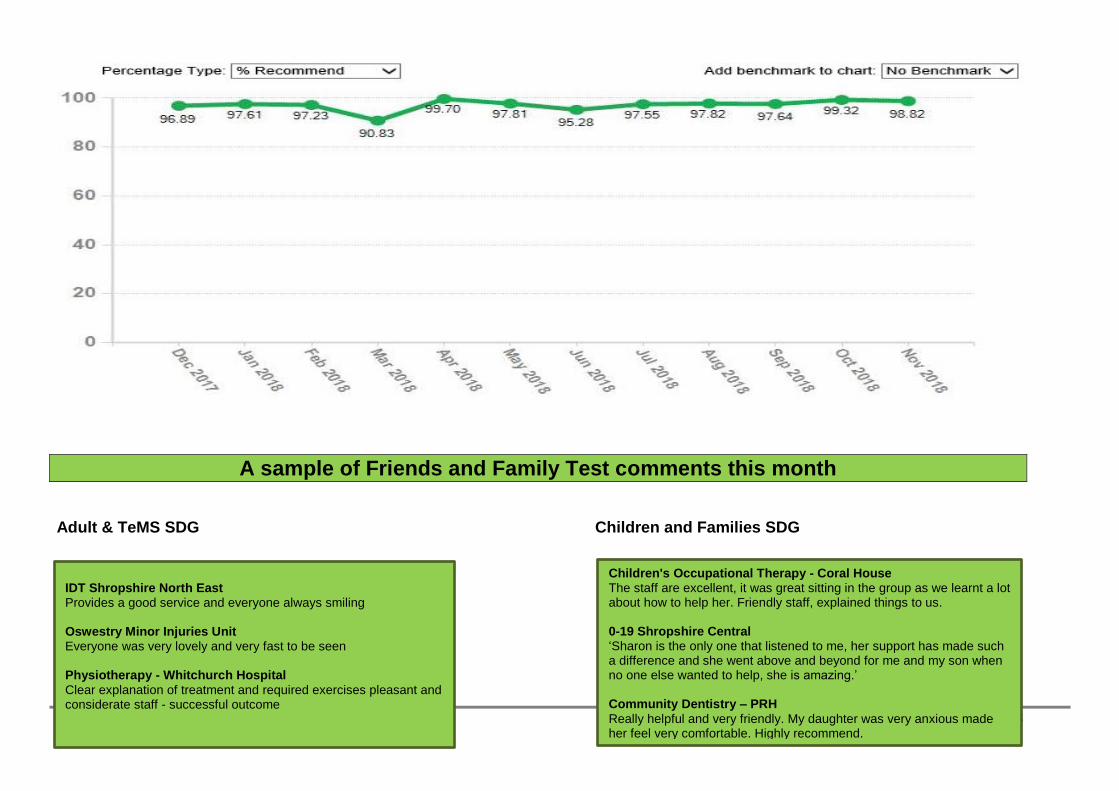
A sample of Friends and Family Test comments this month
Adult & TeMS SDG Children and Families SDG
IDT Shropshire North East Provides a good service and everyone always smiling Oswestry Minor Injuries Unit Everyone was very lovely and very fast to be seen Physiotherapy - Whitchurch Hospital
Clear explanation of treatment and required exercises pleasant and considerate staff - successful outcome
Children's Occupational Therapy - Coral House The staff are excellent, it was great sitting in the group as we learnt a lot about how to help her. Friendly staff, explained things to us. 0-19 Shropshire Central ‘Sharon is the only one that listened to me, her support has made such a difference and she went above and beyond for me and my son when no one else wanted to help, she is amazing.’ Community Dentistry – PRH
Really helpful and very friendly. My daughter was very anxious made her feel very comfortable. Highly recommend.
22 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Adults & TEMs Commentary: Feedback is shared with services. Ludlow Ward has recently had a learning event based on a recent complaint relating to a
patient’s discharge . Immediate actions have been put in place and work remains on going to improve discharge management.
Negotiations are underway to extend Oswestry MIU X-ray provision which has featured regularly in our FFT returns
Responsive
Complaints
Standard and outcomes:
The number of written complaints. Complaints provide valuable feedback to improve care & outcomes
Performance: N/A
Commentary:
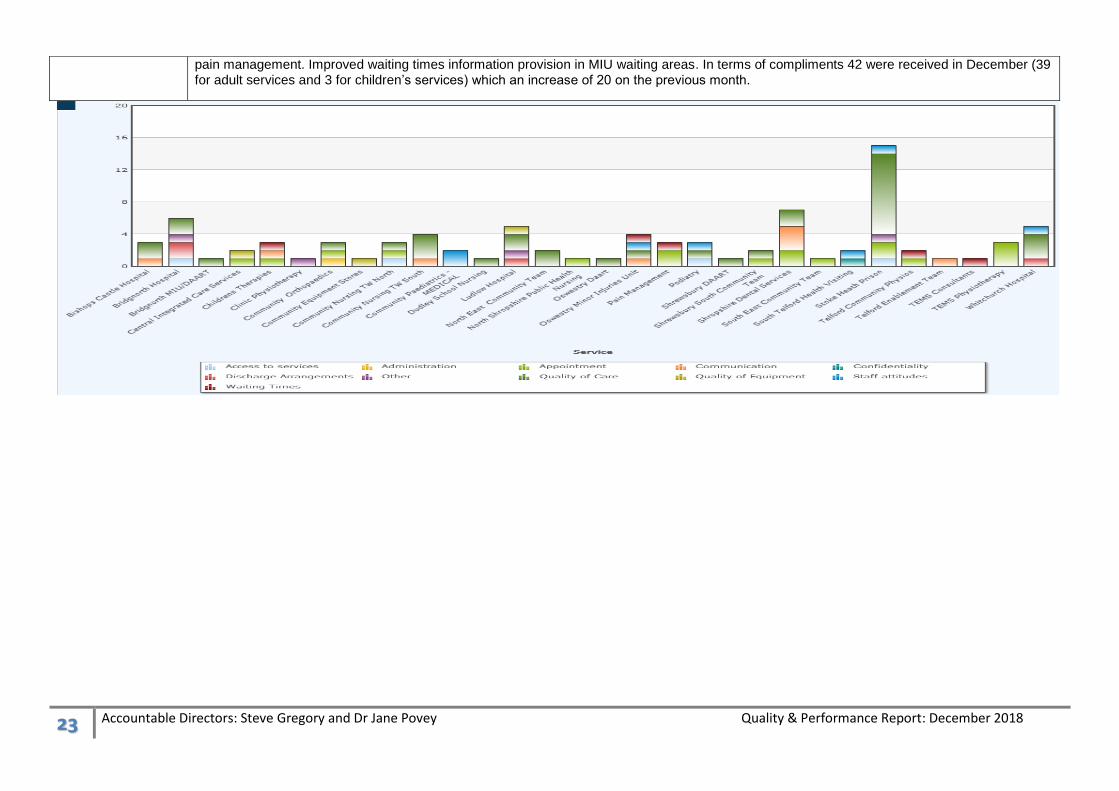
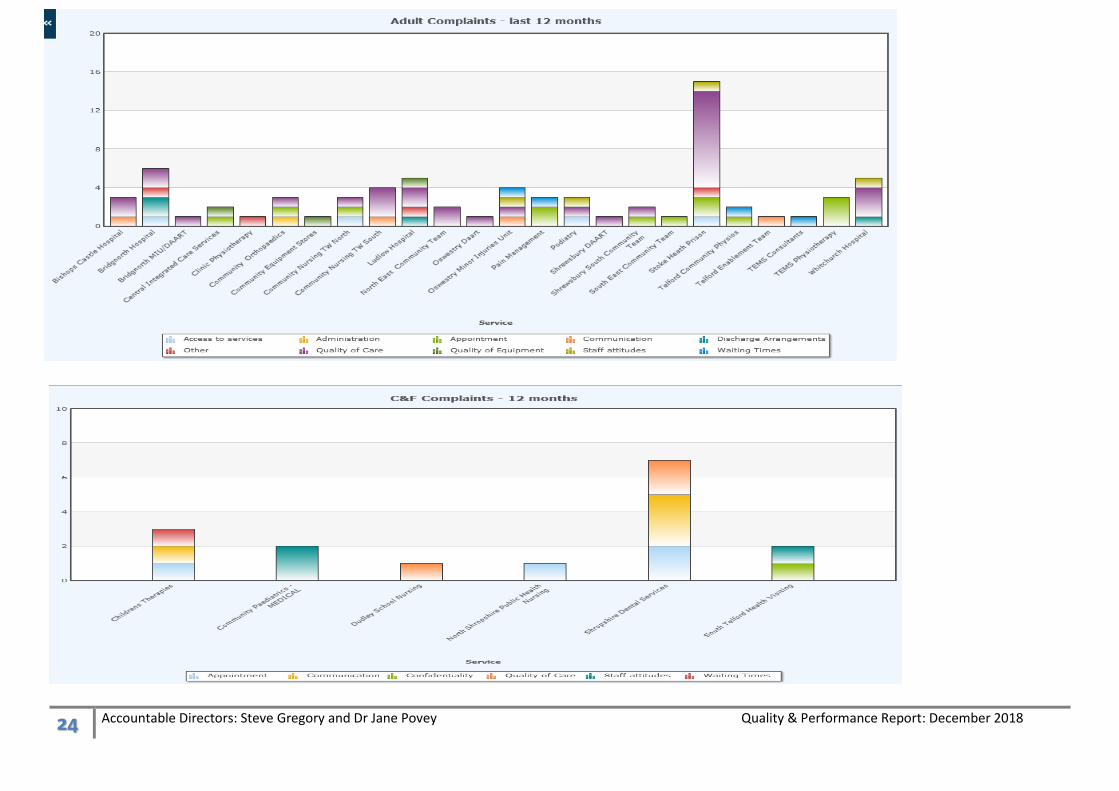
In December a total of 5 complaints received across the Trust. This is the same number as received in November. 4 were related to Adult services and 1 to Children and Families. The main reasons for the complaints this month were Clinical Treatment/Error (1 x Bridgnorth MIU/DAART, 1 x Stoke Heath Prison, 1 x Shropshire Dental Services) which amounted to 3 in total. Appointments/Visits/Referrals (1 x Pain Management, 1 TeMS Physiotherapy) which equated to 2 in total. The Quality and complaints team are working collaboratively with our service delivery group managers to share good practice in responding to complainants, develop further skills and to share any wider learning from complaints. Learning from complaints is discussed at the SDG Q&S monthly meetings. Actions taken in Adult & TeMS SDG as a result of Decembers complaints include the development of improved patient information for Stoke heath prisoners regarding medication prescribing in
Oswestry Minor Injuries Unit x ray open until centre closes Ludlow – Inpatient Did you feel you were involved in decisions about your discharge from hospital? At first yes, but at the very late stages changes were made which weren't discussed with me first and no account taken of what I felt I needed to sort out. I was reassured afterwards but it was very stressful
Whitchurch Minor Injuries Unit What would have made your visit better? The wait.
Community Dentistry – Shrewsbury Please tell us why you gave the answer that you did. It stinks of cigarettes. Health Visiting Wellington What would have made your visit better? Better signage
23 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
pain management. Improved waiting times information provision in MIU waiting areas. In terms of compliments 42 were received in December (39 for adult services and 3 for children’s services) which an increase of 20 on the previous month.
24 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
25 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
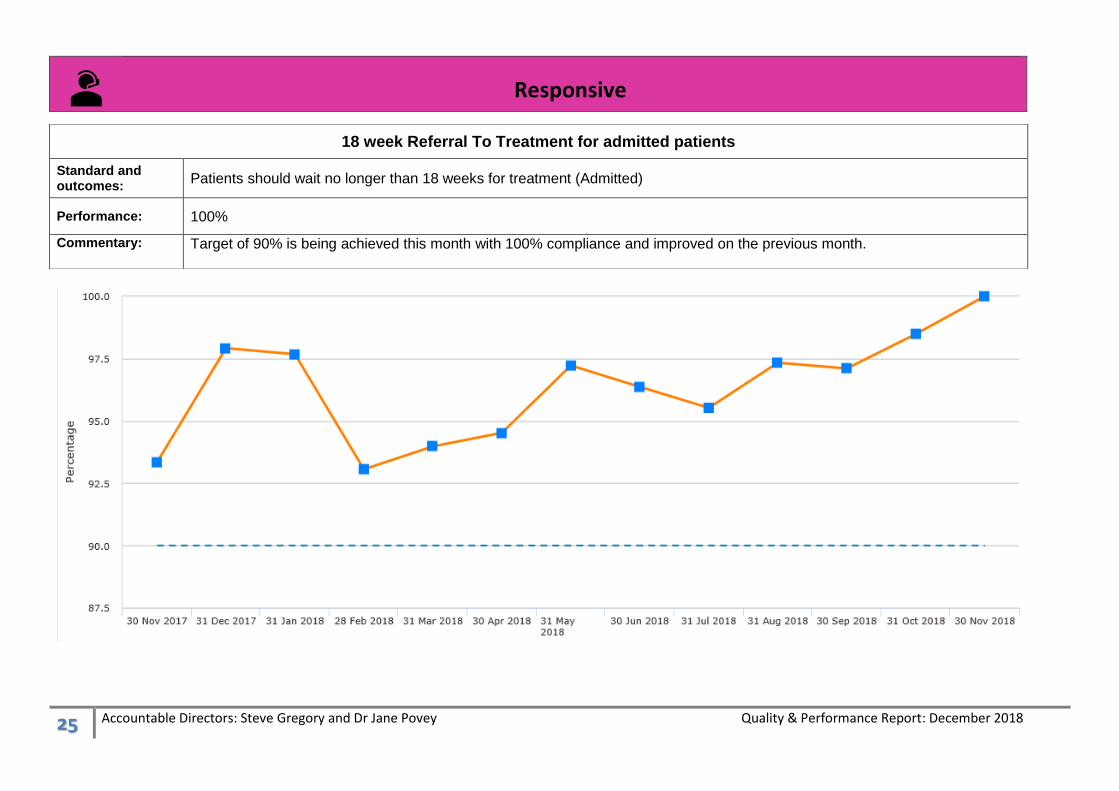
18 week Referral To Treatment for admitted patients
Standard and outcomes:
Patients should wait no longer than 18 weeks for treatment (Admitted)
Performance: 100%
Commentary: Target of 90% is being achieved this month with 100% compliance and improved on the previous month.
26 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
18 week Referral To Treatment for non-admitted patients
Standard and outcomes:
At each month-end, the Trust reports the number of patients on an on-going RTT pathway and the percentage that have been waiting less than 18 weeks. The national standard is that over 92% of the patients should be waiting under 18 weeks. SCHT Patients should wait no longer than 18 weeks for treatment (Non-admitted)
Performance: 88.6%
Commentary: This month’s Combined position is 88.6% a slight increase on last month’s position. The anticipated recovery date is June 2019.TeMS 18 week RTT breaches relate to Rheumatology services with delays associated with diagnostics and sub-optimal clinic utilisation. Non TeMS RTT has also shown a decline in performance and relates to respiratory services with a reduction from 94% to 80%. Actions in place to achieve a recovery position include further training for clinicians and validators and target setting on clock closures.
27 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
Outpatients > 12 week Consultant Led – Community Paediatrics
Standard and outcomes:
Children and young people should wait no longer than 12 weeks to see a Community Paediatrician
Performance: 21.5% waiting 12 weeks or less
Commentary: Performance has improved this month from 33% to 21.5%. Some parents have been offered an appointment within 12 week target, but
they have not accepted appointment due to travel, some parents decline apt offered due to clinic location. All 12 week breaches targets
are recorded on IT system, so that when parents phone in they are given priority. There is a 12 week breach clinic that has increased
capacity in the system. Medical vacancies have been advertised and shortlisting has taken place, interview dates are in place. Locum
consultant cover for recruitment gap has been approved which should had more capacity in January. 12 week target is being reviewed to
move to 18 weeks in line with national targets.
28 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
Proportion of Delayed Transfers of Care
Standard and outcomes:
The Trust aims to discharge patients who no longer need to be in hospital in a timely manner as far as possible to prevent deterioration in their overall condition. The DTOC data relates to the percentage of all occupied beds that are occupied by a patient who is delayed. The National target is 3.5%
Performance: 3.34%
Commentary: There has been a decline in December’s overall performance position compared to the previous month’s position. However overall performance remains in target and is exceeding our recovery plan.
29 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
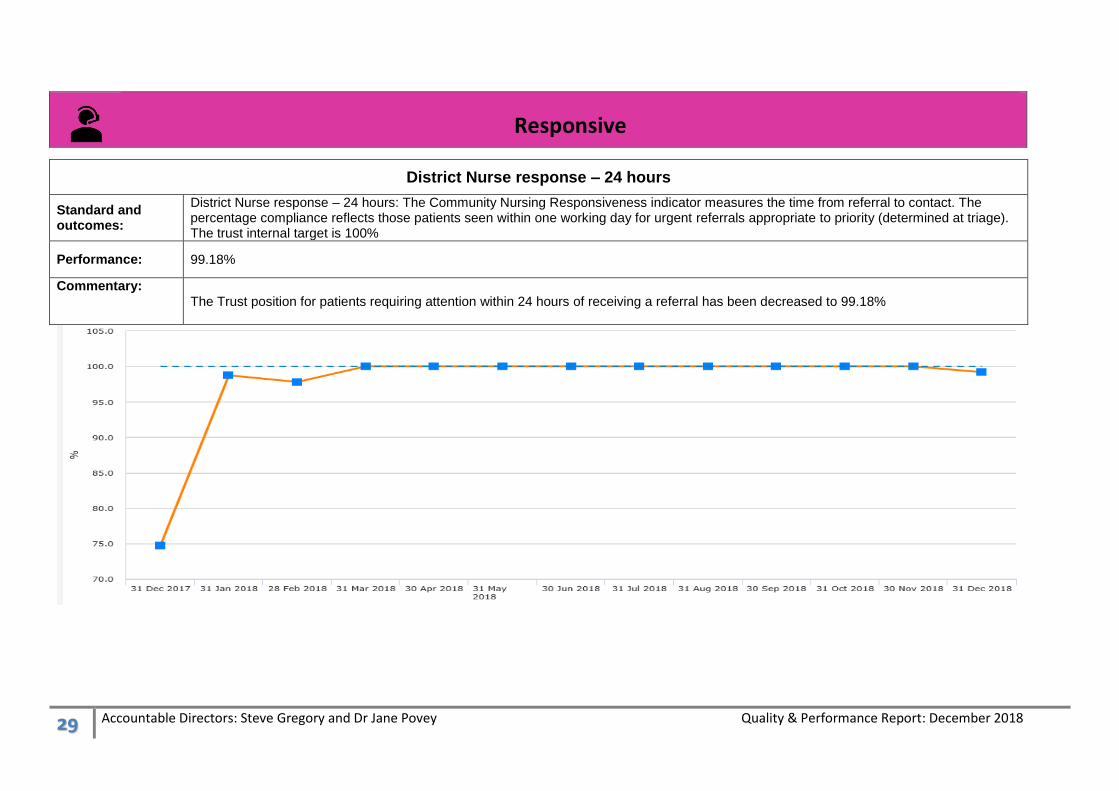
District Nurse response – 24 hours
Standard and outcomes:
District Nurse response – 24 hours: The Community Nursing Responsiveness indicator measures the time from referral to contact. The percentage compliance reflects those patients seen within one working day for urgent referrals appropriate to priority (determined at triage). The trust internal target is 100%
Performance: 99.18%
Commentary:
The Trust position for patients requiring attention within 24 hours of receiving a referral has been decreased to 99.18%
30 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
District Nurse response – 48 hours
Standard and outcomes:
District Nurse response – 48 hours The Community Nursing Responsiveness indicator measures the time from referral to contact. The percentage compliance reflects those patients seen within 2 full working days for routine referrals appropriate to priority (determined at triage) The trust internal target is 100%
Performance: 99.09%
Commentary:
The Trust position for patient’s requiring attention within 24 hours of receiving a referral has reduced to 99.09%
31 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Responsive
MIU Total time in department – discharged within 4 hours
Standard and outcomes:
Patients should spend less than 4 hours before discharge. A target is that 95% of patients should be seen within 4 hours of arriving in a MIU department
Performance: 100%
Commentary:
The Trust Performance is at 100% for December.
32 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Effective
Length of Stay (overall)
Standard and outcomes:
Bed occupancy rates are monitored to establish the utilisation of Community Hospital beds and to ensure patients do not stay longer in hospital than they need to. The average Length of Stay is the number of bed days (1 bed days = 1 bed occupied at 12 midnight) for all inpatients discharged in the month, divided by number of discharges.
Performance: 13 days
Commentary: The length of stay position has been maintained at 13 days across the community hospitals in-patient wards. The average length of stay is variable across sites ranging from 10.3 days at Bridgnorth Hospital to 18.3 days at Whitchurch. Whitchurch Hospital length of stay was longer this month with 5/48 patients having longer hospital stays totalling 42 days or more in December. Red 2 Green work continues to improve this position
33 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Effective
Unexpected deaths
Standard and outcomes:
Unexpected or Sudden or Suspicious/unexplained death are where it was not anticipated that the person would die.
Performance: 0 unexpected deaths
Commentary:
There were no unexpected deaths reported for December 2018
34 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Appraisal Rates - Trust
Standard and outcomes:
The purpose of this indicator is to provide assurance that all staff receive an appraisal within a twelve month period, that work objectives are set in alignment with the Trust objectives and that all staff have a personal development plan to support them in their current job role and future development. The Trust’s internal target is set at 95%
Performance: 86.4%
Commentary: Overall performance in December remains below target and unchanged from November’s position. CYPF were relatively unchanged at 90% A 4% improvement in TeMS & Outpatients to 84%. Adults SDG remained unchanged at 86%.
35 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Appraisal Rates – Adult SDG
Standard and outcomes:
The purpose of this indicator is to provide assurance that all staff receive an appraisal within a twelve month period, that work objectives are set in alignment with the Trust objectives and that all staff have a personal development plan to support them in their current job role and future development. The Trust’s internal target is set at 95%
Performance: 86%
Commentary: Overall performance was unchanged from November. Adults SDG remained the same at 86% with Adult SDG – 743 from 862 Appraisals completed. TeMS/OP – 143 from 171 completed. The largest decline in performance were noted at Oswestry MIU 100% last month to 79% this month with 11 staff out of 14 completing their appraisal and ICS Central from 100% to 83% with 10 out of 12 staff completing their appraisal.
36 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Appraisal Rates – TeMS and Outpatients
Standard and outcomes:
The purpose of this indicator is to provide assurance that all staff receive an appraisal within a twelve month period, that work objectives are set in alignment with the Trust objectives and that all staff have a personal development plan to support them in their current job role and future development. The Trust’s internal target is set at 95%
Performance: 84%
Commentary: The target of 95% is not being met however there was a 11% improvement compared to 2 months ago for TEMS & Outpatients with 143 reviews completed out of a possible 171 at the time of this report, notably in Podiatry.
37 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Appraisal Rates – Children and Families SDG
Standard and outcomes:
The purpose of this indicator is to provide assurance that all staff receive an appraisal within a twelve month period, that work objectives are set in alignment with the Trust objectives and that all staff have a personal development plan to support them in their current job role and future development. The Trust’s internal target is set at 95%
Performance: 90%
Commentary: CYP&F Services is relatively unchanged at 90% in December. Hotspot areas are 0-19 Shropshire North and CCN teams. Team leads have provided reassurance that appraisals have been diaries for areas of lower compliance. Leads have reported data is not accurate & have followed up with HR.
38 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Basic Life Support Training (Adult & Paediatric) (CPR)
Standards: 95% of all Trust staff will have undertaken Basic Life Support Training (Adult & Paediatric) (CPR) within the last 12 months
Performance: 89.17%▲
Commentary:
A significant increase in trust compliance this month (+1.29%), resulting in a record higher compliance figure.
39 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Safeguarding Adults – Level 1 Training Compliance
Standards: 95% of all Trust staff will achieve Safeguarding Training Compliance Level 1 (Adults)
Performance: 96.77%▲
Commentary: A modest increase in performance on last month (+0.47%) resulting in another new record high percentage (and number) of employees holding an in-date competence.
40 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Safeguarding Adults – Level 2 Training Compliance
Standards: 95% of all clinical staff will achieve Safeguarding Training Compliance Level 2 (Adults)
Performance: 91.13%▲
Commentary: Another significant improvement on last month’s position and very close to our target.
41 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Safeguarding Children – Levels 2 & 3 Training Compliance
Standards: 95% of all staff requiring Safeguarding Children Level 2 & 3 Training will achieve compliance
Performance: 87.96%▲
Commentary: Although an increase on last month’s compliance rate (+1.94%) improvement is still required to meet next month’s trust target of 93%, and year-end trust target of 95%.
42 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Trust Overall Mandatory Training Compliance
Standard and outcomes:
Mandatory Training measures the percentage of staff compliant with the requirement for core essential training. 95% of all Trust staff will have 100% compliance with their overall mandatory training
Performance: 92.75% ▲
Commentary: A small increase in compliance this month (+0.60%). This also a much improved compliance figure.
43 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Information Governance
Standards: Information Governance
Performance: 93.07%▲
Commentary: There is almost no change in overall compliance compared to last month for IG. All areas remain on track, however the adult SDG have a challenging position to achieve next month’s target due to the adjusted target of 93% to meet year end requirement.
44 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
45 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Well Led
Attendance at work - Trust
Standard and outcomes:
Supporting staff attendance at work - aiming for less than 3.39% of our staff to be absent from work at any one time
Performance: 6.1%
Commentary: This month has seen a deterioration since September’s improved position, largely driven by an increase in anxiety, stress and other mental health issues. In December 2018 these reasons accounted for 1.89% of all available working days, compared to a total sickness rate of 6.16%. As part of the on-going focus on the wellbeing and resilience of our staff, work continues with support initiatives.
46 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Staff absence is measured as a percentage of available Full Time Equivalents (FTEs) absent, Supporting staff attendance at work - aiming for less than 3.39% of our staff to be absent from work at any one time
Performance: Adults 6.56% / TeMS & OP 5.7%
Commentary: Absence Hotspots areas in headcount include Bishops Castle Inpatients 21.05% (a 6% decline from 14.97 % November’s figure). ICS Central 16.98% (previous month 14.88 %) and Stoke Heath YOI 11.41% Anxiety / Stress is the highest absence reason in most teams and continues to rise. Actions taken previously to recruit of a mental health practitioner/wellbeing worker within the occupational health team were not successful and the job description for this role is being reviewed. Mental Health First Aid sessions are planned for early 2019 At Bishops castle hospital a new ward manager is now in place and further work is being carried out with the team to maximise attendance at work. Operational Managers and HR are supporting teams to facilitate staff return to work
47 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Staff absence is measured as a percentage of available Full Time Equivalents (FTEs) absent, Supporting staff attendance at work - aiming for less than 3.39% of our staff to be absent from work at any one time
Performance: 5.6%
Commentary: Hotspot areas in Headcount: 0-19 North Shropshire 17.37% (team headcount 28), 0-19 South Shropshire 12.36% (27), and 0-19 South Telford Cluster 9.99% (22)
48 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Vacancies Timeline including Sickness Rates
The following data was requested by our Clinical Commissioning Group’s (CCG) at the Trust’s monthly Quality meeting with them. The aim is to identify if there is any
correlation between the number of vacancies and the number of staff absences. From the line graphs below you can see that there is a small relationship with a clearer
50 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
ADULT & TEMS SERVICE DELIVERY GROUP RISK REGISTER WITH SCORES AT 12 AND ABOVE
Title of Risk Owner Consequence
(current) Likelihood
(current) Score Management Actions Action by whom &
When? Progress against
Management/
Mitigating Actions
Done
Failure to achieve safer staffing requirements with framework agency staffing solutions necessitating the use of ‘off framework’ agencies.
AM 4 4 16 Twice weekly conference calls and NHSI weekly reports with on-going monitoring.
Standardised processes in place for the administration of temporary staffing solutions by the centralised bank using framework agencies.
To complete a staffing and establishment / skill mix review
A 7day a week Centralised bank
Continuous Recruitment drives in the localities
12 Rotational nurses out to recruitment.
Recruitment to Assistant Practitioner roles completed
Service Delivery Group Senior management Team- On-going Centralised Bank Admin team – on going Deputy Director of Nursing & Quality 5/18 Service Delivery Group manager Service Delivery Group manager Locality recruitment days held during Summer & early autumn 2018 Adult SDG team and HR
On- going Completed and operational now business as usual Completed and approved and posts being recruited to across 4 sites and MIU On-going rolling programme planned 4 Nurses started programme and a further 13 applicants for the posts Fully operational now as business as usual
Completed Completed 1.6.18 December 2018 On going Completed 9.18 Completed for first cohort
51 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Associate Nurse roles being scoped for march 2019
Business case being developed for a march 2019 start 10 places will be recruited
Title of Risk Owner Consequence (current)
Likelihood (current)
Score
Management Actions Action by whom & When?
Progress against
Management/
Mitigating Actions
Done
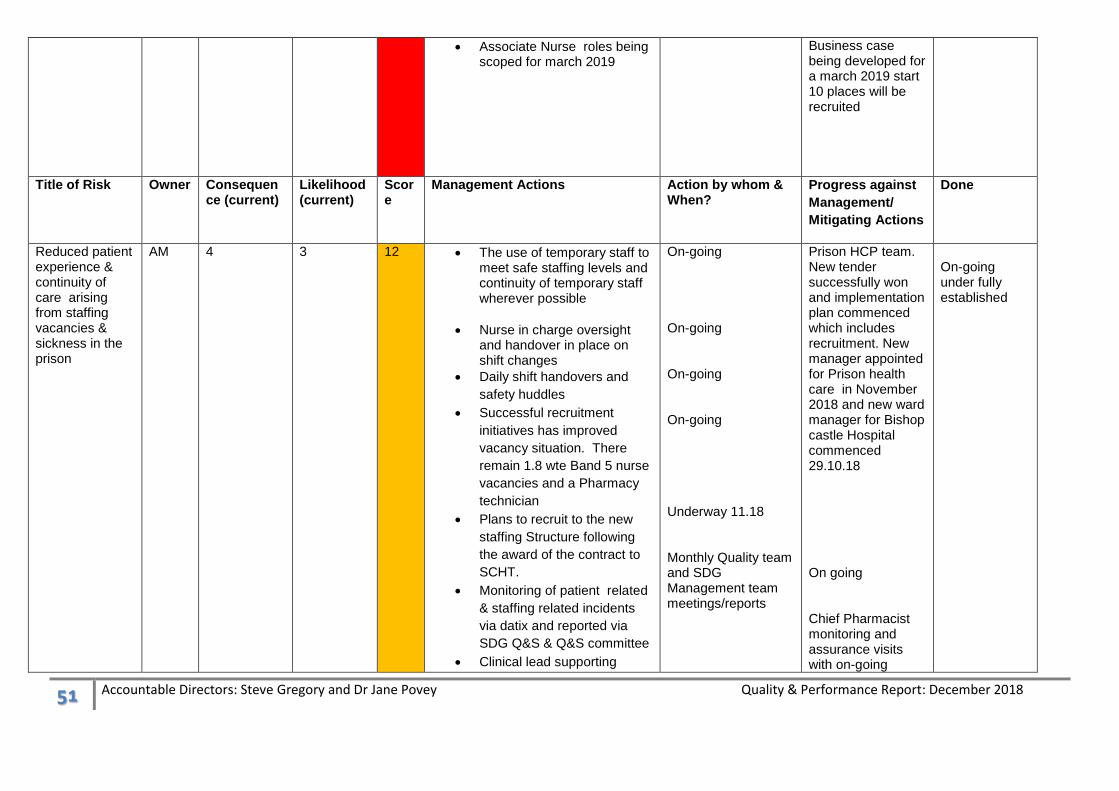
Reduced patient experience & continuity of care arising from staffing vacancies & sickness in the prison
AM 4 3 12 The use of temporary staff to meet safe staffing levels and continuity of temporary staff wherever possible
Nurse in charge oversight and handover in place on shift changes
Daily shift handovers and
safety huddles
Successful recruitment
initiatives has improved
vacancy situation. There
remain 1.8 wte Band 5 nurse
vacancies and a Pharmacy
technician
Plans to recruit to the new
staffing Structure following
the award of the contract to
SCHT.
Monitoring of patient related
& staffing related incidents
via datix and reported via
SDG Q&S & Q&S committee
Clinical lead supporting
On-going On-going On-going On-going Underway 11.18 Monthly Quality team and SDG Management team meetings/reports
Prison HCP team. New tender successfully won and implementation plan commenced which includes recruitment. New manager appointed for Prison health care in November 2018 and new ward manager for Bishop castle Hospital commenced 29.10.18 On going Chief Pharmacist monitoring and assurance visits with on-going
On-going under fully established
52 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Locality Manager and
Medicines management
team with prison work
Medicines management team review prescriptions charts and completing of datix if omitted medications identified
On-going
programme Prison Medicines Governance meetings last one 11.18
Risk of falls resulting in harm for vulnerable patients
AM 3 4 12 Accurate risk assessments to
be carried out within 3 hours
of admission
implementation of Falls
Policy
RCA investigations for all
moderate harm falls &
sharing lessons & action
plans
Review number and severity
of falls each month and
analyse trends
Ensure monitoring of falls
and post falls bundles
Analyse co-relation between
falls staffing and red flag
alerts added to datix forms
Implementation of new ward
handover tool to ensure the
risk of falling is highlighted to
nursing staff
Use of Memory workers to
support Diversional Therapy
All ward staff on-
going
Adult SDG – on
going
On-going monthly
Falls Audit against
NICE quality
Standard
Completed and
action plan to
address gaps
commenced 11.18
On-going monthly-
Review of actions
Review as part of
the falls audit 9/18
February 2019
On going
Falls Task & Finish
group convened to
take the action plan
forward 11.18
Red flags added to
Datix 10.18
On-going monthly
with pilot period
Appointed and
embedded in ward
Completed
53 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Falls Champions link roles
Quality Lead working with
ward managers to create a
‘Falls Map & Clock’ to
support ward learning and
identification of high risk
times /areas
Floor Graphic designed and
procurement process
underway
Falls Task & Finish Group
work stream commenced
Commenced 11.18
Commended 11.18
Commenced 12.18
teams
On-going
Installed but
problems identified
and currently under
review
01/19
54 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Level of acuity &
dependency of
in-patients
increasing. Risk
of clinical care at
times fails to
match patient
acuity/
dependency
levels &
appropriate
treatment
pathways or
interventions are
potentially not
always delivered
in a timely way
AM 4 3 12 Revised standard Operating
procedure in place and
Admission policy
Revised Admission criteria
in place
SBAR/Handover tool revision
and implemented
Datix completion for all
readmissions, measuring
inappropriate transfers.
All ward based RGNs
complete Intermediate life
support training
Revised NEWS2 to be
implemented organisationally
following NHS England
Patient Safety Alert April
2018
All mortality reviews include
a review of appropriateness
of admissions.
Acuity / dependency tool
used as part of admission
documentation
RCA of all significant events
and lessons shared
On-going weekly
monitoring by Senior
Nursing & Medical
Team
Ward staff
Ward staff
Ward staff
Quality Lead & Ward
teams
Mortality Group – on-
going
Ward staff – daily
and Monthly collation
Managers
Rapid alerts and
Lessons learnt group
– monthly as
necessary
Developed and
shared with partner
organisations
On-going and in
use with ward
teams
On-going and
monitoring via
quality team and
service leads
Recovery plan to
achieve compliance
in BLS due 12.18
Task and Finish
Group convened
and work stream
commenced 11.18
Lesson learnt
newsletter and
report shared with
staff and managers
Monitoring via
monthly
performance data
by management
teams and 6
monthly report to
Q&S committee
Reported to Q&S
committee every 6
months
Completed
11.18
Completed
10.18
55 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Title of Risk Owner Consequence (current)
Likelihood (current)
Score
Management Actions Action by whom & When?
Progress against
Management/
Mitigating Actions
Done
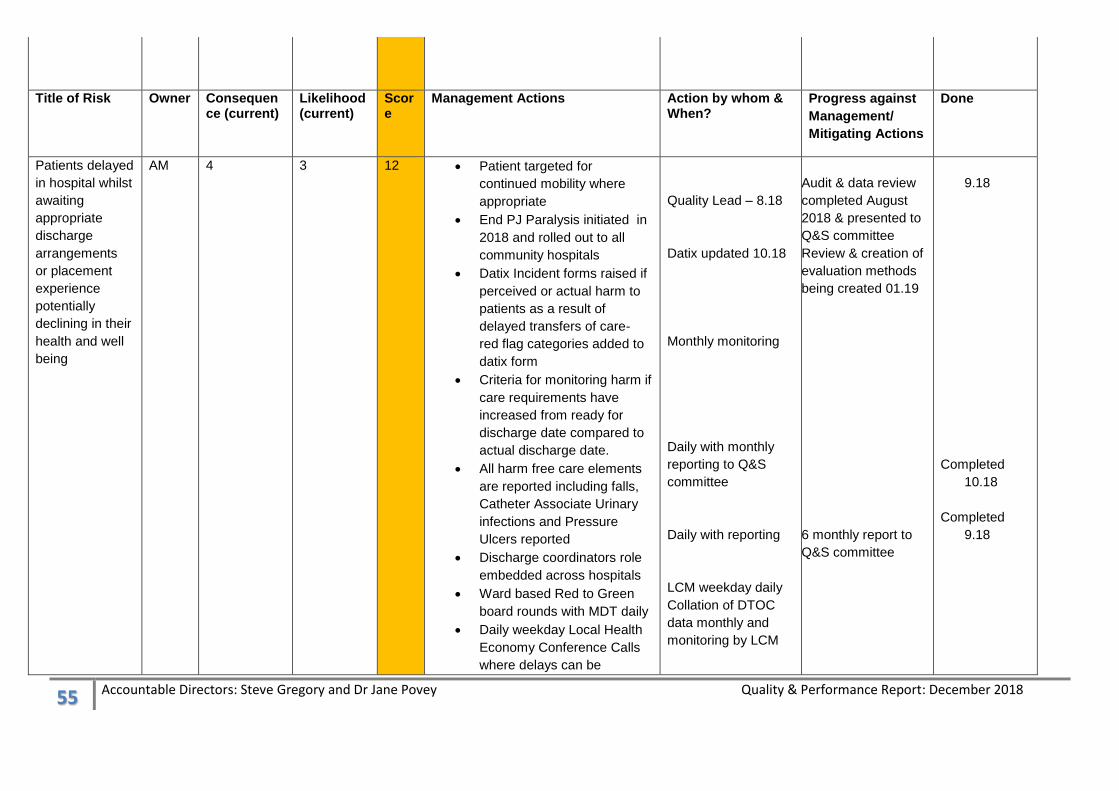
Patients delayed
in hospital whilst
awaiting
appropriate
discharge
arrangements
or placement
experience
potentially
declining in their
health and well
being
AM 4 3 12 Patient targeted for
continued mobility where
appropriate
End PJ Paralysis initiated in
2018 and rolled out to all
community hospitals
Datix Incident forms raised if
perceived or actual harm to
patients as a result of
delayed transfers of care-
red flag categories added to
datix form
Criteria for monitoring harm if
care requirements have
increased from ready for
discharge date compared to
actual discharge date.
All harm free care elements
are reported including falls,
Catheter Associate Urinary
infections and Pressure
Ulcers reported
Discharge coordinators role
embedded across hospitals
Ward based Red to Green
board rounds with MDT daily
Daily weekday Local Health
Economy Conference Calls
where delays can be
Quality Lead – 8.18
Datix updated 10.18
Monthly monitoring
Daily with monthly
reporting to Q&S
committee
Daily with reporting
LCM weekday daily
Collation of DTOC
data monthly and
monitoring by LCM
Audit & data review
completed August
2018 & presented to
Q&S committee
Review & creation of
evaluation methods
being created 01.19
6 monthly report to
Q&S committee
9.18
Completed
10.18
Completed
9.18
56 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
escalated to partners to
facilitate discharge.
Risk of
insufficient
numbers of
substantive
nurses
and/or with
sufficient
skills required to
meet
care needs of
patients and
therefore lead to
harm /poor
patient
experience.
AM 3 4 12 Minimum staffing
establishment agreed and in
place
Staffing levels reviewed daily
Weekly summary of nurse
and HCA fill rates
Other safety indicators and
trends – e.g.. Complaints,
SIs and other harm incidents,
safety thermometer reported
to Q&S and the Board on a
monthly basis.
Monthly reviews of vacancies
and recruitment activity
Internal audit of safe
staffing data/ Acuity reviews
reported twice a year
4 registered nurse rotational
posts for registered recruited
to
On-going Recruitment rolling
programme
Planned timetable of
assistant practitioner and
associate nurse recruitment
Use of centralised bank,
framework agencies
Monitoring of patient &
staffing incidents for staffing
via datix and reported via
Q&S committee
Quality team and Medicines
On-going monitoring
Nurse fill rates
reported to Q&S and
the Board on a
monthly basis
Monthly and
reporting at Q&S
SDG and Committee
Monthly and
reporting at Q&S
SDG and Committee
Bi annual reporting
Locality Managers
Donna Jones LM &
Alison Trumper Dep
DON
On-going
On-going- daily via
datix
Deputy Director of
Nursing & Quality
Agreed & being
operationalized
from 7.18
Reported July 2018
& due again
January 2019
Timetable of
recruitment events
in place
10 Assistant
Practitioners
recruited start end
September 2018
Completed
3 programs
completed by
9.18
57 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
management team
supporting ward teams
Monthly reporting
Inability to
deliver a full
patient service
in TEMS due to
the current
financial position
KT 3 4 A recovery plan in place with
weekly progress updates
monitored by the Senior
team
Provision of a monthly
update to Resource and
Performance Committee
An options appraisal
submitted to R&P for
discussion with the CCG
Karen Taylor On-going
monitoring by SG
lead 12.18
Reduced patient
experience,
delivery of care
to meet needs &
continuity of
care arising
from staffing
vacancies &
sickness
Community
Nursing
Services
AM 3 4 Staffing levels reviewed daily
Monthly summary of nurse
and HCA fill rates
Other safety indicators and
trends – e.g.. Complaints,
SIs and other harm incidents,
safety reported to Q&S and
the Board on a monthly
basis.
Recruitment plans in place
Monthly reviews of vacancies
and recruitment activity
Internal reporting of
cancelled or holding visits
captured via datix
On-going Recruitment rolling
programme
Rotational Nurse post
recruited to
Bank and agency framework
temporary staffing solutions
Daily
Monthly reports
Monthly reports &
analysis
Commenced August
2018 via datix
4 Recruited to and in
recruitment
processes
On going
58 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
used
Monitoring of patient &
staffing incidents for staffing
via datix and reported via
Q&S committee
Senior leadership caseload
reviews commenced in IDT
and
On-going based on
clinical need
Daily via datix and
monthly for trend
analysis
Weekly
Completed 10.18.
On-going
discussion
regarding
recruitment for SE
IDT
Failure to
complete patient
assessment to
identify the risk
of Venous
Thromboembolis
m (VTE) and
bleeding in
community
hospitals leading
to potential
patient harm.
AM 3 4 Staff Notification of
requirements sent
VTE e-learning in place &
monitored via ESR
VTE awareness included on
Trust Induction for all clinical
staff
Review of monthly VTE
reporting and data validation
Updating of VTE policy
VTE awareness programme
and roll out programme to all
existing Nursing staff
commenced July 2018
Nurse Competency
assessments to be
scheduled with medical
teams using a standardised
tool post training
Establish a VTE champion
network
On-going
Monthly & On-going
Final Draft with
Locality Manager
To start Autumn
2018
To start 2019
Progressing and
monitored by VTE
lead 1.19
On- going 1.19
Commenced July
2018
Continues 1.19
Completed 10.18
Underway 1.19
Completed
9.18
59 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
CHILDREN & FAMILIES SERVICE DELIEVRY GROUP RISK REGISTER WITH SCORES AT 12 AND ABOVE
Title of Risk Owner Consequence (Current)
Likelihood (Current)
Score Management Actions
0-19 Public Health Nursing Service (Shropshire) Delivery
NB 4 3 12 Band 3's who do not hold the appropriate qualification/competencies are undertaking an apprenticeship starting Sept 18.
All vacancies have or are in the process of being recruited to.
Continued support for staff from OD team, Head of Nursing & Quality now operationally leading team. Leaders receiving coaching. Staff forum continues. Clear lines of communication in place.
OH, NOSS, HR and one to one support in place. Some long term sickness within the team with appropriate support from HR.
Clearer communication regarding KPI’s and roles and responsibilities in progress.
Paediatric Consultant Staffing and impact on 12 week RTT.
NK 3 4 12 Posts are out to advert and locum cover has been agreed to mitigate recruitment gaps
Prioritise patient caseload most complex patients with highest need seen first
Look closely at individual caseloads to share the work load amongst team – offer flexible work patterns
Get approval for medical locum agency
get necessary development time for senior consultants in team to think creatively about skill mix and to redesign care pathways
Review how appointments are inputted so that it is acknowledged where parents have been offered an appointment within 12 weeks but a later appointment date has been requested.
Improved communication between admin and service lead so that additional clinics can be scheduled to meet service demand.
Referral rates and waiting times Shropshire CDC
AP 3 4 12 Weekly waiting list validation
Monthly review of trends
Risk assessment of each child's needs- agreement about type of assessment
60 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
Sharing information with Paeds and HV to discuss with parents
Sharing information with LA to ensure mitigation re links with special education placements and EHCP processes
Telford 0-19 Public Health Nurse Tender JG 4 3 12 The contract for the 0-19 service in Telford has not been awarded to any of the providers who submitted a bid. We have an opportunity to submit a revised bid in January 2019. This further period of uncertainty could have a negative impact on staff morale leading to increased staff sickness and vacancies with the potential to impact on service delivery.
New tender leadership team to develop revised response to new tender whilst engaging team
Staff are kept informed any changes/updates
Jo Gregory is line manager for team leads and offering one to one support
Continue to recruit to vacant posts to ensure there is enough staff to deliver on current contract
Appropriate support to staff
Lack of availability of Video Fluoroscopy is impacting on care planning
AP 4 3 12 SLT oversight of results using peer review
Liaison with other centres (BCH, GOSH, Newcastle)
Gathering information to ascertain common practices
Liaison with Adult SLT
Unmet Psychological Need HG 3 4 12 There is a need for access to embedded/integrated paediatric psychology service for 24% of all paediatric patients but currently the service is targeted so many children (approximately 900) per annum are not able to access the service they require.
Commissioner led review to be undertaken - initial meetings to meet the psychology team have been arranged. Service Manager and team leader drafting an annual report to support this process.
61 Accountable Directors: Steve Gregory and Dr Jane Povey Quality & Performance Report: December 2018
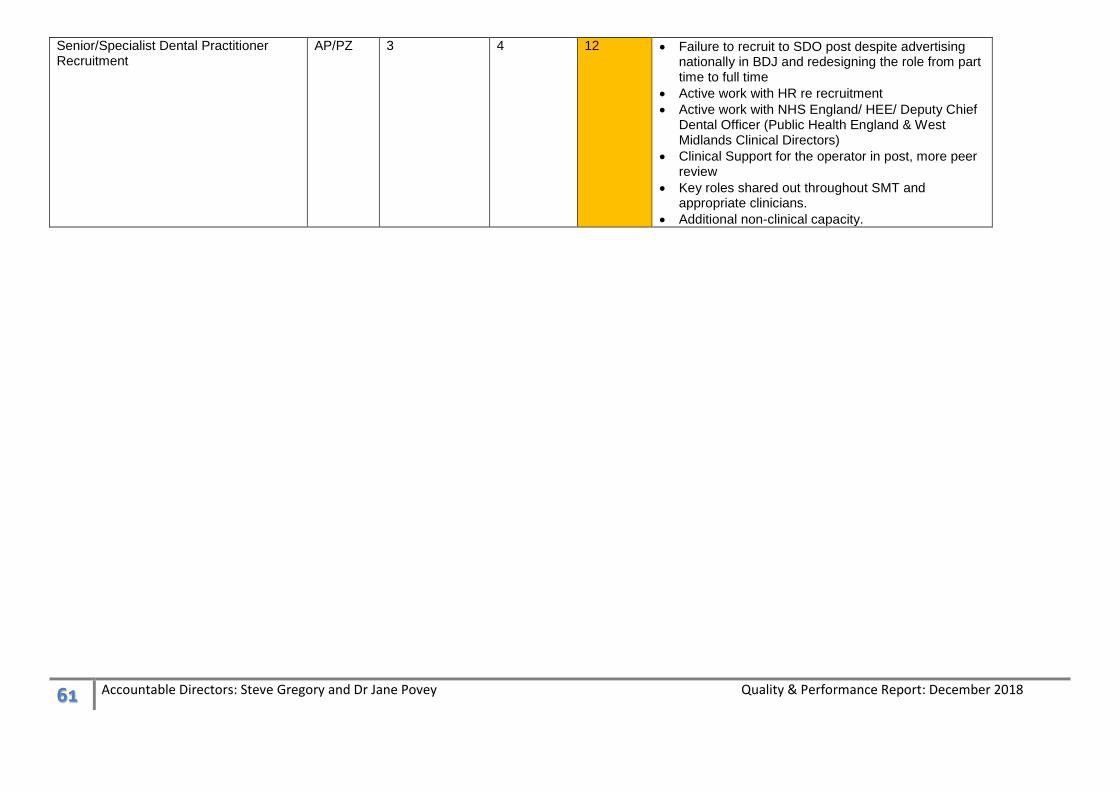
Senior/Specialist Dental Practitioner Recruitment
AP/PZ 3 4 12 Failure to recruit to SDO post despite advertising nationally in BDJ and redesigning the role from part time to full time
Active work with HR re recruitment
Active work with NHS England/ HEE/ Deputy Chief Dental Officer (Public Health England & West Midlands Clinical Directors)
Clinical Support for the operator in post, more peer review
Key roles shared out throughout SMT and appropriate clinicians.